degeneration inflammation synchronisation - sgad.ch · (depression improvement across minnesota:...
TRANSCRIPT
1
Zürich, 06.04.2017 Pasquale Calabrese Professor of Clinical Neuroscience head of neuropsychology and behavioral neurology unit
Unversity of Basel, Switzerland
[email protected] https://npvn.mcn.unibas.ch
Kognitive Störungen bei Depression
neuronale Verschaltungsmuster
Zellzahl, Synapsendichte, Myelinisierung, Verschaltungsmuster, Plastizität
komplexe Kommunikations-
strukturen Sprache, Schrift, Gestik
mentale Repräsentation
Flexibilität,Theory of Mind (ToM), Zeitverarbeitung
Multiple Gedächtnissysteme
deklaratives, prozedurales, Alt- u. prospektives Ged.
emotionale Multiperspektivität
Freude, Wut, Angst, Ekel, Trauer, Überraschung,
Empathie, Ironie, (Selbst-)mitleid, Scham
Antizipation
Ironie, Humor
Empathie, Altruismus
Unser Gehirn - ein „Beziehungsorgan“...
Mehrsprachigkeit
Präferenzen
Abstr
ahie
ren
Sozialkompeten
z
Täuschen, Lügen
(Calabrese, 2017, in press)
Degeneration Inflammation
Synchronisation
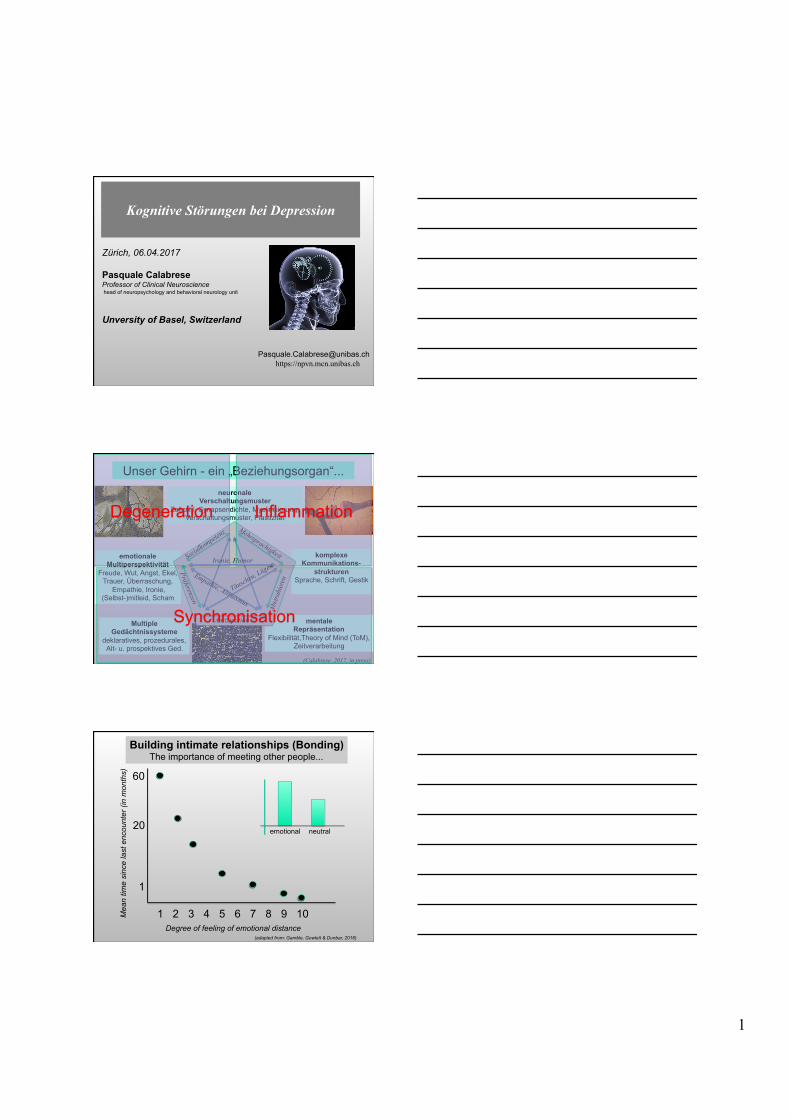
1 2 3 4 5 6 7 8 9 10 Mea
n tim
e si
nce
last
enc
ount
er (i
n m
onth
s)
Degree of feeling of emotional distance
1
20
60
(adapted from: Gamble, Gowlett & Dunbar, 2016)
Building intimate relationships (Bonding) The importance of meeting other people...
emotional neutral

2
Soziale Faktoren
Gehirn
Immun- system
(epi-)Genetik
Bedrohung
Stress
Hirnstamm- nuclei
Verhalten
Bio-Psycho-Soziale Wirkfaktoren der Depression
Vernachlässigung
dACC
Amygdala
IL-1b IL-6
TNF-a CRP
Hypothalamus
Insula
z.B. NFkB IL-1,6,8; TNF-Gene
z.B. HPAA u. SYMP-Aktivierung
z.B. somato-vegetative u. kognitive Symptome
(„Sickness Behavior“)
IL-8
negative Bewertung
Sorge ...
