development and validation of a risk-stratification score for surgical site occurrence and surgical...
TRANSCRIPT
Development and Validation of a Risk-StratificationScore for Surgical Site Occurrence and Surgical SiteInfection after Open Ventral Hernia Repair
Rachel L Berger, BA, Linda T Li, MD, Stephanie C Hicks, PhD, MS, Jessica A Davila, PhD,Lillian S Kao, MD, MS, FACS, Mike K Liang, MD
BACKGROUND: Current risk-assessment tools for surgical site occurrence (SSO) and surgical site infection(SSI) are based on expert opinion or are not specific to open ventral hernia repairs. We aimedto develop a risk-assessment tool for SSO and SSI and compare its performance againstexisting risk-assessment tools in patients with open ventral hernia repair.
STUDY DESIGN: A retrospective study of patients undergoing open ventral hernia repair (n ¼ 888) was con-ducted at a single institution from 2000 through 2010. Rates of SSO and SSI were deter-mined by chart review. Stepwise regression models were built to identify predictors ofSSO and SSI and internally validated using bootstrapping. Odds ratios were converted toa point system and summed to create the Ventral Hernia Risk Score (VHRS) for SSO andSSI, respectively. Area under the receiver operating characteristic curve was used to comparethe accuracy of the VHRS models against the National Nosocomial Infection SurveillanceRisk Index, Ventral Hernia Working Group (VHWG) grade, and VHWG score.
RESULTS: The rates of SSO and SSI were 33% and 22%, respectively. Factors associated with SSOincluded mesh implant, concomitant hernia repair, dissection of skin flaps, and wound class4. Predictors of SSI included concomitant repair, dissection of skin flaps, American Society ofAnesthesiologists class �3, wound class 4, and body mass index �40. The accuracy of theVHRS in predicting SSO and SSI exceeded National Nosocomial Infection Surveillanceand VHWG grade, but was not better than VHWG score.
CONCLUSIONS: The VHRS identified patients at increased risk for SSO/SSI more accurately than theNational Nosocomial Infection Surveillance scores and VHWG grade, and can be used toguide clinical decisions and patient counseling. (J Am Coll Surg 2013;217:974e982.� 2013 by the American College of Surgeons)
Ventral hernia repairs are among themost common generalsurgery procedures, with more than 350,000 performedin the United States each year.1 A myriad of wound
Disclosure Information: Dr Liang is currently an investigator and receivesgrants from Lifecell and Acell. All other authors have nothing to disclose.
Dr Kao is a mentor for a resident grant from the American Society of Colonand Rectal Surgeons and does not receive any salary support from this grant.
Ms Berger and Dr Li contributed equally to this work.
Abstract presented at the Academic Surgical Congress and the AnnualMeeting of the Surgical Infection Society, New Orleans, LA, February 2013.
Received May 24, 2013; Revised July 13, 2013; Accepted August 5, 2013.From the Michael E DeBakey Veterans Affairs Medical Center (Berger,Liang), Michael E DeBakey Department of Surgery, Baylor College ofMedicine (Li, Liang), Department of Statistics, Rice University (Hicks),Houston VA HSR&D Center of Excellence (Davila), and Departmentof Surgery, The University of Texas Medical School at Houston (Kao),Houston, TX.Correspondence address: Mike K Liang, MD, Michael E DeBakey VeteransAffairs Medical Center, 2002 Holcombe Blvd, OCL (112), Houston,TX 77030. email: [email protected]
974ª 2013 by the American College of Surgeons
Published by Elsevier Inc.
complications can occur after open ventral hernia repair(OVHR). These events are cumulatively called surgicalsite occurrences (SSO) and are thought to be related topatient and surgical factors. Specifically, SSO includessurgical site infection (SSI), seroma and hematoma forma-tion, wound dehiscence, and fistula formation.2 Surgicalsite occurrence afterOVHRcan lead to chronicmesh infec-tion and hernia recurrence, both of which can lead to reop-eration and increased risk of subsequent complications.Recognizing the grave consequences of SSO, earlier
efforts have been made to identify risk factors for SSO toguide patient counseling of postoperative risks and to facil-itate outcomes reporting for OVHR; yet there are severallimitations to each of the existing risk-assessment tools.For example, the Ventral Hernia Working Group(VHWG) categorizes patients into 4 grades that predictthe risk of SSO. Patients classified as grade 1 have a “lowrisk” of complications and includes patients with no
ISSN 1072-7515/13/$36.00
http://dx.doi.org/10.1016/j.jamcollsurg.2013.08.003

Abbreviations and Acronyms
ASA ¼ American Society of AnesthesiologistsAUC ¼ area under the receiver operating characteristic
curveBMI ¼ body mass indexNNIS ¼ National Nosocomial Infection SurveillanceOR ¼ odds ratioOVHR ¼ open ventral hernia repairSSI ¼ surgical site infectionSSO ¼ surgical site occurrenceVHRS ¼ Ventral Hernia Risk ScoreVHWG ¼ Ventral Hernia Working Group
Vol. 217, No. 6, December 2013 Berger et al Ventral Hernia Risk Score 975
history of wound infection. Grade 2 describes “comorbid”patients who are smokers, diabetic, obese, immunosup-pressed, or have COPD. Patients who have “potentiallycontaminated” hernias are considered grade 3, and thesepatients have earlier wound infections, stomas, or had“violation of the gastrointestinal tract.” Grade 4 patientswith infected mesh or septic dehiscence are considered“infected.” Based on the hernia grade, the authors proposea plan for the appropriate use of synthetic vs biologic mesh.However, the VHWG grading system was based on expertopinion after literature review rather than on direct patientdata.2
The VHWG model was later modified into a 3-tiersystem by Kanters and colleagues.3 Although this studywas performed on patient data, the authors adapted theoriginal VHWG and omitted certain hernia characteris-tics and variations in operative technique that mightinfluence the rate of postoperative complications. Impor-tant hernia-related factors, such as presence of an incar-cerated hernia, concomitant surgery, acute presentation,and surgery-related factors, such as operative time, useof drains, and extent of tissue dissection, can also affectSSO and SSI rates. Finally, the National NosocomialInfection Surveillance (NNIS) Risk Index is a well-accepted risk-assessment tool, but was created to predictthe risk of SSI after surgical procedures in general andhas not been validated for ventral hernia repairs or SSOspecifically.4 To our knowledge, there is currently no vali-dated risk-assessment tool based on direct patient data toevaluate the risk of SSO or SSI after OVHR.Therefore, the goals of the current study were to iden-
tify factors associated with SSO and SSI for patientsundergoing OVHR, develop prognostic risk-assessmentscores for SSO and SSI, and compare their performanceagainst existing risk-assessment tools. We hypothesizethat risk-assessment scores derived from direct patientdata and specific to open ventral hernias will outperformexisting paradigms.
