department of human services patient flow collaborative learning session 4 breakout session 1 room...
TRANSCRIPT
Department of Human Services
Patient Flow Collaborative Learning Session 4
Breakout session 1
Room M7 and M8
Stephen Vale and Ruth Smith
Department of Human Services
Breakout session 1
Room M7 and M8 9.50 – 10.35
Wendy WoodDirector of Nursing and General Manager, Surgical OncologyPeter MacCallum Cancer Centre
5th May, 2005
Achieving innovations: an executive perspective

An Executive PerspectiveAn Executive Perspective
• Critical Success Factors• Barriers• Effective Project Management• Communication• Managing Resistance• Ongoing Measurement• Making Innovation Mainstream
Critical Success Factors in Critical Success Factors in sustaining organisational changesustaining organisational change
• Executive engagement and support is a critical success factor in sustained organisational change
• Ownership of the change process• Facilitation and access to data• Understanding of resource limitations
and constraints, “no you can’t knock down the Admin wing”
BarriersBarriers
• Getting the team together• Lack of Information• Impatience• Preconceived ideas & bad memories (long)• Negativity of non participating staff• Lack of resources to test the innovation• Rushing the change process• Conflicting goals
Effective Project Effective Project ManagementManagement
• Front line staff own and manage the process and the innovation
• Line manager supports the process, organises meetings and keeps the team focussed
• Small project team, large reference group• Executive sponsor is accessible and ensures
commitment and empowerment of the process
• Scope of project is known at the beginning
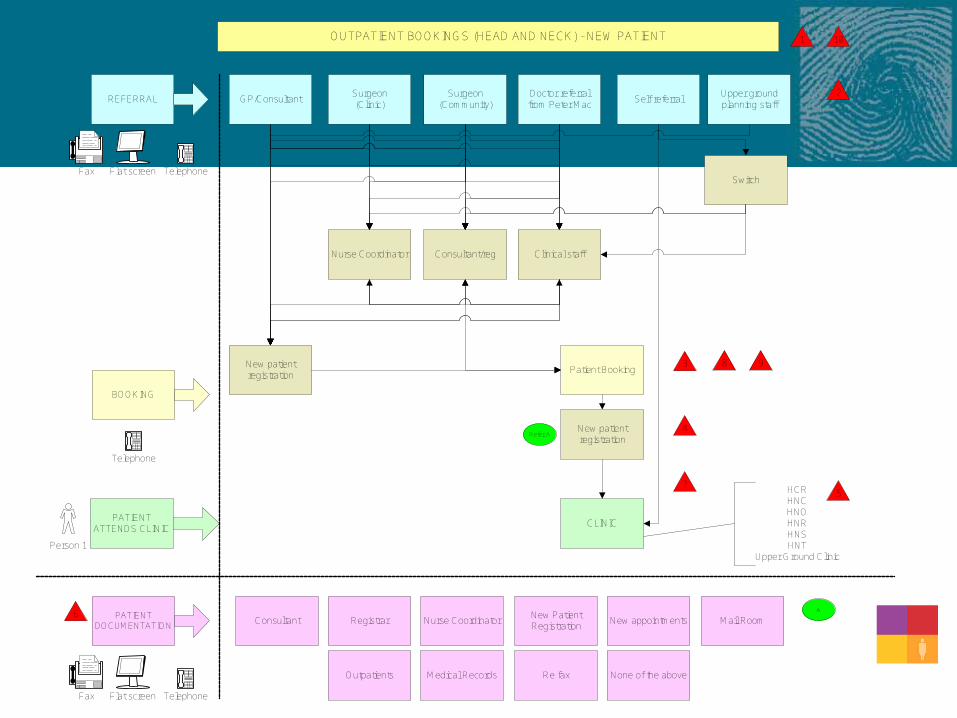
OUTPATIENT BOOKINGS (HEAD AND NECK) - NEW PATIENT
GP/ConsultantSurgeon (Clinic)
Surgeon (Community)
Doctor referral from Peter Mac
Self referralUpper ground planning staff
REFERRAL
New patient registration
Nurse Coordinator Consultant/reg Clinical staff
Patient Booking
Switch
CLINIC
BOOKING
PATIENT ATTENDS CLINIC
PATIENT DOCUMENTATION
Consultant Registrar Nurse CoordinatorNew Patient Registration
New appointments Mail Room
Outpatients Medical Records Re fax None of the above
HCRHNCHNOHNRHNSHNT
Upper Ground Clinic
New patient registration
1
Flat screen TelephoneFax
Flat screen TelephoneFax
Person 1
Telephone
10
2
3
4
5
6
7
8 9
Refer A
A

