development of the national strategy for community...
TRANSCRIPT

Islamic Republic of Afghanistan
Ministry of Public HealthGeneral Directorate of Preventive Medicine
Communicable Diseases Control Directorate
National Malaria and Leishmaniasis Control Programme
NATIONAL STRATEGY FOR COMMUNITY-BASED MANAGEMENT OF MALARIA (CBMM) IN AFGHANISTAN
(2011-2015)
Table of Contents
1

ACKNOWLEDGMENT:.......................................................................................................................2Acronyms:..............................................................................................................................................3
1. BACKGROUND.................................................................................................................................52. SITUATION ANALYSIS:....................................................................................................................7
Malaria Stratification..........................................................................................................................7Health Care System............................................................................................................................8Review of National Policies...............................................................................................................9Community-based health care............................................................................................................9Malaria treatment guidelines and management of fever..................................................................11
Challenges............................................................................................................................................13Ongoing Community-Based Initiatives in Afghanistan.......................................................................14
Pilot Community-Based Management of Malaria in Badkhshan, Kunduz, and Takhar Provinces. 145. STRATEGIC OBJECTIVES:.........................................................................................................156. Strategic Components:..................................................................................................................15
6.1 Case Management; prompt and reliable diagnosis and effective treatment..........................156.2 Capacity Building (Training of health workers and supervisors)..........................................156.3 Advocacy, community sensitization and education...............................................................156.4 Risk Management Strategy....................................................................................................15Strategic Component #1: Case Management; prompt and reliable diagnosis and effective treatment..........................................................................................................................................................15Strategic Component #2: Capacity Building (Training of health workers and supervisors)...........16Strategic Component #3: Advocacy, community sensitization and education................................18Strategic Component #4: Risk Management Strategy.....................................................................18Procurement, storage and distribution..............................................................................................19Stock management...........................................................................................................................19
7. INSTITUTIONAL FRAMEWORK.................................................................................................208. MECHANISM FOR COORDINATION.........................................................................................20
8.1 The National Vector Born Disease Control Task Force (VBDCTF).........................................208.2 The Provincial Vector Born Disease Control Task Force (VBDCTF)..............................22
9. IMPLEMENTATION PLAN..........................................................................................................22Priorities areas and phased implementation.....................................................................................22
10. MONITORING AND EVALUATION........................................................................................2310.1 Integrated supervision........................................................................................................2310.2 Quality control at point of care..........................................................................................23
ANNEX 1 - Stratification of districts of Afghanistan based on reported malaria incidence rate (2009 data)......................................................................................................................................................28ANNEX 2 - Current contents of CHW kit (2009)...............................................................................35ANNEX 3 - Tally Sheets for CBMM developed in the pilot RDT and ACT community-based project..............................................................................................................................................................38ANNEX 4 - Supervision Check List on ACTs and RDTs for Community Health Supervisors..........39ANNEX 5 Timetable of activities........................................................................................................40ANNEX 6 Budget components and financial gaps (USD)..................................................................42ANNEX 7: CBMM training Curriculum.............................................................................................44
2

ACKNOWLEDGMENT:
The Ministry of Public Health would like to acknowledge the contribution made by all stakeholders working in
the first National Community Based Malaria Management Strategic Planning Workshop, which provided a
forum for deliberations of this plan.
The National Malaria & Leishmaniasis Control Task force experts, CBHC directorate, World Health
Organization EMRO, BRAC, HN-TPO and other partners deserve special gratitude for their invaluable technical
guidance and ensuring that Afghanistan’s National Community Based Malaria Management Strategic Plan is
comprehensive, effective and will have a significant impact in terms of rolling back malaria.
Finally, it is important to note that this Strategic Plan should be regarded as a working document. All comments,
feedback and additional case materials will be considered in future reviews in order to make it more relevant .
Dr. M. Sami Nahzat
NMLCP Manager
3
Acronyms:ACTs Artemisinin Combination Therapy
AMS Afghanistan Mortality Survey 2010
BHCs Basic Health Centres
BRAC Bangladesh Rural Accreditation Committee
CBHC Community Based Health Centre
CDC Communicable Disease Control
CIMCI Community Integrated Management of Childhood Illness
CHS Community Health Supervisor
CHWs Community Health Workers
CQ Chloroquine
EMRO East Mediterranean Regional Office
EPHS Essential Package of Hospital Services
GF R8 Global Fund Round 8
GFATM Global Fund fight against AIDS, TB and Malaria
HMIS Health Management Information System
HN-TPO Health Net- Trans cultural Psycho-social organisation
HPRO Health Protection Research Organisation
HSC Health Sub Center
IEC Information, Education and Communication
IM IntramuscularIMCI Integrated Management of Childhood Illness
LLIN Long Lasting Insecticidal Nets
MoPH Ministry of Public Health
MHT Mobile Health Team
NGOs Non- Governmental Organisation
NMCLP National Malaria and Leishmaniasis Control Programme
NMSP National Malaria Strategic Plan
4

ORS Oral Rehydration Salts
PHC Primary Healthcare
PHD Provincial Health Directorate
PR Principal Recipient
RDT Rapid Diagnostic Test
HSC Health Sub centres
TB Tuberculosis
TDR Tropical Disease Research
UN United Nations
UNICEF United Nations Childrens Fund
USAID US Agency for International DevelopmentWHO World Health Organisation
5

1. BACKGROUNDIt is estimated that the number of cases of malaria rose from 233 million in 2000 to 244 million in 2005 but decreased to 225 million in 2009. The number of deaths due to malaria is estimated to have decreased from 985000 in 2000 to 781000 in 2009. Decreases in malaria burden have been observed in all WHO Regions, with the largest proportional decreases noted in the European Region, followed by the Region of the Americas. The largest absolute Decreases in deaths were observed in Africa. The percentage of reported suspected malaria cases receiving a parasitological test has increased between 2005 and 2009, particularly in the African Region (from 26% to 35%), Eastern Mediterranean Region (47% to 68%) and South-East Asia Region excluding India (from 58% to 95%). Data from a limited number of countries suggest that both microscopy and RDTs are less widely available in the private sector than the public sector. A small number of countries, including the Lao People’s Democratic Republic and Senegal, have shown that it is possible to scale up rapidly the availability of malaria diagnostic testing nationwide, provided that attention is given to adequate preparation, training, monitoring, supervision and quality control (world malaria report 2010). Among females, the leading causes of death are infectious and parasitic diseases 18.3 percent and between men 16.2 percent (Afghanistan Mortality survey, 2010 - Chapter 8 causes of death by age and sex Page: 136)
Malaria is an endemic disease and a major public health problem in many Provinces of Afghanistan. It causes a great burden on the health and economic development of individuals, families and communities living in endemic areas. The total number of reported malaria cases were 414407 in 2006, 390729 in 2009 and 392463 in 2010. Majority of these cases were clinically diagnosed: 79.8%, 83.4 % and 82.0% respectively (HMIS 2010). The Government of Afghanistan remains committed to the control of this disease. For this purpose the Government developed the National Malaria Strategy Plan 2008-2013 with a vision of a malaria free Afghanistan.
The main quality-of-care challenge posed by the recent decline in malaria is now in identifying those cases of fever which are in fact caused by malaria and amongst those malaria cases, identifying and treating the correct species of infection. Most fever in Afghanistan is not caused by malaria (even in the most endemic areas, slide positivity rate is rarely above 30%). Most malaria, in turn, is not caused by P. falciparum, but by P. vivax. Because treatment for these two diseases differs, identification of the species is important for treatment outcomes. In summary, the context for deployment of RDTs should be in improving the treatment of fever at community level and ensuring that those with malaria are a) parasitologically confirmed cases and b) treated appropriately. Appropriate treatment, in this context, means that those with parasites are treated with an effective antimalarial, and those without malaria parasites are appropriately treated with non-antimalarial drugs.
The need to identify the presence or absence of malaria parasites (at species level) in providing treatment lends itself to mixture of diagnostic methods each of which is appropriate to the setting. The choice is between microscopy and RDTs. Microscopy is the preferred method in clinic settings with a relatively high throughput of patients, but is also difficult and expensive to maintain because of the need to monitor quality of the microscopists and relatively high fixed costs (such as microscopes and salaries). RDTs may also play a role at clinic level, in areas where microcopy is hard to maintain, where patient throughput is low, or at times when the laboratory is closed.
RDTs can also be deployed at community level, through CHWs, which may improve access to effective treatments for both malarial and non-malarial causes of fever at community level. Programs to increase access to RDTs also encounter challenges, such as maintenance and monitoring of quality, supply and storage of the RDTs (which are heat sensitive), and in training of CHWs. Despite these challenges, there is hope that RDTs have a role to play in improving diagnosis of malaria and non-malarial causes of fever and through accurate diagnosis, to improve the targeting of effective treatments.
6

Accurate diagnosis of malaria (using RDTs and micrsocopy) is also providing more accurate and higher resolution surveillance data in most settings where they have been deployed (either through clinics to communities). Until now, most data has been based on suspected malaria cases (i.e. where there has been no parasite based diagnosis), which results in a persistent over estimate of malaria burden – for example in Takhar province, in 2009, around 13,000 suspected cases were reported through the HMIS system. In clinics which have microscopy (in the most endemic districts of Takhar) slide positivity rate was <1%. If this figure is applied to the number of suspected cases identified, the true number of cases amongst those suspected cases is of the order of 100-200 cases – 2 full orders of magnitude below the estimates based on suspected cases.
This improved accuracy in surveillance can result in the directing of resources more effectively and in earlier detection of outbreaks and epidemics. It has additional advantages in enhancing the type of intensive surveillance that will be required if Afghanistan officially declares the goal of elimination.
The National Strategy for Community-based Management of Malaria (CBMM) in Afghanistan outlines the basic approach to increase access to diagnostic testing of malaria and effective treatment at the community level in all malaria endemic areas of Afghanistan. It aims at mobilising commitment and resources from the Government of Afghanistan, the implementing agencies and the community themselves, providing a common strategy for concerted action. The development of this Strategy builds on the key policy elements of the National Malaria Strategy (NMSP) of Afghanistan (2009-2013), the Basic Package of Health Services (BPHS) for Afghanistan (2009/1388), and the Community-Based Health Care Policy and Strategy (2009-2013). Currently Afghanistan enjoys a strong partnership amongst Government, UN agencies, funding agencies, and national and international NGOs, which creates an enabling environment for successful malaria control.
The CBMM Strategy aim to progressively expand access to highly effective antimalarial treatment with Artesunate + SP (Sulfadoxine-Pyrimethamine) for the treatment of parasite confirmed falciparum malaria and with chloroquine for treatment of parasite confirmed vivax malaria, guided by the use of combination RDTs at peripheral clinics and at community level. The Phase I (first two years of the project) will focus on consolidation of work in the pilot districts of Northern provinces of Badkhshan, Kunduz, and Takhar involved in the community-based deployment of ACTs and RDTs, and will extend in the districts with the highest reported incidence of malaria, while during its Phase II (years 3, 4 and and 5) the programme will extend to the remaining parts of the country . Within each phase, the first year of implementation will focus on the peripheral health facilities which do not currently have microscopy (BHCs and HSC) and the second year will extend the interventions to Heath Posts at community level. The year 5 (Phase III) will aim at consolidation of the results, with focus on refresher training and improving on the coverage targets.
7