METHODSWe conducted a retrospective cohort study on all consec-utive patients undergoing OVHR by the general surgeryservice at the Michael E DeBakey Veterans AffairsMedical Center from 2000 through 2010. InstitutionalReview Board approval was obtained. Patients weredivided into 2 groups based on presence of SSO. Weadopt a previously established definition to identifySSO: SSI at 30 days, seroma, hematoma, wound dehis-cence, or formation of a fistula, as determined fromreview of the electronic medical records by trained chartabstractors or clinicians.2,3 All abstractors were trainedon a data dictionary before chart review, and a qualitycheck was performed that entailed a random selectionof 10% of all cases that were then reviewed in total bythe senior author. To determine the presence of SSI, weused the guidelines described by the Center for DiseaseControl and Prevention.5 Seromas were recorded if thepatient had radiographic evidence of fluid collection orclinical evidence of a seroma.Patient demographic, clinical, and intraoperative data
were also abstracted from the medical records. Demo-graphic data included age, race, and sex. Clinical factorsincluded body mass index (BMI), history of diabetes mel-litus, insulin use, benign prostatic hypertrophy, steroiduse, history of cancer, current smoker, alcohol usedisorder, and American Society of Anesthesiologists(ASA) score. Surgical factors included earlier SSI, earlierventral hernia repair, earlier abdominal surgery, earliermesh implant, and NNIS score. Hernia characteristicsincluded whether the hernia was primary or incisional;whether the procedure was elective or acute; whether thehernia repair was concomitant, incarcerated, and/or recur-rent; and hernia defect area. Incisional hernias weredefined as hernias that formed in the location of a previousincision.6 Concomitant hernia repairs were defined asthose repaired during a procedure for another surgicalindication. Hernia defect area was approximated usingthe formula for an ellipse. Intraoperative factors collectedincluded wound class, duration of operation, use of preop-erative antibiotics, mesh implantation, type of mesh,dissection techniques, and use of drains. Fascial flapswere defined as an incision made on the fascia to facilitatemedial advancement, such as “relaxing fascial incision,component separation, Chevrel technique,” noted in theoperative dictation. The creation of skin flaps was definedas a maneuver that dissected the skin and subcutaneoustissue off of the anterior abdominal wall fascia.Secondary outcomes included length of stay, admission
to the ICU, urinary tract infection, pulmonary infection,ileus, 30-day readmission, reoperation, hernia recurrence,

976 Berger et al Ventral Hernia Risk Score J Am Coll Surg
bowel obstruction, fistula formation, and mortality at anytime after the surgery. Ileus was defined as no return ofbowel function within 3 days after surgery or recoveryand subsequent loss of bowel function without evidenceof bowel obstruction. Recurrence was determined byradiographic data, clinical examination at follow-up visit,or reoperation reports. Follow-up was defined as day ofsurgery until death or last clinical examination.
Statistical analysis
Differences between the 2 groups were compared usingPearson chi-square or Fisher’s exact test. Continuousdata were analyzed using 2-tailed t-test or Mann-Whitney U test for parametric and nonparametric data,respectively. Missing data were estimated by imputation.Excluding other risk-assessment tools (ie, VHWG Grade,NNIS), all variables with a p < 0.2 on univariate analysisand those considered clinically relevant were included inthe multivariate analysis to identify predictors of SSOand SSI. Model selection was performed using a resam-pling technique (bootstrapping). Diagnostics of themodel were assessed using 10-fold cross validation.
Risk score development and validation
The odds ratios from each of the multivariate modelswere converted to a point system by rounding to the near-est whole integer, and summed to create a risk score foreach patient, which is referred to as the Ventral HerniaRisk Score (VHRS) for SSO and SSI. We comparedthe accuracy of the VHRS against the NNIS Risk Index,the VHWG grade, and VHWG score, a point-basedversion of the VHWG criteria (which we derived by con-verting the odds ratios of the risk factors cited by theVHWG into points) using the area under the receiveroperating characteristic curve (AUC), and tested usingDeLong’s test for 2 receiver operating characteristiccurves. All statistics were performed using IBM SPSSsoftware (version 19) and R software (version 2.15.0).