Angst ...
Depression
Zurückweisung
Klin. Beispiel: Depression bei MS
MS-Patienten mit aktiven coping strategien und gutem sozialen Netzwerk und psychosozialer Unterstützung haben eine insgesamt niedrigere DEP und bessere Remission … (Chwastiak et al., 2002)
Zeit
DEP
„Coping“
Diagnoseeröffnung
- „Diagnoseschock“ - Angst - Trauerreaktion
- Selbstbild - Selbstwirksamkeit - Hirnveränderungen
• Lebenszeit-Prävalenz der DEP bei MS = ~ 50 % • DEP = häufigste psychiatrische Komorbidität bei MS (Harel et al, 2007) • Hohe Assoziation mit Suizidalität (30% LZP für suiz. Absichten) (Feinstein, 2002)
• DEP in MS ist ~ 3 – 7 X höher als in d. Allgemeinbevölkerung • DEP ausgeprägter bei Patienten mit cerebraler Läsionslast als bei Pat. mit spinaler Beteiligung
(Calabrese, 2016)
3
Aufmerksamkeit
Zeitverarbeitung geistiges Tempo mentale Kontrolle
Gedächtnis Sprache
Aufmerksamkeit
geistiges Tempo
Gedächtnis
mentale Kontrolle
geistige Ermüdbarkeit
Denkverlangsamung
Abrufstörung
Einspeicherstörung
Konzentration
Schwerbesinnlichkeit
Exekutivstörung
Procrastination
Ideenversiegen
Aktiviertheit
Daueraufmerksamkeit
Rechenstörung
geteilte Aufmerksamkeit
mangelndes multi-tasking
Lerndefizit
Domänen-spezifische Beschreibungsdimensionen kognitiver Symptome bei Depression
Abrufbias
Aufmerksamkeit
Zeitverarbeitung geistiges Tempo
Gedächtnis Sprache Termine
Vereinbarungen Fachwissen
Instruktionen...
Kundenkontakte Teamwork
(Re-)Präsentation Kommunikation...
Arbeitseffizienz Aneignung neuer Techniken
zeitgebundene Aufträge evtl. Akkordarbeit...
Terminplanung Disposition
Betriebsabläufe...
Fokussierung, Detailgenauigkeit Daueraufmerksamkeit
Ablenkbarkeit (Schichtarbeit/Überstunden)...
Multi-tasking Planung von Einzelschritten
Absprache- u. Kritikfähigkeit...
mentale Kontrolle

4
ANNALS OF FAMILY MEDICINE ✦ WWW.ANNFAMMED.ORG ✦ VOL. 9, NO. 4 ✦ JULY/AUGUST 2011
305
Severity of Depression and Magnitude of Productivity Loss
ABSTRACTPURPOSE Depression is associated with lowered work functioning, including absences, impaired productivity, and decreased job retention. Few studies have examined depression symptoms across a continuum of severity in relationship to the magnitude of work impairment in a large and heterogeneous patient popula-tion, however. We assessed the relationship between depression symptom sever-ity and productivity loss among patients initiating treatment for depression.
METHODS Data were obtained from patients participating in the DIAMOND (Depression Improvement Across Minnesota: Offering a New Direction) initiative, a statewide quality improvement collaborative to provide enhanced depression care. Patients newly started on antidepressants were surveyed with the Patient Health Questionnaire 9-item screen (PHQ-9), a measure of depression symptom severity; the Work Productivity and Activity Impairment (WPAI) questionnaire, a measure of loss in productivity; and items on health status and demographics.
RESULTS We analyzed data from the 771 patients who reported being currently employed. General linear models adjusting for demographics and health status showed a signifi cant linear, monotonic relationship between depression symp-tom severity and productivity loss: with every 1-point increase in PHQ-9 score, patients experienced an additional mean productivity loss of 1.65% (P <.001). Even minor levels of depression symptoms were associated with decrements in work function. Full-time vs part-time employment status and self-reported fair or poor health vs excellent, very good, or good health were also associated with a loss of productivity (P <.001 and P = .045, respectively).
