deputy editor this topic last updated: introduction fileadditional risk factors were evaluated in a...
TRANSCRIPT

Bacterial endophthalmitis Author
Marlene L Durand, MD Section Editors
Stephen B Calderwood, MD Jonathan Trobe, MD Deputy Editor
Allyson Bloom, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Sep 2015. | This topic last updated: Sep 08, 2015.
INTRODUCTION — Endophthalmitis refers to bacterial or fungal infection within the eye, including involvement of the
vitreous and/or aqueous humors. It is not caused by viruses or parasites; by convention, infections due to these
organisms are included in the term "uveitis" (eg, cytomegalovirus [CMV] retinitis, toxoplasma chorioretinitis). Most
cases of endophthalmitis are exogenous, resulting from inoculation of organisms from the outside, via trauma, eye
surgery, or as an extension of keratitis (corneal infection). In such cases, the aqueous humor may be seeded first
before extension into the vitreous. The remaining cases are endogenous, resulting from bacteremic or fungemic
seeding of the eye. In endogenous endophthalmitis, organisms usually seed the highly vascular choroid first then
extend anteriorly into the vitreous.
Most cases of endophthalmitis are due to bacteria and present acutely. Acute bacterial endophthalmitis is a vision-
threatening condition and must be managed as an emergency. The clinical outcome depends upon both the virulence
of the infecting organism and the speed with which appropriate therapy is initiated.
Bacterial endophthalmitis can be divided into six categories:
●Acute postcataract surgery
●Chronic pseudophakic
●Post-intravitreal injection (eg, after anti-vascular endothelial growth factor [VEGF] injections)
●Bleb related
●Posttraumatic
●Endogenous
The epidemiology, clinical features, diagnosis, and treatment of bacterial endophthalmitis will be reviewed here.
Fungal endophthalmitis is discussed separately. (See"Epidemiology, clinical manifestations, and diagnosis of fungal
endophthalmitis" and "Treatment of endogenous endophthalmitis due to Candida species" and "Treatment of
exogenous endophthalmitis due to Candida species" and "Treatment of endophthalmitis due to molds".)
ACUTE POSTCATARACT ENDOPHTHALMITIS — Acute postcataract endophthalmitis is the most common form of
endophthalmitis and, in the United States, is almost always due to bacteria. This complication occurs within six weeks
of cataract surgery, with 75 percent of cases presenting in the first postoperative week.
Series from the 1990s noted an incidence of endophthalmitis of 0.1 to 0.2 percent of cases [1-3], whereas a
nationwide prospective study in Sweden from 2002 to 2004 found a somewhat lower incidence of 0.05 percent [4].
Despite the low rate, endophthalmitis represents an important clinical problem since over two million cataract
operations are performed annually in the United States.
Risk factors — The vitreous is much more susceptible than the aqueous humor to infection by exogenously
introduced bacteria (figure 1) [5]. Cataract surgery, which is performed through the anterior chamber, often results in
transient bacterial contamination of the aqueous by the patient's conjunctival flora.
Several studies have shown that bacteria can be isolated from the anterior chamber at the end of cataract surgery in 7
to 43 percent of cases [6-8]. The organism burden in the aqueous is usually low, as demonstrated by quantitative
cultures [6]. None of the study patients developed endophthalmitis, suggesting that the immune system is usually able
to clear a small inoculum of relatively avirulent organisms.
If a communication with the vitreous is inadvertently created during surgery (eg, break in the posterior lens capsule),
the risk of endophthalmitis is much higher (14 times higher in one report) than in patients without a vitreous
communication [4,9].

Additional risk factors were evaluated in a retrospective case-control series of 57 patients with postcataract
endophthalmitis and 220 controls [10]. Implantation of an intraocular lens without a heparinized surface,
immunosuppressive therapy, and wound abnormality were risk factors for infection by logistic regression analysis.
Risk factors noted in other studies include diabetes [2], wound dehiscence or leak [11], age ≥85 [4], and lens implants
made of polypropylene (Prolene) instead of polymethyl methacrylate [12].
Advances in surgery, such as phacoemulsification and foldable synthetic intraocular lenses, have allowed incisions so
small that they are considered self-sealing. These "sutureless" incisions are now primarily made through the cornea
("clear cornea incision"), which may increase the risk of postoperative endophthalmitis [13-16]. There is evidence that
clear corneal incisions gape intermittently during the first few days after cataract surgery. This may allow external
colonizing flora to enter the eye and account for the increased risk of endophthalmitis [17,18].
Symptoms and signs — The onset of symptoms occurs within one week of surgery in 75 percent of cases. Patients
usually give a 12 to 24 hour history of decreasing vision and eye "ache" (they may deny eye "pain"). Patients feel
otherwise well and are afebrile.
On physical examination, findings are confined to the affected eye. The lids often appear normal, although they may
be swollen. The conjunctiva may be injected or edematous (conjunctival chemosis), although these findings can also
represent residual postoperative changes. Visual acuity is decreased, and a hypopyon (layering of white blood cells in
the anterior chamber) is often present (picture 1). The view of the retina is usually hazy, and, in 80 percent of patients,
no retinal vessels can be seen [15]. Slit lamp examination reveals intraocular white blood cells and protein (called
"cells" and "flare," respectively, by ophthalmologists).
Differential diagnosis — The major entity in the differential diagnosis of endophthalmitis is sterile postoperative
inflammation. This can result from various causes, including a reaction to retained native lens fragments, extensive iris
manipulation, or prolonged and complicated surgery [5].
The sterile inflammation can mimic early endophthalmitis, although the manifestations are typically greatest on the first
postoperative day, whereas bacterial endophthalmitis usually develops on day two or later. However, timing of the
onset of symptoms or findings cannot be relied upon to differentiate these entities. Sterile inflammation must be a
diagnosis of exclusion.
Laboratory findings — Laboratory findings are usually normal. Only one-third of patients with endophthalmitis have a
white blood cell count greater than 10,000/microL[19]. The erythrocyte sedimentation rate is usually normal. An
ultrasound of the eye ("B-scan") usually shows increased echogenicity of the vitreous due to intraocular inflammation.
This test can be helpful when the view of the vitreous is obscured by abnormalities in the anterior segment.
Diagnosis — Endophthalmitis is a clinical diagnosis that is confirmed by positive aqueous or vitreous culture.
However, a negative culture does not exclude the diagnosis.
The ophthalmologist can aspirate the aqueous (0.1 mL sample) and/or vitreous (0.2 to 0.3 mL) with a needle in the
office or perform a pars plana vitrectomy in the operating room. A vitrectomy entails the use of a vitrector, an
instrument inserted into the vitreous that simultaneously cuts and aspirates some of the 4 mL of gel-like vitreous into a
canister. During this process, another catheter irrigates the vitreous with saline. By the end of the case, the vitrectomy
canister contains 50 to 100 mL of dilute vitreous washings (figure 2).
