developing the reflective practitioner: supervision in harm reduction programs a training for...
TRANSCRIPT

Developing the Reflective Practitioner:
Supervision in Harm Reduction Programs
A Training for Housing Works 10.29.0757 Willoughby Street, Brooklyn
Prepared and Delivered by Richard Elovich, MPH www.richardelovich.com
Training Contents:
• Introduction (slides 2-5)• The team and group dynamics (slide 6-29)• Supervision, program philosophy, review of harm reduction,
concepts and skills, trainings into practice (30-71)• A supervisory framework for staff-client interactions (72-81)• Supervision as developing reflective practice (82-90)• Monitoring and evaluation (91-104)• Cites and resource material for this training (105-6)
www.richardelovich.com 2

Ground Rules
• Elicit the reasons for having ground rules from participants.– Why might it be important for us to have ground
rules?• Elicit from group members their ideas about
ground rules– Let’s try to make a list of “ground rules” for the
group that will help each of you individually to get the most out of our time together.

www.richardelovich.com 4
Training Contract• Stay focused today. Be on task.• Listening is a key to this training. Reflective
listening. Listening to directions so they don’t have to be repeated and so you get the task or exercise right.
• Listen to new ideas. Listen to what’s coming up inside you in relation to what’s being presented. Try to put your thoughts and feelings into words instead of “shutting down.”
• Acknowledge and respect differences. You can “agree to disagree” on a contentious point and move on.
• Participate in role plays. Go (forward) and grow.
• Everyone has permission to pass. Offer feedback constructively not personally. Try to receive feedback as a gift.
• Learning environment. Try to be okay with taking some learning risks. Stretch past your edge of what you know and what you are comfortable with.
• Confidentiality. Hold the container. Don’t be leaky.
• Turn off phones and beepers.• No cross talk. Allow one person to speak at a
time. Equal time over time. • Start and end on time, including breaks. Be
alert to tendency to fudge this.• Use “I” statements.• Can everybody agree? Is there anything you
absolutely cannot live with?• Now we are off.

LEARNING PROCESS: KNOWLEDGE
• Acquisition of content • Retention (store in memory)• Application (retrieve and use)• Proficiency (integrate and synthesize)
6
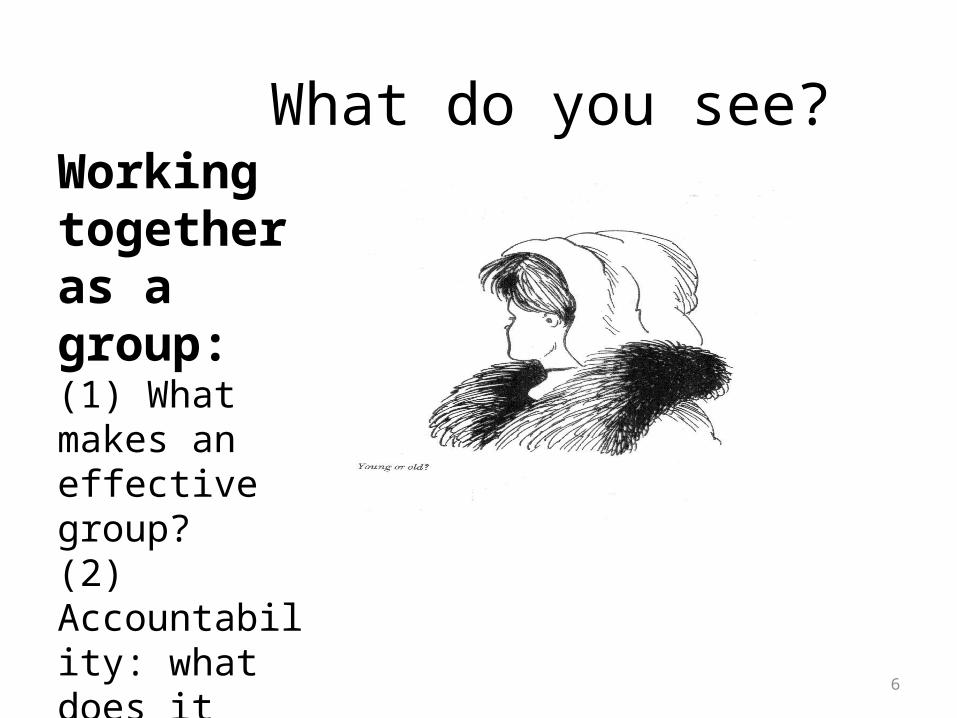
What do you see?Working together as a group: (1) What makes an effective group?(2) Accountability: what does it mean?

GROUPS
• Before we pursue groups as tool. We need to think about what they are.
• We are social animals. We live and die in groups. We get our sense of ourselves socially. Most of what we do is social.

WHAT IS A GROUP?
1. List everything you do in a typical day from the moment you wake up in the morning up to the moment you fall asleep.
2. Delete from your list all the activities you perform with groups of people and see what is left.
3. Let’s discuss.

WHAT IS A GROUP?
• Commuters (regular hour)?• Motorists (regular hour)?• Pedestrians on the street (regular hour)?• Employees in a department of a hospital or
social service setting?• Sidewalk book venders and place holders?• Neighbors during blizzard?