CONCLUSIONS This study shows a relationship between the severity of depression symptoms and work function, and suggests that even minor levels of depression are associated with a loss of productivity. Employers may fi nd it benefi cial to invest in effective treatments for depressed employees across the continuum of depression severity.
Ann Fam Med 2011;9:305-311. doi:10.1370/afm.1260.
INTRODUCTION
Depression is prevalent and incurs substantial indirect costs associ-ated with reduced work functioning, including absences, impaired productivity, and even decreased job retention across a wide
variety of occupations.1-4 In addition, several studies have shown that even minor or subthreshold depression (including dysthymia) is related to poorer work performance.5,6 Fewer studies have examined depression symptoms across a continuum of severity in relationship to the magnitude of work loss that includes both absences and impaired productivity. Simon et al7 found that among outpatients treated for bipolar disorder, depression severity was strongly and consistently associated with a decreased proba-bility of employment and more days of absence due to illness. Backenstrass et al8 characterized a spectrum of depressive symptoms across 3 increasing levels of severity (nonspecifi c, minor, and major) and found an increas-ing number of days of absence due to illness with each additional level of
Arne Beck, PhD1,2
A. Lauren Crain, PhD3
Leif I. Solberg, MD3
Jürgen Unützer, MD, MPH4
Russell E. Glasgow, PhD5
Michael V. Maciosek, PhD3
Robin Whitebird, PhD, MSW3
1Kaiser Permanente, Denver, Colorado
2Department of Family Medicine, Univer-sity of Colorado Denver Health Sciences Center, Denver, Colorado
3HealthPartners Research Foundation, Minneapolis, Minnesota
4University of Washington, Seattle, Washington
5National Cancer Institute, Washington, DC
Confl icts of interest: authors report none.
CORRESPONDING AUTHOR
Arne Beck, PhDKaiser PermanenteInstitute for Health ResearchPO Box 378066Denver, CO [email protected]
ANNALS OF FAMILY MEDICINE ✦ WWW.ANNFAMMED.ORG ✦ VOL. 9, NO. 4 ✦ JULY/AUGUST 2011
308
DEPRESSION SEVERIT Y AND PRODUC TIVIT Y LOSS
the 10-point scale, representing 35.2% of total hours worked, or 12.1 hours of productivity affected while at work. The proportion of expected work time that was missed or affected because of health problems over the previous 7 days (pro-ductivity loss) represented an average of 37.8% of employees’ usual work hours, or 14.2 hours of work missed or work time impaired because of health. Note that the value of productivity loss as calcu-lated (and described in the Methods sec-tion) is not the sum of absenteeism plus presenteeism, because the latter includes only hours actually at work.
Relationship Between PHQ-9 and WPAIFigure 1 graphically shows the relation-ship between each category of depres-sion symptom severity, as assessed with the PHQ-9, and productivity loss. It illustrates the strong linear relationship between depression symptom sever-ity and the combination of work loss and productivity impairment. It also shows that even minor symptoms were associated with a considerable loss of productivity.
The overall multivariate model for productivity loss containing all covari-ates was signifi cant, and the included variables explained 10.5% of the vari-ability among patients in this outcome (F = 10.26, P <.001, model R2 = .105). Table 4 displays the individual variables in the model. There was a positive and signifi cant association between PHQ-9 scores and productivity loss, with each 1-point increase in score associated with an additional 1.65% loss of productivity (P <.001). In addition, full-time vs part-time employment status and fair or poor health vs excellent, very good, or good health were also associated with greater productivity loss (P <.001 and P = .045, respectively).
Because our sample of 771 employed individuals represented only 66% of those with complete baseline data for this analysis, we conducted a subanalysis to determine whether employment status was related to depression severity among all working-age partici-pants, defi ned as those aged 18 to 64 years. Results indicated that mean PHQ-9 scores were higher among the 325 study participants reporting no employment
(mean = 13.30, SD = 4.90) than among the 757 study participants reporting full- or part-time employment (mean = 12.17, SD = 4.31) (t = 3.62, df = 549.2, P <.001).
DISCUSSIONBaseline data from this large sample of patients dem-onstrate a linear, monotonic relationship between depression symptom severity and productivity loss;
Table 4. Relationship of Depression Severity (PHQ-9 Score), Demographics, and Health Status to Productivity Loss
Parameterβ
Coeffi cient Error t Value P Value
PHQ-9 scorea 1.65 0.24 6.98 <.001Age 0.006 0.08 0.07 .94Sex (male) 1.89 2.32 0.82 .41Race/ethnicity (minorityb) 3.36 3.30 1.02 .31Health (fair/poor) 4.80 2.39 2.01 .045Education (high school or less) –1.44 2.30 –0.62 .53Employment status (part time) –9.85 2.60 –3.79 <.001Marital status (not coupledc) 3.73 2.06 1.81 .07
PHQ-9 = Patient Health Questionnaire 9-item screen.