RESULTS
Study characteristics
A total of 888 patients were identified. Overall, 295 (33%)patients had an SSO after OVHR. Of those, 233 had anSSI, the majority of which were superficial SSIs (n ¼166). Patients that had an SSO develop had higher BMI,were more likely to have diabetes, require insulin, havea history of cancer, have alcohol use disorder, and havehigher ASA score (Table 1). Patients with earlier abdom-inal operations, earlier SSI, earlier ventral hernia repairs,and earlier mesh use were also more likely to have anSSO. Additionally, acute hernia repairs, incisional hernia
repairs, concomitant hernia repairs, and repairs involvingincarcerated hernia contents were more likely to result inSSO. Concomitant hernia repairs were most commonlyidentified after laparoscopic cholecystectomies (20%),ostomy reversals (12%), and exploratory laparotomies(12%). The rate of SSO was highest after ostomy reversal(86%).Table 2 describes the differences in intraoperative char-
acteristics based on presence of SSO. Median operativetime was longer for patients in whom an SSO had devel-oped (123 minutes vs 90 minutes; p < 0.01). Patientswho had an SSO were also more likely to have prostheticmesh implanted and skin flaps created.Hernia recurrence was more common among patients
who had an SSO (28% vs 13%; p < 0.01). Patients inwhom an SSO developed also had worse secondaryoutcomes; specifically, longer median length of stay (7days vs 3 days; p < 0.01), more ICU admissions (28.5%vs 8.3%; p< 0.01), and higher rates of urinary tract infec-tion (6.4% vs 1.3%; p < 0.01), pulmonary infection(6.1% vs 1.7%; p < 0.01), central-line infection (2.4%vs 0.3%; p ¼ 0.01), and postoperative ileus (10.8% vs4.0%; p < 0.01) (Table 3). Although there was no differ-ence in mortality, patients in whom an SSO developed hadhigher rates of readmission (38% vs 21%; p < 0.01) andreoperation (31% vs 10%; p < 0.01). Postoperativeimaging was available for 277 (31%) patients. Medianfollow-up was 68.5 months (interquartile range 63.9months) for patients without SSO and 57.3 months(54.5 months) for patients with SSO.
Model development and validation for surgical siteoccurrence
The following independent factors were associated withSSO: mesh implantation (odds ratio [OR] ¼ 1.9; 95%CI, 1.4e2.7), concomitant hernia repair (OR ¼ 2.2;95% CI, 1.5e3.4), creation of skin flaps (OR ¼ 2.2;95% CI, 1.6e3.1), and hernia repair of an infectedwound (OR ¼ 8.7; 95% CI, 3.7e24.1) (K-fold cross-validation error ¼ 0.15) (Table 4). The ORs were con-verted to a point system and summed to acquire theVHRS, which ranged from 0 to 15 points. The accuracyof the VHRS for SSO was better than NNIS (AUC ¼0.68 vs 0.62; p ¼ 0.02) and VHWG grade (0.68 vs0.61; p < 0.01), but not significantly better thanVHWG score in predicting SSO events (p ¼ 0.11)(Fig. 1).Using the VHRS for SSO, we stratified patients into 3
groups from lowest to highest risk: groups I (0 points), II(2 to 4 points), and III (>4 points). The SSO rates forgroups I, II, and III were 17.8%, 49.6%, and 79.6%,respectively (Fig. 2).
