dermatosurgical procedures for vitiligo
TRANSCRIPT

DERMATOSURGICAL PROCEDURES FOR VITILIGO
DR SWATHY LEKSHMI J L
21/08/14

VITILIGO
• Vitelius, vitium
• Multifactorial disease
• Depigmented macules
• Loss of epidermal melanocytes
• Affects all races
• 1% of population

HISTORY OF SURGICAL THERAPY OF VITILIGO1964- Behl, use of Thin theirsch skin graft
1971- Falabella, Suction blister technique
1978- Falabella, Autologous miniature punch graft
1983- Suji and Hamada, Therapeutic spot dermabrasion
1987- Lerner et al, Cultured autologous melanocyte
1989- Gaunthier and Surleve – Bazeille, Non cultured autologous melanocyte rich epidermal cell
suspension
Olsson and Juhlin, refined this technique
1989- Halder et al, Use of ferrous oxide pigment for tattooing
1993- Kahn et al, Melanocyte transplant using ultra thin epidermal sheets

INDICATION FOR SURGERY
1. Stable vitiligo not responding to medical treatment
2. Leukoderma due to burns
3. Piebaldism

STABILITY OF VITILIGO
Absence of new lesionsNo extension of old lesions 1 yearAbsence of Koebner phenomenon
Mini grafting or test grafting
Falabella et al
Unequivocal repigmentation beyond 1mm from the border of test graft

VIDA SCORE
Njoo et al in 1999
Disease activity VIDA score
Active in past 6 weeks +4
Active in past 3 month +3
Active in past 6 months +2
Active in past 1 year +1
Stable for at least I year 0
Stable for 1 year + spon. repigmentation -1

AGE OF THE PATIENTTransplantation procedure better in younger individuals
PREOPERATIVE COUNSELLING
INFORMED CONSENT

CONTRAINDICATION
Active unstable vitiligo

SURGICAL MODALITIES
1. Tissue grafting
2. Cellular grafting
3. Cosmetic tattooing
4. Therapeutic wounding
5. Excision and closure

GRAFTING TECHNIQUES IN VITILIGO
TISSUE GRAFTS
• Suction blister grafting
• Minipunch grafting
• Thin split thickness grafting
• Ultra thin skin grafting (UTSG)
• Mesh grafting
• Flip –top pigment transplantation
• Transplantation of hair follicles
CELLULAR GRAFTS
• Autologous noncultured epidermal cell suspension
• Autologous cultured pure melanocyte transplantation
• Autologous cultured melanocyte – epidermal grafts

PRINCIPLE
GRAFT TAKE ADHERENCE• 1st phase- 72 hrs• Due to fibrin bonding• 2nd phase• Vascular anastomosis & fibro vascular growth
GRAFT REVASCULARIZATION• New vascular channel formation• Compression
CONTRACTURE• Achromic fissure • Perigraft halo• Overlapping at recipient site

SUCTION BLISTER GRAFTINGA technique when the pigmented epidermis is harvested from the donor site by using suction to raise a
blister which is then transferred to vitiliginous area
PRINCIPLE
Cleavage between basal cells& basal lamina
INDICATION
CONTRAINDICATION
• Active lesion
• Infection
• Keloidal tendency

EQUIPMENT• Sterile disposable syringes (20 &50cc)
• 3 way connector
• Tubing
• Dermabrader
• Iris forceps
• Jeweller’s forceps
• Graft spreading rods/spatula
• Sterile glass slides
• Surgical glue ( N – butyl 2 cyanoacrylate)

PROCEDUREDONOR SITE
• Flexor aspect of forearm, medial aspect of upper arm
• Back, upper & medial or posterior aspect of thigh
• Surgical preparation of donor site
• Topical anaesthesia
• Blister is raised using syringe or suction pump with cups
• Base of syringe is applied over donor site

• 3 way connector is attached
• Assembly line- PV tubing,3 way connector,manometer,50cc syringe or suction pump
• Suction to create –ve pressure
• 20 cc syringe with 3 way connector is retained
• Single unilocular non haemorrhagic blister
DEROOFING THE BLISTER
• Roof of the blister is cut
• Roof is inverted onto a glass slide
• Graft is cleaned and spread
• Non adhesive dressing to donor site

