dementia essentials
TRANSCRIPT

Participant manual
2.1 The impact of dementiaThis module considers the impact of dementia and how these changes impact the person living with dementia, their family carers and support professionals.
Learning outcomes• Identify the impact of dementia on all in the support relationship• Identify stress for all in the support relationship• Develop self-care strategies to manage work-related stress
2.2 Person-centred practiceThis module explores the principles of person-centred support.
Learning outcomes• Recognise person-centred care contributes to a person-centred
approach to support• Identify and address the need for a stable, familiar, nurturing
environment of care which maximises the person’s abilities• Identify the need for balance between safety and comfort and
the person’s right to autonomy
Dementia EssentialsCHCAGE005 Provide support to people living with dementia
Module 2

© 2020 Dementia Australia

IntroductionThis is a Dementia Training Australia (DTA) course, funded by the Australian Government and delivered by Dementia Australia.
DTA is a consortium led by the University of Wollongong and consisting of Dementia Australia, La Trobe University, Queensland University of Technology, and the University of Western Australia.
DTA is delivering a coordinated national approach to dementia training for individuals and organisations, with the ultimate goal of improving the care and wellbeing of people with dementia by upskilling the workforce.
For more information about DTA please visit dta.com.au
This course has been designed to provide the essential background knowledge needed to work more effectively as a support provider for people with dementia. It is an accredited course intended for delivery to staff in the aged care industry, rather than family carers. The underlying approach is from the perspective of someone employed to provide support in a professional setting. Examples and case studies used throughout reflect this focus.
Dementia Essentials delivers the national unit of competency, CHCAGE005 Provide support to people living with dementia, which is a core unit in CHC43015 Certificate IV Ageing Support.
AcknowledgementsDementia Training Australia is supported by funding from the Australian Government under the Dementia and Aged Care Services Fund.
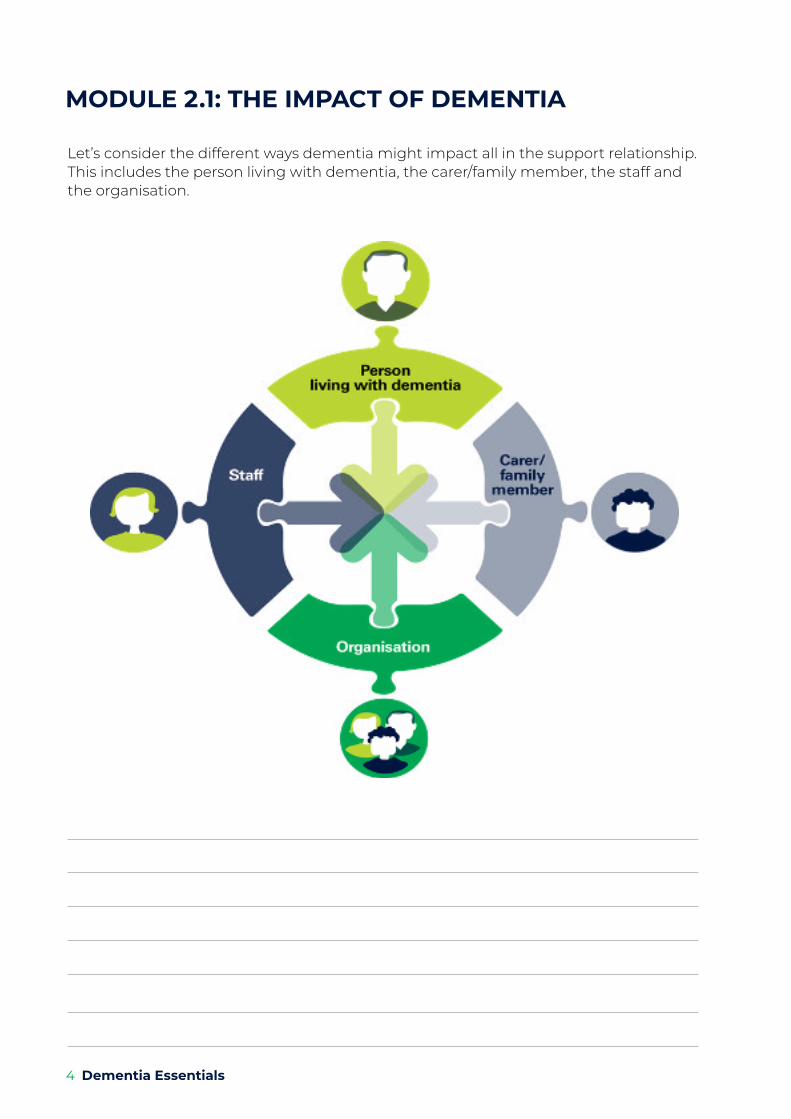
MODULE 2.1: THE IMPACT OF DEMENTIA
Let’s consider the different ways dementia might impact all in the support relationship. This includes the person living with dementia, the carer/family member, the staff and the organisation.
4 Dementia Essentials
Think about the impact of dementia for everyone in the support relationship. Write one impact for each.
Impact on a person with dementia
Impact on a support person
Impact on staff
Impact on the organisation
The most common factor shared by all in the support relationship is:
Module 2.1 & 2.2 5
KEY MESSAGESImpact of dementia on the person The impact of dementia will be different for each person. If the person is not well supported, the impact on their quality of life can be profound.
• Loss of independence – As dementia progresses, a person’s ability to think, reason, and carry out daily tasks will diminish. They will need increasing support to carry out these activities.
• Impaired communication – Over time, the person with dementia will find it more and more difficult to express themselves and be understood by others. Losing the ability to communicate can be one of the most frustrating and difficult problems for people living with dementia, their families and carers.
• Loss of self-esteem – Past social roles often reflect a person’s self-identity. When these life roles fade, and the person’s reality no longer reflects what ‘used to be’, the person with dementia can become confused, distressed and lose self-esteem as their sense of ‘self ’ is lost.
• Depression – It is estimated that 20–30% of individuals with dementia may also have depression at any given time1. People in long-term residential care appear to be particularly at risk of depression. Dementia can contribute to depression through the slow erosion of confidence and self-esteem as a person’s ability to manage their physical and social environment is affected.
• Increased stress – Every person has a certain level of stress they are able to handle. Beyond this, they start to feel overwhelmed. For a person with dementia, it is no different. They already find everyday tasks challenging. When other stressors such as pain or a change in routine or environment add to existing stress levels, it may be too much to cope with.
Impact of dementia on families/carers Dementia impacts on relationships in a number of ways and is different for everyone. Factors such as symptoms, progression, individual personalities, past experiences and coping abilities all play a part in the dementia journey. As the condition progresses, relationship dynamics constantly shift2.
• Roles and identity – Dementia can impact on the roles people hold and consequently their sense of identity within their relationship2. Carers may gradually have to take on more responsibility for care and decision-making, which can sometimes feel overwhelming or exhausting.
• Emotional disconnect – Some family members/carers find it difficult to stay connected with the person as dementia progresses2. As communication difficulties and memory loss get worse over time, it can become harder and harder to remember the person for who they were.
• Anger – Anger is a normal response. Family members/carers may feel angry at having to be a carer. They may be angry with others who do not seem to be helping out or perhaps at the person with dementia for their changed behaviour.
6 Dementia Essentials

