degree of wheat and gluten avoidance in coeliac disease...
TRANSCRIPT

COELIAC DISEASE:
Dr. Kim Faulkner-Hogg
Dietitian
Allergy Unit, RPAH, Sydney
(02) 9515 3323
WHAT IS COELIAC
DISEASE?
Gluten Ingestion
Inflamed Small Intestinal Mucosa
Villous Atrophy
Gluten-Free Diet
Restoration of Health

PREVALENCE of
COELIAC DISEASE
• Historically in Caucasians 1:300 - 1:2000
• Ireland and Scandinavia 1: 100
• Algeria in Africa 1:18
• Australian prevalence 1:2501
• Worldwide Screening Diagnosis 1:266 2
• Worldwide Clinical Diagnosis 1:33452
1. Hovell et al, 2001
2. Fasano & Catasi, 2001
CLASSIC SYMPTOMS
• Malabsorption
• Failure to thrive
• Weight loss
• Muscle wasting
• Diarrhoea
• Abdominal cramp
• Bloating
• Flatus
• Nausea
• Vomiting
• Steatorrhoea
• Weakness
• Bruising
MINOR NON-SPECIFIC
COMPLAINTS
• Headaches
• Dizziness
• Constipation
• Skin rashes
• Tiredness
• Recurrent mouth ulcers

OTHER SIGNS
• unexplained iron or folate deficiency
• delayed menarche
• sub-optimal school performance
• apparent food intolerances
• enamel defects of permanent teeth
• infertility in either gender
• recurrent miscarriages
• general malaise

Malabsorption of
• lipid
• carbohydrate
• protein
• iron
• calcium
• magnesium
• vitamins (especially fat soluble ones)
10-20% of first degree relatives have coeliac disease

RISKS OF UNTREATED DISEASE
• Sub-optimal nutrient absorption– of protein, fat, CHO, iron,
calcium, magnesium, zinc and vitamins
• Low nutritional status– Anaemia
– Reduced bone mineral density
• Increased risk of malignancy
• Infertility
• Neurological disorders– Ataxia
– Epilepsy
– Early Onset Dementia
• Liver disorders
• Peripheral neuropathy
Diagnosis of Coeliac Disease
1. Initially a blood screening test looking for coeliac related antibodies
2. Secondly a small bowel biopsy to look for damage to the small bowel
3. Repeat biopsy generally 6 months later to show recovery of the small bowel

The European Society for Paediatric
Gastroenterology and Nutrition (ESPGAN)
• First biopsy:
• Must show small bowel mucosal atrophy on
a gluten containing diet
• Second biopsy:
• Small bowel should show improvement or
normalization while on a GFD.
• The need for gluten challenge and 3rd biopsy is
assessed individually.
DIAGNOSIS

Coeliac disease
• Normal
• PVA
– partial villous atrophy
• STVA
– subtotal villous
atrophy
• TVA
– total villous atrophy
OTHER CAUSES OF ABNORMAL SMALL
BOWEL MUCOSA
• Cow‟s milk protein
intolerance
• Soya protein intolerance
• Immunodeficiency
syndromes
• Eosinophilic
gastroenteropathy
• Intractable diarrhoea of
infancy
• Gastritis in children
• Parasites, eg giardia
• Tuberculosis
• Human immunodeficiency
virus
• Contaminated bowel
syndrome
• Whipple‟s disease
• Arterial disease of the
small intestine
• Drug & radiation damage
Howdle P. The Practitioner, 1994;238:687-691

GLUTEN-FREE FOODS
• DAIRY
– milk and cheese
• FRUIT
• VEGETABLES
• PULSES
– legumes, beans, nuts and seeds
• MEAT
– beef, chicken, fish
• EGGS
What can be eaten?

GLUTEN-FREE GRAINS
• Maize / Corn
• Rice
• Soy
• Buckwheat
• Millet
• Sorghum
• Tapioca
• Quinoa
• Arrowroot
• Amaranth
What can be eaten?

GLUTEN SOURCES
• Wheat
• Triticale (hybrid of wheat and rye)
• Rye
• Barley
• Possibly oats: controversial
Listed in decreasing order of gluten quantity

SEROLOGICAL SCREENING TESTS
Blood tests cannot diagnose coeliac disease
Blood screening tests available are:
• Anti-gliadin anti-body
• IgA and IgG
• Anti-endomysial anti-body
• IgA and IgG
• Anti-transglutaminase anti-body
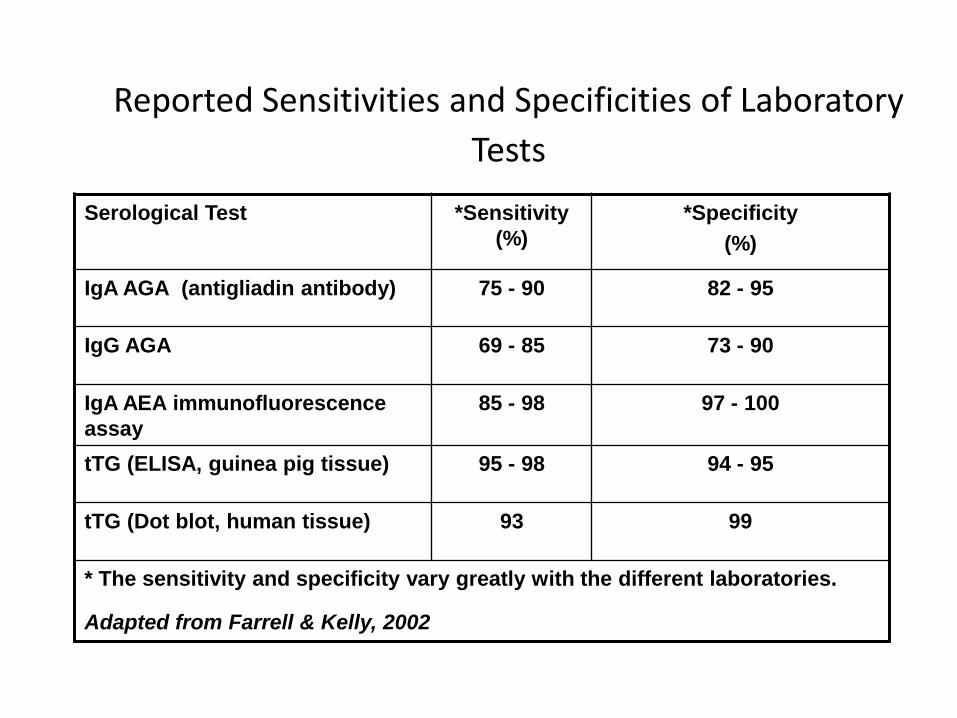
Reported Sensitivities and Specificities of Laboratory
Tests
Serological Test *Sensitivity
(%)
*Specificity
(%)
IgA AGA (antigliadin antibody) 75 - 90 82 - 95
IgG AGA 69 - 85 73 - 90
IgA AEA immunofluorescence
assay
85 - 98 97 - 100
tTG (ELISA, guinea pig tissue) 95 - 98 94 - 95
tTG (Dot blot, human tissue) 93 99
* The sensitivity and specificity vary greatly with the different laboratories.
Adapted from Farrell & Kelly, 2002

