dentoalveolar trauma case treatment with … · diş hekimliği fakültesi, ortodonti anabilim...
TRANSCRIPT
CLINICAL DENTISTRY AND RESEARCH 2016; 40(3): 130-135 Case Report
CorrespondenceNihat AKBULUT DDS, PhD
Department of Oral and Maxillofacial Surgery,
Faculty of Dentistry, Gaziosmanpaşa University,
Tokat, Turkey,
Cellular Phone: +905054489263
E-mail: [email protected],
Nihat AKBULUT, DDS, PhD Associate Professor, Department of Oral and Maxillofacial Surgery,
Faculty of Dentistry, Gaziosmanpaşa University,
Tokat, Turkey
Sibel AKBULUT, DDSAssistant Professor, Department of Orthodontics,
Faculty of Dentistry, Gaziosmanpaşa University,
Tokat, Turkey
Kemal Özgür Demiralp, DDS, PhDMinistry of Health,
Public Hospitals Agency of Türkiye.
Ankara, Turkey
Berkan Çelikten, DDS, PhDResearch Assistant, Department of Endodontics,
Faculty of Dentistry, Ankara University,
Ankara, Turkey
DENTOALVEOLAR TRAUMA CASE TREATMENT WITH INTRUSION OF PERMANENT INCISOR TEETH: IS THIS AN APPLICABLE WAY?
ABSTRACT
Dentoalveolar trauma is a very common case and is usually sudden, circumstantial, unexpected, and accidental. Traffic accident is one of the etiologies of trauma that results in severe brain complications like bleeding. So, the treatment of dentoalveolar injuries may be late because it usually requires emergency care. Avulsions and intrusions are the most complicated and controversial displacement injuries of permanent teeth without body fracture. In this study, we present dentoalveolar injuries and its treatment. This study presents a case concerning dentoalveolar injuries resulting from the intrusion of the 21st, 22nd, and 23rd permanent incisor teeth that was caused by a severe traffic accident with brain trauma. The patient was a soldier and had brain treatment in a hospital. Then, he was given dentoalveolar injury treatment, including surgical reduction and grafting of the surrounding bones of the traumatized teeth by splinting them to the neighboring teeth. In addition, the numbers 21, 22, 23 and 24 were given endodontic treatment in the same session. The patient was re-operated by grafting the adjacent bones of the traumatized teeth due to severe alveolar crest resorption. The healing of the patient after the second operation is acceptable, and follow-up is continuing. For the treatment of a dentoalveolar trauma caused by the intrusion presented here, the decision of immediate extraction or repositioning with grafting, splinting, and making endodontic treatment in the same session is found to be very useful, and close follow-up very crucial.
Keywords: Dental Injury, Dental Trauma, Intrusion
Submitted for Publication: 01.27.2015
Accepted for Publication : 01.10.2016
Clin Dent Res 2016: 40(3): 130-135
130

131
CLINICAL DENTISTRY AND RESEARCH 2016; 40(3): 130-135 Olgu Bildirimi
Sorumlu Yazar Nihat Akbulut
Gaziosmanpaşa Üniversitesi,
Diş Hekimliği Fakültesi,
Ağız Diş Çene Cerrahi Anabilim Dalı,
Tokat, Türkiye
GSM: +905054489263
E-mail: [email protected]
Nihat Akbulut Doç. Dr., Gaziosmanpaşa Üniversitesi, Diş Hekimliği Fakültesi,
Ağız Diş ve Çene Cerrahi Anabilim Dalı,
Tokat, Türkiye
Sibel AkbulutYar. Doç. Dr., Gaziosmanpaşa Üniversitesi,
Diş Hekimliği Fakültesi, Ortodonti Anabilim Dalı,
Tokat, Türkiye
Kemal Özgür Demiralp Sağlık Bakanlığı,
Türkiye Kamu Hastaneleri Kurumu,
Ankara, Türkiye
Berkan Çelikten Araş. Gör., Ankara Üniversitesi, Diş Hekimliği Fakültesi,
Endodonti Anabilim Dalı,
Ankara, Türkiye
DAİMİ KESİCİ DİŞLERİN İNTRÜZYONUNU İÇEREN DENTOALVEOLER TRAVMA VAKA TEDAVİSİ: BU KABUL EDİLEBİLİR
BİR YOL OLABİLİR Mİ?