KEY MESSAGESSeveral models support person-centred practice. Valuing People is a person-centred framework that builds on the work of Tom Kitwood.
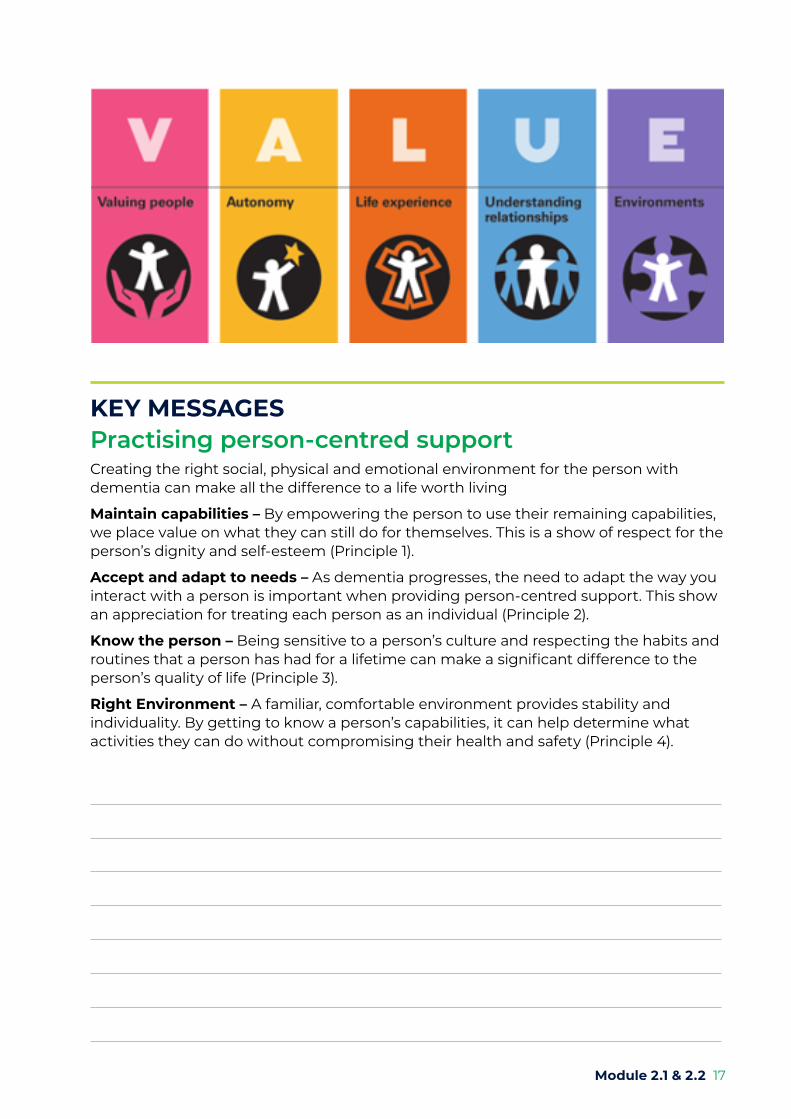
The VALUE acronym represents the underpinning elements that guide person-centred support strategies for people living with dementia and includes:
• Valuing people
• Autonomy
• Life experience
• Understanding relationships
• Environment
Valuing the person living with dementia includes:
• showing that you value the persons opinion
• the values and beliefs of the person are listened to, respected and are incorporated in planning and delivery of support
• Showing interest in the person through listening to their story and experience and responding in a positive manner
Autonomy involves:
• giving people choices
• respecting the choices, they make
• Grief and loss – Grief is an emotional response to loss. People caring for partners may experience grief at the loss of the future that they had planned to share together. Some may be faced with the loss of the person they used to know and the loss of a relationship that was previously shared3.
• Guilt – It is quite common to feel guilty for the way the person with dementia was treated in the past or for other reasons. If the person with dementia goes into hospital or residential care, there may be guilt for not keeping them at home for longer3.
Module 2.1 & 2.2 7

