democratic republic of sao tome and principe ministry of planning and...
TRANSCRIPT

DEMOCRATIC REPUBLIC OF SAO TOME AND PRINCIPE
MINISTRY OF PLANNING AND FINANCE
SOCIAL SECTOR SUPPORT PROJECT (SSSP)
CONSULTANCY REPORT
Consultant: Victor Bomfim
Sao Tome, June 2009
Draft Medical Waste Management Plan
E2343 V2
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

2
INDEX Page Tables and figures ...............................................................................................................3 Abbreviations.......................................................................................................................4 Medical Waste Management Plan.......................................................................................8 1. Introduction.....................................................................................................................9 1.1 Context of the study ......................................................................................................9 1.2 Objectives of the SSSP .................................................................................................9 1.3 Objectives of the MWMP ...........................................................................................10 2. Brief Features of the Country .......................................................................................10 2.1 The Geography ...........................................................................................................10 2.2. Political and Administrative Organization ............................................................... 10 2.3. Demographic Data.....................................................................................................10 2.4. Health and Environment ............................................................................................11 2.4.1. Health and Environmental Policy ...........................................................................11 2.4.2. Organization of the Health Care .............................................................................11 2.4.2.1Administrative Structure ....................................................................................... 11 2.4.2.2. The Structure of Care ...........................................................................................12 2.4.3. Network of Sanitary Structures ...............................................................................12 2.4.3.1. The Public Structure of Care ................................................................................12 2.4.3.2. The Private Structure of Care ...............................................................................13 2.4.4. Assessment of Production of Biomedical Waste .....................................................13 2.4.5. Analysis of the Legislation ......................................................................................13 3. Current Status of Management of Biomedical Waste………………………………....143.1. Analysis of Management Practice of Biomedical Waste ...........................................14 3.1.1. The cleaning Staff ...................................................................................................15 3.1.2. Collection and Separation of Medical Waste ..........................................................15 3.1.3. The System of Intermediate Deposit .......................................................................16 3.1.4. The Evacuation System of Wastes in the Sanitary Structures .................................16 3.1.5. The system of Final Collection in the Structures......................................................17 3.1.6. The Reutilization ......................................................................................................17 3.1.7. The Systems of Internal Treatment...........................................................................18 3.1.8. The System of Transport and Internal Treatment.....................................................18 3.1.9. Environmental Assessment of the Current Systems of Treatment ..........................18 3.2 Current Status of Training and Sensitization................................................................19 3.3 Summary of Factors that Affect a Good Management ................................................19

3
4. Biomedical Waste Management Plan .............................................................................19 4.1The Line of Management of Biomedical Waste ............................................................20 4.1.1. The Chain Collection, Transport and Internal Deposit .............................................20 4.1.1.1. Strategy of Improvement ........................................................................................23 4.1.1.2. Needs Assessment .................................................................................................23 4.1.1.2.1. Equipment of Collection/Deposit .......................................................................24 4.1.2 The Chain Treatment: Choice of Technology ...........................................................24 4.1.2.1. The Technology of Treatment ................................................................................24 4.1.2.2Comparaison of the Systems According to Their Effectiveness and Eco-environmental Criteria .......................................................................................................26 4.1.2.3. The Choice of Technology .....................................................................................28 4.1.3. Alternative Strategies of Implementation of the Elimination ..................................28 4.1.3.1. Treatments – External Elimination .......................................................................28 4.1.3.2. Treatment and Internal Elimination.......................................................................28 4.1.4. Analysis of Strategies ...............................................................................................30 4.1.5. Proposals of Strategy and Perspectives ....................................................................32 4.1.5.1The Management System in Practice: collection, evacuation and treatment. ........34 4.1.5.1.1. The Strategy of Improvement .............................................................................34 4.1.5.1.2. Needs Assessment ..............................................................................................35 4.1.5.2. Financing of the Systems ......................................................................................35 4.1.5.2.1. The Strategy of Financing .................................................................................35 4.1.5.2.2. Financing and Expenditures .............................................................................35 4.2. Training...................................................................................................................... 36 4.2.1. Strategy of Implementation of Appropriate Training .............................................36 4.2.2. Training Needs and Strategy ..................................................................................36 4.2.2.1. Training Strategy .................................................................................................36 4.2.2.2. The Needs..............................................................................................................37 4.3. Sensitization ...............................................................................................................37 4.3.1. The Strategy of Sensitization ................................................................................. 37 4.3.2. Needs Assessment ................................................................................................. 37 4.4. The Strengthening of Legislation and the Search of Sustainable Financing .............40 5. Implementation and Timetable .....................................................................................43 5.1. Detailed Activities of the Action Plan .......................................................................43 5.1.1. Preparatory Activities .............................................................................................45 5.1.2. Implementation .......................................................................................................46 5.1.3. Monitoring and Evaluation..................................................................................... 46 5.1.3.1. Monitoring and Implementation of the Plan .......................................................46 5.1.3.2Evaluation of the System of the Plan .....................................................................46 5.2. Actors and Functions ................................................................................................ 49 6. The Budget. ................................................................................................................. 50

4
ANNEX I. List of People Met ............................................................................................52 ANNEX II. List of Documents ..........................................................................................53
Table nº 1: Geographical Distribution of the Population of STP
Table nº 2: National Health System in STP, 2000 Table nº 3: Public Health System in Washington Table nº 4: Evaluation of Production of Biomedical
Waste in the Hospital Ayres de Menezes Table nº 5: Assessment of Production of Biomedical
Waste (kg) in the PMI Table nº 6: Assessment of Production of Biomedical
Waste in the Hospital Structures Table nº 7: Assessment of Production of Other
Health Centers Table nº 8: Assessment of Production of Health
Posts Table nº 9: Assessment of Production of Community
Health Posts Table nº 10: Estimated Production of Biomedical
Waste per District Table nº 11: Number of People to be Equipped in
Sanitary Structures Table nº 12: Frequency of Sensitization Messages Table nº 13:

5
MEDICAL WASTE MANAGEMENT PLAN 1. Introduction In Sao Tome and Principe the prevention and fight against communicable diseases are a major priority of the Government. However, in recent years it has been registered both at national and regional levels a very rapid spread of some infections, with particular reference to HIV/AIDS. To remedy this situation, the government adopted a National Program to Fight AIDS and to mitigate the health and socio-economic impact of HIV / AIDS at the individual and household levels. The strategic priorities defined under the National Program to Fight AIDS fall perfectly into the major endorsed government policies, including the Poverty Reduction Strategy Paper, and the Millennium Development Goals (MDGs) and other legal instruments ratified by the country 1.1 Context of the study Like many developing countries, the inappropriate handling of infected materials due to improper management of biomedical waste poses a major risk, for health staff and the population. The current management of these wastes predisposes health personnel, but also their families, and street children to several risks of infections and is a source of risk of spread of endemic diseases such as HIV/AIDS, tetanus, viral hepatitis, etc. Faced with this problem, the government, with the support from the Social Sector Support Project (PASS) funded by the World Bank, prepared in 2004 a Medical Waste Management Plan, to support efforts to improve the management of such waste. However, taking into account changes in the fight against HIV/AIDS and the health sector, as well as recent studies and other innovations in this area, there is a need to adapt such a Plan for the preparation of the Additional Financing for the Social Sector Support (SSSP). 1.2 Objectives of the SSSP The overall objective of the SSSP is to improve the health and the education outcomes of the population of Sao Tome and Principe by improving health services, and by making sure that people have access to services of better quality, as well as to support institutions to become more efficient. The project aims to: 1. Improve the efficiency of public provision of social services with greater transparency and accountability according to the approach based on performance and, 2. Improve the participatory approach, including the civil society, by giving a role to the communities. Furthermore, the project aims to reduce the environmental and social impact of the

6
improper handling of materials and products infected with HIV/AIDS. The health component of the project will focus on the strengthening of basic services at the district levels with the provision of maternity services through the provision of infrastructure and equipment, training in management and support in priority areas in STP, namely malaria and HIV/ AIDS. The integration of biomedical waste management in the project is dictated by the fact that there is improper handling of materials infected by the HIV and others, therefore posing a major risk, not only for the health teams, but also for families, street children, the garbage workers who can be source of propagation of the epidemic. The purpose of this study is to analyze the current management of biomedical wastes in STP, explore the level of knowledge of health workers, municipal workers and communities in order to propose an action plan technically feasible, economically viable and socially acceptable for the management of medical waste. In that regard, the additional financing for the SSSP will include the rehabilitation/ construction of some infrastructure, including the rehabilitation/expansion of health centers and housing for health staff in remote areas. The land for these interventions are property of the State at various levels (central, municipal and regional) with relevant permits and in places that will not cause environmental disturbances. Similarly, it is the government’s responsibility to ensure that such infrastructure will comply with the spirit of this document. 1.3 Objectives of MWMP As noted, the purpose of this report is, in light of the current level of sanitation in the country, to upgrade the MWMP prepared in 2004. This update aims to assess the institutional, legislative and regulatory environment, technologies and techniques applied in the disposal of the waste, the behavior of professionals and the public in relation to biomedical waste and the degree of implementation of the planned activities. Finally, the Plan proposes a set of priority actions for the management of biomedical waste in order to improve public health and substantially reduce the spread of HIV/AIDS and other infectious diseases. In this sense, the study was conducted on the basis of a method comprising: - Research and analysis of documents (laws and regulations); - Interviews and workshops with relevant stakeholders in the management of biomedical waste; - Participatory planning sessions (training and awareness); - Visits to health facilities; - Visit to dumps of Penha and the selected location for the new trash (Correia); - Weighing biomedical waste in the determination of production and composition of the waste. This document is divided into 5 chapters:
7
1. Country Background: provides a summary of STP, the status of health organization and health structures, and deals with the legislation on biomedical waste, the estimated production of biomedical waste; 2. Current Management of biomedical wastes in STP: the social and health impacts arising and constraints, and analyzes the state of training and awareness activities for biomedical waste; 3. Action plan for the rational management of biomedical wastes in STP, including technical, organizational, training and awareness and the strengthening of legislation and financial aspects/needs assessment; 4. Implementation of actions to be undertaken, role of the actors and potential partners, monitoring and evaluation, as well as the timetable for implementation. 5. Preparation and proposed budget.
2. Brief characterization of the country 2.1 The Geography Located in the Atlantic Ocean on the equator, the Democratic Republic of Sao Tome and Principe is located 300 km from the west coast of Gabon in the Gulf of Guinea, between latitude 1 º 45 'North and 0 º 25' South in the meridians 6 26'Este and 7 º 30 'West. STP is an archipelago consisting of two islands and four islets in the Gulf of Guinea with an area of 1001 km2. The island of Sao Tome covers an area of 859 km2 while the island of Principe is 142 km2. The Rolas islet is located in the south of Sao Tome on the imaginary line of Ecuador as the Goat Island is located very close to the east of St. Thomas the level of the island of Principe are the islets of the Jockey Cap south Bombom and north. The relief of the country is pretty rough because of volcanic islands. On the island of Sao Tome is the Pico de Sao Tome culminating in the 2024 Prince me, Pico Parrot at a height of 948 m. The climate is tropical humid with two seasons a dry three months (June, July, August) and a wet nine months. Due to the characteristics of relief, there are several micro-climatic zones: the high-altitude areas reach a rainfall of 5000 mm in lowland areas (north and northeast) rainfall ranges from 500 to 1000mm/year. The average annual temperature is 26 º C and 27 º C on the coast and 21 º C in mountainous areas. The air humidity is 22% during most years in the mountains. In areas of medium altitude humidity varies between 70 and 80%. The country has a hydrographic network composed of more than 50 rivers in length between 5 and 27 km and spread out radically from the center of mountainous islands towards the coastline, a total capacity of 2.1 million m3 of water/km2 equivalent to 10.000m3/inhabitant/year. However, 60% of the water lines are located in the southwest and south of both islands.

