desulfovibrio legallii prosthetic shoulder joint infection and a
TRANSCRIPT

Desulfovibrio legallii Prosthetic Shoulder Joint Infection and a Review of Antimicrobial 1
Susceptibility and Clinical Characteristics of Desulfovibrio Infections 2
Shawn Vasoo,1* Erin L Mason,1 Daniel R Gustafson,2 Scott A Cunningham,2 3
Nicolynn C Cole,2 Emily A Vetter,2 Scott P Steinmann,3 Walter R Wilson,1 4
Robin Patel,1,2 Elie F Berbari,1 Nancy K Henry1,4 5
1Division of Infectious Diseases, Department of Medicine, 6
2Division of Clinical Microbiology, Department of Laboratory Medicine and Pathology, 7
3Department of Orthopedic Surgery, 8
4Division of Pediatric Infectious Diseases, Department of Pediatric and Adolescent Medicine, 9
Mayo Clinic, Rochester, Minnesota 10
Keywords: Desulfovibrio, prosthetic joint infection, antimicrobial susceptibility 11
*Correspondence/Reprint Requests to: 12
Shawn Vasoo, MRCP 13
Division of Infectious Diseases 14
Mayo Clinic 15
200 First St S.W. 16
Rochester, MN 55905, USA 17
Phone: (507) 255-1980 18
Fax: (507) 255-7134 19
Email: [email protected] 20
JCM Accepts, published online ahead of print on 21 May 2014J. Clin. Microbiol. doi:10.1128/JCM.00083-14Copyright © 2014, American Society for Microbiology. All Rights Reserved.
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

2
Alternate corresponding author : 21
Nancy Henry, MD, PhD 22
Division of Infectious Diseases 23
Mayo Clinic 24
200 First St S.W. 25
Rochester, MN 55905, USA 26
Phone: (507) 255-8464 27
Fax: (507) 255-7134 28
Email: [email protected] 29
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

3
Abstract 30
We describe a case of shoulder hemiarthroplasty infection with Desulfovibrio legallii. 31
Antimicrobial susceptibilities of 36 Desulfovibrio isolates are presented. Metronidazole and 32
carbapenems exhibited reliable activity, although piperacillin-tazobactam did not. Eleven 33
previous cases of Desulfovibrio infection are reviewed; most arose from a gastrointestinal tract-34
related source. 35
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

4
Case report 36
In July 2013, a 70 year-old woman with a 10 year history of planto-palmar psoriasis, presented 37
to our institution with a six-month history of intermittent fever, chills and left shoulder pain. This 38
had worsened over the preceding two weeks and she had developed diminished range of 39
movement of her left shoulder. She had sustained a closed proximal humerus fracture which 40
had been treated with a humeral endoprosthesis implanted eighteen years prior to presentation. 41
For about eight years through August 2012, she had received treatment for psoriasis with twice 42
yearly intramuscular injections of 80 mg triamcinolone. In August 2012, she was placed on 43
topical treatment and phototherapy. In attempt to improve her psoriasis, the patient reported 44
soaking her hands and feet, which had many fissures and cracks, in Lake Superior and in the 45
Pacific Ocean. Physical examination revealed a well-healed surgical scar over her left shoulder 46
and a scant amount of swelling in the lower axilla. She had an elevated white cell count of 16 x 47
109/L, erythrocyte sedimentation rate of 35 mm/h (normal, 0-29 mm/h) and C-reactive protein of 48
204.3 mg/L (normal, <8 mg/L). An indium111 bone scan showed asymmetric uptake around her 49
left shoulder suggestive of periprosthetic infection. Cell count on the aspirated shoulder joint 50
fluid was 25,075 white blood cells/μL with 99% neutrophils. Cultures of the aspirated joint fluid 51
yielded moderate growth of small, pinpoint, clear colonies on CDC anaerobic sheep blood agar 52
after six days of anaerobic incubation at 35oC (Figure 1a); broth cultures were negative. The 53
colonies measured about 1 mm in diameter, and were grey-green and convex after 10 days of 54
incubation (Figure 1b). Gram stain showed spiral-appearing Gram negative bacilli (Figure 1c) 55
which were motile, indole negative and catalase positive with 15% H2O2. PrepMan Ultra (Life 56
Technologies, Grand Island, NY) was used to prepare DNA for partial 16S rRNA gene PCR 57
using primers 5′-TGGAGAGTTTGATCCTGGCTCAG-3′ and 5′-TACCGCGGCTGCTGGCAC-3′ 58