2. SITUATION ANALYSIS:
Malaria Stratification
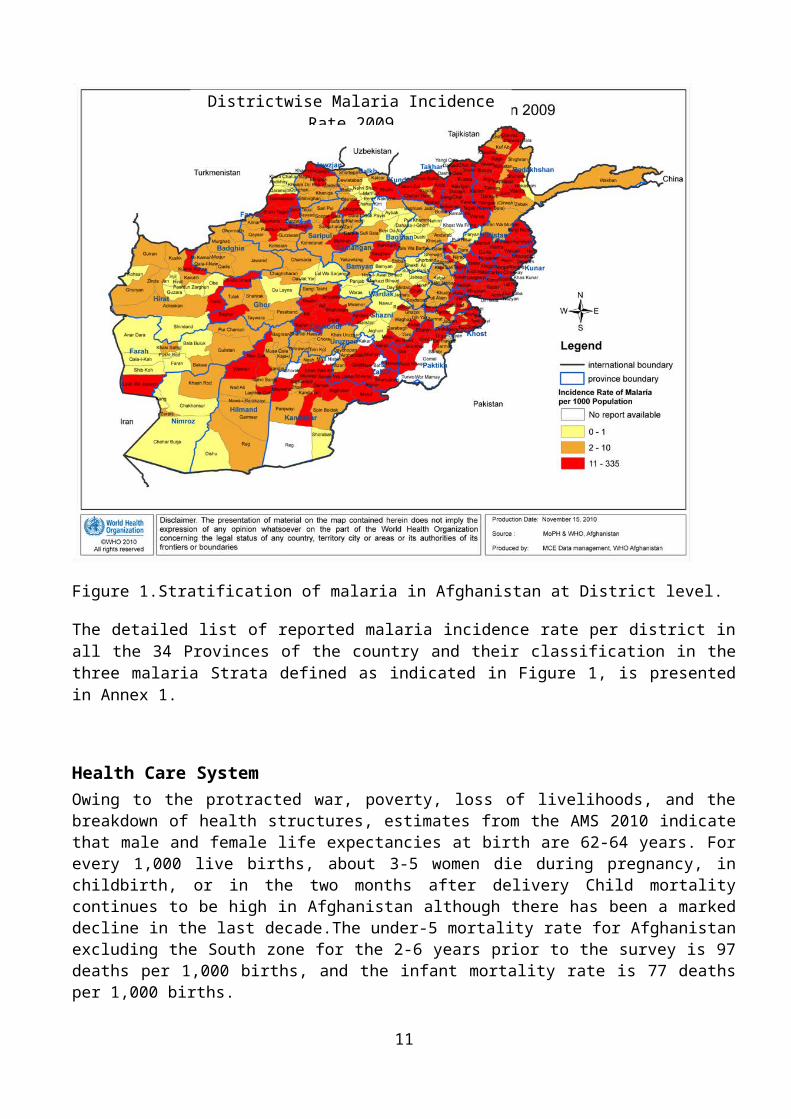
Malaria is endemic in large areas of Afghanistan below 2,000 meters above the sea level and is highly prevalent in river valleys. Major determinates of malaria transmission in the country are altitude and agricultural practices, especially rice cultivation.The risk of malaria transmission in each of the provinces is not homogeneous, and, for this reason, a more accurate stratification of malaria based on incidence of reported clinical malaria per district by BHC and CHC has been used in this document, based on HIMS 2009 data. District in which the reported malaria cases exceeded the median of reported annual malaria incidence rate, i.e. >10/1000, were classified as Stratum 1, those with reported annual malaria incidence rate between 1 and 10/1000 were classified as Stratum 2 and those with reported annual malaria incidence rate of 0-1/1000 cases were classified as Stratum 3. The stratification of malaria at district level using these thresholds is shown in Figure 1 below.
Figure 1.Stratification of malaria in Afghanistan at District level.
The detailed list of reported malaria incidence rate per district in all the 34 Provinces of the country and their classification in the three malaria Strata defined as indicated in Figure 1, is presented in Annex 1.
8
Districtwise Malaria Incidence Rate 2009Afghanistan

Health Care SystemOwing to the protracted war, poverty, loss of livelihoods, and the breakdown of health structures, estimates from the AMS 2010 indicate that male and female life expectancies at birth are 62-64 years. For every 1,000 live births, about 3-5 women die during pregnancy, in childbirth, or in the two months after delivery Child mortality continues to be high in Afghanistan although there has been a marked decline in the last decade.The under-5 mortality rate for Afghanistan excluding the South zone for the 2-6 years prior to the survey is 97 deaths per 1,000 births, and the infant mortality rate is 77 deaths per 1,000 births.The national health policy of Afghanistan aims at providing a standardized package of basic services in all primary health care facilities, as described in the Basic Package of Health Services (BPHS)The Basic Package of Health Services includes six standard types of health facilities, ranging from community outreach provided by CHWs at Health Posts, through outpatient care at Health Sub Centers and Basic Health Centers and provided by Mobile Health Teams, to inpatient services at Comprehensive Health Centers, district hospitals and regional hospital. The section below summarizes the services provided by each type of facility.
Health Posts: At the community level, basic health services are delivered by CHWs from their own homes, which function as community health posts. A health post, ideally staffed by one female and one male CHW, cover a catchments area of 1,000– 1,500 people, which is equivalent to 100–150 families. The CHWs offer basic curative services, including differential diagnosis and treatment of fever as well as a wide array of communicable diseases. Currently no malaria RDTs are available at health post level Except USAID pilot project in North east provinces (Kunduz, Takhar and Badakhshan.
Health Sub Centers: The extremely challenging geography, especially in some parts of the country, the scattered pockets of population, the absence of basic infrastructure such as roads and bridges, ethnic and security issues, etc. all pose difficult questions regarding the establishment of BPHS health facilities based on the number of people covered. A HSC is intended to cover a population of about 3,000-7,000, often residing in remote underserved areas. The HSC is staffed by two technical staff (a male nurse and a community midwife), as well as a cleaner/guard. The HSC provides most of the BPHS services that are available in BHCs. HSCs will refer severe and complicated cases to higher level facilities. The HSCs are not equipped with adequate malaria diagnostic facilities.
Mobile Health Teams: Given all the challenges coupled with the scarcity of trained health workers (particularly females), it may not be feasible to establish staffed fixed centers in some remote areas, where the population is scattered and live in small communities. The principal idea of mobile health services is to establish a limited number of mobile health teams in each province by dividing the province into clusters of districts. The MHT ideally has the following staff, male health provider (doctor or nurse), female health provider (community midwife or nurse), vaccinator and driver. The MHTs are unable to offer just clinical malaria diagnostic services.
Basic Health Center: The BHC is a small facility offering primary outpatient care, immunizations and Maternal and Newborn care. The services of the BHC cover a population of about 15,000–30,000, depending on the local geographic conditions and the population density (can be less than 15,000 where the population is very isolated). The minimal staffing requirements for a BHC are a nurse, a community midwife, and two vaccinators. Mainly BHC offer clinical malaria diagnostic services but some health facilities are equipped with supplies and equipment for malaria microscopy through GF R5, R8 Project.
9

Comprehensive Health Centers: The CHC covers a catchment area of about 30,000–60,000 people and offer a wider range of services than does the BHC. The facility usually has limited beds inpatient care, and a laboratory equipped with microscopes. The staff of a CHC comprises of doctors (male and female), nurses (male and female), midwives, one (male or female) psychosocial counsellor and pharmacy and laboratory technicians. Irregular attendance by the laboratory technicians due to trainings, illness, commitment to other programme related activities, results weakened laboratory diagnostic services. Furthermore, high patient burden and long waiting lists may also limit access to malaria microscopy at CHCs level.
District Hospitals: Each district hospital covers a population of about 100,000–300,000. The district hospital is staffed with a number of doctors, including female obstetricians/gynecologists; a surgeon, an anesthetist, a pediatrician, a doctor who serves as a focal point for mental health: psychosocial counsellors/supervisors; midwives; laboratory and X-ray technicians; a pharmacist; a dentist and dental technician; and two physiotherapists (male and female). HMIS data shows some proportion of malaria cases are diagnosed clinically despite the District Hospitals are equipped with microscopy due to high patient burdens and long waiting lists in the outpatient departments.
Review of National Policies
Community-based health careThe full description of the Community-based Health Care Policy of Afghanistan is provided in other documents1, from only some key elements have been extracted and presented. Community-based health care (CBHC) is the basic strategy of the BPHS, providing the context for the comprehensive interaction between the health system and the communities it serves. Its success depends upon community participation and partnership between the community and the health staff.
The implementation of CBHC recognizes first that families and communities always look after their own health. Religion and cultural norms and beliefs play an important part in health practices, and families are making decisions to maintain health or care for illness every day. In addition, community members understand and have better information on local needs, priorities, and dynamics. The partnership of health services with communities, therefore, has two objectives:
To persuade families and communities to make appropriate use of the health services, promoting health behaviours and social norms;
To accept the guidance and involvement of communities in the implementation of health programs, encouraging them to identify and solve their own problems.
The following principles guide the policy of community-based health care:
CBHC focuses on major health problems for which solutions exist.
The lowest-level health worker can provide essential quality of care.
Health workers are locally identified and recruited.
Health workers are trained incrementally, one skill at a time.
An established list of essential medicines and supplies is used.
Supervision is regular and supportive.
The health worker is accountable to the community.
The community makes a financial or in-kind contribution for the services.
1 Community-Based Health Care Policy and Strategy (2009-2013)
10
COMMUNITY Health facility
CHS
Female & male CHWs
Other influential
people
Private providers
Family Health Action Groups
Community Development
Council(CDC)
Facility Shura-e-SehiCommunity HP
Shura-e-Sehi
Referrals/Reporting
Outreach
Support
Figure 2: Community-Based Health Care System, Afghanistan
VDC
CBHC is not new to Afghanistan; it existed prior to the many years of war and conflict. However, in this period, Afghanistan has reviewed these international concepts and developed an Afghanistan-specific form of CBHC, which was adopted by the Ministry of Health (following the national conference on CBHC of September 2002). The policy on CBHC in Afghanistan is as follows:
1. The community must play the prime role, as community participation is required to ensure both the availability of services and their sustainability. CBHC and related CHWs are community-based and community-owned programs, receiving essential technical and material support from both NGO and MOPH health services channelled through community structures. These channels are often formalized by the establishment of a community health committee made up of representatives from various parts of the community.
2. All levels of the health care system should receive orientation to the principles of CBHC and be trained in responsiveness to referrals from the communities and other responsibilities.
3. The community must fundamentally agree and adopt the standardized CHW job description, with agreement to both preventive and first-level curative activities.
4. Quality training using sequential tasks will take place as close to the community as possible, with national CHW standard curriculum guidelines defining needed competencies but training methods being locally determined.
5. Adequate supervision is to be assured before recruitment and training, preferably provided by the person who does the training.
6. The closest health facility will regularly provide CHWs with a standardized kit of medicines and essential supplies adapted to the local situation and approved for CHW activities.
7. Compensation must be sustainable, with full-time work to be paid and part-time work compensated only by performance-based incentives. When possible, traditional compensation and in-kind contributions will be maintained.
8. Community mechanisms for identifying needs should include also private-sector providers, both traditional and modern.
The Afghan CBHC system is shown in the figure below, which emphasizes the dynamic nature of the system.
The work of the CHWs is overseen by the Shura-e-Sehi. There are two type of Shura-e-Sehi related to the CBHC Program of Afghanistan:
11

Facility Shura o The facility shura works with facility staff to assure the relevance of services to community
needs, and provision of good quality of care and patient satisfaction. Community Shura-e-Sehi
o The community shura provides direction and support to all health-related activities in their community. They select, support and supervise the CHWs in the community; they monitor the community with the CHWs to be able to encourage families to make full use of preventive health services including outreach services; they provide guidance in the adoption and promotion of new behaviors and social norms.
The CHW are identified by the community, among those resident in the area. They are required to be at least 20 year old (and maximum 50 years). Basic literacy is an advantage, but is not essential for the CHW. Women are encouraged to volunteer and be trained as CHW, as the MOPH policy requires that at least 50% of the CHW trainees are women.
The CHWs are volunteers and work part-time. They should be compensated for the services they provide through policies and procedures that are decided locally by communities and the organization that supervises the CHWs. Such remuneration may be in cash or kind, or non-monetary recognition. The CHWs should be compensated for all legitimate expenses (transport and food) when working outside their community. Specifically, approved under this BPHS revision (2009):
Afs100 per month for routine work travel
1. Additional expenses (Afs50) for approved tasks, such as accompanying a suspected TB patient to a facility with a laboratory, or participation to the National Immunization Days and other campaigns.
The CHW is accountable to the local Shura for performance and community satisfaction and technically accountable to the community health supervisor (CHS) assigned by authorities from the nearest health facility. Government will not pay salaries to CHWs, and does not recommend donors and NGOs to do so.
The two types of communities with little or no coverage with CBHC are the urban populations and the nomadic communities. Only few projects have implemented to evaluate the feasibility of different approaches to provide BHC for these populations.
Malaria treatment guidelines and management of fever
The MOPH of Afghanistan has updated the national malaria treatment guidelines and adopted Artesunate + Sulfadoxine/Pyrimethamine as first line treatment of P.falciparum uncomplicated malaria and Chloroquine for P.Vavix uncomplicated malaria but the pregnant women in first trimester with confirmed plasmodium falciparum will be treated with quinine at facility level (see figure 6 ) and Second and third trimester with SP plus AS and for P. vivax with chloroquine. The adoption of ACTs as antimalarial treatment policy was endorsed in the EMRO region in 20032. Afghanistan’s treatment policy was updated in 2009, approved and endorsed by MoPH in October 2010 and will be implemented in all health facilities in January 2011 with the support from the GF R8 grant. 2 WHO (2004) Report of the Third Intercountry Meeting of National Malaria Control Managers, Lahore, Pakistan, 12-15 May 2003. World Health Organisation, Geneva, Switzerland (WHO-EM/MAL/297/E/05.04/140).
12

