developing a framework of competencies for medical...
TRANSCRIPT

Developing a Framework of Competencies for Medical Graduate Outcomes
Final Report
February 2011

Report prepared on behalf of Medical Deans Australia and New Zealand Inc by:
Allan Carmichael Dean, Faculty of Health Science University of Tasmania Professor of Paediatrics & Child Health Medical Science 1 17 Liverpool Street Hobart TAS 7000 Tel: 03 6226 4860 Fax: 03 6226 4862 Email: [email protected]
Monique Hourn Project Manager Competencies Project Medical Deans Australia and New Zealand Inc Level 6 173 – 175 Philip Street Sydney NSW 2000 Tel: 02 9114 1680 Fax: 02 9114 1722 Email: [email protected]

Contents Executive Summary............................................................................................................................... 1 Introduction............................................................................................................................................ 3 Scope, methodology and achievements of the project ......................................................................... 4 Future Use and Next Steps ..................................................................................................................12 Conclusion............................................................................................................................................13 Key Outcomes against the Objectives................................................................................................. 14 Appendices.......................................................................................................................................... 16

1
EXECUTIVE SUMMARY In 2010, the Australian Government Department of Health and Ageing (DoHA) provided funding to Medical Deans Australia and New Zealand Inc (Medical Deans) to document competencies for the medical graduate outcomes required by the Australian Medical Council (AMC), and which depend on clinical placements. The AMC’s forty attributes for medical graduates provided the anchor point for the project. The project evolved from priorities identified from the National Clinical Training Review1 prepared by Medical Deans for the Medical Training Review Panel in 2008. That Review confirmed that medical education faced significant pressures to be able to continue to provide quality clinical training places for the current and projected number of medical students. This current work, translating the AMC forty attributes into a framework of competencies has helped to quantify the learning that occurs in a quality clinical placement and thus will assist in addressing the pressures of increased medical student numbers. The project has been a resounding success. Thirty of the AMC graduate attributes have been successfully delineated into Student Learning Outcomes and then competencies which rely on clinical placements to produce a Framework of Competencies for Medical Graduate Outcomes. The Framework has been endorsed by key stakeholders in medical education in Australia. It has provided a platform to bring key people together in medical education to discuss clinical placements and to provide transparency regarding the learning which occurs in a clinical environment. The key outcomes of the project include:
• defining the current competence – based medical education environment • the development of the Attributes Spectrum • the use of Student Learning Outcomes in the delineation process • the development of an interactive framework utilising eight common clinical rotations identified
in the National Clinical Training Review report • the introduction of lists of common procedural and diagnostic skills • extensive stakeholder consultation • delineation of thirty out of the 40forty AMC attributes into Student Learning Outcomes and
then competencies which rely on clinical placements
Substantial research was conducted on competency frameworks, reports, related projects and competency based education occurring in medical schools. The project has relied on two key findings from this research: - the release of a new definition of competence/competency by the International Competence –
Based Medical Education Collaborators in 2010; and
- the concept of tacit and codified knowledge as explored in the Australian Medical Council’s Consultation Paper on Competence – Based Medical Education in August 20102.
1 Medical Deans, National Clinical Training Review Report to the Medical Training Review Panel, Clinical Training Sub-Committee, February 2008. 2 Australian Medical Council, Competence - Based Medical Education, AMC Consultation Paper , August 2010

2
The introduction of the Attributes Spectrum was a major development for the project. The Attributes Spectrum ranks the AMC graduate attributes according to their degree of reliance on a clinical setting thus allowing for all of the AMC graduate attributes to be developed in a clinical placement. Attributes were ranked in three categories, with those in the red zone, the area designated as predominately acquired in a clinical setting, the initial focus for the delineation process into competencies. Student Learning Outcomes were also introduced to help address the paradigm shift from attributes/statements to an outcomes - based education process. The use of the Student Learning Outcomes as an intermediary step assisted with the identification of competencies which relied on clinical placements. The use of mind mapping software to present the draft framework of competencies was a significant development in conceptualising how the Framework could be presented. The incorporation of the mind mapping enabled the AMC graduate attributes to be mapped to the Student Learning Outcomes, then competencies; and then to the eight common clinical rotations as identified by the National Clinical Training Review Report: Surgery, General Medicine, Obstetrics and Gynaecology, Paediatrics, Mental Health, General Practice, Emergency Medicine/Critical Care and Others. The introduction of lists of common diagnostic and procedural skills has refined the Framework further by aiming to identify the diagnostic and procedural skills which the medical student should have attained on graduation. There has been a progressive consultation with key stakeholders across the medical education continuum to assist with the documentation of the competencies which rely on clinical placements. The consultation process culminated in the convening of these stakeholders at a Consensus Conference, with the main outcomes being:
1. Solid endorsement of the Framework 2. Support for the further development of the lists of common diagnostic and procedural skills for
the medical graduate, specifying the level of achievement for the medical graduate.
3. Strong support for the AMC to review their graduate attributes.
The Framework has now also been endorsed by the Deans as a whole. It will provide a useful resource to assist with the development of new clinical placements or as a resource for evaluating existing clinical placements. Medical Deans is appreciative of the support provided by the Department of Health and Ageing which has ensured that the Competencies Project has developed into a project of importance for medical education.

3
Introduction Medical Deans received funding in early 2010 from the Australian Government to develop a framework of competencies for medical graduate outcomes which rely on clinical placements. The objectives of the project were to: 1. Identify the competencies associated with each of the attributes in knowledge, skills and
attitudes/behaviours specified by the AMC for competent medical graduates and which depend on clinical placements.
2. Use the AMC Accreditation Standards and Processes for medical graduates (including International Medical Graduates), the Medical Deans’ National Clinical Training Review report, the Australian Curriculum Framework for Junior Doctors (ACFJD) and any other relevant reports/projects as the basis of the development of a document that maps competencies to AMC prescribed attributes and which enables graduates to practice at the beginning of the PGY1 Year.
3. Ensure engagement of stakeholders in the identification and specification of competencies. 4. Ensure that the competencies documented are appropriate for a graduating medical student to
commence work as an intern in the standard clinical rotations of the intern year (PGY1). 5. Ensure that the competencies enable a graduating medical student to continue to undertake
further learning and clinical training. This report provides a comprehensive account of the manner in which the project was undertaken and the project’s achievements. It also outlines the potential future use of the Framework. A copy of the Framework of Competencies for Medical Graduate Outcomes is attached as a separate document, and a version of the ‘mind mapped’ Framework accompanies this report.

4
Background For medical schools, adequate clinical places are necessary to produce graduates who are competent to practice safely and effectively as interns. It is also essential for graduates to have had the appropriate foundation for further training in any branch of medicine, and for this training to allow for continued professional development throughout their career. This has become critical as numbers of medical students increase The Medical Deans’ Competencies Project grew out of the 2007 - 2008 Medical Deans’ National Clinical Training Review which identified the need for sufficient and quality clinical placements in medical education. It was felt that by developing a Framework of Competencies which relies on clinical placements, a level of clarity and precision around the training that occurs in a clinical environment could be devised. Research informing the development of the Framework Current literature was reviewed to assist with the development of the Framework and to determine the competence – based medical education environment. There were three significant reports which influenced the development of the Framework: General Medical Council: Tomorrow’s Doctors3 - an example of an outcomes - based framework implemented in medical education in the United Kingdom. United Kingdom medical schools are now being accredited against this framework. Tomorrow’s Doctors is an example of an outcomes - based framework which is implemented at the medical graduate level. The CanMEDS 2005 Physician Competency Framework4 - a world recognised competency framework for physician competencies. The CanMEDS framework provided insight into the development of, and implementation of, a competency framework at the vocational level of medical education. The Future of Medical Education in Canada (FMEC) report5 - an example of a national outcomes measurement and which includes references to competencies. The FMEC report looked at how the education programs for medical doctors can best respond to societal needs. The release of the FMEC report included ten recommendations for medical education in Canada. Of particular significance was recommendation number nine, the adoption of a competency – based and flexible approach. Of significant importance was the release of the International Competence – Based Medical Education Collaborators new definition of Competence, Competencies and Competency - Based Medical Education. The collaborators conducted a systematic review of the literature on Competency Based Medical Education to develop new definitions. The definitions are:
3 General Medical Council, Tomorrow’s Doctors, September 2009. 4 Frank, JR. (Ed). 2005 The CanMEDS 2005 physician competency framework. Better Standards. Better physicians. Better care. Ottawa: the Royal College of Physicians and Surgeons of Canada. 5 The Association of Faculties of Medicine of Canada, Future of Medical Education in Canada (FMEC), A Collective Vision for MD Education, 2010

5
Competency / Competencies - An observable ability of a health professional - Reflects a spectrum - Integrates multiple components such as knowledge, skills, values, and attitudes. - Multiple competencies can be combined - Measureable with respect to a defined outcome
Competency - Based Medical Education
- Is an outcomes - based approach to the design, implementation, assessment and evaluation of a medical education program using an organising framework of competencies.
Competent
- Possessing the required abilities in all domains at a specified stage of medical education or practice.
The Medical Deans’ Competencies Project adopted these definitions when referring to competence, competencies and competency. Of equal importance was the release of the AMC Consultation Paper on Competence – Based Medical Education in August 2010. The AMC internal working party which oversaw this work was chaired by Professor Nicholas Glasgow and also included Professor David Prideaux. Both were members of the Competencies Project Reference Group and Writing Group, enabling a useful sharing of information between the AMC Project and the Competencies Project. The proposed AMC framework makes distinctions between codified knowledge and tacit knowledge. Clinical placements are a combination of codified and tacit knowledge with early clinical experiences comprising mostly codified knowledge. The Reference Group and Medical Deans supported the framework proposed by AMC. This framework has helped to inform the competencies identified which rely on clinical placements. Projects informing the development of the Framework There were a number of key projects being conducted in Australia which had concurrent themes around addressing clinical competence, academic standards and quality and safety. These included the Australian Learning and Teaching Council’s Academic Standards Project for Health, Medicine and Veterinary Science, HWA’s Simulated Learning Environments for Medicine, HWA’s National Health Competency Framework and ACFJD. These related projects helped to inform the development of the Framework, facilitated stakeholder engagement and also provided the conduit for sharing related information. Competency - based education currently in place in medical education A brief review of competence – based education across medical education in Australia revealed that some universities had adopted an outcomes - based approach to curriculum delivery, although there were very few medical schools utilising a competency - based approach. The medical schools at the University of Queensland and the University of Notre Dame were the only two schools identified that have adopted a competency – based approach to sections of their medical curriculum. The most comprehensive demonstration of competence - based education was found at the University of Queensland where a competency - based initiative has been implemented for first year clinical skills sessions using a model of ‘rolling’ assessment. This initiative delivers a highly structured

6
clinical coaching program for first year clinical and procedural skills resulting in improved clinical skills for first year medical students. At the prevocational level, most state prevocational medical councils referenced the Australian Curriculum Framework for Junior Doctors (ACFJD) as the educational curriculum for teaching interns. At the vocational level, the majority of colleges have either adopted, or are in the process of transitioning to a CanMEDS style of framework for the delivery of their curriculum. Methodology Initial activities involved the establishment of a Reference Group whose role was to provide strategic advice and direction for the project. The Reference Group was led by Medical Deans with the Chair of the Reference Group Professor Allan Carmichael, previous President of Medical Deans, and the Deputy Chair, Professor Nicholas Glasgow, a member of the Medical Deans’ Executive and the representative for the Australian Medical Council. Other members of the Reference Group represented major stakeholder organisations across the medical education continuum. A full list of members of the Reference Group Membership is included in Appendix A. Early on, it was clear that it would be beneficial for the project to establish a smaller more specialised Writing Group to help with the delineation process and to help achieve the objectives of the project. The Writing Group included members from Medical Deans, Medical Educators, Confederation of Post Graduate Medical Education Councils (CPMEC), Australian Medical Association – Council of Doctors in Training (AMACDIT) and Australian Medical Students Association (AMSA). A full list of Writing Group Membership is included in Appendix A. In order to contain the scope of the project, the Reference Group decided that the project focus on those clinical placements that occur in the second half of a University Medical Program. This is when the students are full time in their clinical rotations. These clinical placements have also been identified as the pressure point in medical education with the increase in student numbers in the future and the challenges of providing a quality clinical placement. Key stages in the development of the Framework Attributes Spectrum One of the first challenges was identifying which of the AMC graduate attributes relied on clinical placements. This lead to the development of the Attributes Spectrum which identifies and ranks attributes according to their degree of reliance on being acquired in a clinical setting. The Reference Group ranked the forty AMC graduate attributes according to their degree of reliance on being acquired in a clinical setting. This important development for the project provided a system to address the major objective of the project. The Attributes Spectrum also identified a starting point for the delineation process. The delineation process involved translating those attributes which relied on clinical placements, into Student Learning Outcomes and then competencies. The delineation of attributes started with the attributes in the red zone of the Attributes Spectrum (attributes predominately acquired in a clinical setting), and worked up the spectrum towards the yellow zone (attributes which can be acquired in settings other than clinical settings).

7
Sample Attributes Spectrum
Predominately acquired
in settings other than
clinical settings.
Requires some
degree of clinical setting.
Predominately acquired
in clinical settings.
Student Learning Outcomes Now that there was an identifiable starting point for the delineation process, there was still the challenge of undertaking the delineation of attributes into competencies. To help address the paradigm shift from goals, objectives or statements to one of an outcome - based approach; the use of Student Learning Outcomes was incorporated as an intermediary step. Thus the delineation of attributes would focus on those attributes which rely on clinical placements, and delineate them into Student Learning Outcomes and then competencies.
Delineation process concept map
To assist with the delineation process, medical schools were contacted and requested to supply curriculum documents for clinical placements which occur in the second half of a medical program. The documents helped form the basis of the Student Learning Outcomes and competencies. The use of these documents also assisted in developing competencies which were appropriate for the medical graduate and would also ensure further learning. The Student Learning Outcomes (SLO’s) and competencies developed were purposely kept broad and high level so as to avoid a reductionist approach. The intention behind writing the SLO’s and competencies was to capture the essence of the attribute, and express this in an outcome - based/competency model. The goal was to produce a framework which had a functional use – a framework which contained a large number of competencies would be of little benefit.
AMC graduate attributes ordered along the spectrum, according to their degree of reliance on being developed in a clinical setting.

