developing and financing ancillary facilities - ihaconnect.org · long term ground lease = 50-75...
TRANSCRIPT
Developing and Financing Ancillary Facilities

2
Agenda• Mixed Use Trends• Development Process / Hypothetical• Own vs Lease• Financing Structures• Case Studies

Ullom’s Rules of Lawyer Competency• There exists in nature an inverse relationship between the number of
syllables used by a lawyer and his/her actual competence.
• The use of citations and references to IRS regulations serves as further evidence of one’s lack of understanding.
• Clients should actually understand their transactions.
• A Lawyer’s goal ought not be to make his/her clients depend upon him/her.

Mixed Use Development Trends• Healthcare
– Shift from Inpatient to Outpatient
– Fewer “Towers”– Ambulatory and Outpatient
Facilities– New Neighborhoods and
Markets– Re-purposing Retail Space
4

Mixed-Use Development Trends• Medical Village
– Freestanding ER– Urgent Care Clinics– Ambulatory Facilities– Imaging– Wellness / Therapy– Medical Office– Apartments / Senior Housing / Assisted Living– Skilled Nursing– Restaurant– Retail– Hotel
5

Mixed Use Implications• Development and Construction Process• Ownership• Taxes • Finance• Operations
6
Hypothetical Project• Non-profit hospital is considering an ambulatory care center
that will include a free-standing emergency department or urgent care center, imaging center, lab and medical office space
• Hospital has identified a site for the project that is located off-campus
• Hospital doesn’t have the expertise to oversee the planning, design and construction of the project
7

Practical Considerations• Site selection • Developer selection• Own vs Lease • Ownership options• Ownership advantages• Leasing advantages
8

Site Selection • Is the site ideal for the proposed use?
– Accessibility– Data analytics – Land cost– Infrastructure
• The one remaining site– Explore all options– On-market vs off-market – Greenfield vs redevelopment
9
Developer Selection• Identifying the right development partners
– Access to capital– Size of project– Provider alignment
• Experience and efficiencies • Fee for service vs developer ownership• Request for Proposals• Asking for incentives
10

Own vs Lease• Now more than ever organizations are struggling with
ownership decisions• Historical policy of owning “core” assets may no longer hold
– Accounting rule changes– Nature of “core” assets– Costs of Capital– Property Tax Implications
• Reverse monetizations make headlines
11

Ownership Options• Traditional ownership options
– Ownership of land and the building• Non-traditional ownership options
– Condominium form of ownership– Ground leasing arrangements– Joint venture with other providers– Excess land held for future development– Hybrid model
12
Ownership Advantages• Lowest Cost of Capital
– Refresher: One may utilize tax-exempt financing to finance capital projects owned and used by a 501(c)(3) organization in furtherance of its charitable purpose
• Control• Clear Balance Sheet Treatment• Property Tax Exemption
13
Leasing Advantages• Flexibility• Some Level of Off-Balance Sheet• Preservation of Capital and Capital Capacity (maybe)• Some level of control through ownership restrictions, use
restrictions and purchase options
14
Tax-Exempt Financing Basics• Tax-exempt financing
– Owned by a 501(c)(3) organization or governmental unit• Ownership for tax purposes• Capital leases• Joint ventures
– Used in furtherance of charitable purpose• Private use
– Leases– Service/management contracts
• Unrelated trade or business use• Allocation rules
– Various other tax restrictions• Useful Life vs. WAM• Post-issuance compliance
15

Own and Borrow• Pros
– Lowest cost of capital, if qualified for T/E financing
– Property tax exemption– Project delivery options– Control
• Cons– All on balance sheet– More complicated– Transaction costs– Market disclosure– Split development/financing
501(c)(3) Entity
Fee Developer
Investors / Lenders
T/E or Hybrid Financing
Very traditional structure. Health Care System issues debt (likely tax-exempt bonds) through governmental issuer and engages a
fee only developer to build the building.
16