DIAGNOSING COELIAC DISEASE
Gluten must be eaten for the blood & biopsy
tests to be valid
children: eat gluten freely
adults : 30g wheat-based cereal and 2 slices
bread per day
quantities consumed for 3-6 weeks prior to
biopsy
DIAGNOSIS
• Gold Standard
– Small bowel biopsy
• Markers of disease progression??
– Low enzyme levels
• lactase
• sucrase
• alkaline phosphatase
– High intra-epithelial lymphocytes (IEL)
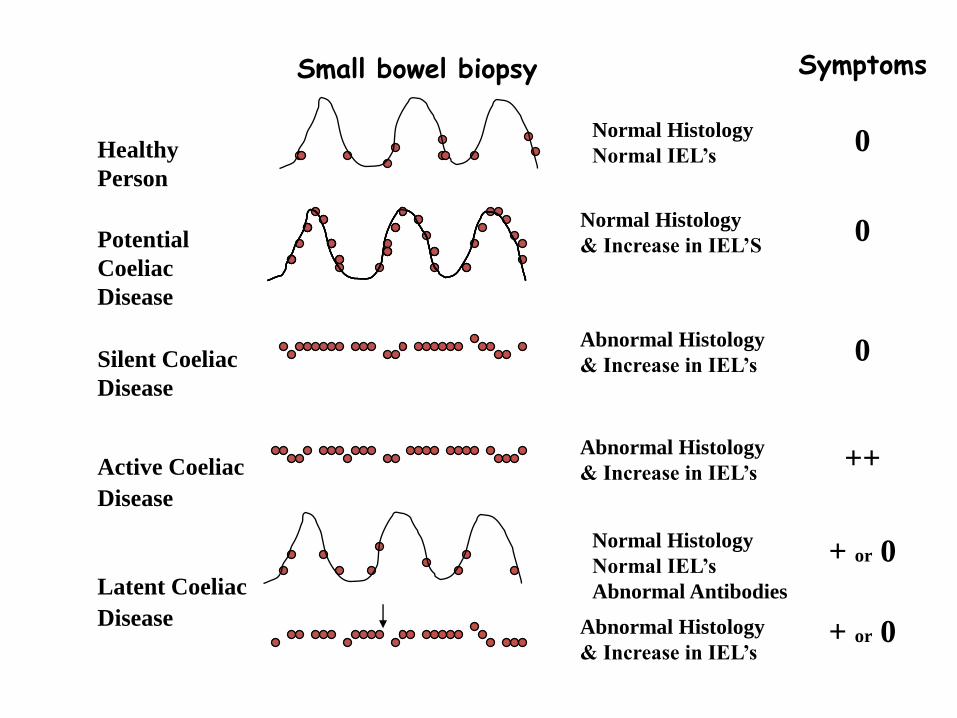
Healthy
Person
Normal Histology
Normal IEL‟s
Abnormal Antibodies
SymptomsSmall bowel biopsy
0
Silent Coeliac
Disease
Abnormal Histology
& Increase in IEL‟s0
Active Coeliac
Disease
Abnormal Histology
& Increase in IEL‟s++
Potential
Coeliac
Disease
Normal Histology
& Increase in IEL‟S0
Latent Coeliac
Disease
+ or 0
Normal Histology
Normal IEL‟s
+ or 0Abnormal Histology
& Increase in IEL‟s
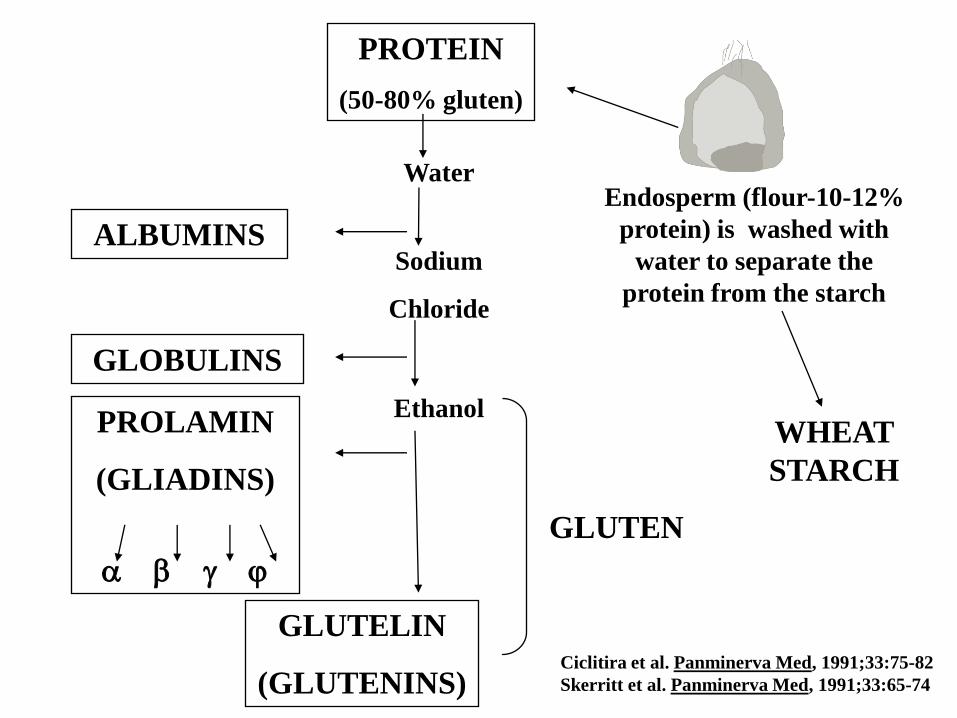
Endosperm (flour-10-12%
protein) is washed with
water to separate the
protein from the starch
PROTEIN
(50-80% gluten)
WHEAT
STARCH
Water
Sodium
Chloride
Ethanol
ALBUMINS
GLOBULINS
GLUTELIN
(GLUTENINS)
PROLAMIN
(GLIADINS)
GLUTEN
Ciclitira et al. Panminerva Med, 1991;33:75-82
Skerritt et al. Panminerva Med, 1991;33:65-74
GLUTEN
WHAT IS IT?
• The main protein in wheat flour
• ~equal mixture of glutenin (a glutelin) and gliadin (a prolamin)
• Gluten makes rising possible
– Gluten stretches around trapped air. It sets when cooked
WHAT CAUSES THE
DAMAGE?
• The alcohol soluble
prolamin; (called gliadin in
wheat)
• AND the glutelins; (called
glutenin in wheat)
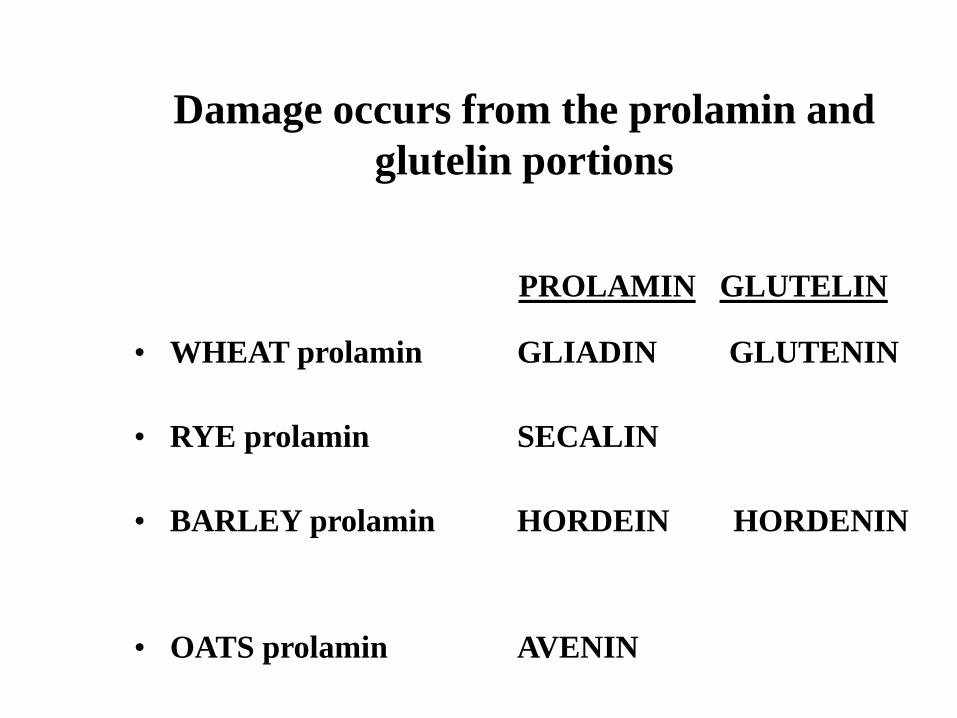
Damage occurs from the prolamin and
glutelin portions
• WHEAT prolamin GLIADIN GLUTENIN
• RYE prolamin SECALIN
• BARLEY prolamin HORDEIN HORDENIN
• OATS prolamin AVENIN
PROLAMIN GLUTELIN