with bidirectional amplification product sequencing performed using the same primers. A 496 bp 59
sequence was generated revealing 100% identity to Desulfovibrio legallii (Strain H1) (base pairs 60
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

5
4 to 499 of GenBank accession number FJ225426) (1, 2). Per our laboratory protocol, for 61
species identification, a >99% agreement with a database strain with >0.8% separation from 62
other species is required. The next best matches were Desulfovibrio sp. canine oral taxon 070 63
clone 1P043 (GenBank accession number JQ295257) (96% match), and Desulfovibrio sp. 64
Canine oral taxon 070 clone 1J008 (GenBank accession number JQ294906) (95% match). 65
Drawing from observations that growth enhancement of sulfate-reducing organisms is enhanced 66
by the addition of magnesium sulfate to broth media (3), we also noted that colony robustness 67
on CDC anaerobic sheep blood agar was enhanced with supplementation with 250 μl of 10% 68
magnesium sulfate. This isolate did not yield a genus- or species-level identification when 69
subjected to matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI 70
TOF MS) using the Bruker MALDI Biotyper (Bruker Daltonics, Billerica, MA), with spectra 71
analyzed by the Bruker Biotyper 3.0 software and library version 3.3.1.0 (4,613 entries); the top 72
match was Clostridium novyi (score 1.457). The library used only contained a single 73
Desulfovibrio entry, for Desulfovibrio fairfieldensis. 74
The isolate was β-lactamase negative (cefinase disc, Becton Dickinson, Franklin Lakes, NJ). 75
Susceptibility testing by E-test methodology (AB Disk, Sweden) showed a penicillin MIC of 1 76
μg/ml (intermediate), and a clindamycin and metronidazole MIC of <0.5 μg/ml to both 77
(susceptible) (Table 1). The patient underwent resection shoulder arthroplasty. Purulent fluid 78
was encountered intraoperatively (Figure 1d). Histopathology of periprosthetic soft tissue 79
revealed fibrovascular tissue with marked acute and chronic inflammation; operative cultures 80
yielded D. legallii from three synovial fluid and five tissue specimens as well as prosthetic joint 81
culture using vortexing/sonication (>100 CFU/10ml sonicate fluid) ( 4, 5). The isolate obtained 82
from sonication cultures had an identical susceptibility pattern to the pre-operative isolate 83
cultured from synovial fluid, except for the penicillin MIC which was 2 μg/ml. Additional testing 84
showed that it had the following MICs by E-test: ertapenem, 1 μg/ml; ceftriaxone, 2 μg/ml; 85
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

6
amoxicillin-clavulanate, 0.25/0.125 μg/ml; piperacilin/tazobactam, >256/4 μg/ml; minocycline, 86
0.5 μg/ml; ciprofloxacin > 32 μg/ml. The patient underwent débridement two weeks after her 87
initial surgery because of persistent drainage from the wound; no deep infection was noted. 88
Cultures from this débridement yielded single colonies of Staphylococcus capitis and Candida 89
glabrata from one of four tissues, results which were considered indicative of contamination. 90
She was treated with six weeks of ertapenem followed by re-implantation with a reverse total 91
shoulder arthroplasty, seven weeks after the resection surgery. At a six months post re-92
implantation, the patient remains well. 93
Desulfovibrio species are non-spore forming, non-fermentative, sulfate reducing, anaerobic 94
Gram negative bacilli. Most are motile with polar flagella and are curved or spiral-shaped. The 95
type species, D. desulfiricans (formerly Spirillum desulfiricans) was described by the Dutch 96
microbiologist Beijerinck in 1895 (6). Since then, 67 species (not including subspecies) have 97
been described (7). They are found in anaerobic niches, including marine, brackish, fresh, and 98
waste water, and are important ecologically for both their harm (e.g., corrosion of steel) and 99
benefits (e.g., as bioremediators) resulting from their unique metabolic pathways (8). 100
Desulfovibrio sp. are part of the oral and gastrointestinal flora of humans and animals (9,10), 101
and the vaginal flora of humans (11). A role for Desulfovibrio sp. in inflammatory bowel disease 102