• recognising when the person requires support in the decision-making process
• ensuring the person is central to the decision making
• balancing risk with the person’s rights and responsibilities
Life experience is the connection between the person’s past, their present-day experience, and their hopes for the future. This experience guides our approach to planning and delivering support.
Get to know the person by:
• reading about their life history and knowing their story e.g. places born/lived; era born/younger years; language(s)spoken; culture; beliefs, values; education; occupation(s); hobbies/interests; volunteering; marital status; family make-up/dynamics; likes/dislikes; pets; music; books; personality; great events/trauma;
• understanding cultural and religious influences and knowing the significant events
• a person’s life experience which is used to support engagement and a sense of purpose
Understanding relationships
Supporting relationships for the person living with dementia include:
• the importance of the meaning of home is understood by staff and incorporated into support planning
• staff are aware of how their approach can impact upon the person living with dementia
• care plans support a rich and active community life based on the individual’s gifts and interests
Environment
Environments are the settings where people live and work as well as the built environment.
A person-centred environment is appreciative and responsive to the culture, meanings and connections of the people within them.
• Ensure the environment is enabling and supports independence
• consumers experience staff behaviour that is consistent with the organisational values
• people living with dementia and those who care for them are seen as experts in what is important to them
8 Dementia Essentials

Consumer story IMPACT ON YOUNGER PERSON WITH DEMENTIA
Mum was diagnosed with Alzheimer’s diseaseHollyMy mum has been diagnosed with Alzheimer’s disease and she had to quit her job. She also doesn’t drive anymore which she hates. At first we noticed that she was being a bit forgetful all the time and she would get words wrong when she was speaking. Dad tried to get her to go to the doctors for about a year but she didn’t go because she thought nothing was wrong. I think maybe she was a bit scared of finding out coz she cries a lot. My little brother doesn’t understand much, but I have spoken with dad about it more and I know it’s going to get worse. That’s hard but it makes me want to do as much with her as I can. I spend time with her and although she sometimes says the same thing I just know she doesn’t remember so there’s no point in yelling at her. I’m worried about what will happen so I spend as much time with her as I can now.
Dad moved into a nursing homeDanielMy dad moved into a nursing home earlier this year. Even though he is only 45, he has to stay at a home for older people because he has dementia and there’s nowhere else he can go. It’s really hard seeing him there, but I still visit lots with my mum and sisters. He had been in hospital for ages before that because things were really hard and we couldn’t look after him at home anymore. The hardest thing is when we leave to go home and he doesn’t understand why he can’t come too. I hate that. The nurses will always distract him so that he doesn’t notice as much and we leave quickly.
My dad has dementia ZoeMy dad got diagnosed with dementia in the front of his brain when I was 13. I’m now 15 and it’s been hard because his dementia has made him act different. It’s a bit like he’s a different person to who he used to be. But deep down I know he’s still my dad and I will love him. He doesn’t mean to do the things he does, he can’t help it. I have to remind myself of that so that I don’t get angry at him.
Module 2.1 & 2.2 9

KEY MESSAGESThe impact of stress The fight or flight response
The body responds to threats by producing chemicals that bring about the physical symptoms, e.g. increased heart rate, perspiration etc. This response prepares our body for either a defensive reaction (fight) or immediate retreat (flight).
In modern society, such threats are more subtle as we are no longer hunted by wildlife predators – but, our body systems still respond in the same way.
Taking physical action helps to remove these chemicals from our bodies; however, this is not how we respond to most present-day “stressors”, therefore, the chemicals build-up and consequently, we experience a state of “stress”.
The impact of stress on the person living with dementiaIn a person living with dementia stress may:
• present as changed behaviour, e.g. calling out, repetitive actions, anxiety, aggression
• present as lowered mood, reduced socialisation and engagement
• impact on a person’s ability to function and consequently, their health and well-being.
The impact of stress on family/carersSigns that a family member or carer may be stressed include:
• Depression
• Reduced sleep
• Irritability
• Tearfulness
• Sickness
• Reduced ability to care
• Complaints
10 Dementia Essentials