Vitrectomy has the highest yield for a positive culture (90 percent of specimens), whereas only 75 percent of vitreous
aspirate specimens are positive [19]. An aqueous aspirate has the lowest yield for a positive culture. In cases with
positive vitreous cultures, simultaneous aqueous cultures are positive in only 40 percent [19].
Aspirates should be cultured on blood agar, chocolate agar, anaerobic media, meat broth, and Sabouraud agar. One
drop should be placed on a slide for Gram stain. Gram stain is positive in approximately 45 percent of cases [19].
If a vitrectomy is performed, 3 mL of the vitreous washings should be aspirated from the canister, centrifuged, and the
pellet smeared on a slide for Gram stain. The remainder of the canister contents should be vacuum filtered through a
0.45 micron filter; the filter paper should then be cut up and placed on the media listed above.
It is not yet clear what role molecular diagnostic techniques, such as polymerase chain reaction (PCR), will have in the
diagnosis of bacterial endophthalmitis. These methods may amplify bacteria that are conjunctival contaminants and
lead to false-positive results. The value of PCR was evaluated in a study that used eubacterial primers to examine
aqueous and vitreous samples from endophthalmitis cases and noninfectious controls [20]. PCR was positive in all 20
culture-positive cases, but also in one of the 20 controls. The use of PCR to diagnose endophthalmitis is being
evaluated in a large multicenter European study [21].
Bacteriology — Since coagulase-negative staphylococci are the predominant organisms colonizing the surface of the
eye, and since most cases of postcataract endophthalmitis are due to the patient's own conjunctival flora [22], it is not
surprising that coagulase-negative staphylococci are the major pathogens in postcataract endophthalmitis. The best
microbiologic data have been provided by the Endophthalmitis Vitrectomy Study (EVS), a multicenter, National
Institutes of Health (NIH)-sponsored prospective study of 420 patients with postcataract endophthalmitis [23]. Thirty-
one percent of patients had negative or equivocal cultures. Organisms isolated in the confirmed culture-positive group
included:
●Coagulase-negative staphylococci – 70 percent
●Staphylococcus aureus – 10 percent
●Streptococci – 9 percent
●Other gram-positive organisms – 5 percent
●Gram-negative organisms – 6 percent
Treatment — Acute endophthalmitis is a medical emergency. The most important component of treatment of
postcataract endophthalmitis is direct injection of antibiotics into the vitreous. Vitrectomy is important in severe cases.
The role of adjunctive systemic antibiotics is unknown.
Intravitreal antibiotics — The ophthalmologist first obtains a vitreous sample for culture and then injects antibiotics
into the vitreous. Intravitreal antibiotics can be injected either as an office procedure (vitreous aspiration and antibiotic
injection, also called "tap and inject") or in the operating room following vitrectomy (a debridement procedure of the
vitreous).
The empiric intravitreal antibiotics used are vancomycin 1 mg plus either ceftazidime 2.25 mg or amikacin 0.4 mg.
Each agent is diluted in 0.1 mL of sterile water or saline. Ceftazidime is usually preferred over amikacin because of
the small risk of macular infarction with injected aminoglycosides. Antibiotic concentrations in the vitreous decline
rapidly following injection, so most last only 24 to 48 hours. Thus, one injection of antibiotics may not maintain levels in
the vitreous long enough to kill all bacteria. A repeat injection of vancomycin or ceftazidime may be indicated after 48
hours if there is persistent or worsening intraocular inflammation; a second injection of amikacin is avoided given
concerns for retinal toxicity. The choice of antibiotic for repeat intravitreal injection is based on the culture result.
Vitrectomy — Vitrectomy is an important component of treatment in eyes with severe infection. Vitrectomy debrides
the inflamed vitreous, similar to incision and drainage of an abscess. Vitrectomy leads to better visual outcomes in
patients who present with severe vision loss. Whether vitrectomy should also be used in less severe cases is unclear.
Similarly, the role of adjunctive oral or intravenous antibiotics in treating exogenous endophthalmitis is unclear.
The Endophthalmitis Vitrectomy Study was a multicenter trial that evaluated the role of vitrectomy and the value of
adjunctive systemic antibiotics in treating postcataract endophthalmitis [19]. This study changed the practice of
treating postcataract endophthalmitis. However, flaws in study design led to controversy regarding the interpretation of
some of the results. Four hundred and twenty patients with postcataract endophthalmitis were randomly assigned to
four treatment arms (2x2 design): vitrectomy versus vitreous "tap" (aspirate or biopsy) and systemic antibiotics versus
none [19]. The systemic antibiotics used were intravenous ceftazidime and amikacin. All patients received intravitreal
antibiotics and all patients assigned to the vitrectomy group received a vitrectomy in the operating room under local
anesthesia.
It is important to note that the vitreous "tap" group in the EVS was not homogeneous. Although a vitreous "tap" is
understood by ophthalmologists to mean needle aspiration of the vitreous (an office procedure using topical
anesthesia), the "tap" group included patients who received the usual needle aspiration of the vitreous, but also those
who received a vitreous biopsy. Two-thirds of the patients had a vitreous "biopsy," which was really a "mini-vitrectomy"
and was performed with a vitrector in the operating room [24,25]. The EVS authors concluded that there was no
difference in visual outcome between the vitrectomy and "tap" groups, except in patients who presented with the worst
vision (light perception only). In these patients, vitrectomy was superior and significantly decreased the chance of
severe visual loss compared with vitreous "tap" (20 versus 47 percent). In patients who presented with hand motion or

better vision, the authors concluded that vitreous "tap" was sufficient. However, objections have been raised to this
conclusion, since the comparison was really vitrectomy versus mini-vitrectomy in the majority of patients. The question
remains whether patients who present with hand motion or better vision, especially those who present with a rapidly
worsening course, might also benefit from vitrectomy (plus intravitreal antibiotics) rather than intravitreal antibiotics
alone.
The EVS demonstrated that vitrectomy sterilizes the vitreous more quickly than intravitreal antibiotics alone.
Approximately 10 percent of each group had a second procedure and vitreous culture during the first week due to
persistent inflammation. Of these patients, vitreous cultures were persistently positive more often in the "tap" group
than the vitrectomy group (71 versus 13 percent), even though both groups had received the same intravitreal
antibiotics [24]. Therefore, a vitrectomy should be considered for patients with endophthalmitis who received only an
initial "tap and inject" on presentation but are failing to improve by 48 hours (or 24 hours in severe cases), since these
patients may have persistent infection.