8
In the south and west of both islands, high volcanic mountains fall precipitously to the sea, although neither island has witnessed any volcanic activity in recent centuries. The mountains descend gradually to small plains in the northeast. São Tomé Peak, the highest point on the main island, rises to 6,640 feet (2,024 meters) above sea level, while Príncipe Peak on the smaller island reaches 3,110 feet (948 meters). These mountainous areas are deeply dissected by the effects of stream erosion, and spectacular isolated volcanic plugs stand out as landmarks. Swift and rocky streams rush down to the coast in every direction.
Sao Tome and Principe is the second smallest state in Africa with a total population of 165,000 and a per capita income of $290. About 54% of the population is living under poverty with limited human development due to weak and inefficient public institutions and limited and fragmented civil society organizations. The delivery of social services is constrained by limited government capacity to plan and implement social strategies and programs and a weak incentive framework which has a negative impact on the performance of public service providers, and weak capacity for social mobilization among civil society. Recently, there has been increasing political instability with four changes of government in two years. Sao Tome and Principe has recently discovered large oil reserves in the Gulf of Guinea bordering with Nigeria which puts the country on the verge of a major economic change. Large blocks for offshore oil production in a Joint Development Zone with Nigeria will be licensed by end of 2003 and oil production is expected to start in 2007. In light of the expected economic development, it is critical to strengthen the institutions and structures for the delivery of social services and to build the necessary human capital for sustained economic development and poverty reduction.
2.2. Political and administrative organization At the administrative level, the country is divided into six districts (Agua Grande, Lembá, Cantagalo, Caué, lobata, Mé-Zochi) and one autonomous region of Principe. The districts of Sao Tome are grouped together for the purpose of the study in three geographical and administrative areas which are: north, center and south, and are divided into villages.
2.3. Demographics With an average density of 133 inhabitants per km2, the population was estimated at 137,599 inhabitants in 2001. This population is distributed unevenly throughout the region with a strong concentration in the central region which comprises more than 62% of the total population of the country. The district of Água Grande, the heart of this region, is home to approximately 38% of the population of Sao Tome and Principe. The population of Sao Tome is very young (66.6% are under 25 years), and is mostly female (50.5% of women against 49.5% men). The urban population represents 55.6% of the total population.
Table nº1 – Geographic Distribution of the Population (2001):

9
District/Region Population % Population Sup. Km2 Densisty Lembá 10.720 7,9 229,5 46,7 Lobata 15.161 11,1 105 144,4 Região Norte 25.881 19 334,5 77,4 Agua Grande 51.591 37,9 16,5 3.126,7 Mé-Zochi 33.976 25,0 122 278,5 Região Centro 85.567 62,9 138,5 617,8 Cantagalo 13.188 9,7 119 110,8 Caué 5.511 4,0 267 20,6 Região Sul 18.699 13,7 386 48,4 Príncipe 5.978 4,4 142 42,0 Região Autónoma 5.978 4,4 142 42,0 São Tomé e Príncipe 136.125 100,0 1001 135,9
Source: Medical Waste Management Plan, 2004, from the RGPH of 2001.
The capital and principal port is São Tomé (population, 1990 estimate, 50,000), located on the northeastern coast of São Tomé island. The population, descendants of peoples who came to the islands beginning in the late 1400s, is composed of six identifiable groups: mestiço, or mixed-blood; angolares, descendants of Angolan slaves; forros, descendants of freed slaves; serviçais, contract laborers from nearby African countries; tongas, children of serviçais born on the islands; and Europeans, mostly from Portugal. Portuguese is the official language, but 90 percent of the people speak Fang, a Bantu language. Most of the people are Christian; 83 percent are Roman Catholic. The per capita income is estimated at $290. About 54% of the population is living under poverty line with limited human development due to weak and inefficient public institutions and limited and fragmented civil society organizations. The delivery of social services is constrained by limited government capacity to plan and implement social strategies and programs and a weak incentive framework which has a negative impact on the performance of public service providers, and weak capacity for social mobilization among civil society. Recently, there has been increasing political instability with four changes of government in two years. Sao Tome and Principe has recently discovered large oil reserves in the Gulf of Guinea bordering with Nigeria which puts the country on the verge of a major economic change. Large blocks for offshore oil production in a Joint Development Zone with Nigeria will be licensed by end of 2003 and oil production is expected to start in 2007. In light of the expected economic development, it is critical to strengthen the institutions and structures for the delivery of social services and to build the necessary human capital for sustained economic development and poverty reduction.
2.4. Health and Environment 2.4.1. Health Policy and the Environment

10
The health policy adopted by the Government of Sao Tome and Principe considers the primary health care as a basis for health development with the predominant role of the district health system. From the environmental point of view, the Government of Sao Tome and Principe approved a number of laws and regulations concerning the management of this sector. The Ministry of Natural Resources, Energy and Environment is responsible for implementing environmental policy in the country. Among the texts produced are: - Law No. 10/99, Environmental Law; - Decree No. 36/99, Regulation on the Procedure for Environmental Impact Assessment; - Decree No. 37/99, Regulation on the Environmental Impact Assessment; - Decree No. 36/1999, Decree on Waste.
2.4.2. Organization of Health Systems and Care 2.4.2.1. Administrative Structure The health organization is under the responsibility of the Ministry of Health and the national system is structured on two levels: - The central level is represented by the Ministry of Health and is responsible to implement the health policy set by the Government. It is at this level that are drawn national plans and the organization and supervision of the implementation of projects and programs assigned to the health sector. The central level also has a role of coordination, monitoring, mobilization and allocation of resources. - The district level is represented by the delegations of health as areas of intervention in all districts. The health district corresponds to administrative territorial division. This level is primary responsible for the implementation of health services within the community. 2.4.2.2. The structure of Care The structure of the system of care also comprises two levels. At the central level, the Hospital Central Dr. Ayres de Menezes is the reference for all health facilities in the country, including the cases of specialties. At the district level, the district health centers are run by medical health representatives, while health centers are run by nurses. The private health facilities, the community health workers, and traditional birth attendants (matrons), who work with the communities, are also part of the system. The following table summarizes the administrative division of responsibilities.
Table n. 2 – The National Health System
Levels Structures Biomedical and Sociomedical Institutions
Specialties
Central or National Ministry of Health Hospital of Reference (Hospital Dr. Ayres de Menezes).
Medicine, Pediatric, Surgery, Gynecology, Radiology, Lab, ORL,
11
Ophthalmology, Other Specialties
Hospital, Health Center of the district, Health Post, Private Sanitary Structures.
Medicina, pequena cirurgia de urgência, laboratório, maternidade, dispensário, farmácia ou depósito.
District Health Delegacy
Community Sanitary Posts
Care, Delivery
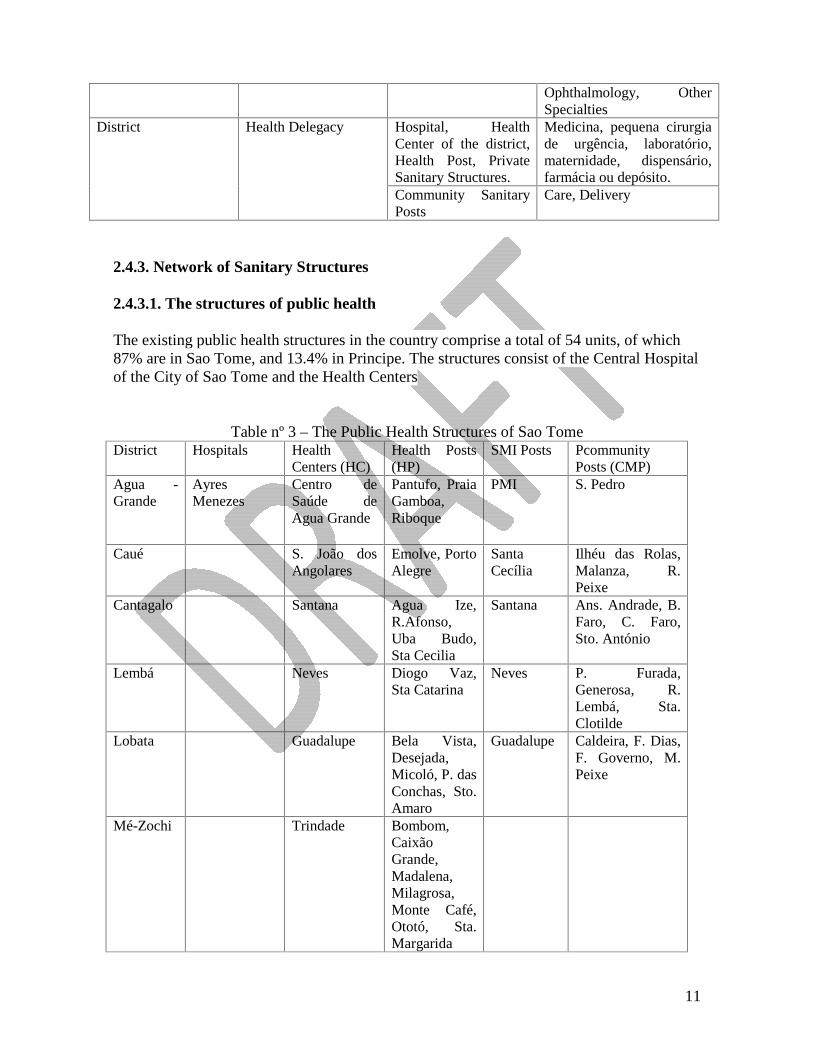
2.4.3. Network of Sanitary Structures 2.4.3.1. The structures of public health The existing public health structures in the country comprise a total of 54 units, of which 87% are in Sao Tome, and 13.4% in Principe. The structures consist of the Central Hospital of the City of Sao Tome and the Health Centers
Table nº 3 – The Public Health Structures of Sao Tome District Hospitals Health
Centers (HC) Health Posts (HP)
SMI Posts Pcommunity Posts (CMP)
Agua -Grande
Ayres Menezes
Centro de Saúde de Agua Grande
Pantufo, Praia Gamboa, Riboque
PMI S. Pedro
Caué S. João dos Angolares
Emolve, Porto Alegre
Santa Cecília
Ilhéu das Rolas, Malanza, R. Peixe
Cantagalo Santana Agua Ize, R.Afonso, Uba Budo, Sta Cecilia
Santana Ans. Andrade, B. Faro, C. Faro, Sto. António
Lembá Neves Diogo Vaz, Sta Catarina
Neves P. Furada, Generosa, R. Lembá, Sta. Clotilde
Lobata Guadalupe Bela Vista, Desejada, Micoló, P. das Conchas, Sto. Amaro
Guadalupe Caldeira, F. Dias, F. Governo, M. Peixe
Mé-Zochi Trindade Bombom, Caixão Grande, Madalena, Milagrosa, Monte Café, Ototó, Sta. Margarida

12
Príncipe M. Quaresma D. Graça
Príncipe – Santo António
Aeroporto, N. Estrela, Picão, Porto Real, Sundy
Total 2 6 24 3 + 3 = 6 21Source: Medical Waste Management Plan, 2004, from the Sanitary Chart of STP, 2000.
2.4.3.2. The structures of private care The private sector is not very significant. This activity is concentrated in the district of Água Grande with some clinics, a dozen structures that practice general consultations, injections and some curative activities of small size. Those structures are not systematically surveyed, and their presence is, in many cases, informal. There is an ongoing project for the official recognition of their existence, through a legislation that seeks to organize their operation. 2.4.4. Evaluation of the production of biomedical waste The assessment is made on the basis of a weekly weigh in the Central Hospital, the PMI and the Health Center of Angolares. Under the previous MWMP, there was a weekly weighing. As part of this update, for reasons of time constraint, we start with the principle that the current situation did not change significantly from the previous one and that the same assessment is still valid, having been confirmed with the authorities in the respective sectors.
Table 4 – Assessment of production of biomedical waste (kg) in the Central Hospital Dr. Ayres de Menezes
Services Total/Day Pediatric services
Medicine Day
Surgery Bloc
SCM SCH Maternity
I II Men Women Sunday 8 11 13 25 10 20 9 7 103 Monday 10 18 15 29 13 23 12 11 131 Tuesday 9 16 14 26 14 22 15 11,5 127,5 Wednesday 14 14 13,5 30 11 21 14 13 130,5 Thursday 15 14 17 25 13 26 14 12 136 Friday 16 16 15 27 12 28,5 10 13 109 Saturday 16 12 14 32 17 24 11 9 137 Total Service
88 101 101,5 194 90 164,5 85 76,5 ------
Total waste per week 874 Média res./dia
125 Média resíduos/ Bed (375)
0.333 0.29
Total BMW/week (25%*) in Kg
218** Average waste
31* Average BMW /
0.88 0.07
*Africa: estimated production: 1,3 a 3 kg/bed/day with 75% a 90% of municipal waste e 10 to 25% de BMW ** Needles represent respectively 1,8 kg of the biomedical waste/per week, 0,254 kg/day SCM – Surgery Services for Women; SCM – Surgery Services for Men