Referral Source
Switch
Triage Nurse
Booked to appropriate clinic
Head & NeckNew Patient booking
Clerk
All relevant info collected prior
to clinic
Patient arrives at appropriate clinicwith all relevant information
Booking confirmed with referral source
& patient
HCRHNCHNOHNRHNSHNT
CommunicationCommunication
• Use every tool in ‘the book’• Team meetings• Written material including hard data &
diagnostics• Newsletter publication• Presentation at Executive & staff forums• Sharing & Celebration is infectious
Improving Flow for Combined Improving Flow for Combined Modality PatientsModality Patients
• While undergoing Radiotherapy Treatment, test results and progress notes are reviewed by the Radiation Therapy Team to evaluate the therapeutic response to the treatment
• This meant that the medical record was often being used in a meeting while the patient was waiting to undergo concurrent chemotherapy, delaying commencement of infusion.
• If patient histories are required in more than 1 area simultaneously, e.g. for delivery of chemotherapy and for chart review, the area where the patient is present will always take priority.
Managing ResistanceManaging Resistance
• Do the hard yards up front• Don’t rush any component of the process• Listen and report back aligned with the
specific concerns• Engage the loudest protestors closely• Address their problems• Don’t be afraid to admit you were wrong

Ongoing MeasurementOngoing Measurement
• Death by measurement! Or lack there of
• Measurements must be meaningful to the team as well as management
• Routine KPI collection and intermittent independent audit
• Do the measurements inform future decisions?
Triage Dermatology Clinic as a Triage Dermatology Clinic as a Sub Group of the Skin & Sub Group of the Skin & Melanoma ServiceMelanoma Service
• March 28th. Triage Dermatology Clinic commenced.
• Approximately 30 patients per clinic
• Attended by 2 Senior Dermatologists and a registrar. 2 Nursing Staff and 2 Clerical Staff
• 15 % referred across to the Plastic Surgeons.• 27 % discharged.• 4 % Radiotherapy.• 51 % Back to the clinic for follow up.• 1 % Melanoma Unit.• 2 % Discharged for treatment elsewhere.
• Advantages: Able to accommodate increased number of referrals in a more timely manner.• Treatment options are now evidence based.• Increased number of patients appropriately discharged.
• Auditing currently underway to monitor the work flow pattern and labour force compatibility in the surgical skin unit.

.Clinic Activity March 2005.Clinic Activity March 2005SKIN & CANCER FOUNDATION - CLINIC STATS
Total patients - 85
0
5
10
15
20
25
30
35
40
45
50
Discharged Surgery RT Melanoma SCF follow up r/v SCF for tx
Follow up
No
. o
f p
ati
en
ts
Embedding –sustaining the Embedding –sustaining the improvementsimprovements
• Not a project, just what we do to improve the patient journey
• Front line staff identified the problems and led the process improvement work
• Project officer assisted with data collection
• Adapted the collaborative objectives to Peter Mac environment – i.e. ambulatory model of care
Patient Flow Projects Patient Flow Projects 2004/05 2004/05
• Improve Waiting Times in Skin & Melanoma Service
• Surgical Pre-Admission Processes• Patient Diary Development • Outpatient Clinics Templates and Staffing
Review• Head & Neck Service• Day Chemotherapy Service• Combined Chemo Radiotherapy Scheduling• Care Planning & Discharge Management
Going organisational wideGoing organisational wide
• Service specific engagement• Communication and listening• Hearing the reasoning behind resistance• Ongoing monitoring of changes to be
vigilant of potential to relapse• Revisit processes to ensure they are
delivering the desired outcome

Making Innovation Making Innovation MainstreamMainstream
• Is the innovation team satisfied with the process and the outcome?
• What is the common ground?• Identify common problems • Initiate innovations that are transferable to
other areas and services• Ensure that innovations are not person
dependent• Share and celebrate noticeable differences
from the patient and staff perspective
Questions
?