TRANSFER OF GRAFT
• Surgical preparation of recipient site
• Anaesthesia -1%lignocaine
• Dermabraded till minute bleeding spots are visible
• CO2 laser can be used
• Graft is placed with dermal side in contact with recipient area
• A gap of 0.5 cm b/w 2 grafts
• Nonadherent dressing is given

POSTOPERATIVE CARE
• Dressing over donor site-24 hrs
• Recipient site-7 days
• Keep the area immobile
COURSE OF THE GRAFT
• Melanocyte transfer-48-72hrs
• Graft dries off by 10-12 days
• Sunlight/PUVA/PUVASOL
• Repigmentation in 3 months

COMPLICATIONS
Donor site: Hematoma Infection Pigmentary changes
Recipient site: Graft rejection Perigraft halo Incomplete pigmentation Hyperpigmentation

ADVANTAGEs
• No scarring at donor site
• Faster repigmentation
• Good colour match-eyelids, lips, areola
• Scar formation, cobble stoning, thick margins, milia are less
• OPD procedure

DISADVANTAGES
• Time consuming
• Raising blister is painful
• Multiple sittings for large areas
• No immediate results

THIN THIERSCH’S SPLIT THICKNESS SKIN GRAFTINGThin split thickness skin graft ,consisting of epidermis and a part of upper papillary dermis harvested from pigmented
donor area is transplanted to recipient site as continuous sheets of tissue grafting
INDICATION
• Stable vitiligo
• Secondary leukoderma
• Piebaldism
CONTRAINDICATION
• Active vitiligo
• Infection
• Altered overlying skin
• Keloidal tendency

EQUIPMENT
Dermabrader – mechanical/ electrical
Skin grafting equipment
• Razor blade holding knife with blade
• Straight artery forceps with razor blade
• Humby’s skin gratfing knife
• Padget’s or Davol’s dermatome
Surgical glue (N- butyl 2-cyanoacrylate)

PROCEDURE
• Recipient site
• Surgical preparation
• LA-Four quadrant infiltration
• Dermabrade evenly
• Extend dermabrasion beyond the margin of lesion
OR
• Ultra pulse CO2 or Erbium- YAG laser ablation
• Hemostasis

Donor site• Anterior, posterior lateral thigh
• Gluteal region
• Abdomen
• Surgical preparation and LA
• KY lubricating jelly applied over cutting knife and donor site
• Stretch the donor site
• Hold the cutting blade parallel to skin surface

• Cut tangentially through upper papillary dermis
• Store the sheets in NS
• Hemostasis
• Dress with framycetin tulle and pressure dressing
• Clean the dermabraded area with NS
• Place appropriate sized graft on abraded bed
• Spread the graft, avoid curling
• Cover with double layer of framycetin tulle
• Pressure dressing

• Immobilization of grafted area
• Antibiotics-8-10 days
• Dressing at recipient site removed after 10-12 days
• Avoid scrubbing for 2 wks
• Pressure garments
• Donor site dressing removed after 10-15 days

COURSE OF GRAFT
• Taken up by 8-10 days
COMPLICATIONS
• Graft rejection
• Beaded appearance
• Perigraft halo
• Mismatch colour
• Superficial scarring at donor site

ADVANTAGES
• Large areas covered in single sitting
• Immediate result
• Good cosmetic results
• Graft survival chance is good
• Quick and safe
DISAVANTAGES
• Mild hyperpigmentation and contracture of grafted site
• Palms, soles ,mucus membrane –difficult to graft
• Surgical expertise

MINIATURE PUNCH GRAFTING
A technique of taking thin, miniature spilt thickness auto skin punch grafts from
normal pigmented donor site and individually grafting them in appropriate
punched out chambers at recipient stable vitiligo site
PRINCIPLE
Donor dominance

INDICATION
• Stable vitiligo of any size
• Adjuvant to medical treatment
• Leukoderma
CONTRAINDICATION
• Active vitiligo
• Altered overlying skin
• Infection
• Keloidal tendency

