developmental disturbances of oral tissues prf. dr. gamal fatah-allah
TRANSCRIPT

DEVELOPMENTAL DISTURBANCES OF ORAL TISSUES
Prf. Dr. Gamal Fatah-ALLAH

Titles • I- Developmental Disturbances of The tongue. • II- Developmental Disturbances of The Oral mucosa • IV- Developmental Disturbances of The lip.
• V- Developmental Disturbances of The Jaws.1. Agnthia. 2. Micrognathia. 3. Macrognathia. 4. Clefts of the jaws. 5. Torus Palatinus & Torus Mandibularis.
• VI- Developmental Disturbances of The Salivary glands. • VII- Developmental Disturbances of The face.• VIII- Syndromes associated with abnormalities of oral tissues

1- Agnathia
• Extremely rare congenital disorder• Complete or partial (a portion of one jaw)
absence of one or both jaws. • Etiology: – Usually associated with other developmental
malformations in the head and neck.

Clinical Features• In the maxilla, one of the maxillary processes
or even the premaxilla may be missing. • In the mandible, unilateral agenesis of the
mandible, the condyle or the ramus.

2- MICROGNATHIA
• Abnormally small one or both jaws. • Types: – Apparent (not true) due to abnormal positioning
of one jaw to the other or to the skull. – True micrognathia may be • Congenital• Acquired.

Congenital Micrognathia• Associated with other congenital abnormalities in multiple
syndromes including: – Fetal alcohol syndrome– Pierre Robin syndrome: cleft palate, micrognathia & glossoptosis– Treacher Collins syndrome.

Clinical Significance Congenital Micrognathia
It is usually self-corrected during growth.•Abnormal tooth alignment. •Glossoptosis; Posterior displacement of the tongue due to small size of the jaw, no support the tongue:
– May leads to obstruction of the oropharynx.– Obstruction is more liable in the supine position (effect of gravity).

Acquired Micrognathia
• Micrognathia that occur after birth. • Causes: – May result from ankylosis tempromandibular
joint during childhood, which may be caused by trauma or by infection.

3- MACROGNATHIA
• An abnormally large jaw, also called prognathic mandible.
• Etiology: – Hereditary. – Paget's disease of bone. – Pituitary gigantism. – Acromegaly.

Clinical Appearance of Macrognathia
• "Gummy smile" (when maxilla is affected). • Mandibular protrusion. – Ramus of mandible forms a less steep angle with
body of mandible. – Mandibular prognathism caused by excessive
condylar growth. – Chin appears prominent.

Clinical Appearance of Macrognathia
• Macrognathia associated with Paget’s disease of bone.

Macrognathia Caused by Acromegaly
Growth of hands, bony changes alter the patient facial appearance including spacing of teeth.

4- Cleft Jaws• Failure of fusion of the two palatine processes
of the maxilla that form the hard palate. • Cleft palate occurs in about one in 700 to 1000
live births worldwide. • Etiology: similar to cleft lip (multifactorial); – Genetic or hereditary factors– Environmental factors.
– http://www.kck.usm.my/ppsg/histology/DF_28.htm
Pathogenesis of Cleft Jaws
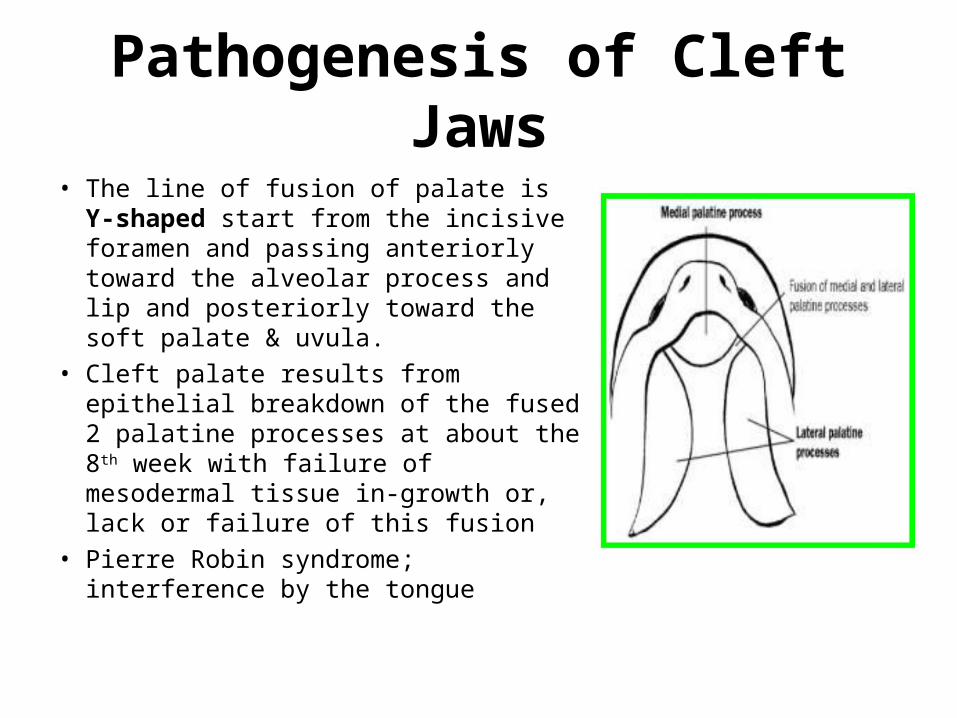
• The line of fusion of palate is Y-shaped start from the incisive foramen and passing anteriorly toward the alveolar process and lip and posteriorly toward the soft palate & uvula.
• Cleft palate results from epithelial breakdown of the fused 2 palatine processes at about the 8th week with failure of mesodermal tissue in-growth or, lack or failure of this fusion
• Pierre Robin syndrome; interference by the tongue