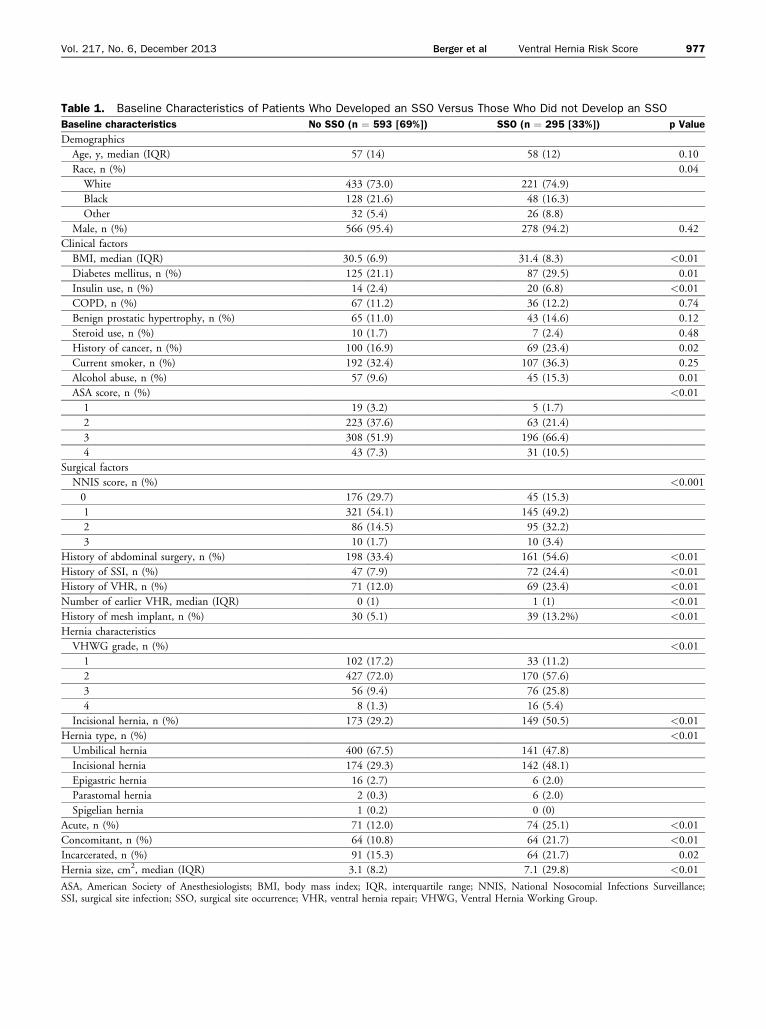
Table 1. Baseline Characteristics of Patients Who Developed an SSO Versus Those Who Did not Develop an SSO
Baseline characteristics No SSO (n ¼ 593 [69%]) SSO (n ¼ 295 [33%]) p Value
Demographics
Age, y, median (IQR) 57 (14) 58 (12) 0.10
Race, n (%) 0.04
White 433 (73.0) 221 (74.9)
Black 128 (21.6) 48 (16.3)
Other 32 (5.4) 26 (8.8)
Male, n (%) 566 (95.4) 278 (94.2) 0.42
Clinical factors
BMI, median (IQR) 30.5 (6.9) 31.4 (8.3) <0.01
Diabetes mellitus, n (%) 125 (21.1) 87 (29.5) 0.01
Insulin use, n (%) 14 (2.4) 20 (6.8) <0.01
COPD, n (%) 67 (11.2) 36 (12.2) 0.74
Benign prostatic hypertrophy, n (%) 65 (11.0) 43 (14.6) 0.12
Steroid use, n (%) 10 (1.7) 7 (2.4) 0.48
History of cancer, n (%) 100 (16.9) 69 (23.4) 0.02
Current smoker, n (%) 192 (32.4) 107 (36.3) 0.25
Alcohol abuse, n (%) 57 (9.6) 45 (15.3) 0.01
ASA score, n (%) <0.01
1 19 (3.2) 5 (1.7)
2 223 (37.6) 63 (21.4)
3 308 (51.9) 196 (66.4)
4 43 (7.3) 31 (10.5)
Surgical factors
NNIS score, n (%) <0.001
0 176 (29.7) 45 (15.3)
1 321 (54.1) 145 (49.2)
2 86 (14.5) 95 (32.2)
3 10 (1.7) 10 (3.4)
History of abdominal surgery, n (%) 198 (33.4) 161 (54.6) <0.01
History of SSI, n (%) 47 (7.9) 72 (24.4) <0.01
History of VHR, n (%) 71 (12.0) 69 (23.4) <0.01
Number of earlier VHR, median (IQR) 0 (1) 1 (1) <0.01
History of mesh implant, n (%) 30 (5.1) 39 (13.2%) <0.01
Hernia characteristics
VHWG grade, n (%) <0.01
1 102 (17.2) 33 (11.2)
2 427 (72.0) 170 (57.6)
3 56 (9.4) 76 (25.8)
4 8 (1.3) 16 (5.4)
Incisional hernia, n (%) 173 (29.2) 149 (50.5) <0.01
Hernia type, n (%) <0.01
Umbilical hernia 400 (67.5) 141 (47.8)
Incisional hernia 174 (29.3) 142 (48.1)
Epigastric hernia 16 (2.7) 6 (2.0)
Parastomal hernia 2 (0.3) 6 (2.0)
Spigelian hernia 1 (0.2) 0 (0)
Acute, n (%) 71 (12.0) 74 (25.1) <0.01
Concomitant, n (%) 64 (10.8) 64 (21.7) <0.01
Incarcerated, n (%) 91 (15.3) 64 (21.7) 0.02
Hernia size, cm2, median (IQR) 3.1 (8.2) 7.1 (29.8) <0.01
ASA, American Society of Anesthesiologists; BMI, body mass index; IQR, interquartile range; NNIS, National Nosocomial Infections Surveillance;SSI, surgical site infection; SSO, surgical site occurrence; VHR, ventral hernia repair; VHWG, Ventral Hernia Working Group.
Vol. 217, No. 6, December 2013 Berger et al Ventral Hernia Risk Score 977

Table 2. Operative Data of Patients Who Developed an SSO Versus Those Who Did not Develop an SSO
Operative data
No SSO SSO
p Valuen % n %
Wound class <0.01
1 502 84.7 198 67.1
2 60 10.1 44 14.9
3 25 4.2 25 8.5
4 6 1.0 28 9.5
Operative time, min, median (IQR) 90.0 71.3 123.5 107.25 <0.01
Received preoperative antibiotics 332 56.0 197 66.8 <0.01
Mesh use <0.01
Synthetic mesh 199 33.6 117 39.7
Biologic mesh 39 6.6 52 17.6
No mesh 355 59.9 126 42.7
Fascial flaps created 43 7.3 36 12.2 0.02
Component separation performed 6 1.0 15 5.1 <0.01
Skin flaps created 102 17.2 111 37.6 <0.01
Fascia closed 476 80.5 213 72.2 0.01
Drains used 102 17.2 101 34.2 <0.01
IQR, interquartile range; SSO, surgical site occurrence.