Chloroquine + primaquine are the standard treatment of P. vivax malaria, while chloroquine is still recommended for the treatment of clinical (unconfirmed) malaria. Artemether /artesunate/IM is the recommended treatment for the management of severe falciparum malaria at health facilities level (HSC, BHC and CHC) as first dose then patient should refer, If referral is not possible, treatment with artemether/ artesunate should continue until the patient is able to receive the medication orally according to the National Malaria Treatment Guideline, Quinine is recommended for treatment of severe falciparum malaria at hospital level. Parasitological confirmation of malaria with microscopy is recommended, but since access to laboratory services is limited, the great majority of cases are still treated on the basis of clinical diagnosis alone.
In order to implement correctly the CBMM strategy, aiming at providing universal access to parasitological confirmation of malaria, specific algorithms for diagnosis and management of fevers suspected as malaria (fever without any obvious cause) will be developed and tested. The standard algorithms provided by WHO (see Figure 3 & 4 below) and Malaria Flow Chart At Health Post Level for the treatment of pregnant women according to the National Malaria Treatment guideline of NMLCP in page 55, will be reviewed and adapted to the specific needs of Afghanistan and also it is requested from reproductive health department of MoPH to add it in ANC guideline.
Figure _3. Algorithm for managing uncomplicated malaria in health facilities
13

Figure _4. Algorithm for managing common childhood illness at community level, as part of the Community IMCI strategy3
Antibiotics, ORS are already part of the CHW kits in Afghanistan and the implementation of CIMCI has already started in several provinces. The CBMM will be fully integrated with the Community IMCI, promoting its implementation for the management of referrals and treatment of malaria, pneumonia, diarrhoea and non-malaria fevers at community level. The introduction of RDT will enable early identification of the non-malaria fevers, which, due to the relatively low prevalence of malaria in most parts of Afghanistan, do represent the large majority of febrile illnesses. It is anticipated that, in addition to identifying cases, this will translate into improved targeting of treatments. Currently, under clinical diagnosis, it is likely that 99%-80% of cases are inappropriately treated with anti-malarials when, in fact, they do not have malaria
Challenges Performance incentive balance for field workers (CHS and CHW)
Health services are supported by a multitude of Partners, creating occasional difficulties for coordinated approaches
Logistic barriers including limited road access to many parts of the country
Lack of clarity over the integration of a historically vertical programme into the BPHS
Low salaries/ incentives for Government staff forcing competent staff to supplement their income through private practice or seek employment in the private, NGO or UN sectors where income is higher
3 Integrated management of childhood illness: caring for newborns and children in theCommunity WHO, 2010* Refer to CHC for anti- relapse therapy of PV with Primaquine
14

Limited mobility of women (as professional staff, health workers, household decision-makers, and patients)
Ongoing insecurity in some areas of the country
Inadequate coverage of population by CHWs
On-going Community-Based Initiatives in Afghanistan
The diagnosis of malaria by CHW is currently based on clinical suspicion of malaria (fever without other obvious causes of fever), and, in practice, treatment is based on the co-administration of Chloroquine. The Basic Pack of Heath Services (BPHS) for Afghanistan does not yet include RDTs and ACTs in the CHW kits which are distributed regularly. Several programmes in the country are already implementing community health programmes, engaging the CHWs. Among the ongoing programmes, the following are:
Family Health Action Group in 9 provinces of the country, with expansion to additional 4 provinces with support from UNICEF. In these programmes the CHWs are trained in providing health education to the community.
With the support of Tech-serve/HSSP there are plans to expand the Post partum family planning program supported by USAID to all 34 provinces of the country.
Additional health education programmes have involved school children from grades 1 to 12 to provide health education to their homes and neighbours.
The comprehensive 6-months training of CHWs has been completed in 10 Provinces. Community IMCI is being implemented in 16 provinces, with plans for expansion in additional 8
provinces. Growth monitoring program is implemented on a pilot level with the support of BASIC and
MoPH/CBHC.
Pilot Community-Based Management of Malaria in Badkhshan, Kunduz, and Takhar ProvincesA community-based deployment of ACTs and RDTs was initiated in the Northern provinces of Badkhshan, Kunduz, and Takhar involving community health workers at health post level. In these provinces the pilot project was implemented by Merlin and CAF (Care for Afghan Families), and involved 300 CHWs working in 150 health posts in 18 Districts. A total of 33 CHS have been trained to supervise the CHWs in these project areas (5 in Badkhshan, 14 in Kunduz and 14 in Takhar).
One pilot project4, was conducted with WHO TDR funding in 2007-8, evaluated the use of RDTs by six CHWs in Nangahar and Kunduz, A second pilot project will start in 20115 to assess the use of RDTs by community health workers using a randomised trial designin Kunduz and Nangahar Provinces.
4 Khohistani K, Nadeeb, S, Leslie T. Home Based Management of Malaria through the BDN (Basic Development Needs) Program in North-East and Eastern, regions of Afghanistan. TDR Final Technical Report, 20085 Health Protection and Research Organisation / ACT Consortium, Afghanistan (LSHTM). Effectiveness of community level deployment of rapid diagnostic tests for malaria in Afghanistan: Cluster Randomised Trial. Trail Protocol (in progress).
15

3. GOAL
To contribute to the improvement of the health status in Afghanistan through theReduction of morbidity and mortality associated with malaria, by involving CHW.
4. STRATEGIC DIRECTION:
To expand access to accurate diagnosis and appropriate treatment for both malaria and non-malarial cases at health post level in all malaria endemic districts.
5. STRATEGIC OBJECTIVES:
Objective of CBMM Strategy are objective of National Malaria Strategic Plan 2009-2013 as below:
To reduce malaria morbidity by 60% by the year 2013
To reduce malaria mortality by 90% by the year 2013
To reduce the incidence of falciparum malaria to sporadic cases by the end of 2013 with a vision to interrupt transmission of PF
6. Strategic Components:
6.1 Case Management; prompt and reliable diagnosis and effective treatment
6.2 Capacity Building (Training of health workers and supervisors)
6.3 Advocacy, community sensitization and education
6.4 Risk Management Strategy
Strategic Component #1: Case Management; prompt and reliable diagnosis and effective treatmentWith the divergence in treatments between vivax and falciparum malaria and relative high cost of ACT compared to chloroquine there is a need for greater emphasis on diagnosis at all levels of the health system; if falciparum malaria is mistakenly treated as vivax treatment failure is assured, and if vivax is treated as falciparum valuable drugs are needlessly wasted. Diagnosis and treatment of malaria should therefore be fully integrated into the general health services. This improves efficiency and coverage and makes better use of limited human and financial resources.
Microscopy should be adopted at the BHC level, with priority given to Stratum 1 districts and selected priority areas in Stratum 2. The estimated number of CHCs and BHCs to be targeted for strengthened malaria diagnosis is 670. Moreover, in epidemic situations and wherever malaria microscopy is not feasible RDTs (COMBO) can be used at the community level to distinguish malaria from other causes of fever. RDTs have been tested in Afghanistan and the decision to implement these as opposed to microscopy will be based on cost-effectiveness analysis. Because symptoms of malaria are non-specific, 70-90% of febrile illnesses submitted to microscopic diagnosis are negative (i.e. slide positivity rates are 10-30% or less). Microscopy & RDT diagnosis are needed to reduce wastage of anti-malarial drugs and to improve management of patients who do not have malaria.
16
ACT has been incorporated into the BPHS as an essential drug and is being used for treatment of confirmed falciparum cases. Vivax malaria should continue to be treated with chloroquine.
Sustained high-quality diagnosis and treatment of malaria (and other diseases) can only be achieved by regular technical monitoring and quality control of microscopy & RDT by Quality Assurance Centres (QAC) of PHD/PMLCPs under direct supervision and coordination through a national quality assurance unit of MoPH/NMLCP.
Targets:
By the end of 2013, 80% of targeted Health Posts in stratum 1 districts will be able to diagnose malaria by RDTs and provide treatment according to NTG
By the end of 2013, 90% of HSCs, MHTs, in Stratum 1 districts will provide high quality RDT diagnosis and treatment according to NTG
By the end of 2015, 100% of HPs, BHCs and HSCs in Stratum 2 and 3 districts will have a continuous supply of ACT+CQ+RDT
Strategic Component #2: Capacity Building (Training of health workers and supervisors)A total of 100 master trainers have been trained already, but the involvement of these trainers will allow to train 17000 CHW + 1700 CHS over 2 years (expected to be trained according to the GFR8 grant agreement) for the following reasons:
Considering the practice to train 20 trainees per batch, in order to train a total of 18'700 health workers (17'000 CHW + 1'700 CHS) over a total 2 year period a total of 935 training courses will need to be conducted. To complete this, working in pairs, the master trainers will need each to run 19 training courses over a period of 2 year
For each health facility 2 health workers should be trained on different periods (in order not to create dysfunctions in the health services), adding complex requirements to the planning and implementation of the training courses.
Finally, the target numbers of trainees (17000 CHW + 1700 CHS) during the 2 years of phase I GF R8 implementation seem disproportionately high compared to the total number of CHW and CHS in the country, estimated at 22'000 and 1200, respectively.
Based on the above, the total training requirements have been recalculated taking into account the number of health facilities to be included in the CBMM (the number of BHCs without microscopy, HSC and HPs enrolled in the CBMM) and the phased plan for implementation of the CBMM programme (see Table 1 below). The number of HPs per district has been calculated from the maximum number of HPs reporting malaria cases per district through the HMIS in the period April 2009 -January 2010. The new HPs will be enrolled over a two years period: for Stratum 1 over years 2 and 3 and for Stratum the HPs will be enrolled over the years 4 and 5. Since the number of active HPs per district may change is number may change over the 5-years implementation of the CBMM Strategy, the training requirements will be reviewed on an annual basis.
Table 1 - Number of health facilities to be involved in the CBMM, during each year of implementation of the strategy
17

Number of Points of Care/Health Facilities enrolled in the CBMM
Year 1 Year 2 Year 3 Year 4 Year 5BHCs
without microscopy
130 - 182 - -
Health Sub-Centers 128 - 333 - -
Health Posts 150 6'465 4'619
From the above Table, the number of trainees has been calculated, taking into account that 2 health workers will be trained for each of the new BHC, HSC and HP enrolled every year. It is assumed that 10% of new trainees will need to be added every year to compensate for drop-outs of health workers trained the previous year (attrition of health workers at various levels).
The supervisors for health workers at BHC and HSC level as well as the Community Health Supervisors (CHS) will also be trained. Their number has been calculated on a ratio of 1/10 per health workers trained.
The minimum number of trainers required have been calculated considering the training courses will be implemented through a single-step Training of Trainers (ToT) approach, considering a ratio of 2 trainers for 22 participants (health workers and supervisors), with the possibility of each trainer to complete 3 training courses over a 4 months periods (during the first 2 quarters of each year). An additional 10% of trainers have been also added in view of possible attrition of trainers as well.
The overall training requirements are calculated as indicated in the Table 2 below.
Table 2 - Number of health workers to be trained, according to the level of implementation of the CBMM
Training requirements
Number trainee and trainers required for the CBMM
Year 1 Year 2 Year 3 Year 4 Year 5Health
workers 516 52 1'087 160 160
CHWs 300 6,496 7,112 5,267 5,082
Supervisors 82 652 755 478 478
Trainers (ToT) 30 239 277 175 175
The standard curriculum of training course for health workers on the diagnosis and treatment of malaria will be 2 days. This will be based on the 2-days training course on RDTs as outlined in WHO training manuals6, plus a full extra day will be devoted to disease management, with specific attention to the 6 How to use a rapid diagnostic test (RDT): A guide for training at a village and clinic level. 2008.The USAID Quality Assurance Project (QAP), University Research Co., LLC, and the World Health Organization (WHO), Bethesda, MD, and Geneva.
18

identification and referral of patients with severe febrile, treatment of uncomplicated malaria with ACTs and chloroquine (for falciparum and vivax malaria , respectively) and patient counselling on when to return.
The training tools for trainers and trainees need to be translated in Farsi and Pashtu, and additional training tools (and time allocation in training courses) will be developed to train the community heath supervisors (CHS). The supervisors, including CHS, will receive in addition to the same 3-days basic training course as described above, also one extra half day training on supervision skills, observation, communication and reporting.
The training of trainers (master trainers) will be of 4 days duration following the curriculum of the WHO Training of Traininers course which has been developed in Yemen. It will include a 3 days for training of trainers on RDT performance, including teaching and communication skills, quality assurance and programmatic/implementation aspects. This will be following by a full day trainining of trainers on the requirements for disease management and half day of training on supportive supervision (refer to annex 7 for the training curriculum)
Strategic Component #3: Advocacy, community sensitization and education
CHS and CHW are conducting "health forum" (2.5 hour) sessions with 10-15 people in the community to share information and education on all aspects related to prevention and treatment of malaria. These education sessions will be repeated at least twice yearly in the communities where the RDTs and ACTs will be deployed as the success of this community-based programme depends on behaviour change for both health providers and consumers.
Strategic Component #4: Risk Management Strategy The implementation strategies in different parts of the country will be reviewed on a
quarterly basis, adapting the deployment of ACTs and RDTs at community according to the changing situation.
The new data of the malaria surveillance from BHCs without microscopy, HSCs and HPs will be used to refine the estimations on expected number of suspected malaria patients attending these facilities and requiring RDT testing.
The emphasis on improved coordination and communication between agencies involved in the implementation of GF R8 malaria grant, with the implementers of BPHS and supporting agencies of CBHC programmes will enable synergies and identification of more sustainable approaches.
Close collaboration and communication between all PRs and GFATM secretariat will enable re-programme of the grant to best serve the need of the population of Afghanistan affected by malaria.
Allowance will be created to adapt the roll-out plan not only on the basis of malaria stratification, as planned, but also on the basis of dynamic factors which may affect access and operations in different parts of the country.
In case the planned high scale-up of implementation of the CBMM strategy at HP level on years 2 and 4 will be operationally not feasible, it is suggested that the roll-out is extended over two years in each phase of the project. Initial priority should be given to districts with higher rates of reporting of falciparum cases.
19