(12) and acute periodontitis (13) has been suggested; however, reported cases of human 103
infection have been infrequent. This may be due to under-recognition of these organisms which 104
are slow growing; they are often involved in polymicrobial infections and some clinical 105
laboratories may lack the ability to identify them. Most infections have arisen from an abdominal 106
source, although a case of polymicrobial brain abscess has been reported which was ascribed 107
to an odontogenic or sinus source (14). 108
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

7
Since the last review of human Desulfovibrio infections from 1977 to 2003 (15), five additional 109
cases of human Desulfovibrio infection have been reported, including three cases of D. 110
fairfieldensis infection (16-18) and two of D. desulfuricans bacteremia (19, 20). All were 111
associated with a gastrointestinal-related source [one case each of gastroenteritis (17), sigmoid 112
diverticulitis (18), and cytomegalovirus colitis (20)]; one case arose following endoscopic 113
retrograde cholangiopancreatography for choledocholithiasis (16), and another from an infected 114
sacral decubitus ulcer in a bedridden patient (19). Warren and Goldstein also described the 115
phenotypic characteristics of 17 human Desulfovibrio isolates (21). These included 15 isolates 116
from intra-abdominal sources (two D. piger, nine D. fairfieldensis, two D. desulfuricans, and two 117
D. vulgaris) and two from blood cultures (one each of D. fairfieldensis and D. desulfuricans). 118
We report an unusual case of a prosthetic joint infection with a novel Desulfovibrio species, D. 119
legallii, and describe human Desulfovibrio isolates identified and subjected to antimicrobial 120
susceptibility testing in our clinical microbiology laboratory. This study was approved by our 121
Institutional Review Board (IRB 13-007249). 122
From 1997-2013, there were thirteen Desulfovibrio isolates from Mayo Clinic patients inclusive 123
of two isolates from the case reported herein (Table 2), and 54 isolates referred to us for 124
identification and/or antimicrobial susceptibility testing (AST), which was performed using the E-125
test, on Brucella blood agar. Isolates were all identified by 16S ribosomal RNA gene sequencing. 126
AST was performed on ten of the Mayo Clinic isolates, and 26 of the referred isolates (Table 1). 127
D. desulfuricans was the most common species (61%) in our study, in contrast to findings by 128
Lobinoux et al. who reported D. piger to be the most common species in 100 consecutive 129
specimens obtained from thoracoabdominal purulent material (22). In our series, Desulfovibrio 130
sp. were most often from blood cultures (87%), followed by abdominal sources (7.5%). 131
Desulfovibrio infections occurred in patients with a median age of 74 years (range 6-93 years), 132
with males comprising 65% of cases. 133
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

8
In the Mayo Clinic series of 12 patients, two-thirds of the isolates were from blood. All but one 134
involved patient had a gastrointestinal portal of infection, the exception being the patient with D. 135
legallii prosthetic joint infection described herein. We hypothesize that this patient, who had 136
been previously immunosuppressed with high dose corticosteroids, and who did not have any 137
symptoms or history referable to the gastrointestinal tract, may have acquired the organism 138
exogenously through water exposure, with D. legallii entering through breaks in her psoriatic 139
skin, and seeding her prosthetic joint. 140
Our report expands on the species which may cause human infections – D. legallii, which is a 141
novel species first described in a Tunisian wastewater digester in 2011 (1), and also two cases 142
D. intestinalis bacteremia. Interestingly, D. intestinalis which was first described in termite 143
hindguts (23), was recently described as part of vaginal flora in 3% of women in a Japanese 144
study (11). Unfortunately, we do not have clinical information on the two referred cases of D. 145