978 Berger et al Ventral Hernia Risk Score J Am Coll Surg
Model development and validation for surgical siteinfection
The following factors were found to be associated withincreased odds of SSI: concomitant hernia repairs(OR ¼ 2.1; 95% CI, 1.4e3.3), creation of skin flaps(OR ¼ 2.3; 95% CI, 1.6e3.4), ASA class �3 (OR ¼2.1; 95% CI, 1.4e3.2), BMI �40 (OR ¼ 3.2; 95% CI,1.7e5.9), and wound class 4 (OR ¼ 6.8; 95% CI,3.2e15.4) (K-fold cross-validation error 0.20) (Table 4).The VHRS for SSI ranged from 0 to 16 points. Thediscriminative power of the VHRS for SSI was more accu-rate than NNIS (AUC ¼ 0.71 vs 0.65; p ¼ 0.03) andVHWG grade (0.71 vs 0.64; p < 0.01), but not signifi-cantly better than VHWG score (p¼ 0.16) (Fig. 3). Usingthe VHRS for SSI, we stratified patients into 5 groupsfrom lowest to highest risk: groups I (0 points), II (2 to3 points), III (4 points), IV (5 to 10 points), and V (11to 16 points). Group I had 7.8% SSI and Group V had83.3% SSI (Fig. 4).
DISCUSSIONWe present a new prognostic risk-assessment tool forpredicting an SSO in patients undergoing OVHR. TheVHRS for SSO includes the following factors: meshimplant, concomitant hernia repair, dissection of skinflaps, and wound class 4. We also identify characteristicsthat are associated with SSI, which include the following5 factors: concomitant hernia repair, dissection of skinflaps, ASA score �3, BMI �40, and wound class 4.
Our overall incidence rates of SSO and SSI were 33%and 22%, respectively, similar to that reported by otherstudies.3,7,8
Although the predictive performance of the VHRS forSSO exceeded both NNIS and VHWG tools, we notethat the accuracy is modest at best (AUC ¼ 0.68). Apossible explanation might be that SSO is a conglomera-tion of several complications, all of which might havedifferent underlying pathophysiology. Therefore, thepredictive power of a model might be limited. Surgicalsite occurrence remains a novel result, and its use inoutcomes research has not yet been firmly established.Surgical site infection might be a preferable result, asthe pathophysiology of SSI is more homogenous. Yetsome experts argued that organ-space SSI is a differentdisease process compared with deep or superficial SSI,9
and restricting the outcomes to deep and superficialSSIs might yield an even better model.Unlike contemporary risk-assessment tools that are
based on expert opinion or are not specific to patientsundergoing OVHR, the VHRS is derived from directpatient data. Additionally, the VHRS, with 4 factors asso-ciated with SSO and 5 factors for SSI, is easier for clini-cians to use compared with the 12 factors required toassess a patient under the VHWG grade model.Three factors were common between the VHRS for
SSO and SSI. In accordance with the surgical literature,we found that wound class was an important independentpredictor of SSO and SSI. A patient with a wound class 4was automatically placed in the highest-risk group for

Table 3. Comparing Outcomes Based on Presence of Surgical Site Occurrence
Outcomes No SSO (n ¼ 593 [67%]) SSO (n ¼ 295 [33%]) p Value
SSI, n (%)
Superficial d 166 (56.3) d
Deep d 38 (12.9) d
Organ-space d 29 (9.8) d
Skin dehiscence/opened, n (%) d 63 (21.4) d
Fascial dehiscence, n (%) d 15 (5.1) d
Seroma, n (%) d 108 (30.2) d
Seroma drained, n (%) d 41 (13.9) d
Hematoma, n (%) d 27 (9.2) d
Hematoma drained, n (%) d 15 (5.1) d
Fistula formation, n (%) d 12 (4.1) d
Length of stay, d, median (IQR) 1 (2) 3 (7) <0.01
Admitted to ICU, n (%) 49 (8.3) 84 (28.5) <0.01
Urinary tract infection, n (%) 8 (1.3) 19 (6.4) <0.01
Pulmonary infection, n (%) 10 (1.7) 18 (6.1) <0.01
Central venous access infection, n (%) 2 (0.3) 7 (2.4) 0.01
Ileus, n (%) 24 (4.0) 32 (10.8) <0.01
30-d readmission, n (%) 123 (20.7) 113 (38.3) <0.01
Reoperation, n (%) 58 (9.8) 91 (30.8) <0.01
Bowel obstruction, n (%) 14 (2.4) 19 (6.4) <0.01
Hernia recurrence, n (%) 79 (13.3) 83 (28.1) <0.01
Mortality, n (%) 66 (11.1) 42 (14.2) 0.18
Follow-up, mo, median (IQR) 68.5 (63.9) 57.3 (54.5) 0.01
IQR, interquartile range; SSI, surgical site infection; SSO, surgical site occurrence.