WHERE DID YOU FIND GROUPS?
• Work environment• Family and kinship• Civic associations (church, PTA, Senegalese
Association)• Informal friendship clusters• Street demonstration• Student organizing

WHAT GROUPS MEAN TO PARTICIPANTS
• Someone learns he does not have a disease and this means he loses group affiliation
• Doctor on television show ER cannot perform surgery any longer and loses his “master” identity.
• Someone attempting to stop drinking as to confront consequences of separating from peer group
QUESTIONS YOU RAISED
• How do people use groups? • What happens to a group when someone is
absent? How does group experience absence of one, two, three members?

What Makes a Group Effective?
• Goals
• Interdependence
• Interpersonal interaction
• Structured Relationships
• Mutual Influence
• Motivation

Goals
• Groups exist for a reason. People join groups in order to achieve goals they are unable to achieve by themselves. A group may be defined as a number of individuals who join together to achieve a goal. It is questionable whether a group could exist unless there was a mutual goal that its members were trying to achieve.

Interdependence.
• A group may be defined as a collection of individuals who are interdependent in some way. According to this definition, the individuals are not a group unless an event that affects one of them affects them all. Conceiving of a group as a dynamic whole in the sense that an event or action that affects one member is likely to affect all.

• You are a member of a team where each individual has a specific role and specific responsibilities
• Who are you accountable to?

Interpersonal Interaction.
• A group may be defined as a number of individuals who are interacting with one another. According to this definition, a group does not exist unless interaction occurs. It is this interaction process that distinguishes the group from an aggregate.

Structured Relationships.• A group may be defined as a collection of individuals whose
interactions are structured by a set of roles and norms. According to this definition, the individuals are not a group unless their interactions are so structured. A social-psychological group is an organized system of two ore more individuals who are interrelated so that the system performs some function, has a standard set of role relationships among its members, and has a set of norms that regulate the function of the group and each of its members.

Mutual Influence.
• A group may be defined as a collection of individuals who influence each other. Individuals are not a group unless they are affecting and being affected by each other; therefore, the primary defining characteristic of a group is interpersonal influence. A group is two or more persons who are interacting with one another in such a manner that each person influences and is influenced by each other person.

Motivation.
• A group may be defined as a collection of individuals who are trying to satisfy some personal need through their joint association. According to this definition, the individuals are not a group unless they are motivated by some personal reason to be part of a group. Individuals belong to the group in order to obtain rewards or to satisfy personal needs. It is questionable that a group could exist unless its members’ needs are satisfied by their membership.

GROUP DYNAMICS• Emphasis on process of group rather than group as an object.
Thinking thorough this a bit will help us use groups not just rotely as received tools but as creative health practitioners who work with group process.
• What a group needs to be. Roles, expectations, norms, and procedures within group
process. Understanding the development and life of a group process.
CREATING PRODUCTIVE GROUPS
A pseudogroup• A traditional work group• An effective group• A high-performance group

Group Dynamics
• Robert Bales (1965) three themes: dependence on the leader; pairing among members for emotional support; fight-flight reactions to a threat to the group.
• Shultz (1958) three issues: affection; inclusion; and control.
• Tuckman (1965) five stages: forming; storming; norming; performing; and adjourning.

• Forming: uncertainty in which members try to determine their place in the group and the procedures and rules of the group.

• Storming: conflicts begin to arise as members resist the influence of the group and rebel against accomplishing the task. Members often confront their various differences and conflict management is the focus of the group.

• Norming: group establishes some consensus regarding a role structure and a set of group norms for appropriate behavior. Cohesion and commitment increase.

• Performing: group members become proficient in working together to achieve the group’s goals and become more flexible in developing its patterns of working together.

• Adjourning: the group disbands.

Stages to Group Development*1. Defining and Structuring Procedures2. Conforming to Procedures and Getting Acquainted3. Recognizing Mutuality and Building Trust4. Rebelling and Differentiating5. Committing and taking ownership of the goals, procedures,
and other members6. Functioning maturely and productively7. Terminating* Johnson and Johnson

What is supervision?
www.richardelovich.com 30

Supervision
• Managing the program • Monitoring the effectiveness of the individual
worker, the team, the service delivery, and the effectiveness of standards, codes of ethics and conduct
• Developing reflective practice in harm reduction oriented service programs
• Assisting individual workers and the team to apply and adapt concepts, approaches, and skills from a training to their practice
www.richardelovich.com 31

ARE CONCEPTS AND SKILLS IN TRAININGS APPLIED AND INTEGRATED INTO THE WORK PEOPLE DO?
www.richardelovich.com 32

• On a Scale of 1 to 10 1 = not evident in the work… 10 = very evident in the work
• Harm Reduction• Stages of Change• Motivational Interviewing• A Strengths Based Approach
• How is each reflected in the work?
www.richardelovich.com 33
PROGRAM PHILOSOPHY
Why articulate program philosophyAssumptions about drug usersHarm reduction among drug usersIntravention and interventionImplications of harm reduction in all domains

Program Philosophy
• An evidence based program philosophy that: examines and clarifies underlying assumptions—about drug use, about the people who use drugs, about opioid dependence and people who are opioid dependent,
• Examines and clarifies the principles, goals, processes, technologies and acceptable outcomes of harm reduction.