• The gliadins and glutenins are the storage proteins of wheat endosperm and they tend to be rich in asparagine, glutamine, arginine or proline but very low in nutritionally important amino acids lysine, tryptophan and methionine
Abrol et al., 1971; Derbyshire et al., 1976; Kirkman et al., 1982;
Larkins 1981; Spencer and Huggins 1982
GLUTEN
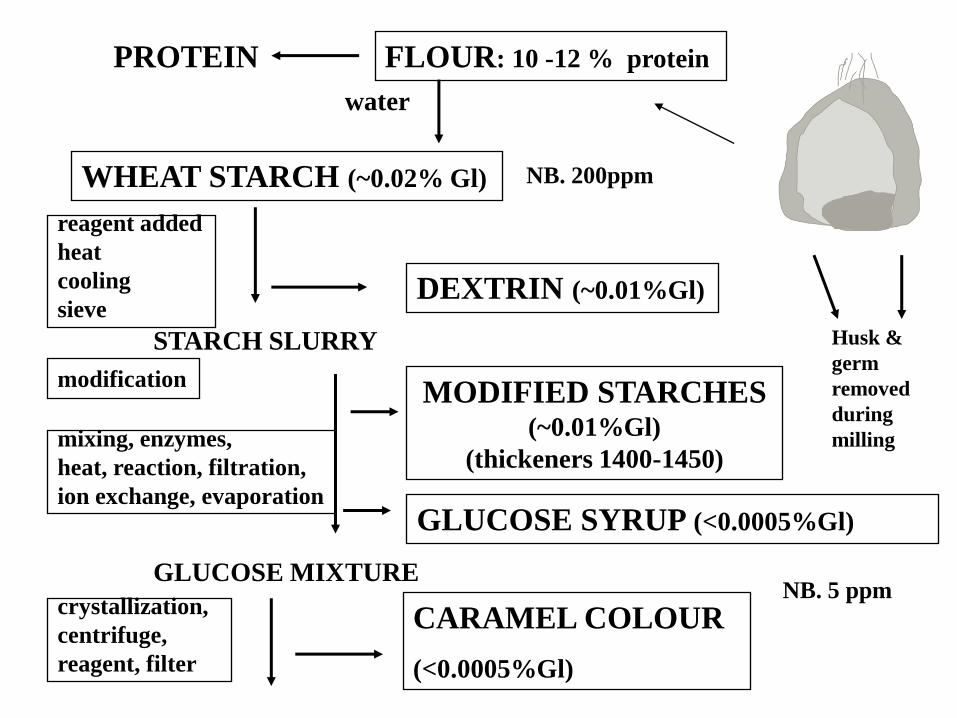
Husk &
germ
removed
during
milling
FLOUR: 10 -12 % proteinPROTEIN
WHEAT STARCH (~0.02% Gl)
reagent added
heat
cooling
sieveDEXTRIN (~0.01%Gl)
STARCH SLURRY
modificationMODIFIED STARCHES
(~0.01%Gl)
(thickeners 1400-1450)mixing, enzymes,
heat, reaction, filtration,
ion exchange, evaporationGLUCOSE SYRUP (<0.0005%Gl)
crystallization,
centrifuge,
reagent, filter
CARAMEL COLOUR
(<0.0005%Gl)
GLUCOSE MIXTURE
water
NB. 5 ppm
NB. 200ppm

VARYING GLUTEN QUANTITIES
*If derived from wheat
Allergy Unit RPAHLevel is decreasing
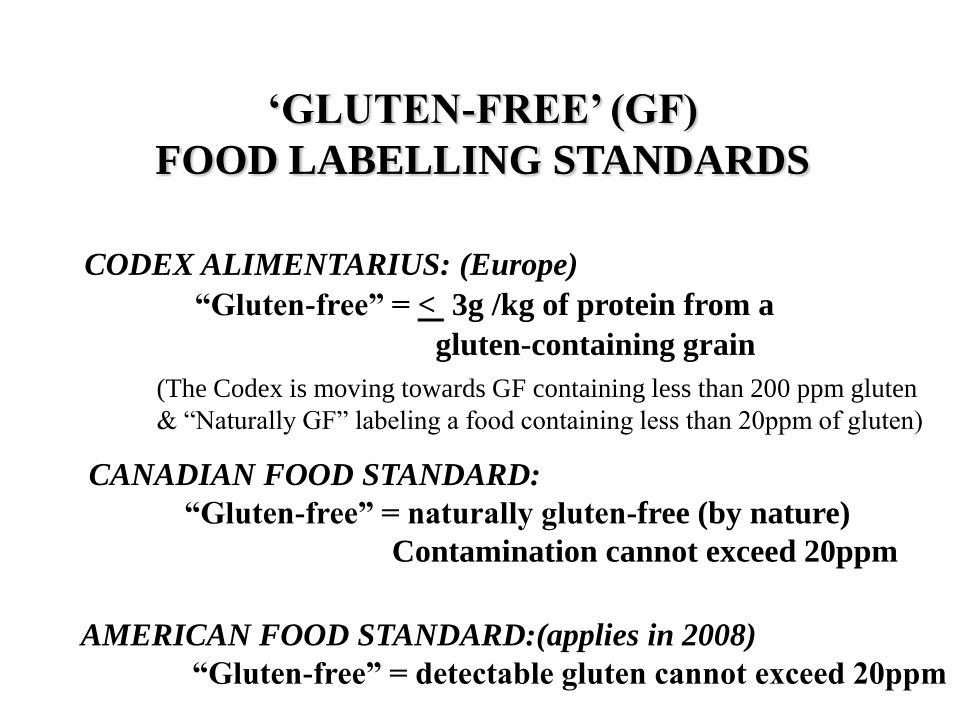
„GLUTEN-FREE‟ (GF)
FOOD LABELLING STANDARDS
CODEX ALIMENTARIUS: (Europe)
“Gluten-free” = < 3g /kg of protein from a
gluten-containing grain
CANADIAN FOOD STANDARD:
“Gluten-free” = naturally gluten-free (by nature)
Contamination cannot exceed 20ppm
(The Codex is moving towards GF containing less than 200 ppm gluten
& “Naturally GF” labeling a food containing less than 20ppm of gluten)
AMERICAN FOOD STANDARD:(applies in 2008)
“Gluten-free” = detectable gluten cannot exceed 20ppm

„GLUTEN-FREE‟ FOOD
LABELLING STANDARDS
There is no single, standard definition of a gluten-free diet
AUSTRALIAN FOOD STANDARDS:
“Gluten-free” = no oats or malt, or products
derived from them AND no detectable gluten
(<0.0005 % gluten; 5ppm)
“Low Gluten” = cannot contain more than 0.002%
gluten (200 parts per million). Oats and malt
products could be used.
1.
2.
The gluten-free food standard is not a medical prescription
• The food standards are designed to produce food for a large population of people with coeliac disease.
• Doctors and dietitians can individualize ingredients to tailor the diet to the requirements of each patient.
THE GLUTEN-FREE DIET
• There is no legislation for a gluten-free DIET
• The ingredients allowed in the LABELING of a gluten-free food influences the advice given to the person with the disease, about what ingredients to include in foods they make and purchase
• A GFD rarely contains zero gluten
• Average gluten intake is 30mg gluten/day (Codex-GFD) 1
• Normal dietary gluten intake is 10-14g gluten/day (i.e. 10000-14000mg)
1. Kaukinen et al. Scand J Gastro, 1999;34(2):163-169

WHAT ADVICE SHOULD
WE BE GIVING?
• Cancer risk
• Symptom persistence
• Biopsy outcome

CANCER RISK
• Intestinal lymphoma
• Adenocarcinoma of the small intestine
• Adenocarcinoma of the pharynx
• Adenocarcinoma of the oesophogus
• Primary liver cancer
• T-cell non-Hodgkin lymphoma of the upper
intestine
• Enteropathy-associated T-cell lymphoma
(rare with poor outcome)
Catassi C et al. Gastroenterology 2005;128:S79-S86
CD is associated with increased risk of:

CANCER RISK
• Before diagnosis of CD
• With in 2 years of the diagnosis of CD
• These cancers are rarely seen in those
adhering to long-term GFD‟s
• Many years of gluten exposure before
starting the GFD increase the risk of
developing cancer
These cancers are generally seen in a person
Studies suggest a GFD protects from these forms of
cancer development
Catassi C et al. Gastroenterology 2005;128:S79-S86
UK CANCER STUDY
T-cell lymphoma: late complication in 5-10% of cases
Normal diet
Reduced gluten diet
Gluten-free diet :- (Codex Alimentarius
guidelines used in the United Kingdom)
Holmes et al. Gut 1989; 30: 333-338.
•“The results indicate that for coeliac patients
who have taken a GFD for 5 years or more, the
risk of developing cancer over all sites is not
increased when compared with the general
population. The risk is increased, however, in
those taking a reduced gluten, or a normal
diet.”
CANCER CONCLUSION
Holmes et al. Gut 1989; 30: 333-338.
SYMPTOMSAustralian Study:
Coeliacs removed malt and wheat starch from their diet
• Symptoms improved in 15 of 22 (68%) in 3 months
• 8 of 22 (36%) required no further interventionFaulkner-Hogg, Selby & Loblay. Scand J Gastro,1999; (8):784-789
Canadian Study:
Coeliacs never eaten wheat starch asked to eat it daily
• 15 of 17 developed symptoms immediately, or over the
next 10 months.
• The 14 in the Control group remained symptom free
Chartrand L. et al. JADA June 1997; 97 (6): 612-618.
SYMPTOMS from oats
British Medical Association:
12 week contaminant-free oat challenge in 19 adults
• 2 developed bloating, abdominal discomfort and or a
rash Lundin KEA et al. Gut, 2003; 52:1649-1652
Finish Study:
5 year follow-up of 43 people eating oats
• initially 5 drop outs: 2 with rash, 2 with abdominal
symptoms and 2 gave no reason
Janatuinen EK et al. The New England Journal of Medicine 1995, Oct;333:1033-1037.