13
Table nº 5: Assessment of Production of Biomedical Waste (kg) in the PMI Services
Day Infant, nutrition, maternal Total/Day
Sun Mon 5 5 Tue 5,5 5,5 Wed 4 4 Thurs 5 5 Fri 4,5 4,5 Sat Total Service
24
Total waste per week 24 Aver. waste/day
4,8 Average waste/patient (206) 0,023
Total BMW/week 25%
6 Average BMW/day
1,2 Average waste/patient (206) 0,006
The weighing conducted in a private clinic shows a total of 19 kg per week, e.g. 2,71kg/day, of which 10% of biomedical waste or 0.271 kg for an average frequency of 30 people per day. Therefore, the production of biomedical waste will be 0.009 kg.
Table nº 6 – Assessment of Hospital Production Production/Kg District Structure Nº of
beds Number of
Patients DMS Nº of days of
hospitalization Occupation rate %
Nº of occupied beds
Day Month
Year
Lembá HAM 375 26001 5.91 153101 11,55 418 33,44 1002
12205
Caué CS Neves 40 24464 13001 89 36 4,7 141 1715 Lobata CS
Angolares 17 702 3.2 2248 61,7 10 1,32 40 482
Príncipe Guadalupe 14 1053 5 5265 103 14,5 1,91 57 698 Total/dia CS
Quaresma 30 1533 5 7665 70 21 2,8 84 1022
Total/Dia 44,17 1325 Total/ano
16122 HAM – Hospital Ayres Menezes
The Central Hospital and the Policlinic of Água Grande along with the Health Posts of Pantufo and Praia Gambôa produce 23 tons of biomedical waste per year. This production represents 83.84% of the total biomedical production in the country. It represents 63 kg per day without the PMI and private structures.
Table nº 7 – Assessment of production of other centers Production, Kg District HC Nº of
patients/year Nº of patients /year
Day Month Year
Água Grande São Tomé 14.558 80 29,6 888 10.804

14
Cantagalo Santana 3.489 10 3,7 111 255
Mé-Zochi Trindade 3.647 10 3,7 111 255
Total/dia 37
Total/mês 1.110
Total/ano 11.314

15
Table nº 8 – Assessment of production of health posts
Distrito ÁguaGrande
Lembá Caué Lobata Cantagalo Mé-Zochi
Structure
PANTUFO
P.GAMBOA
DIOGOVAZ
STA.CATARINA
EMOLVE
P.ALEGRE
BELAVISTA
DESEJADA
MICOLO
P.CONCHAS
STOAMARO
AGUA
IZÉ
RIB.AFONSO
UBA
BUDO
S.CECILIA
BOM
BOM
CAIXGRANDE
MADALENA
MILAGROSA
MONTE
CAFÉ
OTOTO
Sta.MARGARIDA
PolarizedPopulation
5143 9720 632 1910 1910 1227 1804 2484 2109 647 2515 2273 2028 1076 705 11868 4486 2597 803 1893 548 257
Frequency perNA
3908 7387 480 1451 1451 932 1371 1887 1603 492 1911 1965 3239 899 424 3005 4454 3079 1011 1336 460 1830
Frequency/Day 11 20 2 4 4 3 4 5 5 2 5 6 9 3 2 9 13 9 3 4 460 5
Production(25% BMWbase PMI) gr
66 120 12 24 24 18 24 30 30 12 30 36 54 18 12 5478 54 18 24 12 30
Total 186 36 42 126 120 270
Total/day 5580 1080 1260 3780 3600 8100
Total per Year 678890 13140 115330 45990 43800 98550
NB: The daily frequency of Cantagalo and Mé-Zochi is used to estimate the frequency of other districts .For a total polarized population of 28.534,the numberof consultations was 21.702, or a 76% frequency.
The annual production of health posts is 284.72 kg, of which 81 kg are produced in Água Grande and 98kg in Mé-Zochi. Theproduction of the 24 Heath Posts is estimated on average at 35.45 gr/day/each. Taking into account that each of the 21 CHP produce onaverage 1/3 of the Sanitary Posts, or 11,82 gr/day, the following table presents the production of those CSP, which will be 248 gr/dayor 90,55 kg/year.

16
Table nº 9 – Assessment of production of community Health Posts District
Structure
Production per day, gr
Production per month, gr.
Production per year, kg
Agua Grande
Private Clinic 11.82 355 4.3
Lembá P. Furada, generosa, R. Lembá, Sta. Clotilde
47.28 1420 17.257
Caué Ilhéu das Rolas, Malanza, R. Peixe
35.46 1060 12.94
Lobata Caldeira, F. Dias, F. Governo, M. Peixe
47.28 1420 17.26
Cantagalo Ans. Andrade, Bernardo Faro, Claudino Faro, St. António
47.28 1420 1726
Príncipe Aeroporto, N. Estrela, Picão, Porto Real, Sundy
59 1770 21535
Total 248grTotal per month 7.451 kgTotal per year 90.55 kg
Table nº 10 – Estimated production of biomedical waste per district District
Água
Grande
Lembá
Caué
Lobata Cantagal
oMé-Zóchi
Príncipe
Structure
Hospital
12205
Centers
1084 1715 482 698 255 255 1022
Health Posts 68 13 15 46 44 98 Community Health Posts
4.3 17 13 17 17 21
PMI 438 Private Clinics 494 Total per year, Kg 24013 1745 510 761 316 353 1043 Total per Kg 66 5 1.4 2 0.86 0.97 2.86
A total of 8 tons of biomedical waste are at least produced nationally

17
2.4.5. Analysis of the legislation Following the Rio Declaration (1992) on Environment and Sustainable Development, the country has adopted the Environmental Law (Law No. 10/99) with one of its fundamental principles to promote a better quality of individual and collective lives of citizens. This law sets out specific principles that should be taken into account in the general framework of environmental management in Sao Tome and Principe, namely: the principles of precaution and prevention, noting that an environmental impact assessment should be required as a prevention mechanism and as a way to reduce any impact on the environment; the principle of respect of the ability to change the ecosystem; the principle of management and appropriate use and reuse, the principle of citizen participation in decision-making; the principle of the payment by the user, and the principle of payment by the polluter. The objectives of this law are, inter alia, the conservation of the nature, the determination of the quality of the components of the environment, the promotion of public participation in decision-making, the protection of the air and climate, the proper management of waste, a guarantee of lower environmental impact of activities, and the use of best available technology to minimize environmental impacts. The environmental components were well defined and, under its protection, various safeguards mechanisms have been outlined. For the air, it is expected that all mechanical equipment and vehicles that could affect air quality must be equipped with adequate provision or process to eliminate or neutralize the pollutants. With regard to waste and effluents: - The waste and effluents must be collected, stored, transported, disposed and reused so as not to constitute an immediate hazard or potential health risk or cause damage to the environment; - The trash should be accepted in a site determined by the competent authorities and under the conditions provided in a prior authorization. As part of the instruments and mechanisms for environmental policy of Sao Tome and Principe, a fee has been introduced for the use of natural resources, as well as the remaining effluent. In the article 45 of this law, devoted to Environmental Impact Assessment (EIA), there is a definition of the activities subject to environmental impact assessment, and the contents of the (EIA) with an emphasis on public consultation of affected populations. The National Environmental Commission (CNA) is an advisory body endowed with administrative and financial autonomy under the supervision of the Office of the Prime Minister and chaired by the Minister responsible for the environment. CNA brings together representatives from all districts, chambers, NGOs, and trade union organizations. The Decree No. 36/99 on Urban Solid Waste came into force on 30 April 1999, and in its

18
article 7 on the biomedical waste, it stresses the obligation for the Chambers to carry out inventories of sanitation facilities for waste producers, and indicates the quantity, nature, origin and destination of waste generated or collected. The decree defines the powers of the central government and the roles of the Ministry of Environment, Health, Industry, Trade and Tourism in setting out the policy, national and regional plans and directives on the general characteristics and treatment, the final destination but also the promotion of investments related to the control of dumps and other facilities for the treatment and final disposal of waste. The Boards have a role to play in the definition of the systems of collection, processing, planning, organization and implementation of collection, and transportation of the waste. The law also addresses the technical aspects of waste management including: collection, which should take place early in the morning or afternoon, transport (which includes biomedical waste), and screening (only domestic waste). The treatment process recognized or covered by the law concerns the landfill site, incineration, composting and recycling. The facilities receiving waste for treatment and as final destination must hold a license granted by a competent management structure. This license is obtained after providing the following information: - The identification of residual levels (category, type and amount); - The identification of procedures for supervision and registration of waste; - The description of the process or of the technologies used; - The security procedure to use in case of industrial accident. Specific procedures are established, especially for the approval of sites to be authorized to handle disposal: geological features, hydrological and hydro-geological impact study, means and methods of operation and supervision during operation. With regard to incineration: type and capacity of equipment, temperature and time of incineration of the plants, surveillance, characteristics and effluent height of the chimney. For chemical facilities: method, nature and composition of effluent and the respective control. It is specified in the article 26 of the decree that the landfill site should be located at a distance of at least 500 m from residential areas, areas of development of agriculture, protected areas, as well as the sources of the rivers and coastline. Deposits should not be sited less than 200m. However, the decree does not provide for: - The process of collection or disposal of industrial and hospital waste, and the relationship between the content and the quantities of waste, the location of sites of treatment, the type of treatment in relation to the type of waste; - A more detailed classification of biomedical waste and the treatment methods; - The details on how to transport such waste, particularly the standards of vehicles, transport procedures, personnel transport.

19
The Environmental Impact Assessment is regulated by decree No. 37/99, adopted on August 3, 1999 and includes: a pre-assessment, an environmental impact assessment and proper consultation. In terms of implementation, the analysis is done within 60 days. 3. Update on the management of hospital waste 3.1. Analysis of the management practices of hospital waste The biomedical waste management carried out both by public health facilities and private sector varies widely depending on the structures, but usually comprises two fundamental components: a comprehensive internal management of infectious waste made by the health facilities themselves, and a second internal management ensured by the health facilities with the disposal of waste collected by the municipality or the private sector. However, in general, the image conveyed from the point of view of hygiene in most of the structures visited is not the best. It shows a great lack of care with regard to waste management situations, such as syringes scattered on the ground around the animal waste. In certain situations, some wild dumps and biomedical waste are found mixed with other waste. There is no management plan for these residues. The production of biomedical waste is not rigorously known, and there is no systematic weigh, even at the level of equipment destruction / disposal.