8
Critiquing against Australian Curriculum Framework for Junior Doctors (ACFJD) The competencies developed for each attribute were dynamically critiqued against the ACFJD. This critiquing against the ACFJD helped to develop competencies which were not beyond the level of the medical graduate. By analysing the competencies against the ACFJD, vertical integration was also addressed. Using the ACFJD as a benchmark has established the basis for a future mapping exercise of the competencies developed for the medical graduate to the ACFJD capabilities. Lists of common diagnostic and procedural skills The delineation process for attributes pertaining to diagnostic and procedural skills (attributes 18 and 15) lead to the development of lists of common diagnostic skills and procedural skills. The use of lists in the Framework aims to identify what diagnostic and procedural skills a medical graduate should have attained regardless of the medical program they undertook. These lists were developed via a modified Delphi technique from data obtained from three medical schools. Refinement of these lists will help in the identification of competencies which are developed in a clinical setting. These lists will be useful to health service providers as it will help to identify the competencies medical graduates have acquired in clinical settings. Common clinical rotations The draft Framework utilised the Attributes Spectrum as the foundation of the framework. The introduction of the eight common clinical rotations as identified by the National Clinical Training Review Report was incorporated into the Framework. The eight clinical rotations provided the context for the development of the Student Learning Outcomes and competencies in a clinical setting. The eight common clinical rotations as identified by the National Clinical Training Review Report are: Emergency Medicine/Critical Care, General Practice and Community, General Medicine/Medicine, Obstetrics and Gynaecology, Psychiatry and Mental Health, Paediatrics, Surgery and Others.
Draft framework including eight common clinical rotations concept map
The mapping of competencies to the eight common clinical placements has helped set the context for the competencies which have been developed. Currently, all of the competencies developed are mapping to all of the eight clinical rotations. This is to be expected as the delineation process focused on those attributes which are developed in a clinical setting.

9
Mind mapping software A noteworthy outcome regarding the development of the Framework was the incorporation of mind mapping software to present the Framework. The use of an electronic format for the Framework provided a more interactive and dynamic way to present the framework. The mind mapping allows for greater flexibility as information can be added or subtracted, according to the needs of the user. The electronic format also permits the user to map backwards from the competencies to the AMC attributes. Whilst the mind mapping concept is good, it is still in its developmental stage. It is hoped that future work will involve the refining of the electronic format to enable a more sophisticated version. Writing Group The Writing Group advanced the project work significantly and its meetings were a major component of the methodology of the project enabling the project’s objectives to be achieved. The face to face nature of the meetings allowed for consultation with key figures in medical education to ensure stakeholder engagement. The meetings also assisted in the utilisation of medical educator’s expertise in identifying competencies appropriate for the medical graduate. Stakeholder Consultation There was extensive consultation with stakeholders throughout the entire project term. Competence – based medical education is currently a topic of significant interest in not only medical schools but also heath departments, prevocational medical education councils and specialty colleges. Stakeholders from related projects, medical schools, health departments and prevocational medical education colleges showed interest in the Competencies Project due to the unique focus of the project on clinical placements. This level of stakeholder consultation is demonstrated by the large number of people/organisations consulted with over the project period. A list of people/organisations consulted is attached as Appendix B. In depth discussions were held with a number of key stakeholders to assist with the documentation of competencies. Medical schools, Clinical Rotation Leaders, Heads of Clinical Departments in medical schools, post graduate medical education councils and Health Workforce Australia were consulted to discuss the level necessary for a medical graduate to commence work as an intern. These discussions assisted with the documentation of Student Learning Outcomes and competencies and also assisted with the contextualisation of the project work. The project was reported on at key meetings where Medical Deans were represented. Of particular importance were the presentations at the Medical Deans’ Annual Conference and to the Australian Medical Council’s Medical Schools Accreditation Committee (MedSAC). The presentation to the Deans at the Medical Deans’ Annual Conference gave the Deans the opportunity to comment on the direction and progress of the project. The project received solid endorsement from the Deans and recognition that this was a useful project for medical education. This was very pleasing as it reinforced the direction of the project and generated significant interest from medical schools in the upcoming Consensus Conference. Following on from the Medical Deans’ Annual Conference, the Chair and the Project Manager presented the project to the MedSAC board meeting in October 2010. This was an opportunity to brief the AMC on the work conducted thus far. It was also an opportunity to advise the AMC that there had been a number of attributes identified by the Writing Group deemed suitable for revision. It is hoped that there will be future collaborations with the AMC regarding the review of their attributes.

10
The convening of the Consensus Conference was an opportunity to bring together stakeholders for a face to face meeting to discuss and refine the work conducted on the Framework. The participation was opened up to a wider stakeholder audience, namely individuals and organisations that had been consulted during the project period. The wider participation facilitated greater stakeholder buy in and an excellent opportunity to elicit targeted feedback. The participation consisted of individuals from the Reference Group, Writing Group, Medical Schools, AMSA, Health Departments, CPMEC and related projects. A full participation list is included as Appendix C. The Consensus Conference was a resounding success. It provided a large stakeholder audience with a significant insight into the work being undertaken on the development of competencies which rely on clinical placements. There was substantial targeted feedback elicited, and solid endorsement of the Framework was achieved. The major outcomes from the Consensus Conference were: 1. A wider stakeholder audience being made aware of the Competencies Project and having a
greater understanding of the work conducted during the project period. 2. Solid endorsement of the draft framework. There was general acknowledgement that the
Competencies Project was a valuable project for outlining the competencies which a graduate will acquire in a clinical placement. The framework may be used to assist schools in achieving the AMC graduate attributes in clinical settings.
3. Strong endorsement of the need to review the AMC medical graduate attributes. 4. Support for a proactive approach to coordinating the various projects in the health and education
sectors which are addressing clinical competence, academic standards, quality and safety, especially HWA’s simulated learning environments project.
5. Strong support for further development of the list of graduate skills and competencies related to investigations, clinical examinations and procedures. Further work to complete these lists was seen as high priority.
6. Feedback on the delineated attributes and lists of common diagnostic and procedural skills be incorporated into the Framework and reviewed by the Writing Group and the Reference Group.
7. Recommendations for a second stage phase of the project to include mapping the competencies developed with the ACFJD capabilities specifying the level of achievement of competencies at each level.
Notes from the Consensus Conference are attached as Appendix D. The Consensus Conference yielded a significant amount of feedback on the Student Learning Outcomes and then competencies. There was also a large amount of feedback provided regarding the lists of common diagnostic and procedural skills for the medical graduate. Following the Consensus Conference, the project focused on the feedback provided on the Student Learning Outcomes and then competencies in order to refine the Framework. The feedback was collated and reviewed by the Writing Group at the last meeting in January 2011. The Writing Group reviewed all of the thirty delineated attributes and refined the Framework accordingly.

11
Refining the Framework The final Writing Group Meeting produced some significant changes to the Attributes Spectrum and the Framework. In order to address the challenge of interrelated attributes and competencies there were four significant changes. 1. Better alignment of attributes which have concurrent themes around knowledge and
understanding and the skills associated with these attributes. 2. Attributes 4 and 5 specifying knowledge and understanding for management and diagnostic
procedures, were moved down the Attributes Spectrum so that they are next to attributes 19 and 17 specifying the associated skills and abilities for management and diagnostic procedures.
3. For attributes which have concurrent themes, the competencies can refer to those attributes. 4. The inclusion of the AMC graduate attribute ‘stem’ in the Attributes Spectrum. The stems are:-
Knowledge and Understanding Attributes 1 -12 ‘Graduates completing basic medical education should have knowledge and understanding of’: Skills Attributes 13 -25 ‘Graduates completing basic medical education should have developed the following skills and abilities’: Attitudes as they affect Professional Behaviour Attributes 26 – 40 ‘At the end of basic medical education, students should demonstrate the following professional attitudes that are fundamental to medical practice’: The stems are included as a footnote at the bottom of the Attributes Spectrum.
The Reference Group endorsed the changes to the Attributes Spectrum and the Framework at its final meeting in January, 2011. The final version of the Attributes Spectrum is attached as Appendix E. The completed Framework of Medical Graduate Outcomes is attached as Appendix F. As mentioned previously, there is also a mind mapped version of the Framework which accompanies this report. Endorsement of the Framework There has been a solid endorsement of the Framework and this is represented by the extensive consultation which occurred during the project period. The endorsement of the Framework is also demonstrated by the attendance of such a diverse stakeholder group at the Consensus Conference. The Consensus Conference Participation and Notes are further evidence to the level of support the Competencies Project has received. The Deans endorsed the Competencies Framework at the Medical Deans’ 2010 Annual Conference and have continued to provide support at the meetings of the Medical Deans Executive. A letter of support from Medical Deans is attached as Appendix G.

12
Future Use of the Framework The Competencies Project provides some clarity and transparency around the learning that occurs in a clinical training environment. It is Medical Deans’ intention that once the lists of common diagnostic and procedural skills for the medical graduate have been further developed the Framework will be made available to medical schools for their use. It is anticipated that the Framework will be particularly helpful for medical schools that are establishing new clinical placements, such as those growth places currently being established under Health Workforce Australia’s Clinical Training Funding. The Framework has also been identified as being useful for clinical supervisors who are teaching medical students in clinical placements. There may be opportunity to liaise further with Heads of Disciplines and Heads of Clinical Schools to establish if the Framework would be beneficial for clinical teachers. Once the Framework is ready for release to medical schools, it is hoped that there will be an opportunity to discuss the Framework further with medical schools and establish how it can be used to help develop and refine clinical placements. Next steps The next logical body of work for the Competencies Project is further refinement of lists of common diagnostic and procedural skills for the medical graduate. There was overwhelming support for this obtained at the Consensus Conference. As this work falls out of the scope of the current project, incorporating the feedback obtained on these lists and refining the lists of common diagnostic and procedural skills will form the basis of a second stage of work. It is anticipated that this will involve further consultation with medical schools and Directors of Clinical Training to ascertain the content of the lists of common diagnostic and procedural skills. The refinement of these lists will also aim to identify to what level of achievement the medical graduate has obtained these skills. A draft version of lists of common diagnostic and procedural skills is included as Appendix F. Mapping of the medical graduate competencies to the ACFJD was also seen as a beneficial exercise to address vertical integration. Once the common diagnostic and procedural skills have been established and the level of achievement specified, future work will involve a mapping exercise to the ACFJD skills and procedures section. The aim of this exercise will be to articulate what level of skill is obtained for the medical graduate and what level of achievement there is for the same skill after PGY2. Future work will also involve the refining of the delineation process for Attribute 21 – which references the National Patient Safety Education Framework. This is a 214 page document with a four point matrix system which identifies the levels of a health worker from cleaners to the CEO of a hospital. This attribute needs to be reviewed separately so that there is a not large amount of competencies developed relating to the National Patient Safety Education Framework. This would potentially slant the Competencies Framework in a different direction. Future recommendations also involve the coordination of the various projects in health and education sectors to ensure that the projects align, and true vertical integration of the curriculum can occur, thus improving clinical education. The sharing of information in the future with HWA’s Simulated Learning Environments project for Medicine will help to align the Competencies Project and HWA’s project findings. The alignment of future work for the Competencies Project with existing projects in medical education will ensure an

13
integrated approach to projects which aim to improve the quality of clinical placements in medical schools. There was also strong support for the revision of the AMC graduate attributes from the Reference Group and participants of the Consensus Conference. Medical Deans will liaise with the AMC at a future date when the AMC undertakes this process. At the time of writing this Final Report, Health Workforce Australia have provided in principle support for a second stage of work to proceed on the further development of the lists of common diagnostic and procedural skills for the medical graduate. The development of these lists of diagnostic and procedural skills was seen as a high priority from key stakeholders. The Competencies Project hopes to retain the expertise of the Reference Group and Writing Group should this funding become available. Conclusion The Developing a Framework of Competencies for Medical Graduate Outcomes Project has achieved significant results in the last twelve months. The framework of competencies which rely on clinical placements has provided some precision and transparency around the learning which occurs in a clinical placement. The project has brought together key figures in medical education to discuss the quality and content of clinical training. It is hoped that the future intended work of the Competencies Project will encourage innovation and diversity in teaching and learning to help assist with capacity building to create quality clinical placements for the future. This project would not have been possible without the support from the Strategic Medical Education Section, Australian Government Department of Health and Ageing. Medical Deans is grateful for their support and looks forward to working with the Department on future related work.

14
Summary of Key Outcomes against Project Objectives A summary of the major outcomes of each project objective follows: 1. Identify the competencies associated with each of the attributes in knowledge, skills and
attitudes/behaviours specified by the AMC for competent medical graduates and which depend on clinical placements.
Key achievements:
• The development of the Attributes Spectrum which identified which attributes relied on clinical placements.
• The delineation of thirty of the AMC’s graduate attributes which rely on clinical placements, as identified on the Attributes Spectrum, into Student Learning Outcomes and then competencies.
• The incorporation of the Attributes Spectrum, Student Learning Outcomes and competencies into a mind mapping framework to develop a Framework of Competencies for Medical Graduate Outcomes.
2. Use the AMC Accreditation Standards and Processes for medical graduates (including
International Medical Graduates), the Medical Deans’ National Clinical Training Review report, The Australian Curriculum Framework for Junior Doctors (ACFJD) and any other relevant reports/projects as the basis of the development of a document that maps competencies to AMC prescribed attributes and which enables graduates to practice at the beginning of the PGY1 Year.
Key achievements:
• The AMC graduate attributes are the anchor point for the project to identify attributes which rely on clinical placements, and to delineate competencies from these attributes.
• The Medical Deans’ National Clinical Training Review report was utilised to identify the eight common clinical rotations which forms the basis of clinical placements for the project.
• The competencies developed were dynamically critiqued against the ACFJD. • Relevant reports and projects helped in the development of the framework, these have been
covered extensively in Progress Report 1, 2, Draft Final Report and in Section One of this report.
3. Ensure engagement of stakeholders in the identification and specification of competencies.
Key achievements: • Extensive consultation with the Reference Group and Writing Group which includes
representatives from key organisations in medical education. • Liaising with related projects with concurrent themes around competency and academic
standards. • Involvement of the medical schools in the determination of competencies and the level required
for a graduating medical student. • Convening of the Consensus Conference which was a major forum of key stakeholders to discuss
the proposed framework and to elicit targeted feedback.
4. Ensure that the competencies documented are appropriate for a graduating medical student to commence work as an intern in the standard clinical rotations of the intern year (PGY1).
Key achievements:
• Utilisation of medical educators with expertise in teaching medical graduates.
15
• Competencies developed were dynamically critiqued against ACFJD to ensure they were appropriate for a graduate to commence work as an intern.
• Consultation with medical schools to ensure competencies developed were appropriate for the medical graduate.
• Convening of the Consensus Conference to elicit feedback as to the level necessary for a medical graduate.
5. Ensure that the competencies enable a graduating medical student to continue to undertake
further learning and clinical training.
Key achievements: • The introduction of lists of common diagnostic and procedural skills which can be added to
through the prevocational and vocational years. • Cross referencing competencies developed to ACFJD to address vertical integration. By achieving the principle objectives of the project, the Medical Deans’ Competencies Project has achieved the aim of the project which was to identify and document competencies for the medical graduate outcomes required by the AMC and which depends on clinical placements.