ÖZ
Dentoalveoler travma çok sık karşılaşılan bir durumdur ve genellikle ani gelişir, koşullara bağlı olarak, beklenmedik şekilde ve kazara oluşur. Trafik kazaları, kanama gibi ciddi beyin komplikasyonlarına neden olan travma etiyolojilerinden biridir. Bu tür durumlar genellikle acil müdahale gerektirdiğinden, dentoalveoler yaralanmaların tedavisi daha sonraya ertelenebilir. Avülsiyonlar ve intrüzyonlar, gövde fraktürü olmayan daimi dişlerin, en komplike ve tartışmalı deplasman yaralanmalarıdır. Bu çalışmada dentoalveolar yaralanmalar ve tedavisi sunulmaktadır.Bu çalışma, beyin travması ile birlikte ciddi bir trafik kazası sonucu gelişen 21, 22 ve 23 nolu daimi dişlerin intrüzyonu ile sonuçlanan bir dentoalveolar yaralanma vakası ile ilgilidir. Hasta bir askerdi ve öncelikle bir hastanede beyin tedavisi gördü. Daha sonra travmatize dişlerin, komşu dişlere splintlenerek, bu dişlerin çevresindeki kemiğin greftlenmesi ve cerrahi redüksiyonunu içeren bir dentoalveolar tedavi gördü. Ayrıca 21, 22, 23 ve 24 nolu dişlere aynı seans endodontik tedavi yapıldı. Hasta şiddetli alveolar kret rezorbsiyonu nedeni ile travmatize dişlere komşu kemiğin greftlenmesi suretiyle tekrar opere edildi. İkinci operasyon sonrası hastanın iyileşmesi tatmin ediciydi ve hastanın takibi devam etmektedir.Burada sunulan intrüzyonun neden olduğu bir dentoalveoler travma tedavisi için, immediat ekstraksiyon veya aynı seans greftleme, splinte etme ve endodontik tedavi yapılması kararı faydalı bulunmuştur ve hastanın sık aralıklarla takibi çok önemlidir.
Anahtar Kelimeler: Dental yaralanma, dental travma,
intrüzyon
Yayın Başvuru Tarihi : 27.01.2015
Yayına Kabul Tarihi : 10.01.2016
Clin Dent Res 2016: 40(3): 130-135

132
CLINICAL DENTISTRY AND RESEARCH
INTRODUCTION
Dental or orofacial injury or trauma, especially due to a traffic accident or a sports activity, is the second most prevalent type of dental injury, after caries, affecting an individual rather than the population.1, 2 Apart from the body fractures of teeth, avulsions and severe intrusions are the most seen traumatic complications in adult patients.3
Intrusive luxation in permanent dentition is a rare tooth related injury, with a prevalence of 0.5–1.9% in all dental injuries.2,4,5 Intrusion of teeth due to trauma is a type of dental injury that includes the dislocation of the tooth in an apical direction into the alveolar bony crests or jaws that is also called ‘intrusive luxation’.4,6 This kind of injury usually involves the anterior teeth of the upper jaw and is more seen in the deciduous than in permanent dentition.6
Pulp necrosis, external or internal root resorption, ankylosis, marginal bone loss, pulp canal obliteration, paralysis or disturbance of root development, and gingival retraction may occur as a consequence of an intrusive luxation.5,7
Management of intrusions is controversial but has the widest choice of treatment options such as earlier surgical management with endodontic treatment, following the case for the spontaneous eruption of intrusive teeth, orthodontic traction, and others. There is, however, no consensus about the ideal treatment to achieve or obtain an optimal outcome.4,5,7 In the literature, there are many important guidelines about the treatment of intruded teeth as provided by the American Association of Endodontists (AAE), the Royal College of Surgeons of England (RCSE), and the International Association of Dental Traumatology (IADT).8,9 Also, IADT updated the guidelines on the evaluation and management of accidental or traumatic dental injuries in 1988, 2001, 2007, and later updated in 2012.1,9
The abovementioned literature demonstrate that the amount of intrusion is the crucial factor in obtaining pulp and tooth survival. Many studies carried out in this field have shown that intrusions up to 3 mm enable perfect results, whereas the prognosis of incisors with severe (> 6 mm) intrusion is unpromising because of inflammatory root resorption and pulp necrosis. Teeth with intrusion beyond 6 mm should immediately be surgically repositioned or extracted, followed by root canal treatment, which is the next choice.8 In another study, intrusion is classified in a condition of being totally or partially embedded into the alveolar bone.10
In the current study, a multidisciplinary treatment of a case with a severely intruded anterior, three incisors is presented.