Why have a Program Philosophy
• The program philosophy should be consistently reflected in program policies and practices.
• In order to be evaluated, a program’s specific policies and procedures—like any health or medical program—need to be logically consistent with its overall philosophy.
• Moreover, programs need to inform and, if needed, clarify philosophy, policies, and procedures to each and every member of the service delivery team and to clients/patients, their relatives, as well as members of the local community.

Exercise
• In smaller groups, divide a flip chart sheet into three components of harm reduction program philosophy:
• examine and clarify underlying assumptions—about drug use, about the people who use drugs, about patterns of opioid dependence and people who are opioid dependent
• Identify and discuss the principles, goals, processes, technologies, and outcomes of harm reduction.
• How should the program philosophy be consistently reflected in program policies and practices.

Each group presents:

Putting Harm Reduction Trainings Into Action
Understanding the Harm Reduction Model to apply it consistently in service
delivery to injection drug users
www.richardelovich.com 39
Managing a Harm Reduction Oriented Service Program
– Management of Staff• Team Meetings• Supervision• Clear Policies and Procedures• The Learning Environment• Reducing Burn-out
www.richardelovich.com 40

Where should we focus?
• Each supervisor presents a thumbnail sketch of a client. Getting to the bottom line?
• Why now?• What are themes that emerge?• Selecting a case to examine that helps identify
a problem or problem solving, engages the group in thinking about practice, and is an opportunity to learn together
www.richardelovich.com 41

www.richardelovich.com 42

Trainings
• Harm Reduction• Stages of Change• Motivational Interviewing• A Strengths Based Approach• Reflective Practice
www.richardelovich.com 43

Two Salient Features of Harm Reduction
1. the harm reduction model is clearly predicated upon the recognition that some “behavioral outcomes” have greater situational importance than others. Specifically, the harm reduction model prioritizes the prevention of HIV transmission.
2. As a strategy by which to achieve reduction in the transmission of HIV, harm reduction is based on the recognition that particularly behavioral goals must be tailored to the specific needs and real-life capacities of the individuals to whom they are directed.
44www.richardelovich.com

www.richardelovich.com 45

www.richardelovich.com 46

www.richardelovich.com 47
www.richardelovich.com 48

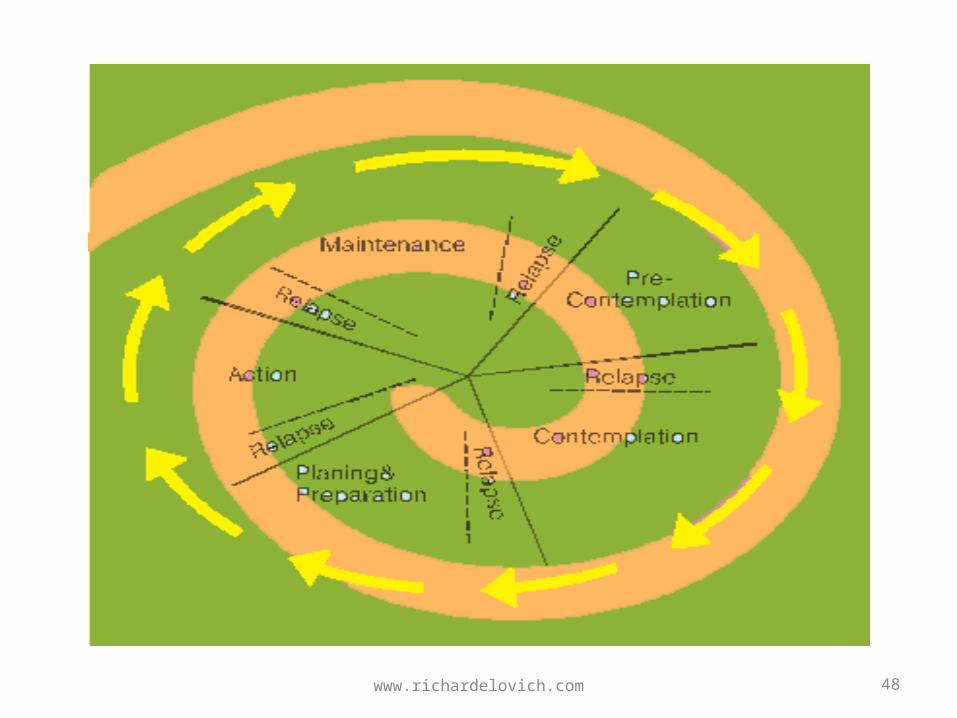
• Research consistently shows that (1) attunement to drug user readiness, interest, or capacity to change, i.e., attunement to individual drug users expectations of his encounter with help(ers), and (2) the quality of the helping relationship (respect, credibility, trust, rapport) are directly associated with positive results.
www.richardelovich.com 49

www.richardelovich.com 50

www.richardelovich.com 51

Facets of Harm Reduction
• Acknowledges real and tragic harms associated with licit and illicit drug use.
• Seeks to have greatest impact on reducing drug related problems by engaging people wherever they are on spectrum of drug use.
• Involve drug users in setting realistic incremental goals for change.
52www.richardelovich.com