A subsequent US study attempted to survey ophthalmologists who had treated 1213 endophthalmitis cases in five
states between 2003 and 2004 (cases identified by Medicare claims) but received responses for only 719 cases (59
percent) and included only 615 cases (51 percent) [26]. The study concluded that vitrectomy offered no benefit, but its
retrospective nature and poor survey response rate confound interpretation of the data.
Adjunctive systemic antibiotics — Systemic antibiotics alone are not effective in treating bacterial endophthalmitis.
Whether systemic antibiotics provide any benefit as adjunctive therapy to intravitreal antibiotics is unknown. Systemic
antibiotics that cross the blood-eye barrier may prolong intravitreal antibiotic concentrations achieved following
intravitreal antibiotic injection. This may be helpful in killing bacteria in the vitreous. However, there are no studies that
have adequately evaluated this. The EVS concluded that adjunctive systemic antibiotics did not improve visual
outcome and were not necessary to treat postcataract endophthalmitis [19]. However, staphylococci accounted for 80
percent of the study isolates [23], but the systemic antibiotics used in the study (amikacin plus ceftazidime) have poor
activity against staphylococci. In addition, amikacin does not cross the blood-eye barrier, so it is ineffective in treating
endophthalmitis. It has been suggested that more effective systemic antibiotics (eg, a regimen that included
intravenous vancomycin) might have demonstrated a benefit [27].
Since the EVS, only retrospective reviews of adjunctive systemic antibiotics have been published. A study from
western Australia that reviewed 213 cases of postcataract endophthalmitis from 1980 to 2000 found that patients who
received various adjunctive oral antibiotics had better visual outcomes compared with those who did not receive
adjunctive antibiotics [25]. However, it is difficult to draw any conclusions from this study given the lack of a uniform
antibiotic regimen and the retrospective study design. Another study reviewed 72 cases of postcataract
endophthalmitis between 2000 and 2009 treated with intravitreal injection of antibiotics (excluding patients treated with
initial vitrectomy in addition to intravitreal antibiotics) [27]. All patients received an oral fluoroquinolone for 10 days
after intravitreal injection of antibiotics; ciprofloxacin was used between 2000 and 2004 (in 48 patients)
and moxifloxacin was used between 2005 and 2009 (in 24 patients). There were no significant differences in patient or
surgical characteristics between the two groups. After controlling for potentially confounding factors such as
ciprofloxacin resistance, moxifloxacin use was significantly associated with a good visual outcome (20/40 or better;
adjusted odds ratio 4.07, 95% CI 1.11-14.9).
Approach to therapy — We recommend the following approach to therapy for patients with postcataract bacterial
endophthalmitis:
●Cultures of the vitreous should be obtained by needle aspiration or vitrectomy as soon as endophthalmitis is
suspected.
●Antibiotics should be injected into the vitreous as soon as endophthalmitis is suspected and vitreous cultures
are obtained. Intravitreal antibiotics are the most important component of endophthalmitis therapy. Empiric
intravitreal antibiotics are usually given when the etiology is unknown, and these include vancomycin 1 mg plus
either ceftazidime 2.25 mg or amikacin 0.4 mg. Ceftazidime is favored over amikacin because of toxicity
concerns.
●Vitrectomy should be performed for eyes with severe vision loss on presentation (light perception vision only or
worse) and should be considered for cases that fail to improve after 24 to 48 hours. Vitreous aspiration ("tap and
inject") may be used initially for other cases. Intravitreal antibiotics are injected at the end of the vitrectomy as
above.
●The intraocular lens implant does not need to be removed, except in cases of chronic endophthalmitis or those
due to fungi. (See 'Chronic pseudophakic endophthalmitis' below and "Treatment of exogenous endophthalmitis
due to Candida species" and "Treatment of endophthalmitis due to molds".)
●The value of adjunctive systemic antibiotics in treating postcataract endophthalmitis is unknown. We
recommend adjunctive systemic antibiotics for severe cases (see 'Adjunctive systemic
antibiotics' above). Moxifloxacin (400 mg orally once daily) achieves excellent vitreous levels [28] and, as noted
above, a retrospective study using 10 days of therapy suggested some benefit [27]. Oral linezolid (600 mg twice
daily) can be used as adjunctive therapy in staphylococcal endophthalmitis, but it has been inadequately studied
for this indication. Linezolid achieves therapeutic intraocular levels [29] and has excellent coverage of gram-
positive bacteria. Whether intravenous antibiotics are indicated as adjunctive therapy in fulminant postcataract
endophthalmitis cases has not been studied. In practice, few ophthalmologists use them.
●If the eye is not improving by 48 hours after the initial intravitreal antibiotic injection (ie, unchanged or
worsening intraocular inflammation based on the ophthalmologist's examination), there are two things one
should consider: a second injection of intravitreal antibiotics and vitrectomy (if this has not already been
performed). In fulminant cases, these should be considered at 24 rather than 48 hours. For this second injection
of intravitreal antibiotics, either intravitrealvancomycin and/or ceftazidime should be given, based on culture
results. A second injection of amikacin is avoided, if possible, due to toxicity concerns. A repeat culture of the
vitreous should also be obtained. In rare cases, a third injection of intravitreal antibiotics may be indicated 24 to
48 hours after the second injection, especially if repeat vitreous cultures are positive.
Visual outcome — About half of eyes with postcataract endophthalmitis will eventually recover 20/40 vision, whereas
10 percent will lose useful vision (5/200 or worse) [19]. The outcome of postcataract endophthalmitis depends on the
virulence of the pathogen: the worst outcomes are seen in cases due to streptococci of any type and the best
outcomes occur in cases due to coagulase-negative staphylococci or cases that are culture negative [19].
CHRONIC PSEUDOPHAKIC ENDOPHTHALMITIS — Chronic pseudophakic-related endophthalmitis is a rare
complication of cataract surgery. During cataract surgery, most of the opacified native lens (cataract) is removed,
leaving behind some residual native lens and the posterior portion of the lens capsule. An artificial intraocular lens
(IOL) is placed in front of this in the posterior chamber, the space between the lens and iris. "Pseudophakic" refers to
the intraocular lens. Chronic pseudophakic endophthalmitis is usually caused by Propionibacterium acnes. A few
cases have been caused by coagulase-negative staphylococci and diphtheroids. This infection is characterized by
low-grade intraocular inflammation that may persist for months. It is often misdiagnosed as noninfectious iritis and
typically improves with topical corticosteroid therapy but flares each time corticosteroids are stopped. It may be
months before the correct diagnosis is made.
Symptoms include decreased vision in nearly all patients and eye pain (usually mild) in approximately half of patients.