Morning TeaMorning Tea
Meet us back here for
Better clinics: improving the patient journey
at 10.55

Department of Human Services
Breakout session 2Room M7 and M8
10.55 – 11.45
Catherine McCarthy and Ruth SmithPatient Flow Collaborative
5th May, 2005
Better clinics: improving the patient journey

Department of Human Services
Better clinics: improving the patient journey
Catherine McCarthySt. Vincent’s Health
Ruth SmithClinical Innovation Agency
AimsAims
• To share ideas regarding outpatient services improvement
• To look at a whole system approach to improving outpatient department effectiveness
Change principlesChange principles
D: Appointment
systems
C: Outpatient
effectiveness
B: Clinic
scheduling
E: Make it mainstrea
m
A: Focus on patients’ journey
A Step GuideA Step Guide
• Focus on the patient journey

A Step GuideA Step Guide
• Reviewing outpatient clinic schedules - access and treatment rates- seasonal variation- booking systems
A Step GuideA Step Guide
• Outpatient Effectiveness- FTA Rates- Start & finish times- Productivity profiles- Analysis of outcomes
• An example – Chesterfield and North Derbyshire NHS Trust

What was the Problem?What was the Problem?
• Clinic regularly finished early or started late
• Clinics cancelled at short notice
• Clinic slots reduced through annual leave - rescheduling
DiagnosisDiagnosis
• Clinic Review Form– Clinic overview– New:follow up ratio– Hospital cancellations– Patient cancellations– Unused slots and overbooks– Issues and actions
ResultsResults
• FTA rates reduced from 10% to 3%
• Patient cancellation rates fell from 16% to 10%
• Hospital cancellations rates fell from 14% to 3%
• Increase in overall attendances from 745 to 88%

A Step GuideA Step Guide
• Appointment Systems- Booking Systems- Partial Booking
• Benchmarking against similar health services

A Step GuideA Step Guide
• Make it mainstream
Be prepared!

Better Clinics: Improving the Better Clinics: Improving the patient journeypatient journey
Project Overview Project Goals Project implementation and milestones Key Performance Indicators Questions?
Project OverviewProject Overview
AimsThe ‘Better Clinics’ Project Started August 2003
to: Improve the effectiveness and efficiency of the
service offered to patients. Improve the process for referring medical
practitioners. Enhance the role of medical, nursing and clerical
staff working within the department.
CLIF – implementation of recommendations
Project OverviewProject Overview
Method Current processes and practices were reviewed
Steering committee established Design team established Drivers group and other committees to ‘drive’ the change
Interviews with key stakeholders were conducted
Open forums were conducted and formal submissions were requested.
SWOT analysis
Communication strategy developed Internal strategy External strategy
Project OverviewProject Overview
Goals
Recommendations structured around:
Structure
Strategy
Systems
Skills & Staffing,
Style
Shared Values at St. Vincent’s Clinics.
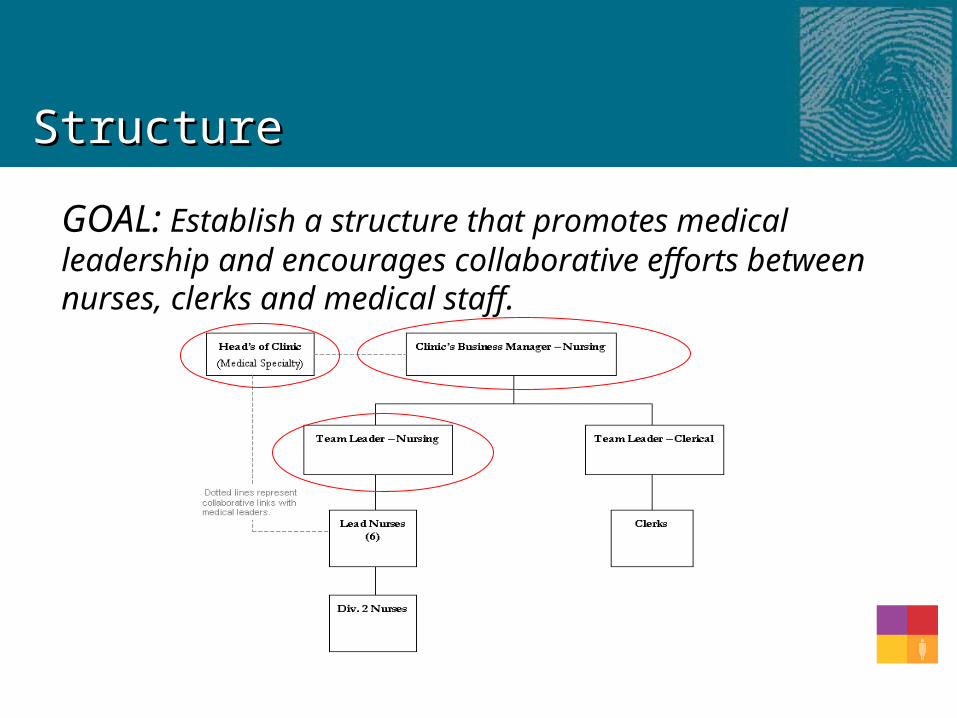
StructureStructure
GOAL: Establish a structure that promotes medical leadership and encourages collaborative efforts between nurses, clerks and medical staff.
StructureStructure
Results Heads of Clinic Appointed and operational Clinics Business Manager commenced November
2004 Lead Nurses appointed November – January Team Leader clerical commenced December 2004 Team Leader nursing Commenced December 2004
Position descriptions Education packages and workshops Staff satisfaction (change management)