EQUIPMENTS
• Skin punches (1.5, 2, 2.5mm)
• Small Jeweller's or graft holding forceps
• Small curved tip scissors
• Sterile petridish/ bowl

PROCEDURE
• Test grafting
• Recipient site
• Surgical preparation and LA
• Rotate the punch(2mm) to the depth of mid dermis
• Take such cuts 5-10mm apart
• Lift the edge and cut through mid dermis
• 25 -60 grafts
• Dilate punched out chambers

• Donor site – anterior, posterior, lateral aspect of thigh
gluteal region
retro auricular area
• Surgical preparation
• LA -1% lignocaine / adrenaline
• Rotate the punch (2.5mm) to the depth of upper dermis
• Take such cuts 1-2mm apart

• Lift the edge and cut through upper dermis
• Take a few extra grafts
• Transfer the graft to sterile bowl
• Haemostasis
• Dressing with tulle ,gauze and Elastoplast bandage

• Place the grafts to recipient area
• Haemostasis by saline soaked dressing
• 3 layer dressing at recipient area
• Immobilization if needed
• Special areas –lips
• Extra grafts stored for 24-48 hrs.

FOLLOW UP
• Donor site - dressing removed after 8-10 days
• Recipient site- after 24 hrs
• Antibiotics -8-10 days
• Exposure to sunlight / PUVA
• Oral or topical steroids
COURSE OF THE GRAFT
• Donor site heals with secondary intention
• Graft is take up by 8-10 days
• Perigraft pigment spread -1 month
• Completes in 3-6 months
• Average spread from a 2.5 mm graft- 5-10mm

COMPLICATIONS
Recipient site
cobble stoning
variegated appearance
static graft
depigmentation of graft
perigraft halo
graft rejection
hypertrophic scar & keloid
Donor site
depigmentation
scar
allergic contact dermatitis

ADVANTAGES
• High success rate
• Easy, fast, least expensive
• Performed on any site
DISADVANTAGES
• No immediate results
• angle of mouth & nipple

MESH GRAFTING
A technique where graft is expanded by making slits in it such that it appers like
a mesh, allows the coverage of large area with a smaller graft
PROCEDURE
Donor site
• Split thickness graft of 0.025 inch thickness
• Graft is meshed with Ampligraft (1:1, 1:2, 1:4)
• Graf is transferred to recipient site
• Recipient site is dressed with tulle
• Dressing is removed after 1 wk
• Phototherapy after 1 wk

ADVANTAGES
• Meshing allows coverage of large areas
• Coverage of areas with variable contour
DISADVANTAGES
• Scarring at donor site
• Thick graft causes beading at margin
• Inferior cosmetic results

FLIP- TOP PIGMENT TRANSPLANTATIONA technique in which graft is placed b/w a flap of epidermis & dermis at recipient site
PROCEDURE
• A thin split thickness graft is harvested
• Graft is kept moist
• A similar flap of epidermis is raised at recipient site
• One end of epidermis is left in contact
• Flap is turned to expose dermal side
• Graft is placed in contact with dermis
• Flap is put back in position
• Cyanoacrylate glue
• Dressings

FOLLOW UP
• Dressing is removed after 1 wk
• Phototherapy
ADVANTAGES
• Flap acts as a biological dressing
DISADVANTAGES
• Beading at margins