20
3.1.1. The cleaning staff The cleaning staff in health institutions is composed of support staff responsible for the cleaning, pre-collection and collection of household waste and biomedical waste and the cleaning of all areas. The staff is therefore especially recruited for these tasks. This staff usually works without full protection. The cleaning and evacuation of the facility is managed by the staff of the structures. The collection and transport abroad is carried out by private individuals or by the municipality or by each sanitary structure itself.
Collection and separation of biomedical waste The pre-collection and collection of waste (household waste and assimilated waste, including biomedical) are made through vessels of various types: plastic buckets or aluminum bearing, or through the crates. Almost all of these collection containers generally receive, almost with no distinction, rests of meals, drug packaging, injection ampoules, used towels, bottles of serum, syringes, needles, blood bags, etc. The residues are hardly packed (bagged). While the Central Hospital does not have bins for the collection of waste, the policlinic of Agua Grande and the PMI make available such equipments to ensure thorough cleaning of its premises.
The organization of the separation of waste varies according to health facilities and services that integrate these structures, particularly with respect to needles and placentas. The needles of the syringes are often separated from the source and are collected in bottles or infusion, in plastic bottles recovered or collected in plastic containers or in safety boxes in the maternity, injection units, and in the chirurgical block. Because of the lack of these equipments in the laboratory, boxes to collect analysis are used for that purpose. In some rare cases, the team of health care uses a cart equipped with care bins and a receptacle to receive needles. The bins are used to receive the cotton swabs and used syringes, etc. The cotton, discarded gloves, used tampons, pads, etc as well as the blood bags are locked up in boxes without any packaging and sent to the final or intermediate gathering. The materials used in surgeries and delivery are sent, separately, to the laundry room of the Central Hospital. Surgical derivatives of small proportions are packaged in boxes without special separation, while the big pieces are packed, chilled and sent to the cemetery. At the Blood Bank of the Central Hospital Ayres de Menezes, the blood bags of seropositive indivduals (Hepatitis B) and HIV (AIDS) are separated and collected separately in a box before disposal by the hospital system (burning). In the block of delivery, the rests of the birth (placenta and derived liquid) are delivered to family members, or are buried in the yard or placed in bags and then buried in the hospital. Newborns dead are evacuated to the morgue for burial in the cemetery. In Radiology, the non exploitable plates are separated and deposited. However, the health center of Guadeloupe (in Lobata) carries out the separation of infectious waste throughout the entire line of the management system.

21
3.1.3. The internal storage system Generally, the waste is placed in bins located in areas not specified in the corridor or in the front yard of services. Note that the waste that had been initially separated, are also put in these boxes, which invalidates the efforts of separation made at source. These boxes are often too full or the waste is placed to the side, which constitutes a danger to the personal of collection - evacuation. 3.1.4. Systems of disposal of waste within the health structures The disposal of waste, separated or not, is done by the support staff or by specific staff assigned to this task. The handcarts and tricycles are used in the Central Hospital, the crates are also transported directly by one or two assistants on the basis of size or weight of the crate. The disposal of waste is done mainly early morning and late in the day. 1.7. Systems of internal treatment At the Central Hospital, the waste separated at source, particularly needles, joins the circuit of collection and interim storage, and then finally goes to a container. There are discarded needles or syringe without plunger, needles still embedded in the syringes, with or without the plunger, which is particularly dangerous for the personal of collection. Thus there is a break in the line management of biomedical waste, causing a malfunction in the system of collection, in particular for longer needles that should not be discarded in any place so as to avoid any risk. These wastes are then burned in an incinerator recently purchased by the Central Hospital. In the Central PMI of Sao Tome, cutting waste are handled separately through the burning behind the building itself, directly on the floor. In the case of maternity of Angolares, the needles are burned immediately, in a small excavation. The health center of Guadeloupe has a "furnace for incineration" functional at the back of the building, but near a school. The HP of Santo Antonio is located halfway between an occupied dwelling, and the waste is burned in an ’oven for incineration " every day during the afternoon, the ashes are then collected and transported in a bucket to dump on the next installment. As for the placentas they are thrown into the excavations made within the health structure. In the central hospital, the placentas are burned along with other waste, such as infected blood bags. 3.1.8. Transport system and external processing There are several ways of transporting, including the intervention of the municipality (Chambers), and the use of the own resources of the health structures. Once a week (usually on Saturday), the burned products of the central hospital are transported in a truck hired by the central hospital staff with very weak protection (no boot, no uniform) or through an automatic truck and deposited in a trash situated a few miles. The waste from the kitchen is instead discharged by the Board. Waste from other structures of the city of São Tomé is transferred to the trash by the Board at the same time with the waste from other households collected within the same system. The

22
presence of children playing with garbage is a common reality. The trash is guarded by an officer of the Board who also directs the trucks according to the nature of the waste to the precise places where the trash should be deposited. Therefore, in Sao Tome, it is possible to find waste not completely burned from the hospital, biomedical waste that has not undergone any treatment from the Policlinic of Agua Grande and other private clinics. In Angolares, the biomedical waste and other wastes are transported by the vehicle of the Health Center and unloaded in a warehouse 4 km from the city. Municipal Waste Management in Sao Tome and Principe: The Case of Sao Tome
The House District of Sao Tome carries out a daily collection of all solid waste early in the morning. Sometimes it goes throughout the day and night. The collection is made with automatic vehicles obtained with the support of Taiwanese cooperation, but also with some private vehicles. The staff working on the collection consists of agents supported by local council prison. The works are accompanied by drivers and supervised by a responsible. All wastes, including biomedical wastes, are transported without any charge-discharge to Boa Morte where an enforcement agent guides vehicles to the areas chosen for storage. It is also noted that individuals transport their waste to the trash located 3 km from the city center, once of difficult access, but which has benefited from some improvements. Currently, the site is surrounded by houses, whose number is constantly growing. City workers make a small recovery activity with their bags tied to vehicles, but, even so, they are not adequately protected. Washerwomen wash their clothes every day in a small stream that passes right beside the trash. The environmental situation is degrading more and more. The Ministry of Environment and the safeguard District Board decided, after mutual consultation, to move the trash to a site identified in Correia (cp. topographical plans) more or less close to this town. The study of impact will be conducted before the assignment of the locality. Studies are currently underway in order to provide the local conditions for the implementation of a landfill to be built with support from the Spanish Cooperation (preliminary studies). The site seems to meet the technical conditions necessary for the implementation of that structure, awaiting an evaluation by the government. Access to this location is less difficult. There are, for now, homes nearby. It is a system of composting, incineration and controlled landfill. The Case of Guadalupe
A small tractor is used for the collection at the main road and the market; the collection is carried out by five officers. The waste collected is transported to an easily accessible recycle bin, and that needs to be improved. The residues of the health center are transported by means of the center, including a 4x4 vehicle offered by the French cooperation. The infectious waste and sharps are incinerated in an incinerator installed behind the building between it and a school. The case of Angolares
The Board carries out a group collection with a tractor with 8 operators, and the waste is deposited in water along the main road. This collection is carried out 3 times a week. The

23
wastes are then transported to a valley near the main road that goes to Angolares, turned into trash with an anarchic deposit taking down a beach, although not very crowded.
Current Status of Training and Awareness
With rare exceptions, the health staff was not trained on the management of biomedical waste. The Health School Training Program exists in the city of Sao Tome since 1979, providing training to nurses, laboratory technicians, statisticians, midwives, etc. Previously, the training was conducted in the different structures. At present, a functional facility is operational and serves as a place for training. From 1979 to 2000, 484 officers were trained in various areas. During the period 2002-2005, 108 nurses and 12 midwives were added to the already 28 nurses trained in 2003. The only course of sanitation for nurses (40 hours) and midwives (20h) addresses the management of solid and liquid waste, and air pollution. However, biomedical waste is not taught in a specific and detailed manner. Indeed, the curriculum is as follows: sanitation (general - definition); basic activities of sanitation, water sanitation (health and economic importance); treatment of excreta and waste, water treatment, food hygiene, school hygiene, hygiene of the workplace; hygiene of habitat, control of animal and insect vectors. On awareness, the issue of waste is often relegated to a second plan due to the lack of resources to cope with an increasingly important job (increase of the number of consultants). However, the delegates of health centers (HC) raise awareness about the health structures and safe handling of biomedical wastes. They have even notified about the need for specific training on biomedical waste in order to initiate a change of attitude in their work and in the use of services by the staff. 3.3 Summary of factors that limit a sound management Although a cleaning structure is part of the organizational framework of the staff, the situation may be characterized by:
- The lack of a defined management plan approved by the health structure; - The lack of processing equipment in most structures, - Insufficient support for pre-collection, using the bins - Lack of training and information for staff involved in the management of biomedical
wastes - Risks and absence of measures on its handling, - Non-enforcement of existing legislation
4. The Biomedical Waste Management Plan
The Biomedical Waste Management Plan of Sao Tome and Principe is structured around various components depending on the conditions of the waste. Specifically, it takes into

24
account the biomedical waste along the system of collection until the final disposal around the country. In order to ensure the quality and effectiveness of the system of management and the security of the personnel, the following provisions were incorporated into the preparation of the Plan: - Improve the quality of services of cleaning and management of biomedical waste in a streamlined operating environment, through the development of management plans for all structures; - Improve and increase resources for pre-collection and collection of waste in general and biomedical wastes in particular, promoting the separation from the source; - Provide personal protective equipment (masks, gloves, uniforms, etc.). - Establish an adapted collection - removal - storage - transport and disposal system; - Encourage the development of vigorous regulations adapted to the local context; - Organize training sessions on the rational management of biomedical waste; - Sensitize the stakeholders on the need to respect the rules. The proposed Management Plan is structured around (4) four key areas, according to the causes of malfunction, inefficiency and the level of efficiency found in the analysis of the situation: namely: - The structure and equipment of the system; - The strengthening of the institutional, legislative and regulatory framework - The implementation of information campaign and awareness; - The implementation of a national training program As stipulated in the terms of reference, a strategic framework for implementation at the institutional level has been proposed, and it is now up to the government of Sao Tome and Principe to make a choice among the range of proposals presented. However, the advantages and disadvantages of the different scenarios are highlighted. The general objectives of the Action Plan are summarized as follows:
4.1. Line management of biomedical waste
4.1.1. The chain of collection, transportation and disposal procedure
25
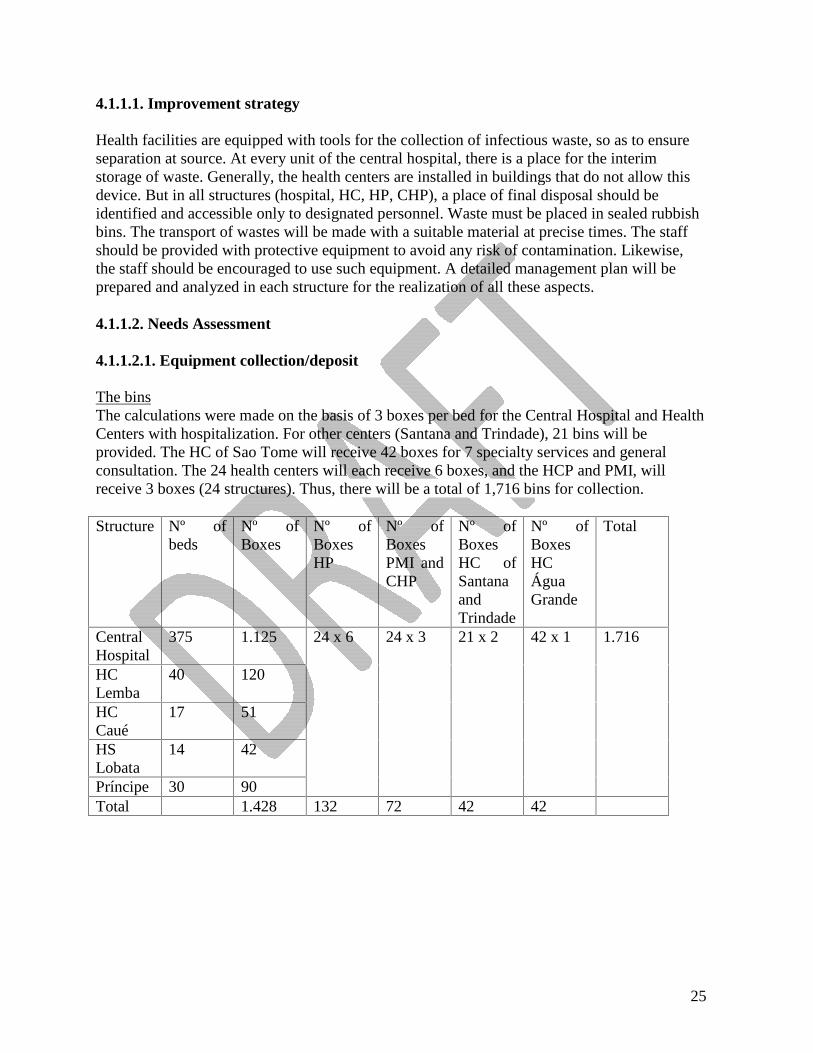
4.1.1.1. Improvement strategy Health facilities are equipped with tools for the collection of infectious waste, so as to ensure separation at source. At every unit of the central hospital, there is a place for the interim storage of waste. Generally, the health centers are installed in buildings that do not allow this device. But in all structures (hospital, HC, HP, CHP), a place of final disposal should be identified and accessible only to designated personnel. Waste must be placed in sealed rubbish bins. The transport of wastes will be made with a suitable material at precise times. The staff should be provided with protective equipment to avoid any risk of contamination. Likewise, the staff should be encouraged to use such equipment. A detailed management plan will be prepared and analyzed in each structure for the realization of all these aspects. 4.1.1.2. Needs Assessment 4.1.1.2.1. Equipment collection/deposit The bins The calculations were made on the basis of 3 boxes per bed for the Central Hospital and Health Centers with hospitalization. For other centers (Santana and Trindade), 21 bins will be provided. The HC of Sao Tome will receive 42 boxes for 7 specialty services and general consultation. The 24 health centers will each receive 6 boxes, and the HCP and PMI, will receive 3 boxes (24 structures). Thus, there will be a total of 1,716 bins for collection. Structure Nº of
beds Nº of Boxes
Nº of Boxes HP
Nº of Boxes PMI and CHP
Nº of Boxes HC of Santana and Trindade
Nº of Boxes HC Água Grande
Total
Central Hospital
375 1.125
HC Lemba
40 120
HC Caué
17 51
HS Lobata
14 42
Príncipe 30 90
24 x 6 24 x 3 21 x 2 42 x 1 1.716
Total 1.428 132 72 42 42