StrategyStrategy
GOAL: Establish a strategic profile which outlines the vision and commitment of each clinic and implement systems to evaluate Clinic performance.
– Develop a Clinic Business Model for each specialty (Clinic Function, Patient Mix, Commitment, Appointment times etc.)
– Develop a Monthly Clinic Report outlining key performance indicators (e.g. FTA rates, discharge rates, clinic access)
StrategyStrategy
Results Business model template established KPI’s developed Communication strategy
– Getting it ‘out there’– Red and Blue News (Newsletter)– Meetings– Mentor Program– Reports– Posters
Patient information brochure
Clinic Business ModelClinic Business Model
1. Clinic overview
2. Leadership and structure
3. Patient volume and mix
4. General clinic protocols
5. Specific protocols (Patient Management and discharge)
6. Clinic meetings
7. Performance Measurement

NewsletterNewsletter
PostersPosters
SystemsSystems
GOAL: Develop the processes to manage the Clinics and improve efficiency generally
– Streamline the triage process whereby Lead Nurses make initial bookings on the same day as referral. (Medical review and alterations of bookings conducted retrospectively)
– Implementation of new internal and external referral guidelines

SystemsSystems
Measurements Patient and staff survey IT changes to support the project overall Allied Health contract arrangements Referral template distributed Triage guidelines (under development) Mentor program
Skills and staffingSkills and staffing
GOAL: Develop the capability, skills and leadership of staff working within the clinics– Training program to address Clinic nursing
needs; Process/system/IT needs; leadership needs
Skills and StaffingSkills and Staffing
Measurements Staff survey Staff training program Education planner Appraisals Portfolio development Division 2 support role
Style and valuesStyle and values
GOAL: Develop teams and relationships by information sharing and collaboration.
– HOC’s and Lead Nurses Quarterly Meeting
– Regular meetings for key groups
Style and valuesStyle and values
Measurements Workshops Team building exercises Code of conduct Meetings calendar
KPI’sKPI’s
Clinic Appointment activity Clinic visits - Numbers of new and review patient
appointments attended. Patient attendance – rate of attendance Clinic visit duration - Average time between a patient
appointment and the patient’s departure time. Patient discharge rate - Proportion of (new and review)
patients discharged. Dictation turnaround - Average time taken to type and
dispatch dictated medical correspondence
KPI’sKPI’s
Referral activity Referral Outcome - Proportion of appointment requests
(referrals) in month receiving a response. Booking response time - Proportion of appointment requests
(referrals) in month receiving a response within 7 days. Clinic access - Proportion of appointment requests receiving an
appointment within 8 weeks, and within 12 weeks
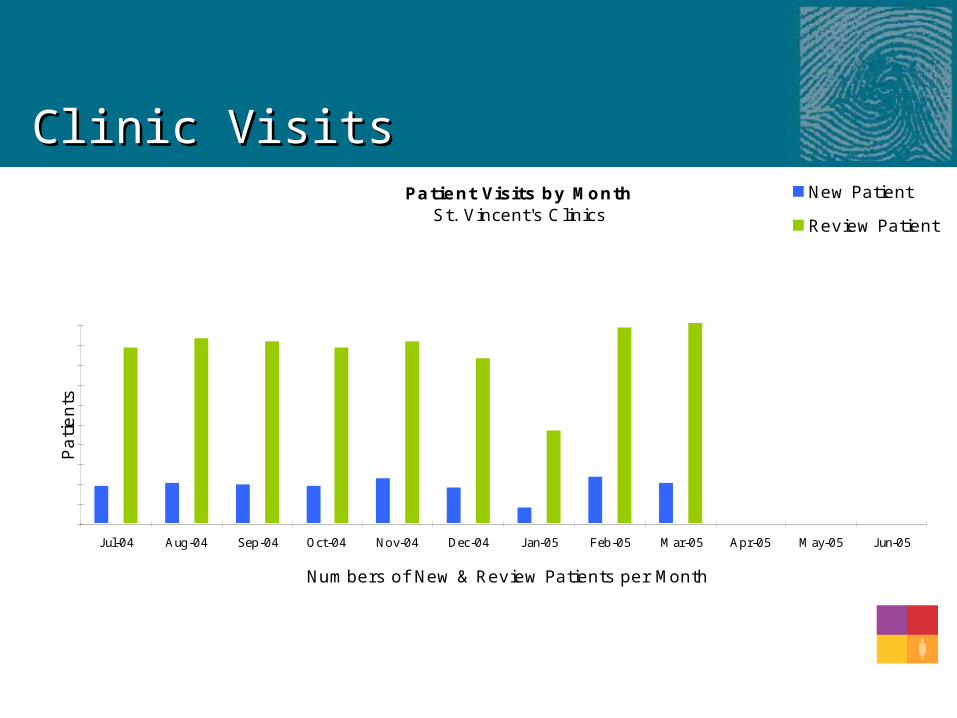
Clinic VisitsClinic VisitsPatient Visits by Month
St. Vincent's Clinics
J ul-04 Aug-04 Sep-04 Oct-04 Nov-04 Dec-04 J an-05 Feb-05 Mar-05 Apr-05 May-05 J un-05
Numbers of New & Review Patients per Month
Pa
tie
nts
New Patient
Review Patient

Patient attendancePatient attendance
Patient Attendance by MonthSt. Vincent's Clinic
J ul-04 Aug-04 Sep-04 Oct-04 Nov-04 Dec-04 J an-05 Feb-05 Mar-05 Apr-05 May-05 J un-05
Percentage of patients attending their clinic appointment
% A
tte
nda
nce
Clinic Average
Clinic Target