Facets of Harm Reduction II
• Provides risk reduction options rather than seeking to impose uniform label or outcome for all participants.
• Uses low threshold easy-to-access and flexible services to encourage engagement by the most reticent or chaotic.
• Fits the service model to the population, rather than population to the service model.
53www.richardelovich.com
Facets of Harm Reduction III
• Integrates harm reduction into other health & human services or into natural settings of target population.
• Rather than the demand for abstinence as the only acceptable goal, uses a hierarchy of goals, with the immediate focus on addressing the most pressing and practical needs.
54www.richardelovich.com

Facets of Harm Reduction IV• The harm reduction models serves a service delivery
principle in which the task is that of providing risk reduction education and the tools that will enable an individual to make the most health-promoting choices possible in a given set of circumstances and situations.
• As such, it contrasts rather sharply with approaches to service delivery that are predicated upon “cure” versus “failure to cure” or upon idioms of failure, blame, and deviance.
• It also contrasts with “incentive” strategies for behavioral change that rely on the mediums of coercion, penalty, and criminalization.
55www.richardelovich.com

Facets of Harm Reduction V• The harm reduction model contrasts with many of the
more “mainstream” or “established” behavior change models whose behavioral goals are derived from outside the particular social and economic conditions and context in which drug users live.
• Establishing an effective relationship with an DU can be more important than telling the individual that he should not use drugs or he should get into treatment.
• The health and well-being of the individual DU and the direct response to the needs that he or she presents and defines as primary, are first-order goals of service delivery, not an abstract set of agency standards and procedures that have been “cut and pasted” across all interactions.
56www.richardelovich.com
Facets of Harm Reduction VI
• In attempting to develop services for DUs, it is critical that we remember to fit the service model to the drug user, rather than the drug user to the service model.
• The harm reduction model reminds us that we cannot offer constructive assistance until we know that person to whom we are reaching out, not as an epidemiological category or as a marginalized or stigmatized sub-population or class of people, and that we cannot know that person until we are prepared to we are prepared to listen and provide them with the opportunity to be heard.
57www.richardelovich.com
“Cure” versus “Failure to Cure”• Many service delivery systems focused on abstinence from drugs as the
only healthy and safe choice, an initiative that has proven to be largely a failure among injection opiate users.
• The clear message was that drug use was wrong and that use endangered access to services.
• Implicitly, emphasis on an abstinence model, communicated to drug users who failed to measure up to this standard that they were in some way wrong, deficient, and perhaps unworthy of services or the community. Along with the criminalization of drug possession and the stigmatization of heroin and opiate dependence, this has led many drug users to either stay away, alienated, or to misrepresent their drug use, thus negating any possibility of therapeutic discussion, including a critical opportunity for HIV intervention.
58www.richardelovich.com

• Many service delivery systems focused on abstinence from drugs as the only healthy and safe choice, an initiative that has proven to be largely a failure among injection opiate users.
• The clear message was that drug use was wrong and that use endangered access to services.
• Implicitly, emphasis on an abstinence model, communicated to drug users who failed to measure up to this standard that they were in some way wrong, deficient, and perhaps unworthy of services or the community. Along with the criminalization of drug possession and the stigmatization of heroin and opiate dependence, this has led many drug users to either stay away, alienated, or to misrepresent their drug use, thus negating any possibility of therapeutic discussion, including a critical opportunity for HIV intervention.
59www.richardelovich.com

The Fallacy of “Anchoring”• The provider makes an assumption based on available
data and throws an anchor down. We may act from biases or feelings or what others expect from us.
• Everything gets built up from the anchor.• Despite challenging data, i.e. low numbers of IDUs
engaged in needle exchange, the provider is reluctant to pull up anchor and look for alternative area to look.
• You lose your wallet on a dark street but you only look for it under the street lights. Grounded ethno-epidemiology looks outside the convenience biases of the street lights. Coupled with good outreach, this is a good beginning for program improvements.
60www.richardelovich.com

Putting Harm Reduction Trainings Into Action
Understanding the Harm Reduction Model to apply it consistently in service
delivery to injection drug users
www.richardelovich.com 61

A Strengths Based Approach• First, to establish a helping or therapeutic alliance, the counselor needs to develop
what is sometimes called “accurate empathy,” which means, putting his or her own opinions or judgments aside in order to accept the person as he is (rather than who the counselor thinks he should be), so that the individual doesn’t have to justify or defend himself.
– Accurate empathy on the part of the counselor means being genuinely interested in understanding the individual’s perspective on his experiences or allowing him to describe the situation as he sees it.
– This is distinct from the medical practice of labeling or diagnosing a person and his behavior. • Secondly, to help someone change, the counselor must have hope for this
particular person, no matter how hopeless he seems or feels about himself. The counselor must see within the person possibilities, resiliencies, and capacities for change and even transformation.
• Thirdly, research on optimal treatment outcomes demonstrates that in addition to establishing respect and trust, the counselor needs to be attuned to the individual’s stage of readiness for change. Change can be incremental, and clients are viewed as amenable to change when abstinence is not the only option.
62www.richardelovich.com