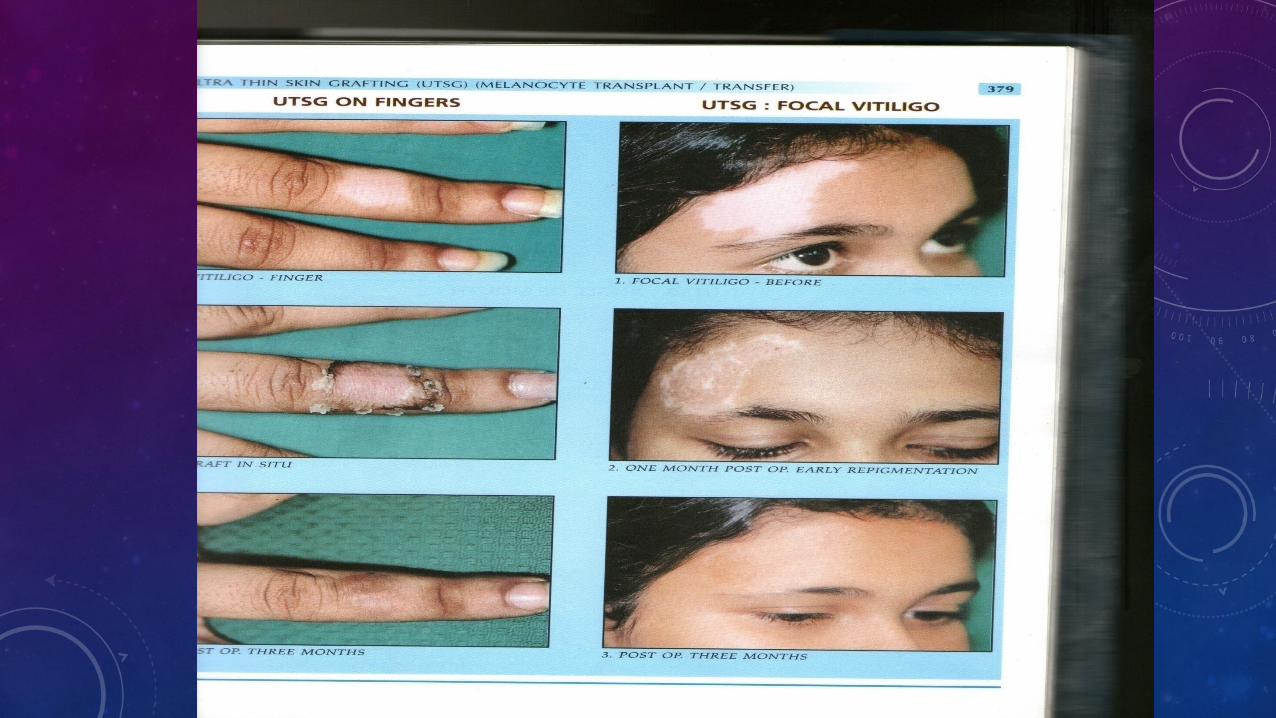
ULTRA THIN GRAFTING (UTSG)(MELANOCYTE TRANSPLANT/ TRANSFER)
Technique consists of an ultra thin SSG containing epidermis and uppermost papillary dermis
MECHANISM OF ACTION
• Migration of melanocyte and keratinocyte from the graft , followed by multiplication in the
vitiliginous area
• Process accelerated by PUVA/ PUVASOL therapy

INDICATION
1. Stable vitiligo
2. 2ndary leukoderma
3. Piebaldism
4. As an adjuvant to medical treatment

CONTRAINDICATIONS
1. Active lesion
2. Infections
3. Keloid tendency
4. Altered overlying skin
PREOPERATIVE WORKUP
INSTRUMENTS
1. Dermabraders
2. Power dermatome
3. Iris scissors
4. Jeweller’s forceps
5. Graft spreading rods
6. Surgical glue
7. Sterile petri dish

PROCEDURE
DONOR SITE
1. Surgical preparation of site
2. Anaesthesia
3. Lubrication of donor site by KY jelly
4. Donor site made taut by stretching
5. Usually a 0.125mm graft harvested from donor site using power dermatome
6. Put in sterile petri dish
RECEPIENT SITE
1. Surgical preparation
2. Mark beyond the vitiliginous area all along the periphery
3. Divide and mark the area into linear segments
4. Anaesthesia
5. Dermabrade up to marked area till pinpoint bleeding appears
6. Achieve haemostasis, cover area with moist saline gauze
7. CO2 laser ablation
8. Place graft on abraded area
9. Spread graft using spatula, 3-5 mm beyond marked area
10.Fix graft with glue: N- Butyl 2- Cyanoacrylate
11.Dress wound

POST OPERATIVE
1. Antibiotics
2. Analgesics
3. Immobilisation if required
FOLLOWUP
• Dressing opened after 24 hrs
• Seroma if present is drained
• Wound redressed
• 2nd dressing removed after 10- 12 days

COURSE OF GRAFT
• Melanoctye transfer to recipient dermis by 48-72 hrs
• Graft dries off or macerates by 10 – 12 days
• Sunlight or PUVA therapy on exposed area
COMPLICATIONS
• Donor site - reversible hypo/ hyperpigmentation
• Recipient site : graft rejection, reactivation of vitiligo.