16
List of Appendices
A. Reference Group and Writing Group Membership
B. Stakeholder Consultation List
C. Consensus Conference Participation
D. Consensus Conference Notes
E. Final Attributes Spectrum
F. Framework of Competencies
G. Deans’ Letter of Support

Reference Group and Writing Group Membership Appendix A
Medical Deans’ Competencies Project Final Report February 2011
Reference Group Member
Representing
Professor Allan Carmichael (Chair) Medical Deans Professor Nicholas Glasgow (Deputy Chair) Medical Deans and Australian Medical Council Dr Andrew Singer Department of Health and Ageing Ms Meredith Williams Department of Health and Ageing Dr Jagdishwar Singh Confederation of Post Graduate Medical Education
Councils Dr Gregory Keogh Confederation of Post Graduate Medical Education
Councils/Clinical Education and Training Professor David Prideaux Medical Educators Professor Fiona Lake Medical Educators/Clinical Teachers Dr Michael O’Sullivan Australian Medical Association Council Doctors in
Training Mr Sam Whitehouse Australian Medical Students’ Association Dr Morton Rawlin Committee of Presidents of Medical Colleges Dr Geoff Copland Clinical Supervisors Associate Professor Andrew Clinical Supervisors Ms Teresa Valentine Health Workforce Australia Ms Monique Hourn Medical Deans
Member Representing Professor Allan Carmichael Medical Deans Professor Nicholas Glasgow Medical Deans and Australian Medical Council Professor David Prideaux Medical Educators Dr Jagdishwar Singh Confederation of Postgraduate Medical Education
Councils Professor Fiona Lake Medical Educators/Clinical Teachers Dr Michael O’Sullivan Australian Medical Association Council Doctors in
Training Mr Sam Whitehouse Ms Monique Hourn
Australian Medical Students’ Association Medical Deans

Sta
keho
lder
Con
sulta
tions
A
ppen
dix
B
Sta
keho
lder
Org
anis
atio
n
Indi
vidu
al
Occ
asio
n/M
eetin
g
Dea
ns
All
Dea
ns
MD
AN
Z M
idye
ar M
eetin
g 20
10
MD
AN
Z A
nnua
l Gen
eral
Mee
ting
MD
AN
Z A
nnua
l Con
fere
nce
MD
AN
Z M
idye
ar M
eetin
g 20
11
Indi
vidu
al D
eans
P
rofe
ssor
Alla
n C
arm
icha
el
Pro
fess
or N
icho
las
Gla
sgow
P
rofe
ssor
Ric
hard
Hay
s P
rofe
ssor
Bre
ndan
Cro
tty
Pro
fess
or A
lison
Jon
es
Pro
fess
or J
ustin
Bei
lby
Mul
tiple
tim
es
Mul
tiple
tim
es
Med
ical
Sch
ools
D
r Je
nnife
r S
chaf
er (
UQ
) D
r K
aren
D’S
ouza
(D
eaki
n)
A/P
rof R
osa
Can
ales
e (N
otre
Dam
e S
ydne
y)
Ms
Jenn
ifer
Lind
ley
(Mon
ash)
P
rofe
ssor
Phi
llip
Jone
s (U
NS
W)
Pro
fess
or D
avid
Prid
eaux
(F
linde
rs)
Dr
Fio
na H
awth
orne
(U
Q)
Pro
fess
or F
iona
Lak
e (U
WA
) P
rofe
ssor
Chr
is D
enni
s (S
ydne
y)
Dr
Julie
Ash
(F
linde
rs)
A/P
rof M
ellic
k C
heha
de (
Ade
laid
e)
A/P
rof W
endy
Hu
(UW
S)
A/P
rof A
ndre
w H
ill (
Auc
klan
d)
Ms
Joy
Rud
land
(O
tago
) P
rofe
ssor
Dav
id H
arris
(S
ydne
y)
Pro
fess
or Ia
n S
ymon
ds (
New
cast
le)
A/P
rof S
elze
r (M
onas
h)
Pro
fess
or B
en C
ann
y (M
onas
h)
A/P
rof C
ampb
ell (
Mon
ash)
A
/Pro
f Gar
y R
oger
(G
riffit
h)
Pro
fess
or G
eoff
McC
oll (
Mel
bour
ne)
A/P
rof C
arol
e S
teke
tee
(Not
re D
ame
Fre
man
tle)
Pro
fess
or M
icha
el F
rom
mer
(S
ydne
y)
Pro
fess
or R
icha
rd M
urra
y (J
CU
) P
rofe
ssor
Dav
id K
andi
ah (
UW
A)
Pro
fess
or B
rian
Jolly
(M
onas
h)
Pro
fess
or J
ames
Vic
kers
(U
TA
S)
Pro
fess
or C
raig
Zim
itat (
UT
AS
)
Mul
tiple
tim
es
Mul
tiple
tim
es
Mul
tiple
tim
es
Mul
tiple
tim
e M
ultip
le ti
mes
M
ultip
le ti
mes
M
ultip
le ti
mes
M
ultip
le ti
mes
Dep
artm
ent o
f Hea
lth a
nd A
gein
g M
r T
ony
Hyl
and
Ms
Mer
edith
Will
iam
s P
rofe
ssor
Jud
y S
earle
M
s Li
na C
achi
a D
r A
ndre
w S
inge
r
Mul
tiple
tim
es
Mul
tiple
tim
es
Mul
tiple
tim
es
Mul
tiple
tim
es

Sta
keho
lder
Org
anis
atio
n
Indi
vidu
al
Mee
ting
C
onfe
dera
tion
for
Pos
t Gra
duat
e M
edic
al E
duca
tion
Cou
ncils
(C
PM
EC
) D
r Ja
gdis
hwar
Sin
gh
Dr
Gre
g K
eogh
M
s D
ebor
ah P
altr
idge
Mul
tiple
tim
es
Mul
tiple
tim
es
Aus
tral
ian
Med
ical
Cou
ncil
Pro
fess
or N
icho
las
Gla
sgow
P
rofe
ssor
Hea
ther
Ale
xand
er
Ms
The
anne
Wal
ters
M
ed S
AC
Boa
rd
Mul
tiple
tim
es
Oct
ober
201
0 B
oard
Mee
ting
Aus
tral
ian
Med
ical
Ass
ocia
tion
– C
ounc
il of
Doc
tors
in
Tra
inin
g D
r M
icha
el B
onni
ng
Dr
Mic
hael
O’S
ulliv
an
Mul
tiple
tim
es
Aus
tral
ian
Med
ical
Stu
dent
s’ A
ssoc
iatio
n (A
MS
A)
Mr
Ros
s R
ober
ts –
Tho
mso
n M
r S
am W
hite
hous
e M
ultip
le ti
mes
H
ealth
Wor
kfor
ce A
ustr
alia
(H
WA
) M
s Lu
isa
Abi
uso
Ms
Ter
esa
Val
entin
e P
rofe
ssor
Liz
Far
mer
Mul
tiple
tim
e M
ultip
le ti
mes
A
ustr
alia
n Le
arni
ng a
nd T
each
ing
Cou
ncil
(ALT
C)
Pro
fess
or C
hris
tine
Ew
an
Pro
fess
or A
man
da H
ende
rson
A
/Pro
f Mar
ee O
’Kee
fe
Hea
lth W
orkf
orce
Aus
tral
ia –
rel
ated
pro
ject
s S
imul
ated
Lea
rnin
g E
nviro
nmen
ts P
roje
ct
Nat
iona
l Hea
lth C
ompe
tenc
y F
ram
ewor
k
Pro
fess
or B
rian
Jolly
M
s K
atie
Wal
ker
Ms
Bev
erle
y S
utto
n A
/Pro
f Sha
ron
Bro
wni
e P
rofe
ssor
Hel
en C
hene
ry
Mul
tiple
tim
es
Mul
tiple
tim
es
Mul
tiple
tim
es
Com
mitt
ee o
f Pre
side
nts
Med
ical
Col
lege
s (C
PM
C)
M
r Le
s A
polo
ny
Dr
Mor
ton
Raw
lin
Mul
tiple
tim
es
Roy
al A
ustr
alia
n C
olle
ge o
f Psy
chia
tris
ts
Dr
And
rew
Gos
bell
N
SW
Hea
lth D
epar
tmen
t D
r Li
nda
Mac
pher
son
Ms
Rob
yn B
urle
y
NS
W C
ET
I D
r G
reg
Keo
gh
Q
ueen
slan
d H
ealth
C
linE
dQ
A/P
rof V
icto
ria B
razi
l
Clin
ical
Sup
ervi
sors
D
r G
eoffr
ey C
opla
nd
A/P
rof A
ndre
w H
ill
Dea
ns
Med
ical
sch
ools
C
PM
EC
C
PM
C
DoH
A
HW
A
AM
AC
DIT
A
MS
A
Clin
ical
sup
ervi
sors
M
edic
al E
duca
tors
Ref
eren
ce G
roup
Mem
bers
hip
Writ
ing
Gro
up M
embe
rshi
p R
efer
ence
Gro
up M
eetin
gs 1
– 6
W
ritin
g G
roup
Mee
tings
1 -
3

Consensus Conference Participation Appendix C
Reference Group Organisation
Professor Allan Carmichael (Chair) Medical Deans
Professor David Prideaux Medical Educator/Flinders University
Dr Andrew Singer (Medical Advisor) DoHA
Associate Professor Andrew Hill Clinical Supervisors
Mr Sam Whitehouse AMSA
Dr Jagdishwar Singh CPMEC
Ms Teresa Valentine HWA
Dr Gregory Keogh CPMEC/Director of CETI
Dr Morton Rawlin CPMC
Dr Geoffrey Copland Clinical Supervisors
Ms Monique Hourn Medical Deans
DEANS or Nominees UNIVERSITY
Professor Warwick Bagg Auckland
A/Professor Gary Rogers Griffith
Professor Richard Murray James Cook
Professor Ben Canny Monash
Professor Geoff McColl Melbourne
A/Professor Carol Steketee Notre Dame Fremantle
Professor Michael Frommer Sydney
Professor David Kandiah UWA
A/Professor Craig Zimitat UTAS
External Stakeholders Representing
A/Professor Maree O'Keefe ALTC
Professor Amanda Henderson ALTC
Ms Deborah Paltridge CPMEC
A/Professor Victoria Brazil ClinEdQ
Dr Jennifer Schafer UQ
Professor Brian Jolly Monash University/HWA SLE Audit Project
Ms Beverley Sutton Monash University/HWA SLE Audit Project
Dr Linda MacPherson NSW DOH
Professor Liz Farmer Health Workforce Australia
Mr Philip Pogson Facilitator
Ms Giti Datt Medical Deans (scribe)

Consensus Conference Participation Appendix C
Referenc e Group Apologies
Professor Nicholas Glasgow (Deputy Chair) Medical Deans/ANU/AMC
Professor Fiona Lake Medical Educators/UWA
Dr Michael O’Sullivan AMACDIT
Professor Allison Jones UWS
Ms Meredith Williams DoHA

Appendix D
Competencies Project Consensus Conference
Notes Thursday, 11 November 2010 Melbourne Airport Hilton Victoria South Ballroom 10am – 4pm Attendees : Professor Allan Carmichael (Chair), Professor David Prideaux, Dr Andrew Singer, A/Prof Andrew Hill, Mr Sam Whitehouse, Dr Jagdishwar Singh, Ms Teresa Valentine, Dr Greg Keogh, Dr Morton Rawlin, Dr Geoffrey Copland, Ms Monique Hourn, Professor Warwick Bagg, A/Prof Gary Rogers, Professor Richard Murray, Professor Ben Canny, Professor Geoff Mccoll, A/Prof Carole Steketee, Professor Michael Frommer, Professor David Kandiah, A/Prof Craig Zimitat, A/Prof Maree O’Keefe, Professor Amanda Henderson, Ms Deborah Paltridge, A/Prof Victoria Brazil, Dr Jennifer Schafer, Professor Brian Jolly, Ms Beverley Sutton, Dr Linda MacPherson, Professor Liz Farmer, Mr Philip Pogson, Ms Giti Datt. Apologies: Professor Nicholas Glasgow, Professor Fiona Lake, Dr Michael O’Sullivan, Ms Meredith Williams, Professor Alison Jones. Session 1: Setting the scene Participants were provided with a background to the project, an overview and comments from key stakeholders. Key discussion points included: • Student Learning Outcomes as part of the framework help to delineate attributes which have
multiple components. SLO’s allows for the illustration of tacit knowledge which cannot always be codified into competencies.
• The framework presented is not a prescriptive approach but a descriptive one which will allow medical schools to do things in a different way.
• Acknowledgments that the AMC graduate attributes require revision; they do not capture observable behaviour. This project will be able to provide feedback to the AMC about which attributes need revising.
• The need to acknowledge simulation in a clinical setting and to link in the Competencies Project project with HWA’s SLE project.
DoHA perspective • The competencies project will provide better delineation around what occurs in a clinical
placement. • Vertical integration is the ultimate goal. There is a level of consistency that DoHA would like to
see whilst taking into consideration that medical schools would like to retain control over their own approaches.
• A hopeful outcome would be that medical schools will be able to do things as they see best for their program but ultimately we will all be heading towards a common outcome.
HWA perspective • HWA are interested in delineating what occurs in a clinical placement but also looking at future
meanings of the health workforce and competencies. • HWA are conducting a suite of competency projects looking at the national and international
competency landscape.
• There are parallels between this project and clinical supervision and the competence of supervisors.
• HWA is very supportive of any efforts to make competencies more explicit any profession.
CPMEC perspective • This project runs in parallel with the prevocational training project, ACFJD. • This project is useful for supervisors because they will now understand what they have to do on
the ground as clinical supervisors. • The delineation of the attributes can help form the basis of situational learning and assessment. • The competencies presented today are sound building blocks for future work, collaboration is
important and projects need to keep on mapping to make sure things align. • Simulation will be an important component of future work. Medical Educators perspective • Competency-Based frameworks are a way of organising curriculum and it focuses on outcomes
which is good because things can be transparent and students can be clear on what they need to achieve. It is easy to relate to practice.
• Negatives to Competency-Based frameworks – they are difficult to write. There is a very real risk of them being reductionist. There are some things that you cannot measure, like observable behaviour.
• A medical graduate has to have lots of contact with lots of patients to move from novice to expert. • This project is important in increasing transparency and clarity particularly as we are expanding
our clinical placements. UQ perspective • UQ developed a competency based assessment for their year one MBBS program due to the
increase in student numbers and wanting to maintain standards. • Broke year one down into sections and ended up with a list of competencies. This project was
piloted one year and then implemented the next year. • Outcomes of the project were that everyone knew what they had to do, teachers, students and
examiners. • All students are assessed and if students do not reach the standard they are given extra teaching
until they do. No student falls through the cracks. • Now looking at other areas of the course where this can be implemented and linked into other
areas of the curriculum.
Session 2: Review of work developed Participants were provided with a brief overview of the methodology of the delineation process, introduction of appendices A & B and demonstration of the mind mapping framework. Key discussion points included: • Need to revise previous competencies developed to ensure consistency in the framework. • Mind mapping tool would be a useful tool to generate a report which identifies gaps. • Where competencies are interrelated and are expressed in other attributes, the approach has had
to be an ad hoc one. If this project is to deal with this systematically another matrix would be needed.