KEY MESSAGESThe impact of stress on staffStress affects staff in many ways (5) including:
• affecting the way we think – forgetfulness, indecisiveness, apathy, hopelessness, poor concentration (making daily tasks more difficult to manage)
• impact on eating and sleeping patterns
• emotionally – anxiety, depression, tension, anger
• behaviourally – increased drinking and smoking, insomnia, accident proneness, weight problems, obsessive-compulsive behaviour, nervousness, gambling
The impact of stress on the organisationAt an organisational level, signs of stress can be seen in:
• Increased sick leave
• Increased staff turn over
• Poorer work output
• Increased incident reports
• Disharmony amongst workers
• Staff burnout
• Gaps in service provision
• Lack of/poor quality policies and procedures
• Family complaints
• Increased costs
Module 2.1 & 2.2 11

KEY MESSAGESReducing stressEveryone has different ways to manage stress. Managing stress improves well-being and may positively impact on the caring role, so it can be useful to learn better ways to deal with it.
For the person with dementia:
• To reduce stress, consider:
• Person-centred support approaches
• Engaging them in tasks and activities that provide a sense of purpose and belonging
• Early intervention – pre-empt the person’s needs
• Independence and choice is respected
• Supportive/enabling environment
• Counselling support
For family/carers
To reduce stress, consider:
• HomeCare Packages
• Carers education and support groups
• Discussing concerns with a general practitioner
• Multicultural services, e.g. community groups
• Religious/spiritual services, e.g. local church groups
• Short term respite opportunities including planned activity groups or day centre programs
• Options for permanent residential care
• Counselling
• Dementia Behaviour Management Advisory Service (DBMAS)
For staff
To reduce stress, consider:
• Acknowledging feelings of stress – this is a good first step
• Discuss concerns with the supervisor or team leader
• Actively seek further training and education to support improved practice
• Try to: – Understand what situation makes you feel stressed – Understand what situations you can and can’t control – What supports are available to help you manage the stress
• Keeping healthy, e.g. good nutrition, exercise and sleep
• Tapping into relaxation and mindfulness techniques
12 Dementia Essentials
• Avoiding increased alcohol/smoking/illicit drugs
• Seeking counselling support – e.g. to help with time management, to debrief or to help address personal issues that might impact on work
For the organisation
To reduce stress, consider:
• Referring to the Severe Behaviour Response Team (SBRT)
• DBMAS – it supports carers of people with dementia who experience changed behaviours, provides comprehensive assessment, evaluation and interventions
• Dementia Australia – provider free counselling to carers, education and training across the sector as well as onsite consultancy in the workplace
• Dementia Training Australia – offers a wide range of training courses for individuals and a number of organisational offerings including tailored training packages and its award-winning environmental design education services.
• Employee Assistance Programs (EAP) – these programs offer free counselling sessions to staff members
Module 2.1 & 2.2 13
KEY MESSAGESWhat are person-centred principles? Person-centred principles value and respect the person and treat each person as an individual. Knowing what is important to the person creates an environment that promotes inclusion, connection and purposeful activity.
A person-centred environment:
• Empowers the person to use their remaining capabilities
• Meets human emotional needs
• Includes familiar personal belongings
• Accepts changes and adapts accordingly
• Respects and balances comfort and safety with the person’s right to take a risk understanding behaviour.
What is person-centred support?Person-centred support is a holistic approach to dementia care developed by Professor Tom Kitwood, focusing on the individual and utilising aspects such as the person’s past history, routines, personal preferences and needs. The concept is based on meeting the needs of the whole person in order to create a feeling of well-being.
Traditionally, dementia was placed within the fields of medicine and psychiatry, which led to an over-emphasis on the ‘treatment’ of people with dementia. This model lacked the recognition of the person with the illness; who they are, their life before the illness and how they currently feel. The approach also overlooked the influence of the social and physical environments on a person with dementia.
Person-centred support, on the other hand, seeks to view the person with dementia as a whole and addresses the influence of factors beyond the physical changes in the brain.
Further reading: Kitwood’s Model of Person-centred Care is universally accepted as best practice in dementia support.
MODULE 2.2: PERSON-CENTRED PRACTICE
14 Dementia Essentials
KEY MESSAGESKitwood’s five aspects of emotional needIn 1997, Kitwood proposed a model of human emotional need made up of five interconnected areas, all of which are aspects of the desire to be loved. He proposes that this desire for love is central to being a person and our sense of well-being. In this respect, people with dementia are no different.
The five aspects are:
Comfort – Comfort is achieved through empathy and support received from another person. In dementia support, the need for comfort is likely to be strong as the person deals with grief and loss – e.g. a loss of abilities or a past way of life.
Attachment - Bonds between people are a primary and instinctive human need; this need may be greater in a person with dementia.
Inclusion – The need to belong to a group and to have social interaction with others is a strong human characteristic. Inclusion in a group for people with dementia is often difficult. Non-acceptance may cause a person to withdraw. Conversely, inclusion in a group can lead to greater interaction.
Occupation – To be involved in some form of activity in a way that draws on a person’s abilities and skills results in a meaningful outcome for the individual. Lack of activity or occupation potentially results in boredom, apathy and a sense of futility for people with dementia.
Identity – Identity is about knowing who we are and where we fit in the world. Person-centred support can help to preserve self-identity by knowing about the person’s past – their “narrative” or history – so that even if they lose parts of themselves through memory loss, other people still hold this knowledge.
Module 2.1 & 2.2 15
KEY MESSAGESPerson-centred care principlesA person-centred approach has become synonymous with good quality support and has grown to be internationally associated with successful health care outcomes.
Kitwood’s theory of person-centred care has evolved over time and is underpinned by four key principles which are:
Principle 1: Valuing and respecting the person
Principle 2: Treating each person as an individual
Principle 3: Knowing what is important for the person
Principle 4: Creating an environment that promotes:
• Freedom
• Inclusion
• Connection
• Purposeful activity
We often consider that we are providing person-centred care because the person is at the centre of our care, that is, we do things FOR the person or TO the person when really it needs to be WITH the person.
This can only be done by each individual as they interact with the person with dementia. It does not require extra time, staff, money or changes to the organisation.
16 Dementia Essentials
KEY MESSAGESPractising person-centred supportCreating the right social, physical and emotional environment for the person with dementia can make all the difference to a life worth living
Maintain capabilities – By empowering the person to use their remaining capabilities, we place value on what they can still do for themselves. This is a show of respect for the person’s dignity and self-esteem (Principle 1).
Accept and adapt to needs – As dementia progresses, the need to adapt the way you interact with a person is important when providing person-centred support. This show an appreciation for treating each person as an individual (Principle 2).
Know the person – Being sensitive to a person’s culture and respecting the habits and routines that a person has had for a lifetime can make a significant difference to the person’s quality of life (Principle 3).
Right Environment – A familiar, comfortable environment provides stability and individuality. By getting to know a person’s capabilities, it can help determine what activities they can do without compromising their health and safety (Principle 4).
Module 2.1 & 2.2 17