Clinic Visit DurationClinic Visit DurationClinic Visit Duration by Month
St. Vincent's Clinics
J ul-04 Aug-04 Sep-04 Oct-04 Nov-04 Dec-04 J an-05 Feb-05 Mar-05 Apr-05 May-05 J un-05
min
s
Clinic Average
Clinic Target
Average time (minutes) between patient appointment time and departure time
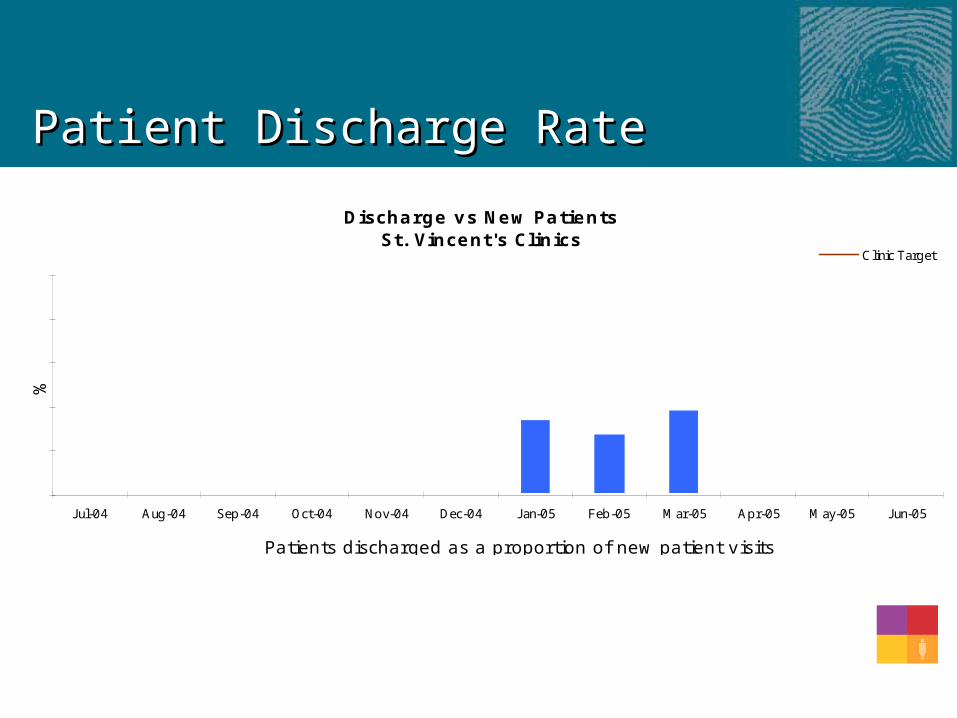
Patient Discharge RatePatient Discharge Rate
Discharge vs New PatientsSt. Vincent's Clinics