Breakout session 1: Participants formed break out groups and provided feedback on a set of attributes from varied positions along the attributes spectrum. Key discussion points included: • The need to change some of the verbs at the beginning of the competencies. • The introduction of a glossary of verbs so there is a consensus for what verbs are in the
competency and how they were used. • In general, participants were happy with the principles of the SLO’s and the competencies. • Some of the SLO’s and competencies developed from attributes in the yellow zone of the
attributes spectrum are beyond the level of a graduate and need revision. • The stem of SLO’s ‘the student has the ability to’ has created some difficulty. • Recognise that content may be modified by context. • Need a broader clinical input into the framework to make sure that things are lined up
appropriately. • Need to develop a ‘laundry list’ of common conditions and common information technology
resources to show what is relevant. Summation of breakout session one: • Participants endorsed the principles behind the SLO’s and competencies developed. • There is the need for further revision of the work presented. • Possible development of a glossary of verbs, laundry lists of common conditions and information
technology resources. • Acknowledgement that there will be difficulties in trying to capture metacognitive and tacit
knowledge in words/competencies. • General consensus that the AMC graduate attributes need to be revised. • General support for a proactive approach to coordinating the various projects in the health and
education sectors which are addressing clinical competence, academic standards, quality and safety.
Breakout session 2: Review of appendices A & B Participants resumed their break out groups and reviewed appendices A & B. Key discussion points included: • Need to identify at what level graduates need to be familiar with diagnostic skills and procedural
skills. • Need to be more specific about procedural skills; i.e.’ need to know about versus perform’. • Need to decipher with diagnostic skills whether the graduate can interpret the report or point out
abnormal findings to the patient. • Need to define ‘What is a procedure and what is an examination’? • Possible introduction of a matrix for diagnostic skills and procedural skills. i.e. understand,
observe, under supervision, performs independently. • Need to add procedural skills as they relate to men’s health. • Need to get program directors together to discuss the detail in appendix A & B. • Important to map to ACFJD. • Need to differentiate between interpretation of reports and interpretation of films. • Cross check lists to ensure that there is not a doubling up of procedures and diagnostics.

Summation of breakout session two: • Need to recognise the framework from a practitioner centric point of view which includes patients
and risks to patients. Risk needs to be managed versus what students need to achieve. Important that health services are involved with this work.
• Possible incorporation of a statement that students should not do these things until we are absolutely certain that they can do them in a simulated environment.
• Important and helpful to look at these lists. We don’t have a common list of diagnostic or procedural skills across our medical schools. Further refine of these lists will help to establish what graduates should be able to do.
• The formation of these lists will help supervisors know what they have to teach to medical students.
Session 3 Related Projects ACFJD • ACFJD has been picked up and modified by New Zealand. • Project has not been funded since June. • Looking to implement assessment but need to learn from the UK junior doctor problems.
HWA: SLE Project • SLE project has revealed that medical schools are very interested in SLE. • AMC does not have a view at the moment as to whether they recommend simulation as a method
of teaching. • There are some topics which are being taught almost entirely in simulation e.g. basic life support. • The project has revealed that one size does not fit all when it comes to simulation.
ALTC Academic Standards Project • Academic Standards Project looks at the attributes of a graduate on the day they graduate as
opposed to certification for competency to practice. • The focus of the project is to look at the outcomes of graduates at the professional entry level
standard. What does every graduate need to have? • The project was able to obtain competency standards or accreditation standards for all
disciplines. Thematic analysis was conducted and competency standards were mapped to all six threshold learning outcomes.
• Information is being disseminated to relevant discipline bodies and hopefully there will be something available publicly through the ALTC very soon.
AMC Competence-Based Medical Education Paper • The paper released in August is the penultimate draft. • There will be a conference in December to look at the how tacit and codified knowledge sits within
a competency based framework.
Recommendations • General agreement that the framework presented is a useful one, and that it is useful for medical
schools and perhaps medical education in general particularly in the area of assisting medical schools to have more specification around the competencies a graduate could be expected to acquire in a clinical placement. The framework could be used as a tool to assist schools as they look at new clinical placements and clinical settings.
• General support for the AMC to review their graduate attributes.

• Support for the means of coordinating other projects in the sector which focus on clinical competence.
• Agreement that we ought to develop a common list of very basic skills/competencies around examinations and procedures. General agreement that there is a place for simulation in the acquisition of these skills and competencies.
• May be useful to develop a simulation spectrum for which skills can be acquired in a simulation setting.
• Feedback provided regarding the rewording of SLO’s and competencies will be incorporated by the Writing Group and the Reference Group.
• There is some discontinuity between the attributes. The ordering of attributes according to skills, knowledge and attitudes or importance of clinical placements results in a loss of cohesion of the actual outcome which we are looking for. The project may have to look at some matrix which brings those together.
• Recommendation that schools use the work from this project to investigate the quality of their clinical placements so that schools don’t make the assumptions that the standards are there when it could be an inadequate environment. There may need to be further consultation with heads of clinical schools for this to occur.
Summation and Action Plan • Integrate and implement the recommendations mentioned above and weave into the draft final
report. • Incorporate vertical integration into this project by talking with other organisations such as
CPMEC and CPMC, other groups represented such as MTRP and higher education groups such as ALTC. Meeting concluded at 3.30pm

ATTRIBUTES SPECTRUM Appendix E
For Attributes 1- 12 “Graduates completing basic medical education should have knowledge and understanding of” For Attributes 13 – 25 “Graduates completing basic medical education should have developed the following skills and abilities” For Attributes 26 – 40 “At the end of basic medical education students should demonstrate the following professional attitudes that are fundamental to medical practice”
© Medical Deans Australia and New Zealand, Competencies Project
(1) Scientific method relevant to biological, behavioural and social sciences at a level adequate to provide a rational basis for present medical practice, and to acquire and incorporate the advances in knowledge that will occur over their working life. (2) The normal structure, function and development of the human body and mind at all stages of life, the factors that may disturb these, and the interactions between body and mind. (27). Recognition that the doctor should have the necessary professional support, including a primary care physician, to ensure his or her own well-being. (36). An appreciation of the systems approach to health care safety, and the need to adopt and practise health care that maximises patient safety including cultural safety. (30) A commitment to ease pain and suffering. (7) The principles of health education, disease prevention and screening. (38). A desire to achieve the optimal patient care for the least cost, with an awareness of the need for cost-effectiveness to allow maximum benefit from the available resources. (31). A realisation that it is not always in the interests of patients or their families to do everything that is technically possible to make a precise diagnosis or to attempt to modify the course of an illness. (10) Systems of provision of health care in a culturally diverse society including their advantages and limitations, the principles of efficient and equitable allocation and use of finite resources, and recognition of local and national needs in health care and service delivery. (3) The aetiology, pathology, symptoms and signs, natural history, and prognosis of common mental and physical ailments in children, adolescents, adults and the aged. (35) An appreciation of the responsibility to contribute towards the generation of knowledge and the professional education of junior colleagues. (34) An appreciation of the responsibility to maintain standards of medical practice at the highest possible level throughout a professional career. (24) The ability to interpret medical evidence in a critical and scientific manner and an understanding of the epidemiology of disease in differing populations and geographic locations. (29) Respect for community values, including an appreciation of the diversity of human background and cultural values. (26) Recognition that the doctor’s primary professional responsibilities are the health interests of the patient and the community. (33) A realisation that doctors encounter clinical problems that exceed their knowledge and skills, and that, in these situations, they need to consult and/or refer the patient for help, in clinical, cultural social and language related matters as appropriate. (12) The principles of ethics related to health care and the legal responsibilities of the medical profession. (28) Respect for every human being, including respect of sexual boundaries. (25) The ability to use information technology appropriately as an essential resource for modern medical practice. (9) Factors affecting human relationships, the psychological, cultural and spiritual well-being of patients and their families, and the interactions between humans and their social and physical environment. (40) A realisation that one's personal, spiritual, cultural or religious beliefs should not prevent the provision of adequate and appropriate information to the patient and/or the patient's family, or the provision of appropriate management including referral to another practitioner. (8).The principles of amelioration of suffering and disability, rehabilitation and the care of the dying. (6). Normal pregnancy and childbirth, the more common obstetrical emergencies, the principles of antenatal and postnatal care, and medical aspects of family planning. (20) Communication skills, including being able to listen and respond, as well as being able to convey information clearly, considerately and sensitively to patients and their families, doctors, nurses other health professionals and the general public. (21) The skills needed to work safely as an intern, as outlined in the National Patient Safety Education Framework developed by the Australian Council for Quality and Safety in Health Care. (22) The ability to counsel patients sensitively and effectively and to provide information in a manner that ensures patients and families can be fully informed when consenting to any procedure. (37). A commitment to communicating with patients and their families, and to involving them fully in planning management. (39). A preparedness to work effectively in a team with other health care professionals. (11). Indigenous health, including the history, cultural development and health of the Indigenous peoples of Australia or New Zealand. (13) The ability to construct, in consultation with a patient, an accurate, organised and problem-focused medical history. (14) The ability to perform an accurate physical and mental state examination. (32) An appreciation of the complexity of ethical issues related to human life and death, including the allocation of scarce resources. (23) The ability to recognise serious illness and to perform common emergency and life-saving procedures, including caring for the unconscious patient and cardiopulmonary resuscitation. (15) The ability to choose, from the repertoire of clinical skills, those that are appropriate and practical to apply in a given situation. (16) The ability to interpret and integrate the history and physical examination findings to arrive at an appropriate diagnosis or differential diagnosis. (4) Common diagnostic procedures, their uses and limitations. (17) The ability to select the most appropriate and cost effective diagnostic procedures. (18) The ability to interpret common diagnostic procedures. (5) Management of common conditions including pharmacological, physical, nutritional and psychological therapies. A more detailed knowledge of management is required for those conditions that require urgent assessment and treatment. (19) The ability to formulate a management plan, and to plan management in concert with the patient.
Predominately
acquired in
settings other than
clinical settings.
Requires some
degree of
clinical setting.
Predominately
acquired in clinical
settings.