Establishing the “Quozon”• First, to establish a helping or therapeutic alliance, the counselor needs to develop
what is sometimes called “accurate empathy,” which means, putting his or her own opinions or judgments aside in order to accept the person as he is (rather than who the counselor thinks he should be), so that the individual doesn’t have to justify or defend himself.
– Accurate empathy on the part of the counselor means being genuinely interested in understanding the individual’s perspective on his experiences or allowing him to describe the situation as he sees it.
– This is distinct from the medical practice of labeling or diagnosing a person and his behavior. • Secondly, to help someone change, the counselor must have hope for this
particular person, no matter how hopeless he seems or feels about himself. The counselor must see within the person possibilities, resiliencies, and capacities for change and even transformation.
• Thirdly, research on optimal treatment outcomes demonstrates that in addition to establishing respect and trust, the counselor needs to be attuned to the individual’s stage of readiness for change. Change can be incremental, and clients are viewed as amenable to change when abstinence is not the only option.
63www.richardelovich.com

Fundamental Tools for all members of the team: Creating the “Quozon”
• Accurate empathy• Open-ended questions• Reflective listening• Eliciting ambivalence• Exploring ambivalence• Motivational Interviewing

Accurate Empathy• The principle of empathy is acceptance.• Through respectful reflective listening the counselor
seeks to understand the client’s perspective without judging, criticizing or blaming.
• Acceptance is not the same thing as approval or agreement.
• Ironically, this kind of acceptance of people as they are seems to free them to change, whereas insistent non-acceptance tends to immobilize the change process. The person focuses on defending, arguing, winning the argument or the counselor’s acceptance, rather than self- reflection and self-assessment.

Accurate Empathy cont
• Express empathy, which helps create the safe and non-judgmental setting for the participant, regardless of the setting
• Skillful reflective listening is a fundamental tool of motivational interviewing
• Ambivalence is accepted as a normal part of human experience and change, rather than a pathology or sign of incapability or defensiveness or resistance.

Figure I Источник: Прохаска, Норкросс, ДиКлименте (1994)
Прекращение
Поддержание
Действие
Подготовка
Созерцание
Присозерцание
Figure I Источник: Прохаска, Норкросс, ДиКлименте (1994)
Прекращение
Поддержание
Действие
Подготовка
Созерцание
Присозерцание
67www.richardelovich.com

68www.richardelovich.com

69www.richardelovich.com

70www.richardelovich.com

Common ways to raise the issue of safer behaviour include:
• situational cues: if the user has an abscess, complains of sickness, says they have recently been to hospital or had hepatitis, or a recent HIV test, these are all good points at which to start talking about less risky injection
• incorporate a HIV prevention message in a broader conversation focusing on IDUs’ health in general or the social, health and other problems of IDUs
• an occasional chat like `How are you', `How are things going', might be enough to get a conversation started in which health will be one subject

A framework is like a floor plan, a blueprint, or way of looking at something
• Let’s look at the staff-client interaction framed by three Habermasian concepts: communicative action and strategic action; system and lifeworld; and macro and micro interactional(Habermas, 1984).
• Habermas’s concepts rooted in the early critical theory of the Frankfurt School have been utilized in medical sociology to retheorize and illuminate doctor-patient relations in terms of doctor-patient communication and interactions in ways that integrate micro-macro perspectives (Scambler, 2001; Scambler G., 2001; Waitzkin, 1989, 2001).
www.richardelovich.com 72

The Professional – Client InteractionCrudely rendered, the tension between communicative action and strategic action for Habermas is between a transaction whose outcomes are achieved jointly and one appearing to be mutually structured but whose results in fact organized toward a particular end.
www.richardelovich.com 73

Communicative ActionCommunicative action refers to interaction mediated through talk and oriented to ‘consensual coordination of individually planned patterns of action. Instances of communicative action express claims that are subject to critical evaluation. Speakers can ‘rationally motivate’ hearers to accept their contributions because they can assume the ‘warranty’ for providing good reasons that would stand up to hearers’ challenges of claims, i.e., that the communication is true or not true, appropriate or inappropriate, justifiable or unjustifiable, sincere or not sincere.
www.richardelovich.com 74
Strategic ActionStrategic action on the other hand occurs when one party aims through speech to produce an effect on others. He instrumentalizes speech for purposes that are contingently related to what is said. Strategic action is oriented to achievement of an object rather than to understanding. In one form, open strategic action, the clinician/speaker openly pursues an aim of influencing the hearer. Here, there is an associated claim to power, as in asymmetrical relations with a subordinate.
www.richardelovich.com 75

The tension between the twoCommunicative action is one where one interlocutor (the patient) communicates with another (the doctor) in such a way that identification and assessment of a problem is achieved jointly, and action (treatment) emerges from the encounter.
In “strategic” communication, by contrast—the kind we have seen to be most common in the funded service setting--the exchange is organized toward a particular desired end. While the doctor may engage the patient in conversation, he has objectives in the encounter that exist prior to and with little consideration of what the patient says and he hears.
www.richardelovich.com 76

