department of surgery queen elizabeth hospital dr cheng mina
TRANSCRIPT
Department of SurgeryQueen Elizabeth Hospital
Dr Cheng Mina

Questions to answerWho
Who deserves urgent referral?Who needs operation?
WhenWhen to intervene?
WhatWhat to do?

Carotid symptomsHemimotor / hemisensory signsTransient monocular visual loss (Amaurosis fugax)
AsymptomaticCarotid bruitNo evidence that presence or absence of bruit or quality of
bruit correlate with degree of stenosis
J.H. Hammond, R.P. Eisinger: Carotid bruits in 1000 normal subjects. Arch Intern Med. 109, 1962, 563, 5.P.A. Wolf, W.B. Kannel, P. Sorlie, et al.: Asymptomatic carotid bruit and risk of stroke: the Framingham Study.
JAMA. 245, 1981, 1442, 5.
Who deserves urgent referral Risk of stroke after a TIA only 1–2% at 7 days
and 2–4% at 30 daysM.F. Giles, P.M. Rothwell: The need for emergency treatment of transient
ischaemic attack and minor stroke. Expert Rev Neurother. 5, 2005, 203, 10.
Naylor: Time is brain. The Surgeon. 5, 2007, 23–30.
Evidence suggests that these data dangerously underestimate the true risk
P.M. Rothwell, C.P. Warlow: Timing of TIAS preceding stroke: time window for prevention is very short. Neurology. 64, 2005, 817, 20.PubMed
M.F. Giles, P.M. Rothwell: Risk of stroke early after transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol. 6, 2007, 1063, 72.

Who deserves urgent referral Review of 10126 patientsAfter TIA 2 day stroke risk 3.1% 7 day stroke risk 5.2%
ABCD system to predict the 7-day stroke risk after TIA (Max score 6)
A Age > 6oB SBP > 140mmHg C Clinical features ( weakness, speech disturbance)D Duration (< 10 min, 10-59 min, >60 min)
7-day stroke risk <3 -> 0% 4 -> 2% 5 -> 16% 6-> 35%
P.M. Rothwell, M.F. Giles, E. Flossman, et al.: A simple score (ABCD) to identify individuals at high early risk of stroke after transient ischaemic attack. Lancet. 366, 2005, 29–36
Who deserves urgent referralUK Department of Health’s National Stroke
Strategy November 2007 Carotid imaging <24 hours after TIA if ABCD
score ≥4
The National Stroke Strategy; www.dh.gov.uk/stroke.

Duplex USGCombination of B mode real-time imaging and waveform analysis by pulsed wave dopplerIdentifies up to 95% of carotid lesionsSensitivity 89% for 70-99% stenosisNon-invasiveOperator dependentSociety of Radiologists in USG Consensus ConferenceUSG criteria for degree of stenosisBased on the North American Symptomatic Carotid
Endarterectomy Trial (NASCET) measurement methodICA PSV, ICA EDV, plaque estimate, ICA/CCA PSV ratio
Grant EG, Benson CB, Moneta GL et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis– Society of Radiologists in Ultrasound Consensus Conference. Radiology 2003; 229:340–6.

3 methods to measure ICA stenosis NASCET ECSTCommon carotid
method“Gold standard” Catheter angiography
stroke/death risk 1.5%
Not routine work up nowadays

Contrast enhanced MRASensitivity 95% and specificity 79%
for 70–99% stenosesSensitivity 100% if combined with
USGNon-invasiveGadolinium causes nephrogenic
systemic fibrosis in 3-5% of patients with renal impairment
I. Borisch, M. Horn, B. Butz, et al.: Preoperative evaluation of carotid artery stenosis: comparison of contrast-enhanced MR angiography and duplex
sonography with digital subtraction angiography. Am J Neuroradiol. 24, 2003, 1117, 22.
D.C. Johnston, J.D. Eastwood, T. Nguyen, et al.: Contrast-enhanced magnetic resonance angiogrophy of carotid arteries. Utility in routine clinical practice.
Stroke. 33, 2002, 2834, 8.
Best medical treatmentBP < 140/90 mmHgDM controlSmoking cessationAvoid heavy consumption of alcoholRegular physical activityLow salt, low saturated fat, high fruit and
vegetable diet rich in fibreReduce weight if BMI elevated
The European Stroke Initiative Executive Committee and the EUSI Writing Committee: European Stroke Initiative recommendations for stroke management – Update 2003. Cerebrovasc Dis. 16, 2003, 311,
37.
Role of statin therapyThe British Heart Protection Study
20000 patients with angina, stroke/ TIA, DM or claudication
40 mg simvastatin daily25% RRR in any major coronary event, stroke and need of
revascularization at 5 yearsIrrespective of age, gender or cholesterol level
Heart Protection Study Collaborative Group: MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20536 high-risk individuals: a randomised placebo controlled trial. Lancet. 360, 2002, 7–22.
European Stroke InitiativeAll patients (symptomatic/ asymptomatic) should take
statin
The European Stroke Initiative Executive Committee and the EUSI Writing Committee: European Stroke Initiative recommendations for stroke management – Update 2003. Cerebrovasc Dis. 16, 2003, 311, 37.