Attr
ibut
e 19
& 5
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
Feb
ruar
y 20
11
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(5)
Man
agem
ent o
f com
mon
co
nditi
ons
incl
udin
g ph
arm
acol
ogic
al, p
hys
ical
, nu
triti
onal
and
psy
chol
ogic
al
ther
apie
s. A
mor
e de
taile
d kn
owle
dge
of m
anag
emen
t is
requ
ired
for
thos
e co
nditi
ons
that
re
quire
urg
ent a
sses
smen
t and
tr
eatm
ent.
1. T
he s
tude
nt h
as th
e ab
ility
to
unde
rsta
nd a
nd w
here
app
ropr
iate
app
ly
the
man
agem
ent o
f com
mon
con
ditio
ns
incl
udin
g th
e us
e of
pha
rmac
olog
ical
, ph
ysic
al, n
utrit
iona
l and
psy
chol
ogic
al
ther
apie
s.
2. T
he s
tude
nt h
as th
e ab
ility
to id
entif
y an
d m
anag
e th
ose
cond
ition
s w
hich
re
quire
urg
ent a
sses
smen
t and
trea
tmen
t. A
lso
refe
r to
attr
ibut
e 19
1.
Iden
tifie
s a
rang
e of
man
agem
ent o
ptio
ns in
clud
ing
phar
mac
olog
ical
, ph
ysic
al, n
utrit
iona
l and
psy
chol
ogic
al th
erap
ies
avai
labl
e to
man
age
com
mon
con
ditio
ns.
2.
Id
entif
ies,
ass
esse
s an
d tr
eats
com
mon
con
ditio
ns w
hich
req
uire
urg
ent
man
agem
ent.
Als
o re
fer
to a
ttrib
ute
19
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(1
9) T
he a
bilit
y to
form
ulat
e a
man
agem
ent p
lan,
and
to p
lan
man
agem
ent i
n co
ncer
t with
a
patie
nt.
1. T
he s
tude
nt h
as th
e ab
ility
to fo
rmul
ate
an a
ppro
pria
te m
anag
emen
t pla
n.
2. T
he s
tude
nt h
as th
e ab
ility
to in
clud
e pa
tient
pre
fere
nces
in th
e fo
rmul
atio
n of
a
man
agem
ent p
lan.
1.
Iden
tifie
s th
e di
agno
ses/
issu
es r
equi
ring
man
agem
ent.
2.
E
xpla
ins
diag
nose
s/is
sues
or
pres
entin
g pr
oble
m to
the
patie
nt.
3.
Sel
ects
the
mos
t app
ropr
iate
man
agem
ent o
ptio
n(s)
and
form
ulat
es a
m
anag
emen
t pla
n in
con
cert
with
the
patie
nt.
4.
Iden
tifie
s in
form
atio
n, c
omm
unity
res
ourc
es a
nd o
ther
res
ourc
es w
hich
co
uld
assi
st w
ith th
e m
anag
emen
t pla
n.
5.
Com
mun
icat
es c
lear
sta
tem
ents
reg
ardi
ng th
e ne
xt s
tep;
incl
udin
g in
vest
igat
ions
, tre
atm
ent,
inte
rven
tions
and
pla
ns r
egar
ding
con
tinui
ty o
f ca
re.
6.
Dem
onst
rate
s so
und
com
mun
icat
ion
skill
s al
low
ing
the
iden
tific
atio
n of
pa
tient
pre
fere
nces
and
incl
usio
n th
roug
h ne
gotia
tion
of th
ose
proc
edur
es in
to th
e fin
al p
lan.
7.
D
emon
stra
tes
know
ledg
e of
the
impa
ct o
f diff
eren
t cul
tura
l, so
cial
, re
ligio
us a
nd li
ngui
stic
bac
kgro
unds
on
man
agem
ent p
lans
.
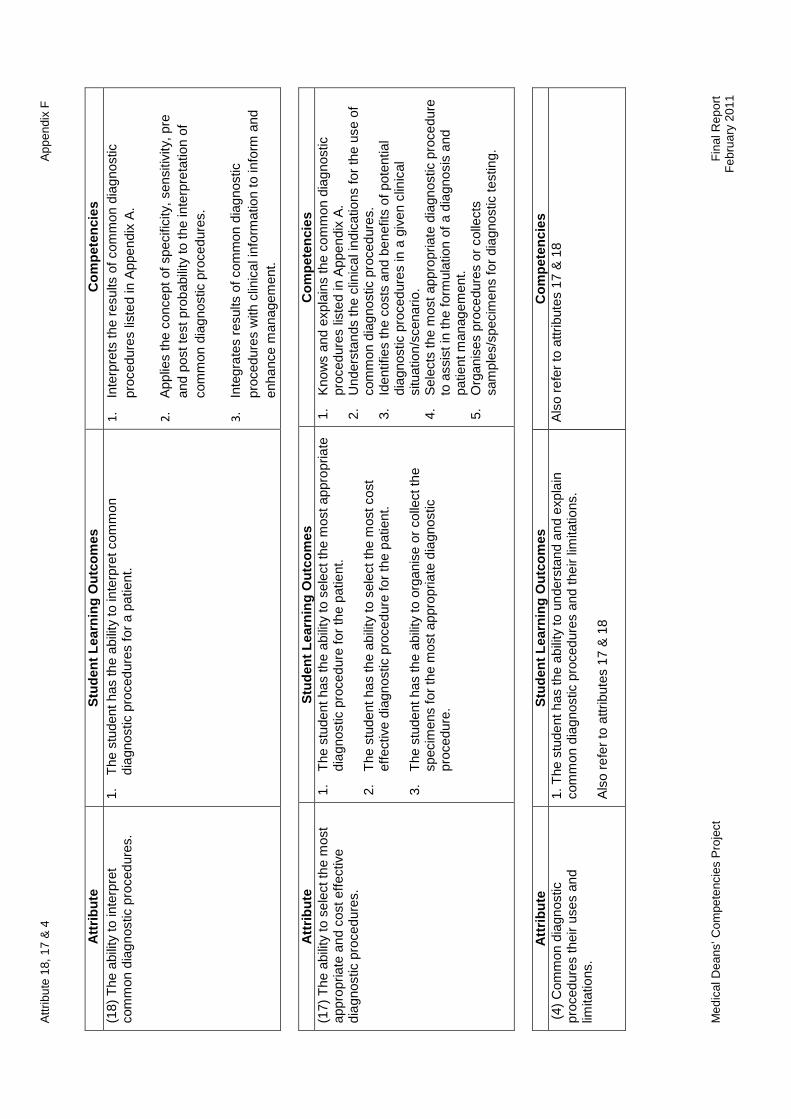
Attr
ibut
e 18
, 17
& 4
App
endi
x F
M
edic
al D
eans
’ Com
pete
ncie
s P
roje
ct
F
inal
Rep
ort
Feb
ruar
y 20
11
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(17)
The
abi
lity
to s
elec
t the
mos
t ap
prop
riate
and
cos
t effe
ctiv
e di
agno
stic
pro
cedu
res.
1.
The
stu
dent
has
the
abili
ty to
sel
ect t
he m
ost a
ppro
pria
te
diag
nost
ic p
roce
dure
for
the
patie
nt.
2.
The
stu
dent
has
the
abili
ty to
sel
ect t
he m
ost c
ost
ef
fect
ive
diag
nost
ic p
roce
dure
for
the
patie
nt.
3.
The
stu
dent
has
the
abili
ty to
org
anis
e or
col
lect
the
spec
imen
s fo
r th
e m
ost a
ppro
pria
te d
iagn
ostic
pr
oced
ure.
1.
Kno
ws
and
expl
ains
the
com
mon
dia
gnos
tic
proc
edur
es li
sted
in A
ppen
dix
A.
2.
Und
erst
ands
the
clin
ical
indi
catio
ns fo
r th
e us
e of
co
mm
on d
iagn
ostic
pro
cedu
res.
3.
Id
entif
ies
the
cost
s an
d be
nefit
s of
pot
entia
l di
agno
stic
pro
cedu
res
in a
giv
en c
linic
al
situ
atio
n/sc
enar
io.
4.
Sel
ects
the
mos
t app
ropr
iate
dia
gnos
tic p
roce
dure
to
ass
ist i
n th
e fo
rmul
atio
n of
a d
iagn
osis
and
pa
tient
man
agem
ent.
5.
Org
anis
es p
roce
dure
s or
col
lect
s sa
mpl
es/s
peci
men
s fo
r di
agno
stic
test
ing.
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(4)
Com
mon
dia
gnos
tic
proc
edur
es th
eir
uses
and
lim
itatio
ns.
1. T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d an
d ex
plai
n co
mm
on d
iagn
ostic
pro
cedu
res
and
thei
r lim
itatio
ns.
Als
o re
fer
to a
ttrib
utes
17
& 1
8
Als
o re
fer
to a
ttrib
utes
17
& 1
8
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(18)
The
abi
lity
to in
terp
ret
com
mon
dia
gnos
tic p
roce
dure
s.
1.
The
stu
dent
has
the
abili
ty to
inte
rpre
t com
mon
di
agno
stic
pro
cedu
res
for
a pa
tient
.
1.
Inte
rpre
ts th
e re
sults
of c
omm
on d
iagn
ostic
pr
oced
ures
list
ed in
App
endi
x A
.
2.
App
lies
the
conc
ept o
f spe
cific
ity, s
ensi
tivity
, pre
an
d po
st te
st p
roba
bilit
y to
the
inte
rpre
tatio
n of
co
mm
on d
iagn
ostic
pro
cedu
res.
3
. In
tegr
ates
res
ults
of c
omm
on d
iagn
ostic
pr
oced
ures
with
clin
ical
info
rmat
ion
to in
form
and
en
hanc
e m
anag
emen
t.

Attr
ibut
e 16
& 1
5
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
F
inal
Rep
ort
Feb
ruar
y 20
11
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(1
6) T
he a
bilit
y to
inte
rpre
t and
inte
grat
e th
e hi
stor
y an
d ph
ysic
al e
xam
inat
ion
findi
ngs
to a
rriv
e at
an
appr
opria
te d
iagn
osis
or
diffe
rent
ial
diag
nosi
s.
1.
The
stu
dent
has
the
abili
ty to
con
duct
a p
atie
nt
inte
rvie
w.
2.
The
stu
dent
has
the
abili
ty to
per
form
a
stru
ctur
ed p
robl
em fo
cuse
d ph
ysic
al
exam
inat
ion.
3.
T
he s
tude
nt h
as th
e ab
ility
to in
tegr
ate
info
rmat
ion
obta
ined
from
a p
atie
nt in
terv
iew
an
d ph
ysic
al e
xam
inat
ion.
4.
T
he s
tude
nt h
as th
e ab
ility
to in
tegr
ate
info
rmat
ion
and
to u
tilis
e cl
inic
al r
easo
ning
to
arriv
e at
a d
iagn
osis
and
diff
eren
tial d
iagn
osis
.
1.
Con
duct
s a
prob
lem
focu
sed,
str
uctu
red
clin
ical
inte
rvie
w.
2.
E
licits
info
rmat
ion
for
the
purp
oses
of a
pat
ient
hi
stor
y fr
om th
e pa
tient
, rel
ativ
es, p
erso
ns
pres
ent f
or th
e in
terv
iew
. 3.
C
ondu
cts
a pr
oble
m fo
cuse
d st
ruct
ured
ph
ysic
al e
xam
inat
ion.
4.
C
ondu
cts
a w
hole
per
son
phys
ical
ex
amin
atio
n or
org
an(s
)/sy
stem
spe
cific
ph
ysic
al e
xam
inat
ion
as a
ppro
pria
te.
5.
Inte
grat
es th
e in
form
atio
n ob
tain
ed to
arr
ive
at
an a
ppro
pria
te d
iagn
osis
and
diff
eren
tial
diag
nosi
s.
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(1
5) T
he a
bilit
y to
cho
ose
from
the
repe
rtoi
re o
f cl
inic
al s
kills
, tho
se th
at a
re a
ppro
pria
te a
nd
prac
tical
to a
pply
in a
giv
en s
ituat
ion.
1.
The
stu
dent
has
the
abili
ty to
per
form
a r
ange
of
dia
gnos
tic a
nd th
erap
eutic
clin
ical
ski
lls.
2.
The
stu
dent
has
the
abili
ty to
ana
lyse
a c
linic
al
pres
enta
tion
and
sele
ct a
ppro
pria
te c
linic
al
skill
s fo
r th
e si
tuat
ion.
1.
Ana
lyse
s th
e cl
inic
al p
rese
ntat
ion
and
dete
rmin
es th
e re
quire
d cl
inic
al s
kills
.
2.
Per
form
s di
agno
stic
and
ther
apeu
tic c
linic
al
skill
s as
list
ed in
App
endi
x B
.
3.
Rec
ogni
ses
the
limits
of h
is/h
er c
linic
al s
kills
. 4.
R
ecog
nise
s th
e lim
its o
f his
/her
aut
horit
y.
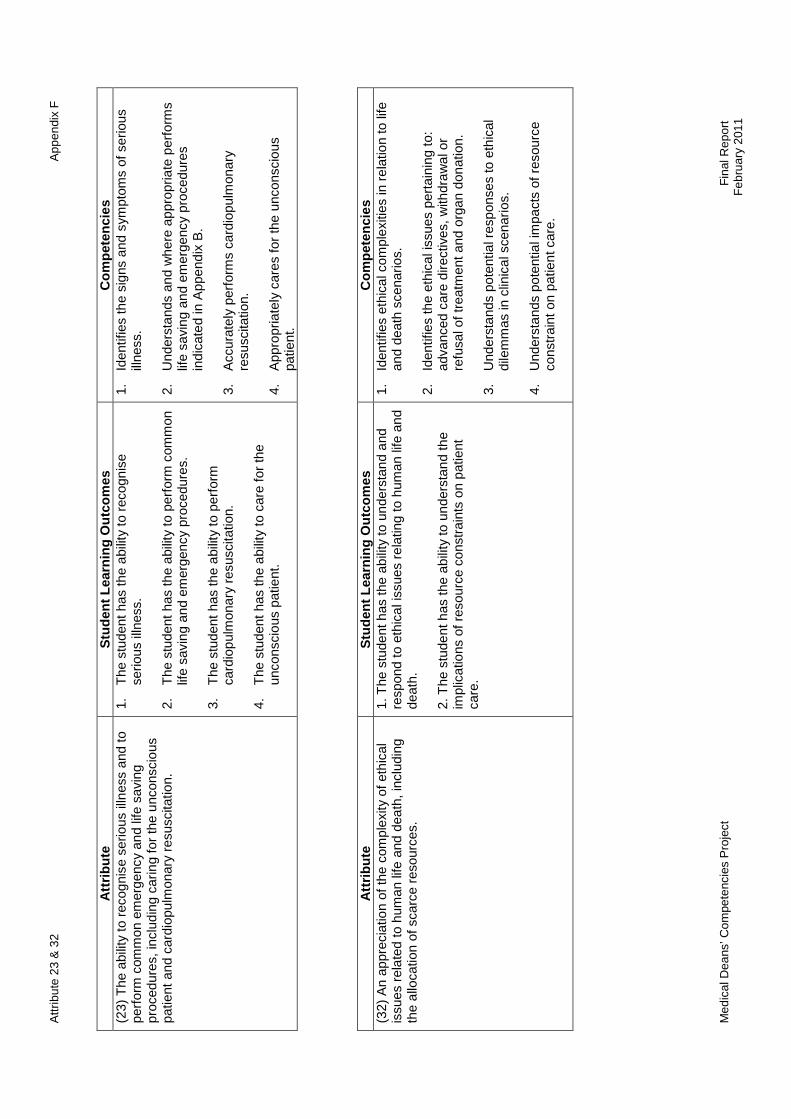
Attr
ibut
e 23
& 3
2
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
F
ebru
ary
2011
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
me
s C
ompe
tenc
ies
(2
3) T
he a
bilit
y to
rec
ogni
se s
erio
us il
lnes
s an
d to
pe
rfor
m c
omm
on e
mer
genc
y an
d lif
e sa
ving
pr
oced
ures
, inc
ludi
ng c
arin
g fo
r th
e un
cons
ciou
s pa
tient
and
car
diop
ulm
onar
y re
susc
itatio
n.
1.
The
stu
dent
has
the
abili
ty to
rec
ogni
se
serio
us il
lnes
s.
2.
The
stu
dent
has
the
abili
ty to
per
form
com
mon
lif
e sa
ving
and
em
erge
ncy
proc
edur
es.
3.
The
stu
dent
has
the
abili
ty to
per
form
ca
rdio
pulm
onar
y re
susc
itatio
n.
4.
The
stu
dent
has
the
abili
ty to
car
e fo
r th
e un
cons
ciou
s pa
tient
.
1.
Iden
tifie
s th
e si
gns
and
sym
ptom
s of
ser
ious
ill
ness
.
2.
Und
erst
ands
and
whe
re a
ppro
pria
te p
erfo
rms
life
savi
ng a
nd e
mer
genc
y pr
oced
ures
in
dica
ted
in A
ppen
dix
B.
3.
Acc
urat
ely
perf
orm
s ca
rdio
pulm
onar
y re
susc
itatio
n.
4.
App
ropr
iate
ly c
ares
for
the
unco
nsci
ous
patie
nt.
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(3
2) A
n ap
prec
iatio
n of
the
com
plex
ity o
f eth
ical
is
sues
rel
ated
to h
uman
life
and
dea
th, i
nclu
ding
th
e al
loca
tion
of s
carc
e re
sour
ces.
1. T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d an
d re
spon
d to
eth
ical
issu
es r
elat
ing
to h
uman
life
and
de
ath.
2.
The
stu
dent
has
the
abili
ty to
und
erst
and
the
impl
icat
ions
of r
esou
rce
cons
trai
nts
on p
atie
nt
care
.
1.
Iden
tifie
s et
hica
l com
plex
ities
in r
elat
ion
to li
fe
and
deat
h sc
enar
ios.
2.
Iden
tifie
s th
e et
hica
l iss
ues
pert
aini
ng to
: ad
vanc
ed c
are
dire
ctiv
es, w
ithdr
awal
or
refu
sal o
f tre
atm
ent a
nd o
rgan
don
atio
n.
3.
Und
erst
ands
pot
entia
l res
pons
es to
eth
ical
di
lem
mas
in c
linic
al s
cena
rios
. 4.
U
nder
stan
ds p
oten
tial i
mpa
cts
of r
esou
rce
cons
trai
nt o
n pa
tient
car
e.
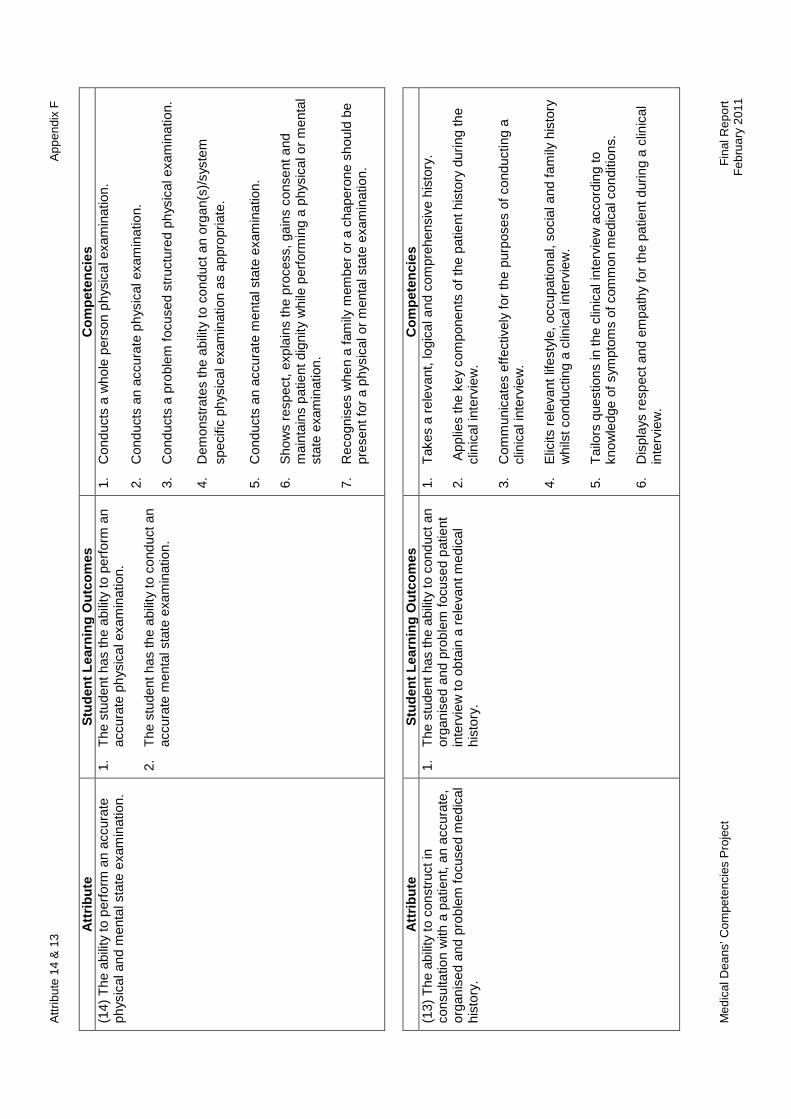
Attr
ibut
e 14
& 1
3
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
F
ebru
ary
2011
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(13)
The
abi
lity
to c
onst
ruct
in
cons
ulta
tion
with
a p
atie
nt, a
n ac
cura
te,
orga
nise
d an
d pr
oble
m fo
cuse
d m
edic
al
hist
ory.
1.
The
stu
dent
has
the
abili
ty to
con
duct
an
orga
nise
d an
d pr
oble
m fo
cuse
d pa
tient
in
terv
iew
to o
btai
n a
rele
vant
med
ical
hi
stor
y.
1.
Tak
es a
rel
evan
t, lo
gica
l and
com
preh
ensi
ve h
isto
ry.
2.
App
lies
the
key
com
pone
nts
of th
e pa
tient
his
tory
dur
ing
the
clin
ical
inte
rvie
w.
3.
Com
mun
icat
es e
ffect
ivel
y fo
r th
e pu
rpos
es o
f con
duct
ing
a cl
inic
al in
terv
iew
. 4.
E
licits
rel
evan
t life
styl
e, o
ccup
atio
nal,
soci
al a
nd fa
mily
his
tory
w
hils
t con
duct
ing
a cl
inic
al in
terv
iew
. 5.
T
ailo
rs q
uest
ions
in th
e cl
inic
al in
terv
iew
acc
ordi
ng to
kn
owle
dge
of s
ympt
oms
of c
omm
on m
edic
al c
ondi
tions
. 6.
D
ispl
ays
resp
ect a
nd e
mpa
thy
for
the
patie
nt d
urin
g a
clin
ical
in
terv
iew
.
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
me
s C
ompe
tenc
ies
(1
4) T
he a
bilit
y to
per
form
an
accu
rate
ph
ysic
al a
nd m
enta
l sta
te e
xam
inat
ion.
1.
T
he s
tude
nt h
as th
e ab
ility
to p
erfo
rm a
n ac
cura
te p
hys
ical
exa
min
atio
n.
2.
The
stu
dent
has
the
abili
ty to
con
duct
an
accu
rate
men
tal s
tate
exa
min
atio
n.
1.
Con
duct
s a
who
le p
erso
n ph
ysic
al e
xam
inat
ion.
2.
Con
duct
s an
acc
urat
e ph
ysic
al e
xam
inat
ion.
3.
Con
duct
s a
prob
lem
focu
sed
stru
ctur
ed p
hys
ical
exa
min
atio
n.
4.
Dem
onst
rate
s th
e ab
ility
to c
ondu
ct a
n or
gan(
s)/s
yste
m
spec
ific
phys
ical
exa
min
atio
n as
app
ropr
iate
. 5.
C
ondu
cts
an a
ccur
ate
men
tal s
tate
exa
min
atio
n.
6.
Sho
ws
resp
ect,
expl
ains
the
proc
ess,
gai
ns c
onse
nt a
nd
mai
ntai
ns p
atie
nt d
igni
ty w
hile
per
form
ing
a ph
ysic
al o
r m
enta
l st
ate
exam
inat
ion.
7.
R
ecog
nise
s w
hen
a fa
mily
mem
ber
or a
cha
pero
ne s
houl
d be
pr
esen
t for
a p
hysi
cal o
r m
enta
l sta
te e
xam
inat
ion.