KEY MESSAGESBefore you commence Module 3 – Communication, please complete the pre-class activities, including the assessment task using the Sunflower Communication tool.
PRE-CLASS ACTIVITIES
Activity Completed
Watch the video: Enhance your communication
Short reading: 20 things not to say or do to a person with dementia by Kate Swaffer 2014
Write your reflections on the discussion board in the Dementia Learning Platform
Collect an item: find an item of personal significance for reminiscence activity to share during virtual classroom
Portfolio of Evidence – Assessment One (1): Complete Sunflower Communication tool
Watch:
video Enhance your communication https://www.youtube.com/watch?v=AJVjVgBTACI
Read:
Kate Swaffer 2014, 20 things not to say or do to a person with dementia https://kateswaffer.files.wordpress.com/2014/06/20-things-not-to-say-or-do-to-a-person-with-dementia_kate-swaffer_-june2014.pdf
Write:
your response to the reflection question on the discussion board in Dementia Learning Platform.
Reflection question: After reading Kate Swaffer’s (2014) communication tips ’20 things not to say to a person living with dementia’, what is one communication improvement you will make to maximise engagement for a person with dementia?
18 Dementia Essentials
Collect an item:
People with dementia often feel more at home in the past, particularly as memory loss progresses and their understanding of the current environment diminishes. Reminiscence is one communication approach which involves using a person’s memories and recollections as a means to create rapport and reinforce the person’s identity.
Reminiscence involves the discussion of past activities, events and experiences with the person with dementia, sometimes with the aid of tangible prompts such as photographs, household or familiar items from the past, music or other sound recordings. Knowing something about the person’s past allows us to reminisce with the person while assisting with daily living activities and also may help with understanding behaviour.
Collect one (1) item of personal significance that is familiar and stimulates a positive memory for YOU. Bring this item to share during the Module 3.0 virtual classroom for a group reminiscence activity.
PORTFOLIO OF EVIDENCE – ASSESSMENT ONE (1)Complete the Sunflower Communication tool
Information gathered from the person with dementia or a carer, or family member provides expert knowledge of needs, wants preferences and life routines to provide person-centred care. The Sunflower can be used as a conversation starter and to assist with reorientation, validation and reminiscence.
Effective communication is an important factor in the provision of care. Effective communication is directly related to Aged Care Quality Standards: Standard 1 Consumer dignity and choice to ensure the person is treated with dignity and respect, maintain their independence, decision making and identity and to live the life they choose.
Assessment Instructions:1. In the workplace, consult a person with dementia and ask their verbal consent to
participate. Do not undertake this activity with a person who does not provide verbal consent. This can be completed with the person, or on your own with what you know about the person. Do not include any identifying information such as surname, date of birth or address.
2. Read the Guide to completion attached to the Sunflower template to become familiar with the information you would like to collect about the person.
3. Use verbal and non-verbal communication skills to maximise engagement.4. Ask the person living with dementia, the questions on the petals of the flower.5. Fill in their answers on the sunflower picture. The flower’s centre identifies the
person’s name or what they like to be called, and the petals collect important individualised information about that person.
Download the Sunflower template from: https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0008/285380/ACI-Agedcare-CHOPs-Sunflower.pdf
Submission Instructions: This activity will be explored further in the classroom. Please do not submit your assessment task before the Virtual Classroom Module 3 session.
Module 2.1 & 2.2 19

