development of evidence based “best standard treatments” in pediatric rheumatology carol a....
TRANSCRIPT

Development of Evidence Based
“Best Standard Treatments” in Pediatric Rheumatology
Carol A. Wallace MDProfessor of Pediatrics
University of Washington School of MedicineSeattle Children’s Hospital and Research Institute
Immediate Past Chair of CARRA

Why do we want “Best Standard Treatments”?
• Standardized care results in decreased variation in patient care, which has been shown to result in improved quality and outcomes
• Enable comparative effectiveness research to identify the safest, most effective and most cost effective treatments
• Prevent complications by use of safest possible treatments
• Disseminated widely to improve overall standards of patient care nationwide

1950 1960 1970 1980 1990
2
4
6
8
( )
Annual USA Cancer Mortality Rate Children <15 Years
CCG
NWTSG
IRSG
CALGB Pediatric Division
SWOG Pediatric DivisionPOG
The National Childhood Cancer Mortality Rate and the Pediatric Cooperative Groups
2000
Mortality per
100,000, Age-
Adjusted
2005
COG

How do we develop evidence based
Best Standard Treatments?• Analyze data from clinical trials• Analyze data from large prospective
cohorts followed from initial presentation with detailed information on treatment and outcomes
We have neither available data sources…
In the absence of data, one approach is to start with development of
“Consensus Treatment Plans”
• Consensus formed; with broad input• Reasonable, common and practical• Once developed, these can facilitate
the development of evidence based Best Standard Care by:– Decreasing treatment variation– Enabling analysis of prospectively collected data
of presenting features, treatments and outcomes

Comparative Effectiveness Research in Pediatric Rheumatic Diseases: Leveraging
CARRA for Improved Child Health
In response to NIAMS RFA 05-AR-102
CARRA-“ ”

Childhood
Arthritis and Rheumatology
Research Alliance

CARRA is:
A research net work of North American Pediatric Rheumatologists and Health Care Professionals dedicated to improving the treatment and health related outcomes of children with rheumatic diseases through clinical research.

CARRA Site Map
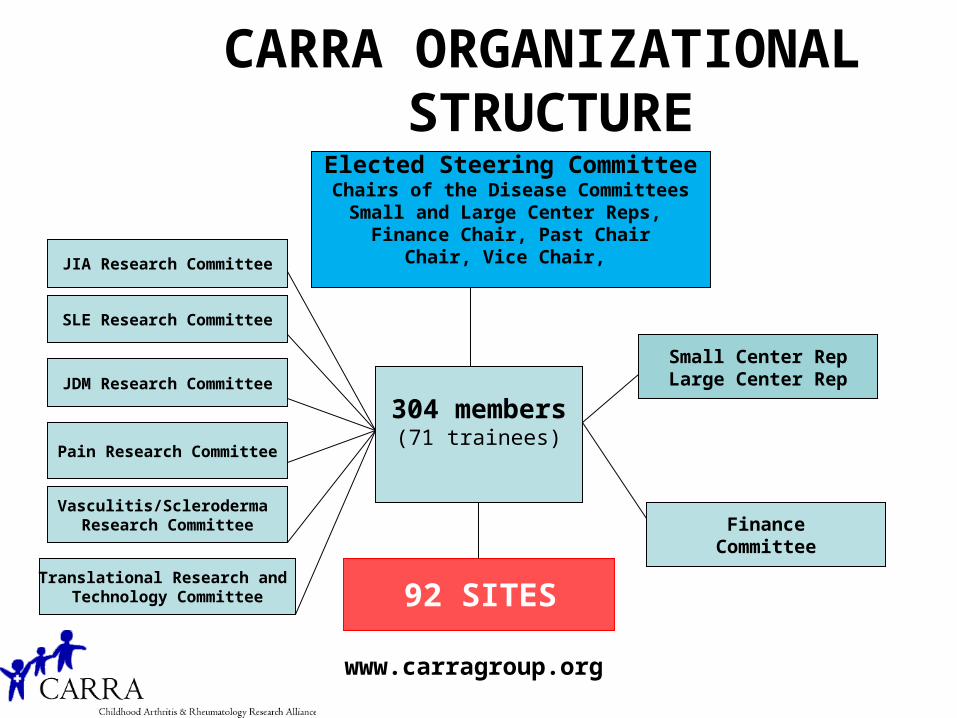
CARRA ORGANIZATIONAL STRUCTURE
Elected Steering CommitteeChairs of the Disease Committees
Small and Large Center Reps, Finance Chair, Past Chair
Chair, Vice Chair, JIA Research Committee
SLE Research Committee
JDM Research Committee
Pain Research Committee
Vasculitis/Scleroderma Research Committee
Translational Research and Technology Committee
FinanceCommittee
304 members(71 trainees)
www.carragroup.org
92 SITES
Small Center RepLarge Center Rep