The line of fusion of palate is Y-shaped starting from the incisive foramen and passing anteriorly toward the alveolar process and lip and posteriorly toward the soft palate & uvula.

Classification of Cleft Palate 1. Cleft uvula (Bifid uvula) is the mildest form. 2. Incomplete cleft:
– Cleft uvula & soft palate. – Clefts uvula, soft palate & part of the hard.
3. Complete cleft:– Unilateral cleft: extending from the uvula to the incisive
foramen in the midline and alveolar process unilaterally. – Complete bilateral clefts: involving the soft and hard palate and
the alveolar process on both sides of the premaxilla, leaving it free and often mobile.
4. Cleft lip and palate (50%). 5. Submucosal cleft: is defect in muscle and
sometimes bone of the palate, with intact mucosa.
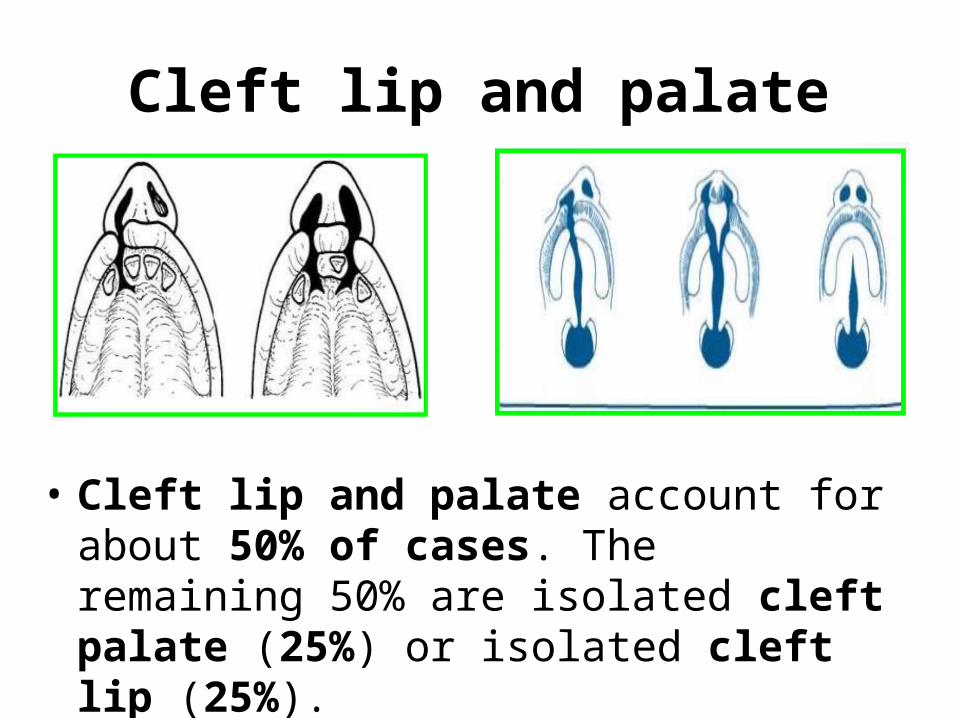
Cleft lip and palate
• Cleft lip and palate account for about 50% of cases. The remaining 50% are isolated cleft palate (25%) or isolated cleft lip (25%).

