dental implant biomechanics, treatment planing, and prosthetic considerations
TRANSCRIPT

BIOMECHANICS, TREATMENT PLANING, AND PROSTHETIC
CONSIDERATIONSChapter 76

Biomechanical considerations
• Osseointegrated implant provide predictable means of replacing missing teeth
• Load-bearing capacity of implants > anticipated loads during function
• If applied loads > load-bearing capacity
Failure : Mechanical, Biologic

• Implant failure• Mechanical failure : screw
loosening, bend, fracture of the implants
• Biologic failure : resorption-remodeling response of bone around implants Progressive bone loss
Biomechanical considerations

• Teeth are suspended within the supporting alveolar bone by periodontal ligament
Physiologic movement
Teeth movement: orthodontic
Implant- VS Tooth-retained restoration
Excessive forces

• Osseointegrated dental implants : direct contact with alveolar bone
No periodontal ligament
Destructive alveolar bone
Implant- VS Tooth-retained restoration
Excessive forces
Load-bearing capacity
• The bone appositional index : percentage of bone-to-implant contact
• Several factors influence load-bearing capacity• Number and size of implant• Angulations of implant position• Quality of the bone-to-implant interface

Load-bearing capacity• Posterior maxilla : less dense
trabecular, thin cortical plate layer
poor bone quality • Anterior mandible : dense
trabecular, thick cortical plate layer

• Surface modification : altered microtopography achieve higher bone apposition index
• Lack of bone height ≠ long implant -> reduce bone-to-implant contact
Use of short, wide implants
Increase load-bearing capacity
Load-bearing capacity
Angulation and arrangement
• Angulation of implants in relation to the plane of occlusion and the direction of the occlusal load
• Axial loads are well-tolerated • Implant at an angle of 20 degrees or more -
>resorptive remodeling response of bone

• Nonaxial loads concentrated stresses around the neck of the implant
Angulation and arrangement

Mechanism of implant failure• Excessive occlusal loads• Load resulting in microdamage: fracture, cracks, and
delaminations• Resorption-remodeling response of bone• Loss of bone at the bone-to-implant interface as a
result of remodeling• Vicious cycle of continues loading, additional
microdamage, and bone loss progressing to implant failure

• Distal cantilivered pontics were used to replaced missing maxillary posterior teeth
Nonaxial occlusal forces
Angulation and arrangement

• Distal angulation and the curve of Spee
Nonaxial loads
Angulation and arrangement

Treatment planing with dental implants
• Anterior-posterior (A-P) implant spread • Distance from the middle
of the most anterior implant to the distal edge of the most posterior implant
Edentulous maxilla
• Implant-supported prosthesis : provide stability comfort and restore confidence • Poor ridge form with a marginally stable
conventional maxillary denture : 2 or 4 implants provide greater stability and security of a maxillary denture in function

Edentulous maxilla• Implant-supported prosthesis : provide stability
comfort and restore confidence • Lack of posterior support with an intact mandibular
anterior dentition : Combination syndrome “Hammer and anvi”

• Implant-supported prosthesis : provide stability comfort and restore confidence • Palatal coverage is not tolerated
Minimum of four implants with adequate A-P spread
Edentulous maxilla

• Implant-assisted maxillary overdenture is preferred over an implant-supported fixed prosthesis -> labial flange can provide lip support
Edentulous maxilla

Edentulous mandible
• Mandibular complete denture is more problematic especially for pt with severely atrophic mandibular ridge
• Two-implant-assisted overdenture -> treatment of choice