Wheat starch, malt and oats
cause symptoms in
only SOME people
with coeliac disease.
SYMPTOM CONCLUSION

Faulkner-Hogg, Selby & Loblay. Scand J Gastroenterol 1999; (8):784-789.
Australian Study:
Withdrawal of wheat starch and malt for 3 months
• No change in the biopsy outcomes; villous
improvement was not seen
United Kingdom Study:
6 week daily ingestion of wheat starch product
• No villous atrophy occurred
Ciclitara et al. Clinical Nutrition 1985:39C;303-308.
BIOPSY: short-term

Catassi C, et al. Gut 1993;34:1515-1519.
Group 1
100mg gliadin / day (200mg gluten) Minimal IEL changes
No biopsy height damage
Group 2
500mg gliadin / day : (1 g gluten)More pronounced changes in both IEL and
villi height
BIOPSY: 4 week short term studyStudy done in children

BIOPSY: short-term
Capsules of gluten given daily for 90 days to 33 CD
adults with normal biopsies
Biopsy performed before and after capsules
• 10 mg gluten did not cause mucosal damage
• 50 mg gluten caused minimal histological damage
(and 15% regained symptoms)
He suggests there may be a threshold of tolerable
gluten
Catassi Cet al. American Gastroenterological Assoc 2005 Abstract only
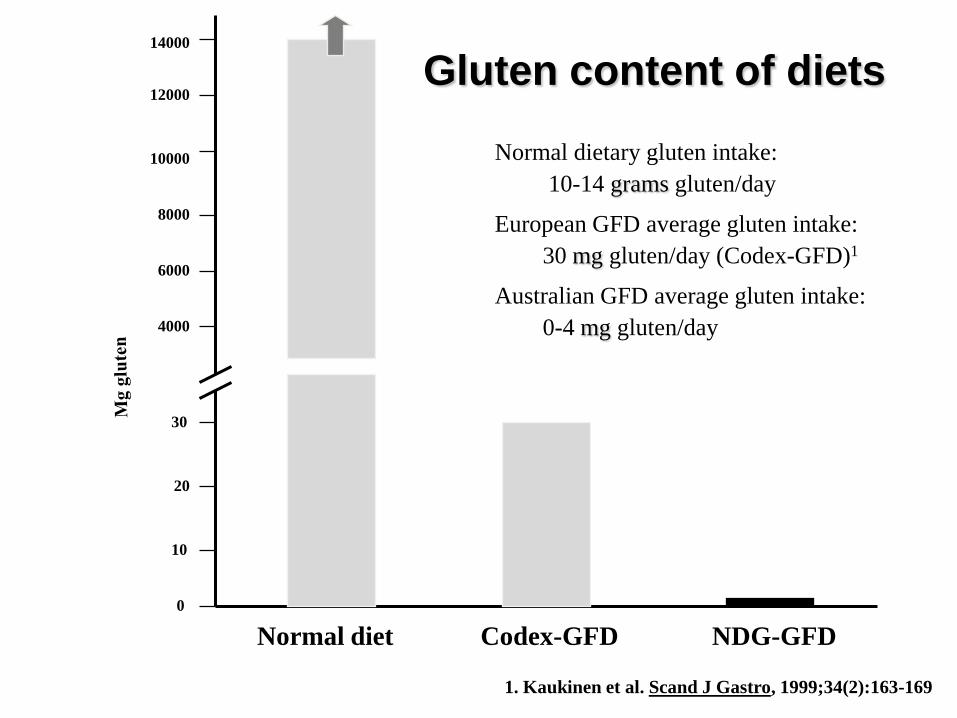
Gluten content of diets
30
20
10
0
14000
12000
10000
8000
6000
Normal diet Codex-GFD NDG-GFD
4000
Normal dietary gluten intake:
10-14 grams gluten/day
European GFD average gluten intake:
30 mg gluten/day (Codex-GFD)1
Australian GFD average gluten intake:
0-4 mg gluten/day
1. Kaukinen et al. Scand J Gastro, 1999;34(2):163-169

BIOPSY: longer-term
Swedish Study:
• Study outline
– 52 children & adults
– Average gluten eaten was 34mg/day (R=5-150)
– Mean 10 months in the study (R: 6-24)
• Conclusion
– No damage to the biopsy
– Some symptom persistence
Kaukinen et al, Scand J Gastro, 1999;34(2):163-169.

BIOPSY: longer-term
Australian 2 year follow-up study:
• Study outline
• 39 subjects
• Diet excluded wheat starch and malt
• 2 years: mean gluten intake 3-4mg /day
• Conclusion
• Abnormal biopsy results did not return to normal
due to excluding Codex-gluten ingredients
• There is no significant difference in the gluten
intakes in those whose biopsy changed from normal
to abnormal or abnormal to normal, during the 2
year period.Faulkner-Hogg, Selby and Loblay:-unpublished to date

BIOPSY: Oats
British Medical Association:
12 week oat challenge in 19 adults
• Consumed 50g contaminant free oats per day
• 1 developed severe villous atrophy to oats
Lundin KEA et al. Gut, 2003; 52:1649-1652
Janatuinen EK et al. Gut, 2002;50:332-335.
Finnish Study:
5 year follow-up on free consumption of contaminant free
oats
• 45 began the study and 23 lasted the 5 years
• Concluded no biopsy damage. Abnormal biopsies were
treated as non compliance

50mg gluten per day caused minimal damage in 1 study
100mg gliadin (200mg gluten) per day causes minimal villous damage.
500mg gliadin (1g gluten) per day causes definite villous damage
The small number of studies appear to suggest that the ingestion of wheat starch and malt, in the amounts generally consumed in Europe, (mean 34mg gluten /day) in products labelled as gluten free, does not lead to damage of the small bowel mucosa.
The Australian study did not see an improvement in biopsy outcomes with prolonged avoidance of malt and wheat starch
50g oats per day can damage the mucosa in some people
BIOPSY CONCLUSION

Small amounts of gluten are found in oats, wheat starch, malt and some products derived from these.
Cancer
After 5 years, a gluten-free diet containing wheat starch and malt, can still decrease the risks of developing coeliac related cancers.
Small Bowel Mucosa
European studies suggest wheat starch does not cause mucosal damage
The removal of wheat starch and malt for 2 years, did not improve the small bowel mucosa in most subjects in the Australian study.
Oats can cause mucosal damage
Symptoms
However some people are more symptomatic when consuming these trace amounts of gluten [oats, wheat starch & malt].
OVERALL CONCLUSIONS