What makes CARRA a Network?
Member Participation
Disease Specific Committee work
Conduct of Research
Education, training and mentoring
Annual Meeting
Collaborations with other organizations

A Research Network Can…
Improve the standard of care through clinical studies
Promote a “culture” of research at Pediatric Rheumatology sites
Develop Best Standard Treatments for better patient outcomes

Specific Aims CARRA-• To develop multiple standardized treatment
plans for use in new onset patients with: JIA, SLE, JDM and localized scleroderma– Use of consensus methodology– Specify of outcome measures, data collection
details and time points• Develop mechanisms to enable rapid
dissemination and use of the consensus developed treatment plans
• Develop analysis plans for the data collected to determine the clinical efficacy and safety of patients treated with these plans

Overall Concept of CARRA-• When a new patient presents, a physician
would choose to use one of the standardized treatment plans that most fits what they would normally do.
• Data would be collected on the patients treated with these standardized treatments
• Data would be analyzed to determine the most efficacious treatment with the least side effects
• Thru this process, we would create evidence based “Best Standard Treatment”

Carol Wallace (contact PI) Norm Ilowite (PI)
JDM Module Ann Reed - Leader
JIA Module Yuki Kimura- Leader
Linear Scl Module Rob Fuhlbrigge-Leader
SLE ModuleEmily Von Scheven Leader
Adam HuberCo-leader
Esi Morgan DeWittCo-leader
Hermine BrunnerCo-leader
Suzanne LiCo-Leader
CARRA-

Carol Wallace (contact PI) Norm Ilowite (PI)
Dan Solomon
Overall Grant Consultant
JDM Module Ann Reed -Leader
JIA Module Yuki Kimura-Leader
Linear Scl Module Rob Fuhlbrigge-Leader
SLE ModuleEmily Von Scheven Leader
Adam HuberCo-leader
Esi Morgan DeWittCo-leader
Hermine BrunnerCo-leader
Suzanne LiCo-Leader
Advisory BoardChair- Edward GianniniDan Solomon, Brian Feldman, Pamela Weiss, Peter Boehm, Vincent Del Gaizo
CARRA-

Carol Wallace (contact PI) Norm Ilowite (PI)
Dan Solomon
Overall Grant Consultant
JDM ModuleAnn Reed - Leader
JIA Module Yuki Kimura-Leader
Linear Scl Module Rob Fuhlbrigge -Leader
SLE Module Emily Von SchevenLeader Lay MembersLay Members
Lay Members Lay Members
Adam HuberCo-leader
Esi Morgan DeWittCo-leader
Hermine BrunnerCo-leader
Suzanne LiCo-Leader
Advisory BoardChair- Edward GianniniDan Solomon, Brian Feldman, Pamela Weiss, Peter Boehm, Vincent Del Gaizo
CARRA-

Consensus Methodology Choices
• Convene a panel of experts• NIH model:
– Public discussion of questions and evidence before an expert panel, followed by private unstructured deliberations of the panel
• Delphi Questionnaire Technique• Nominal Group Technique• Combination of the Delphi
Questionnaires and Nominal Group Technique