Vol. 217, No. 6, December 2013 Berger et al Ventral Hernia Risk Score 979
SSO, where 80% of patients had an SSO; likewise, havinga wound class 4 procedure placed the patient in risk group4 for SSI, where>50% of patients had an SSI. Among ourcohort of patients undergoing OVHR, there was a robustdistribution of wound classifications. Concomitant herniarepair was also found to be a predictor for both SSO andSSI. Although earlier studies suggest favorable outcomesof concomitant umbilical hernia repair after laparoscopiccholecystectomy,10 more recent studies found that herniarepair with mesh implantation is associated with higherrates of complication in clean-contaminated cases.11-13
Similarly, concomitant hernia repairs often follow
Table 4. Ventral Hernia Risk Score for Surgical Site Occurrenc
Variable
VHRS for SSO
OR 95% CI
Mesh implant 1.9 1.4e2.7
Concomitant hernia repair 2.2 1.5e3.4
Skin flaps created 2.2 1.6e3.1
ASA score �3 d d
BMI �40 d d
Wound class 4 8.7 3.7e24.1
ASA, American Society of Anesthesiologists; BMI, body mass index; OR, odds raHernia Risk Score.
procedures involving bowel resection, suggesting that theremight be a role for interval hernia repair for selectedpatients. In our study, most concomitant hernia repairswere associated with laparoscopic cholecystectomies,ostomy reversals, and exploratory laparotomies, and therate of SSO was highest after ostomy reversal.We also identified the creation of skin flaps as a predictor
for SSO and SSI. A potential explanation might be that theincreased dissection required to lift skin flaps can lead totissue devascularization and greater dead space, both ofwhich could facilitate bacterial growth.14,15 In our univar-iate analysis, we found that wider skin flaps had
e and Surgical Site Infection
VHRS for SSI
Points OR 95% CI Points
2 d d d
2 2.1 1.4e3.3 2
2 2.3 1.6e3.4 2
d 2.1 1.4e3.2 2
d 3.2 1.7e5.9 3
9 6.8 3.2e15.4 7
tio; SSO, surgical site occurrence; SSI, surgical site infection; VHRS, Ventral
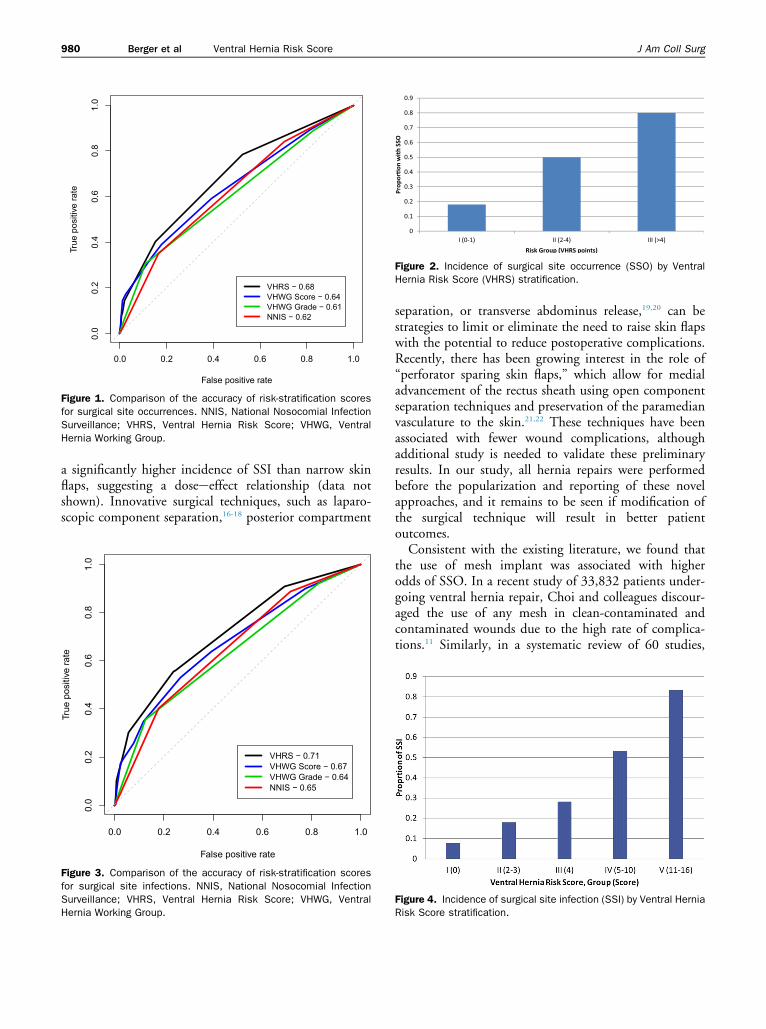
Figure 2. Incidence of surgical site occurrence (SSO) by VentralHernia Risk Score (VHRS) stratification.
False positive rate
True
pos
itive
rate
0.0 0.2 0.4 0.6 0.8 1.0
0.0
0.2
0.4
0.6
0.8
1.0
VHRS − 0.68VHWG Score − 0.64VHWG Grade − 0.61NNIS − 0.62
Figure 1. Comparison of the accuracy of risk-stratification scoresfor surgical site occurrences. NNIS, National Nosocomial InfectionSurveillance; VHRS, Ventral Hernia Risk Score; VHWG, VentralHernia Working Group.