intestinalis bacteremia. There were two isolates each of D. fairfieldensis and D. piger, with one 146
of the D. piger isolates originating from our institution. D. fairfieldensis and D. piger have so far 147
only been described as human-related bacteria (24). 148
Our results corroborate previous reports showing that Desulfovibrio sp. are predictably 149
susceptible to metronidazole, but that piperacillin-tazobactam, which is commonly used to treat 150
anaerobic infections, is not reliably active. Regarding carbapenems, 23 isolates were tested in 151
our study; ertapenem and/or imipenem were uniformly active. However discrepant 152
susceptibilities to carbapenems have been reported (17), so we suggest that AST be performed 153
for the specific carbapenem used for treatment, particularly for isolates from sterile sources. 154
Although AST was not performed on the two referred D. fairfieldensis isolates, this species has 155
been associated with antimicrobial resistance, including resistance to ertapenem/meropenem 156
(17, 21). D. fairfieldensis may be more virulent than other species given reports of invasive 157
infections (16, 25), however, putative virulence factors remain to be elucidated. Based our 158
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

9
series, however, it appears that D. desulfuricans is the species most commonly associated with 159
bacteremia and other sites of infection in humans. 160
Anaerobes are an uncommon cause of prosthetic joint infection (26), and Desulfovibrio sp. as a 161
genus have been reported infrequently as causes of human infection. However, as illustrated by 162
this case of D. legallii prosthetic joint infection, such infections may occur in a susceptible host 163
with risk factors. It is likely that with more widespread use of technologies such as sequencing 164
and MALDI TOF MS in the clinical laboratory (27), these types of organisms will be more readily 165
identified, providing further insight into the role of Desulfovibrio sp. in human disease. 166
167
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
10
Acknowledgements 168
We would like to thank Dr. Bobbi S. Pritt for her assistance with the photomicrograph of the 169
Gram stain of the D. legallii isolate and the outstanding technologists of the Mayo Clinic 170
bacteriology laboratory for their work with the isolates described herein. 171
Funding 172
Dr. Patel is supported by research grants from the National Institutes of Health (R01 AR056647 173
and R01 AI91594). 174
This study was presented in part at the114th General Meeting of the American Society of 175
Microbiology, Boston, MA, May 17 – 20, 2014.176
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

11
References 177
1. Thabet OB, Wafa T, Eltaief K, Cayol JL, Hamdi M, Fauque G, Fardeau ML. 2011. 178
Desulfovibrio legallis sp. nov.: a moderately halophilic, sulfate-reducing bacterium 179
isolated from a wastewater digestor in Tunisia. Curr Microbiol 62:486-491. 180
2. Euzéby J. 2013. List of new names and new combinations previously effectively, but not 181
validly, published. Int J Syst Evol Microbiol 63:1-5 182
3. Jouseimies-Somer HR, Summanen P, Citron DM, Baron EJ, Wexler HM, Finegold 183
SM. 2002. Appendix D, p. 220-221. In Wadsworth-Ktl Anaerobic Bacteriology Manual, 184
6th ed. Star Publishing Company, Belmont, Calif. 185
4. Piper KE, Jacobson MJ, Cofield RH, Sperling JW, Sanchez-Sotelo J, Osmon DR, 186
McDowell A, Patrick S, Steckelberg JM, Mandrekar JN, Fernandez Sampedro M, 187
Patel R. 2009. Microbiologic diagnosis of prosthetic shoulder infection by use of implant 188
sonication. J Clin Microbiol 47:1878-1884. 189
5. Trampuz A, Piper KE, Jacobson MJ, Hanssen AD, Unni KK, Osmon DR, Mandrekar 190
JN, Cockerill FR, Steckelberg JM, Greenleaf JF, Patel R. 2007. Sonication of 191
removed hip and knee prostheses for diagnosis of infection. N Engl J Med 357:654-663. 192
6. Beijerinck, WM. 1895. Ueber Spirillum desulfurcans als Ursache von Sulfatreduction. 193
Centralbl.Bakteriol. II. Abt. 1:1-9, 49-59, 104-114. 194
7. Leibniz-Institut DSMZ - Deutsche Sammlung von Mikroorganismen und 195
Zellkulturen GmbH. Prokaryotic Nomenclature Up-to-Date. Desulfurovibrio. 2013. 196