501(c)(3) Entity
Developer REIT
REIT Investors
Long Term Ground Lease = 50-75 years
Improvements = Operating Lease Back
Build, Monetize, Leaseback
• Pros– Partial off-balance sheet
treatment*– Turn-key development/financing– Greater project delivery control– Simplified execution
• Cons– Property tax– Higher cost of capital/lease rate
Typical Developer/REIT Structure. Health System executes turn-key arrangement with Developer who
sources capital, builds building and sells to REIT. Developer/REIT may be on in the same or separate
entities. Alternatively, Health System may fund construction of building and “monetize” (sell)
building to REIT when completed.
17
*Accounting treatment subject to accounting rules applicable to each health care entity. Consult your accounting advisors for an assessment of accounting treatment.

501(c)(3) Entity Developer
REIT Investors
Long Term Ground Lease = 50-75 years
Non-Qualifying Improvements = Operating Lease Back
Hybrid Solution• Pros
– Lower blended cost of capital– Partially off-balance sheet*– Partial property tax exemption
• Cons– Partially on-balance sheet– Partial property taxes– More complicated– Transaction costs– Market disclosure
Qualifying Improvements = Capital LeaseTri-Party Lease to Include Issuer
T/E Bond Market
Capital Lease Portion Marketedas Tax-Exempt Obligation
Hybrid to take advantage of tax-exempt portion. Health System signs turnkey agreements with Developer. Taxable portion is traditional Developer/REIT lease. Tax-exempt
portion is separated (condo) from remainder and owned by Health System or leased under a capital lease by Health System. Capital for tax-exempt portion sourced at tax-
exempt rates.
18
*Accounting treatment subject to accounting rules applicable to each health care entity. Consult your accounting advisors for an assessment of accounting treatment.

The Best of Both Worlds• Hybrid Solutions for Mixed Use Projects• “Own” the Portion Used by Nonprofit/Gov’t
– Fee Ownership; Condominium; Capital Lease; Installment Purchase
• Lease or Allow Third Party Ownership for Private Portion – Operating Lease– Third Party Ownership
19
Hybrid Benefits• Pros
– Lower blended cost of capital– Partially off-balance sheet*– Partial property tax exemption
• Cons– Partially on-balance sheet– Partial property taxes– May be more complicated– Transaction costs– Market disclosure
20
*Accounting treatment subject to applicable accounting rules. Consult your accounting advisors for an assessment of accounting treatment.

501(c)(3) Entity
Fee Developer
Conduit Owner
Investor
Long Term Ground LeaseTerminates Upon Repayment
Improvements = Operating Lease BackLease Includes Tax Use Covenants
T/E Obligation• Secured by Lease
Payments & Leasehold Mortgage
• Recourse to Project• Non-Recourse to Issuer
Tax-Exempt Credit Tenant Lease / “Conduit Ownership”• Pros
– Lower cost of capital• Lower than REIT, not as
low as Own and Borrow
– Off-balance sheet*– Property tax exempt
• Dependent on state law
• Cons– Unknown market/
investor reception/funding vehicle– More complicated structure– Market disclosures
Relatively new structure applied in Higher Education, new structure to the Healthcare market. Health System enters into an operating lease with another 501(c)(3) or Governmental Unit that will serve as the owner of the building. Health System manages development and construction in same way as if Health System owned facility. Because both ownership and use are by 501(c)(3) and/or Governmental Unit, building may be financed tax-exempt. Building is on owner’s balance sheet, not Health System’s.
21
*Accounting treatment subject to accounting rules applicable to each health care entity. Consult your accounting advisors for an assessment of accounting treatment.