J ul-04 Aug-04 Sep-04 Oct-04 Nov-04 Dec-04 J an-05 Feb-05 Mar-05 Apr-05 May-05 J un-05
%
Clinic Target
Patients discharged as a proportion of new patient visits
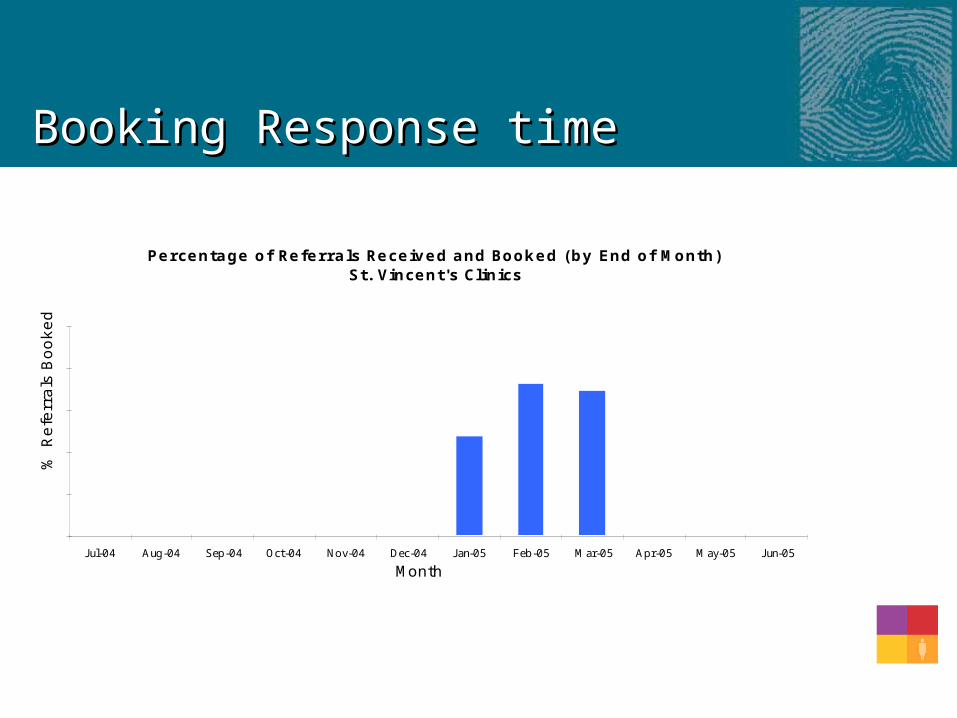
Booking Response timeBooking Response time
Percentage of Referrals Received and Booked (by End of Month)St. Vincent's Clinics
J ul-04 Aug-04 Sep-04 Oct-04 Nov-04 Dec-04 J an-05 Feb-05 Mar-05 Apr-05 May-05 J un-05
Month
% R
efe
rra
ls B
oo
ke
d