After the Virtual Classroom session, you must finalise this assessment task.
Please scan and upload the completed task onto the learning platform no later than seven days after the Module 6 Virtual Classroom session.
20 Dementia Essentials
FURTHER INFORMATIONSupport:Support services available to people with dementia and their carers include:
Commonwealth Home Support Programme (CHSP)
The CHSP is available to people:
• aged 65 years and over, or 50 and over for Aboriginal and Torres Strait Islander people
• in all states and territories – except Victoria and Western Australia where there are some differences (Please contact your respective State/Territory Government Department for more information)
• who are at risk of premature or inappropriate admission to long term residential care
• carers of older Australians eligible for services under the Commonwealth HACC Program
The services provided under the Commonwealth Home Support Program (CHSP) include:
• nursing care
• allied health services like podiatry, physiotherapy and speech pathology
• domestic assistance, including help with cleaning, washing and shopping
• personal care, such as help with bathing, dressing, grooming and eating
• social support
• home maintenance
• home modifications
• assistance with food preparation in the home
• delivery of meals
• transport
• assessment, client care coordination and case management
• counselling, information and advocacy services
• centre-based day care
• support for carers including respite services
• Multicultural services – community support and/day centres
• Carers’ associations – provides support for family members.
• General practitioners
• Residential care • Short term (respite) • Permanent care
To find out about services in your area, contact My Aged Care on 1800 200 422
Module 2.1 & 2.2 21
Accessing services
Referral for services for a person with dementia can be made via:
• MyAgedCare website myagedcare.gov.au
• Self-referral (client or family)
• Another care agency
• General practitioner
• Medical specialist
• Hospital social worker
• Aged Care Assessment Service (ACAS)
Dementia Australia services
Dementia Australia is the national peak body and charity providing representation and support for people living with dementia, their families and carers at a personal, community and advocacy level.
Services vary in each State and Territory however they may include respite and social support; counselling; accredited and non-accredited education and training across the sector; onsite consultancy at the workplace and research.
For more information in your locality, contact:
dementia.org.au
National Dementia Helpline 1800 100 500
Dementia Support Australia
For more information in your locality, contact: 1800 699 799

22 Dementia Essentials
GlossaryThe following resources were used in generating this glossary: At your fingertips - Dementia Alzheimer’s and other dementias, H. Cayton, Dr. N. Graham, Dr. J. Warner; The Australian Oxford Paperback Dictionary, F. Ludowyk, B. Moore
Acetylcholine
Agnosia
Apraxia
Aphasia
AIDS
Alzheimer’s disease
Amyloid
Anticholinesterase drugs
Antioxidants
Antipsychotic drugs
Aricept
Blood pressure
Brain scan
Bradykinesia
Cerebral cortex
Cholesterol
Cholinergic
Cholinesterase inhibitor
Chromosomes
One of a group of chemicals known as neurotransmitters. Found throughout the brain, acetylcholine enables nerve cells to communicate with each other. In Alzheimer’s disease, the levels of acetylcholine are lower than usual.
Inability to recognise familiar objects, people, sounds, shapes or smells.
Inability to make familiar movements despite having muscular strength and co-ordination.
Impaired ability to produce, comprehend or use language.
Abbreviation for Acquired Immune Deficiency Syndrome.
The commonest cause of dementia. It usually begins after the age of 65 and results in gradual, progressive loss of memory and other functions of the brain.
A protein that is found in the brains of people with Alzheimer’s disease. It is deposited throughout the brain in microscopic clumps known as plaques. Its function is unknown and it may be the cause of the deterioration of brain function.
Also known as cholinesterase inhibitors, these dementia drugs stop the breakdown of acetylcholine. Aricept and Exelon are examples.
Substances such as vitamin E, C and beta carotene are thought to protect the body cells from the damaging effects of oxidation.
A range of tranquillisers, also known as neuroleptic drugs, that help to reduce symptoms of aggression.
The brand name for donepezil, a cholinesterase inhibitor.
The amount of stress placed on the walls of the arteries, veins and heart chambers by the flow of blood.
A general term to mean any investigation that produces pictures of the brain. A CT scan or MRI scan shows slices through the brain. A SPECT scan shows the brain’s blood supply.
An abnormal condition that features slowness of speech and movements.
The outer layers of the brain, involved in thinking, memory and the interpretation of perception or the senses.
Substance found in animal fats and oils, and is also made in the body. It is necessary for the making of vitamin D in the skin and for making various hormones. Too much cholesterol can be responsible for deposits in blood vessels and eventual restriction of blood flow.
Referring to acetylcholine. For example, a cholinergic neurone is a brain cell that contains the chemical acetylcholine.
An alternative name for anti-cholinesterase drug.
Microscopic thread-like structures that are present in all cells. They are collections of genes, which contain the genetic information that is transmitted from generation to generation.