Clinical Features of Cleft Palate

Complete unilateral clefts Extending from the uvula to the incisive foramen in the midline
and alveolar process unilaterally.
Complete bilateral cleftsSoft and hard palate and the alveolar process on both sides of the premaxilla, (free and often mobile premaxilla).

Cleft lip with Cleft Palate
A. Incomplete unilateral cleft of the lip,
B. Unilateral cleft lip, alveolus, and palate,
C. Bilateral cleft of the lip, alveolus, and palate,
D. Isolated (median) cleft palate.

Submucosal Cleft of Palate
• A defect in muscle and sometimes bone of the palate, while the covering mucosa is intact.

5- Torus Palatinus & Torus Mandibularis
• Nodular protuberances of mature bone. • They are nonneoplastic and rarely a source of
discomfort and of little clinical significance. • Slow growth & asymptomatic • The cause is unknown, but may be hereditary.• Mandibular and palatal tori do not often
occur together in the same individual.

Torus Palatinus
• Sessile, nodular mass of bone that appears along the midline of the hard palate.
• any age but usually appears during 2nd or 3rd decades. • It has a slow growth and is asymptomatic. • It may be nodular, spindled, lobular or flat.

Clinical Appearance of Torus Palatinus

Torus Mandibularis
• Bony exophytic growths along the lingual aspect of the mandible above the mylohoid ridge.
• Solitary or multiple nodular masses (may coalesce).
• Usually bilateral, occurring in the premolar region.
• Sometimes on one side only. • 2nd & 3rd decades.

Clinical Appearance of Torus Mandibularis
The tori are almost bilateral, occurring in the premolar region.

Titles • I- Developmental Disturbances of The tongue. • II- Developmental Disturbances of The Oral mucosa • IV- Developmental Disturbances of The lip. • V- Developmental Disturbances of The Jaws.
• VI- Developmental Disturbances of The Salivary glands.
1. Aplasia.2. Atresia. 3. Aberrancy (Latent Bone Cyst).
• VII- Developmental Disturbances of The face. • VIII- Syndromes associated with abnormalities of oral tissues:

1- Aplasia of Salivary Glands
• Aplasia of any one or group of salivary glands may be, unilaterally or bilaterally.
• The congenital absence of major salivary glands is an extremely rare disorder.
• It becomes manifest with the development of xerostomia and its sequelae.

2- Atresia of Salivary Glands
• Uncommon congenital absence or closure of a duct or tubular structure (failure of canalization or orifice formation)
• It leads to distention of the gland followed by atrophy.
• It may affect the submandibular duct and a cyst (Retention cyst) may develop as a consequence.

3- Aberrancy "Latent or Static Bone Cyst" Stafne Bone Cyst
• Developmental disorder • Ectopic salivary gland tissue inside the
mandible; – Overextension of an accessory lateral lobe of the
submandibular gland during development of the mandible causing anatomic indentation of the posterior lingual mandible.
– Very rarely the sublingual salivary glands in the anterior area of the mandible.

Clinical Features of Latent Bone Cyst
• Asymptomatic, well-circumscribed cystic lesion within the bone, usually below the inferior alveolar canal. Occasionally bilateral

Sialography of Latent Bone Cyst
injection of radiopaque material in the orifice of the salivary gland duct.

Biopsy
Reveals normal salivary gland tissue.

Main Points Discussed in this Lecture• Anomalies of jaws are:• Agnathia is extremely rare, only a portion of jaw is missing. • Micrognathia may be apparent or true. True micrognathia may be
congenital or acquired.• Macrognathia mainly affects the mandible & the cause may be
hereditary, pituitary gigantism, acromegaly or Paget’s disease of bone.
• Cleft palate occur along the Y-shaped line of fusion & may be: affect uvula only- uvula and soft palate-uvula, soft palate and part of hard palate- complete unilateral cleft-complete bilateral cleft-associated with cleft lip or not.
• Torus palatinus is nodular mass of bone occur in the midline of hard palate.
• Torus mandibularis is usually bilateral in the premolar region.

Main Points Discussed in this Lecture
• Anomalies of salivary glands– Aplasia, atresia & aberrancy.
• Aberrancy is the ectopic presence of salivary gland tissue (usually submandibular gland) in the body of mandible that appear radiographically as well defined radiolucent lesion below the inferior dental canal (Stafne bone cyst).