Development process for Consensus Treatment Plans
***** Workgroup*****

Development process for Consensus Treatment Plans
***** Workgroup*****
Initial CARRA wide surveys
JIA: new onset systemic JIASLE: new onset nephritisJDM: new onset moderate to severe diseaseLocalized scleroderma: new onset
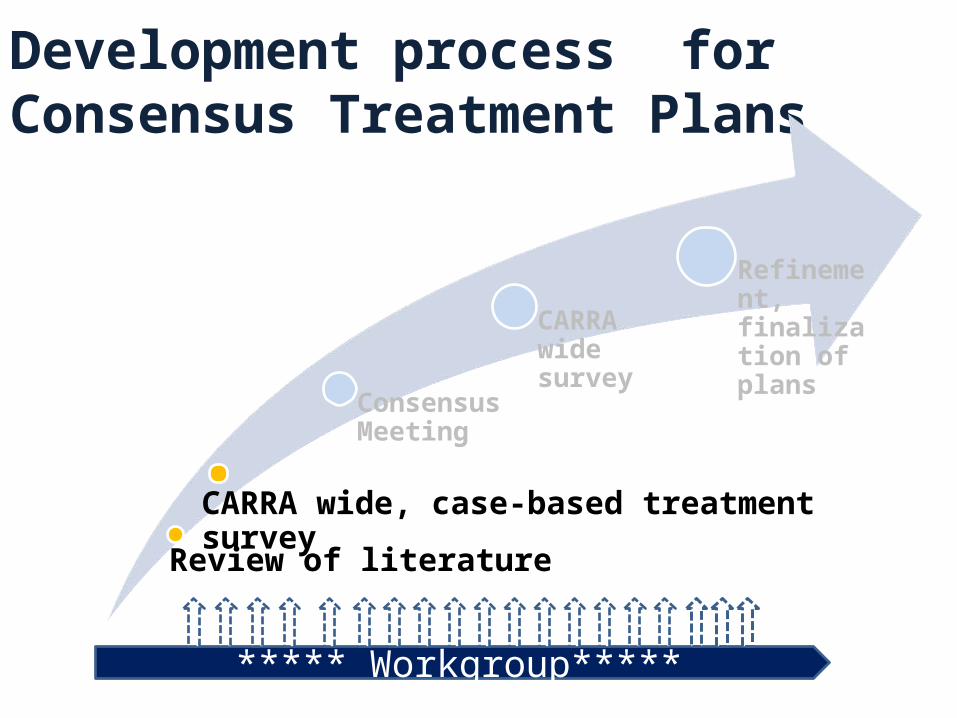
Development process for Consensus Treatment Plans
CARRA wide, case-based treatment survey
Consensus Meeting
CARRA wide survey
Refinement, finalization of plans
***** Workgroup*****
Review of literature
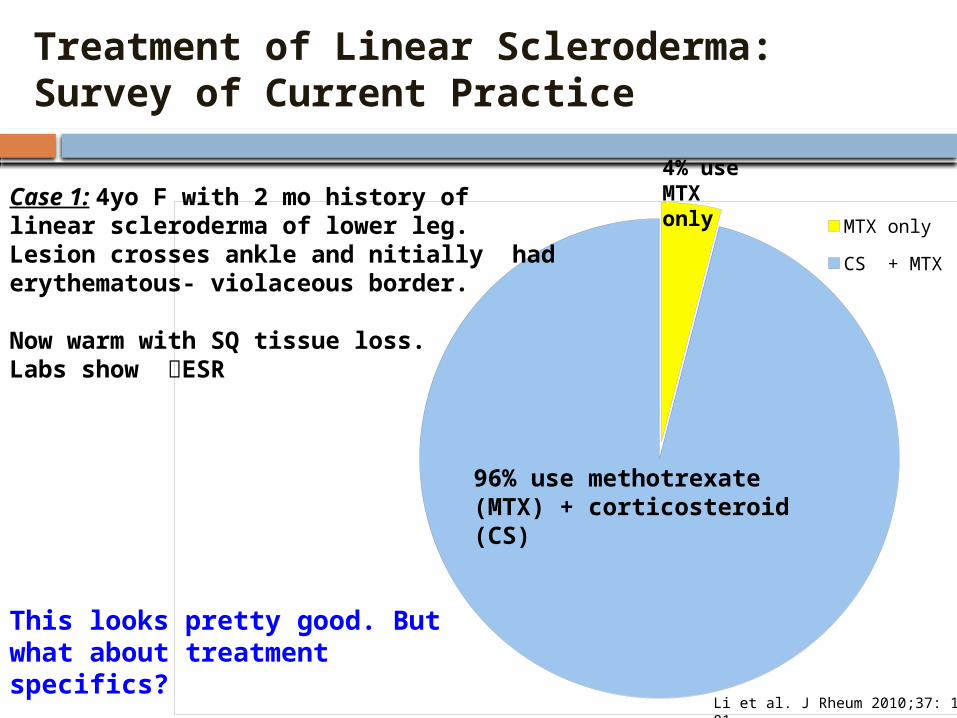
Treatment of Linear Scleroderma: Survey of Current Practice
Case 1: 4yo F with 2 mo history of linear scleroderma of lower leg. Lesion crosses ankle and initially had erythematous- violaceous border.
Now warm with SQ tissue loss. Labs show ESR
Treatment of Linear Scleroderma: Survey of Current Practice
MTX only
CS + MTX
Case 1: 4yo F with 2 mo history of linear scleroderma of lower leg. Lesion crosses ankle and nitially had erythematous- violaceous border.
Now warm with SQ tissue loss. Labs show ESR
96% use methotrexate (MTX) + corticosteroid (CS)
4% use MTX only
This looks pretty good. But what about treatment specifics?
Li et al. J Rheum 2010;37: 175-81

What type of CS were chosen?
no CS
Oral CS only
IV CS only
IV + Oral CS
30% use oral CS
39% use IV CS
27% use IV + Oral CS
Case 1: 4 yo F with linear scleroderma of leg4% do not use CS
How about specific CS doses and dosing regimens?

