department of physiology and pharmacology imperfection of ... · 10/31/2014 2 drugs and ckd •...
TRANSCRIPT

10/31/2014
1
Decreased Nuclear Receptor Activity Mediates
Downregulation of Drug Metabolizing
Enzymes in Chronic Kidney Disease Through
Epigenetic Modulation
October 20, 2014
Department of Physiology and Pharmacology
Brad Urquhart, PhDAssistant Professor
Department of Physiology and Pharmacology
Department of Medicine (Nephrology, Clinical Pharmacology)
Department of Paediatrics
Lawson Health Research Institute
Imperfection of Drug Therapy
Disease
Environment
Genetics
•• AbsorptionAbsorption
•• DistributionDistribution
•• Metabolism Metabolism
•• ExcretionExcretion
Factors Mediating Factors Mediating
Drug DispositionDrug Disposition
Yeung et al. Kidney International (2014)
Chronic Kidney Disease (CKD)Stage Description GFR
(ml/min/1.72m2)
1 Kidney damage with normal or ↑GFR
≥ 90
2 Kidney damage with mild ↓GFR
60–89
3 Moderate ↓GFR 30–59
4 Severe ↓GFR 15–29
5 Kidney failure <15 or anuric
Am J Kidney Dis.
2011;57(3)(suppl 2):S32-S56
Pe
rce
nt
of
po
pu
lati
on
• Characterized by a progressive
decline in renal function over time.
• Major causes of CKD include diabetes and renal vascular
disease (including high blood pressure)
• CKD is estimated to affect between 1.9 million and 2.3
million Canadians

10/31/2014
2
Drugs and CKD
• Patients with CKD take 7-12
medications concurrently to
control a variety of co-
morbidities.
• These patients have an increased
incidence of adverse drug
events, often due to increased
blood drug concentrations.
• Many drugs are excreted by the
kidney so GFR adjusted dosing in
patients with CKD is common.
Metabolism
Renal
Bile
Drug Elimination
Wienkers and Heath (2005) Nat Rev Drug Discov. 4 (10) 825-33
Does CKD impact hepatic drug metabolism?
CYP3A
CYP2D6
CYP2E1
CYP1A
CYP2C
Shimada et al. (1994) J. Pharmacol. Exp. Ther. 270 (1) 414-23
Cytochrome P450 Mediated Drug Metabolism
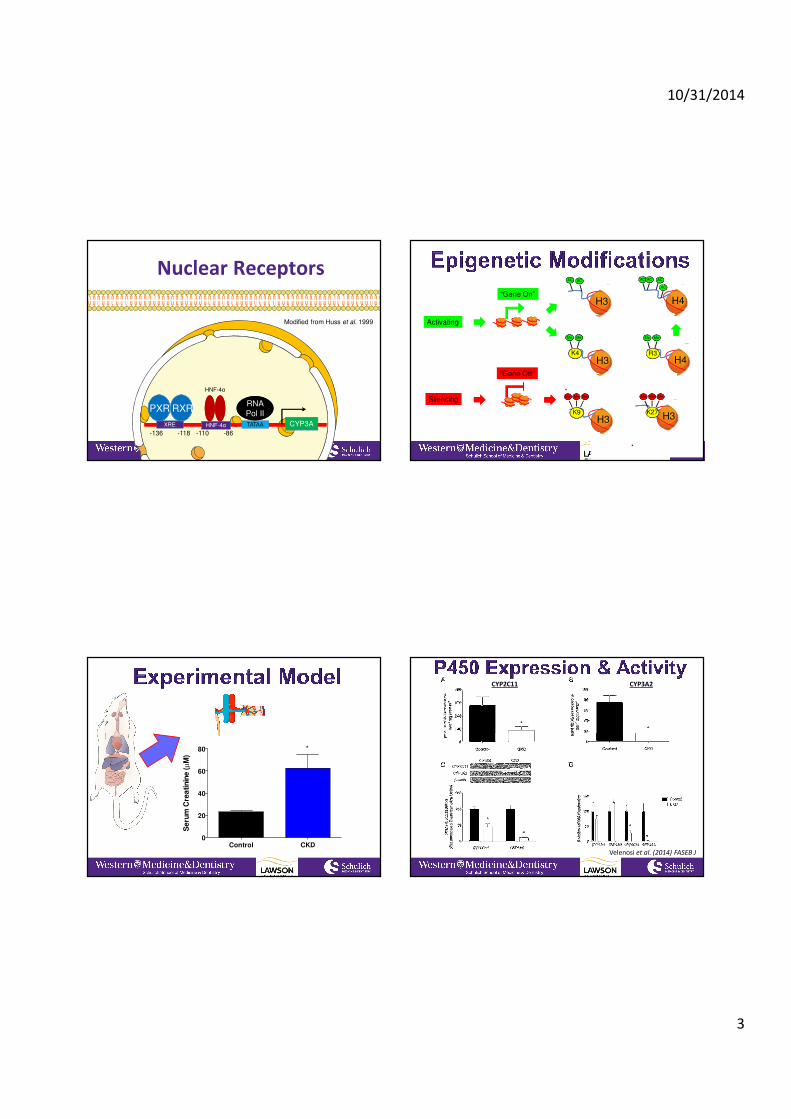
Nuclear Receptor and Epigenetic Changes in CYP3A
and CYP2C Mediated Metabolism in CKD.
HypothesisHypothesis
Altered drug metabolism in CKD is secondary to decreasednuclear receptor binding to the CYP3A and CYP2Cpromoter which is associated with histone modulation.
ObjectiveObjective
1. To determine nuclear receptor binding in CKD.
2. To investigate the epigenetic modulation of hepatic drugmetabolizing enzymes in CKD.
3. To evaluate uremic toxins that may downregulatehepatic CYP3A.
10/31/2014
3
CYP3ATATAAXRE HNF-4α
HNF-4α
PXR RXR
Modified from Huss et al. 1999
-118-136 -110 -86
RNA
Pol II
RNA
Pol II
Nuclear Receptors
H3
AC AC
H4
AC AC
AC
AC
Activating
Silencing
H3K9
MeMeMe
H3K4
MeMe
“Gene On”
“Gene Off”
H4R3
MeMe
H3K27
MeMeMe
Control CKD0
20
40
60
80
Se
rum
Cre
atin
ine
(µ
M)
*
Velenosi et al. (2014) FASEB J
CYP2C11 CYP3A2