The strong partnership amongst Government of Afghanistan, UN agencies, funding agencies, and national and international NGOs creates an unique environment for implementing effective public health approaches.
Procurement, storage and distribution
Procurement will be done on yearly basis with staggered deliveries at 6-month intervals of both ACTs and RDTs in order to adjust order quantities and allow flexibility in re-scheduling deliveries in order to minimise risks of over-stocks or stock-outs.
Stocks will be kept at the Provincial level and delivery of RDTs and ACTs at Provincial level will be under the responsibility of the Implementing Agencies, i.e. BRAC and HNI-TPO. In principle the ACTs and RDTs should be delivered to the BPHS implementers, in order to avoid the creation of parallel programs. NMCLP Provincial units should be informed of the transfer of diagnostic tests and ACTs from Implementing Agency to the BPHS implementers.
Clear guidelines are needed on management of storage and distribution to maintain the RDTs under cool conditions. The Guidelines on Transport, Storing and Handling Malaria Diagnostic Tests in Health Facilities and at Central and Peripheral Storage Facilities, developed by the USAID/Deliver Project will be adapted, translated in Dari & Pashto and duplicated for use in training and programme support activities.
Supply to BHCs and HSCs will be based on a "pull system", with demand generated by the BHCs and HSCs. The HPs will be receiving the additional supplies ACTs and RDTs+ancillary items (not yet included in the CHW kits) through the CHCs and/or BHCs which are currently supplying the CHW kits. Delivery of ACTs and RDTs will be managed by the BPHS implementers, without creating new parallel systems.
Stock management
The stock management of ACT and RDTs will be the responsibility of the BPHS implementers, after receiving specific briefing on stock management, temperature monitoring and reporting. Quarterly reports on status of stocks will be provided by the BPHS implementers to NMLCP in order to guide possible re-deployment on of stocks (a loan-basis) according to needs. The NMLCP will keep a limited stock of ACT and RDTs for emergency and response at central level - the replenishment of this stock will need re-programming of GF funds.
7. INSTITUTIONAL FRAMEWORK
20

The Provincial Manager, responsible for the malaria team (often including one epidemiologist, two vector control officer, one IEC officer, two technicians), has the main role of coordinating, monitoring and supervising all malaria control activities in the province, and the malaria-related activities implemented as part of the BPHS. He reports to the Provincial Health Director.
The Provincial Project Manager/Focal Point of the Implementing Agency, in close liaison with Provincial Health Director, is responsible for implementation of specific activities of the malaria plan of action in the Province, according to set targets. He/she manages the funds and logistics, and generates specific reports to submit to its funding agencies (to the PR for GFATM-related activities). A LLIN officer, with dedicated staff, is responsible for managing the LLIN distribution campaigns and all related activities, including reporting on these.
The Community-Based Health Care (CBHC) Department does not have Provincial unit/teams responsible for coordinating all activities managed at community level. In certain Provinces this function is performed by the PHC unit, and in other a PHD Coordinating Committee is in place to coordinate all programmes and implementing agencies (NGOs). Implementation of the activities by Implementing Agencies (NGOs) is monitored by the Provincial teams, while the central level is responsible for planning, budgeting, training of trainers, data analysis and interpretation, including data from the HMIS relevant to the project, and processing the reports prepared by Provincial managers.
8. MECHANISM FOR COORDINATION
In order to bring together the many players which are supporting the Ministry of Public Health in the process of rehabilitating the health services, Task Forces are formed in the health sector to provide a forum for discussion, planning and policy making. These task forces play an important role in coordination and have representation from MoPH, WHO, UNICEF, BPHS implementers, NGOs, and other sectors, including multiple stakeholders and funding agencies.
The NMLCP has a task force to coordinate prevention and control activities related to malaria named as VBDCTF (Vector Born Disease Control Task Force), which is operational at both National and Provincial Levels.
8.1 The National Vector Born Disease Control Task Force (VBDCTF) The Vector Born Disease Control Task Force (VBDCTF) aims to promote, design, monitor and
implement malaria and leishmaniasis control within the framework of relevant policy documents (i.e. BPHS, NMSP, EPHS and other relevant policies).
The MoPH is the leading agency if the VBDCTF on issues related to policy and implementation of control of malaria, leismaniasis and other vector-born diseases; all members coordinate closely with the relevant Department of the MoPH, which is the National Malaria and Leishmaniasis Control Programme.
The VBDCTF represents the main technical and policy forum for the control of malaria, leishmaniasis and other vector born diseases in Afghanistan. When possible, all changes in malaria control policy should be approved by consensus by the VBDCTF. In its decision making the
21

VBDCTF reviews the scientific, technical and programmatic evidence before making policy decisions to ensure evidence-based programme implementation.
The VBDCTF promotes the control of malaria, leishmaniasis and other vector born diseases at all levels of government, health sector and other sectors. It also oversees the achievement of the relevant Millennium Development Goals and other nationally approved development targets. It promotes equity in the health sector, particularly concerning the role of women.
The VBDCTF maximises the effectiveness of activities through coordination of activities among all members. It also provides an information and technical knowledge forum for sharing of information and technical updates. It advocates for funding of projects which aim to prevent and control malaria, leismaniasis and other vector-born diseases.
Permanent Members of VBDCTF:
MoPH: Manager Program support coordinator, NMLCP technical advisor, other NMLCP staff as an appropriate.
WHO: WHO Medical Officer, Afghanistan, and other WHO staff as appropriate
NGOs: Health Net-TPO, BRAC, ACTD, HPRO
Non-permanent Members of VBDCTF:
The VBDCTF may invite either permanently, or on ad hoc basis other partners or organisations, such as funding agencies, media, members of other task-force of MoPH, as may be necessary to reach the objectives of the task force.
Mode of Action:
The VBDCTF will meet on the second Wednesday of each month at 10AM. In case of any urgent issue, NMLCP manger may convene the task force before the mentioned date.
The meetings are called and organised by the Manager NMLCP (or his representative).There is no specific budget to cover the cost of the attending VBDCTF meeting in any such cost must be born by the organizations represented by the member.
Decisions will be made by consensus and transparently. In the event that consensus cannot be reached then the permanent members will attempt to achieve consensus. If this fails, then the NMLCP Manager has the final say.
Minutes of the meetings are public documents; they shall be communicated IN DRAFT form to permanent members. Once finalised and approved; minutes shall be communicated to all members, who are free to distribute them as they see fit.
8.2 The Provincial Vector Born Disease Control Task Force (VBDCTF)
22

The same structure established at central level is also present at Provincial level under the coordination of the Provincial Public Health Directorate. At Provincial level the following members contribute to the work of the Task Force:
PHD: Provincial Public Health Director, Provincial Malaria & Leishmaniasis Control Program Manager, Provincial CDC Manager, PHA, Provincial TB Manager, Provincial HMIS Manager, BPHS Implementer.
NGOs: HealthNet TPO and BRAC
9. IMPLEMENTATION PLAN
Priorities areas and phased implementation
The Community-Based Management of Malaria (CBMM) strategy will be implemented in a phased manner during the 5 years period 2011-2015.
Year 1: ACT+CQ+RDT deployment in all BHCs (without microscopy) and HSCs in all Districts in Stratum 1 and in 150 Health Posts (to continue the pilot project)
The continuation of the CBMM pilot project in 150 Health Posts (involving 300 CHWs and 33 CHS), in the 18 districts of Badakhshan , Kunduz and Takhar, will help to consolidate the lessons learnt and guide the implementation of the community-based management of malaria to all Health Posts in all HP of Districts in Stratum 1, in Year 2. Moreover, consolidated experience in the use of RDTs in BHC and HSC will be important to ensure supervision and support to CHW from the same catchment areas involved in these activities.
Year 2: ACT+CQ+RDT deployment in all BHCs (without microscopy), HSCs as well as in all HPs of Districts in Stratum 1
This phased, yet large-scale, deployment of CBMM in years 1 and 2, will allow to acquire experience and data on programmatic requirements for implementation of this strategy in the remaining part of the country. It will also allow to refine supervision and support systems, as well as to improve the cost-effectiveness of the interventions.
The focus on districts with higher malaria burden (Stratum 1) during the first two years of the project will also enable further improvement of the malaria stratification in the country. Since most of the reported malaria cases are only clinical suspected malaria cases (not confirmed by microscopy), this strategy will prioritize the introduction of malaria diagnosis by RDTs for areas where the majority of cases are reported based on clinical diagnosis alone.
The further extension of the CBMM in years 3, 4, and 5 will be phased as described below, up to the total extension of the strategy to the whole country.
Year 3: Same as Year 2 plus ACT+CQ+RDT deployment in all BHCs (without microscopy) and HSCs in all low risk Districts of Stratum 2 and Stratum 3
23

Year 4: Same as Year 3 plus ACT+CQ+RDT deployment in all HPs in low risk Districts (Stratum 2+3)
Year 5: Same as Year 4, with consolidation of results and further increase of coverage targets (see Table 3 below)
10. MONITORING AND EVALUATION
The relevant data collection forms which will used at BHC, HSC and HP levels will be developed by NMLCP in collaboration with HIMS Department to include ACT treatment and testing by RDTs. As much as possible existing data flow and reporting system will be used to monitor the implementation of the programme. Key indicators (outcome and impact) specific for surveys will be implemented to monitor the effectiveness of the programme.
In line with the national malaria control strategic plan (2008-2013) the programme implementation will be monitored on the basis of the data and indicators listed in Table 3, below.
10.1 Integrated supervision
A specific checklist has been developed during the implementation of the CBMM in the pilot districts (see Annex 4). This will be reviewed and adapted for use in the whole programme. The supervision of CHWs will be performed by CHS. While CHS are paid by BPHS implementers, the CBMM implementing agencies (BRAC and HNI-TPO) will cover the additional costs to supervise the CBMM-related activities. Standard reimbursement fees for transport and other activities for both CHS and CHWs will be defined in close collaboration with CBHC and implementing partners.
For the supervision of BHC and HSC, programme supervisors from the Implementing Agencies will be involved, and they will need to receive a specific training to assess the quality of malaria case management in health facilities.
10.2 Quality control at point of care
The main activities to control the quality of RDTs and ACTs deployment at point of care should be part of the supervision visits by CHS and programme supervisors and focus on: 1) conditions of storage; 2) checking temperature monitoring charts; 3) direct observation of health workers in performing the test, interpreting the results, dispensing the treatment and recording the data on case, results and treatment.
Monitoring of the daily max temperature of the warehouses in areas exposed to high temperature will be done before and during the implementation phase. The temperature monitoring charts with minimum-maximum thermometer should be available in all health facilities and warehouses in all places where the daily temperature is expected to exceed 30 °C.
24