CS use in LS: Dosing regimens and duration
Pred 0.75x6 Pred 0.5 x1
Pred 0.5 x2 Pred 0.5 x6
Pred 0.5 xNS Pred 1 x1
Pred 1 x2 Pred 1 x 2.5
Pred 1 x3 Pred 1 x6
Pred 2 x0.5 Pred 2 x1
Pred 2 x2 Pred 2 x3
Pred 2 x6 Pred 2 xNS
IV 1/wk x1 IV 1/wk x2
IV 1/wk xNS IV 1/mo x1
IV 1/mo x6 IV 1/mo x7
IV 1/mo x18 IV 3/mo x1
IV 3/mo x3 IV 3/mo x24
IV 3/mo+add IVMP IV 3/mo xNS
IV 3/wk x0.25 IV 3/wk x0.5 +add IVMP
IV 3/wk x3 IV 3/wk x NS
IV 1/mx6 + pred2/kg x 12 IV 1/m x1 + pred1/kg x1
IV 1/wk x1 +pred 0.5 x1 IV 1/wk x3 +pred0.5x3
IV 1/wkx1 +pred 1/kgx1 IV 1/wk xNS +pred 1/kg x3
IV 1/wkx1 +pred 2/kg x1 IV 1/wkx1 +pred 0.5x1
IV 1/wkx2 +Pred 2/kgQOD x1 IV 1/wk x2 +pred 2/kg x1
IV 3/mo x1 then pred IV 3/mox1 +pred2/kg QOD x1
IV 3/mox3 then pred IV 3/mox1+pred 1/kgx1
IV 3/mo x3 +pred 1/kgx1 IV 3/mox6 +pred 1/kgx1
IV 3/wkX0.25 then pred IV 3/wkX0.25 +pred0.5/kg x2
IV 3/wk x0.25 +pred 0.5x1 IV 3/wk X0.25 +pred2/kg x2
IV 3/wk X0.25 +pred 1/kg x3 IV 3/wk xNS =Pred 1/kg x1
IV 3/wk x0.5 +pred 1/kg x3 IV 3/wk x0.25 +pred 2/kg x1
IV 3/wk x0.5 +pred 2/kg x1 IV 3/wk x0.5 +pred 2/kg x3
IV 3/wk x1 +pred 2/kg x1 IV 3/wk x0.25 +pred 1/kgx 1
IV 3d/mo x 3 mo: 27 PR
Pred 1mg/kg/d x 1 mo: 9 PR
3 main oral CS regimens:-1 mg/kg/d (28)-2 mg/kg/d (18)-0.5 mg/kg/d (11)
4 IV CS regimens:-3d/mo (33)-1/wk (19)-3d/wk (19)-1/mo (5)