Case Study #1 – Sun Devil• Hospital Campus Development • Two Components
– ASC and Imaging Center (Hospital Portion)– Medical Office Building (Private Portion)
• Hospital Owns All Land – Land Leases Private Portion to Developer
• One Developer; Integrated and Efficient Construction Process• Hospital to Issue Bonds and Own Hospital Portion• Developer to Own Private Portion, Lease Space to Hospital
and Third Parties22
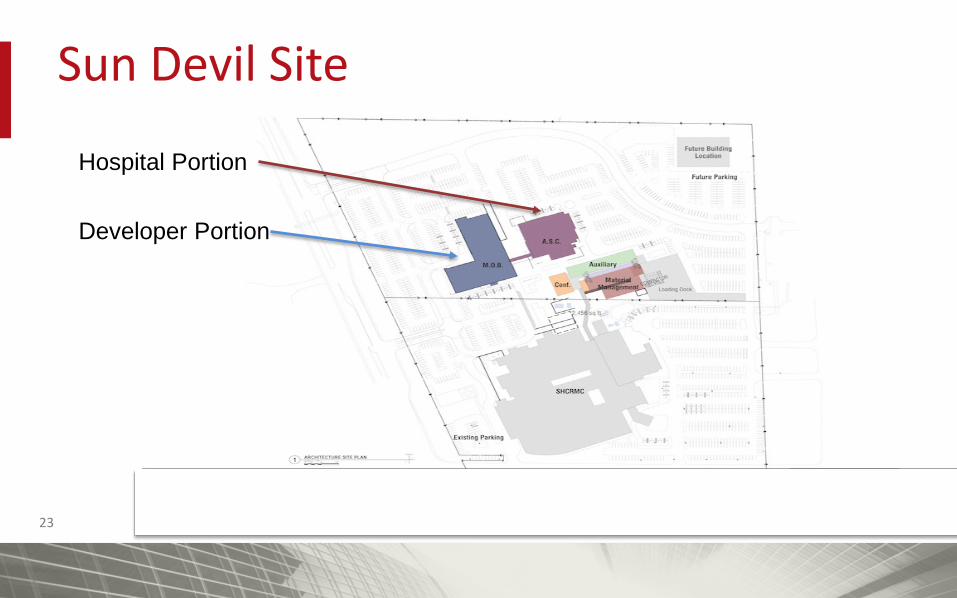
Sun Devil Site
23
Hospital Portion
Developer Portion

Sun Devil Financing• Multiple Lenders
– Bond Purchaser = Bank #1– Developer Lender = Bank #2
• Bank Rights Conflicts Arise on Eve of Closing• Delayed Closing and Nearly Missed Construction Season
• Financing and Use Rights Were Not Coordinated• Development and Construction was Integrated, but not
Financing24
Case Study #2 – Rocky Mountain High
CLIENT DISCUSSION:• We would like a shiny new Wellness Center on campus• A Wellness Center meets our strategic plans and would be a great success• We will need some space in the Center for appropriate service lines• By the way, we can’t spend any money • Oh yea, and we don’t want to actually own the Wellness Center because
we don’t want it on our balance sheet• Oh, one more thing -- we can’t take on any debt or any obligation that
looks like debt or really any obligations at all• We’d like it built and operating ASAP• THANKS SO MUCH FOR YOUR HELP, YOU’RE THE BEST!25

2626
It’s Alive! Creativity to Meet Goals
Nonprofit NewcoHealth System
Developer / Manager PROJECT
Development Agreement
Long TermGround Lease
ManagementAgreement
Condit Issuer
Investors
Loan AgreementPromissory Note
Tax Exempt Bonds1.Senior Series2.Mezzanine Series3.Zero Coupon (“Equity”)
Investment Bankers
Local Government
Community College
Health System
Newco GovernanceNot Controlled nor Consolidated
27
Closing Comments• Mixed-Use Trends Are Real• More Providers are Considering Ownership• Hybrid and Novel Financing Structures = Lowest Blended Cost• Just Like Development and Construction, Financing Must be a
Coordinated Effort• Creativity is Needed
27

Please visit the Hall Render Blog at http://blogs.hallrender.com for more information on topics related to health care law.
Andrew Dick(317) [email protected]
Anchorage | Annapolis | Dallas | Denver | Detroit | Indianapolis | Milwaukee | Raleigh | Seattle | Washington, D.C.
Jerimi Ullom(317) [email protected]