Perhaps there is NOT ONE GFD prescription to suit everyone.
• The Codex Alimentarius uses the concept that „gluten-
free‟ refers to a harmless level of gluten when ingested
indefinitely
• Doctors and dietitians can use repeated assessments to
help tailor the diet to the persons sensitivities
• Some of our clients may be able to use some Codex
defined ingredients periodically…such as wheat starch
100mg gliadin 200mg gluten 2.5g wheat flour1
20mg gluten = 100g Codex wheat starch2
~ ≤0.02% gluten in Australian wheat starch3
Residual Gluten
1. Catassi C, et al. Gut 1993;34:1515-1519
2. Hischenhuber C et al. Aliment Pharmacol Ther, 2005;23:559-575
3. Wheat Starch Australia (verbal 1993)
Codex & Australian wheat starch
100mg gliadin 200mg gluten 1000g Codex/Oz wheat starch
25mg gliadin 50mg gluten 250g Codex/Oz wheat starch
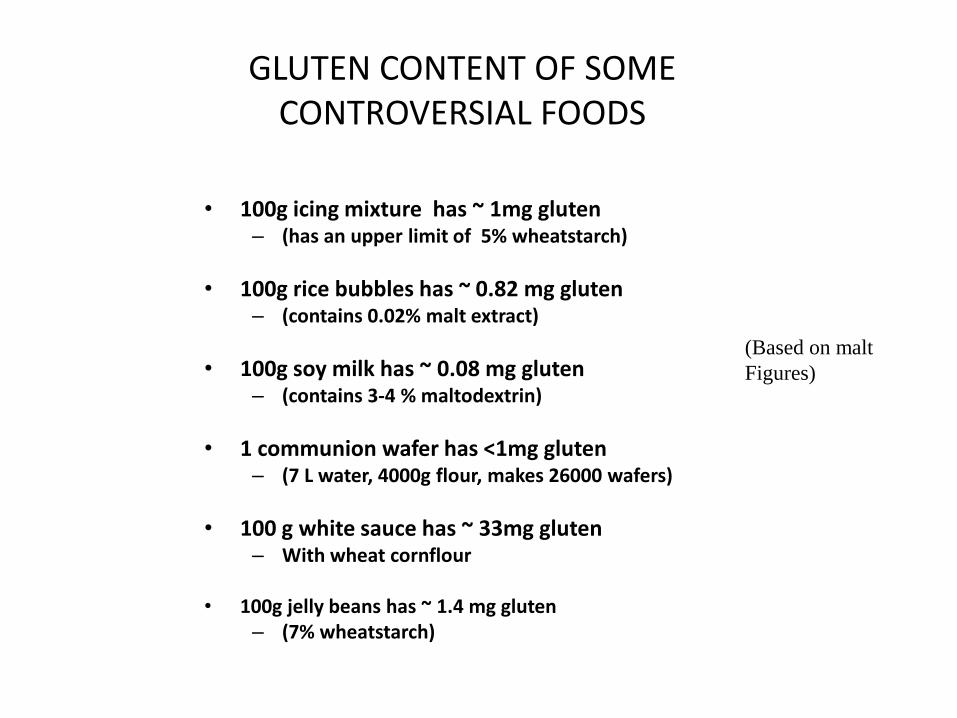
GLUTEN CONTENT OF SOME CONTROVERSIAL FOODS
• 100g icing mixture has ~ 1mg gluten– (has an upper limit of 5% wheatstarch)
• 100g rice bubbles has ~ 0.82 mg gluten– (contains 0.02% malt extract)
• 100g soy milk has ~ 0.08 mg gluten– (contains 3-4 % maltodextrin)
• 1 communion wafer has <1mg gluten– (7 L water, 4000g flour, makes 26000 wafers)
• 100 g white sauce has ~ 33mg gluten– With wheat cornflour
• 100g jelly beans has ~ 1.4 mg gluten– (7% wheatstarch)
(Based on malt
Figures)
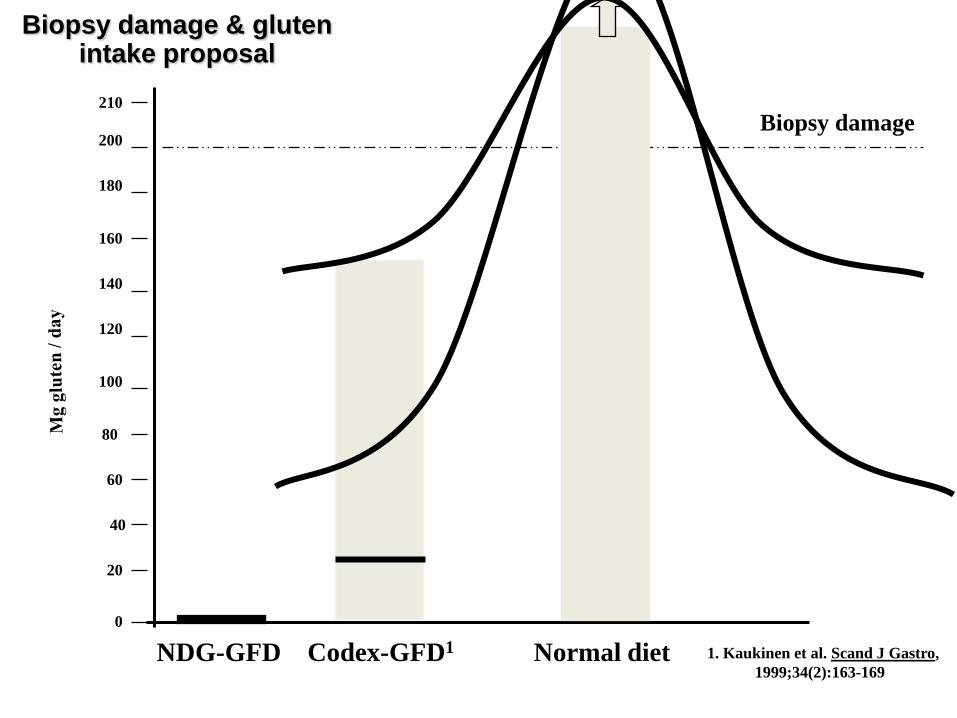
Biopsy damage & gluten intake proposal
60
40
20
0
180
160
140
120
100
Codex-GFD1NDG-GFD
80
1. Kaukinen et al. Scand J Gastro,
1999;34(2):163-169
200
210
Normal diet
Biopsy damage
Perhaps there is NOT ONE GFD prescription to suit everyone.
Repeated assessments can help tailor the diet to the persons sensitivities.

Allowed Ingredients for the newly diagnosed
*If derived from wheat
Allergy Unit RPAH

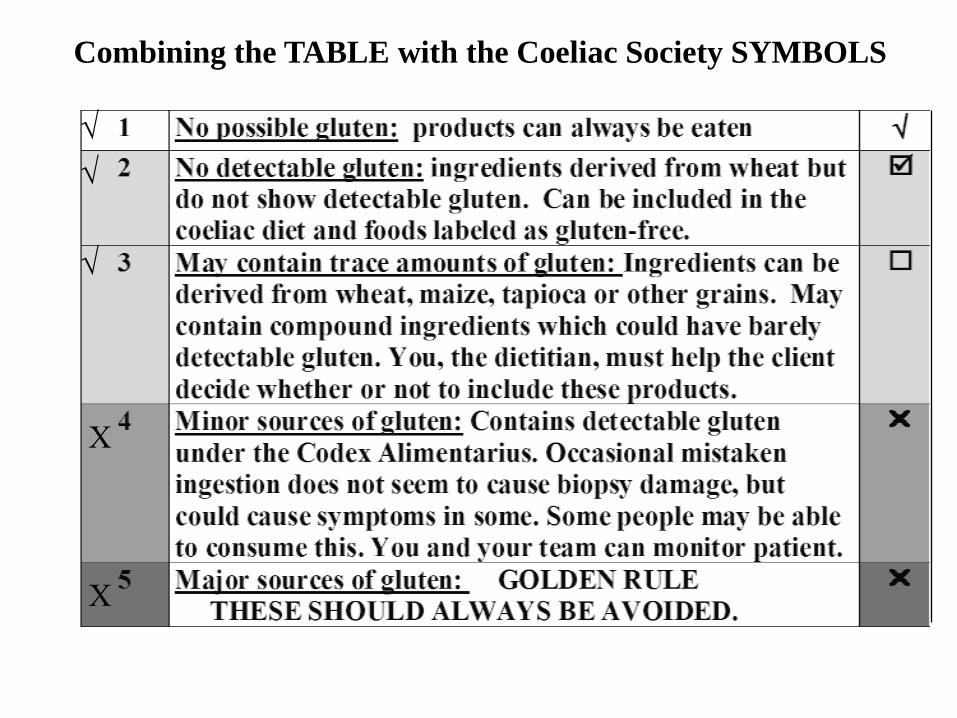
Combining the TABLE with the Coeliac Society SYMBOLS

PATHOGENESIS
• Environmental
– Breastfeeding
• May decreases risk of developing CD in some
circumstances
– Gluten exposure
• More CD in cultures who eats the most wheat
– Twin studies
• 25% discordance suggests environmental factors
involved