This case report also emphasizes how severely intruded multiple teeth can successfully be treated with immediate surgical repositioning, repetitive grafting procedures, and endodontic treatment.
CASE REPORT
A 21-year-old male patient, who is a soldier, was referred to our dentistry faculty. He had a history of severe traffic accident with brain trauma, dentoalveolar injuries caused by the severe intrusion of the number 21, 22, and 23 permanent incisor teeth without body fracture and was given emergency care in a military hospital. The patient’s general health was normal, and the neurological status was fully treated after the emergency care. Clinical and radiological examinations and the treatment plan were immediately carried out by a multidisciplinary team, including Oral and Maxillofacial Surgery, Restorative Dentistry, Endodontic, and also Orthodontic Clinics, which contributed to the treatment within their own expertise (Figure 1a). Firstly, because of the complexity of the said dentoalveolar trauma, antibiotic therapy (Amoklavin 1000 mg, Deva Holding A.Ş., Istanbul, Türkiye) was given to the patient.As a consequence of the severity of intrusive luxation and completed root development, immediate surgical repositioning of the intruded teeth was the initial treatment plan. After the administration of local anesthesia, the intruded teeth were repositioned by a surgeon and splinted with a rectangular stainless steel wire-composite filling material by a restorative treatment specialist and an orthodontist. At this stage, the endodontic treatment, including calcium hydroxide intracanal medicament, was carried out to the number 21, 22, 23, and 24 of teeth by the an endodontist. The premolar tooth was found have high vertical and horizontal percussion sensitivity. Because of this, the premolar tooth was included in the endodontic treatment. All teeth were prepared and calcium hydroxide dressing was performed to root canals for 2 weeks. Then, the root canals were filled with AH Plus (Dentsply Maillefer, Tulsa, OK) and gutta-percha. The restoration of the teeth was made with composite resin (Filtek Z250, 3M Espe, St. Paul, MN, USA). Aesthetic restorations were left to be done after the treatment was concluded. At the end of all this process, the patient was discharged with optimal postoperative care and prescription. One week later, the patient was recalled for the removal of silk sutures (Figure 1b).
133
Dentoalveolar trauma Case treatment
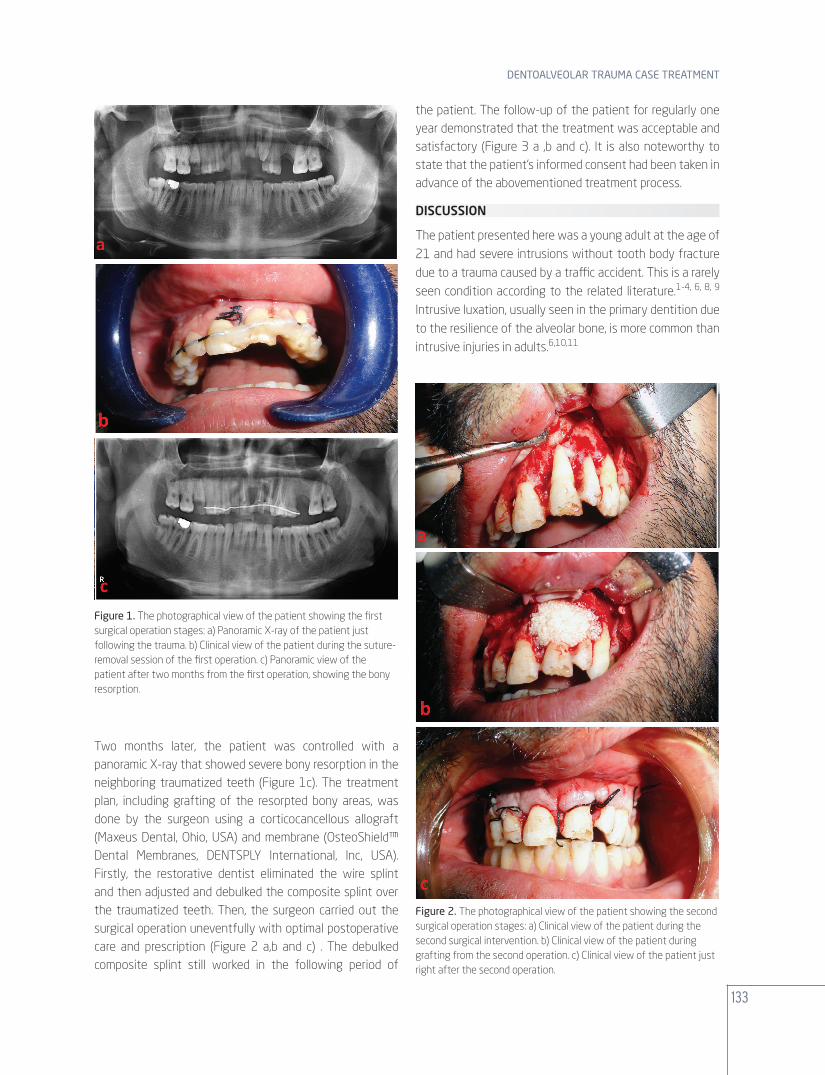