980 Berger et al Ventral Hernia Risk Score J Am Coll Surg
a significantly higher incidence of SSI than narrow skinflaps, suggesting a doseeeffect relationship (data notshown). Innovative surgical techniques, such as laparo-scopic component separation,16-18 posterior compartment
False positive rate
True
pos
itive
rate
0.0 0.2 0.4 0.6 0.8 1.0
0.0
0.2
0.4
0.6
0.8
1.0
VHRS − 0.71VHWG Score − 0.67VHWG Grade − 0.64NNIS − 0.65
Figure 3. Comparison of the accuracy of risk-stratification scoresfor surgical site infections. NNIS, National Nosocomial InfectionSurveillance; VHRS, Ventral Hernia Risk Score; VHWG, VentralHernia Working Group.
separation, or transverse abdominus release,19,20 can bestrategies to limit or eliminate the need to raise skin flapswith the potential to reduce postoperative complications.Recently, there has been growing interest in the role of“perforator sparing skin flaps,” which allow for medialadvancement of the rectus sheath using open componentseparation techniques and preservation of the paramedianvasculature to the skin.21,22 These techniques have beenassociated with fewer wound complications, althoughadditional study is needed to validate these preliminaryresults. In our study, all hernia repairs were performedbefore the popularization and reporting of these novelapproaches, and it remains to be seen if modification ofthe surgical technique will result in better patientoutcomes.Consistent with the existing literature, we found that
the use of mesh implant was associated with higherodds of SSO. In a recent study of 33,832 patients under-going ventral hernia repair, Choi and colleagues discour-aged the use of any mesh in clean-contaminated andcontaminated wounds due to the high rate of complica-tions.11 Similarly, in a systematic review of 60 studies,
Figure 4. Incidence of surgical site infection (SSI) by Ventral HerniaRisk Score stratification.

Vol. 217, No. 6, December 2013 Berger et al Ventral Hernia Risk Score 981
Bellows and colleagues found that 87% of incisionalhernia repairs using biologic mesh had a complication,such as SSI, seroma, or hematoma, but because of inade-quacies in the literature, the authors were unable to eval-uate the incidence of SSO as defined by the VHWG.12
Two patient factors were predictors for SSI only. Theassociation between obesity and postoperative infectionis well established in the surgical literature.23-26 For easeof clinical application, we presented our analysis usingdiscrete values for BMI. BMI was also a significantpredictor for SSO when analyzed as a continuous variable(OR ¼ 1.07; 95% CI, 1.04e1.10), suggesting thata patient’s risk for SSO rises with increasing BMI. Itremains to be seen how very low BMI might influenceSSO rates. In our study population, the lowest BMIwas 16.1, and only 4 patients had BMI <17. HigherASA classification (3 or 4) was also a predictor for SSI,which is consistent with previous studies and other risk-stratification scales, including NNIS and VHWG.2,4,7,27
As a global assessment of patient comorbidity, the ASAclassification not only considers factors that are used todetermine VHWG grade, such as presence of chronicobstructive pulmonary disease and diabetes, but also eval-uates the severity of these disease processes, and might bea better measure of patient comorbidity burden.In our study, patients with an SSO had worse
outcomes, such as higher rates of readmission, reopera-tion, and recurrence. Because SSO events are thoughtto be related to patient factors, there might be an oppor-tunity to improve outcomes by addressing specific riskfactors. Patients who meet the VHRS criteria for high-risk groups might benefit from patient optimization strat-egies (ie, weight-loss programs, smoking cessation, andexercise programs) or modified surgical techniques (ie,interval hernia repair, limiting or avoiding skin flaps,and limiting tissue dissection).
Limitations
There are several limitations in our study. First, the retro-spective nature of the study might introduce bias in theidentification of SSO and SSI events. Fewer than 10 casesreported in the current study were included in an earlierrandomized controlled trial at our institutiondtheresearch notes from those cases were not used in the dataabstraction. We strove to minimize variability by main-taining strict definitions of SSO and SSI, and we notethat our rates are within the range of reported rates.Although we internally validated the VHRS with thereceiver operating characteristic curve and used internalresampling (bootstrapping), which minimizes overfittingand improves the likelihood of strong external validity,our study lacks external validation. To adjust for
confounding factors, we believed that it was necessary toinclude perioperative variables, which can limit the preop-erative use of the VHRS, although we believe that manyperioperative factors are potentially predictable. Forexample, patients with wound class IV hernias are typicallyknown before surgery, and surgeons might anticipate theneed to create skin flaps. Finally, we conducted this studyamong the Veteran population, which is predominatelymale and has higher comorbidities compared with thegeneral population. Therefore, extrapolation of the studyfindings must be approached with caution.
CONCLUSIONSWe present a validated, risk-assessment tool for patientsundergoing OVHR for SSO and SSI that is derivedfrom direct patient data. The accuracy of the VHRS forSSO and SSI exceeds that of existing risk-assessment toolsfor both outcomes, but remains modest. The VHRS forSSO and SSI can stratify patients into 3-risk and 5-riskgroups, respectively, and can be used to guide preoperativepatient counseling and to identify patient at higher risk forSSO or SSI who might benefit from interval ventral herniarepair, optimization of comorbidities, and modification ofsurgical techniques. Additional studies are planned to eval-uate the external validity of the VHRS for SSO and SSI ina separate cohort and to evaluate the effectiveness of risk-reduction strategies based on this score.
Author Contributions
Study conception and design: Berger, Li, Davila, Kao,Liang
Acquisition of data: Berger, Li, LiangAnalysis and interpretation of data: Berger, Li, Hicks,Kao, Liang
Drafting of manuscript: Berger, Li, Hicks,Critical revision: Berger, Li, Hicks, Davila, Kao, Liang
REFERENCES
1. Poulose BK, Shelton J, Phillips S, et al. Epidemiology and costof ventral hernia repair: making the case for hernia research.Hernia 2012;16:179e183.