MTX Treatment Regimens in LS0.3 pox15 0.3 po x240.3, 0.6 sq/po x 25 0.5 sq x60.5 sq x7 0.5 sq x 90.5 sq x12 0.5, 1 po x 130.5 sq x 13 0.5, 0.75 sq x 130.5,1 sq x14 0.5 sq x180.5, 0.3 sq x21 0.5 po x240.5 sq x24 0.5, 1 sq x260.5 sq/po x36 0.5 sq x12+0.5 NS xNS 0.6 po x120.6sq x15 0.6 sq xNS0.6 sq/po, po x NS 0.75 po x120.75, 1 sq, 0.5po x 24 0.75 po x240.75 sq x 24 0.75 sq x300.75 po x NS 0.8 sq x NS0.875 sq/po, 0.75 sq, 1 po x 14 0.875 sq/po x 241 sq x 3 1 sq x121 sq, 20 sq x13 1 sq/po, 1 sq x151 sq x 15 1 sq, 0.5 sq x 181 sq/po, 15 sq/10po x 18 1 sq x 181 po x 24 1 sq x 241 sq, 0.3po x 24 1 po x 271 sq x 27 1 sq, 0.75sq x301 sq/po x 30 1 sq x301 sq x 36 1 sq x 421 sq x 48 1 sq/po x 481 po, 1 taper x 18 1 sq/10 sq x24+1 sq/po, taper x>12 1 sq, taper x>101 sq x>12 1 sq, 0.5 sq x 12+1 sq x 36+ 1 sq x NS1 sq, 15 po x 24_ 10 sq x1310 po x 15 10 sq/po, 15 po x 2610 sq/po, 15 sq/po x30 10 po x NS12 sq/po x 24 12 po x NS12.5 sq/po,1sq,, 10 po x12 15 po x 1215 sq x12 15 sq/po x 1215 sq x15 15 po x 2415 sq x 24 15 po, 10 po x 2615 sq/po x30 15 sq x 3615 sq/po x 42 15 sq x 48
13 different initial doses27 different initial doses and routes
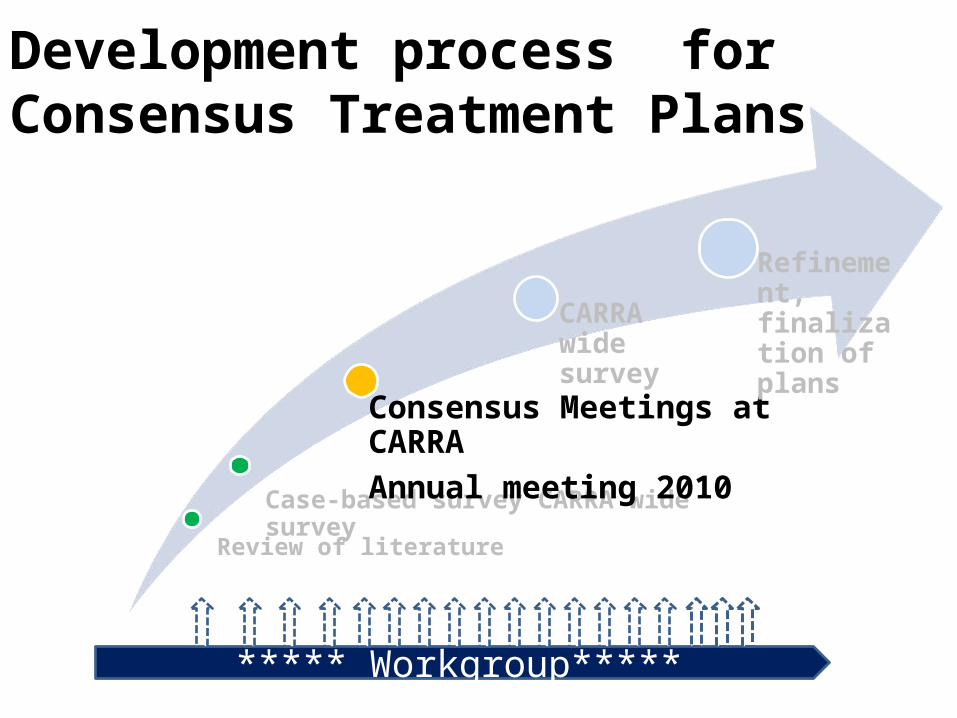
Development process for Consensus Treatment Plans
Case-based survey CARRA wide survey
Consensus Meetings at CARRA
Annual meeting 2010
CARRA wide survey
Refinement, finalization of plans
***** Workgroup*****
Review of literature

Consensus methodologies facilitated and promoted the highest quality team work
However, this is REALLY hard and time consuming!
CARRA-
CARRA- Guiding Principles
• Evidence-based when possible– Considered the best available literature
• Compatible with the current practice– Assessed by the surveys
• Consensus agreement– Delphi Questionnaires– Nominal group technique

Development of ConsensusStandardized Treatments
• Distill what we do- using collective judgment and consensus processes
• Forced us to:– Think critically about what we do– Use facts when present, not beliefs
or “this is how I always do this”– Emphasis on decreased variation
Development of Consensus Standardized Treatments
• Not rigorous protocols- but rather menus of standardized treatments
• Not perfect or exactly what each physician might do, but what he/she can live with
• The goal is to reduce variation so we can treat in a standardized fashion, collect data and compare patient outcomes
Common Module Work • Define the patient characteristics
and exclusions for use of the treatment plans
• What to do if better, worse or adverse event
• Essential data to be collected• Essential labs to be collected• Key data collection time points
Challenges• Steroids
– How to standardize dosages and routes– Standardization of steroid taper rate
• JIA:– Patient characteristics: how early to allow treatment -
may need to treat before fulfilling ILAR criteria for JIA– Include a new medication not yet approved?
• SLE: Induction and maintenance, or just induction?
• Linear scleroderma:– Lack of outcome measures – Lack of definitions for improvement, worsening