http://www.dsmz.de/bacterial-diversity/prokaryotic-nomenclature-up-to-date/prokariotic-197
nomenclature-up-to-date.html (Accessed 11 Nov 2013). 198
8. Butlin KR, Adams ME, Thomas M. 1949. The isolation and cultivation of sulphate-199
reducing bacteria. J Gen Microbiol 3:46-59. 200
9. Beerens H, Romond C. 1977. Sulfate-reducing anaerobic bacteria in human feces. Am 201
J Clin Nutr 30:1770-1776. 202
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

12
10. Nakao K, Tanaka K, Ichiishi S, Mikamo H, Shibata T, Watanabe K. 2009. 203
Susceptibilities of 23 Desulfovibrio isolates from humans. Antimicrob Agents Chemother 204
53:5308-5311. 205
11. Ichiishi S, Tanaka K, Nakao K, Izumi K, Mikamo H, Watanabe K. 2010. First isolation 206
of Desulfovibrio from the human vaginal flora. Anaerobe 16:229-233. 207
12. Rowan F, Docherty NG, Murphy M, Murphy B, Calvin Coffey J, O'Connell PR. 2010. 208
Desulfovibrio bacterial species are increased in ulcerative colitis. Dis Colon Rectum 209
53:1530-1536. 210
13. Loubinoux J, Bisson-Boutelliez C, Miller N, Le Faou AE. 2002. Isolation of the 211
provisionally named Desulfovibrio fairfieldensis from human periodontal pockets. Oral 212
Microbiol Immunol 17:321-323. 213
14. Lozniewski A, Maurer P, Schuhmacher H, Carlier JP, Mory F. 1999. First isolation of 214
Desulfovibrio species as part of a polymicrobial infection from a brain abscess. Eur J 215
Clin Microbiol Infect Dis 18:602-603. 216
15. Goldstein EJ, Citron DM, Peraino VA, Cross SA. 2003. Desulfovibrio desulfuricans 217
bacteremia and review of human Desulfovibrio infections. J Clin Microbiol 41:2752-2754. 218
16. Pimentel JD, Chan RC. 2007. Desulfovibrio fairfieldensis bacteremia associated with 219
choledocholithiasis and endoscopic retrograde cholangiopancreatography. J Clin 220
Microbiol 45:2747-2750. 221
17. Urata T, Kikuchi M, Hino T, Yoda Y, Tamai K, Kodaira Y, Hitomi S. 2008. Bacteremia 222
caused by Desulfovibrio fairfieldensis. J Infect Chemother 14:368-370. 223
18. Gaillard T, Pons S, Darles C, Beausset O, Monchal T, Brisou P. 2011. [Desulfovibrio 224
fairfieldensis bacteremia associated with acute sigmoiditis]. Med Mal Infect 41:267-268. 225
19. Liderot K, Larsson M, Borang S, Ozenci V. 2010. Polymicrobial bloodstream infection 226
with Eggerthella lenta and Desulfovibrio desulfuricans. J Clin Microbiol 48:3810-3812. 227
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

13
20. Verstreken I, Laleman W, Wauters G, Verhaegen J. 2012. Desulfovibrio desulfuricans 228
bacteremia in an immunocompromised host with a liver graft and ulcerative colitis. J Clin 229
Microbiol 50:199-201. 230
21. Warren YA, Citron DM, Merriam CV, Goldstein EJ. 2005. Biochemical differentiation 231
and comparison of Desulfovibrio species and other phenotypically similar genera. J Clin 232
Microbiol 43:4041-4045. 233
22. Loubinoux J, Jaulhac B, Piemont Y, Monteil H, Le Faou AE. 2003. Isolation of 234
sulfate-reducing bacteria from human thoracoabdominal pus. J Clin Microbiol 41:1304-235
1306. 236
23. Frohlich J, Sass H, Babenzien HD, Kuhnigk T, Varma A, Saxena S, Nalepa C, 237
Pfeiffer P, Konig H. 1999. Isolation of Desulfovibrio intestinalis sp. nov. from the hindgut 238
of the lower termite Mastotermes darwiniensis. Can J Microbiol 45:145-152. 239
24. Loubinoux J, Valente FM, Pereira IA, Costa A, Grimont PA, Le Faou AE. 2002. 240
Reclassification of the only species of the genus Desulfomonas, Desulfomonas pigra, as 241
Desulfovibrio piger comb. nov. Int J Syst Evol Microbiol 52:1305-1308. 242
25. Loubinoux J, Mory F, Pereira IA, Le Faou AE. 2000. Bacteremia caused by a strain of 243
Desulfovibrio related to the provisionally named Desulfovibrio fairfieldensis. J Clin 244
Microbiol 38:931-934. 245
26. Berbari EF, Hanssen AD, Duffy MC, Steckelberg JM, Ilstrup DM, Harmsen WS, 246
Osmon DR. 1998. Risk factors for prosthetic joint infection: case-control study. Clin 247
Infect Dis 27:1247-1254. 248
27. Schmitt BH, Cunningham SA, Dailey AL, Gustafson DR, Patel R. 2013. Identification 249
of anaerobic bacteria by Bruker Biotyper matrix-assisted laser desorption ionization-time 250