2. BreuingK, Butler CE, Ferzoco S, et al. Incisional ventral hernias:review of the literature and recommendations regarding thegrading and technique of repair. Surgery 2010;148:544e558.
3. Kanters AE, Krpata DM, Blatnik JA, et al. Modified herniagrading scale to stratify surgical site occurrence after openventral hernia repairs. J Am Coll Surg 2012;215:787e793.
4. Gaynes RP, Culver DH, Horan TC, et al. Surgical site infec-tion (SSI) rates in the United States, 1992-1998: the NationalNosocomial Infections Surveillance System basic SSI riskindex. Clin Infect Dis 2001;33[Suppl 2]:S69eS77.
5. Alexander JW, Solomkin JS, Edwards MJ. Updated recom-mendations for control of surgical site infections. Ann Surg2011;253:1082e1093.

982 Berger et al Ventral Hernia Risk Score J Am Coll Surg
6. Muysoms FE, Miserez M, Berrevoet F, et al. Classification ofprimary and incisional abdominal wall hernias. Hernia 2009;13:407e414.
7. Farrow B, Awad S, Berger DH, et al. More than 150 consecutiveopen umbilical hernia repairs in a major Veterans Administra-tion Medical Center. Am J Surg 2008;196:647e651.
8. Davies SW, Turza KC, Sawyer RG, et al. A comparative anal-ysis between laparoscopic and open ventral hernia repair ata tertiary care center. Am Surg 2012;78:888e892.
9. Anderson DJ. Surgical site infections. Infect Dis Clin NorthAm 2011;25:135e153.
10. Karner E, Unalp HR, Derici H, et al. Laparoscopic cholecys-tectomy accompanied by simultaneous umbilical hernia repair:a retrospective study. J Postgrad Med 2007;53:176e180.
11. Choi JJ, Palaniappa NC, Dallas KB, et al. Use of mesh duringventral hernia repair in clean-contaminated and contaminatedcases: outcomes of 33,832 cases. Ann Surg 2012;255:176e180.
12. Bellows CF, Smith A, Malsbury J, et al. Repair of incisionalhernias with biological prosthesis: a systematic review ofcurrent evidence. Am J Surg 2013;205:85e101.
13. Cavallaro A, Lo ME, Di VM, et al. Use of biological meshesfor abdominal wall reconstruction in highly contaminatedfields. World J Gastroenterol 2010;16:1928e1933.
14. Chang N, Mathes SJ. Comparison of the effect of bacterialinoculation on musculocutaneous and random pattern flaps.Plast Reconstr Surg 1982;70:1e10.
15. Feng LF, Price D, Hohn D, Mathes SJ. Blood flow changesand leukocyte mobilization in infection: a comparison betweenischemic and well-perfused skin. Surg Forum 1983;34:603.
16. Rosen MJ, Jin J, McGee MF, et al. Laparoscopic componentseparation in the single-stage treatment of infected abdominalwall prosthetic removal. Hernia 2007;11:435e440.
17. Giurgius M, Bendure L, Davenport DL, et al. The endoscopiccomponent separation technique for hernia repair results inreduced morbidity compared to the open component separa-tion technique. Hernia 2012;16:47e51.
18. Rosen MJ, Williams C, Jin J, et al. Laparoscopic versus open-component separation: a comparative analysis in a porcinemodel. Am J Surg 2007;194:385e389.
19. Novitsky YW, Elliott HL, Orenstein SB, et al. Transversusabdominis muscle release: a novel approach to posteriorcomponent separation during complex abdominal wall recon-struction. Am J Surg 2012;204:709e716.
20. Krpata DM, Blatnik JA, Novitsky YW, et al. Posterior andopen anterior components separations: a comparative analysis.Am J Surg 2012;203:318e322.
21. Ghali S, Turza KC, Baumann DP, et al. Minimally inva-sive component separation results in fewer wound-healingcomplications than open component separation for largeventral hernia repairs. J Am Coll Surg 2012;214:981e989.
22. Saulis AS, Dumanian GA. Periumbilical rectus abdominisperforator preservation significantly reduces superficial woundcomplications in “separation of parts” hernia repairs. PlastReconstr Surg 2002;109:2275e2280.
23. Olsen MA, Higham-Kessler J, Yokoe DS, et al. Developinga risk stratification model for surgical site infection afterabdominal hysterectomy. Infect Control Hosp Epidemiol2009;30:1077e1083.
24. Manilich E, Vogel JD, Kiran RP, et al. Key factors associatedwith postoperative complications in patients undergoing colo-rectal surgery. Dis Colon Rectum 2013;56:64e71.
25. Wick EC, Hirose K, Shore AD, et al. Surgical site infectionsand cost in obese patients undergoing colorectal surgery.Arch Surg 2011;146:1068e1072.
26. Smith RL, Bohl JK, McElearney ST, et al. Wound infectionafter elective colorectal resection. Ann Surg 2004;239:599e605.
27. Tang R, Chen HH, Wang YL, et al. Risk factors for surgicalsite infection after elective resection of the colon and rectum:a single-center prospective study of 2,809 consecutive patients.Ann Surg 2001;234:181e189.