PATHOGENESIS
• Genetic Factors
− 10% increased prevalence in first degree relatives
− 75% twin concordance
− Human leukocyte antigen (HLA) similarity
• HLA-DQ2, HLA-DQ8
General population genes
HLA DQ2 or DQ8
95-98% of people with CD
Kagnoff M,
Gastroenterology 2005;
128:S10-S18
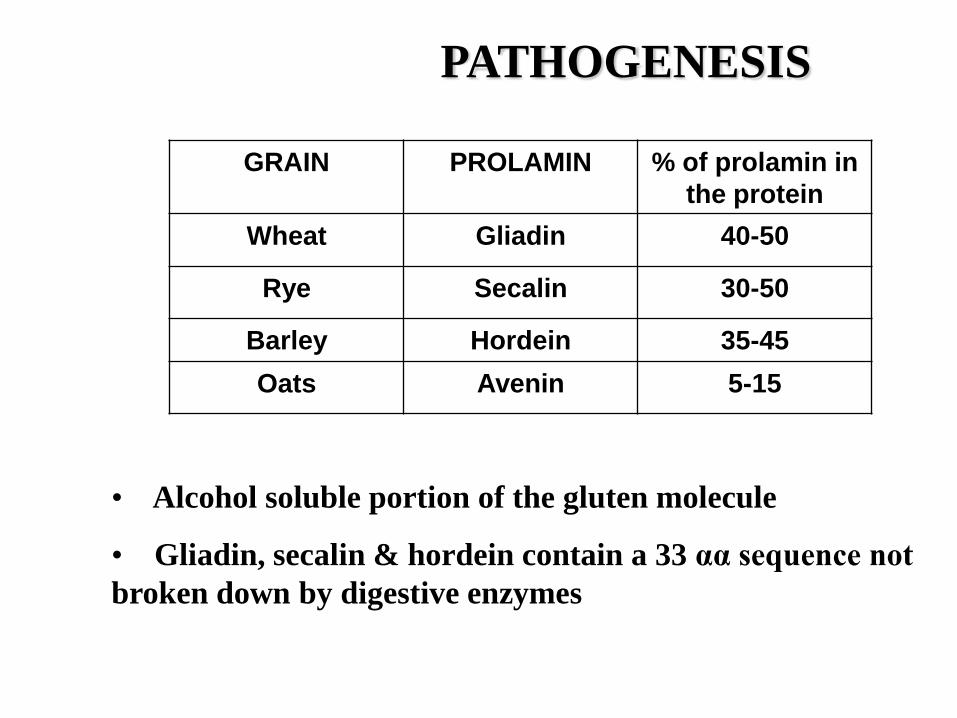
PATHOGENESIS
GRAIN PROLAMIN % of prolamin in
the protein
Wheat Gliadin 40-50
Rye Secalin 30-50
Barley Hordein 35-45
Oats Avenin 5-15
• Alcohol soluble portion of the gluten molecule
• Gliadin, secalin & hordein contain a 33 αα sequence not
broken down by digestive enzymes
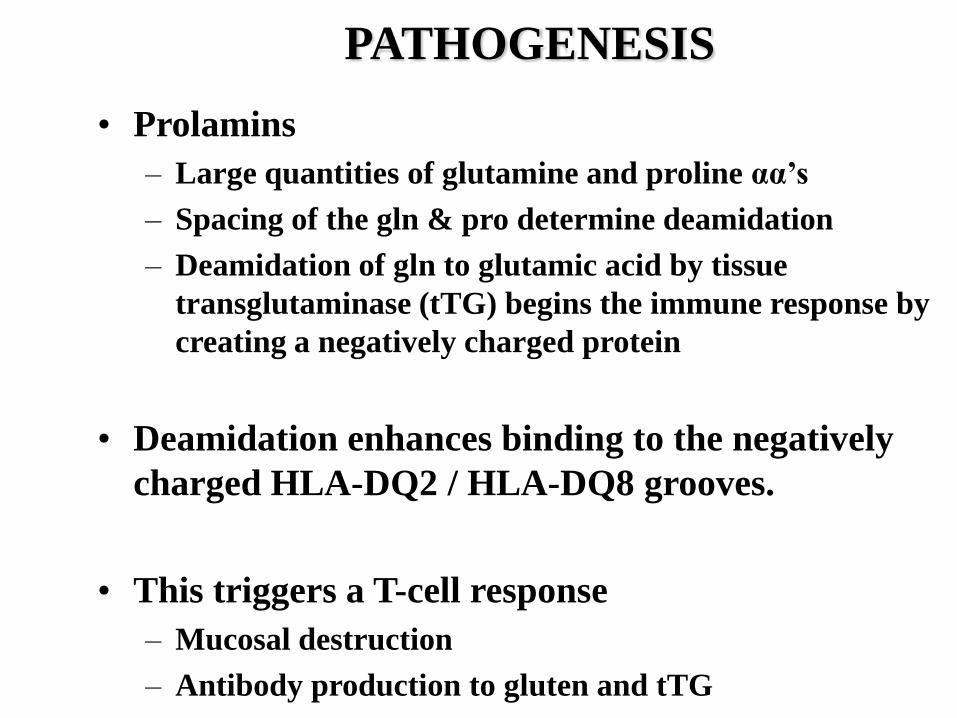
PATHOGENESIS
• Prolamins
– Large quantities of glutamine and proline αα‟s
– Spacing of the gln & pro determine deamidation
– Deamidation of gln to glutamic acid by tissue
transglutaminase (tTG) begins the immune response by
creating a negatively charged protein
• Deamidation enhances binding to the negatively
charged HLA-DQ2 / HLA-DQ8 grooves.
• This triggers a T-cell response
– Mucosal destruction
– Antibody production to gluten and tTG
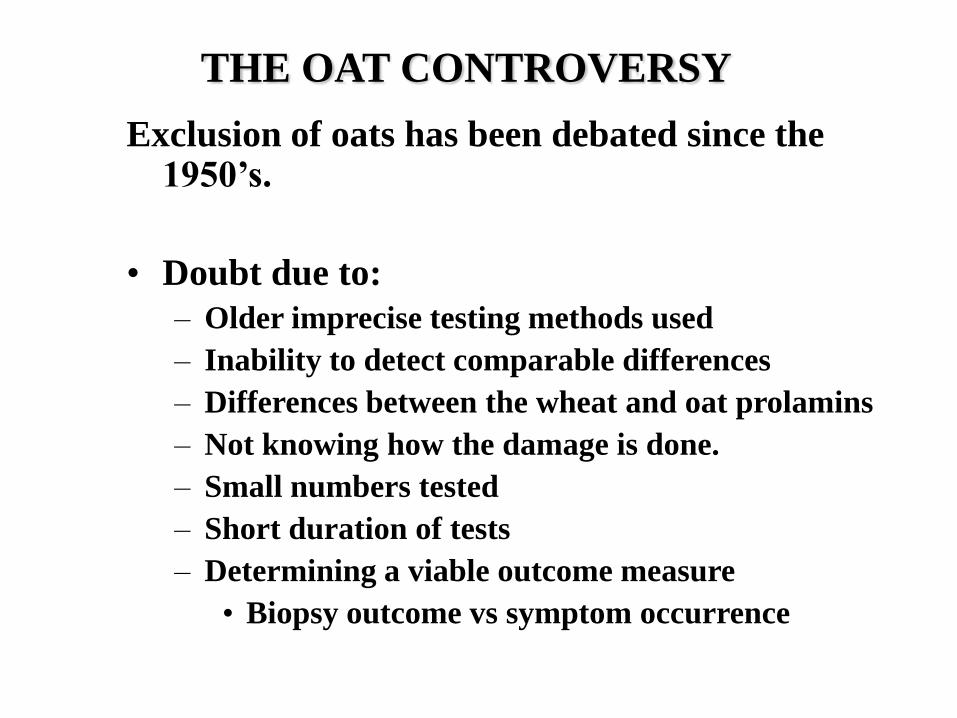
THE OAT CONTROVERSY
Exclusion of oats has been debated since the 1950‟s.
• Doubt due to:
– Older imprecise testing methods used
– Inability to detect comparable differences
– Differences between the wheat and oat prolamins
– Not knowing how the damage is done.
– Small numbers tested
– Short duration of tests
– Determining a viable outcome measure
• Biopsy outcome vs symptom occurrence
THE OAT CONTROVERSY
In 2004: study consensus indicates that 50g oats per day is OK for most adults, while 25g oats per day is recommended for children with CD.
– Most people did not experience symptoms or mucosal damage from oats
– A small number of people are symptomatic
– Even less develop mucosal damage