Table 3 - Key indicators to monitor inputs, process, outcome of CBMM programm
25

26
No Indicator Formula Source of data
Targets Level Frequency Remarks11 12 13 14 15
1
Number of RDT received in the country by implementing
agencies
Number of RDTs received in the country per year by funding and implementing agencies
Program records
Nationalyearly
2
Number of RDT delivered to BPHS implementers at
provincial level
Number of RDTs delivered at provincial level to BPHS implementers
Program records
Provincial/National Every 6
months
3
Proportion of targeted BHCs and HSCs reporting no RDT
stock outs
Numerator: Number of targeted BHCs and HSCs reporting no RDT stock outs per month Denominator: Number of targeted BHCs and HSCs submitting monthly stock reports on RDT
Malaria Information
System.PMLCP/
BPHS
Provincial/National
Quarterly
4
Proportion of targeted HPs reporting no RDT stock outs
Numerator: Number of targeted HPs reporting no RDT stockouts on tally sheetsDenominator: Number of targeted HPs submitting tally sheets with RDT stocks
Malaria Information
System.PMLCP/
BPHS
Provincial/National
Quarterly
5Number of ACT received in the country by implementing
agencies
Number of ACTs received in the country per year by funding and implementing agencies
Program records
Nationalyearly
6Number of ACT delivered to
BPHS implementers at provincial level
Number of ACTs delivered at provincial level to BPHS implementers (every 6 months)
Program records
Provincial/National Every 6
months
7
Proportion of targeted BHCs and HSCs reporting no ACT
stock outs
Numerator: Number of targeted BHCs and HSCs reporting no ACT stockouts per month Denominator: Number of targeted BHCs and HSCs submitting monthly stock reports on ACT
Malaria Information
System./HMIS
Provincial/National
Quarterly
8
Proportion of targeted HPs reporting no ACT stockouts
Numerator: Number of targeted HPs reporting no ACT stockouts on tally sheetsDenominator: Number of targeted HPs submitting tally sheets with ACT stocks
Malaria Information
System.PMLCP/
BPHS
Provincial/National
Quarterly
9 Numerator: Number of reported malaria cases confirmed by RDT Malaria
The HMIS data flow in relation to malaria reporting at Provincial and Central levels is shown in the Figure 6 below.
Figure 6. Reporting data flow (HMIS and other reporting systems relevant to CBMM)
27

ANNEX 1 - Stratification of districts of Afghanistan based on reported malaria incidence rate (2009 data)Stratum 1 = Districts with reported malaria cases exceeded the median of reported annual malaria incidence rate per district, i.e. >10/1000; Stratum 2 = Districts with reported annual malaria incidence rate between 1 and 10/1000; and Stratum 3 = Districts with reported annual malaria incidence rate of 0-1/1000 cases.
Pop = district population data provided by Central Statistics office (2009); IR = reported annual malaria incidence rate, based on HIMS reports of 2009
Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Badakhshan Baharak 26200 14.5 Arghanjwa 14700 9.6 Eshkashem 12600 1.0
Badakhshan Darayim 56000 35.4 Keren -O- Menjan 8700 1.3
Badakhshan Darwaz 24100 24.6 Khash 34600 6.3
Badakhshan Darwazi Bala 21100 12.7 Kofab 20400 6.4
Badakhshan Fayzabad 59800 85.1 Sheikai 24000 8.9
Badakhshan Jurm 34100 19.1 Shighnan 25300 2.3
Badakhshan Khwahan 15100 47.7 Wakhan 13600 1.2
Badakhshan Kishim 73500 131.8 Yamgan (Girwan) 23400 8.8
Badakhshan Kohistan 15100 22.4 Zebak 7100 1.8
Badakhshan Raghastan 36000 11.9
BadakhshanShar -i- Buzurg 47600 40.5
Badakhshan Shuhada 31400 11.5
Badakhshan
Tagab (Kishmi Bala) 25500 70.0
Badakhshan Tashkan 27200 46.3
Badakhshan Urgo 71300 28.2
Badakhshan Wardug 19900 14.5
Badakhshan Yaftali Sufla 48100 56.4
Badakhshan Yawan 29500 21.8
Badghis Ab Kamari 66900 2.7 Dahana-I- Ghuri 53500 0.2
Badghis Ghormach 50100 5.8 Dih Salah 29100 0.8
Badghis Jawand 71800 3.1 Dushi 60800 0.2
Badghis Muqur 21600 7.5 Nahreen 62800 0.2
Badghis Murghab 88400 2.7
Badghis Qadis 82800 2.4
Badghis Qala-I- Naw 59800 4.3
Baghlan Andarab 23200 4.4
Baghlan Baghlani Jadid 154900 7.3
Baghlan Burka 47900 4.4
Baghlan Khenjan 27700 2.1
Baghlan Pul -i- Hisar 25200 2.9
Baghlan Puli Khumri 188000 1.4
Baghlan Tala Wa Barfak 27500 4.7
28

Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Balkh Khulm 63500 36.6 Chahar Bolak 73600 3.0 Balkh 108400 0.2
Balkh Sholgara 103300 18.3 Chimtal 83500 7.3 Chahar Kint 40500 0.5
Balkh Dawlatabad 95000 1.7 Dihdadi 61300 0.4
Balkh Kaldar 18200 4.3 Marmul 10300 0.0
Balkh Kishindih 44300 4.6 Nahri Shahi 40900 0.8
Balkh Mazari Sharif 326100 1.3
Balkh Shortepa 36000 9.8
Balkh Zari 39900 5.5
Bamyan Kahmard 33100 23.2 Shibar 26800 1.0 Bamyan 75500 0.3
Bamyan Shayghan 21800 19.6 Yakawlang 79500 5.0 Panjab 62000 0.2
Bamyan Waras 99300 0.1
Daykundi Gitti 30500 13.9 Mir amor 57000 8.2
Daykundi Gizab 61400 29.7 Sangi Takht 46100 1.3
Daykundi Gujran 31900 33.0
Daykundi Ishtarlee 43400 12.5
Daykundi Khadir 42400 16.7
Daykundi Nili 37100 16.9
Daykundi Shahristan 60500 15.9
FarahLash -i- Juwayn 25500 15.9 Bakwa 32300 2.2 AnarDara 25300 0.9
Farah Gulestan 39400 4.6 Bala Buluk 65000 0.6
Farah Khaki Safed 27600 2.2 Farah 100600 0.3
Farah Pur Chaman 48600 9.3 Pusht Rod 37000 0.0
Farah Qala-I-Kah 28000 0.3
Farah Shib Koh 21300 0.1
Faryab Balcheraqh 47500 13.2 Almar 63900 1.9 Andkhoy 35300 0.1
Faryab Dawlatabad 44100 15.2 Garziwan 69000 5.0Khani Chahar Bagh 21100 0.0
FaryabKhwaja Sabz Posh 46200 51.0 Kohistan 49600 9.5 Qaramqol 17900 0.3
Faryab Maymana 71500 13.4 Qaysar 129600 7.4 Qurghan 42900 0.2
Faryab Pashtun Kot 171700 21.1
Faryab Shirin Tagab 74100 29.3
Ghazni Ab Band 25000 24.9Bahrami Shahid (Jaghatu) 28900 1.2 Jaghuri 160600 0.2
Ghazni Ajristan 26200 48.3 Dih Yak 44500 1.9 Malestan 74600 0.0
Ghazni Andar 113500 11.3 Ghazni 146200 4.6 Nawur 86000 0.8
Ghazni Gellan 52700 20.3 Giro 33200 6.3
Wali Muhammadi Shahid 18300 0.7
Ghazni Muqur 45700 33.9 Khwaja Umary 17300 6.2
Ghazni Nawa 27100 80.4 Qarabagh 129900 5.4
Ghazni Rashidan 16300 13.2 Waghaz 35100 5.4
Ghazni ZanaKhan 11500 1.6
Ghor Saghar 31600 34.3 Chaghcharan 123100 2.6 Dawlat Yar 29800 0.2
Ghor Charsada 24900 1.2 Duleena 32800 0.3
Ghor Pasaband 86300 2.7Lal-o-Sar-i-I Jangal 101900 0.0
29

Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Ghor Shahrak 54400 5.4
Ghor Teyora 83200 5.6
Ghor Tolak 46900 3.9
Hilmand Lashkar Gah 92700 31.4 Bughran 74200 5.4 Dishu 18600 0.0
Hilmand NawZad 46300 14.4 Garm seir 80000 8.3
Hilmand Washeir 14200 46.5 Kajaki 65000 3.0
Hilmand Musa Qala 53800 5.7
Hilmand Nad Ali 107500 3.8
Hilmand Nahr -i- Sarraj 106500 2.3
Hilmand Nawa-I- Barak Zayi 84600 6.5
Hilmand Reg -i- khan sheen 24000 2.7
Hilmand Sangin Qalah 54400 9.4
Hirat Chishti Sharif 21600 15.4 Adraskan 48900 6.9 Guzara 133600 0.4
Hirat Farsi 27900 21.0 Ghoryan 79600 8.5 Hirat 386600 0.1
HiratKushki Kuhna 41600 23.8 Gulran 85700 7.0 Injil 222500 0.3
Hirat Karukh 57900 6.2 Kohsan 49500 0.8
Hirat Kushk 112700 8.2 Obeh 68800 0.2
Hirat Zinda Jan 52000 5.5Pashtun Zarghun 91200 0.2
Hirat Shindand 162600 0.9
Jawzjan Khamyab 12700 13.4 Aqcha 53900 4.2
Jawzjan Mangajak 39000 27.4 Darzab 44700 3.9
Jawzjan Qarqin 22200 27.6 Fayzabad 37900 5.9
Jawzjan Qush Tepa 21400 34.1 Khanaqa 35800 10.0
Jawzjan Khwaja Du Koh 24500 7.2
Jawzjan Mardyan 35100 4.6
Jawzjan Shibirghan 149500 6.7
Kabul Kalakan 27600 14.6 Bagrami 50500 1.0 Estalif 30600 0.0
Kabul Surobi 50500 20.3 Chahar Asyab 33300 9.0 Kabul 2831400 0.7
Kabul Dih Sabz 49100 5.7
Kabul Farza 19600 2.8
Kabul Guldara 20900 8.8
Kabul Khaki Jabbar 13000 4.5
Kabul Mir Bacha Kot 47600 1.5
Kabul Musayi 21300 4.9
Kabul Paghman 110000 1.2
Kabul Qarabagh 69500 7.7
Kabul Shakardara 74900 2.9
Kandahar Arghandab 56400 16.6 Kandahar 481100 8.5 Shorabak 10400 0.4
Kandahar Arghistan 31300 48.3 Nesh 12200 5.4
Kandahar Daman 31500 42.1 Panjwayi 79200 2.4
Kandahar Khak Reiz 20800 10.5 Spin Boldak 103000 5.4
Kandahar Maroof 30000 10.5 Zhari 78100 1.3
30

Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Kandahar Maywand 53400 14.9
KandaharShah Wali Kot 39400 37.0
Kapisa
Hisa-i-Duwumi Kohistan 40900 17.6 Koh Band 21400 1.2 Alasay 34400 0.6
KapisaMahmudi Raqi 58400 10.8 Kohistan 61900 6.9
Kapisa Tagab 73600 12.0 Nijrab 102300 2.0
Khost Bak 20100 60.9Mando Zayi (Ismayel Khel) 51300 4.2
Khost Gurbuz 23800 16.8 Musa Khel 37300 7.3
Khost Jaji Maydan 21900 86.3
Khost Khost(Matun) 124900 14.8
KhostNadir Shah Kot 29000 21.7
Khost Qalandari 9300 33.8
Khost Sabari 64500 14.6
Khost Shemal 12400 12.6
Khost Spera 22200 17.1
Khost Tani 54200 14.4
Khost Terezayi 40700 11.9
Kunar Asadabad 30000 92.1
Kunar Bar Kunar 20000 143.1
Kunar Chapa Dara 28200 86.4
Kunar Chawki 32500 150.2
Kunar Dangam 15400 138.6
Kunar Dara-I-Pech 49800 71.9
Kunar Ghaziabad 17000 83.1
Kunar Khas Kunar 31800 141.4
Kunar Marawara 18600 39.3
Kunar
Narang (Tara-gn-o-Badil) 27500 149.1
Kunar Nari 25100 87.1
Kunar Noor Gul 28800 120.4
Kunar Sar kani 24800 158.9
KunarShigal O Sheltan 26600 138.3
Kunar Wata Pur 24900 101.4
Kunduz Aliabad 42900 20.3 Kunduz 277900 9.4
Kunduz Archi 76900 28.8
Kunduz Chahar Dara 66800 10.5
KunduzHazrat Imam Sahib 210500 21.5
Kunduz Khanabad 145200 30.9
Kunduz Qalay-I- Zal 62700 13.9
Laghman Alingar 88000 64.9
Laghman Alishing 64900 35.7
Laghman Dawlat Shah 30200 53.0
31

Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Laghman Mihtarlam 124500 47.2
Laghman Qarghayi 89200 45.6
Logar Azra 18500 28.9 Baraki Barak 79600 2.4
Logar Kharwar 23900 17.2 Charkh 40400 2.5
Logar Khushi 21900 2.8
Logar Muhammad Agha 68700 9.0
Logar Puli Alam 96000 2.5
Nangarhar Achin 91200 74.9
Nangarhar Bati Kot 68900 134.7
Nangarhar Bihsud 103400 43.2
Nangarhar Chaparhar 54800 98.3
Nangarhar Dara-I-Nur 36700 36.6
Nangarhar Dih Bala 36700 274.4
Nangarhar Dur Baba 21200 131.9
Nangarhar Goshta 24800 137.8
Nangarhar Hisarak 28000 29.1
Nangarhar Jalalabad 183000 37.4
Nangarhar Kama 69900 67.8
Nangarhar Khogyani 118600 96.4
Nangarhar Kot 47400 179.5
Nangarhar Kuz Kunar 50100 69.2
Nangarhar LalPur 18600 335.2
NangarharMuhmand Dara 40900 205.2
Nangarhar Nazyan 13300 176.1
NangarharPachir Wa Agam 38700 62.6
Nangarhar Rodat 62900 40.3
Nangarhar Sherzad 60300 48.9
Nangarhar Shinwar 54500 72.1
Nangarhar Surkh Rod 109600 13.9
Nimroz KhashRod 23100 1.3Asl-i-Chakhansur 21600 0.3
Nimroz Zaranj 50700 4.0 Chahar Burjak 24100 0.0
Nimroz Kang 20400 0.8
NuristanBarg -i- Matal 14200 49.2
Nuristan DuAb 7100 70.6
Nuristan Kamdesh 23100 30.4
Nuristan Mandol 18000 21.1
Nuristan NoorGram 29400 24.6
Nuristan Paroon 12300 33.2
Nuristan Wama 10000 63.2
Nuristan Waygal 17800 77.9
Paktika Dila 22900 32.0 Barmal 31600 3.2
Paktika Gomal 7000 295.6
32

Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Paktika Jani Khel 21800 26.7
Paktika Mata Khan 22700 30.7
Paktika Nika 11300 112.7
Paktika Omna 11000 86.2
Paktika Sar Hawza 21100 34.6
Paktika Sarobi 11400 54.0
Paktika Sharan 45500 109.2
Paktika Urgoon 50300 58.3
Paktika Waza Khwa 21100 55.0
Paktika Yahya Khel 15800 22.4
Paktika Yosuf Khel 12300 47.7
PaktikaZarghun Shahr 27200 15.4
Paktika Ziruk 17500 14.3
Paktya Ahmadabad 25300 11.0 Chamkanay 45500 7.6 Sayid Karam 58400 1.0
PaktyaDand Wa Patan 24200 84.8 Wuza Zadran 32300 9.3
Paktya Gardez 75300 12.2 Zurmat 97800 9.7
Paktya Jaji 57300 20.4
Paktya JaniKhel 31800 24.7
PaktyaLija Ahmad Khel 20800 26.0
Paktya Shwak 5100 67.5
Panjsher Rukha 20900 13.0 Bazarak 17100 4.0 Paryan 13400 0.7
Panjsher Shutul 9900 14.2 Dara 22700 2.3
Panjsher Uanaba 16300 39.8Hisa-I-Awal Panjsher 36400 2.1
Parwan Bagram 94300 5.3 Ghorband 88100 0.2
Parwan Chaharikar 158800 1.4 Shekh Ali 22400 0.7
Parwan Jabalussaraj 58100 1.9 Surkhi Parsa 37200 0.2
Parwan Kohi Safi 28200 6.8
Parwan Salang 23700 3.3
Parwan Sayd Khel 41500 5.1
Parwan Shinwari 37400 2.9
Samangan Dara-I-Suf Bala 58800 1.1 Aybak 93200 0.8
Samangan Feroz Nakhchir 11900 7.3Dara-I-Suf Payin 65000 0.2
Samangan Hazrat -i- Sultan 37700 4.5Khuram Wa Sarbagh 36300 0.9
Samangan Ruyi Du Ab 41500 0.1
Sari Pul Balkhab 45800 10.1 Gosfandi 51600 4.4
Sari Pul Sozma Qala 45000 19.2 Kohistanat 72800 8.4
Sari Pul Sangcharak 91700 1.6
Sari Pul Sari Pul 140300 8.4
Sari Pul Sayyad 49700 3.0
Takhar Baharak 28100 21.2
Takhar Bangi 31900 34.0
Takhar ChahAb 70800 31.2
33

Province Name
Stratum 1 Stratum 2 Stratum 3District Name Pop IR District Name Pop IR District Name Pop IR
Takhar Chal 25700 25.6
Takhar Darqad 24500 34.4
Takhar Dashti Qala 29100 27.0
Takhar Eshkamish 53700 16.8
Takhar Farkhar 42500 27.8
Takhar HazarSumuch 12500 30.2
Takhar Kalafgan 32000 35.6
TakharKhwaja Bahawuddin 21200 21.0
Takhar Khwaja Ghar 60800 21.2
Takhar Namak Ab 11100 98.7
Takhar Rustaq 149000 45.6
Takhar Taluqan 203300 16.5
Takhar Warsaj 34500 19.3
Takhar Yangi Qala 40200 34.0
Uruzgan Chorah 46500 5.5
Uruzgan Dihrawud 55400 9.0
Uruzgan Khas Uruzgan 51400 1.4
Uruzgan Shahidi Hassas 53700 3.6
Uruzgan Tirin Kot 93200 7.1
WardakChaki Wardak 76800 12.3 Day Mirdad 28200 5.0
Hisa-I- Awali Bihsud 33700 0.2
Wardak Jaghatu 41600 1.5 Jalrez 48200 0.6
Wardak Maydan Shahr 36600 1.0 Markazi Bihsud 108600 0.2
Wardak Saydabad 105700 2.3 Nirkh 51800 0.7
Zabul Arghandab 29700 15.4 Daichopan 35800 6.0
Zabul Atghar 7900 57.3 Mizan 12500 2.2
Zabul Qalat 31900 37.4
Zabul Shahjoy 53200 47.2
Zabul Shamulzayi 23500 49.2
Zabul Shinkay 21400 11.6
ZabulTarnak -O- Jaldak 15600 16.2
34

ANNEX 2 - Current contents of CHW kit (2009)
No Description Strength Unit Quantity New quantity Remarks
I. Monthly-based Expendable items
1 Sol Gentian Violet 1% 50ml/10ml Bottle 1 10-Feb
2 Tab Cotrimoxazole 480mg Tab 150 300
3 Packet ORS Packet 25 50) during the summer Jawza- Sunbullah(
4 Coated tablet Ferrous sulfate +folic acid
)60mg iron +400 ug folic(
Coated Tablet
200 500
5 Tab Chloroquine 250mg 250mg Tab 60 100) during the summer Jawza- Sunbullah(
6 Tab Paracetamol 500mg 500mg Tab 150 500
7 Tetracycline Eye ointment Ointment 3 10
8 Tab Mebendazole 100mg Tab 60 100
9 Tab contraceptive ( Ethinyl estradaiol+levonorgestrol)
Sachet 12 15
10 Tab. Pyrimethamine+Sulfadoxine
Fansidar((
25mg+500mg Tab 12 18 all months and 30(during the summer Jawza-Sunbullah)
11 Condom Piece 100 200
12 Retinol (Vitamin A) 50000 iu Cap 60
13 Multi vitamin coated tab 500
14 Chlorine 500ml Bottle 3
15 Depo Medroxy Progesterone Acetate(DMPA)
150mg Bottle 5
16 Zinc tab 20mg Tab 400
17 plastic bags Small size Small size bags
150g For distribution of medicine
18 Referral card Sheets 100
II. Quarterly -based Expandable items
19 Chlorhexidine solution 5% 500ml Bottle 1
20 Gauze bandage hydrophyl 7.5*10
roll 15 30
21 Leucoplast(2.5*5) roll 1 3
35

No Description Strength Unit Quantity New quantity Remarks
22 Cotton 200gr roll 1
23 Gauze Pad Sterile 10*10cm Piece 3-Oct 30
24 Triangular bandage (handkerchief )
Piece 2 Considering Infection prevention
25 Art paper Piece 2
26 Collared pencils or markers Dozen 1
27 Towel medium size 30*20cm Piece 1
28 Soap Bar Piece 3
29 Permanent Marker Piece 2
30 Pen Piece 3
31 Simple Plastic File Piece 1
32 Pencil Piece 1
33 Note book 100 Pages Copies 1
34 Pictorial Tally sheet Copies 1 Once every six month.
35 sterile Gloves piece 100
36 Pencil sharpner Piece 1
37 Clean delivery kit set 0 4
III. Non-Expendable itemsNote: these items can be resupplied based on assessments or demand by CHWs when old or dysfunctional.
38 Dressing forceps metallic 14.5 cm
Piece 1
39 Scissors Piece 1
40 Sterilizer small size Piece 1
41 Kidney Dish Medium Piece 1
42 Metal square tray medium Piece 1
43 Pot medium size Piece 1
44 Soap dish Piece 1
45 Table spoon Piece 1
46 Measurements glass with ml scale ( metallic)
Piece 1
47 Bag ( locally made cloth)( Piece 1
48 Ruler metallic 30cm Piece 1
49 CHW manual Set 1
36
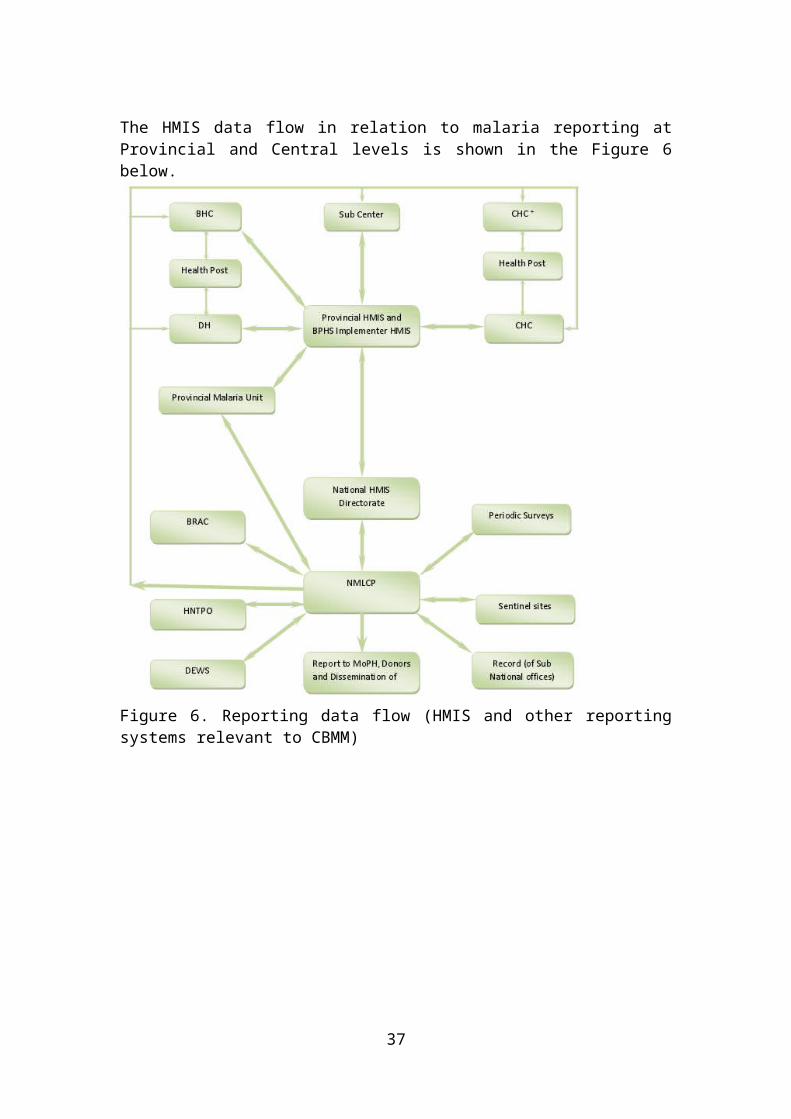
No Description Strength Unit Quantity New quantity Remarks
50 Flip chart ( Paper) material Set 1
51 Educational posters Set 1 Quality assurance process suggest list of IEC materials to be supplied to HP
52 Metallic box (medium) size Piece 1
53 Thermometer (Digital) Piece 1
54 Tape for measuring arm circumference
Piece 1
55 Stop watch/Timer Piece 1
37