SLE Breakout sessions
Topic Group CoordinationM= moderatorN= note taker
1 Outcome measures/response variables
M: Hermine BrunnerN: Joyce Hsu
2 Cyclophosphamide plan M: Emily von SchevenN: Eyal Muscal
3 Mycophenolate plan M: Anne EberhardN: Marisa Klein-Gitelman
4 Steroid regimens – doses and tapering
M: Lynn PunaroN: Linda Wagner-Weiner
5 QOL/patient perspectives/ AEs
M: Stacey ArdoinN: Nandini Moorthy, Jenny Palter

Regimen AMTX alone
BMTX + Intravenous steroid
CMTX + Oral prednisone
MTX weekly dose
1mg/kg SQ (max 25 mg)
1mg/kg SQ (max 25 mg) 1mg/kg SQ (max 25 mg)
Steroiddose, Duration
None 30 mg/kg/dose (max 1gm)EITHER: 3 consecutive daily doses/mo, OR: 1 dose/weekDuration: 3 months
2 mg/kg/d (max 60 mg) divided bidDuration: at least 2 weeks
Steroid taper targets
None None Dose reduced to:1 mg/kg/d (max 30 mg) by end of wk 80.5 mg/kg/d (max 15 mg) by end of wk 160.25 mg/kg/d (max 7.5 mg) by end of wk 24Off CS by end of week 48
Localized Scleroderma Consensus Treatment Plans

JIA Module• Developed 4 treatment plans:
– Steroid only– Methotrexate– Anakinra– Tocilizumab
• Possible steroid plans :– IV 30/kg/day X 3 days– Oral
• 1 mg/kg/day – taper over 1, 3 or 6 months• 2 mg/kg/day – taper over 1, 3 or 6 months

ASSESS AT 3 MONTHS If Improved
*If on PO PDN, taper PDN Continue same dose MTX, reassess monthly
If Unchanged , Worse, or on >50% steroid doseContinue same dose PDN and MTX , Plus
Add additional therapy, choose and follow either: anakinra plan or tocilizumab plan
ASSESS AT 1 MONTH
If ImprovedContinue same dose MTXStart/Continue PDN taper,
reassess monthly
If UnchangedIncrease MTX to 1mg/kg (30mg
max) SQ weekly ; Continue same dose PDN , reassess monthly
If WorseIncrease MTX to 1mg/kg SQ
weekly; Increase (or continue) PDN to 2mg/kg (max 100mg);
repeat IV MP, reassess monthlyASSESS AT 1-2 WEEKS
ImprovedTaper PDN (if on)
(choose rapid, fast, slow)
UnchangedContinue same dose PDN
Optional: Add or repeat IV MP (can be weekly)
WorsenedIf not on oral PDN, add at 1mg/kg;
If on PDN, increase to 2mg/kg; Add/Repeat IV MP (can be weekly)
Plan B: MethotrexateMethotrexate (MTX) 0.5mg/kg PO or SQ weekly
Optional corticosteroids : PDN 1mg/kg (60mg max); IV MP pulse 30mg/kg X 3 d

Systemic JIA data collectionCategory Items
History demographics, date symptom onset, comorbidities, medications, recent rash or serositis, suspected MAS
Patient and Physician assessments
painHRQOL physical functionparent/patient global assessmentprovider global assessment
Physical Exam Ht, Wt, BMI, active joint count, hepatomegaly, lymphadenopathy, rash, serositis, splenomegaly
Labs CBC c-reactive protein, ESR, ferritinalbumin, LDH
Treatment-related factors
MedicationsSAE or IME if discontinuation then provide reason

Development process for Consensus Treatment Plans
Case-based CARRA wide survey
Consensus Meeting
CARRA wide survey
Refinement, finalization of plans; CARRA 2011 meeting
***** Workgroup*****
Review of literature

Consensus Treatment Plans developed for new onset:
• Systemic JIA– Steroids– MTX +/- steroids– Anakinra +/steroids– Tocilizumab +/steroids
• Juvenile Dermatomyositis– Pred + MTX – Pred + MTX + IV methylpred– Pred + MTX + IV methylpred
+ IVIG
• Renal disease in SLE– Cell cept induction– IV cytoxan induction
• Linear Scleroderma– MTX– MTX +Oral steroid– MTX + IV methyl pred
•All Modules have submitted the Treatment Plans and their
development for publication

Next Steps• Parallel to this effort has been the development of
a large foundational pediatric rheumatology registry: CARRAnet – 60 participating pediatric rheumatology sites– 6,000 patients enrolled
• Plan is that new onset patients treated with one of the Consensus Treatment Plans will have specific data collected using the CARRAnet platform

Consensus Treatment Plans
CARRA website
Publication progress: JDM – AC&R SLE – AC&R Systemic JIA – revision AC&R Localized scleroderma – revision AC&R