• Implant-supported fixed prosthesis • 4,5, or 6 implants arranged in an appropriate arc
of curvature with at least 1 cm of A-P spread • distal extension cantilevers up to twice the A-P
spread
Edentulous mandible
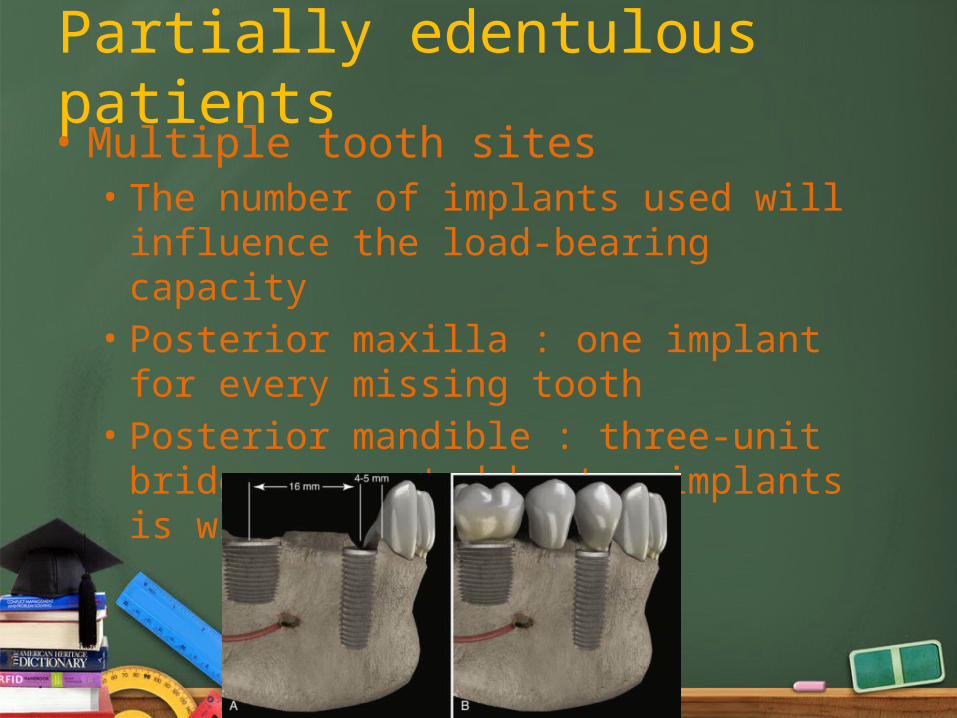
Partially edentulous patients• Multiple tooth sites• The number of implants used will influence the
load-bearing capacity• Posterior maxilla : one implant for every missing
tooth• Posterior mandible : three-unit bridge supported
by two implants is widely accepted
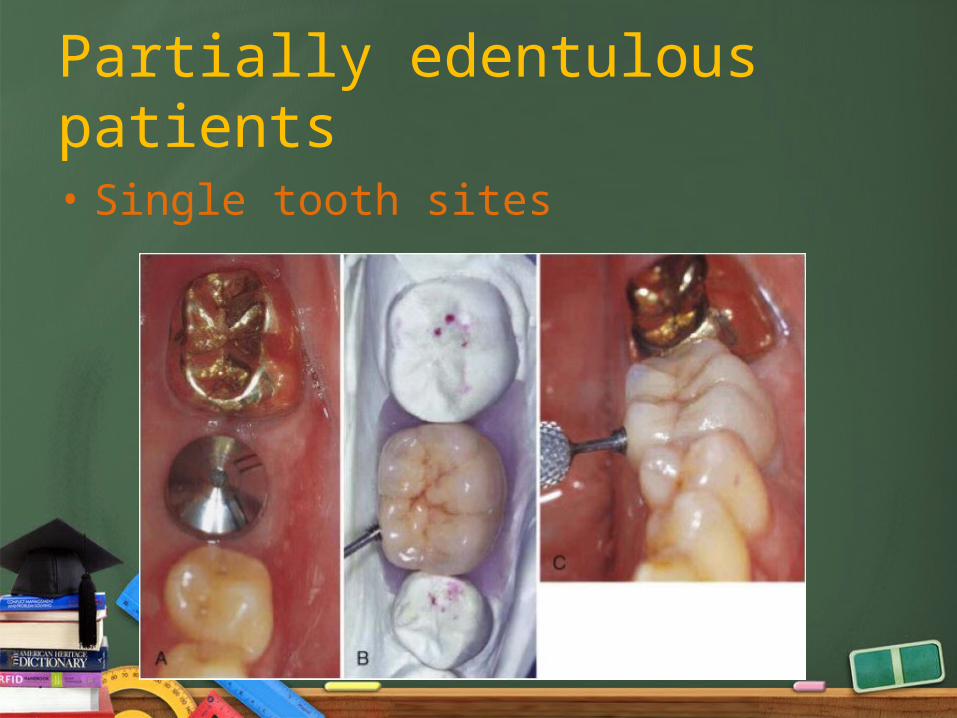
• Single tooth sites
Partially edentulous patients

• Implant: Adequate number, size and position to sustain the occlusal loads
• Residual ridge and site permits : wide diameter implants should be used for molar replacement
Strategies to avoid implant overload
Strategies to avoid implant overload
• Place implants perpendicular to the occlusal plane• Place implants in tooth positions• Use an implant for each unit being replaced• Avoid the use of cantilevers in linear configurations• Avoid connecting implants to teeth

Strategies to avoid implant overload
• If connecting implants to teeth, use a rigid attachment
• Control occlusal factors such as cusp angles and width of occlusal table
• Restore anterior guidance if possible

• Occlusal design• Limit the width of occlusal table• Flattening the cusp angles• Avoid Cantilevered restoration
Strategies to avoid implant overload

• Connecting implant to teeth• Keep implant-supported restorations separate
from natural teeth
• Implants and teeth function differently
• Connect with the rigid system
Strategies to avoid implant overload

Conclusions
• The biomechanics must be factored into the planning at the beginning of any implant treatment
• To achieve long-term, predictable success