ANNEX 3 - Tally Sheets for CBMM developed in the pilot RDT and ACT community-based project
38

ANNEX 4 - Supervision Check List on ACTs and RDTs for Community Health Supervisors
39
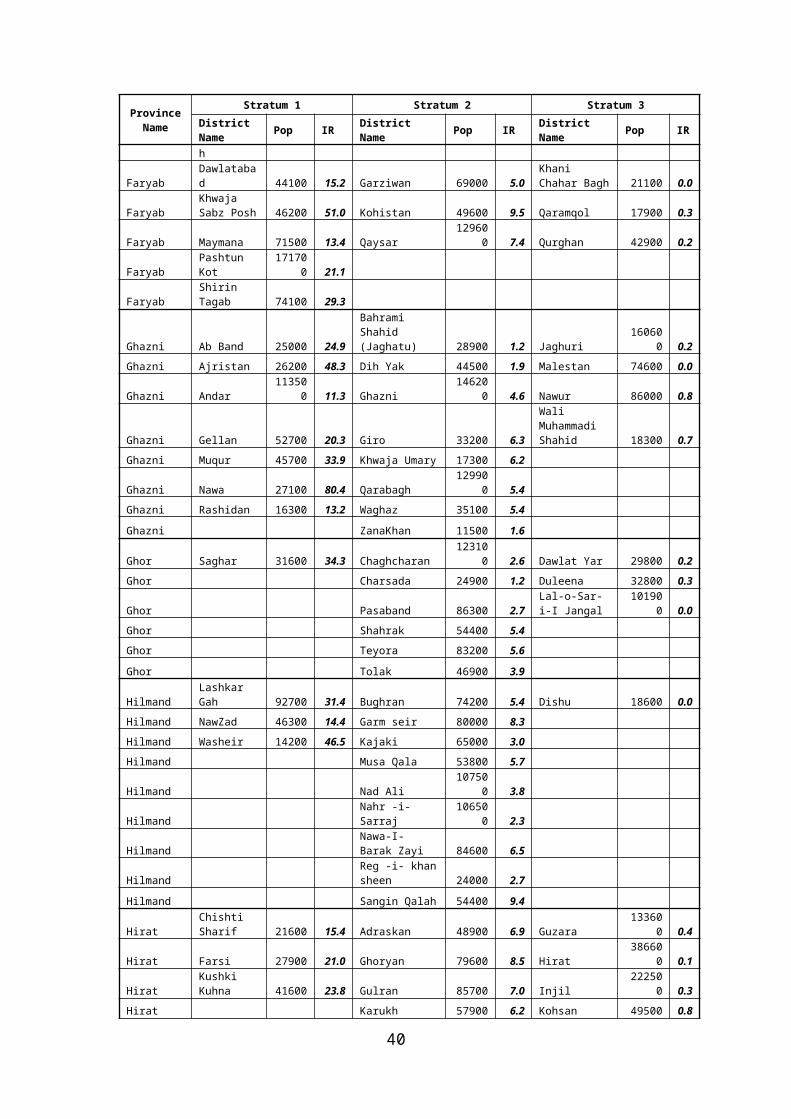
ANNEX 5 Timetable of activities
The quarterly plan of implementation of the activities outlined in the CBMM Strategy is provided in the Table below.
Year 1 Year 2 Year 3 Year 4 Year 5
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Programme planning and management
Writing TORs for malaria CBMM coordinator
X
Appoint malaria CBMMCoordinator
X
Development of Guidelines
Case management of fever
X
40

Year 1 Year 2 Year 3 Year 4 Year 5
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Fever management algorithms
X
RDT quality assurance at point of care
X
RDT transport and storage methods
X
Develop IEC materials X
RDT procurement and logistics
RDT, gloves, sharp boxes procurement
X X X X X
Receive RDTs (staggered delivery)
X X X X X X X X X X
Distribution of RDT and other supplies to the field
X X X X X X X X X X
ACT procurement and logistics
ACT procurement X X X X X
Receive ACTs (staggered delivery)
X X X X X X X X X X
Distribution of ACTs to the field
X X X X X X X X X X
RDT Quality Assurance
Write SOPs and Job Aids for RDTs
X
RDT Post-shipment lot-testing (as appropriate)
X X X X X
Training
Develop training tools for RDTs and ACTs
X
Develop training tools for supervisors
X
41

Year 1 Year 2 Year 3 Year 4 Year 5
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Conduct Training of Trainers courses
X X X X X
Training of health workers and supervisors
X X X X X X X X X X
Communication
Community sensitization X X X X X X X X X X X X X X X X X X
Supervision
Regular supervision X X X X X X X X X X X X X X X X X X
Monitoring and evaluation
Review record forms and procedures
X
Monitoring outcome indicators
X X X X X X X X X X X X X X X X X X
Operational Research
Introduction of RDTs in DH and CBC
X X X X
Evaluating incentive schemes for CHWs
X X X X
Malaria treatment seeking behaviour
X X X X
ANNEX 6 Budget components and financial gaps (USD)
The annual budget (in USD) for the main activities outlined in the CBMM Strategy are presented in the Table below. Funding for commodities which are already supplied by BPSH are not included, i.e. for the procurement and distribution of chloroquine, primaquine and antibiotics for the management of non-malaria fevers of bacterial origin. The funding gap has been calculated only for years 1 and 2, in view of the firm commitment from the GFR8.
Activity Year 1 Year 2 Year 3 Year 4 Year 5
Development of Guidelines
Guidelines for RDT transport and storage
10,000
Fever management
5,000
42

Activity Year 1 Year 2 Year 3 Year 4 Year 5
algorithm
Supervision checklists and temp. charts
5,000
RDT procurement and supply management
RDT, gloves, sharp boxes procurement
111,350 171,982 284,228 389,978 389,978
Distribution of RDT and other supplies to the field (10%)
11,135 17,198 28,423 38,998 38,998
ACT procurement and supply management
ACT procurement 11,329 17,497 28,918 39,677 39,677
Distribution of ACTs to the field (10%)
1,133 1,750 2,892 3,968 3,968
RDT Quality Assurance
Post-shipment lot-testing of RDTs (as appropriate)
100 100
Training
Instructions and training manual for supervisors
5'000
Training of trainers 4,620 36,805 42,644 26,991 26,991
Training of health workers 4,896 42,982 42,670 32,559 31,452
Training of supervisors 574 4,563 5,286 3,346 3,346
Communication
Community sensitization(health forum)
3,000 129,300 129,300 221,680 221,680
Supervision
Regular supervision 4,920 38,880 12,660 29,880 44,220
Monitoring and evaluation
Develop record forms, survey procedures
10,000
Health facility survey for outcome indicators
5,000 5,000 5,000 5,000 5,000
OR: introduction of RDTs in DH and CBC
20,000
43

Activity Year 1 Year 2 Year 3 Year 4 Year 5
OR: evaluating incentive schemes for CHWs
25,000
OR: malaria treatment seeking behaviour
20'000
TOTAL FUNDS REQUIRED
188,057 486,056 607,021 792,077 805,310
BUDGET AVAILABLE (R8 GF malaria)*
392,573 656,528 551,610 565,313 579,701
FINANCIAL GAP -204,516 -170,472 55,411 226,764 225,609
* calculated from approved funding Global Fund R8 malaria grant
The total core budget required to implement the 5 years strategy is USD 2,878,521. Considering the total funding available to implement the GF R8 grant, amounting to USD 2,745,725 the funding gap amounts to USD 132,796 for the 5 years implementation of the CBMM Strategy.
ANNEX 7: CBMM training CurriculumContents
1. Background2. Introduction of CBMM
What is CBMM What CBMM offers Why CBMM CBMM providers Components of CBMM Why CHW training on CBMM
3. Necessity of the curriculum 4. Contents of the curriculumChapter one:General information about malaria
What is malaria Signs & symptoms of malaria Causative agents of malaria Vector of malaria Mode of transmission of malaria Diagnosis of malaria Prevention of malaria
Chapter two:Introduction of RDT
What is RDT Advantage and disadvantage of RDT Procedure of RDT use Storage of RDT
Chapter three:Practical use of RDT
Technique of blood collection from patient’s finger Use of RDT for malaria diagnosis Interpretation of the result of RDT
Chapter four:
44

Treatment of malaria Introduction of ACT Treatment of malaria by using ACT flow chart of Malaria treatment
Chapter five:Sessions of the training
Objective of the session Methods of lesson Topic of the session Materials
Annex1. Annex a - Instructions for the training2. Annex b – Training schedule3. Annex c- Pre-test4. Annex d- Post-test5. Annex e- pictorial instruction for RDT use6. Annex f- Malaria Treatment Dosage Chart 7. Annex g- RDT follow up tally sheet8. Annex h- RDT monthly Aggregated report9. Annex i- ACT use tally sheet10. Annex j- Monthly report on ACT use11. Annex k - Referral form
Background
Malaria is an endemic disease and a major public health problem in many Provinces of Afghanistan. It causes a great burden on the health and economic development of individuals, families and communities living in endemic areas. The total number of reported malaria cases were 427,743 1n 2006, 390729 in 2009 and 390121 in 2010. Majority of these cases were clinically diagnosed: 79.77%, 83.40% and 80.04% respectively(HMIS 2010). The Government of Afghanistan remains committed to the control of this disease. For this purpose the Government developed the National Malaria Strategy Plan 2008-2013 with a vision of a malaria free Afghanistan. Two priority targets mentioned in NMSP 2008-2013 include:
By the end of 2013, 60% of targeted Health Posts will be able to diagnose malaria by RDTs
By the end of 2009, in order to strengthen malaria control at the community level, the NMLCP and all PMLCPs will have a Community-Based Component including Home Management of Malaria (CBMM)
Introduction of CBMM-
What is CBMM (Community Based Management of Malaria)It is a care delivery strategy at community level to diagnose and provide effective treatment for uncomplicated plasmodium falciparum malaria which will reduce the burden of morbidity and mortality due to malaria in endemic areas.
What CBMM offers?At present at health post level CHWs have Sulfadoxine Pyrimethamine and Chloroquine in their kit to treat malaria. CHWs are treating malaria without any confirmed diagnosis. CBMM approach will include RDTs and ACTs in their kits along with SP and Chloroquine. RDTs will be used for rapid diagnosis of malaria and ACTs will be used to treat confirm uncomplicated falciparum malaria cases.
Why CBMM?
The Government of Afghanistan is committed to provide health care services to the entire nation to improve the health condition of the people. But unfortunately in some geographical areas communities are remotely located from the health facilities limiting access to health services. During 2010, 31,2267 malaria cases were clinically diagnosed throughout Afghanistan from which 137,670 cases i.e. 40.08% were clinically diagnosed at health post level. Therefore CBMM will play a pivotal role in confirming malaria diagnosis at health post level up to households. This will limit the excess use of Chloroquine & SP as well as prevent resistance (plasmodium falciparum) to Sulfadoxine Pyrimethamine. In addition to
45

the treatment, CHWs will be able to differentiate the severe cases and refer to health facilities for proper management. This strategy will assist weak health care systems, where women and children cannot reach health facilities and where self-treatment is common and often misguided.
CBMM providers:
Community Health Workers will provide specific health care services (diagnosis using RDT and treatment via ACT) at health post level.
Community Health Supervisors will monitor and supervise activities of the CHWs
Component of CBMM Diagnosis of malaria by using RDT test Treatment of uncomplicated Plasmodium falciparum malaria by ACT
Why CHWs training on CBMM?A health post operates as a basic health service is delivered by the CHW. This grassroots level health service delivery point is ideally staffed by one male and one female CHW. CHWs provide care to an average of 27% of the total number of outpatients visiting the health facilities (2008). The numbers of outpatients have increased with the expansion of health posts as a result of which over the past two years, the numbers seen per health post have increased by 50%. Unlike health facilities, there is no decline in visits during the winter months, 40% - 45% of childhood illnesses are managed by CHWs. (CBHC Policy and Strategy, Page 9), highlighting the importance trained CHWs contributes towards malaria diagnosis and treatment at community level.
Why this curriculum?
This curriculum is developed for training CHWs & CHS on CBMM. As mentioned above the Government of Afghanistan is committed to control malaria in Afghanistan. Introduction of RDTs for early diagnosis of malaria and establishment of CBMM at community level are key interventions that will reduce morbidity and mortality of malaria. This curriculum will help to enhance their knowledge about malaria as well as it will build their confidence to introduce RDT for early diagnosis and ACT for treatment of falciparum malaria at community level.
Chapter one:General information about malaria & approach to a malaria suspected patient
What is malaria- Malaria is a vector borne parasitic febrile communicable disease.
Symptoms of malaria The main symptom is fever Fever may result in chills Fever appears at the same time of the day Fever disappears with sweating After the disappearance of fever individual feels well/ healthy Other signs and symptoms of malaria are:
Headache Joint and body pain Shivering Vomiting Diarrhoea (especially in children)
Causative agent of malaria: Malaria is caused by a parasite called Plasmodium. There are four main types of Plasmodium.
These are- Plasmodium falciparum (Pf) Plasmodium vivax (Pv) Plasmodium malariae (Pm) Plasmodium ovale (Po) In Afghanistan Pv is more prevalent than Pf
Vector of malaria: Female anopheles mosquito is the vector of malaria
46