Eye examination with a slit lamp reveals white blood cells in the anterior chamber and, in nearly all patients, a
characteristic white plaque in the posterior lens capsule. A hypopyon and white blood cells in the anterior vitreous
(anterior vitritis) are also seen in some patients.
For years, this process was thought to be a reaction to the remaining native lens tissue and was called toxic lens
syndrome or phacoanaphylactic endophthalmitis. That the inflammation typically decreased with topical corticosteroid
therapy added support to this misdiagnosis. Vitreous culture was negative or grew only P. acnes, initially thought to be
a contaminant. Subsequent Gram stain and electron microscopy studies of the removed lens capsule showed small
gram-positive rods, consistent with P. acnes, adherent to the capsular remnants [30].
Diagnosis is often difficult and is based on clinical suspicion supported by cultures of the aqueous or posterior lens
capsule. However, cultures of the aqueous are often negative, even in cases where subsequent electron microscopy
of the removed lens or lens capsule demonstrates organisms [31]. Anaerobic cultures should be included if possible.
The highest yield for culture is usually by sampling the white plaque in the posterior lens capsule, but this can only be
obtained by surgery (removal of the intraocular lens and posterior lens capsule). Aspirate of the aqueous can be
performed in an outpatient ophthalmology procedure room using a topical anesthetic.
Treatment requires at least vitrectomy and intravitreal vancomycin, although 50 percent of cases recur with this
treatment alone [32,33]. Removing part of the lens capsule (partial capsulectomy), in addition to vitrectomy and
intravitreal vancomycin, reduced the recurrence rate in one study to 14 percent [33]. However, in another study, this
treatment was associated with a 44 percent recurrence rate [34]. Exchanging the IOL for a new one improved

outcomes considerably. The combination of total capsulectomy, IOL exchange or removal, vitrectomy, and intravitreal
antibiotics cured all cases in both studies. This was true whether this treatment was used as initial therapy or as
treatment of recurrence after other therapy had failed. Systemic antimicrobial therapy is not indicated.
POST-INTRAVITREAL INJECTION ENDOPHTHALMITIS — Neovascular, or "wet" macular degeneration, accounts
for about 10 percent of cases of macular degeneration. Regular (usually monthly) injections of anti-vascular
endothelial growth factor (VEGF) medications into the vitreous are often used to treat wet macular degeneration. Each
injection carries a risk of endophthalmitis similar to that of cataract surgery. A study using a Medicare database of
41,000 injections found the rate of postinjection endophthalmitis to be 0.09 percent per injection [35]. Since these
injections are usually repeated monthly for many months, there is a substantial cumulative risk of postinjection
endophthalmitis over time. In many centers, post-VEGF injection endophthalmitis is seen more often than postcataract
endophthalmitis.
The bacteriology of postinjection endophthalmitis is similar to that of postcataract endophthalmitis, except that the
proportion of cases due to viridans streptococci is much higher (30 percent versus 9 percent) [36]
(see 'Bacteriology' above). This may be due to the fact that these injections occur in an office setting rather than the
operating room. Masks are usually not worn, and patient and medical personnel often converse before and during the
procedure. Speaking transmits oral flora bacteria into the air, and these organisms can contaminate the ocular
surface; wearing a mask or avoiding talking reduces the risk of contamination [37]. In a multicenter study from France
involving over 300,000 intravitreal injections, all ophthalmologists wore surgical gowns and hats, sterile gloves, and
face masks, and the endophthalmitis rate was 0.021 percent [38]. Only 43 percent of cases were culture-positive, and
of those, coagulase-negative staphylococci caused 78 percent and streptococci only 4 percent.
BLEB-RELATED ENDOPHTHALMITIS — A filtering bleb is used to treat severe glaucoma that has failed medical
management. It is a surgically created defect in the sclera, covered only by conjunctiva, which allows excess aqueous
humor to leak out of the anterior chamber and be absorbed into the systemic circulation. It is usually placed in the
superior portion of the eye and, when the upper lid is raised, it may be seen as a small bump in the sclera. A bleb can
also rarely occur as a complication of other types of eye surgery.
A bleb may become infected (blebitis) (picture 2), and bacteria may enter the eye, resulting in endophthalmitis. The
onset of endophthalmitis is usually abrupt and typically occurs months to years following surgery. In a retrospective
study of late-onset bleb-related endophthalmitis, infection developed suddenly an average of two years
postoperatively (range one month to eight years) [39].
The incidence of endophthalmitis after bleb surgery in various studies depends on the duration of follow-up and
ranges from 0.06 to 13.2 percent [2,40,41]. One study used a Kaplan-Meier method to calculate incidence following
bleb surgery, based on retrospective data on 239 eyes in 198 patients. The probability of developing endophthalmitis
was 1.3 percent per patient-year, with a five-year probability of 7.5 percent [42].
Patients with bleb-related endophthalmitis present with sudden onset of eye pain and decreased vision. The eye is
often red with purulence over the bleb, although bleb-related endophthalmitis may occur without any signs of blebitis.
The clinical diagnosis of endophthalmitis is confirmed by vitreous cultures, although vitreous cultures were negative in
45 percent of cases in one study [43]. Cultures of the infected bleb should also be obtained. Most studies of late-onset
endophthalmitis report that 50 percent of culture-positive cases are due to streptococci (viridans streptococci or S.
pneumoniae). Haemophilus influenzae and Moraxella catarrhalis are other major pathogens [43,44]. In contrast, one
study found that streptococci caused only about 20 percent of cases, whereas S. aureus and Staphylococcus
epidermidis caused approximately 30 percent each [39]. Cases of late-onset endophthalmitis due to Enterococcus
faecalis or gram-negative bacilli other than H. influenzae or M. catarrhalis (eg, Serratia) have been reported [43],
although these cases are unusual. Early onset bleb-related endophthalmitis, developing within four to six weeks of
surgery, is uncommon, and all four culture-positive cases were caused by S. epidermidis in one study [43].
The outcome of bleb-related endophthalmitis is typically poor, with only 13 percent of 32 patients in one study
achieving 20/40 or better visual acuity [44]. Almost one-half of patients in this study were left with minimal
vision (5/200 or worse), including 10 patients (31 percent) who lost all vision in the infected eye.
No prospective study has determined optimal therapy. Although the Endophthalmitis Vitrectomy Study (EVS) is often
cited for treatment approaches to all types of endophthalmitis, this study was of postcataract endophthalmitis only. In
addition, there were design flaws in the study and results should be interpreted with caution even for postcataract
endophthalmitis. (See 'Treatment' above.)
For treatment of bleb-related endophthalmitis, the author recommends a three-pronged approach:
●Vitrectomy, rather than vitreous aspirate, based on the likelihood that infection will be caused by bacteria (eg,
streptococci) known to cause fulminant infections in the eye.