ADVANTAGES OF PROCEDURE
• Simple and easy , less time consuming
• High success rate
• Excellent cosmetic result
• Graft itself acts as biological dressing.
DISADVANTAGES
• Expensive
• Sophisticated instruments
• Surgical expertise

CELLULAR GRAFTS

ADVANTAGES OF CELLULAR GRAFTS
• Smaller amount of donor tissue is needed
• Donor recipient ratio -1:8 -1:150
• Post op pain and morbidity less
• Application of cell suspension is easier – ear, umbilicus, genitals
• Immobilization needed is less
• More suitable for certain areas like finger tips

INDICATIONS
• Stable vitiligo
• Segmental and focal vitiligo
• Piebaldism
• Post burn leukoderma
• Chemical leukoderma
• Nevus depigmentosus
• Halo nevus

CONTRAINDICATIONS
• Bleeding disorders
• Active vitiligo
• Keloidal tendency

NONCULTURED MELANOCYTE GRAFTING-EPIDERMAL SUSPENSIONS
• BASIC PRINCIPLE
• To separate the melanocyte and basal cells by trypsinisation
• Prepare a suspension which is applied on dermabraded lesional skin
• Donor to recipient ratio of 1:5 or 1:10

EQUIPMENTS• Trypsin – EDTA solution of 0.25%
• Trypsin inhibitor
• Dulbecco’s Modified Eagle’s Medium(DMEM)/Nutrient mixture F-12
• Centrifuge
• Aerobic incubator
• Micromotor diamond fraise dermabrader or CO2 laser
• Dermatome or suction apparatus
• Pasture pipette or calibrated micropipette
• Fine pointed forceps
• Centrifuged tubes and petridishes
• Collagen dressing

PROCEDURE
OBTAINING THE DONOR
• Thin uniform graft by split thickness or SBT
• Cover the donor site with tulle dressing

PREPARATION OF CELL SUSPENSION
Trypsinisation
• Skin sample to a petri dish containing 8ml 0.25% trypsin- EDTA
• Placed with epidermis facing upwards
• Incubated in aerobic incubator – 37deg C for 50 minutes
• Adding 5 ml trypsin inhibitor
Separation of epidermis from dermis
• Using a pair of non toothed forceps
• Repeated teasing
• Additional incubation if needed
• Epidermis is transferred to suitable medium

• Medium- DMEM medium with F-12 nutrient mixture
Centrifugation
• Material is placed in a centrifuge tube and centrifuge – 2000 rpm for 10 mts
• A cell pellet is formed at bottom of tube
• Supernatant fluid is discarded
• Pellet is re suspended in 0.8 ml DMEM medium
• A drop of suspension is observed under invertor microscope

Transplantation
• Recipient area is abraded down to DEJ using diamond fraise dermabrader
• OR
• CO2 laser ablation
• Cell suspension is applied with a pipette
• The area is covered with transparent collagen film
• Dressing with sterile gauze ,moistened with DMEM/F-12 f/b Tegaderm dressing

POST OPERATIVE CARE
• Instructed not to move the area for 48 hrs
• Dressing removed after 1 week
• Complete epithelisation takes 6-10 days
• Pigmentation within 4 wks of grafting
• Phototherapy after 3 weeks
• Complete pigmentation in 3-6 months

DISADVANTAGES
• Specific cell culture grade biochemical and media
• Well equipped operating room
• More expensive
• Time consuming