Antiplatelet agentsAspirin is the first line agentReduces long term risk of stroke by 25%Low dose is good enough (80 to 325 mg daily)Clopidogrel(Plavix) 75 mg is the second line agent
Antiplatelet Trialists Collaboration: Secondary prevention of vascular disease by prolonged anti-platelet treatment.
Br Med J. 296, 1988, 320, 31.
NICE (The National Institute for Health and Clinical Excellence)Combination of aspirin and dipyridamole (Persantin)
for 3 years in stroke/TIA patients on conservative treatment
Only aspirin after 3 years or after CEA
NICE Technology Appraisal Guidance 90: In Vascular disease – clopidogrel and dipyridamole: quick reference guide. 2005, 25 May.
Who needs operation CEASymptomaticCarotid Endarterectomy Trialists Collaboration
(CETC)Combined data from 3 studies
ECST (European Carotid Surgery Trial)NASCET (North American Symptomatic Carotid
Endarterectomy Trial)VA (Veteran’s Affairs)
5 years outcomes, > 6000 patients
Carotid Endarterectomy Trialists Collaboration: P.M. Rothwell, M. Eliasziw, S.A. Gutnikov, et al.: Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. for the Lancet.
361, 2003, 107, 16.Carotid Endarterectomy Trialists Collaboration: P.M. Rothwell, M. Eliasziw, S.A. Gutnikov, et al.: Endarterectomy
for symptomatic carotid stenosis in relation to clinical subgroups and timing of surgery. for the Lancet. 363, 2004, 915, 24.
P.M. Rothwell, M. Eliasziw, S.A. Gutnikov, et al.: Sex difference in the effect of time from symptoms to surgery on benefit from carotid endarterectomy for transient ischaemic attack and minor stroke. Stroke. 35, 2004, 2855,
61.
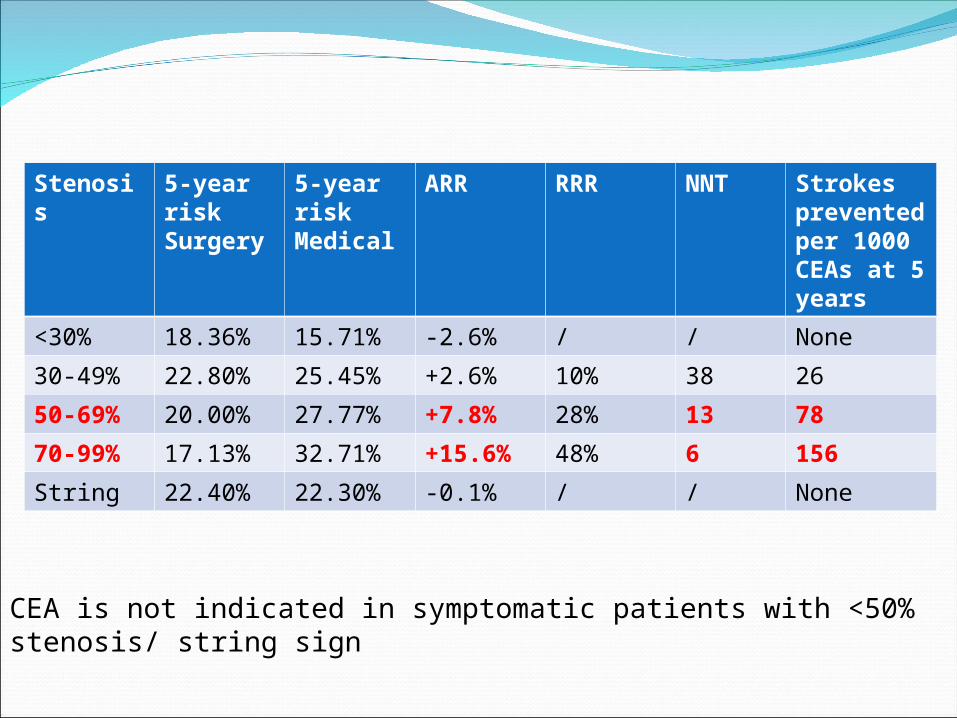
Stenosis
5-year riskSurgery
5-year riskMedical
ARR RRR NNT Strokes prevented per 1000 CEAs at 5 years
<30% 18.36% 15.71% -2.6% / / None
30-49% 22.80% 25.45% +2.6% 10% 38 26
50-69% 20.00% 27.77% +7.8% 28% 13 78
70-99% 17.13% 32.71% +15.6% 48% 6 156
String 22.40% 22.30% -0.1% / / None
CEA is not indicated in symptomatic patients with <50% stenosis/ string sign