●Intravitreal vancomycin (1 mg) plus either ceftazidime (2.25 mg) or amikacin (0.4 mg). Intravitreal antibiotics
may be repeated after 48 hours if marked vitreous inflammation persists, although repeat injections of
aminoglycosides should be avoided due to concern for toxicity (macular infarction). Injection of corticosteroids
may also be considered in cases with marked vitritis, although the possible benefit is uncertain.
●The role of adjunctive systemic antibiotics in exogenous endophthalmitis is unknown (see 'Approach to
therapy' above). In bleb-related endophthalmitis, however, most patients have severe infection and we
recommend adding oral moxifloxacin 400 mg daily for 7 to 10 days. The value of adjunctive intravenous (IV)
antibiotics has not been evaluated and ophthalmologists rarely use them, but IV antibiotics should be considered
for fulminant cases.
POSTTRAUMATIC ENDOPHTHALMITIS — Endophthalmitis occurs after penetrating trauma to the globe of the eye
in 3 to 10 percent of cases [45,46]. Endophthalmitis is much more likely to occur after lacerating injury with a metal
object than after injury from glass or blunt trauma. The risk of endophthalmitis is also increased by the presence of
retained intraocular foreign bodies, delay in repair of more than 24 hours [47], and disruption of the lens [47-49].
Bacillus cereus is one of the major pathogens in most studies and causes a fulminant endophthalmitis [50]. B.
cereus endophthalmitis is characterized by abrupt onset of symptoms 12 to 24 hours after eye injury, and a ring
corneal infiltrate. Most eyes lose all vision even with prompt treatment. Other causes of posttraumatic endophthalmitis
include coagulase-negative staphylococci, streptococci, and gram-negative bacilli such
as Klebsiella and Pseudomonas and molds [51,52].
Because of the fulminant nature of posttraumatic endophthalmitis, we advocate the same aggressive treatment as
described above for bleb-related endophthalmitis. To prevent endophthalmitis after open globe (penetrating) eye
trauma, we recommend two days of systemic prophylactic antibiotics (eg, intravenous vancomycin plus either
intravenous ceftazidime or oral ciprofloxacin) after the penetrating eye injury. A review of 558 cases of open globe
injuries revealed a very low rate (0.9 percent) of endophthalmitis following a protocol that included two days of
prophylactic systemic antibiotics [53].
Molds may cause posttraumatic endophthalmitis, although this is rare in temperate climates. The presentation of mold
endophthalmitis is usually subacute. (See"Epidemiology, clinical manifestations, and diagnosis of fungal
endophthalmitis", section on 'Clinical manifestations'.)
ENDOGENOUS BACTERIAL ENDOPHTHALMITIS — Endogenous bacterial endophthalmitis is rare in the United
States and results from bacterial seeding of the eye during bacteremia. A retrospective review of a 10-year period at a
large acute care hospital and an adjoining eye specialty hospital identified only 28 cases [54].
Sources of bacteremia include endocarditis, urinary tract infections, abdominal abscesses (including liver), meningitis,
indwelling catheters, procedures such as endoscopy that cause transient bacteremia, and illicit injection drug use. In
the United States, endocarditis is a major cause of endogenous endophthalmitis, causing 40 percent of cases in one
series [54]. However, in Taiwan, Singapore, and other East Asian nations, Klebsiella pneumoniae is the major cause
of endophthalmitis associated with liver abscess, accounting for up to 60 percent of cases [55]. (See "Clinical features,
diagnosis, and treatment of Klebsiella pneumoniae infection", section on 'Endophthalmitis'.)
Patients with endogenous bacterial endophthalmitis may present with symptoms of their bacteremia or may only
complain of eye pain and decreased vision. Half of patients in one series reported no systemic symptoms and over
half saw an ophthalmologist first [54]. In another series, fewer than 20 percent of patients had fever on presentation,
and 40 percent had an unremarkable general physical examination [56]. Patients who do not have systemic symptoms
may initially be misdiagnosed as having noninfectious uveitis. Endophthalmitis should be considered in any patient
complaining of decreased vision or eye pain in the setting of possible bacteremia or injection drug use.
The diagnosis of endogenous endophthalmitis is established by clinical findings consistent with endophthalmitis (eg,
vitritis, hypopyon) in the setting of positive blood cultures or by positive vitreous or aqueous cultures in patients

presenting with endophthalmitis but who do not have a history of recent eye trauma or surgery. Blood cultures are
positive in 75 percent of those tested, as are vitreous cultures [54].
The microbiology of endogenous endophthalmitis varies with the patient population. In North America and Europe,
streptococci (S. pneumoniae, S. milleri group, group A, group B) cause 30 to 50 percent of cases, S. aureus causes
25 percent, and gram-negative bacilli cause 30 percent [54,56]. In Asia, gram-negative bacilli, especiallyKlebsiella,
cause the majority of cases of endogenous endophthalmitis [55,57].
The treatment of endogenous endophthalmitis includes intravitreal and systemic antibiotics. The duration of systemic
antibiotics should be determined by the need to treat the underlying source of bacteremia (eg, six weeks in many
cases of endocarditis). Systemic antibiotics alone will not effectively treat endophthalmitis, however, and all patients
with endogenous endophthalmitis require intravitreal antibiotic injection. Vitrectomy plus intravitreal antibiotic injection
is indicated in most cases, rather than intravitreal antibiotic injection alone, because of the virulent nature of most of
the pathogens involved. Vitrectomy debrides the vitreous and leads to better visual outcome in severe cases of
endophthalmitis. If the eye worsens over the next 24 to 48 hours, a second intravitreal antibiotic injection should be
given. A third injection may also be given if there is still no improvement after a similar time interval or if cultures from
the second vitreous sample were positive. The basis for this approach is discussed above. (See 'Intravitreal
antibiotics' above and 'Approach to therapy' above.)
FUNGAL ENDOPHTHALMITIS — Fungal endophthalmitis due to yeasts (eg, Candida albicans) is very different from
that due to molds (eg, Aspergillus or Fusarium). While Candida endophthalmitis is usually treated successfully, mold
endophthalmitis often results in the loss of vision. Fungal endophthalmitis is discussed separately.
(See "Epidemiology, clinical manifestations, and diagnosis of fungal endophthalmitis" and "Treatment of endogenous
endophthalmitis due to Candida species" and"Treatment of exogenous endophthalmitis due to Candida
species" and "Treatment of endophthalmitis due to molds".)