AUTOLOGOUS CULTURED MELANOCYTE TRANSPLANTATION
• In vitro cultured melanocytes
• Donor to recipient ratio of 1:20-1:30
• Mutagenicity and possible risk of cancer
• TPA (12-tetradecanoylphorbol 13-acetate)

PROCEDURE• Donor skin is obtained by shave excision
• Trypsinization
• Melanocytes and keratinocytes are separated
• Melanocytes are seeded in a melanocyte medium
• Hu 16 medium- Ham’s F12 nutrient mixture
gentamicin
recombinant human FGF
isobutylmethylxanthine
cholera toxin
20% fetal calf serum
• Melanocytes are cultured for 15-30 days
• Melanocytes are detached from culture plates

• Recipient area –superficial dermabrasion or CO2 laser ablation
• Suspension is transplanted on the denuded area (1000-2000 /mm sq.)
• Free suspension or co-culture with keratinocytes or integrated into
epidermal sheets
• Site is secured with gauze f/b occlusive dressing
• Bed rest for 8-10 hrs
• Dressing is changed after 1 week

AUTOLOGOUS CULTURED MELANOCYTE-EPIDERMAL GRAFTS
• Co-cultivation of keratinocytes and melanocytes
• Cultured epidermal sheet is attached to petrolatum gauze
• Recipient area is prepared
• Gauze is applied on the recipient site

MODIFICATION AT SPECIAL SITESEyelids - SBEG for small area
Thin /Ultrathin split thickness graft
Lips -SBEG for small lesion
Thin split thickness graft for larger areas
Areola -Entire area
Acral areas – Mini punch grafting
SBEG/ Thin spilt thickness graft for dorsal areas
Genitals – Rule out genital herpes
SBEG/ Thin spilt thickness graft
Mini punch/ Non cultured melanocyte suspension.
Hairy areas

TRANSPLANTATION OF HAIR FOLLICLES
INDICATION
• Vitiligo in hair bearing areas
PROCEDURE
• A strip of hair is removed from occipital area
• Cut into smaller pieces
• Transplanted onto vitiligo patch
• Recipient site is dressed
• Remove after 1 wk.
• Phototherapy

ADVANTAGES
• Leucotrichia
• No cobble stoning
• Good colour match
DISADVANTAGE
• Cumbersome procedure
• Scarring

THERAPEUTIC WOUNDING
PRINCIPLE
• Inflammatory cytokines stimulate follicular and perilesional melanocytes
INDICATIONS
• Stable vitiligo over cosmetically unimportant hairy areas
• Small narrow resistant streaks

CONTRAINDICATION
• Active lesion
• Infection
• Bleeding disorder
• Atrophic overlying skin
• Cosmetically important areas
• Keloidal tendecy

• EQUIPMENT
• Electrical or manual dermabrader
• CO2 laser
• LN2with spray unit
• 50% TCA
• 88% liquid phenol
• 26G needle

THERAPEUTIC WOUNDING MODALITIES
1. Dermabrasion- medium to large hairy areas
2. CO2 laser ablation
3. LN2 cryosurgery
4. Chemosurgery
5. Needling
6. Others- electrocautery, radiocautery

SUPERFICIAL DERMABRASION
• LA /GA
• Sequential planing of hairy vitiligo areas to the junction of mid &deep papillary dermis
• Allow the wound to heal by secondary intention

CO2 LASER ABLATION
• Shaving and surgical preparation
• Mark the periphery of lesion
• LA/ GA
• Set laser parameters to cause vaporisation
• Small adjacent areas are ablated
• Bubbling of epidermis which can be easily wiped off
• Dressing

POST OPERATIVE
• Change dressing after 8-10 days
• Oral antibiotics- 7 days
• PUVA/ PUVASOL after wound healing
COMPLICATIONS
• Persistent erythema
• Hypo/hyper pigmentation
• Scarring

ADVANTAGES
• Simple free hand technique with no bleeding
DISADVANTAGES
• At least 25% of hair should be black
• Expensive

LIQUD NITROGEN CRYOSURGERY• LA
• Spray the LN2(-196 deg C) over the lesion
• Freeze it for 10-20 sec
• Wound healing by secondary intention
POST OPERATIVE CARE
• Oral antibiotics
• Change dressing after 24 hrs
• Crust falls off within 7-15 days