The System and the LifeworldFor Habermas, this tension between strategic action and communicative action exists within a system which is also divided—between the system of power relations and that of the lifeworld—the circumstances and sets of relations and resources in which a person experiences the macro structures. When a person enters a hospital he becomes a patient, is to a lesser or greater extent isolated from the lifeworld, and for the period he is there is subject to objectives and procedures of the system of knowledge and expertise that is independent of him. If, by contrast, a patient is treated on an outpatient basis, he remains embedded in a different set of relations that also determine his ability and interest to engage.
www.richardelovich.com 77

The System and the Lifeworld (con’t)Ideally, for Habermas , the life world and communicative action are in harmony, reflecting a social world within which individuals interact with others to decide and organize their affairs in the private sphere of their families or households or in the wider public sphere. By contrast, strategic communication sits more comfortably in the sphere of the system, comprised of the economy and state, each operating with their own apparatus, financial gain and power. When economy and the state intrude in inappropriate and unaccountable ways into the lifeworld they can be said to ‘colonize’ it. In just this fashion the ‘voice of medicine’ has partially colonized the ‘voice of the lifeworld’ in hospital doctor-patient encounters and relations.
www.richardelovich.com 78

The System and the Lifeworld (con’t)How do we connect this framework with a better understanding of harm reduction?
How does this help us think about and identify tensions that may exist between agency imperatives and the culture in service delivery (the system) and the communicative action and lifeworld pattern expected in harm reduction approaches.
What does this have to do with reflective practice?
www.richardelovich.com 79

www.richardelovich.com 80

Maslow’s Hierarchy of Needs
81www.richardelovich.com
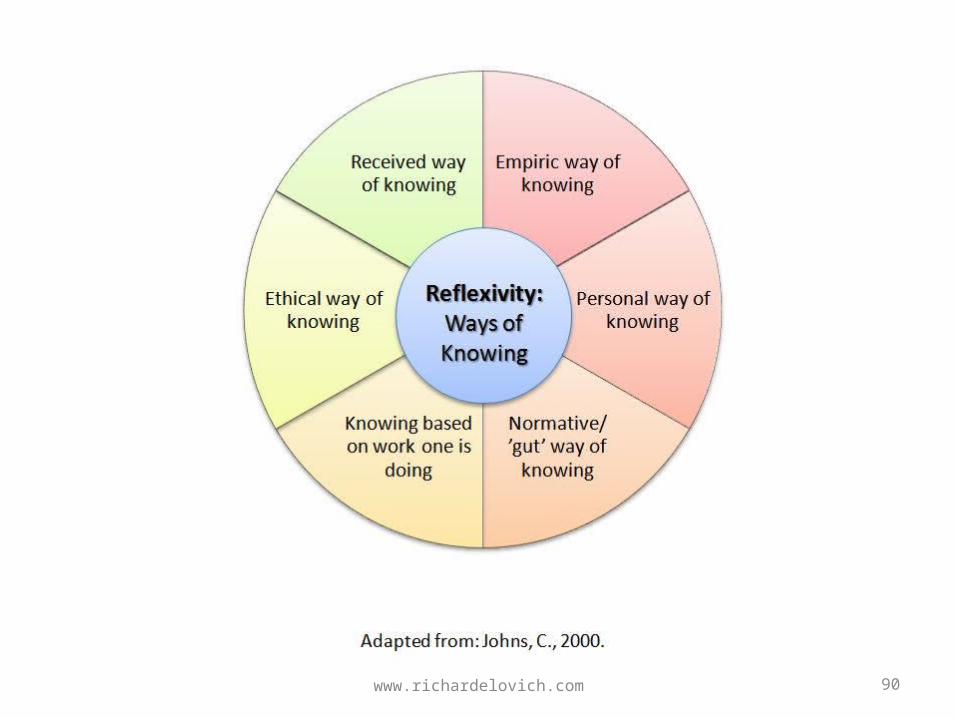
Reflective Practice
www.richardelovich.com 82

www.richardelovich.com 83

www.richardelovich.com 84
www.richardelovich.com 85

www.richardelovich.com 86

www.richardelovich.com 87

www.richardelovich.com 88

www.richardelovich.com 89
www.richardelovich.com 90

Monitoring and Evaluation
www.richardelovich.com 91

92
ASTOR MODEL FOR PROGRAM MONITORING
• The purpose of organizing program The purpose of organizing program description according to ASTOR Model description according to ASTOR Model (Sigma Research, UK) is for clarity and (Sigma Research, UK) is for clarity and coherence, connecting programmatic aims coherence, connecting programmatic aims with settings, target populations, with settings, target populations, objectives and activities, and resources. objectives and activities, and resources. Aims can be measured for impact.Aims can be measured for impact.
www.richardelovich.com