Two months later, the patient was controlled with a panoramic X-ray that showed severe bony resorption in the neighboring traumatized teeth (Figure 1c). The treatment plan, including grafting of the resorpted bony areas, was done by the surgeon using a corticocancellous allograft (Maxeus Dental, Ohio, USA) and membrane (OsteoShield™ Dental Membranes, DENTSPLY International, Inc, USA). Firstly, the restorative dentist eliminated the wire splint and then adjusted and debulked the composite splint over the traumatized teeth. Then, the surgeon carried out the surgical operation uneventfully with optimal postoperative care and prescription (Figure 2 a,b and c) . The debulked composite splint still worked in the following period of
the patient. The follow-up of the patient for regularly one year demonstrated that the treatment was acceptable and satisfactory (Figure 3 a ,b and c). It is also noteworthy to state that the patient’s informed consent had been taken in advance of the abovementioned treatment process.
DISCUSSION
The patient presented here was a young adult at the age of 21 and had severe intrusions without tooth body fracture due to a trauma caused by a traffic accident. This is a rarely seen condition according to the related literature.1-4, 6, 8, 9 Intrusive luxation, usually seen in the primary dentition due to the resilience of the alveolar bone, is more common than intrusive injuries in adults.6,10,11
Figure 1. The photographical view of the patient showing the first surgical operation stages: a) Panoramic X-ray of the patient just following the trauma. b) Clinical view of the patient during the suture-removal session of the first operation. c) Panoramic view of the patient after two months from the first operation, showing the bony resorption.
Figure 2. The photographical view of the patient showing the second surgical operation stages: a) Clinical view of the patient during the second surgical intervention. b) Clinical view of the patient during grafting from the second operation. c) Clinical view of the patient just right after the second operation.

134
CLINICAL DENTISTRY AND RESEARCH
In the present study, the intrusion detected was totally embedded into the alveolar bone that was also observed in the literature. Total intrusion was more frequent than the partial kind10 as seen compatible with our case.The intruded teeth were mostly maxillary central incisors with a percentage of 90%. This is related to their anatomic position in the maxillary dental arch.7,11 In our cases, maxillary left central, lateral, and canine teeth were intruded due to traumatic injury.