Implementation of Consensus Treatment Plans
Protocol for the CARRA Registry and Consent form allows for data collection that will cover the basic registry and additional sub-studies.
Actual additional data collection will occur at sites participating in the pilot studies.
All CARRA members are encouraged to use the CTP on new patients, regardless of participation in the pilot studies
Consensus Treatment Plans: Pilot Studies
JDM: Friends of CARRA and CUREJM 10 sites/ 40 patients
Systemic JIA: Arthritis Foundation 15 sites/ 30 patients
SLE: Lupus Foundation of America 15 sites/ 40 patients
Localized Scleroderma: Arthritis Foundation 11 sites/ 50 patients

Future Steps• Analysis of the data collected through the
CARRAnet platform will allow for comparisons between treatments for determination of effectiveness, outcomes and side effects
• Evidence based Best Standard Treatments can then be identified and widely disseminated
• Over time these can be improved upon in an iterative fashion to improve the outcomes of children with rheumatic diseases
• Development of standardized treatment plans for additional phases/categories of disease are underway


ASSESS AT 3 MONTHS Patient on <50% starting steroid dose
Continue to taper PDN, reassess monthlyIf improved, continue PDN taper
If unchanged or worsened, add additional therapy (plan B, C, D)
Patient on >50% starting steroid doseContinue same dose PDN , Plus
Add additional therapy, choose and follow either : methotrexate, anakinra, tocilizumab plan
ASSESS AT 1 MONTH
If ImprovedContinue (or initiate) PDN taper
If Unchanged or WorseIncrease (or continue) PDN to 2mg/kg (max 100mg);
repeat IV MP (can be weekly), reassess monthlyASSESS AT 1-2 WEEKS
ImprovedTaper PDN
(choose rapid, fast, slow)
UnchangedContinue same dose PDN
Add or repeat IV MP
WorsenedIncrease PDN to 2mg/kg (max
100mg); Repeat IV MP
Plan A: SteroidPrednisone (PDN) 1mg/kg (max 60mg) daily
Optional IV MP pulse 30mg/kg (max 1g) daily for 3 days