Notes: The model had an estimated intercept of 36.50 and an error of 1.74. Positive estimates indicate loss of productivity; negative estimates indicate gain of productivity. Productivity loss is defi ned as the combination of absenteeism (percent of time missed in the past 7 days due to health) and presenteeism (percent impairment at work in the past 7 days due to health). These measures were obtained from the Work Productivity and Activity Impairment (WPAI) questionnaire.
a The general linear model shows the relationship between PHQ-9 score and productivity loss adjusted for all other variables listed in the table.b Combination of Hispanic ethnicity and non-white race categories listed in Table 2.c Divorced, separated, widowed, or never married.
Figure 1. Productivity loss (absenteeism and presenteeism combined) by PHQ-9 score at enrollment: percent of work time missed or impairment at work in past 7 days.
PHQ-9 = Patient Health Questionnaire 9-item screen.
Note: For comparison, the norm for productivity loss for individuals without depression or other chronic conditions is 8.0%.
0
10
20
30
40
50
60
29.6
38.0
46.9
51.3
7-9 10-14 15-19 ≥20
PHQ-9 score at enrollment
Perc
ent
„Work-Productivity“ – aus Sicht des Betroffenen
„Work-Productivity“ – aus Sicht des Arbeitgebers

5
0102030405060708090
100
25%
klinischer
Eindruck
73%
Screening
92%
Testbatterie
<10 min.
% W
ahrsc
heinl
ichke
it eine
ko
gnitiv
e Dys
funkti
on zu
erke
nnen
Gifford & Cummings (1999)
>30 min.
zeigen sich Kognitive Störungen im klinischen Eindruck?
Kognitive
Signatur der
Depression
050100150200250300350400450
ohne Ton mit Ton mit Ton ohne Ton
Ctrl.DEPFTDSCHold
Aufmerksamkeit
1
35
79
1113
15
1. T
rial
2. T
rial
3. T
rial
4. T
rial
5. T
rial
List
B
6. T
rial
dela
y
ADDEPRCTRL
Gedächtnis
**
A,B,C... 1,2,3...
1A,2B,3C...
mentale Kontrolle geistiges tempo
Kognitiver Depressions-Index (CODEX) (Prof. Dr. P. Calabrese & Prof. Dr. G. Hasler)
Vorlesen einer 10-gliedrigen Wortliste: VersA, SchadenB, ZeitA, ÄrgerB, SchrittA, SorgeB, GlanzA, WundeB, LobA, LastB Pkte:___
Aufmerksamkeit a) Geteilte Aufmerksamkeit Verlieren Sie bei einer Unterhaltung mit mehreren Personen schnell den Faden? b) Daueraufmerksamkeit Fällt es Ihnen schwer, sich über einen längeren Zeitraum mit einem Thema zu beschäftigen? c) Konzentration Sind Sie leicht ablenkbar? d) Aktiviertheit Reagieren Sie prompt, wenn man Sie anspricht? Gedächtnis a) Einspeicherstörung Müssen Sie eine Information mehrfach hören oder lesen, bis Sie diese verstanden haben? b) Lerndefizit Bereitet es Ihnen Mühe, sich an Ereignisse vom Vortag zu erinnern? c) Abrufstörung Haben Sie Schwierigkeiten, sich an die Bedeutung bestimmter Begriffe oder Dinge zu erinnern? d) Abrufbias Erinnern Sie unangenehme Ereignisse besser als angenehme? Mentale Kontrolle a) Rechenstörung Bereitet Ihnen das Kopfrechnen Mühe? b) mangelndes Multi-Tasking Haben Sie Schwierigkeiten, mehrere Dinge gleichzeitig zu erledigen? c) Exekutivstörung Bereitet es Ihnen Probleme, die Einzelschritte einer Aufgabe bei der Ausführung zu berücksichtigen? d) Prokrastination Neigen Sie dazu, Dinge, die Sie zu erledigen haben, aufzuschieben? Geistiges Tempo a) geistige Ermüdbarkeit Strengen Sie geistige Tätigkeiten wie Lesen, Schreiben oder Zuhören an? b) Denkverlangsamung Benötigen Sie mehr Zeit als üblich, um über etwas nachzudenken? c) Schwerbesinnlichkeit Strengt es Sie an, sich einzelne Details einer Sache oder eines Ereignisses vorzustellen? d) Ideenversiegen Haben Sie Mühe, einen Gedanken zu formulieren oder über einen längeren Zeitraum festzuhalten?