Attr
ibut
e 11
& 3
9
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
F
inal
Rep
ort
Feb
ruar
y 20
11
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(39)
A p
repa
redn
ess
to
wor
k ef
fect
ivel
y in
a te
am
with
oth
er h
ealth
car
e pr
ofes
sion
als.
1.
The
stu
dent
has
an
abili
ty to
und
erst
and,
res
pect
and
in
corp
orat
e th
e ro
les
of o
ther
hea
lth p
rofe
ssio
nals
in
heal
th c
are.
2.
T
he s
tude
nt h
as a
n ab
ility
to w
ork
effe
ctiv
ely
in a
team
w
ith o
ther
hea
lthca
re p
rofe
ssio
nals
.
3.
The
stu
dent
has
the
abili
ty to
und
erst
and
his/
her
role
in a
te
am w
ith o
ther
hea
lth p
rofe
ssio
nals
.
1.
Iden
tifie
s an
d ac
ts u
pon
his/
her
role
in a
hea
lth c
are
team
.
2.
Iden
tifie
s ro
les
of o
ther
hea
lth p
rofe
ssio
nals
in a
hea
lth
care
team
.
3.
Dis
play
s pr
ofes
sion
al c
ourt
esy
for
othe
r he
alth
car
e pr
ofes
sion
als
in a
hea
lth c
are
team
. 4.
C
ontr
ibut
es to
team
wor
k by
beh
avin
g in
wa
ys w
hich
m
axim
ises
the
team
’s e
ffect
iven
ess.
• A
ttrib
ute
39 h
as b
een
iden
tifie
d by
the
Writ
ing
Gro
up a
s re
quiri
ng r
evis
ed b
y th
e A
MC
. .
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
me
s C
ompe
tenc
ies
(1
1) In
dige
nous
hea
lth,
incl
udin
g th
e hi
stor
y,
cultu
ral d
evel
opm
ent a
nd
heal
th o
f the
Indi
geno
us
peop
les
of A
ustr
alia
and
N
ew Z
eala
nd.
1.
The
stu
dent
is a
war
e of
, and
abl
e to
rel
ate
to, t
he fa
ctor
s w
hich
con
trib
ute
to th
e st
atus
of I
ndig
enou
s he
alth
. 2.
T
he s
tude
nt u
nder
stan
ds th
at c
ultu
re is
impo
rtan
t to
Indi
geno
us p
eopl
e an
d ca
n af
fect
thei
r he
alth
and
sen
se
of w
ell-b
eing
. 3.
T
he s
tude
nt u
nder
stan
ds A
ustr
alia
n/N
ew Z
eala
nd h
isto
ry
and
is a
war
e of
the
expe
rienc
e of
Indi
geno
us p
eopl
es a
nd
how
this
impa
cts
on In
dige
nous
hea
lth a
nd h
ealth
car
e.
4.
The
stu
dent
und
erst
ands
the
dive
rsity
of I
ndig
enou
s cu
lture
s, e
xper
ienc
es a
nd c
omm
uniti
es.
1.
App
lies
an u
nder
stan
ding
of I
ndig
enou
s m
orta
lity
and
mor
bidi
ty p
atte
rns
and
thei
r im
pact
as
wel
l as
reco
gnis
ing
issu
es a
ssoc
iate
d w
ith a
cces
s to
hea
lth c
are.
2.
D
emon
stra
tes
a w
orki
ng k
now
ledg
e of
the
soci
al
dete
rmin
ants
of I
ndig
enou
s he
alth
incl
udin
g th
e im
pact
of
colo
nisa
tion,
life
styl
e, n
utrit
ion,
soc
ioec
onom
ic fa
ctor
s,
geog
raph
y an
d ac
cess
to h
ousi
ng, e
duca
tion
and
heal
th
care
. 3.
C
onsi
ders
the
hist
oric
al, c
ultu
ral,
soci
al a
nd p
oliti
cal
fact
ors
whi
ch im
pact
on
the
heal
th o
f an
Indi
geno
us
patie
nt.
4.
Dem
onst
rate
s a
sens
itive
and
res
pect
ful a
ppro
ach
whe
n in
tera
ctin
g w
ith In
dige
nous
peo
ple
/ pat
ient
s an
d pr
actic
es w
ith th
e kn
owle
dge
that
Indi
geno
us c
ultu
res
are
dive
rse.
5.
P
lans
and
pro
vide
s ca
re in
a c
ompr
ehen
sive
and
cu
ltura
lly s
ecur
e w
ay.

Attr
ibut
e 37
& 2
2
App
endi
x F
M
edic
al D
eans
’ Com
pete
ncie
s P
roje
ct
F
inal
Rep
ort
Feb
ruar
y 20
11
A
ttrib
ute
S
tude
nt L
earn
ing
Ou
tcom
es
Com
pete
ncie
s
(22)
The
abi
lity
to c
ouns
el p
atie
nts
sens
itive
ly a
nd
effe
ctiv
ely,
and
to p
rovi
de in
form
atio
n in
a m
anne
r th
at e
nsur
es p
atie
nts
and
fam
ilies
can
be
fully
in
form
ed w
hen
cons
entin
g to
an
y pr
oced
ures
.
1. T
he s
tude
nt h
as th
e ab
ility
to c
ouns
el p
atie
nts
sens
itive
ly a
nd e
ffect
ivel
y.
2. T
he s
tude
nt h
as th
e ab
ility
to c
usto
mis
e in
form
atio
n to
mee
t the
req
uire
men
ts o
f pat
ient
s an
d fa
mili
es.
3. T
he s
tude
nt h
as th
e ab
ility
to o
btai
n in
form
ed
cons
ent f
rom
pat
ient
s, fa
mili
es a
nd o
ther
s as
re
quire
d.
1.
Em
path
ises
with
and
sho
ws
com
pass
ion
tow
ards
pat
ient
s an
d th
eir
fam
ilies
.
2.
Effe
ctiv
ely
com
mun
icat
es w
hils
t cou
nsel
ling
patie
nts.
3.
Iden
tifie
s ho
w a
nd w
here
to s
ourc
e ap
prop
riate
info
rmat
ion
for
patie
nts
and
thei
r fa
mili
es.
4.
P
rovi
des
rele
vant
info
rmat
ion
and
optio
ns,
cont
extu
alis
ed to
the
circ
umst
ance
s of
pa
tient
s an
d th
eir
fam
ilies
.
5.
Exp
lain
s m
anag
emen
t opt
ions
for
the
purp
oses
of i
nfor
med
con
sent
.
6.
Exp
lain
s ad
vers
e ef
fect
s, r
isks
, ben
efits
and
po
ssib
le o
utco
mes
of a
pro
cedu
re to
a p
atie
nt
for
the
purp
oses
of i
nfor
med
con
sent
.
7.
Ens
ures
that
pat
ient
s an
d th
eir
fam
ilies
are
fu
lly in
form
ed w
hen
cons
entin
g to
m
anag
emen
t opt
ions
.
8.
Doc
umen
ts p
atie
nt c
onse
nt.
• A
ttrib
ute
22 h
as b
een
iden
tifie
d by
the
Writ
ing
Gro
up a
s an
attr
ibut
e th
at c
ould
be
revi
sed
by th
e A
MC
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(3
7) A
com
mitm
ent t
o co
mm
unic
atin
g w
ith p
atie
nts
and
thei
r fa
mili
es, a
nd to
invo
lvin
g th
em fu
lly in
pl
anni
ng m
anag
emen
t.
1. T
he s
tude
nt h
as th
e ab
ility
to c
omm
unic
ate
effe
ctiv
ely
with
a p
atie
nt in
volv
ing
them
fully
in
plan
ning
man
agem
ent i
n a
rang
e of
set
tings
. 2.
The
stu
dent
has
the
abili
ty to
app
ropr
iate
ly
invo
lve
and
com
mun
icat
e w
ith fa
mily
mem
bers
an
d ot
hers
in m
anag
emen
t pla
ns.
1.
Dem
onst
rate
s so
und
com
mun
icat
ion
skill
s al
low
ing
the
iden
tific
atio
n an
d in
clus
ion
of
patie
nt a
nd fa
mily
pre
fere
nces
in th
e m
anag
emen
t pla
n.
2.
In
corp
orat
es k
now
ledg
e of
diff
eren
t cul
tura
l, so
cial
, rel
igio
us a
nd li
ngui
stic
bac
kgro
unds
in
com
mun
icat
ing
man
agem
ent p
lans
to p
atie
nts
and
thei
r fa
mili
es.