10/31/2014
4
Velenosi et al. (2014) FASEB JVelenosi et al. (2014) FASEB J
Velenosi et al. (2014) FASEB J

10/31/2014
5
Mechanism?
mRN
A
Enzym
e
CONTROL UREMIA
mRN
A
HNF-4αPXR RXR
CYPCYPAc Ac Ac
Enzym
e
RNA Pol IIHNF-4αPXR RXR
CYPCYPAc Ac Ac
RNA Pol II
Possible Mechanism For Hepatic Drug Metabolizing Enzyme DownPossible Mechanism For Hepatic Drug Metabolizing Enzyme Down--
regulation in CKD.regulation in CKD.Metabolomics
• Hundreds of uremic toxins
accumulate in kidney disease.
• Do any of them accumulate in
the liver?
• Sensitive QTOF mass
spectrometer: can quantify
and identify small molecules.
• Application to drug toxicity :
pharmacometabolomics
XEVOXEVO--G2G2--S Mass SpectrometerS Mass Spectrometer
Metabolomic InvestigationControl
Chronic Kidney Disease
Homogenize in acetonitrile
Homogenize in acetonitrile
UPLC-MS
-40
-30
-20
-10
0
10
20
30
40
-80 -70 -60 -50 -40 -30 -20 -10 0 10 20 30 40 50 60 70 80
t[2
]O
t[1]P
Scores Plot: Control vs. CKD
CKD
Control
EZinf o 2 - CKD AST-120 Rat Liver Neg Mode Control v s CKD (M2: OPLS-DA) - 2014-09-29 14:03:10 (UTC-5)
Hennop, Velenosi et al. unpublished

10/31/2014
6
-1.0
-0.8
-0.6
-0.4
-0.2
-0.0
0.2
0.4
0.6
0.8
1.0
-0.1 0.0 0.1
p(c
orr
)[1
]P (
Co
rre
lati
on
)
p[1]P (Loadings)
S-Plot (Control = -1, CKD = 1)
EZinf o 2 - CKD AST-120 Rat Liv er Neg Mode Control vs CKD (M2: OPLS-DA) - 2014-09-29 14:10:14 (UTC-5)
Metabolomics of Liver Samples in CKD Conclusions and Future Directions
CONCLUSIONSCONCLUSIONS
• PXR and HNF4α binding to CYP2C11 and CYP3A2promoters is decreased in CKD.
• Changes in histone acetylation are associated withdecreased CYP2C11 and CYP3A2 expression in CKD.
FUTURE DIRECTIONSFUTURE DIRECTIONS
• Metabolomic investigation to determine which uremic toxins are elevated in the liver.
AcknowledgementsAcknowledgements
Urquhart lab
• Dave Feere, MSc
• Anzel Hennop
• Andrew Kucey
• Alvin Tieu
• Dr. Ben Thomson
• Tom Velenosi
• Andrew Wong
Collaborators
• Dr. Tom Nolin (University of
Pittsburgh)
• Dr. Andrew House
• Linda Asher, RN
Dr. Ben Thomson
David Feere, MScTom Velenosi,
PhD Candidate
Cocktail:• CMPF
• Creatinine• P-Cresyl sulfate
• Indoxyl Sulfate• Guanidinosuccinic acid
• Hippuric acid• Indole-3-acetic acid
• Methylguanidine• Urea
DM
SO
Indoxy
l Sul
fate
Cock
tail
0
50
100
150
Rela
tive m
RN
A E
xp
ressio
n
* *
Velenosi et al. unpublished

10/31/2014
7
-2 0 2 40
50
100
150
Log [Indoxyl Sulfate] µM
Re
lati
ve
mR
NA
Ex
pre
ss
ion
(% C
on
tro
l)
Normal Uremia
-2 0 2 40
50
100
150
**
Log [Indoxyl Sulfate] µM
Re
lati
ve
mR
NA
Ex
pre
ss
ion
(% C
on
tro
l)
NO FBS Media FBS Media
Velenosi et al. unpublished
Mechanism?
I
mRN
A
Enzym
e
CONTROL UREMIA
mRN
A
HNF-4αPXR RXR
CYPCYPAc Ac Ac
Enzym
e
RNA Pol IIHNF-4αPXR RXR
CYPCYPAc Ac Ac
RNA Pol II
Possible Mechanism For Hepatic Drug Metabolizing Enzyme DownPossible Mechanism For Hepatic Drug Metabolizing Enzyme Down--
regulation in CKD.regulation in CKD.
Indoxyl Sulfate?