SUMMARY AND RECOMMENDATIONS
●Endophthalmitis refers to bacterial or fungal infection within the eye, including involvement of the
vitreous and/or aqueous humors. Most cases of endophthalmitis are exogenous, resulting from inoculation of
organisms from the outside, via trauma, eye surgery, or as an extension of keratitis (corneal infection). In such
cases, the aqueous humor may be seeded first before extension into the vitreous. The remaining cases are
endogenous, resulting from bacteremic or fungemic seeding of the eye. In endogenous endophthalmitis,
organisms usually seed the highly vascular choroid first then extend anteriorly into the vitreous.
(See 'Introduction' above.)
●Most cases of endophthalmitis are due to bacteria and present acutely. Acute bacterial endophthalmitis is a
vision-threatening condition and must be managed as an emergency. The clinical outcome depends both upon
the virulence of the infecting organism and the speed with which appropriate therapy is initiated.
(See'Introduction' above.)
●Bacterial endophthalmitis can be divided into five categories:
•Acute postcataract surgery
•Chronic pseudophakic
•Postinjection (eg, after intravitreal injection of anti-vascular endothelial growth factor [VEGF] medications)
•Bleb related
•Posttraumatic
•Endogenous (see 'Introduction' above)
Acute postcataract endophthalmitis
●Acute postcataract endophthalmitis is the most common form of endophthalmitis and, in the United States, is
almost always due to bacteria. Approximately 95 percent of cases are caused by gram-positive bacteria,
particularly coagulase-negative staphylococci (70 percent). (See 'Diagnosis' above and 'Bacteriology' above.)
●The most important component of treatment is direct injection of antibiotics into the vitreous. For severe cases,
immediate vitrectomy (followed by intravitreal injection of antibiotics) is also essential. Specific recommendations
are reviewed above. (See 'Approach to therapy' above.)
Chronic pseudophakic endophthalmitis

●Chronic pseudophakic-related endophthalmitis is a rare complication of cataract surgery; "pseudophakic" refers
to the intraocular lens. Chronic pseudophakic endophthalmitis is usually caused by Propionibacterium acnes.
Treatment requires at least vitrectomy and intravitreal vancomycin, although 50 percent of cases recur with this
treatment alone. Removal of the residual lens capsule and exchange or removal of the intraocular lens may also
be necessary for cure. Systemic antibiotics are not indicated. (See 'Chronic pseudophakic
endophthalmitis' above.)
Post-intravitreal injection endophthalmitis
●Endophthalmitis may occur after an intravitreal injection of medications to treat "wet" age-related macular
degeneration. The incidence is approximately 0.1 percent per injection; since injections are typically given
monthly for many months, the cumulative risk is substantial. The bacteriology is similar to postcataract
endophthalmitis except that the incidence of viridans streptococci is higher. This may be due to the fact that
these injections are performed in the office setting and masks are not usually worn. Having patient and physician
(and anyone in the room) either wear masks or completely refrain from talking before and during the procedure
may decrease ocular surface contamination with oral flora bacteria, such as viridans streptococci. This in turn
may decrease the rate of postinjection endophthalmitis.
Bleb-related endophthalmitis
●A filtering bleb is a surgically created defect in the sclera that is used to treat severe glaucoma that has failed
medical management. Bleb-related endophthalmitis can be caused by a range of gram-positive and gram-
negative bacteria, but streptococci, Haemophilus influenzae, and Moraxella catarrhalis are major pathogens. For
treatment, we recommend a three-pronged approach that includes vitrectomy, intravitreal vancomycin plus
either ceftazidime or amikacin, and a systemic antibiotic that achieves good intravitreal concentrations and treats
the most likely pathogens (eg, oral moxifloxacin). (See 'Bleb-related endophthalmitis' above.)
Posttraumatic endophthalmitis
●Posttraumatic endophthalmitis occurs after penetrating trauma to the globe of the eye in 3 to 10 percent of
cases. Bacillus cereus is one of the major pathogens in most studies and causes a fulminant endophthalmitis.
Because of the fulminant nature of posttraumatic endophthalmitis, we recommend immediate vitrectomy,
intravitreal vancomycin plus either ceftazidime or amikacin, and a systemic antibiotic that achieves good
intravitreal concentrations. For initial empiric treatment, the systemic antibiotic chosen should cover B. cereus.
To prevent endophthalmitis after eye trauma, we recommend initial systemic prophylactic antibiotics (eg,
intravenous vancomycin plus either intravenous ceftazidime or oral ciprofloxacin for 48 hours).
(See 'Posttraumatic endophthalmitis' above.)
Endogenous endophthalmitis
●Endogenous bacterial endophthalmitis is rare in the United States and results from bacterial seeding of the eye
during bacteremia. In North America and Europe, streptococci (Streptococcus pneumoniae, S. milleri group,
group A, group B) cause 30 to 50 percent of cases, Staphylococcus aureus causes 25 percent, and gram-
negative bacilli cause 30 percent. In Asia, gram-negative bacilli (especially Klebsiella) cause the majority of
cases. (See 'Endogenous bacterial endophthalmitis' above.)
●The treatment of endogenous endophthalmitis includes intravitreal and systemic antibiotics. Systemic
antibiotics alone will not effectively treat endophthalmitis, however, and all patients with endogenous
endophthalmitis require intravitreal antibiotic injection. Vitrectomy plus intravitreal antibiotic injection is indicated
in most cases, rather than intravitreal antibiotic injection alone, because of the virulent nature of most of the
pathogens involved. (See 'Endogenous bacterial endophthalmitis'above.)
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Javitt JC, Vitale S, Canner JK, et al. National outcomes of cataract extraction. Endophthalmitis following inpatient surgery. Arch Ophthalmol 1991; 109:1085.
2. Kattan HM, Flynn HW Jr, Pflugfelder SC, et al. Nosocomial endophthalmitis survey. Current incidence of infection after intraocular surgery. Ophthalmology 1991; 98:227.
3. Aaberg TM Jr, Flynn HW Jr, Schiffman J, Newton J. Nosocomial acute-onset postoperative endophthalmitis survey. A 10-year review of incidence and outcomes. Ophthalmology 1998; 105:1004.
4. Lundström M, Wejde G, Stenevi U, et al. Endophthalmitis after cataract surgery: a nationwide prospective study evaluating incidence in relation to incision type and location. Ophthalmology 2007; 114:866.
5. Mandelbaum S, Forster RK. Exogenous endophthalmitis. In: Ocular Immunology and Infection, Pepose JS, Holland GN, Wilhelmus KR (Eds), Mosby, St. Louis 1996. p.1298.
6. Dickey JB, Thompson KD, Jay WM. Anterior chamber aspirate cultures after uncomplicated cataract surgery. Am J Ophthalmol 1991; 112:278.