Attr
ibut
e 21
& 2
0
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
F
ebru
ary
2011
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(2
1) T
he s
kills
nee
ded
to w
ork
safe
ly a
s an
inte
rn, a
s ou
tline
d in
th
e N
atio
nal P
atie
nt S
afet
y E
duca
tion
Fra
mew
ork
deve
lope
d by
the
Aus
tral
ian
Cou
ncil
for
Qua
lity
and
Saf
ety
in H
ealth
Car
e.
1.
The
stu
dent
has
the
abili
ty to
wor
k sa
fely
.
2.
The
stu
dent
has
the
abili
ty to
app
ly th
e re
leva
nt
skill
s of
the
Nat
iona
l Pat
ient
Saf
ety
Edu
catio
nal
Fra
mew
ork
appr
opria
te fo
r a
doct
or c
omm
enci
ng
inte
rnsh
ip.
The
re w
ill b
e a
link
crea
ted
in th
e m
ind
map
fram
ewor
k to
th
e N
atio
nal P
atie
nt S
afet
y E
duca
tion
Fra
mew
ork.
To
be d
eter
min
ed
Attr
ibut
e 21
nee
ds to
be
take
n ou
t and
wor
ked
on b
y a
noth
er g
roup
.
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(20)
Com
mun
icat
ion
skill
s,
incl
udin
g be
ing
able
to li
sten
and
re
spon
d, a
s w
ell a
s be
ing
able
to
conv
ey
info
rmat
ion
clea
rly,
cons
ider
atel
y an
d se
nsiti
vely
to
patie
nts
and
thei
r fa
mili
es, d
octo
rs,
nurs
es, o
ther
hea
lth p
rofe
ssio
nals
an
d th
e ge
nera
l pub
lic.
1. T
he s
tude
nt h
as th
e ab
ility
to c
omm
unic
ate
effe
ctiv
ely
with
pat
ient
s an
d fa
mili
es in
a r
ange
of s
ettin
gs.
2. T
he s
tude
nt h
as th
e ab
ility
to c
omm
unic
ate
effe
ctiv
ely
with
oth
er h
ealth
pro
fess
iona
ls a
nd th
e ge
nera
l pub
lic.
1.
List
ens
and
resp
onds
em
path
etic
ally
usi
ng v
erba
l, no
n ve
rbal
and
writ
ten
form
ats.
2.
Rec
ogni
ses
and
deal
s w
ith b
arrie
rs to
effe
ctiv
e co
mm
unic
atio
n in
a r
ange
of s
ettin
gs.
3.
C
omm
unic
ates
pro
fess
iona
lly a
nd c
onsi
dera
tely
with
the
heal
th c
are
team
for
optim
al p
atie
nt o
utco
mes
.
4.
Inte
ract
s pr
ofes
sion
ally
with
the
gene
ral p
ublic
.

Attr
ibut
e 6
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
F
inal
Rep
ort
Feb
ruar
y 20
11
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(6
) N
orm
al p
regn
ancy
and
chi
ldbi
rth,
the
mor
e co
mm
on o
bste
tric
al e
mer
genc
ies,
the
prin
cipl
es o
f ant
enat
al a
nd p
ostn
atal
car
e,
and
med
ical
asp
ects
of f
amily
pla
nnin
g.
1. T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d no
rmal
pr
egna
ncy
and
child
birt
h.
2. T
he s
tude
nt h
as th
e ab
ility
to a
pply
kno
wle
dge
rega
rdin
g th
e m
ore
com
mon
obs
tetr
ical
em
erge
ncie
s.
3. T
he s
tude
nt h
as th
e ab
ility
to a
pply
the
prin
cipl
es o
f an
tena
tal a
nd p
ostn
atal
car
e.
4. T
he s
tude
nt h
as th
e ab
ility
to e
xpla
in th
e m
edic
al
aspe
cts
of fa
mily
pla
nnin
g.
1.
Exp
lain
s no
rmal
pre
gnan
cy a
nd c
hild
birt
h.
2.
P
artic
ipat
es u
nder
sup
ervi
sion
in th
e m
anag
emen
t of a
nor
mal
chi
ldbi
rth.
3.
E
xpla
ins
the
mor
e co
mm
on o
bste
tric
al
emer
genc
ies
incl
udin
g pa
in a
nd b
leed
ing.
4.
E
xpla
ins
the
prin
cipl
es o
f ant
enat
al c
are.
5.
E
xpla
ins
the
prin
cipl
es o
f pos
tnat
al c
are.
6.
C
omm
unic
ates
effe
ctiv
ely
with
pat
ient
s in
re
gard
s to
the
med
ical
asp
ects
of f
amily
pl
anni
ng in
clud
ing
advi
ce o
n co
ntra
cept
ion,
fe
rtili
ty a
nd d
ealin
g w
ith a
n un
wan
ted
preg
nanc
y.

Attr
ibut
e 8
A
ppen
dix
F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
F
inal
Rep
ort
Feb
ruar
y 20
11
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(8
) T
he p
rinci
ples
of
amel
iora
tion
of s
uffe
ring
and
disa
bilit
y, r
ehab
ilita
tion
and
care
of t
he d
ying
.
1. T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d an
d am
elio
rate
suf
ferin
g.
2. T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d an
d ap
ply
the
prin
cipl
es o
f man
agin
g di
sabi
lity.
3.
The
stu
dent
has
the
abili
ty to
und
erst
and
and
appl
y th
e pr
inci
ples
of r
ehab
ilita
tion.
4.
The
stu
dent
has
the
abili
ty to
und
erst
and
and
appl
y th
e pr
inci
ples
for
care
of t
he d
ying
.
1.
Con
trib
utes
as
a te
am m
embe
r in
the
man
agem
ent o
f suf
ferin
g,
disa
bilit
y, r
ehab
ilita
tion
and
care
of t
he d
ying
.
2.
Und
erst
ands
and
app
lies
the
prin
cipl
es o
f am
elio
ratio
n of
suf
ferin
g.
3.
P
rovi
des
peop
le w
ith a
dis
abili
ty w
ith th
e re
sour
ces
and
info
rmat
ion
requ
ired
to a
ttain
inde
pend
ence
and
sel
f det
erm
inat
ion.
4.
Und
erst
ands
and
app
lies
the
prin
cipl
es o
f reh
abili
tatio
n in
clud
ing
enab
ling
peop
le to
mai
ntai
n or
ach
ieve
thei
r op
timal
phy
sica
l, se
nsor
y, in
telle
ctua
l, so
cial
and
psy
chol
ogic
al fu
nctio
ning
leve
ls.
5.
U
nder
stan
ds a
nd a
pplie
s th
e pr
inci
ples
of p
allia
tive
care
incl
udin
g sy
mpt
om r
elie
f and
psy
chol
ogic
al s
uppo
rt fo
r pa
tient
s an
d th
eir
fam
ily.
6.
U
nder
stan
ds a
nd a
pplie
s th
e pr
inci
ples
of e
nd o
f life
pla
nnin
g an
d ca
re.
7.
E
ngag
es w
ith p
atie
nts
and
thei
r fa
mili
es to
ass
ess
thei
r ne
eds
incl
udin
g or
gani
sing
app
ropr
iate
sup
port
and
ber
eave
men
t co
unse
lling
.
8.
Rec
ogni
ses
and
appr
ecia
tes
the
need
to c
all o
n ap
prop
riate
sup
port
s fo
r se
lf an
d ot
her
mem
bers
of t
he h
ealth
car
e te
am.

Attr
ibut
e 40
& 9
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
F
inal
Rep
ort
Feb
ruar
y 20
11
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(4
0) A
rea
lisat
ion
that
one
’s o
wn
pers
onal
, sp
iritu
al, c
ultu
ral o
r re
ligio
us b
elie
fs s
houl
d no
t pr
even
t the
pro
visi
on o
f ade
quat
e an
d ap
prop
riate
in
form
atio
n to
the
patie
nt a
nd/o
r th
e pa
tient
’s
fam
ily, o
r th
e pr
ovis
ion
of a
ppro
pria
te
man
agem
ent i
nclu
ding
the
refe
rral
to a
noth
er
prac
titio
ner.
1. T
he s
tude
nt h
as th
e ab
ility
to r
ecog
nise
his
/her
ow
n pe
rson
al, s
pirit
ual,
cultu
ral o
r re
ligio
us v
alue
s.
2. T
he s
tude
nt h
as th
e ab
ility
to r
ealis
e th
at h
is/h
er
own
spiri
tual
, cul
tura
l or
relig
ious
bel
iefs
sho
uld
not p
reve
nt a
ppro
pria
te p
atie
nt m
anag
emen
t. 3.
The
stu
dent
has
the
abili
ty to
rea
lise
whe
n re
ferr
al to
ano
ther
pra
ctiti
oner
is a
ppro
pria
te.
1.
Iden
tifie
s hi
s/he
r ow
n pe
rson
al s
pirit
ual,
pers
onal
, cul
tura
l and
rel
igio
us b
elie
fs.
2.
C
omm
unic
ates
app
ropr
iate
info
rmat
ion
to
patie
nts
and
thei
r fa
mili
es ir
resp
ectiv
e of
hi
s/he
r ow
n be
liefs
. 3.
P
lans
app
ropr
iate
pat
ient
man
agem
ent
irres
pect
ive
of h
is/h
er o
wn
belie
fs.
4.
Ref
ers
to a
noth
er p
ract
ition
er w
hen
appr
opria
te.
Attr
ibu
te
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(9
) F
acto
rs a
ffect
ing
hum
an r
elat
ions
hips
, the
ps
ycho
logi
cal,
cultu
ral,
spiri
tual
wel
l-bei
ng o
f pa
tient
s an
d th
eir
fam
ilies
, and
the
inte
ract
ions
be
twee
n hu
man
s an
d th
eir
soci
al a
nd p
hys
ical
en
viro
nmen
ts.
1.
The
stu
dent
has
the
abili
ty to
und
erst
and
the
effe
ct th
at h
uman
rel
atio
nshi
ps h
ave
on a
pa
tient
’s h
ealth
.
2.
The
stu
dent
has
the
abili
ty to
und
erst
and
the
impa
ct o
f soc
ial a
nd p
hys
ical
env
ironm
ents
on
heal
th, i
nclu
ding
the
psyc
holo
gica
l, cu
ltura
l an
d sp
iritu
al w
ell b
eing
of p
atie
nts
and
thei
r fa
mili
es.
1.
Iden
tifie
s th
e ke
y fa
ctor
s in
hum
an
rela
tions
hips
that
can
affe
ct h
ealth
.
2.
Rec
ogni
ses
the
impo
rtan
ce o
f psy
chol
ogic
al,
cultu
ral a
nd s
pirit
ual w
ell b
eing
of p
atie
nts
and
thei
r fa
mili
es a
nd h
ow th
is c
ontr
ibut
es to
he
alth
.
3.
Rec
ogni
ses
the
impa
ct o
n a
patie
nt’s
hea
lth o
f th
eir
soci
al a
nd p
hys
ical
env
ironm
ent.
4.
Id
entif
ies
the
soci
al d
eter
min
ants
of i
ndiv
idua
l an
d po
pula
tion
heal
th in
clud
ing
risk
fact
ors.
5.
Dem
onst
rate
s cu
ltura
lly a
ppro
pria
te c
are.

Attr
ibut
e 25
& 2
8
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
F
ebru
ary
2011
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(2
5) T
he a
bilit
y to
use
in
form
atio
n te
chno
log
y ap
prop
riate
ly a
s an
ess
entia
l re
sour
ce fo
r m
oder
n m
edic
al
prac
tice.
1.
The
stu
dent
has
the
abili
ty to
use
in
form
atio
n te
chno
log
y as
an
appr
opria
te r
esou
rce
for
acce
ssin
g qu
ality
and
up
to d
ate
info
rmat
ion.
2.
The
stu
dent
has
the
abili
ty to
use
in
form
atio
n te
chno
log
y fo
r op
timal
pat
ient
car
e.
1.
Effi
cien
tly a
cces
s re
leva
nt in
form
atio
n fo
r pa
tient
man
agem
ent,
rese
arch
and
on
goin
g pr
ofes
sion
al d
evel
opm
ent u
sing
info
rmat
ion
tech
nolo
gy.
2.
E
valu
ates
the
qual
ity a
nd r
elev
ance
of i
nfor
mat
ion
foun
d us
ing
info
rmat
ion
tech
nolo
gy.
3.
Pro
ficie
ntly
use
s av
aila
ble
elec
tron
ic p
atie
nt m
anag
emen
t sys
tem
s in
var
ious
he
alth
car
e se
tting
s.
4.
App
lies
info
rmat
ion
gain
ed to
opt
imis
e pa
tient
car
e.
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
me
s C
ompe
tenc
ies
(2
8) R
espe
ct fo
r ev
ery
hum
an
bein
g, in
clud
ing
resp
ect o
f se
xual
bou
ndar
ies.
1. T
he s
tude
nt h
as th
e ab
ility
to
disp
lay
resp
ect f
or e
very
hum
an
bein
g.
2. T
he s
tude
nt h
as th
e ab
ility
to
dem
onst
rate
res
pect
for
sexu
al
boun
darie
s.
Als
o re
fer
to a
ttrib
ute
14
1.
Tre
ats
patie
nts
with
dig
nity
at a
ll tim
es in
clud
ing
durin
g in
terv
iew
s an
d ph
ysic
al
exam
inat
ions
. 2.
R
espe
ct fo
r pa
tient
s se
xual
bou
ndar
ies
durin
g a
patie
nt in
terv
iew
and
a
phys
ical
exa
min
atio
n.
A
lso
refe
r to
attr
ibut
e 14

