destination safe care transitions – staying on track hiloni bhavsar, md assistant professor,...
TRANSCRIPT

Destination Safe Care Transitions – Staying on TrackHiloni Bhavsar, MDAssistant Professor, General Internal MedicineUH Quality Institute LiaisonPhysician Informaticist, UHCare
Chrissie Blackburn, MHAPrincipal Advisor, Patient and Family EngagementUniversity Hospitals & UHCMCInstitute for Healthcare Quality and Innovation
Nancy DeSantisManager, Patient Access Services
Khaliah Fisher-Grace, MSN, RN, CPHQ, PCCNSenior Quality Improvement NurseInstitute for Healthcare Quality & InnovationUniversity Hospitals Case Medical Center
Stefan Gravenstein, MD, MPHProfessor of MedicineInterim Chief, Division of Geriatrics and Palliative CareCenter for Geriatrics and Palliative CareCase Medical Center
Mary Ann Gravenstein, MD
Faisal A. Khan, Esq.Assistant General Counsel
Jonathan S. Lever, MPH, NREMT-PSenior Clinical Data AnalystInstitute for Healthcare Quality & InnovationUniversity Hospitals Case Medical Center
Edmundo Mandac, MDDepartment of Emergency MedicineInterim Chair - UHCMC
Lee Manning Schoeppler, RN, MSN, MBA, NEA-BC Agency Administrator, Director of Clinical Integration University Hospitals Home Care & Hospice
George V. Topalsky MD, F.A.C.P.UH Internal Medicine CenterCo medical director Southwest RegionSite director UH Independance health center
Laura Wilson, BSN, RNClinical System Liaison, Electronic Medical Records (EMR)/ UHCareUH Conneaut Medical Center
Cynthia B.R.Zelis, MD, MBAVice President Clinical IntegrationUniversity Hospitals Cleveland
Corinne Hurley, RN, MSNDirector, Institute for HealthCare Quality and InnovationPhysician Office Based Care
Elizabeth Ingram BSClinical Application AnalystUHCare Ambulatory EMR

Disclosures
• Speakers in this presentation have no disclosures.

Objectives
• Identify and describe national and local best practices in transitions
of care through experts and patient perspective
• Understand the resources available within the UH system today
• Understand the implications of poor transitions of care on patient
experience, readmissions, and reimbursement
• Attendees will write an “I will…” statement at the end of the
presentation to apply one transition of care best practice to their
current workflow

Overview
• Background information on transitions of care
• Best practices
• Case: Dr. Mary Ann Gravenstein
• Workshop
• Large group discussion

Clinical Integration
“The Key to Health Care Reform”
-American Hospital Association, Feb 2010
“Clinical Integration is the extent to which patient care services
are coordinated across people, functions, activities, and sites
over time so as to maximize the value of services delivered to the
patient.”
-S Shortell, R Gilles, D. Anderson
- Remaking Health Care in America, 2000

Patient
Primary Care Provider
Laboratory
Specialty Providers
Radiology
Post Acute Care
Therapy
Home Health Care
Acute Care Hospitals
Emergency Dept.
Clinical Integration is a TEAM
EffortWHY CLINICAL INTEGRATION?
• Quality• Communication• Patient
Experience• Work Flow
Efficiency• Lower Litigation
Risk • Cost Reduction• System
Revenue

Transitions of Care: Potential Consequences
• Quality
• Communication
• Patient Experience
• Work Flow Efficiency
• Litigation Risk
• Readmission• Prolonged Length of
Stay• Duplication of tests• Inaccurate treatment
• Poor Patient Satisfaction• Decreased patient
loyalty• Increased work for staff• Incomplete
documentation• Risk of Joint Defense


ED/Urgent Care Best Practices: RECIPROCITY
Visit Timeline ED/UC/SNF/Hospital Best Practice Community Physician
At intake • Notify PCP about hospital utilization • Provide clinical info when referring patients for ED/UC evaluation
During visit • Invite PCP to participate in EOL discussions• Provide patient with effective education• Provide patient with written d/c instructions• Provide patient with f/u phone #• Perform medication reconciliation• Schedule outpatient f/u appointment
• Provide ED/UC/Hospital with phone access to outpatient staff who can answer clinical questions
• Provide ED/hospital with access to outpatient clinical info
At discharge • Provide PCP with hospital contact info• Provide PCP with summary clinical info
• Confirm receipt of hospital d/c info
After discharge
• F/U with high risk pts via phone• Conduct outpatient f/u• Perform outpatient med reconciliation
Communication of Key Info(Based on Evidence and local input)
Community Physician’s
Office
ED/UC/ SNF/Hospital