7. Sherwood DR, Rich WJ, Jacob JS, et al. Bacterial contamination of intraocular and extraocular fluids during extracapsular cataract extraction. Eye (Lond) 1989; 3 ( Pt 3):308.
8. Tervo T, Ljungberg P, Kautiainen T, et al. Prospective evaluation of external ocular microbial growth and aqueous humor contamination during cataract surgery. J Cataract Refract Surg 1999; 25:65.
9. Menikoff JA, Speaker MG, Marmor M, Raskin EM. A case-control study of risk factors for postoperative endophthalmitis. Ophthalmology 1991; 98:1761.
10. Montan PG, Koranyi G, Setterquist HE, et al. Endophthalmitis after cataract surgery: risk factors relating to technique and events of the operation and patient history: a retrospective case-control study. Ophthalmology 1998; 105:2171.
11. Bainbridge JW, Teimory M, Tabandeh H, et al. Intraocular lens implants and risk of endophthalmitis. Br J Ophthalmol 1998; 82:1312.
12. Driebe WT Jr, Mandelbaum S, Forster RK, et al. Pseudophakic endophthalmitis. Diagnosis and management. Ophthalmology 1986; 93:442.
13. Cooper BA, Holekamp NM, Bohigian G, Thompson PA. Case-control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal wounds. Am J Ophthalmol 2003; 136:300.
14. Nagaki Y, Hayasaka S, Kadoi C, et al. Bacterial endophthalmitis after small-incision cataract surgery. effect of incision placement and intraocular lens type. J Cataract Refract Surg 2003; 29:20.
15. Taban M, Behrens A, Newcomb RL, et al. Acute endophthalmitis following cataract surgery: a systematic review of the literature. Arch Ophthalmol 2005; 123:613.
16. Lalwani GA, Flynn HW Jr, Scott IU, et al. Acute-onset endophthalmitis after clear corneal cataract surgery (1996-2005). Clinical features, causative organisms, and visual acuity outcomes. Ophthalmology 2008; 115:473.
17. Behrens A, Stark WJ, Pratzer KA, McDonnell PJ. Dynamics of small-incision clear cornea wounds after phacoemulsification surgery using optical coherence tomography in the early postoperative period. J Refract Surg 2008; 24:46.
18. Taban M, Sarayba MA, Ignacio TS, et al. Ingress of India ink into the anterior chamber through sutureless clear corneal cataract wounds. Arch Ophthalmol 2005; 123:643.
19. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol 1995; 113:1479.
20. Therese KL, Anand AR, Madhavan HN. Polymerase chain reaction in the diagnosis of bacterial endophthalmitis. Br J Ophthalmol 1998; 82:1078.
21. Seal D, Reischl U, Behr A, et al. Laboratory diagnosis of endophthalmitis: comparison of microbiology and molecular methods in the European Society of Cataract & Refractive Surgeons multicenter study and susceptibility testing. J Cataract Refract Surg 2008; 34:1439.
22. Speaker MG, Milch FA, Shah MK, et al. Role of external bacterial flora in the pathogenesis of acute postoperative endophthalmitis. Ophthalmology 1991; 98:639.
23. Han DP, Wisniewski SR, Wilson LA, et al. Spectrum and susceptibilities of microbiologic isolates in the Endophthalmitis Vitrectomy Study. Am J Ophthalmol 1996; 122:1.
24. Doft BH, Kelsey SF, Wisniewski SR. Additional procedures after the initial vitrectomy or tap-biopsy in the Endophthalmitis Vitrectomy Study. Ophthalmology 1998; 105:707.
25. Ng JQ, Morlet N, Pearman JW, et al. Management and outcomes of postoperative endophthalmitis since the endophthalmitis vitrectomy study: the Endophthalmitis Population Study of Western Australia (EPSWA)'s fifth report. Ophthalmology 2005; 112:1199.
26. Gower EW, Keay LJ, Stare DE, et al. Characteristics of Endophthalmitis after Cataract Surgery in the United States Medicare Population. Ophthalmology 2015; 122:1625.
27. Hooper CY, Lightman SL, Pacheco P, et al. Adjunctive antibiotics in the treatment of acute bacterial endophthalmitis following cataract surgery. Acta Ophthalmol 2012; 90:e572.
28. Lott MN, Fuller JJ, Hancock HA, et al. Vitreal penetration of oral moxifloxacin in humans. Retina 2008; 28:473. 29. Fiscella RG, Lai WW, Buerk B, et al. Aqueous and vitreous penetration of linezolid (Zyvox) after oral
administration. Ophthalmology 2004; 111:1191. 30. Piest KL, Kincaid MC, Tetz MR, et al. Localized endophthalmitis: a newly described cause of the so-called
toxic lens syndrome. J Cataract Refract Surg 1987; 13:498. 31. Adán A, Casaroli-Marano RP, Gris O, et al. Pathological findings in the lens capsules and intraocular lens in
chronic pseudophakic endophthalmitis: an electron microscopy study. Eye (Lond) 2008; 22:113. 32. Winward KE, Pflugfelder SC, Flynn HW Jr, et al. Postoperative Propionibacterium endophthalmitis. Treatment
strategies and long-term results. Ophthalmology 1993; 100:447. 33. Clark WL, Kaiser PK, Flynn HW Jr, et al. Treatment strategies and visual acuity outcomes in chronic
postoperative Propionibacterium acnes endophthalmitis. Ophthalmology 1999; 106:1665.

34. Aldave AJ, Stein JD, Deramo VA, et al. Treatment strategies for postoperative Propionibacterium acnes endophthalmitis. Ophthalmology 1999; 106:2395.
35. Day S, Acquah K, Mruthyunjaya P, et al. Ocular complications after anti-vascular endothelial growth factor therapy in Medicare patients with age-related macular degeneration. Am J Ophthalmol 2011; 152:266.
36. McCannel CA. Meta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents: causative organisms and possible prevention strategies. Retina 2011; 31:654.
37. Doshi RR, Leng T, Fung AE. Reducing oral flora contamination of intravitreal injections with face mask or silence. Retina 2012; 32:473.
38. Dossarps D, Bron AM, Koehrer P, et al. Endophthalmitis After Intravitreal Injections: Incidence, Presentation, Management, and Visual Outcome. Am J Ophthalmol 2015; 160:17.
39. Waheed S, Ritterband DC, Greenfield DS, et al. New patterns of infecting organisms in late bleb-related endophthalmitis: a ten year review. Eye (Lond) 1998; 12 ( Pt 6):910.
40. Greenfield DS, Suñer IJ, Miller MP, et al. Endophthalmitis after filtering surgery with mitomycin. Arch Ophthalmol 1996; 114:943.