When to intervene
• Maximum risk of stroke is within first 7 to 14 days• Maximum benefit to prevent stroke if < 2 weeks
Coull AJ, Lovett JK, Rothwell PM. Population based study of early risk of stroke after transient ischaemic attack or minor stroke: implications for public education and organization of services. Br Med J 2004; 328:326–8.
Naylor AR. Time is brain! The Surgeon 2007; 5:23–30.

Effect of delay to CEA on 5 year prevention of ipsilateral stroke
< 2 weeks 2 to 4 weeks
4 to 12 weeks
>12 weeks
ARR by CEA at 5 years
18.5%
9.8% 5.5% 0.8%
NNT 5
10 18
125
Strokes prevented per 1000 CEA
185 98 55 8
Unnecessary procedure
815 902 945 992Reanalysis of CETC data in patients with NASCET 50–99% stenoses (i.e. ECST 70–99%) undergoing CEA

Delay to surgery concept • Early CEA is associated with procedural risk
• Retrospective review of 1046 symptomatic patients undergoing CEA in New York
• 30 day stroke/death risk • 5.1% <4 weeks 1.6 % >4 weeks
C.B. Rockman, T. Maldonado, G.R. Jacobowitz, et al.: Early endarterectomy in symptomatic patients is associated with poorer perioperative outcomes. J Vasc Surg. 44, 2006, 480, 7.
CETC suggests that even if a surgeon operated <2 weeks with a 10% procedural risk, he/she was likely to prevent more strokes than by waiting >12 weeks and then operating with a 0% risk

Asymptomatic carotid stenosis5 to 10% population >65 years
12% with PVD
25% with HT
Prophylactic surgery to prevent stroke
Two important studies
ACAS Asymptomatic Carotid Atherosclerosis Study 1995
ACST Asymptomatic Carotid Surgery Trial 2004
ACAS 1995/ ACST 2004ACAS, 1662 patientsCEA can reduce ipsilateral strokeCriticism:
30 day death/stroke only 2.3% (i.e. not generalizable)
No benefit in womenCEA did not prevent disabling stroke
ACST, 3120 patientsCEA significantly reduced risk of fatal and
disabling strokeSignificant benefit only in patients <75 years

ARR NNT 30 day stroke
Number of stroke prevented at 5 year per 1000 CEA
NASCET 70 to 99%
17% 5.9 5.4% (1.1% death)
170
ACAS70 to 99%
5% 20 2.3% 50
ACST70 t0 99%
5.3% 19 2.8% 53

CEA or carotid stenting?CAVATAS, SPACE, EVA-3S, ICSS
Widely criticizedE.g. No EPD or not mandatory, no lead-in phase
CREST (Stenting versus Endarterectomy for Treatment of Carotid Artery Stenosis) 20102522 patients from 2000 to 2008 in USABoth symptomatic and asymptomatic carotid
stenosisSingle carotid stent with EPD systemLead-in phase

CEA or carotid stenting?CREST
No significant difference in stroke + MI + death during perioperative period (CAS 5.2%, CEA 4.5%; P = 0.38) and after 4 years (CAS 7.2%, CEA 6.8%; P = 0.51)
More perioperative stroke in CAS group (CAS 4.1%, CEA 2.3%; P = 0.01)
More perioperative MI in CEA group(CAS 1.1%, CEA 2.3%; P = 0.03)
Similar 4-year ipsilateral stroke rate (CAS 2%, CEA 2.4%; P = 0.85)
Younger patients CAS better, older patients CEA better