Module 2.1 & 2.2 23
CJD (Creutzfeldt Jakob disease)
Cognition
Cognitive tests
Community care
Complementary medicine
Confabulation
Confusion
Dehydration
Delirium
Dementia
Depression
Diabetes
Diagnosis
Disinhibition
Disorientation
Donepezil
Down syndrome
A very rare form of dementia caused by an infectious agent called a prion. As well as loss of memory, CJD commonly causes muscle jerking, blindness and problems with walking. Death occurs within a year or so.
The faculty of knowing or perceiving things.
Tests that assess how well a person can think and how well his or her memory is working.
A term covering health and social care services delivered to people in the community, usually in their own home.
An approach to health care that explores alternatives to conventional treatments. Acupuncture, homeopathy, aromatherapy and spiritual healing are examples of complementary therapies.
Producing false memories to replace memories that are no longer capable of being stored. A person may guess an answer or imagine an event and then mistake it for an actual memory. Although it may be seen by others as lying, the person is unaware that their memories are false or inaccurate.
A state in which problems with memory and concentration impair the function of the mind.
A state in which there is insufficient water in the body. It occurs when a person’s fluid intake fails to balance fluid loss through sweating, vomiting or diarrhoea.
Features confusion, speech disorders, anxiety and sometimes hallucinations. Often has a rapid onset and lasts from hours to weeks. Fluctuations in conscious state.
A term used to describe impairment of brain function, involving memory, thinking and concentration. Dementia usually becomes progressively worse, eventually making it impossible for someone to cope with living without help. There are many causes of dementia, including Alzheimer’s disease, vascular dementia, Lewy body disease and Pick’s disease.
An illness in which the main symptoms are feeling low, tearfulness and loss of enjoyment. Depression can affect sleep, appetite, motivation and concentration. It is treatable.
Occurs when the amount of sugar in the blood cannot be regulated. There are several types of diabetes.
The process of identifying and naming a disease from a person’s symptoms and signs. Getting a diagnosis may only involve talking with the doctor and having a physical examination. In other cases, special investigations may need to be done as well.
Loss of feelings of shame or embarrassment that normally help control a person’s actions. Disinhibition results in inappropriate or improper behaviour.
A state in which someone loses their awareness of time and place. For example, they may fail to recall the date or even the year, and may not be able to say where they are.
The generic name of Aricept, a dementia drug that is a cholinesterase inhibitor. It works by increasing the amount of a certain substance (acetylcholine) in the brain.
A genetic condition caused by an extra copy of chromosome 21 that results in slowed growth, abnormal facial features and intellectual disabilities.