of flight mass spectrometry with on-plate formic acid preparation. J Clin Microbiol 251
51:782-786. 252
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

Table 1 Desulfovibrio isolates evaluated in the Mayo Clinic Clinical Microbiology
Laboratory, 1997-2013
Species [total no. isolates from 1997-2013] and antimicrobial (no. tested)a
MIC (μg/ml) Susceptible, no. (%), of isolates testede
Range MIC50
MIC90
Desulfovibrio sp. [18]b,c Clindamycin (8) <0.5 - 1 <0.5 <0.5 8 (100%)
Penicillin (9) <0.5 - 32 8 8 2 (22%) Ampicillin-sulbactam (3) <0.5-0.5 - - 3(100%)
Piperacillin-tazobactam (1) >256/4 - - 0 (0%) Ertapenem (1) <0.5 - - 1 (100%) Imipenem (3) <0.5-0.5 - - 3 (100%)
Metronidazole (9) <0.5 <0.5 <0.5 9 (100%) D. desulfuricans [40]b,d
Clindamycin (21) <0.5 - >256 <0.5 1 20 (95%) Penicillin (22) <0.5-16 4 16 3 (14%)
Piperacillin-tazobactam (15) 32/4 ->256/4 128/4 >256/4 2 (13%) Ertapenem (15) <0.5 – 1 <0.5 0.5 15 (100%)
Imipenem (2) <0.5 - 1 - - 2 (100%) Metronidazole (23) <0.5 <0.5 <0.5 23 (100%)
D. fairfieldensis [2]b - - - - D. intestinalis [2]b
Clindamycin (1) <0.5 - - 1 (100%) Penicillin (1) 2 - - 0 (0%)
Piperacillin-tazobactam (1) 32/4 - - 1 (100%) Ertapenem (1) <0.5 - - 1 (100%)
Metronidazole (1) <0.5 - - 1 (100%) D. legallii [2]b
Clindamycin (2) <0.5 - - 2 (100%) Penicillin (2) 1-2 - - 0 (0%)
Amoxicillin-clavunalate (1) 0.25/0.125 - - 1 (100%) Piperacillin-tazobactam (1) >256/4 - - 0 (0%)
Ceftriaxone (1) 2 - - 1 (100%) Ertapenem (1) 1 - - 1 (100%)
Ciprofloxacin (1) >32 - Minocycline (1) 0.5 - - -
Metronidazole (2) <0.5 - - 2 (100%) D. piger [3]b
Clindamycin (1) <0.5 - - 1 (100%) Penicillin (1) 8 - - 0 (0%)
Metronidazole (1) <0.5 - - 1 (100%) aNot all isolates were tested for antimicrobial susceptibility. The numbers in square brackets indicate the number of isolates isolated in our laboratory or submitted to our laboratory for identification; the numbers in round brackets indicate the number of isolates which underwent antimicrobial susceptibility testing. All isolates were from unique patients, with the exception of the two D. legallii isolates which came from the same patient (as presented in this report). Susceptibility testing was performed via the E-test methodology (AB Biodisk). bSources of isolates: 18 Desulfovibrio isolates: Blood (17), abdominal (1); 40 D. desulfuricans isolates: Blood (35), abdominal (3), spine (1), urine (1); 2 D. fairfieldensis isolates: Blood (2) ; 2 D. intestinalis isolates: Blood (2); 2 D. legallii isolates (from the same patient, as reported in this paper): Synovial fluid (1), prosthetic joint (1); 3 D. piger isolates: Blood (2), abdominal (1). cThere was no species identification for these 18 isolates as they did not meet criteria for speciation by 16S rRNA gene sequencing. dOf 35 isolates tested for β-lactamase production (8 Desulfovibrio sp., 21 D. desulfuricans, 1 D. intestinalis, 2 D. legallii, 3 D. piger), only 1 D. desulfuricans isolate tested positive by the cefinase disk test. eInterpretive criteria per CLSI Document M100-S24 (Susceptible = S, Intermediate = I, Resistant = R, numbers refer to MIC in μg/ml): Amoxicillin/clavunalate (S <4/2; I 8/4; R > 16/8); ceftriaxone (S < 16; I 32; R >64); clindamycin (S < 2; I 4; R > 8), ertapenem (S <4; I 8; R > 16); imipenem (S <4; I 8; R > 16); metronidazole (S < 8; I 16; R >32); penicillin (S<0.5; I 1; R >2); piperacillin/tazobactam (S <32/4; I 64/4; R>128/4). There are no CLSI interpretive criteria for ciprofloxacin or minocycline.
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

Table 2. Twelve cases of Desulfovibrio infection from 1997-2013, Mayo Clinic, Rochester, Minnesota Case Year Genus/Species Source Antimicrobial susceptibilitya Co-isolated
organismsb Age (years) / Genderc
Diagnosis Outcome Susceptible Intermediate/
Resistant 1 2013
(this report)
Desulfovibrio legallii
Synovial fluid, prosthetic joint, and periprosthetic tissue
CLI, MTZ, ETP
PCN - 70/F Left shoulder prosthetic joint infection
Recovered
2 2012 D. desulfuricans Urine from percutaneous nephrostomy
CLI, MTZ, PCN
- Anaerobic gram positive bacilli, anaerobic Gram positive cocci, Streptococcus agalactiae, Actinobaculum schaalii Propionimicrobium sp.