26
The estimate was made for different types of structures. Thus, 24 batches of 25 content will be delivered to the Central Hospital (50 services, e.g. 600 cases per year), 29 lots for HC and PMI (about 10 servings, or 120 cases a year), 25 lots to HC (about 13 servings, or 156 cases per year). Personal protective equipment consists of a lot containing a pair of boots, a uniform, gloves and a pair of shades. The total number of persons responsible for management of biomedical waste in terms of collection - transportation - storage stands at 339. Table nº 13 – Number of people to be equipped in the sanitary structures Structure Number of People per
Structure Number of Structures Total
Central Hospital 101 1 101 HC Hospitalization 20 4 80 HC without maternity ePMI
10 5 50
HC 3 22 66 CHP 2 21 42 Total 339
For interim and final storage, 4 boxes of 2m2 will be built at the central hospital. In all health centers and PMI, the final repository will be made of a setting of 4 m2 with three crates. It should be found at the PS levels, a place with 2 m2 to place a crates. At the Policlinic of Agua Grande, the existing site will be provided with 4 crates.
Structures Box Local Surface of Final Deposit
Boxes
Central Hospital 4 x 2 = 8 m2 1 x 10 m2 = 10 m2 10 Health Centers 6 x 4 m2 = 24 m2 18 PMI 3 x 4 = 12 m2 9 Health Posts 22 x 2 m2 = 44 m2 22 Policlínic of Água Grande
4
8 m2 90 m2 63
At the Central Hospital, two tricycles should be purchased to replace the existing equipment in poor conditions. The Polyclinic and the PMI will have a total of 4 stand-door bins. Also a total of 28 wheelbarrows should be purchased and sent to other health centers and clinics.

27
4.1.2 The treatment chain: determination of technology 4.1.2.1. Treatment technologies Treatment technologies currently available for treatment and disposal of biomedical waste are very diverse. There are two categories of devices: those that allow the elimination of pathogens, reducing the volume and weight of the waste; and those whose final outcome is the destruction of microbes and their support. The following techniques will be used for this purpose: steam sterilization, incineration, landfill, refrigeration and freezing, chemical inactivation and neutralization, disinfection after grinding. 4.1.2.2. Comparison of systems according to effectiveness and eco-environmental criteria The incineration and steam sterilization are currently two of the most frequently used methods for the treatment of biomedical waste. The combination of the two techniques is, in some cases desirable, particularly if the burning takes place outside the health structure. The following tables define the categories of biomedical waste, its current management and the types of treatment and disposal fittest. Note that, in effect, incineration is a more radical technique, but the landfill remains the technique resulting in virtually all technologies.
Table nº 15 – Elimination chain according to the categories
Example of investment and operating costs Pyrolytic incinerator dual-chamber: 0.4 to 1 ton per day: 50,000 a $ 100,000 holding $ 380 per ton of waste, Chemical disinfection: virhoplan 50,000 to 100,000 $ and 100 to 12,000 dollars per ton;
TYPE OF MAIN ELIMINATION
PREVIOUS CONDITION
NON TREATED WASTE
RESULTIING CHAIN
Separation at source Incineration Esterilization
ATERRO Separation at source (hospital)
Anatomic biomedical waste
Contaminated non-anatomic radioactive or dangerous
Esterilization Refrigeration
FreezingIncineration
INCINERATION Chemicals Radioactive Content under pressure landfill
CHEMICAL DESINFECTION
Mechanical trituration
landfill
IRRADIATION Trituration Landfill
28
Moist heat treatment: from 50,000 to 200,000 $, and $ 400 per ton Microwave: 50,000 $ per 250 kg per hour, 3,000 tons per year De Montfort (dual fuel) 1,000 a $ 3000 SICIM (spontaneous combustion) $ 2500 Vulcain (propulsion air) $ 5000 + air incinerator fuel from $ 10,000 to more than $ 50,000 4.1.2.3. Choice of technology The choice of disposal system must meet the criteria set out above and in particular, take into account the local context. Therefore, it should take into account: - The economic context; a more radical waste disposal would be better. - For this system, the structures should invest in a reasonable amount of material at an acceptable price; - The operating cost should be affordable by the budgets of health facilities. Given its relatively high investment costs as well as the cost of maintenance, and the fact that its implementation requires a high technique, the microwave is not very recommended in developing countries in general and, therefore, in Sao Tome and Principe. Although it is technically less complex, the sterilization by autoclave is expensive and is not radical. The landfill could also be a solution for treatment. In this case, however, all guarantees should be done to prevent pollution of groundwater. This is also true for the equipped or burned pit. Because they are relatively cheap, but also because of the possibility of renewal after depreciation and especially because of the daily maintenance, the incinerators of medium and small capacity should not present major problems provided the staff members are trained on their use. Also the health and environmental impact is low if there is effective equipment. Given the estimated production of biomedical waste in health facilities, the choices can be on various types of treatment that can be combined: incineration, deposit in a trash, but also the specific destruction of sharp materials. An incinerator of small capacity could be used for all health facilities in the city of Sao Tome. Moreover, health centers will be equipped with incinerators of the type Montfort. 4.1.3. Alternative strategies for implementing the disposal
4.1.3.1. Treatments - External articles This chain implies that the health structures will organize a treatment of their waste in their facilities after a separation at source. The waste will then transported to the disposal site. For the transportations, variants can be analyzed: 1. Polarization of biomedical waste for the structures with equipment disposal. Transportation is provided by a private structure, or by their own structures, or in combination. These structures will charge fees for processing, treatment/disposal. 2. Installation of treatment plant in a location outside the existing health structures. The investment would be undertaken by a company’s of assets and would involve the public

29
hospitals, municipalities, clinics and other private health facilities. The operation of the treatment plant will be provided by a private management company that would be in charge of shipping. 3. Because of their experience and responsibility in the management of solid waste (household waste) and landfill waste, the municipalities could secure the investment and operation of systems of treatment/disposal of biomedical wastes. To this end, they could receive funding from the state or receive grants from the development partners. They would have to contract with health facilities that produce biomedical waste, which could allow them to increase their available resources in the management of waste and to pay the producers for the treatment of non-assimilated disposal by the domestic refuse. 4. Investment and operation undertaken by private developers equipped with technical and financial capacity. Thus, the removal is done by a private company that for example offers and manages its incinerator, since the waste is provided by health facilities. Transportation may be provided by the same company or by other means listed above. The selected private company will be responsible for collection - transport - transfer and disposal of waste in the trash as well as of all the necessary equipment and structures. The transport equipment will also be the responsibility of the company in case of subcontracting of part of the system with well-defined conditions. 4.1.3.2. Treatment and internal disposal This fifth variant comprises two phases: 1) The decontamination of waste at source to remove or reduce the obligation to resort to external solutions; 2) Burning within the structure 4.1.4. Analysis of Strategies VARIANT 1: Polarization through existing treatment equipment.
This variant appears to be operating in Sao Tome in the absence of performing material in the structures and this scheme would be applicable only in Sao Tome. VARIANT 2: Creation of a Patrimonial Company The implementation of this strategy is influenced by the following preconditions: the political will of the government to participate in the investment and to select a management company through a bidding process; the implementation of means of control at the health administration structures so that they send their waste to treatment plants for the maintenance; the allocation of the structures relying on the public budget for waste disposal. A contract should be signed with all parties that manage health facilities. VARIANT 3: Intervention of municipalities – Chambers.
30
Currently the dump sites are not operational for this type of waste. The advantages of this variant will be only effective if there is a licensing system to private companies and adopted by municipalities that have difficulties with the efficiency and regularity of its service. VARIANT 4: Full Management by a Private Developers One or various private companies invest in the purchase and provision of equipment and are in charge of management of the waste disposal. VARIANT 5: Treatment and internal disposal Option for the internal elimination is applicable to isolated structures located far from the potentially polarizing structures because the shipping cost will be exorbitant if it is adopted a system of collection of three times per week. But the generalization of this scheme creates a lack of economies of scale (the permanence of fixed costs regardless of the size of the health structure in question) and each structure will be required to equip itself with qualified personnel for management of these units whatever amount of biomedical waste it produces.
4.1.5. Strategies and perspectives 4.1.5.1. Management systems in practice: collection, disposal and treatment. 4.1.5.1.1. Improvement strategy
The Government of Sao Tome and Principe should make a choice of different strategies. However, three alternatives are presented: a) The biomedical waste is discharged by the Board through a special equipment for transport and sent temporarily for the trash of Boa Morte, a special space where plants will be created for that purpose. Then, the waste will be transferred to the discharge of Correia if this site is finally chosen to install the incinerator; b) The same operation of transport and treatment will be performed by a private company; c) The same operation is carried out under its own control by the sanitation services. The advantage of involving the Board is that it will incorporate into its operation this new business that allows a transfer of investment to the Central Hospital, which currently pays for this service to a private company. Thus, the amount spent now could be invested in the purchase of packaging bags. Private organizations will continue to be served as currently done. The first investment in transport equipment and treatment will be made by the project and the renewal by the Board.