THE OAT CONTROVERSY
• OATS ARE NOT GLUTEN-FREE
• Studies all used uncontaminated oats
• Oats in Australia are contaminated
– 0.004 – 0.005% gluten (40-50 parts per million)
– Therefore OATS remain excluded from the Australian gluten-free food standard

THE OAT CONTROVERSY
Gramineae
Pooideae
Chloridiodeae
Bambusoideae
“Triticeae”
–wheat: gliadin (40-50%)
–rye: secalin (30-50%)
–barley: hordein (35-45%)
“Aveneae”
–oats: avenin (5-15%)
Panicoideae
Corn
Sorghum
Millet
Rice
THE OAT CONTROVERSY
Why are oats tolerated by most?
1. Oats contain very small amounts of damaging prolamin compared with wheat?
• They are taxonomically related to wheat but
• They only have 5-15% avenin
2. The oat prolamin itself does not contain many disease activating αα sequences that remain undigested by gut enzymes
• Wheat contains ~ 50
• Rye contains ~ 60
• Barley contains ~ 35
• Oats contain few disease activating sequences
Kagnoff M, Gastroenterology 2005;128:S10-S18
OATS; Summary
• ~15% coeliacs eating oats develop symptoms. (my unquotable figure)
• Fewer develop biopsy damage
• Finland, Sweden, Norway & the United Kingdom are consuming contaminant free oats while on a GFD.
• American Gastroenterological Society allows people to trial oats
• Currently OATS are excluded in the Australian Gluten- Free Food Standard
• Oats could be incorporated into the Low Gluten Food Standard.
OATS Summary
Some patients will be able to tolerate oats
e.g. Many asymptomatic clients
eg: IDDM, anaemic or non GI centered
How to monitor outcome?
Blood tissue transglutaminase antibodies at baseline and then
after 6 months and one year
(Freedom Foods sells and uncontaminated oat cereal)

Clinical Disorders Associated with Coeliac Disease.
• Gastrointestinal
– Liver disease
– Mouth ulcers
– IBS
– Adenocarcinoma
• Neurological
– Epilepsy
– Ataxia
– Peripheral Neuropathy
• Psychiatric
– Depression
– Schizophrenia
• Endocrine– IDDM– Infertility both sexes– Thyroid disease– Addison’s disease
• Renal– IgA nephropathy
• Locomotor– Osteopenia/porosis– Arthritis
• Dermatological– Dermatitis herpetiformis
Duggan JM. Coeliac Disease the great imitator. MJA 2004;180(10):524-526.
DERMATITIS HERPETIFORMIS
• Skin rash of itchy
blisters on elbows knees
and buttocks
• Most have coeliac
disease
• IgA deposits in the skin
• Sulpher drugs
• Gluten-free diet for life

AUTOIMMUNE THYROID
DISEASE (ATD)
The most commonly associated autoimmune
disorder
Occurs in 14-30% of patients with CD
1 in 30 adults with ATD develop coeliac disease.
People can have either hyper or hypo thyroid
disease
Research differs about whether the GFD improves
thyroid function
ATD shares a common genetic background with
CD
Velluzzi et al, Am J Gastroenterol, 1998;93:976-979 &
Larizza et al, The Journal of Pediatrics, 2001;139(5):738-740

DIABETES
IDDM highly linked with coeliac disease
Usually diabetes is diagnosed before coeliac disease
1:45-50 (2-5%) of children with IDDM will have
coeliac disease
• silent coeliac disease
• delayed growth, mild GI, low iron
1:50 adults with IDDM & 1:340 adults with NIDDM &
CD
• silent coeliac disease
• anaemia, mild GI symptoms
Begin a gluten-free diet ASAP

• IDDM children are screened for CD
• Usually less symptomatic
• Usually more issues with compliance
• ?? More relaxed diet approach
• Gluten-free foods tend to have a higher glycaemic
index
• Oats have a low glycaemic index, if tolerated
• Glucose levels require monitoring
• Insulin regime may alter
DIABETES and COELIAC DISEASE
OSTEOPOROSIS
• OSTOEPENIA, or low bone mineral density,
can lead to OSTEOPOROSIS if bone loss
continues
• Those with untreated coeliac disease have
more osteoporosis
OSTEOPOROSIS:Contributing Factors to Low Bone Mineral Content
• Abnormal biopsy
– absorption of calcium
– absorption of Vitamin D
– absorption of fatty acids
• Secondary
hyperparathyroidism
– the loss of bone mineral
– increased need for vit D
– efficiency of vitamin D
uptake receptor altered
• Lactose Intolerance
– calcium intake
• Amenorrhoea
• No exercise
• Smoking and caffeine intake
OSTEOPOROSIS:Treatment Options
• Gluten-free Diet
– may not promote re-mineralization
• slows down the progression of the disease
– vitamin D receptor works a little more
efficiently
• Exercise
– weight bearing exercise is beneficial
OSTEOPOROSIS:Treatment Options
• Hormone Replacement Therapy
– for women, this slows the progression
• Medication
– „Biphosphanates‟
• high cost
• Calcium
– 1.5g per day has been proposed for middle-
aged coeliacs
– any calcium salt supplement is acceptable if
taken for long enough

INTRODUCING GLUTEN TO BABIES
• Formulae should be gluten free
• Breast feeding is generally recommended

INTRODUCING GLUTEN TO BABIES
• Gluten is with-held from the babies diet until the age of one, if at least one parent has CD– delays the symptoms but does not prevent the disease
– hoped to prevent some babies getting coeliac disease
• At age one introduce gluten foods– look for change in bowel habit
– irritability
– signs of pain and distress
– longer-term…look for delayed growth if the child appears to be asymptomatic
Traditionally
INTRODUCING GLUTEN TO BABIES
• No current agreed upon guidelines
• Conflicting results in papers
1. Prolonged breast feeding thought to be protective
i. May decrease the amount of gluten the baby receives
ii. Breast milk protects against gastrointestinal infections
a. Infection → increased gut permiability
b. Infection → increased tTG expression
iii. Human milk IgA antibodies may decrease the immune response to ingested gluten
Recent thoughts on the issue:
Akobend AK et al. Arch Dis Child, 2006;91:39-43
Ivarsson A et al. Am J Clin Nutr, 2002;75:914-921
INTRODUCING GLUTEN TO BABIES
2. Quantity of gluten eaten should be small
i. Those diagnosed with CD had greater quantities of gluten than those without CD
ii. Avoid gluten follow-on formulaes
Recent thoughts on the issue:
Ivarsson A et al. Am J Clin Nutr, 2002;75:914-921
Fälth-Magnusson et al. Pediatr Allergy Immunol, 1996;7:1-5
Farrell RJ. JAMA, 2005;293(19):2343-2351
INTRODUCING GLUTEN TO BABIES
3. Introduce gluten between 4-9 months
• Controversial
a. Some say 4-6 months and not after 7 months
b. Others say 6-9 months
c. Agree on not before 4 months
d. Is it that gluten quantity is less when they are younger…and not the timing that is important?
Recent thoughts on the issue:
Challacombe DN et al. Arch Dis Child, 1998;79(2):198-199
Farrell RJ. JAMA, 2005;293(19):2343-2351
Ivarsson A et al. Am J Clin Nutr, 2002;75:914-921

INTRODUCING GLUTEN TO BABIES
• Introduce gluten while breast feeding–Perhaps human milk IgA antibodies decrease the
immune response to ingested gluten so it becomes better
tolerated
–Perhaps less gluten is eaten while weaning from breast
(mostly referring to absence of gluten formulaes)
Recent thoughts on the issue:
Auricchio S et al. J Paediatr Gastroenterol Nutr, 1983;2:428-433
Fälth-Magnusson et al. Pediatr Allergy Immunol, 1996;7:1-5
Ivarsson A et al. Am J Clin Nutr, 2002;75:914-921