Clinic AccessClinic Access
Referrals with Appointment Date within 12 weeks by MonthSt. Vincent's Clinics
J ul-04 Aug-04 Sep-04 Oct-04 Nov-04 Dec-04 J an-05 Feb-05 Mar-05 Apr-05 May-05 J un-05
Percentage of referrals with appointment date within 12 weeks
%
Where to from here?Where to from here?
Monitor and develop Refine data collection Evaluate ‘flow-on’ effect Further staff and patient surveys Evaluation of project overall
Questions
?

LunchLunch
Meet us back here for
Team tabletop presentations
at 12.45
Team presentations12.45– 3.15
Ruth Smith Room M7 and M8
•Peninsula Health
•Royal Children’s Hospital
•Maroondah Hospital
•Bendigo Healthcare Group
•Royal Victorian Eye and Ear Hospital
•Sir Charles Gairdner Hospital

Tabletop presentationsTabletop presentations
The aim of this session is to;• Promote discussion• Share “peer to peer” practical
experiences of innovation• Increase energy for change and shared
learning• Spread ideas between teams
Session formatSession format
• 2 teams per table• Team A has 15 minutes to share experiences
with team B• Whistle blows• Team B has 15 minutes to share experiences
with team A• Rotation 1• Continued….• Working afternoon tea is available
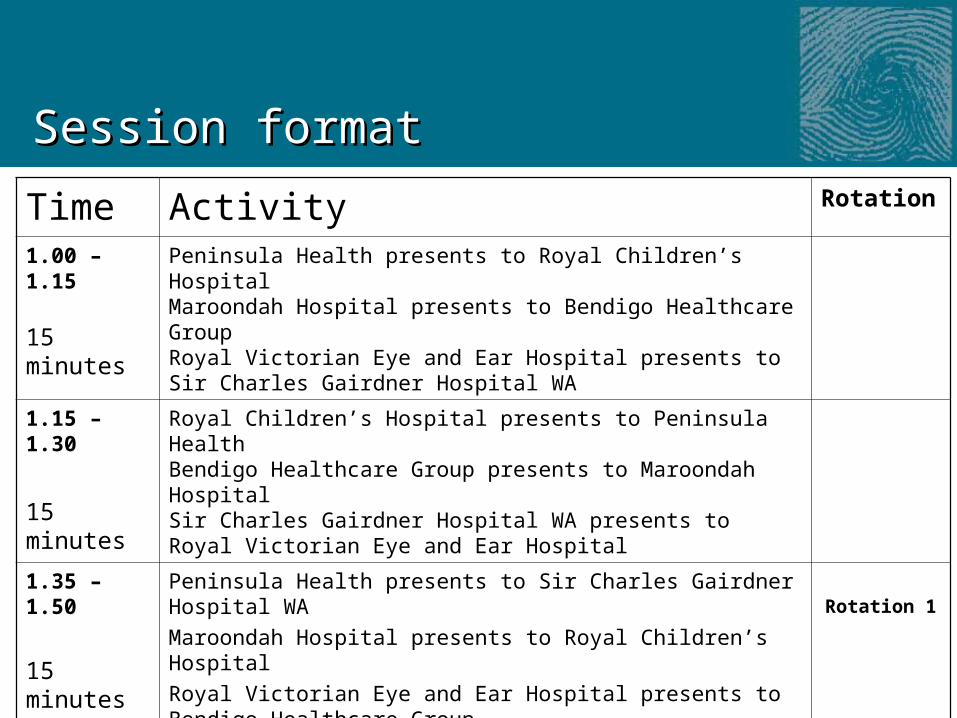
Session formatSession format
Time Activity Rotation
1.00 – 1.15 15 minutes
Peninsula Health presents to Royal Children’s HospitalMaroondah Hospital presents to Bendigo Healthcare GroupRoyal Victorian Eye and Ear Hospital presents to Sir Charles Gairdner Hospital WA
1.15 –1.30
15 minutes