31
A private investment in transport equipment and processing will first require the publication of a law, since it involves the payment of a fee to be calculated as a pro rata of the waste produced, and to be reviewed annually, according to the opening of new clinics. Being the first investment to be made by the project, the sanitation facilities will organize themselves to form a transport team and a team responsible for processing. The replacement of the equipment will be ensured by these structures on the basis of charges for these two services. In short, it is proposed the creation of a patrimonial society, which will be the "owner" of the transport equipment purchased in the first investment through the project and will be responsible for management. Indeed:
- the private sector has concerns about investing in processing equipment because interest rates for lending in the commercial banks are very high (34%) and there is any assurance that the companies will be paid by sanitary structures;
- The Chambers may have difficulties in ensuring the continuity of the services; - Health facilities may endorse to a leading structure the operation and renewal of
equipment, because the patrimonial rights are common. The patrimonial company created by the Ministry of Health will charge taxes at public and private health facilities to ensure the operation and replacement of equipment, and that the liability of such charges meet the criteria that needs to be regulated. It has the responsibility of contracting a management company or composing a team (hiring some of the sanitation agents) that will operate the transport of biomedical waste to the place of treatment and disposal. At the other districts levels, there are more other constraints that must be noted, in particular the fact that the land for the installation of infrastructures is very limited, and the services provided by the Chambers are deficient. For example, the incineration practiced now in Angolares and Guadalupe presents many problems (proximity of housing and schools). Improving the treatment of biomedical waste will be ensured through: the abandon of in situ burning as an alternative; the disinfection of the waste after its deposit, the review of urban development plans in order to locate the sites identified to serve as a deposit. The final proposal is, therefore, the following: Actual site not appropriate
Needle Placentas Others DBM Transport Preparation of sites outside the structures
HC maternity
Tank Incinerator Montfort Tricycle Yes
HC without maternity
Incinerator Montfort Tricycle Yes
Actual site appropriate HC maternity
Destruction by the incinerator of São Tomé with the strategy of change of “safety box”
Tank Incinerator Montfort No
32
HC without maternity
Incinerator Montfort No
Health Posts
Destroyer Hole of the incinerator built
CHP Destroyer Hole of the incinerator built
Needs Assessment a) Collection and transportation
Purchase of two (02) closed cars to the collection in Sao Tome. In health centers, the frequency of collection will be 3 times per week (Praia, Gamboa, Pantufo). If we estimate that 80% of the health centers are located in places not suitable for making a treatment plant, we have to prepare and get 6 spaces and 10 tricycles for transportation. b) Treatment: incineration A small model modern incinerator will be purchased to serve the sanitation of the city of Sao Tome, six pits for placentas and 6 incinerators Montfort will be built. For 20 health centers and 20 community health centers, 40 hand destroyers of needles and 40 holes incineration holes will be built. 4.1.5.2. Funding Systems 4.1.5.2.1. Financing Strategy The plan should be financed jointly by the partners and the State of Sao Tome and Principe. A key aspect is how the system works and the renewal of equipment to enable an effective sustainability and the improvement of management of biomedical waste, which can only be managed locally. The company in Sao Tome will include in its taxes the renewal of the mobile equipment and the incinerator. Each structure will put in the preparation of its annual budget a line for the procurement of equipment of protection, etc. Community participation can be requested through increased cost of health care as determined by the Ministry of Health. 4.1.5.2.2. Expenditure Financing The mobilization of resources to finance this plan may be assured through a donor conference to be organized by the Ministry of Health to set an amount of about USD 5,000, or through other alternatives with the usual partners of Sao Tome and Principe, in order to quickly address the issue, given the urgency of the situation. Therefore, the Democratic Republic of Sao Tome and Principe is committed, through the Ministry of Health, to make the necessary efforts to implement that plan in order to change the existing environmental settings.

33
4.2. Training 4.2.1.Strategy of implementation of formal training In general, the personnel involved in the collection of biomedical waste have not received any training on waste management. Apart from some concepts treated in the academic training for doctors and nurses, especially on hospital hygiene, no specific training is provided on biomedical waste management to staff of health facilities. The same is true for the Chambers. The maintenance made in the House of Guadalupe and Angolares showed a deficit in this area: the municipal officers have no knowledge of the biomedical waste. The assessment of training modules taught in the School of Health revealed the lack of a specific course on the management of biomedical waste. Only a few elements are contained in the course of environmental sanitation. The modules to be introduced will be the entire chain of management (screening, pre-collection, storage, collection, transport, treatment, disposal), and good practices, and will address particularly the development of management plans to be carried out in each structure, but also the risks to health and the environment. The target audience for training is:
- The administrative staff responsible for such enforcement (officers, hospital directors, heads of clinical trials),
- Doctors, nurses and midwives and laboratory technicians, auxiliary medical personnel (maids, stretcher-bearers);
- Agents assigned to biomedical waste management in the context of the management plan,
- The municipal staff assigned to this group (technical surface, managers dumps), - The entities involved in the awareness program (NGOs, CBOs) instructors, teachers of
high school. 4.2.2. Training Strategy and Needs 4.2.2.1. Training Strategy
The training will take place at several levels:
- A consultant /trainer will be recruited to train a core group of trainers in the Institute of Health Sciences. The beneficiaries of the training will be: 1 trainer, the 7 delegates of Health, 1 public health physician for intervention in public health and 1sanitation officer;
- These 10 graduates will provide cascade training for the health personnel in the public and private sectors as well as community workers, at the Institute of Health Sciences

34
The one-week sessions will take place, at the first level, for the staff of the Hospital and health centers in each district involving 30 people. In the districts, the training will also involve the District Boards and the private sector, as well as NGOs and CBOs. At another level, the health delegates will meet for a week, and will provide training to staff of community health centers, which is the third level. The training shall take place once a year per district for 30 people. For the new students of the Institute of Health Sciences a special module will be introduced after consultation between the Ministry of Education and the Ministry of Health, The agents responsible for the operation and maintenance of plant equipment will receive appropriate training before starting to operate the equipment. For Monfort incinerators of pits for placentas, and incineration holes, manufacturers will go to aspecial session to become aware of the details of construction through the members of the structure responsible for infrastructure, equipment and materials of the Ministry of Health 4.2.2.2. Needs The total number of staff was estimated according to the size of the infrastructure and the involvement of district and private actors.
Table nº 11: Number of People to be trained in the Sanitary Structures
Structures Number of People per Structure
Number of Structure Total
Central Hospital 300 1 300 Health Centers 30 7 210 Health Posts 15 22 330
Community Health Posts 15 21 315 Total 1.155
NB*: The representatives of the districts, NGOs and CBO are among the people to be trained. A lump sum around $10,000.00 will be allocated for the special training of the companies selected for the construction of incinerators MONFORT for pit and holes and incineration holes by an expert from WHO. 4.3. Awareness 4.3.1. Awareness Strategy The objectives of raising awareness among decision-makers, health personnel, garbage workers, and the general population are mainly to:
- Avoid intentional or accidental exposure to waste, in particular biomedical waste and sharp or pointed materials;
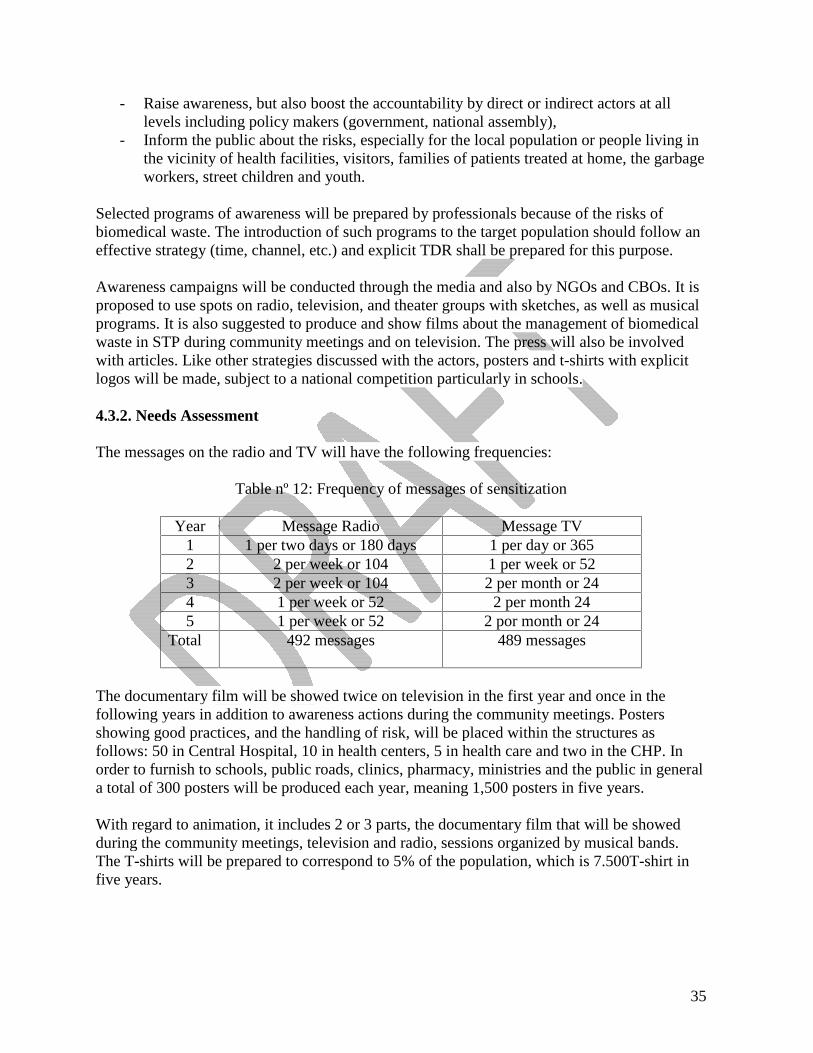
35
- Raise awareness, but also boost the accountability by direct or indirect actors at all levels including policy makers (government, national assembly),
- Inform the public about the risks, especially for the local population or people living in the vicinity of health facilities, visitors, families of patients treated at home, the garbage workers, street children and youth.
Selected programs of awareness will be prepared by professionals because of the risks of biomedical waste. The introduction of such programs to the target population should follow an effective strategy (time, channel, etc.) and explicit TDR shall be prepared for this purpose. Awareness campaigns will be conducted through the media and also by NGOs and CBOs. It is proposed to use spots on radio, television, and theater groups with sketches, as well as musical programs. It is also suggested to produce and show films about the management of biomedical waste in STP during community meetings and on television. The press will also be involved with articles. Like other strategies discussed with the actors, posters and t-shirts with explicit logos will be made, subject to a national competition particularly in schools. 4.3.2. Needs Assessment The messages on the radio and TV will have the following frequencies:
Table nº 12: Frequency of messages of sensitization
Year Message Radio Message TV
1 1 per two days or 180 days 1 per day or 365 2 2 per week or 104 1 per week or 52 3 2 per week or 104 2 per month or 24 4 1 per week or 52 2 per month 24 5 1 per week or 52 2 por month or 24
Total
492 messages 489 messages
The documentary film will be showed twice on television in the first year and once in the following years in addition to awareness actions during the community meetings. Posters showing good practices, and the handling of risk, will be placed within the structures as follows: 50 in Central Hospital, 10 in health centers, 5 in health care and two in the CHP. In order to furnish to schools, public roads, clinics, pharmacy, ministries and the public in general a total of 300 posters will be produced each year, meaning 1,500 posters in five years. With regard to animation, it includes 2 or 3 parts, the documentary film that will be showed during the community meetings, television and radio, sessions organized by musical bands. The T-shirts will be prepared to correspond to 5% of the population, which is 7.500T-shirt in five years.
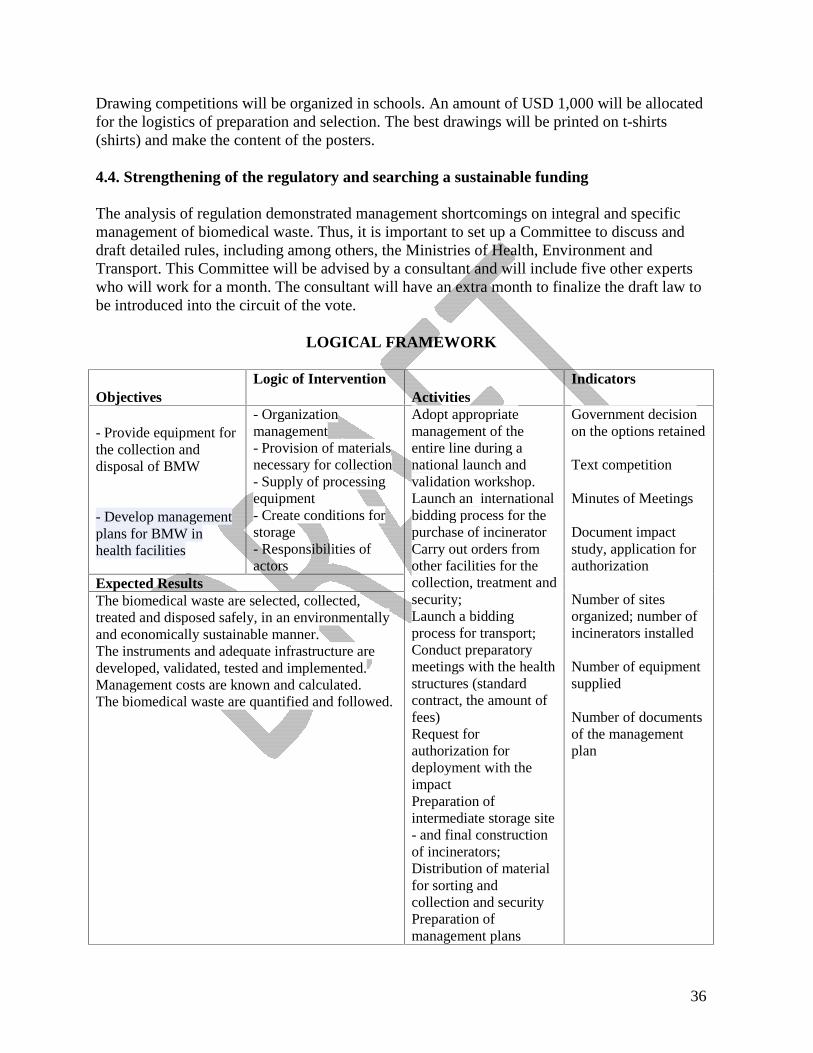
36
Drawing competitions will be organized in schools. An amount of USD 1,000 will be allocated for the logistics of preparation and selection. The best drawings will be printed on t-shirts (shirts) and make the content of the posters. 4.4. Strengthening of the regulatory and searching a sustainable funding The analysis of regulation demonstrated management shortcomings on integral and specific management of biomedical waste. Thus, it is important to set up a Committee to discuss and draft detailed rules, including among others, the Ministries of Health, Environment and Transport. This Committee will be advised by a consultant and will include five other experts who will work for a month. The consultant will have an extra month to finalize the draft law to be introduced into the circuit of the vote.
LOGICAL FRAMEWORK
Objectives Logic of Intervention
Activities Indicators
- Provide equipment for the collection and disposal of BMW
- Develop management plans for BMW in health facilities
- Organization management - Provision of materials necessary for collection- Supply of processing equipment - Create conditions for storage - Responsibilities of actors
Expected Results The biomedical waste are selected, collected, treated and disposed safely, in an environmentally and economically sustainable manner. The instruments and adequate infrastructure are developed, validated, tested and implemented. Management costs are known and calculated. The biomedical waste are quantified and followed.
Adopt appropriate management of the entire line during a national launch and validation workshop. Launch an international bidding process for the purchase of incinerator Carry out orders from other facilities for the collection, treatment and security; Launch a bidding process for transport; Conduct preparatory meetings with the health structures (standard contract, the amount of fees) Request for authorization for deployment with the impact Preparation of intermediate storage site - and final construction of incinerators; Distribution of material for sorting and collection and security Preparation of management plans
Government decision on the options retained
Text competition Minutes of Meetings Document impact study, application for authorization Number of sites organized; number of incinerators installed Number of equipment supplied Number of documents of the management plan