ASSESS AT 3 MONTHS If Improved
*If on PO PDN, taper PDN Continue same dose ANK
reassess monthly
If Unchanged , Worse, or on >50% steroid dose Continue same dose PDN
Plus eitheradd MTX, or switch to tocilizumab plan
ASSESS AT 1 MONTH
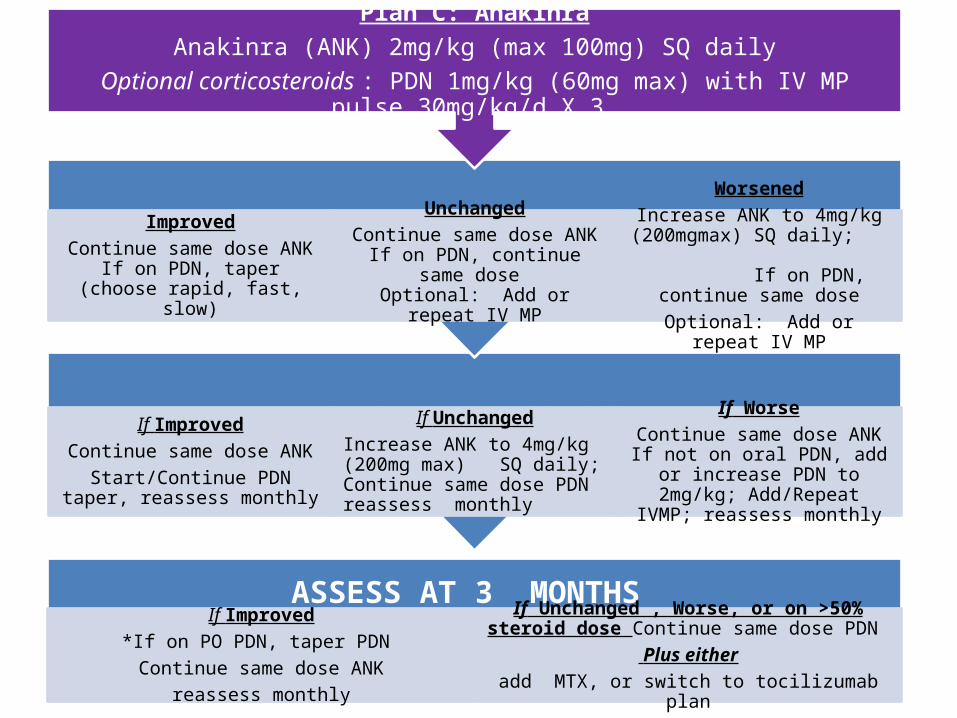
If ImprovedContinue same dose ANKStart/Continue PDN taper,
reassess monthly
If UnchangedIncrease ANK to 4mg/kg (200mg max) SQ daily; Continue same dose PDN reassess monthly
If WorseContinue same dose ANK
If not on oral PDN, add or increase PDN to 2mg/kg; Add/Repeat
IVMP; reassess monthlyASSESS AT 1 -2 WEEKS
ImprovedContinue same dose ANK
If on PDN, taper (choose rapid, fast, slow)
UnchangedContinue same dose ANK
If on PDN, continue same dose Optional: Add or repeat IV MP
WorsenedIncrease ANK to 4mg/kg
(200mgmax) SQ daily; If on PDN, continue same
doseOptional: Add or repeat IV MP
Plan C: AnakinraAnakinra (ANK) 2mg/kg (max 100mg) SQ daily
Optional corticosteroids : PDN 1mg/kg (60mg max) with IV MP pulse 30mg/kg/d X 3
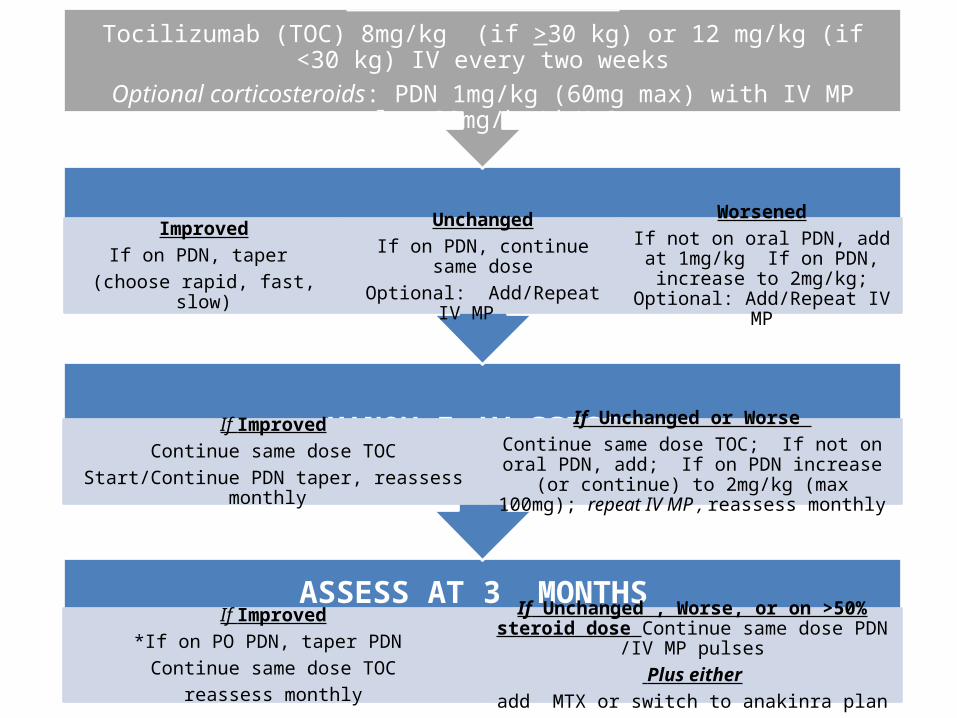
ASSESS AT 3 MONTHS If Improved
*If on PO PDN, taper PDN Continue same dose TOC
reassess monthly
If Unchanged , Worse, or on >50% steroid dose Continue same dose PDN /IV MP pulses
Plus eitheradd MTX or switch to anakinra plan
ASSESS AT 1 MONTH
If ImprovedContinue same dose TOC
Start/Continue PDN taper, reassess monthly
If Unchanged or Worse Continue same dose TOC; If not on oral PDN, add; If
on PDN increase (or continue) to 2mg/kg (max 100mg); repeat IV MP , reassess monthly
ASSESS AT 2 WEEKS
ImprovedIf on PDN, taper
(choose rapid, fast, slow)
UnchangedIf on PDN, continue same doseOptional: Add/Repeat IV MP
WorsenedIf not on oral PDN, add at 1mg/kg
If on PDN, increase to 2mg/kg; Optional: Add/Repeat IV MP
Plan D: TocilizumabTocilizumab (TOC) 8mg/kg (if >30 kg) or 12 mg/kg (if <30 kg) IV every two weeks
Optional corticosteroids: PDN 1mg/kg (60mg max) with IV MP pulse 30mg/kg/d X 3