48-Hour Readmission Review Pilot (UH Case)
• 136 patient readmitted within 48 hours, November 2014 – March 2015
• 39 reviews completed
Measure % Yes
All-or-none and standard of care met 2.6
Notify community MD office about observation/admission 74.6
Provide receiving MDs with hospital clinicians contact info 58.5
Patient education prior to discharge 92.4
Written discharge instructions prior to discharge 87.9
Follow-up phone number prior to discharge 72.3
Medication reconciliation 95.4
Schedule follow-up appt 87.7
Provide PCP office with patient summary 75.4
PCP participated EOL discussions during visit 96.8EOL=end of life
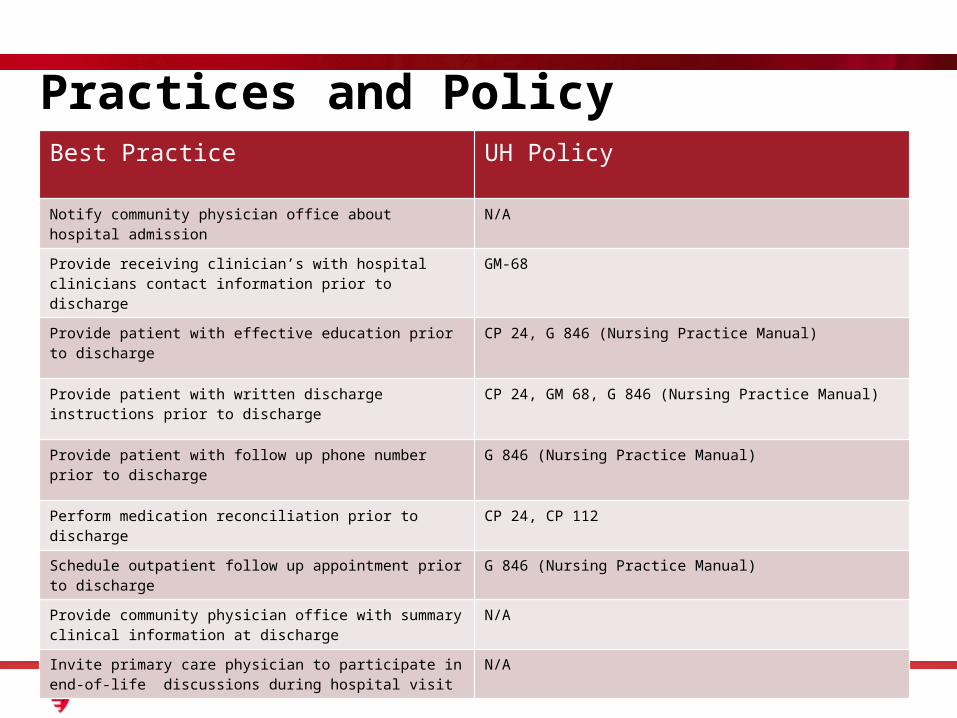
Practices and PolicyBest Practice UH Policy
Notify community physician office about hospital admission N/A
Provide receiving clinician’s with hospital clinicians contact information prior to discharge
GM-68
Provide patient with effective education prior to discharge CP 24, G 846 (Nursing Practice Manual)
Provide patient with written discharge instructions prior to discharge
CP 24, GM 68, G 846 (Nursing Practice Manual)
Provide patient with follow up phone number prior to discharge G 846 (Nursing Practice Manual)
Perform medication reconciliation prior to discharge CP 24, CP 112
Schedule outpatient follow up appointment prior to discharge G 846 (Nursing Practice Manual)
Provide community physician office with summary clinical information at discharge
N/A
Invite primary care physician to participate in end-of-life discussions during hospital visit
N/A

Best Practices
• In an ideal world….
• Presenting diads
• Think about the practices during the case presented
• Use the practices at your table to apply them to the case

THEME then best practices by setting1 Notify of PCP of encounter and disposition
Hospital to PCP Notify community MD office about outpatient observation and hospital admission
Hospital to SNF Notify community MD office about encounter and disposition
SNF to ED/Hospital Notify community MD office about encounter and disposition
PCP to ED/Hospital N/A
ED/UC to PCP Notify community MD office about encounter and disposition
ED/UC to Hospital Notify community MD office about encounter and disposition
Coaching Patient/caregiver write contact information in PHR of each provider through care transitions

Introduction

Case Presentation
Patient falls at home
Arrives in EDX-ray shows
comminuted fx
Ortho MD attempts closed reduction
without pain meds
Admitted inpatient
Patient gets long-leg cast
Admit med rec is not correct
Discharged to acute rehab
Pain control inadequate
Discharged to home with home
health
Home health monitors INRs
PCP appt. madeScheduling amb
= can’t go to PCP office
No appt. = no opiates or INR management
Rehab doc fills opiates
Follow up with ortho
Eventually gets PCP follow up

Workshop

Group Discussion