93
Aims of ASTORS
• Aims are (1) identified and therefore Aims are (1) identified and therefore pragmatically anchored in preliminary needs pragmatically anchored in preliminary needs assessment and ongoing assessment in action assessment and ongoing assessment in action of gaps, unmet needs, or specific areas in need of gaps, unmet needs, or specific areas in need of change; (2) exist in logical relation to setting, of change; (2) exist in logical relation to setting, target groups, objectives and activities and target groups, objectives and activities and resource allocation. Objectives can be resource allocation. Objectives can be monitored and the aim or impact can be monitored and the aim or impact can be assessed or measured.assessed or measured.
www.richardelovich.com

94
Setting of ASTOR
• Setting (context)Setting (context): Where does intervention : Where does intervention occur? How do people come into contact occur? How do people come into contact with it?(Derived, again, from needs with it?(Derived, again, from needs assessment.)assessment.)
www.richardelovich.com

95
Target of ASTOR
• Target groupTarget group: Among whom is the : Among whom is the proposed change intended to occur? proposed change intended to occur? What is the profile of the population we are What is the profile of the population we are targeting? Is the epidemiological category targeting? Is the epidemiological category or population we use meaningful “on the or population we use meaningful “on the ground” to the people we are targeting for ground” to the people we are targeting for an intervention?an intervention?
www.richardelovich.com

96
Objectives of ASTOR
• Objectives and methodsObjectives and methods: What does the : What does the intervention consist of? Monitorable intervention consist of? Monitorable activities in program to achieve aim.activities in program to achieve aim.
www.richardelovich.com
97
Resources of ASTOR
• ResourcesResources: Human and financial costs. : Human and financial costs. How much time will it take? How much time will it take?
www.richardelovich.com

98
NEEDS ASSESSMENT• Needs assessment allows us to draw evidence
together to determine what variables affect the dependent variable. If we know the variables that affect the incidence of injecting drug use we can construct a more detailed and operational layer of aims. From the map of variables, we start turning the variables into aims. For example, if not having information about the association of injection drug use to exposure to HIV has an impact on the numbers of young people starting to inject heroin, then we will construct a specific aim to increase awareness.
www.richardelovich.com

99
• Mapping out the aims, based on needs assessment, and then situating them within a larger social picture, allows us to build up a complex picture of what effects drug demand in a specific population. Programs start with the best aims they can come up with based on the evidence available. Aims describe the situation we are working towards; or, stated differently, need is an absence of an aim being met. As health professionals, we determine the ideal situation we think a population should be in and then map how far away from that situation the population is. It is the practitioner’s job to move the population closer to the aims we have for them.
www.richardelovich.com
Monitoring con’t
• Consistent use of unique identifier systems across all program encounters and activities can produce data for a report on service utilization
• Qualitative interviews can add insight and deeper understanding of utilization patterns.
www.richardelovich.com 100

Criteria for an Evaluation I.• An evaluation cannot be undertaken without
first determining through monitoring reports that:
• (1) there is a logical connection between the aim and the objectives of the activity;
• (2) members of the target population are being reached in the settings in which the provider agreed upon and in sufficient numbers and with sufficient regularity;
• (3) proposed activities are taking place in the manner that was proposed;
• (4) resources were available to support these activities.
www.richardelovich.com 101

Client Driven Evaluation II.
• Clients in a focus group identify domains that are of concern to them, e.g., health, housing, social relationships, nutrition, drug use, legal status, etc.
• Within each domain, clients’ brainstorm and identify first individually and then as a group: worst outcome, best outcomes, and incremental outcomes.
• How would they know?www.richardelovich.com 102

Client Driven Evaluation III.
• Clients discuss and try to arrive at a group consensus of findings.
• This identical process is repeated in 1-2 other focus groups.
• Findings are refined and tested out in 2-3 other groups.
www.richardelovich.com 103

Client Driven Evaluation IV.
• This can then be constructed as both a quantitative and qualitative evaluation that is consistent with harm reduction and peer-driven.
www.richardelovich.com 104