Mode of transmission: Female anopheles bites a malarial patient and gets Plasmodium with blood This infected mosquito bites a healthy individual and introduces Plasmodium into the blood. Malaria undergoes a sexual cycle inside the infected individuals After a period of time the healthy individual suffers from malaria
Figure: Mode of transmission of malaria
Diagnosis of malaria: malaria can be diagnosed Clinically By microscopic examination of blood of the suspected person By using RDT (Rapid Diagnostic Test)
Prevention of malaria:
There are three main ways in which we try to reduce the spread of malaria: Treat people who are sick with malaria quickly so that the microorganisms cannot be sucked
up by a mosquito, Reduce the numbers of mosquitoes by controlling their breeding sites, and Preventing mosquito bites by using bed nets with insecticide.
The most effective method is the use of long lasting insecticidal nets.
47

Approach to the patient:Step 1. Register the patient. If the CHW is illiterate the family member or patient or patient’s family member will help to register the patient.Step 2. Please follow the procedures
1. ASK about : ( ask the patient or guardian in case of children) The chief complaints: fever, headache, earache, throat pain, chilling, vomiting, cough,
breathing difficulties, burning micturition. Present illness: explanation of the above symptoms eg patient complains of fever and CHW
must enquire after the fever history Past history of the complaints: History of body feeling hot within 2-3 days, duration of the
symptoms History of past illness: history of past episode of fever, malaria etc
2. LOOK: Observe the appearance- ill looking/ unconsciousness/ drowsiness/ stable3. FEEL: Use the back of your palm to check if the patient’s forehead feels hot4. Inspect the patient for : (more emphasise in case of children) Ear discharge ( ask about ear pain) Infection of the skin Fast breathing / breathing difficulties Sore throat ( ask about throat pain)5. TEST Measure body temperature with thermometer from armpit (≥37.5°C/99.5° F or above) if the
patient has fever Use RDT (if needed)
Action to be taken By CHW:1. If the patient’s symptoms are similar to that of malaria and his/her condition is stable without
any danger sign, use RDT. Treat the patient with ACT or Chloroquine if the result is positive for the malaria test. Give the first dose instantly.
2. Refer the patient with danger signs to the nearest health facility.
The danger signs are: He/she is uunable/unwilling to drink or feed (breastfeeding for children) He/she vomits everything History of convulsions Presence of Lethargy / drowsiness / unconsciousness she is severely anaemic 3. Refer the patient of less than 5 months age with RDT positive result to the nearest health
facility. 4. Refer the pregnant women (1st trimester) with RDT positive result to the nearest health
facility.
N.B. Please follow the malaria flow chart and treatment guideline.
48

Chapter TwoIntroduction of RDT
What is RDT (Rapid Diagnostic Test)RDT is a malaria diagnostic device that detects malaria specific protein (antigens) which is produced by malaria parasites. It has
• Space A for buffer• Space S for blood sample• Window C for control• Window test for Pf or PAN (Plasmodium another- P. vivax, or P. malaria or P. ovale) result
Advantages of RDT:
No need for laboratory facilities Easy to carry Simplicity and rapidity of the tests. No need for electricity or laboratory equipment. Minimal requirement for training (basic skills acquired in 1 day). Acceptable levels of sensitivity and specificity, and
Disadvantages of RDT:
More expensive than microscopy. Prolonged positive result after effective treatment. Storage conditions of RDTs
Procedure of RDT use:
1-Prepare the materials needed• RDT • new, unopened lancet• Alcohol swab • disposable gloves• timer or watch• Safety box• Pencil or marker for labeling the RDT• Record book and pen for results
Take time to explain briefly to the patient what you are going to do2- Check - Expiration date of the RDT - Colour of desiccant DO NOT use expired damaged RDT or if there is a sign of exposure to humidity!3- Wear disposable gloves.Doing the test (1)
1) Open the RDT packet and take out device just before use 2) Label RDT with patient’s name or ID before doing the test3) Clean the patient’s finger with an alcohol swab and let it dry before doing a finger prick4) Discard used lancet immediately in the safety box 5) Touch the surface of the blood with the collecting tube/device to get 5 m L of blood DO NOT collect too much blood as this may affect the test result
6) Slowly deliver the blood from the collecting tube onto the sample wall (S) 7) Discard the used blood collecting tube immediately in the sharp box 8) Invert the buffer bottle vertically and slowly dispense the required number of drops into the buffer well (A)
49

9) Wait for the prescribed time (e.g.15-20 minutes) before reading the results Storage of RDT:
• Keep RDTs in the coolest part of the room, but never freeze them. They do not need refrigeration
• Protect RDTs from excessive heat (Keep it within 40-300 C)• Store away from direct sunlight• Do not store close to a wall or ceiling, as both absorb heat during the day• Store a minimum of 30 cm away from walls and ceiling• Do not store directly on the ground• To reduce damage from moisture, water, and pests, store on a shelving unit or shelf, if
possible
Chapter Three:Practical use of RDT
Technique of the blood collection: Take alcohol swab and clean the patient’s finger Let it dry before the pricking Open the lancet Prick the finger with lancet Discard the lancet in to the sharp box Swab the first drop of blood Press the pricked finger for second drop of blood Touch the surface of the blood with the collecting tube to get 5 m L of blood Slowly deliver the blood from the collecting tube on to the sample wall (S) Discard the used blood collecting tube immediately in the safety box
Practical use of RDT: Participants will follow the instruction of RDT use (mentioned above) They will follow the given Pictorial procedure of RDT use They will apply on patients Otherwise they will form groups and do the practical on each other.
Interpretation of the result:• Invalid result (the test device is invalid):
a. No line in the control window orb. No line in the control & test window
• Valid result( the test device is valid):a. Red line only in the control window orb. Red line in the control & test window
• Negative resulta. Red line in the control window andb. No line in the test window
• Positive resulta. Red line in the control window andb. Red line in the test window
Interpretation of positive result:
50
Picture of RDTs with result mentioned above
Picture of RDTs with result mentioned above
Picture of RDTs with result mentioned above
Picture of RDTs with result mentioned above

a. Red line in control window & in Pf line of test window – Pf malaria caseb. Red line in control window & in PAN line of test window – Pv malaria casec. Red line in control window , in Pf line & PAN line of test window – mix infection
After doing the test1) Discard used gloves, swab, and desiccant in a non-sharp waste container 2) Keep used RDTs in the box. Return used RDTs for replacement with new RDTs 3) Record results in the register.
Chapter Four:Treatment of malaria
What is ACT:ACT - it is artemisinin combination therapy. It includes Artesunate 50/100mg + SP (sulfadoxine500 mg +Pyrimathamine 25 mg).Treatment of P. falciparum malaria: Artesunate(50 mg or 100 mg ) and SP( sulfadoxine500 mg +Pyrimathamine 25 mg) the recommended drugs for effective malaria treatment in Afghanistan
Dosage ChartFirst Day Second day Third day Remarks
Age SP Artesunate Artesunate Artesunate5-11 months Half tablet Half tablet
Of 50 mgHalf tablet Half tablet
Childblister
1-6 years One tablet One tablet Of 50 mg
One tablet One tablet
7-13 years Two tablets Two tablets Of 50 mg
Two tablets Two tablets
Above 13 years Three tablets Two tablets Of 100 mg
Two tablets Two tablets Adult blister
Important; Day1 dose should be administrated as a Direct Observation therapy(DOT) Remind the patient to complete the treatment. Advice the patient to sleep under a long lasting insecticidal net to prevent Malaria attack
NoteThe dose chart is only applicable for:Blister 1: adult blisterArtesunate 100 and sulfadoxin +Pyrimthamine 500mg+25mg TABLETBlister 2 Children BlisterArtesunate 50 mg and Sulfadoxin + Pyrimethamine 500 mg + 25 mg TABLET
Treatment of P. vivax malaria:Chloroquine (150mg base tablet)
Age (years)
Weight (kg)
DAY 1(no. of tablets)
DAY 2(no. of tablets)
DAY 3(no. of tablets)
<1 <10 ½ ½ ½1-<3 10-<14 1 1 ½3 –< 5 14-19 1 ½ 1 ½ ½5-11 20-35 2 ½ 2 ½ 111-12 36-50 3 3 214+ 50+ 4 4 2
(Source: Revised National Treatment Guideline, April, 2010)
Treatment of mix infection: Treat as Pf malaria.
51
Picture of RDTs with result mentioned above

Malaria Flow Chart At Health Post Level
52
Registration of the patient Use RDT
RDT positive (Pf/PAN)
RDT negative
Patient Stable.Treat the patient
Patient with danger signRefer to health facility
Children less than 5 month.Refer to health facility
Pregnant women (1st trimester)Refer to health facility
If Pf positive treat with ACT
If both Pf & PAN positive treat with ACT
If only PAN positive treat with Chloroquin-e
Pregnant women (2nd & 3rd trimester) If only PAN positive treat with Chloroquine
Pregnant women (2nd & 3rd trimester) If only Pf or both Pf & PAN positive treat with ACT
Patient comes back with symptoms after treatment
Refer the patient to the nearest health facility
Treat the patient as usual according to CHWs guideline

Chapter five:
Session 1: WELCOME and INTRODUCTION During this session, the participants will:
Register Introduce each other Share their expectations of the training Introduce with the rules & norms of the training Undertake a pre-test Introduce about goal & objectives of the training Know about the general information of malaria
Objective:At the end of the session the participants will be able to
Define malaria Describe signs & symptoms of malaria Identify the causative agent of malaria Name the vector of malaria Describe the mode of transmission of malaria List the main malaria prevention methods.
Method: Question and answer Pictorial presentation Lecture with discussion
Topics:General Information about malaria
What is malaria Signs & Symptoms of malaria Causative agent of malaria Vector of malaria Mode of transmission of malaria Prevention of malaria
Materials:
Note books Pen, Pencil Posters/ Pictures Flip Chart
Session 2: Introduction of Rapid Diagnostic TestObjective: At the end of the session the participants will able to
Know what is RDT Describe advantages & disadvantages of RDT Use RDT to diagnose malaria Store RDT at health post level
Methods: Demonstration of RDT Question and answer
Topics:
Materials: RDT Kits Pictorial instruction about RDT use
53
What is RDT Advantage and disadvantage of RDT Procedure of RDT use Storage of RDT

Safety box Register form
Session3: Practical use of RDT
Objective : At the end of the session the participants will able to
• Collect patient’s blood for RDT• Use RDT for diagnosis of malaria• Interpret the result of RDT
Method: Practical group work Practical use of RDT
Topic: Technique of blood collection from patient’s finger Use of RDT for malaria diagnosis Interpretation of the result of RDT
Material: RDT Lancet Alcohol swab Buffer Dropper Pictorial instruction about RDT use Timer/ Watch
Session 4: Management of malaria
Objective:At the end of the session the participants will able to
Define ACT Treat the falciparum malaria cases by using ACT
Methods: Lecture with discussion Demonstration of ACT Role play
Topics: Introduction of ACT Treatment of malaria by using ACT
Materials: ACT (Dosage forms) Pictorial demonstration of ACT, Dosage & treatment
Session 5: Reporting on RDT, ACT & malaria cases
Objective:At the end of the session the participants will able to
Report on used RDT, positive & negative RDT Report on ACT use Report on malaria cases
Methods: Demonstration of reporting formats Small group discussion
Topics: Reporting system about RDT
54

Reporting system about ACT use Reporting system about malaria cases
Materials:
Different kinds of reporting formats
Session 6: Reporting on RDT, ACT & malaria cases
Methods: Question and answer Discussion
Topics: Review of the previous lessons Post test End evaluation of course
Materials: Post test sheet Course evaluation sheet
55