37
Objectives Logic of Intervention Activities
Indicators
Development of knowledge of direct and indirect actors Awareness of the actors on the dangers of poor management of biomedical waste and the risk of certain attitudes and practices.
Awareness, information Awareness, inform policy makers and the general population, indirect actors.
Expected Results
All exposed persons are informed and aware of the trauma and health risks related to biomedical waste
Organize a drawing competition Disseminate messages on the radio Write newspaper articles Spending on TV spots, Show the movie on TV, Show the theater on TV Organize community meetings to raise awareness (opera-shows) Produce posters Produce T-shirts
Documents the process, depicts No messages Extracts from newspapers No. spots CD Movies Audio CD Number of meetings Show organized No posters Number of T-shirts distributed
Objectives Logic of Intervention Activities Indicators
Improve the attitudes of actors Change in practice Improve knowledge on BMW
Streamline the current practices
Resultados Esperados
Health staff and staff of the district municipalities, CBO and NGOs know the different aspects of management of biomedical waste, sound practices and safe attitudes; selection, collection and elimination are organized.
Train the trainers Train the staff of CS and other Train the staff of HP and CHP Train health staff Form handlers of incinerators Train staff of the Boards.
Nº and % of staff trained
Logic of Intervention Logic of Intervention Activities Indicators
Provide STP with specific regulations on biomedical waste Set out of a framework for implementation and consultation
Development of coherent national policy.
Set up a team of implementation; Organization of a national ceremony; Creation of a working basis for the drafting of the law.
Certificate of constitution Minutes of the launch workshop of constitution The law is published in the national newspaper
Expected Results
A law on the management of biomedical waste is approved and published. The project activities are tracked, evaluated, funded and disseminated.
Drafting of the law Vote of the law
Objectives Logic of Intervention Activities Indicators

38
Organize actual actors in a more functional way
Set out an effective system of elimination and transport
Expected Results
The BMW of all health facilities are selected, evacuated and treated in an environmentally sound way.
Identification of all private health facilities; Setting the forms of organization; Discussion of terms of partnership with all stakeholders; Purchase of rolling means; Construction of safety boxes; Purchase of an incinerator and construction of other equipment.
List of geographical location of private health facilities. Document the plan. Contracts signed. Invoices and number of tricycles on the ground. No. boxes functional and the number of incinerators and others.
5. Implementation and Timeframe 5.1. Detailed activities of the Action Plan The implementation of the Action Plan comprises three phases: the preparation phase, the implementation phase with periodic monitoring, and the final evaluation. 5.1.1. Preparatory Activities The Preparation Workshop By grouping together the main actors of biomedical waste management, this workshop will share experiences on issues of biomedical waste in Sao Tome and Principe and the details of the proposed Action Plan in order to obtain a consensus on strategies. It will be a first opportunity to make contact with a view to establishing a partnership between the actors. The Conference of Donors The aim is to group the main funding bodies present in STP and invite other organizations interested in the subject to the detailed presentation of the action plan to enable its co-financing with the government of Sao Tome, where each agency can engage in a priority area in the project. Selection of Documents These are the following documents: the TOR for the consultant regarding training, awareness and launch of a particular application, the various proposals for the purchase of equipment and materials for the realization of infrastructure such as Montfort type incinerators and local storage.
39
Consultation Meetings and Current Status In order to get an understanding of the contracts, the amounts of fees per structure, the transport and disposal of biomedical waste, etc. workshops will be organized at the level of the sanitation structure and the patrimonial company. Initial Assessment This study is needed to appraise the feasibility of some arrangements, and the location of these impact studies. This should be done by a local multidisciplinary team. The Implementation Committee An implementation committee or an inter-sectoral committee will be set out. The team will comprise people with a mix of useful skills to accomplish its mission. This committee is appointed by a ministerial decree, and will liaise with the Directorate of Planning of the Ministry of Health and the SSSP. It could serve as a facilitator in consultation meetings between the public and the private sector and in the process of the setting up of the company of assets with the Ministry of Planning and Finance. Preparatory activities shall take place in a period of 6 months, while the evaluation of start-up will last two months. 5.1.2. Implementation This phase, which will last four and a half years, refers specifically to the procurement, supply and distribution of materials and equipment, installation of incinerators in Sao Tome, the construction of Montfort type incinerators, the pits for placenta and incineration holes, training and awareness. For these two points, there will be a training model for a year, while the training will be implemented for the last three years and awareness campaigns will go over the five years of the implementation of the Action Plan. This phase will be devoted also to the creation of a working framework for the drafting of the law and to facilitate its approval and adoption. At the end of the second year of implementation, the text of the law should be available and applied. 5.1.3. Monitoring and Evaluation 5.1.3.1. Monitoring of the Implementation of the Plan The monitoring is based on the collection and analysis of data to see if the project proceeds as planned and to make immediate adjustments if necessary. It is therefore an activity that will consist of regular discussions with health facilities on the basis of the Action Plan. 5.1.3.2. Evaluation of the Planning System Two evaluations will be made: an internal mid-term evaluation and an external evaluation during the month following the end of the project.

40
Internal Assessment This assessment is made by the Directorate of Planning of the Ministry of Health. The aim is to determine the existence and effectiveness of structures and systems necessary to ensure the proper implementation of the Action Plan and to maintain the relationship between the objectives and mechanisms/methods of the Action Plan. The financial partners, the project beneficiaries and other partners will fully participate in this one-month evaluation, which will require the completion of visits to all districts. External Evaluation External evaluation is to measure the effectiveness of the project and its performance and identify lessons learned. This evaluation will focus primarily on the aims, objectives and purpose of the action plan as represented in the logical framework. The mission of the external evaluation will be done at the end of the project by one external consultant and will last one month. 5.2. The actors and functions The implementation of the action plan will require the involvement of various stakeholders:
- The Ministry of the Environment in collaboration with the Ministry of Health should set all laws and regulations concerning the environment and health,
- The Ministry of Health will be the pillar of the national policy in all aspects of public health,
- The Ministry of Transport, regarding the transport of hazardous materials; - The Local Government; - Local, private companies of STP, which can invest in the context of arrangements set
out in Plan; - The health structures both public and private, which are the main producers and agents
involved in internal management. - The NGOs working in the fight against AIDS and malaria, which may invest
enormously in awareness; - The press to convey information regarding the management of biomedical wastes and
risks experienced by health workers and the public; - Multilateral and bilateral cooperation agencies, which may wish to finance activities
(Portugal, Taiwan, UNICEF, UNDP, WHO, etc.). - The Implementation Committee (COM) for the implementation of some activities and
the monitoring of implementation by other actors.
4.3. Partnership Framework for Implementtion
Activities
Implementation
Monitoring
Supervisão Training

41
TDR and selection of trainer Preparation of targeted modules Cascade training Training in operation and maintenance of equipment Continuing education
COM International ConsultantInternational ConsultantNational TrainersConstructor WHO
General Direction of Forestry (DF) and Ministry of Health
Direction of Planning Direction of Planning Health Structure
Ministry of health SSSP
Awareness TDR program Drawing competition for posters Confection of posters Distribution / dissemination Awareness
CNES CNES CNES CNES COM Professionals CBO, NGO
DF and Ministry of Health
Strengthen the regulation National Consultant (lawyer) leads a working group
DPS/General Direction of Environment (Legal Service)
Distribution of equipment
DPS COM
Initial study Local team/COM Organization of infrastructure
Health Strcuture DPS
Donors Conference Ministry of Health Monitoring COM DP Specific assessment of training
International Consultant
Implementation Committee DFS
Internal evaluation External evaluation
Local team International consultant
Timetable ACTIVITY Year 1 Year 2 Year 3 Year 4 Year 5
PREPARATORY ACTIVITIES Launching workshop
Initial Assessment
Set up an implementation committee, patrimonial company Conference of donors
Elaboration of bidding documents
Meetings for concertations
Implementation

42
Distribution of material of selection and collection and security
Organization of local of intermediate and final storage and installation and construction of incinerators
Training of trainers Training in “cascada” Continous training Develop the Management Plan Organize the drawing competition Show the film in the sanitary structures Disseminate messages in the radio Show spots and films at TV Show theatre at the TV Community meetings Prepare posters Make and distribute T-shirts
Set up a legal working group Develop the draft law
Monitoring of Implementation
Training Evaluation Mid-Term Evaluation Final evaluation