CHEMICAL SURGERY WITH 50% TCA/ 88% PHENOL
• Clean the area
• No LA
• Apply 0.5-1 ml 88% phenol
• Frosting
• Neutralisation with cold water if TCA is used
• Drink plenty of water for next 4 hrs
• Topical antibiotic ointment
• PUVA/ PUVASOL after 15 days

COMPLICATIONS• Immediate burning sensation & discomfort• Superficial scarring• Hyperpigmentation
ADVANTAGES• No LA is required• Adjuvant to medical treatment• Safe, simple
DISADVANTAGES• Applicable in areas where cosmetic importance is secondary• Multiple sittings for large areas• At least 25% of hair should be black

NEEEDLING
• Surgical preparation of the area
• No LA
• Puncture very superficially at junctional hyperpigmented border
• Tip of needle reaches up to upper papillary dermis
• Make multiple punctures
• Haemostasis

• Antibiotic ointment -1-2 days
• Crusting and scab in 2-4 days
• PUVA/ PUVASOL can be continued
• Tiny projections of pigmentation by 15 th day
• Repeat in every 15-20 days

COSMETIC TATTOOING
Process of uniform implantation of minute, metabolically inert, pigment granules into dermis so as to artistically create a permanent cosmetic camouflage
EQUIPMENT• Mechanical or Manual punch/ Watchmaker’s pin - vise or • Electrical machine- Double coil reciprocating gun type Rotatory pencil type• Spatula• Sterile bowl• Glycerine

TATTOO PIGMENTS- autoclaved
• White titanium dioxide
• Red cinnabar, mercuric sulphate
• Black iron oxide
• Yellow cadmium sulphate
• Camel yellow iron oxide
• Light brown iron oxide
• Dark brown iron oxide
INDICATIONS
• Stable vitiligo
• Leukoderma
• To fill up the gaps of alopecia
• Flap decorative tattooing
• Defining eyelid or lip margins
CONTRAINDICATIONS
• Active vitiligo
• Infection
• Allergy to pigments

PROCEDURE
• Take a basic pigment powder
• Add NS or isopropyl alcohol
• Add 2 -3 drops of glycerine
• Add various pigments to the basic paste
• Tattoo operation - Electrical
• Consent, shaving, premedication
• Surgical preparation of the part
• LA
• Inject NS for ballooning
• Apply thin coat of antibiotic ointment

• Dip the needle in pigment bowl
• Stretch the tattoo site
• Hold the tattoo machine in pencil grip
• Hold the needle tip above skin surface and start machine
• Follow – Reference dot method or Pigment line method

SHADING
• Stretch the skin and give a thick coat of pigment paste
• Move the needle tip in a clockwise circular motion
• Concurrently move linearly from one end to another
• Overlap the circle during each circular movement
• Spiral flaring effect
• Wipe away the excess pigment
• Skip areas if present repeat the procedure
• Haemostasis with cold sponge pressure
• Topical antibiotic
• No dressing

SEQUALE
• Swelling, pain and crusting
• Crust will fall off by one week
COMPLICATIONS
• Local trauma
• Secondary infection
• Transmission of infection
• Pigment extrusion
• Reaction to pigment
• Leaching out
• Halo effect
• Change in colour shade

TOUCH UP TATTOOINGADVANTAGES
1. Instant camouflage
2. Good cosmetic match in dark skinned
3. Cosmetic procedure preferred in certain locations like angle of mouth, nipple and genitalia
4. Inexpensive office procedure
DISADVANTAGES
5. Not useful in larger areas
6. Touch up tattooing
7. Transmission of infection

Choice of method according to area and site
Preferred Alternative
AREA Small area SBEG, STG PG
Moderate NCES, STG PG
Relatively large area CM,CE, NCES, STG
SITE Finger and toes PG, SBEG NCES
Palm and soles PG
Eyelids SBEG, NCES, STG MPG
Nipple and areola SBEG, NCES
Genitals NCES, SBEG, CM

THANK YOU