66/F Bilateral hydronephrosis with right emphysematous pyelitis, suspected colo-ureteral/vesical fistula, herpes encephalitis
Died, secondary to herpes encephalitis
3 2012 D. desulfuricans Blood (positive at 76 hours)
MTZ PCN - 76/M Bacteremia presumed secondary to diverticulitis
Recovered
4 2011 D. desulfuricans Spine tissue CLI, MTZ, PCN
- Mobiluncus curtisii, Candida albicans, Clostridium clostridioforme
60/M Colonic rupture with colonic-dural fistula, Metastatic renal cell carcinoma; cervical, thoracic and lumbar spinal instrumentation, for bone metastases
Died
5 2008 D. piger Blood (positive at 44 hours)
CLI, MTZ PCN Ergerthella lenta, Bacteroides ovatus
73/F Bacteremia secondary to pericolonic abscess, Sigmoid diverticulitis
Recovered
6 2005 D. desulfuricans Blood (positive at 3 days)
CLI, MTZ PTZ, ETP
PCN - 74/F Bacteremia secondary to presumed gastrointestinal translocation, Transient, post-operative small bowel obstruction complicating transverse colectomy for colon cancer
Recovered
7 2005 D. desulfuricans Blood (positive at 4 days)
CLI, MTZ AMS, ETP
PCN In peritoneal fluid: Escherichia coli, Klebsiella pneumoniae, anaerobic Gram negative and positive rods
57/M Perforated acute appendicitis, HIV infectiond
Recovered
8 2004 Desulfovibrio sp.
Blood (positive at 3 days)
CLI, MTZ PCN E. lenta, anaerobic Gram negative rod, Bacteroides fragilis
60/M Perforated acute appendicitis
Recovered
9 2002 Desulfovibrio sp.
Blood (positive at 5 days)
- - Candida parapsilosis 74/M Septic shock, complicated intra-abdominal infection post aortic aneurysm repair
Died
10 2000 Desulfovibrio sp.
Blood (positive at 5 days)
- - In subphrenic abscess: vancomycin resistant enterococci
45/M Subphrenic abscess/right empyema, complicated intra-abdominal infection following surgery for diverticulitis
Recovered
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
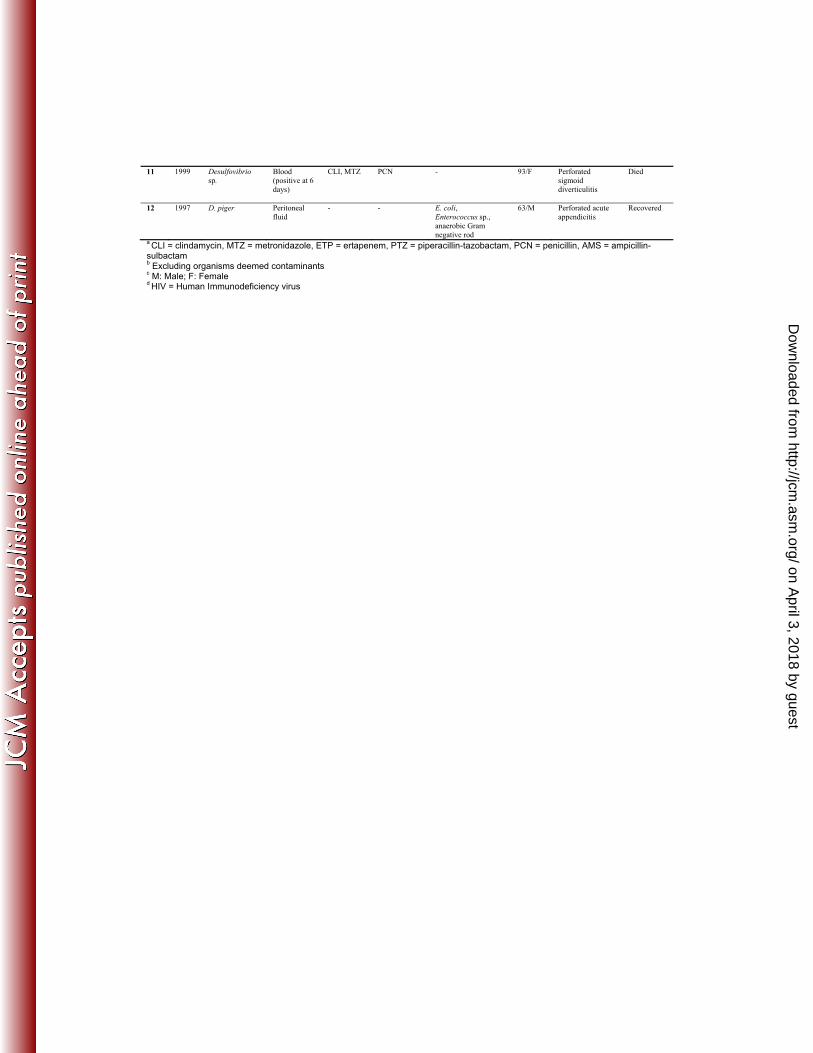
11 1999 Desulfovibrio sp.