Attr
ibut
e 12
, 33
& 2
6
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
F
ebru
ary
2011
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(33)
A r
ealis
atio
n th
at d
octo
rs e
ncou
nter
clin
ical
pr
oble
ms
that
exc
eed
thei
r kn
owle
dge
and
skill
s,
and
that
, in
thes
e si
tuat
ions
, the
y ne
ed to
con
sult
and/
or r
efer
the
patie
nt fo
r he
lp, i
n cl
inic
al, c
ultu
ral
soci
al a
nd la
ngua
ge r
elat
ed m
atte
rs a
s ap
prop
riate
.
1.
The
stu
dent
has
the
abili
ty to
rec
ogni
se w
hen
the
clin
ical
enc
ount
er e
xcee
ds h
is/h
er
know
ledg
e an
d sk
ill le
vel.
2.
The
stu
dent
has
the
abili
ty to
rec
ogni
se w
hen
the
y ne
ed to
ref
er o
r co
nsul
t with
ano
ther
pr
actit
ione
r.
3.
The
stu
dent
has
the
abili
ty to
rec
ogni
se w
hen
to r
efer
reg
ardi
ng c
linic
al, c
ultu
ral,
soci
al a
nd
lang
uage
rel
ated
mat
ters
.
1.
Kno
ws
his/
her
own
leve
l of s
kill
and
know
ledg
e.
2.
Ack
now
ledg
es w
hen
the
clin
ical
sce
nario
ex
ceed
s th
eir
leve
l of s
kill
and
know
ledg
e.
3.
C
onsu
lts a
nd c
omm
unic
ates
with
ano
ther
pr
actit
ione
r as
app
ropr
iate
.
4.
Ref
ers
to a
ppro
pria
te s
uppo
rt s
ervi
ces.
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
nci
es
(26)
Rec
ogni
tion
that
the
doct
or’s
prim
ary
prof
essi
onal
res
pons
ibili
ties
are
the
heal
th
inte
rest
s of
the
patie
nt a
nd th
e co
mm
unity
.
1.
The
stu
dent
has
the
abili
ty to
rec
ogni
se th
at
the
doct
or’s
prim
ary
prof
essi
onal
re
spon
sibi
litie
s ar
e th
e he
alth
inte
rest
s of
the
patie
nt a
nd th
e co
mm
unity
.
1.
Mak
es p
atie
nt c
are
his/
her
prim
ary
prof
essi
onal
res
pons
ibili
ty.
2.
U
nder
stan
ds th
e pr
ofes
sion
al r
espo
nsib
ility
of
the
doct
or e
xten
ds fr
om th
e in
divi
dual
pat
ient
to
the
heal
th in
tere
sts
of th
e co
mm
unity
.
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(1
2) T
he p
rinci
ples
of e
thic
s re
late
d to
hea
lth c
are
and
the
lega
l res
pons
ibili
ties
of th
e m
edic
al
prof
essi
on.
1.
The
stu
dent
has
the
abili
ty to
und
erst
and
the
prin
cipl
es o
f eth
ics
as th
ey r
elat
e to
hea
lth
care
. 2.
T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d th
e le
gal r
espo
nsib
ilitie
s of
the
med
ical
pro
fess
ion.
1.
Mai
ntai
ns e
thic
al a
nd le
gally
app
ropr
iate
st
anda
rds
at a
ll tim
es.
2.
U
nder
stan
ds th
e le
gal r
espo
nsib
ilitie
s of
hea
lth
prof
essi
onal
s es
peci
ally
thos
e re
latin
g to
in
form
ed c
onse
nt, d
uty
of c
are,
con
fiden
tialit
y an
d co
nflic
t of i
nter
est.

Attr
ibut
e 29
& 2
4
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
F
inal
Rep
ort
Feb
ruar
y 20
11
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(2
9) R
espe
ct fo
r co
mm
unity
val
ues,
incl
udin
g an
ap
prec
iatio
n of
the
dive
rsity
of h
uman
bac
kgro
und
and
cultu
ral v
alue
s.
1. T
he s
tude
nt h
as th
e ab
ility
to r
espe
ct
com
mun
ity v
alue
s.
2. T
he s
tude
nt h
as th
e ab
ility
to a
ppre
ciat
e th
e di
vers
ity o
f hum
an b
ackg
roun
ds a
nd c
ultu
ral
valu
es.
Als
o re
fer
to a
ttrib
ute
28
1.
Res
pect
s al
l pat
ient
s, th
eir
fam
ilies
and
co
lleag
ues
rega
rdle
ss o
f age
, gen
der,
rac
e,
lang
uage
, cul
ture
, dis
abili
ty, r
elig
ion,
sex
ual
orie
ntat
ion
or e
cono
mic
sta
tus.
2.
Res
pect
s co
mm
unity
val
ues.
3.
App
reci
ates
div
ersi
ty o
f hum
an b
ackg
roun
ds.
4.
P
ract
ices
in a
cul
tura
lly s
afe
man
ner.
Als
o re
fer
to a
ttrib
ute
28
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
mes
C
ompe
tenc
ies
(2
4) T
he a
bilit
y to
inte
rpre
t med
ical
evi
denc
e in
a
criti
cal a
nd s
cien
tific
man
ner
and
an u
nder
stan
ding
of
the
epid
emio
log
y of
dis
ease
in d
iffer
ing
popu
latio
ns a
nd g
eogr
aphi
c lo
catio
ns.
1. T
he s
tude
nt h
as th
e ab
ility
to in
terp
ret m
edic
al
evid
ence
in a
crit
ical
and
sci
entif
ic m
anne
r.
2. T
he s
tude
nt h
as th
e ab
ility
to u
nder
stan
d th
e ep
idem
iolo
gy
of d
isea
se in
diff
erin
g po
pula
tions
an
d ge
ogra
phic
loca
tions
.
1.
Inte
rpre
ts m
edic
al e
vide
nce
in a
crit
ical
and
sc
ient
ific
man
ner.
2.
Und
erst
ands
how
dis
ease
affe
cts
diffe
ring
popu
latio
ns a
nd g
eogr
aphi
c lo
catio
ns.
3.
A
pplie
s ep
idem
iolo
gica
l dat
a in
man
agin
g th
e he
alth
of p
atie
nts
and
thei
r co
mm
uniti
es.

Attr
ibut
e 34
& 3
5
App
endi
x F
Med
ical
Dea
ns’ C
ompe
tenc
ies
Pro
ject
Fin
al R
epor
t
F
ebru
ary
2011
Attr
ibut
e
Stu
dent
Lea
rnin
g O
utco
me
s C
ompe
tenc
ies
(3
4) A
n ap
prec
iatio
n of
the
resp
onsi
bilit
y to
m
aint
ain
stan
dard
s of
med
ical
pra
ctic
e at
the
high
est p
ossi
ble
leve
l thr
ough
out a
pro
fess
iona
l ca
reer
.
1. T
he s
tude
nt h
as th
e ab
ility
to ta
ke r
espo
nsib
ility
to
mai
ntai
n st
anda
rds
of m
edic
al p
ract
ice
at th
e hi
ghes
t pos
sibl
e le
vel.
1.
Dem
onst
rate
s m
aint
enan
ce o
f hig
hest
pr
ofes
sion
al s
tand
ards
of m
edic
al p
ract
ice.
2.
D
emon
stra
tes
self
dire
cted
lear
ning
.
3.
Rec
ogni
ses
and
artic
ulat
es le
arni
ng g
oals
ar
isin
g fr
om c
linic
al s
cena
rios.
4.
Iden
tifie
s le
arni
ng a
ctiv
ities
that
will
ena
ble
him
/her
to a
ddre
ss le
arni
ng g
oals
. 5.
U
nder
take
s ap
prop
riate
lear
ning
act
iviti
es.
6.
See
ks fe
edba
ck fr
om p
eers
, tut
ors,
pat
ient
s an
d co
lleag
ues.
A
ttrib
ute
S
tude
nt L
earn
ing
Out
com
es
Com
pete
ncie
s
(35)
An
appr
ecia
tion
of th
e re
spon
sibi
lity
to
cont
ribut
e to
war
ds th
e ge
nera
tion
of k
now
ledg
e an
d th
e pr
ofes
sion
al e
duca
tion
of ju
nior
co
lleag
ues.
1. T
he s
tude
nt h
as th
e ab
ility
to c
ontr
ibut
e to
war
ds
the
gene
ratio
n of
kno
wle
dge.
2.
The
stu
dent
has
the
abili
ty to
con
trib
ute
tow
ards
th
e pr
ofes
sion
al e
duca
tion
of ju
nior
col
leag
ues.
1.
Par
ticip
ates
effe
ctiv
ely
in r
esea
rch
activ
ities
.
2.
Und
erta
kes
teac
hing
, inc
ludi
ng d
evel
opm
ent
of te
achi
ng s
kills
as
part
of p
rofe
ssio
nal
deve
lopm
ent.
3.
C
ontr
ibut
es to
the
prof
essi
onal
edu
catio
n of
pe
ers
and
juni
or c
olle
ague
s.

Diagnostic Procedures Appendix F
Medical Deans’ Competencies Project Final Report February 2011
Appendix A: List of Common Diagnostic Procedures as relates to Attribute 18 The student has the ability to interpret or understands:
• Electrocardiograms • Chest X-rays • Spiral CT • MRI • Ultrasound • Full Blood Counts, including liver function tests, urea, creatine and cardiac enzymes • Endocrine function tests including thyroid functioning, plasma glucose, urine albumin and
excretion rate in diabetics, serum cortisol, and serum parathyroid levels. • Observes endoscopic procedures including Upper GI, lower GI, colonoscopy and ERCP
procedures. • Interpretation of plain films, CT, Ultrasound and MRI with common medical surgical, obstetric,
gynaecological and paediatric conditions • Interpretation of doppler and duplex scans • Common haematology, biochemistry and microbiology tests • CT scanning, broncoscopy, fine needle aspiration biopsy, pleural tap and thoracoscopic
biopsy • Angiography • Blood gas measurements
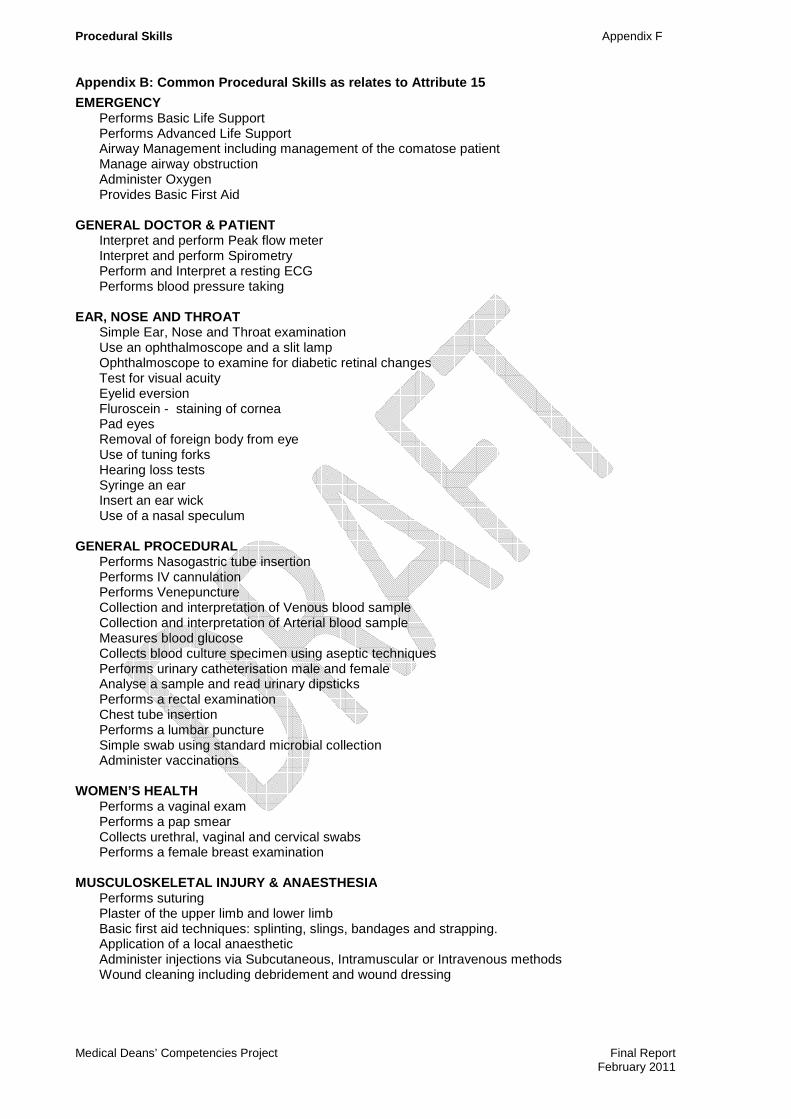
Procedural Skills Appendix F
Medical Deans’ Competencies Project Final Report February 2011
Appendix B: Common Procedural Skills as relates to Attribute 15
EMERGENCY Performs Basic Life Support Performs Advanced Life Support Airway Management including management of the comatose patient Manage airway obstruction Administer Oxygen Provides Basic First Aid
GENERAL DOCTOR & PATIENT Interpret and perform Peak flow meter Interpret and perform Spirometry Perform and Interpret a resting ECG Performs blood pressure taking
EAR, NOSE AND THROAT Simple Ear, Nose and Throat examination Use an ophthalmoscope and a slit lamp Ophthalmoscope to examine for diabetic retinal changes Test for visual acuity Eyelid eversion Fluroscein - staining of cornea Pad eyes Removal of foreign body from eye Use of tuning forks Hearing loss tests Syringe an ear Insert an ear wick Use of a nasal speculum
GENERAL PROCEDURAL Performs Nasogastric tube insertion Performs IV cannulation Performs Venepuncture Collection and interpretation of Venous blood sample Collection and interpretation of Arterial blood sample Measures blood glucose Collects blood culture specimen using aseptic techniques Performs urinary catheterisation male and female Analyse a sample and read urinary dipsticks Performs a rectal examination Chest tube insertion Performs a lumbar puncture Simple swab using standard microbial collection Administer vaccinations
WOMEN’S HEALTH Performs a vaginal exam Performs a pap smear Collects urethral, vaginal and cervical swabs Performs a female breast examination
MUSCULOSKELETAL INJURY & ANAESTHESIA Performs suturing Plaster of the upper limb and lower limb Basic first aid techniques: splinting, slings, bandages and strapping. Application of a local anaesthetic Administer injections via Subcutaneous, Intramuscular or Intravenous methods Wound cleaning including debridement and wound dressing

Phone +61 2 9036 3363 Phone +61 2 9114 1680 Fax +61 2 9114 1722 Email [email protected] Level 6, 173 – 175 Phillip Street, Sydney NSW 2000
24 January 2011 To whom it concerns,
Endorsement of Medical Deans’ Competencies Project: Framework of Competencies for Graduate Outcomes which rely on clinical placements .
Medical Deans Australia and New Zealand Inc (Medical Deans) has undertaken a project, with funding from the Australian Government’s Department of Health and Ageing, to develop a framework of competencies for medical graduate outcomes which rely on clinical placements. The has project aimed to provide some precision around the purpose and content of clinical training in order to assist the continuing significant pressures on educational bodies and the Australian health system to be able to provide a sufficient number of high quality clinical training placements for the increased number of medical students. The Competencies Project has generated significant stakeholder interest and buy in throughout the project period. The project has achieved endorsement from a broad range of medical education groups, Medical Schools and the Deans. In particular, the Framework has achieved solid endorsement from Deans of Medical Schools with the project being acknowledged as beneficial for aiming to define graduate outcomes from clinical placements. Medical Deans endorses the Framework of Competencies for Graduate Outcomes which rely on Clinical Placements and supports further work developing the framework. Medical Deans looks forward to continuing the work of the Competencies Project in consultation with our stakeholders. Kind regards,
Professor James Angus President