41. Kim EA, Law SK, Coleman AL, et al. Long-Term Bleb-Related Infections After Trabeculectomy: Incidence, Risk Factors, and Influence of Bleb Revision. Am J Ophthalmol 2015; 159:1082.
42. DeBry PW, Perkins TW, Heatley G, et al. Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol 2002; 120:297.
43. Ciulla TA, Beck AD, Topping TM, Baker AS. Blebitis, early endophthalmitis, and late endophthalmitis after glaucoma-filtering surgery. Ophthalmology 1997; 104:986.
44. Kangas TA, Greenfield DS, Flynn HW Jr, et al. Delayed-onset endophthalmitis associated with conjunctival filtering blebs. Ophthalmology 1997; 104:746.
45. Soheilian M, Rafati N, Mohebbi MR, et al. Prophylaxis of acute posttraumatic bacterial endophthalmitis: a multicenter, randomized clinical trial of intraocular antibiotic injection, report 2. Arch Ophthalmol 2007; 125:460.
46. Sabaci G, Bayer A, Mutlu FM, et al. Endophthalmitis after deadly-weapon-related open-globe injuries: risk factors, value of prophylactic antibiotics, and visual outcomes. Am J Ophthalmol 2002; 133:62.
47. Thompson JT, Parver LM, Enger CL, et al. Infectious endophthalmitis after penetrating injuries with retained intraocular foreign bodies. National Eye Trauma System. Ophthalmology 1993; 100:1468.
48. Thompson WS, Rubsamen PE, Flynn HW Jr, et al. Endophthalmitis after penetrating trauma. Risk factors and visual acuity outcomes. Ophthalmology 1995; 102:1696.
49. Jonas JB, Budde WM. Early versus late removal of retained intraocular foreign bodies. Retina 1999; 19:193. 50. Miller JJ, Scott IU, Flynn HW Jr, et al. Endophthalmitis caused by Bacillus species. Am J Ophthalmol 2008;
145:883. 51. Abu el-Asrar AM, al-Amro SA, al-Mosallam AA, al-Obeidan S. Post-traumatic endophthalmitis: causative
organisms and visual outcome. Eur J Ophthalmol 1999; 9:21. 52. Alfaro DV, Roth DB, Laughlin RM, et al. Paediatric post-traumatic endophthalmitis. Br J Ophthalmol 1995;
79:888. 53. Andreoli CM, Andreoli MT, Kloek CE, et al. Low rate of endophthalmitis in a large series of open globe
injuries. Am J Ophthalmol 2009; 147:601. 54. Okada AA, Johnson RP, Liles WC, et al. Endogenous bacterial endophthalmitis. Report of a ten-year
retrospective study. Ophthalmology 1994; 101:832. 55. Wong JS, Chan TK, Lee HM, Chee SP. Endogenous bacterial endophthalmitis: an east Asian experience and
a reappraisal of a severe ocular affliction. Ophthalmology 2000; 107:1483. 56. Binder MI, Chua J, Kaiser PK, et al. Endogenous endophthalmitis: an 18-year review of culture-positive cases
at a tertiary care center. Medicine (Baltimore) 2003; 82:97. 57. Jackson TL, Eykyn SJ, Graham EM, Stanford MR. Endogenous bacterial endophthalmitis: a 17-year
prospective series and review of 267 reported cases. Surv Ophthalmol 2003; 48:403.

Eye anatomy in cross section
Hypopyon in endophthalmitis
A postoperative eye showing endophthalmitis with conjunctival injection and a hypopyon, the layering
of white blood cells in the anterior chamber. Reproduced with permission from the department of
Ophthalmology and Vision Science, University of Toronto. Graphic 59911 Version 4.0
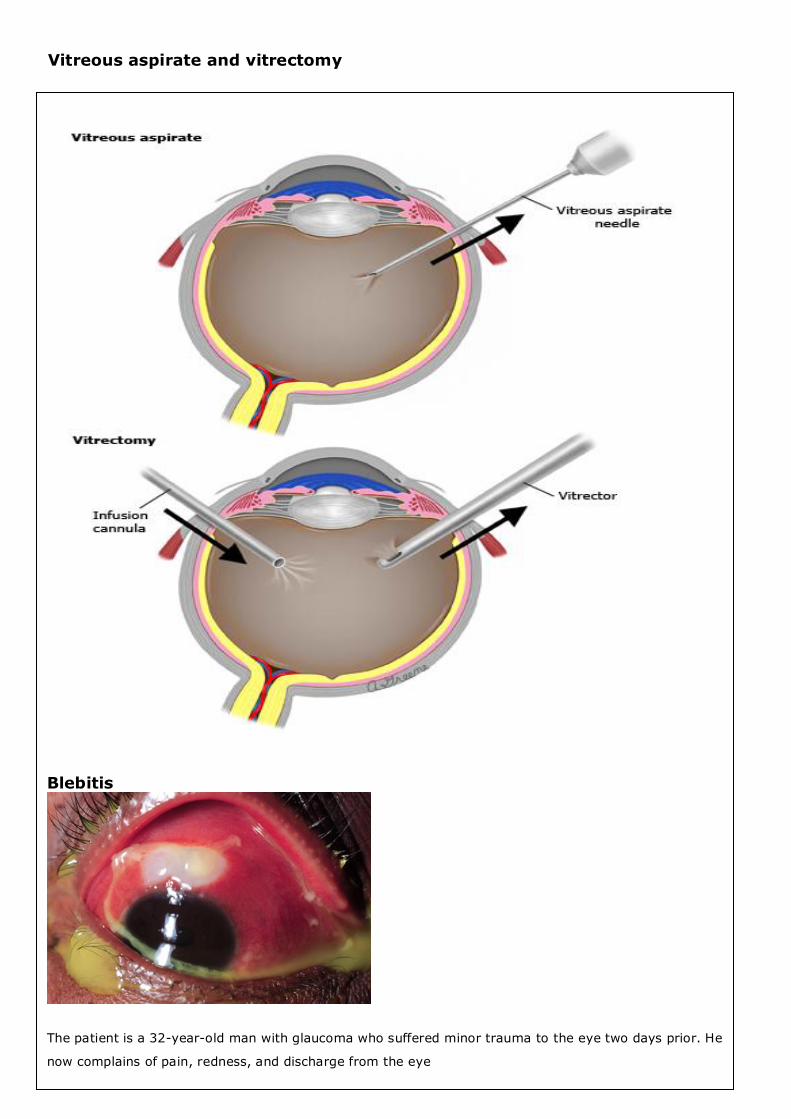
Vitreous aspirate and vitrectomy
Blebitis
The patient is a 32-year-old man with glaucoma who suffered minor trauma to the eye two days prior. He
now complains of pain, redness, and discharge from the eye