INTRODUCING GLUTEN TO BABIES
USA suggests introducing gluten between 6-9 months as per the general population
Sweden suggests introducing gluten between 4-6 months, while the general population do this after 6 months
Australia does not have a general protocol although introducing solids to babies is now not recommended to begin until 6 months
Recent thoughts on the issue:
INTRODUCING GLUTEN TO BABIES
• The least reproducible result was the timing of the gluten introduction as the beneficial effect may be due to gluten quantity and not timing at all.
Perhaps in Australia????
– Prolonged breast feeding should be encouraged until several months after gluten has been introduced
– Gluten introduction could be between 6-9 months
– Small amounts should be introduced slowly
– Mix gluten grain foods with GF foods until well after age 1
Recent thoughts on the issue:
• The biopsy generally always returns to normal in children
• Symptomatic improvement is usually faster and more complete than adults
• GFD‟s begun before age 4, show better long-term compliance
• Early GFD‟s reduce the risk of developing associated disorders
• Early GFD‟s allow for peak bone mineral density to be obtained in teen years
CHILDREN and the GFD

COELIAC SOCIETIES
All clients should join the Coeliac Society
• Membership ~$33 per year + $35 annually
– Handbook on coeliac disease
– Ingredient List booklet
– Quarterly magazine
• The Australian Coeliac
– Restaurant card
– Recipes & food mail order pamphlets
The Coeliac Society of NSW Inc: 02 9487 5088
COELIAC SOCIETIES
• Seminars
• Cooking demonstrations / lessons
• Educational material
• Dinners
• Picnics
• Support group activities
• Recipes
• Hints about travelling
• Current research information

STRUCTURING YOUR PATIENT INTERVIEW
• Measure height and weight
1. Understand the risk factors and reasons for remaining
gluten-free for life
2. Understand why and where large and trace sources of
gluten can be found in foods and ingredients
3. Develop skills in reading and interpreting food labels.
KEY FOCI OF THE FIRST
APPOINTMENT IS 3 FOLD
READING A FOOD LABEL
• Nutritional Claim
– “Gluten-free”: no detectable gluten, AND no
oats or malt
– Australian Registered trademarks for gluten-
free
Registered trademarks owned by the
Coeliac Society of Australia Inc.

• This is the proposed Registered
trademark that will start to appear in
the USA in 2008. It will certify that the
product is glutenfree to 10ppm of
gluten. However a product will be able
to be called glutenfree at 20ppm.
Internationally recognized gluten-free
symbol.
If produced overseas and sold in Australia
it must contain no detectable gluten.
Overseas this symbol can contain Codex-
defined ingredients.
Certified
Glutenfree
GF

READING A FOOD LABEL• As of December 20th 2004, the source of all ingredients that
have been derived from a gluten containing grain must be
declared.
• Starch (wheat)
• Thickener 1422 (wheat)
• Hydrolysed vegetable grain (wheat)
• Malt (barley)
• Soy sauce (wheat)
• NB. The source does not need to be declared if it is gluten-
free. ie from maize, rice etc
• Starch
• Statements can be used instead:
• “Some ingredients are derived from gluten containing grains”
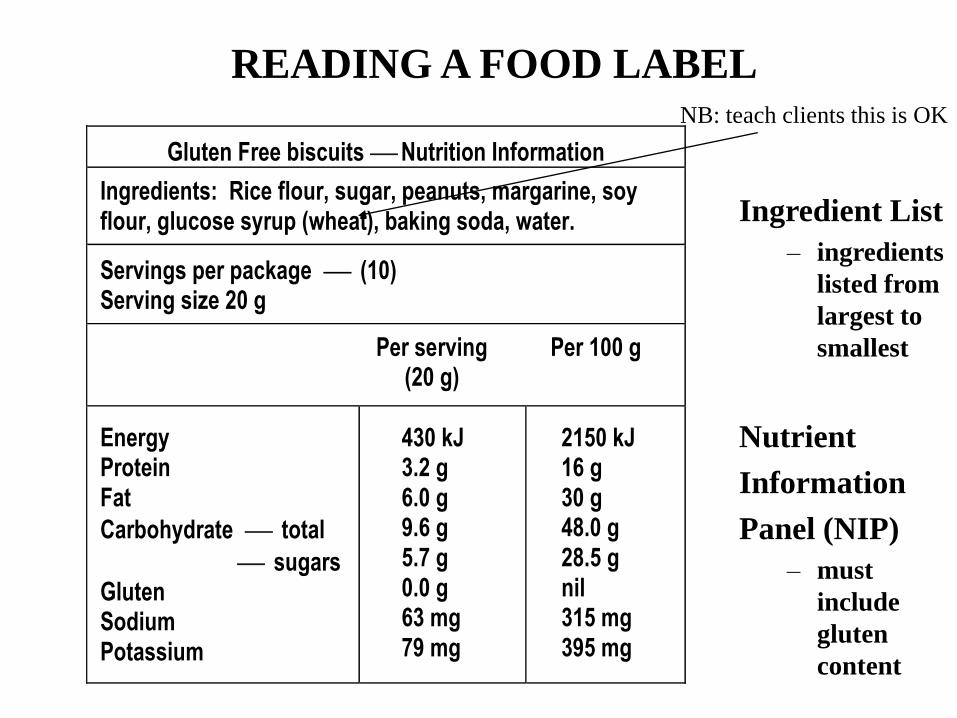
READING A FOOD LABEL
Gluten Free biscuits Nutrition Information
Ingredients: Rice flour, sugar, peanuts, margarine, soy flour, glucose syrup (wheat), baking soda, water.
Servings per package (10) Serving size 20 g
Per serving Per 100 g (20 g)
Energy Protein Fat
Carbohydrate total
sugars Gluten Sodium Potassium
430 kJ 3.2 g 6.0 g 9.6 g 5.7 g 0.0 g 63 mg 79 mg
2150 kJ 16 g 30 g 48.0 g 28.5 g nil 315 mg 395 mg
NB: teach clients this is OK
Ingredient List
– ingredients
listed from
largest to
smallest
Nutrient
Information
Panel (NIP)
– must
include
gluten
content
PRACTICAL ISSUES
• Caution when eating at restaurants
• Diet history
– suggested meal and snack substitutions
• Supplements
– iron, calcium or multi-vitamin
MEDICATIONS & SUPPLEMENTS
• Pharmaceutical companies have different labeling laws
– From July 2004 wheat starch can no longer be called gluten-free
– Active ingredients are declared
– Gluten derived excipients need to be declared
• CHECK ALL MEDICATIONS, VITAMIN & MINERAL SUPPLEMENTS AND OTHER ELIXERS PRESCRIBED.
PATIENT FOLLOW-UP
• Balancing the diet
– are gluten-free grains in the diet
• Calcium
– intake assessment
– Dx in early teens: GFD allows peak bone mass to be reached
– dietary modification
– non-dairy suggestions if required
– supplements if required
– bone mineral density scan suggestion
One month follow-up

PATIENT FOLLOW-UP
• Fibre
– GF grains/flours are lower in fibre
– suggest ways to increase dietary fibre
– Bulking agents: eg. Psyllium
• Iron
– Were they anaemic at diagnosis?
– Suggest ways to increase dietary iron
– Short-term supplement may be needed
• Folate
– Most GF food is not fortified
– Suggest ways to obtain dietary folate
– Supplements may be required
– Especially important for pregnancy
One month follow-up
PATIENT FOLLOW-UP
• After the second biopsy
– ? Frequency & severity of symptoms
– ? Biopsy improvement
– ? Coping
• Does the GFD need to be more strict?
– Assess all foods, medications and drinks
– Alter diet if symptoms persist (no column 3)
• Result of BMD scan
• Screening of family members
• ? Need Psychologist or Social Worker
Six month follow-up
PATIENT FOLLOW-UP
Required if the 6 month follow-up suggested a need: e.g still symptomatic, doctor concerned about abnormal biopsy or raised serum antibodies.
• Assess diet, drinks and medication
– Brands of food and medication
– Frequency of takeaway / restaurants
– Type of snacks
– Holy Communion wafers
– How they choose GF food items (label reading)
• Make dietary changes if gluten is found
• If no gluten is found
– Suggest possible elimination diet only if symptoms persist while GF
– Inform the doctor of status of GFD
1 year follow-up

HOSPITALIZATION ISSUES
• Know what gluten-free food is available
• Interview the patient as soon as possible
– how sensitive are they
– they may be required to bring food
• Enteral Feeds (read all labels)
– mostly gluten-free
– check the new intensive care feeds
• Oral supplements
– e.g.. Ensure and Sustagen are gluten-free