24 Dementia Essentials
Enduring Power of Attorney (EPA)
Epileptic seizures
Exelon
Frontotemporal dementia
Frontal lobes
Galantamine
Generic
Genes
Geriatrician
Hallucination
HIV
Huntington’s disease
Incontinence
Korsakoff’s syndrome
Lewy body disease
Limbic region
Memantine
A legal document in which one person gives another the power to handle his or her financial affairs. An EPA can only be drawn up if the person handing over this power can understand what he or she is doing. The EPA comes into force only after it has been officially registered.
Caused by a group of nervous system disorders that produce an uncontrolled electrical discharge in the brain.
The brand name for rivastigmine, a dementia drug that improves the function of nerve cells in the brain. It works by preventing the breakdown of a chemical that is important for the processes of memory, thinking, and reasoning.
A dementia in which the disease process mainly affects the frontal lobes of the brain. Memory is affected less than in other dementias, but there may be major problems with loss of motivation and disinhibition.
Parts of the cerebral cortex situated at the front of the brain. This is the area of the brain that controls movement of the body. It is also involved in ‘higher functions’, such as planning ahead, problem-solving and initiative.
The generic name of Reminyl, a type of dementia drug that is a cholinesterase inhibitor. It works by increasing the amount of a certain substance (acetylcholine) in the brain
A generic drug is a drug that is sold under its official medical name (its generic name) rather than under a patented brand name.
Material contained within the chromosomes. Genes carry the blueprint for the body; information that dictates how our bodies are built up, including the colour of our eyes and skin, how tall we are, our gender and many other details. Some genes have defects, or mutations, that cause disease.
A doctor who specialises in the treatment of physical illnesses in older people.
A perception (hearing, seeing, smelling or feeling something) without appropriate stimulus. For example, hearing voices when there is no-one there. Hallucinations are quite common in people with dementia.
Abbreviation for Human Immunodeficiency Virus.
Also sometimes called Huntington’s chorea, a disease in which mental deterioration is accompanied by involuntary twitching and muscle spasms.
Involuntary or inappropriate passing of urine or faeces. Help is available from continence advisors.
A memory disorder caused by lack of vitamin B1 (thiamine) sometimes caused by alcoholism.
A type of dementia in which abnormal collections of proteins called Lewy bodies, occur in the brain. People with Lewy body disease typically show more variation in their mental abilities from day-to-day than is usual with other dementias.
Situated deep inside the brain, this region is responsible for functions such as eating, sleeping, consciousness and emotions.
A dementia drug, which works by altering chemicals called NMDA receptors in the brain. It may slow the progression of dementia in some people.
Module 2.1 & 2.2 25
Memory
MRI scan
Neuroleptic drugs
Neurologist
Neurone
Neurotransmitters
Occiptal lobe
Parietal lobes
Parkinson’s disease
Person-centred care
PET scan
Pick’s disease
Posterior Cortical Atrophy
Prevalence
Progressive Supranuclear Palsy
Reality orientation
Reminiscence therapy
Reminyl
Rivastigmine
Temporal lobes
The retention in the mind of information that may be recalled later.
Abbreviation for Magnetic Resonance Imaging scan. A type of brain scan that creates pictures using a powerful magnetic field rather than X-rays.
Another name for antipsychotic drugs.
A doctor who specialises in the diagnosis, treatment and management of diseases of the nervous system.
A nerve cell.
A group of chemicals in the brain that enables nerve cells to communicate with each other. Groups of adjacent nerve cells tend to use the same neurotransmitter. Examples include acetylcholine, serotonin and dopamine.
Part of the cerebral cortex situated at the back of the brain, responsible for interpreting what is seen.
Part of the cerebral cortex situated on either side of the brain above the ears. Responsible for anything to do with order and structure.
A chronic disease of the nervous system that is characterised by slowness of movements, a tremor and an expressionless face. Some affected people also develop dementia.
A holistic approach to dementia care focusing on the individual and utilising aspects such as the person’s past history, routines, personal preferences and needs.
Abbreviation for Positron Emission Tomography scan. A sophisticated brain scan which is able to look at the brain in great detail. It is not generally available in clinical practice.
A rare dementia which commonly affects younger people than Alzheimer’s disease. It affects language and personality before there is any significant change in memory.
Refers to gradual and progressive degeneration of the outer layer of the brain (the cortex) in the part of the brain located in the back of the head (posterior).
Rate of occurrence.
A rare condition that causes problems with control of gait, balance and vision.
A psychological treatment in which every opportunity is taken to make people with dementia aware of the time, where they are and the world around them.
A treatment that aims to stimulate people’s memories by means of old films, pictures, music, etc.
The brand name for galantamine, a dual-action dementia drug. It is anticholinesterase drug and also works by stimulating areas of the brain called nicotinic receptors.
The generic name for Exelon, a dementia drug.
Parts of the cerebral cortex situated behind the temples, and responsible for our memory.

26 Dementia Essentials
Sedative drugs
Side effects
Snoezelen
Stroke
Syndrome
Thyroid
Tranquillisers
Validation
Vascular dementia
Vitamins
Drugs used to reduce symptoms of anxiety and agitation and to help people sleep. Sedative drugs increase confusion in people with dementia.
The unwanted ‘extra’ effects that occur in addition to the desired therapeutic effects of a drug. Most drugs have some side effects. These will vary from person to person and commonly disappear when the body becomes used to a particular drug.
A special room designed to gently stimulate the senses and to calm people who are agitated.
A result of a haemorrhage in the brain, or of a blood clot in an artery of the brain, leading to paralysis of part or all of one side of the body, or loss of speech, or loss of consciousness or death. The paralysis may be sudden or gradual in onset.
A group of signs and symptoms that occur together and are typical of a particular disorder or disease.
A gland in the neck that produces a chemical known as thyroid hormone. This hormone is essential to the workings of the body. Thyroid hormone deficiency is a rare cause of dementia.
Drugs used to help people who are very anxious. These drugs can cause increased confusion in people with dementia.
A technique used in caring for people with dementia that focuses on feelings rather than confusion.
A type of dementia associated with problems affecting the circulation of blood to the brain, such as may result from a series of small strokes.
Chemical compounds essential to health that are found in many foods. Vitamin deficiency is a rare cause of dementia.
Module 2.1 & 2.2 27

28 Dementia Essentials