Individualized treatmentFor CAS
Previous neck surgeryPrevious neck
irradiationContralateral vocal cord
palsyRestenosis after CEAHigh carotid bifurcation
(above C2)Extension of plaque to
intracranial ICA/ proximal CCA below clavicle
For CEA
Poor femoral vessel for access
Heavily calcified or angulated aortic arch
Heavily calcified or markedly tortuous carotid artery
ConclusionWho
Who deserves urgent referral? Who needs operation?
WhenWhen to intervene?
WhatWhat to do?

ConclusionWho
Who deserves urgent referral? ABCD scoreWho needs operation?
WhenWhen to intervene?
WhatWhat to do?

ConclusionWho
Who deserves urgent referral? ABCD scoreWho needs operation? Symptomatic 70-99% +/- Symptomatic 50-69%, Asymptomatic 70-99%
WhenWhen to intervene?
WhatWhat to do?

ConclusionWho
Who deserves urgent referral? ABCD scoreWho needs operation? Symptomatic 70-99% +/- Symptomatic 50-69%, Asymptomatic 70-99%
WhenWhen to intervene? < 2 weeks
WhatWhat to do?

ConclusionWho
Who deserves urgent referral? ABCD scoreWho needs operation? Symptomatic 70-99% +/- Symptomatic 50-69%, Asymptomatic 70-99%
WhenWhen to intervene? < 2 weeks
WhatWhat to do? Individualized treatment

Thank You

Stroke Commonest cause of death after CAD and cancerAcute loss of focal cerebral function >24 hrs with
vascular cause80% ischaemic20% haemorrhagic (intracerebral/ subarachnoid)80% of ischaemic stroke affect carotid territory

Aetiology of carotid territory infarction
Thromboembolism from ICA 50%Small vessel disease 25%Cardiac brain embolism 15%Haematological disease 5%Non-atheromatous disease 5%
Dennis MS, Bamford JM, Sandercock PAG et al. Incidence of transient ischaemic attacks in Oxfordshire, England. Stroke
1989; 20:333–9.

Thromboembolism from ICAMiddle cerebral vessel territoryAtherosclerotic plaque formationStenosis at ICA originAcute disruption of plaqueRupture, ulceration, intraplaque
haemorrhage Exposure of inner core of thrombogenic
subendothelial collagenThrombus formation

Asymptomatic carotid stenosisCarotid bruit4% over 45 years old, 12% over 60 years old70% symptomatic ICA stenosis of 70 to 90% 40% symptomatic ICA stenosis of 90 to 99%30% ICA occlusion No evidence that presence or absence of bruit or
quality of bruit correlate with degree of stenosisBruit not due to ICA disease
Systolic cardiac murmurs, bruit from vertebral and ECA
J.H. Hammond, R.P. Eisinger: Carotid bruits in 1000 normal subjects. Arch Intern Med. 109, 1962, 563, 5.
P.A. Wolf, W.B. Kannel, P. Sorlie, et al.: Asymptomatic carotid bruit and risk of stroke: the Framingham Study.
JAMA. 245, 1981, 1442, 5.
Carotid symptomsHemimotor / hemisensory signsTransient monocular visual loss (Amaurosis fugax)
DDX: epilepsy, brain tumour/ aneurysm, hypoglycemia, migraine
TIA precipitated by hot bath, heavy meal and exercise -> Significant carotid stenosis should be suspected

Guidelines for imaging The National Guideline for Stroke 2004
Duplex finding confirmed with MRA before operation
Or Second duplex if conservative treatment offered
J.M. Wardlaw, F.M. Chappell, M. Stevenson, et al.: Accurate, practical and cost-effectiveassessment of carotid stenosis in the UK. Health Technol Assess. 10, 2006, 1–182, iii–iv, ix–x.
The Society of Radiologists in USG ConsensusAll vascular laboratories should have a system for
quality assuranceNASCET measurement is mandatory
V. Vidak, A. Hebrang, B. Brkljacic, et al.: Stenotic occlusive lesions of internal carotid artery in diabetic patients. Coll Antropol. 31, 2007, 775, 80.