Royal Children’s Hospital presents to Peninsula HealthBendigo Healthcare Group presents to Maroondah HospitalSir Charles Gairdner Hospital WA presents to Royal Victorian Eye and Ear Hospital
1.35 – 1.50
15 minutes
Peninsula Health presents to Sir Charles Gairdner Hospital WA
Maroondah Hospital presents to Royal Children’s Hospital
Royal Victorian Eye and Ear Hospital presents to Bendigo Healthcare Group
Rotation 1
1.50– 2.05
15 minutes
Sir Charles Gairdner Hospital WA presents to Peninsula Health
Royal Children’s Hospital presents to Maroondah Hospital
Bendigo Healthcare Group presents to Royal Victorian Eye and Ear Hospital
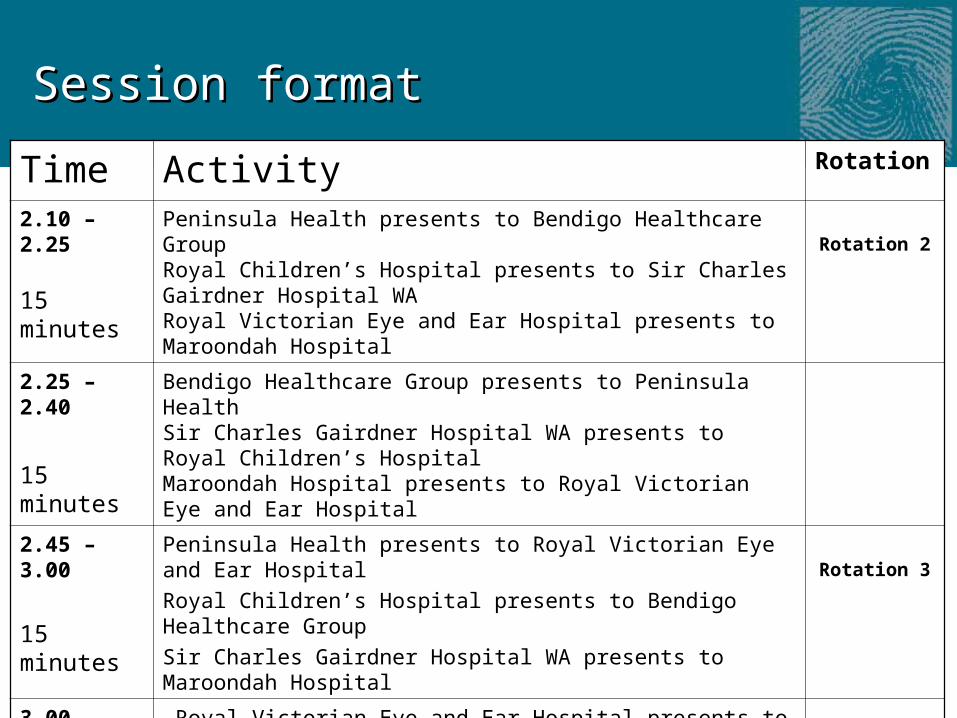
Session formatSession format
Time Activity Rotation
2.10 – 2.25 15 minutes
Peninsula Health presents to Bendigo Healthcare GroupRoyal Children’s Hospital presents to Sir Charles Gairdner Hospital WARoyal Victorian Eye and Ear Hospital presents to Maroondah Hospital
Rotation 2
2.25 –2.40
15 minutes
Bendigo Healthcare Group presents to Peninsula HealthSir Charles Gairdner Hospital WA presents to Royal Children’s Hospital Maroondah Hospital presents to Royal Victorian Eye and Ear Hospital
2.45 – 3.00
15 minutes
Peninsula Health presents to Royal Victorian Eye and Ear Hospital
Royal Children’s Hospital presents to Bendigo Healthcare Group
Sir Charles Gairdner Hospital WA presents to Maroondah Hospital
Rotation 3
3.00 – 3.15
15 minutes
Royal Victorian Eye and Ear Hospital presents to Peninsula Health
Bendigo Healthcare Group presents to Royal Children’s Hospital
Maroondah Hospital presents to Sir Charles Gairdner Hospital WA

Meet us back in the plenary for
Team planning time
at 3.20