Sources for this Training and Resource Material I.
• Burrows, D. (1999). How to Start and Manage a Needle Exchange Program: A quide for countries in Central and Eastern Europe and Newly Independent States of the former Soviet Union: International Harm Reduction Development
• Clatts, D., Atillasoy. (1995). Hitting A Moving Target: The Use of Ethnographic Methods in the Development of Sampling Strategies for the Evaluation of AIDS Outreach Programs for Homeless Youth in New York City. In A. Lambert, Needle (Ed.), Qualitative Methods in Drug Abuse and HIV Research. Rockville: NIDA Research Monograph.
• el-Bassel, N., & Gilbert, L. (2002). Women's Wellness Treatment. New York: Columbia University School of Social Work.
• Elovich, R. (1998). Harm reduction counseling skills for addiction professionals. Albany, NY: New York State Office of Alcoholism and Substance Abuse Services.
• Elovich, R. (2006a). Promising Practices: Drug Demand Reduction Program’s Treatment and Rehabilitation Improvement Manual. Tashkent: USAID Drug Demand Reduction Program in Central Asia.
• Elovich, R. (2006b). Starting Drug Treatment 'Where People Are At': Acupuncture and Treatment Readiness. NADA India Foundation News Substance Use and HIV/AIDS, January, 2006.
• Elovich, R., & Wolfe, D. (2003). Manual for Primary Care Providers: Effectively Caring for Active Substance Users. New York: New York Academy of Medicine.
• Greenhalgh, T., Robb, N., Scambler, G. (2006). Communicative and strategic action in interpreted consultations in primary health care: a Habermasian perspective. Soc Sci Med(63), 1170-1187.
• Habermas, J. (1984). The theory of communicative action. Boston: Beacon Press.
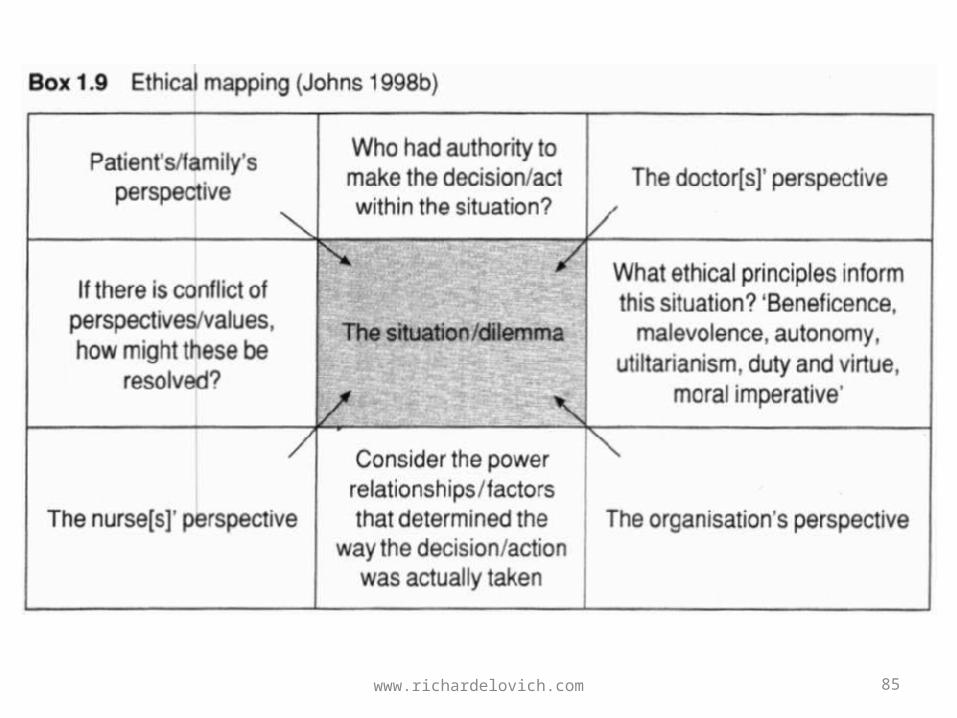
• Johns, C. (2000). Becoming a reflective practitioner : a reflective and holsitic approach to clinical nursing, practice development, and clinical supervision. Oxford ; Malden, MA, USA: Blackwell Science.
• Johnson, D. W., & Johnson, F. P. (2002). Joining together : group theory and group skills (8th ed.). Boston: Allyn and Bacon.
www.richardelovich.com 105

Sources for this Training and Resource Material II.
• Marlatt, G. (1985). Relapse Prevention: General Overview. In G. a. G. Marlatt, J (Ed.), Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors (pp. 3-348). NY: Guilford Press.
• Marlatt, G. (2000). Harm Reduction: Basic Principles and Strategies. The Prevention REsearcher, 7(2).
• Miller, W. R., & Rollnick, S. (2002). Motivational interviewing : preparing people for change (2nd ed.). New York: Guilford Press.
• Munson, M. A., Schmitt, R.L. (1996). Triggering and interpreting past drug-related frames: An insider's view of a treatment modality at an adolescent drug treatment facility. Studies in Symbolic Interaction, 20, 39 - 72.
• Prochaska, D. (1986). Toward a Comprehensive Model of Change. In M. W. a. H. N (Ed.), Treating Addictive Behaviors: Processes of Change. New York: Plenum Press.
• Reinarman, C., Waldorf, D, Murphy, S. and Levine, H. (1997). The Contingent Call of the Pipe: Bingeing and Addiction Among Heavy Cocaine Smokers. In C. a. L. Reinarman, H. (Ed.), Crack in America: Demon Drugs and Social Justice (pp. 77-97): University of California.
• Ruefli, T., Rogers, SJ. (2004). How do drug users define their progress in harm reduction programs? Qualitative research to develop user-generated outcomes. Harm Reduction Journal (HRJ), 1(8), 1-13.
• Scambler, G. (2001). Habermas, critical theory and health. London ; New York: Routledge.
• Scambler G., a. B. N. (2001). System, lifeworld, and doctor-patient interaction. In G. Scambler (Ed.), Habermas, Critical Theory and Health. London: Routledge.
• Taleff, M. (2006). Critical Thinking for Addiction Professionals. New York: Springer Publishing Company.
• White, M. E., D. (1990). Narrative Means to Therapeutic Ends. NY: W.W. Norton.
www.richardelovich.com 106