Intruded teeth may encounter some complications. Pulp necrosis, as a complication, was frequently seen in literature reports.5,11,12 If the endodontic treatment is delayed, traumatic intruded teeth may have the apical external or internal root resorption due to the necrotic and infective pulp tissue remnants. So, management options of the intruded teeth treatment are controversial. As we know from the literature, the treatment of intruded teeth has three choices including waiting for spontaneous eruption, orthodontic traction, and immediate surgical repositioning following the root canal treatment.5,7,11,12 But, severely intruded teeth in permanent dentition cannot wait for the spontaneous eruption or orthodontic traction due to the pulp necrosis, root resorption, ankylosis, and obliteration of the pulp canal.5,7,12
Immediate surgical repositioning is indicated for teeth classified as “root almost completed” and “apical end of the root completed”, and also in cases of multiple intrusions like the presented case in this study.5,7,11,12
The clinical criterion reported by Andreasen et al.5 to indicate either surgical or orthodontic repositioning was that the amount of tooth displacement should be less than 6-7 mm, regardless of the root development stage. Multiple-intrusion cases necessitate immediate surgical repositioning of the severely intruded teeth. In addition, the surgical repositioning of the traumatized teeth is recommended to be carried out at a proper distance from the root surface to provide adequate room for endodontic access.7 In this case study, immediate surgical repositioning of severely intruded teeth was the selected treatment option and caused no adverse complications. Previous knowledge and our results, including that of 29 intruded permanent teeth by Kinirons, Sutcliff, and Ebeleseder et al.,7 failed to show that surgical repositioning increased the prevalence of resorption.According to the literature survey, we have not encountered any dentoalveolar dental injury case treated with additional surgical intervention like grafting. We determined marginal bone loss especially in the surrounding of the left central tooth after two months from the first treatment procedures carried out by our multidisciplinary team. So, we repeated the bone grafting and finally obtained acceptable results. In addition, we removed the wire splint after two months from the first dentoalveolar injury intervention, but we did not remove all the composite splints especially on the interface of the teeth due to severe bone support loss. Therefore, it is found to be a useful and applicable treatment for this kind of trauma case.
Figure 3. The photographical view of the patient showing the healing stages: a) Panoramic view of the patient after one year of follow-up showing the acceptable bone healing. b) Clinical lower front view of the patient after one year of follow-up showing the acceptable appearance. c) Clinical front view of the patient after one year follow-up showing the acceptable appearance.
135
Dentoalveolar trauma Case treatment
CONFLICT OF INTEREST
There is no conflict of interest.
ACKNOWLEDGEMENT
This study was presented as an oral presentation at ‘’18th Balcan Stomatological Society Congress 25-28 April 2013, Skopje’’.
REFERENCES
1. Kullman L, Al Sane M. Guidelines for dental radiography immediately after a dento-alveolar trauma, a systematic literature review. Dent Traumatol 2012; 28: 193-199.
2. Gomes GB, da Costa CT, Bonow ML. Traumatic intrusion of permanent teeth: 10 years follow-up of 2 cases. Dent Traumatol 2013; 29: 165-169.
3. Bucher K, Neumann C, Hickel R, Kuhnisch J. Traumatic dental injuries at a German university clinic 2004-2008. Dent Traumatol 2013; 29: 127-133.
4. Tsilingaridis G, Malmgren B, Andreasen JO, Malmgren O. Intrusive luxation of 60 permanent incisors: a retrospective study of treatment and outcome. Dent Traumatol 2012; 28: 416-422.
5. Gondim JO, Diniz MB, de Abreu-e-Lima FC, Pansani CA, Moreira Neto JJ. Alternative treatment modalities for immature intruded permanent incisors: report of 2 cases. Pediatr Dent 2009; 31: 340-345.
6. Chan AW, Cheung GS, Ho MW. Different treatment outcomes of two intruded permanent incisors--a case report. Dent Traumatol 2001; 17: 275-280.
7. Mazumdar D, Roy P, Kumar P. Management of intrusive luxation with immediate surgical repositioning. J Conserv Dent 2009; 12: 69-72.
8. Kenny DJ, Barrett EJ, Casas MJ. Avulsions and intrusions: the controversial displacement injuries. J Can Dent Assoc 2003; 69: 308-313.
9. Malmgren B, Andreasen JO, Flores MT, Robertson A, DiAngelis AJ, Andersson L et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent Traumatol 2012; 28: 174-182.
10. Carvalho V, Jacomo DR, Campos V. Frequency of intrusive luxation in deciduous teeth and its effects. Dent Traumatol 2010; 26: 304-307.
11. Neto JJ, Gondim JO, de Carvalho FM, Giro EM. Longitudinal clinical and radiographic evaluation of severely intruded permanent incisors in a pediatric population. Dent Traumatol 2009; 25: 510-514.
12. Shanmugam HV, Arangannal P, Vishnurekha C, Nichani MH, Vijayaprabha K. Management of intrusive luxation in the primary dentition by surgical repositioning: an alternative approach. Aust Dent J 2011; 56: 207-211.