Blood (positive at 6 days)
CLI, MTZ PCN - 93/F Perforated sigmoid diverticulitis
Died
12 1997 D. piger Peritoneal fluid
- - E. coli, Enterococcus sp., anaerobic Gram negative rod
63/M Perforated acute appendicitis
Recovered
a CLI = clindamycin, MTZ = metronidazole, ETP = ertapenem, PTZ = piperacillin-tazobactam, PCN = penicillin, AMS = ampicillin-sulbactam b Excluding organisms deemed contaminants c M: Male; F: Female d HIV = Human Immunodeficiency virus
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
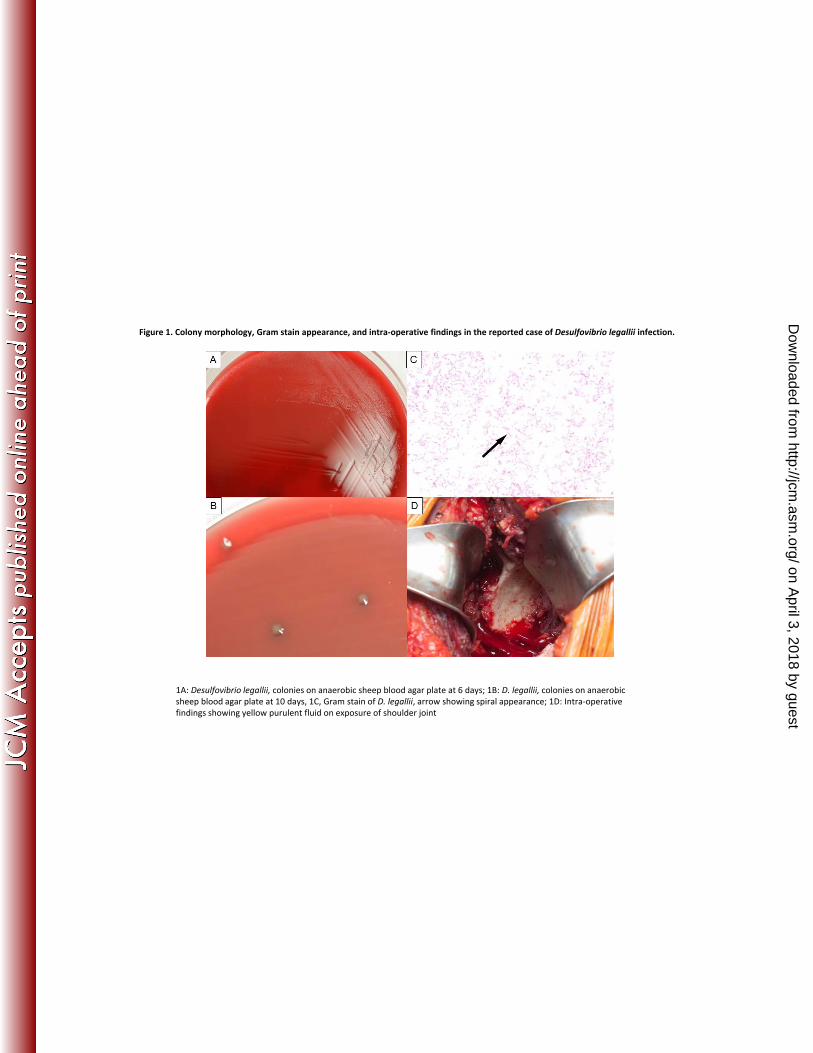
Figure 1. Colony morphology, Gram stain appearance, and intra-operative findings in the reported case of Desulfovibrio legallii infection.
1A: Desulfovibrio legallii colonies on anaerobic sheep blood agar plate at 6 days; 1B: D legallii colonies on anaerobic1A: Desulfovibrio legallii, colonies on anaerobic sheep blood agar plate at 6 days; 1B: D. legallii, colonies on anaerobic sheep blood agar plate at 10 days, 1C, Gram stain of D. legallii, arrow showing spiral appearance; 1D: Intra-operative findings showing yellow purulent fluid on exposure of shoulder joint
on April 3, 2018 by guest
http://jcm.asm
.org/D
ownloaded from