43
6. Budget
The budget was calculated according to the needs assessment for each component of the Management Plan: management, treatment, training,sensitization.
Designation Unities Quantity Unit Price $ Amount $ Amount DobrasEQUIPMENTS OF SANITARY STRUCTURES
Boxes U 1.807 15 27.105 426.497.175Hand Cars U 28 56 1.568 24.672.480Small cars U 4 420 1.680 26.434.800Needledestroyer U 41 500 20.500 322.567.500Needle receiver Lot 370 20 7.400 116.439.000Protectiveequipment Lot 359 50 17.950 282.443.250Preparation of sites for deposit m2 98 120 11.760 185.043.600Preparation of sites for treatment U 6 300 1.800 28.323.000Incineratorssmall models U 1 35.000 35.000 550.725.000ncineratorsMontfort U 6 3.000 18.000 283.230.000Expotation toolsandincinerators
Lot 6 50 300 4.720.500
Tanks forplacentas U 6 1.000 6.000 94.410.000Hole for inicneration U 40 50 2.000 31.470.000Sub-total 151.063 2.376.976.305
EQUIPMENT OF TRANSPORT OF BIOMEDICAL WASTETricycles U 12 3.000 36.000 566.460.000Small vehicles U 2 90.000 180.000 2.832.300.000Sub-total 216.000 3.398.760.000
SENSITIZATIONSpot TV U 489 17 8.313 130.805.055Spot radio U 492 28 13.776 216.765.360Posters U 1.500 1 1.500 23.602.500Sketches U 3 165 495 7.788.825T-Shirts U 7.500 1 7.500 118.012.500Drawing competition FF 1 1.000 1.000 15.735.000Film documentary FF 1 1.000 10.000 15.7350.000Sub-total 44.584 701.529.240
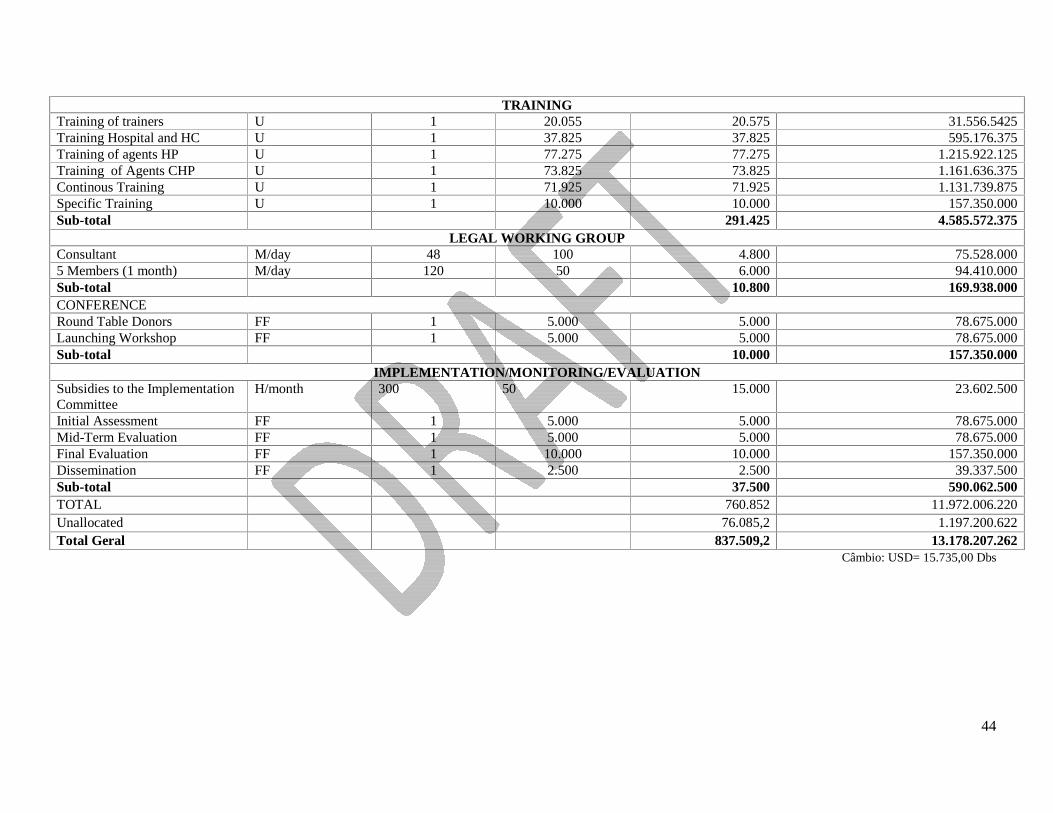
44
TRAININGTraining of trainers U 1 20.055 20.575 31.556.5425Training Hospital and HC U 1 37.825 37.825 595.176.375Training of agentsHP U 1 77.275 77.275 1.215.922.125Training of AgentsCHP U 1 73.825 73.825 1.161.636.375ContinousTraining U 1 71.925 71.925 1.131.739.875Specific Training U 1 10.000 10.000 157.350.000Sub-total 291.425 4.585.572.375
LEGAL WORKING GROUPConsultant M/day 48 100 4.800 75.528.0005 Members (1 month) M/day 120 50 6.000 94.410.000Sub-total 10.800 169.938.000CONFERENCERound TableDonors FF 1 5.000 5.000 78.675.000Launching Workshop FF 1 5.000 5.000 78.675.000Sub-total 10.000 157.350.000
IMPLEMENTATION/MONITORING/EVALUATIONSubsidies to the ImplementationCommittee
H/month 300 50 15.000 23.602.500
Initial Assessment FF 1 5.000 5.000 78.675.000Mid-Term Evaluation FF 1 5.000 5.000 78.675.000Final Evaluation FF 1 10.000 10.000 157.350.000Dissemination FF 1 2.500 2.500 39.337.500Sub-total 37.500 590.062.500TOTAL 760.852 11.972.006.220Unallocated 76.085,2 1.197.200.622Total Geral 837.509,2 13.178.207.262
Câmbio: USD= 15.735,00 Dbs

45
ANNEXES
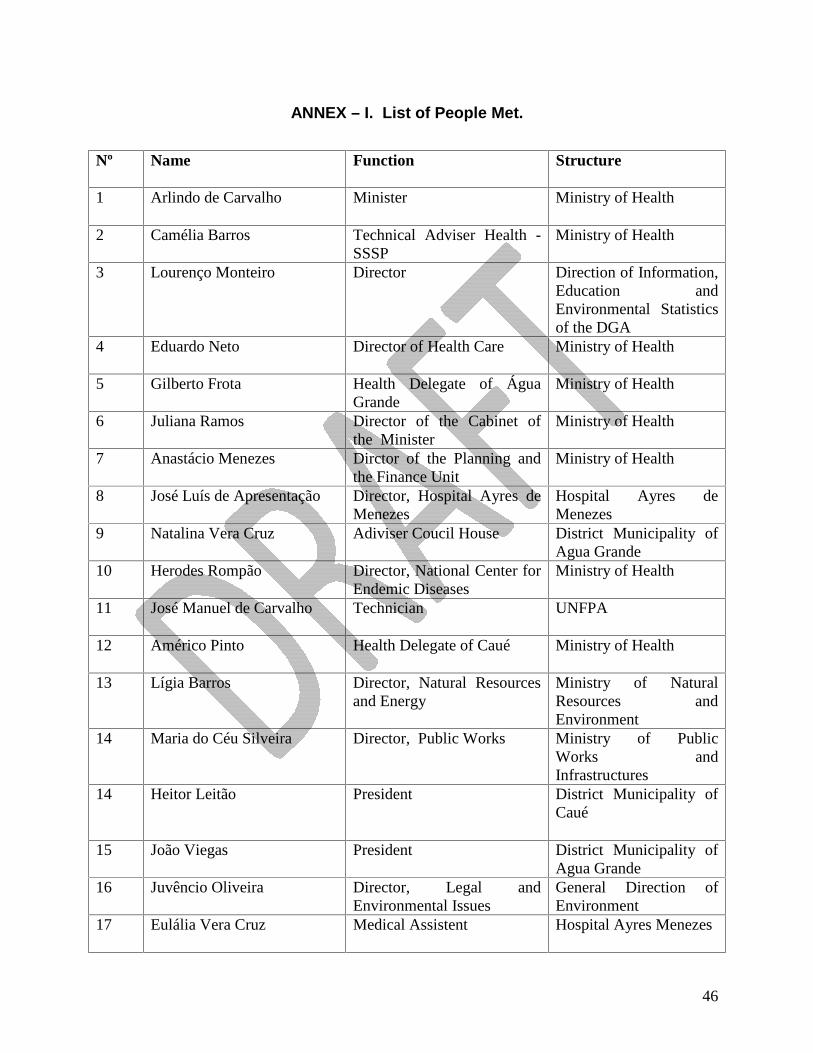
46
ANNEX – I. List of People Met.
Nº Name Function Structure
1 Arlindo de Carvalho Minister Ministry of Health
2 Camélia Barros Technical Adviser Health -
SSSP Ministry of Health
3 Lourenço Monteiro Director Direction of Information, Education and Environmental Statistics of the DGA
4 Eduardo Neto Director of Health Care Ministry of Health
5 Gilberto Frota Health Delegate of Água Grande
Ministry of Health
6 Juliana Ramos Director of the Cabinet of the Minister
Ministry of Health
7 Anastácio Menezes Dirctor of the Planning and the Finance Unit
Ministry of Health
8 José Luís de Apresentação Director, Hospital Ayres de Menezes
Hospital Ayres de Menezes
9 Natalina Vera Cruz Adiviser Coucil House District Municipality of Agua Grande
10 Herodes Rompão Director, National Center for Endemic Diseases
Ministry of Health
11 José Manuel de Carvalho Technician UNFPA
12 Américo Pinto Health Delegate of Caué Ministry of Health
13 Lígia Barros Director, Natural Resources and Energy
Ministry of Natural Resources and Environment
14 Maria do Céu Silveira Director, Public Works Ministry of Public Works and Infrastructures
14 Heitor Leitão President District Municipality of Caué
15 João Viegas President District Municipality of Agua Grande
16 Juvêncio Oliveira Director, Legal and Environmental Issues
General Direction of Environment
17 Eulália Vera Cruz Medical Assistent Hospital Ayres Menezes

47
ANNEX II – Bibliography
1. Plano de Gestão dos Resíduos Biomédicos da Guiné Bissau - Mbaye Mbengue FAYE –
Consultor, Dakar – Senegal, Março, 2003;
2. Plano de Gestão dos Resíduos Biomédicos de São Tomé e Príncipe – Djibril Doucouré, Rapport Préliminaire (2003);
3. Manejo de resíduos peligrosos/biomédicos en los laboratorios de diagnóstico universitários - Bogotá; Universidad Colegio Mayor de Cundinamarca; 1999?. [19];
4. Relatório de Actividades de 2002 e 2003, Hospital Dr. Aires Menezes;
5. Ministério da Saúde, Escola de Formação de Quadros da Saúde, Levantamento das formações efectuadas nos anos 1979-1989 e 1992-2000;
6. Plano de Manejo e de Gestão dos Parques Naturais Obô de São Tomé e Príncipe – Dário Cesarini, Carlos Albuquerque – 2008.
7. Relatório Nacional do estado Geral da Biodiversidade de São Tomé e Príncipe, Hamilton Vaz, Faustino Oliveira – Maio de 2007
8. Inventário sobre Gases com Efeito de Estufa – 2005;
9. Resíduos Biomédicos - Gestão Global de Resíduos Mário Esteves, Lisboa. Março de 2007.
10. Plano Nacional do Ambiente para o Desenvolvimento Durável – PNADD - 1999;
11. Estratégia Nacional da Biodiversidade – ENPAB STP - 2005