JA NEIN
Abfrage der 10-gliedrigen Wortliste: VersA, SchadenB, ZeitA, ÄrgerB, SchrittA, SorgeB, GlanzA, WundeB, LobA, LastB Pkte:___ Gesamtzahl erinnert:___ negativ Bias (WorteA/WorteB):____
Cognitiver Depressions-Index (CODEX)

6
Aufmerksamkeit
Gedächtnis geistiges Tempo
Mentale Kontrolle
*
*
*
*
*
*
* * * * * *
*
*
*
*
Die CODEX-dimensionen
Attention
memory mental speed
mental control
*
*
*
*
*
*
* * * * * *
*
*
*
*
Aufmerksamkeit
Gedächtnis geistiges Tempo
Mentale Kontrolle
*
*
*
*
*
*
* * * * * *
*
*
*
*

7
Aufmerksamkeit
Gedächtnis geistiges Tempo
Mentale Kontrolle
*
*
*
*
*
*
* * * * * *
*
*
*
*
Aufmerksamkeit
Gedächtnis geistiges Tempo
Mentale Kontrolle
*
*
*
*
*
*
* * * * * *
*
*
*
*
Aufmerksamkeit
Gedächtnis geistiges Tempo
Mentale Kontrolle
*
*
*
*
*
*
* * * * * *
*
*
*
*

8
Vers Schaden
Zeit Ärger Schritt Sorge Glanz Wunde
Lob Last
Vers
Zeit
Schritt
Glanz
Lob
Schaden
Ärger
Sorge
Wunde
Last
Vers Schaden
Zeit Ärger Schritt Sorge Glanz Wunde
Lob Last
1 2 3 4 5 6 7 8 9
10 7,85
4,5 3,7
5,75
2,18
3,43
total positive negative total positive negative
CTRL (n=42)
DEP (n=16)
*

9
Kognitiver Depressions-Index (CODEX) (Prof. Dr. P. Calabrese & Prof. Dr. G. Hasler)
Vorlesen einer 10-gliedrigen Wortliste: VersA, SchadenB, ZeitA, ÄrgerB, SchrittA, SorgeB, GlanzA, WundeB, LobA, LastB Pkte:___
Aufmerksamkeit a) Geteilte Aufmerksamkeit Verlieren Sie bei einer Unterhaltung mit mehreren Personen schnell den Faden? b) Daueraufmerksamkeit Fällt es Ihnen schwer, sich über einen längeren Zeitraum mit einem Thema zu beschäftigen? c) Konzentration Sind Sie leicht ablenkbar? d) Aktiviertheit Reagieren Sie prompt, wenn man Sie anspricht? Gedächtnis a) Einspeicherstörung Müssen Sie eine Information mehrfach hören oder lesen, bis Sie diese verstanden haben? b) Lerndefizit Bereitet es Ihnen Mühe, sich an Ereignisse vom Vortag zu erinnern? c) Abrufstörung Haben Sie Schwierigkeiten, sich an die Bedeutung bestimmter Begriffe oder Dinge zu erinnern? d) Abrufbias Erinnern Sie unangenehme Ereignisse besser als angenehme? Mentale Kontrolle a) Rechenstörung Bereitet Ihnen das Kopfrechnen Mühe? b) mangelndes Multi-Tasking Haben Sie Schwierigkeiten, mehrere Dinge gleichzeitig zu erledigen? c) Exekutivstörung Bereitet es Ihnen Probleme, die Einzelschritte einer Aufgabe bei der Ausführung zu berücksichtigen? d) Prokrastination Neigen Sie dazu, Dinge, die Sie zu erledigen haben, aufzuschieben? Geistiges Tempo a) geistige Ermüdbarkeit Strengen Sie geistige Tätigkeiten wie Lesen, Schreiben oder Zuhören an? b) Denkverlangsamung Benötigen Sie mehr Zeit als üblich, um über etwas nachzudenken? c) Schwerbesinnlichkeit Strengt es Sie an, sich einzelne Details einer Sache oder eines Ereignisses vorzustellen? d) Ideenversiegen Haben Sie Mühe, einen Gedanken zu formulieren oder über einen längeren Zeitraum festzuhalten?
JA NEIN
Abfrage der 10-gliedrigen Wortliste: VersA, SchadenB, ZeitA, ÄrgerB, SchrittA, SorgeB, GlanzA, WundeB, LobA, LastB Pkte:___ Gesamtzahl erinnert:___ negativ Bias (WorteA/WorteB):____
Cognitiver Depressions-Index (CODEX)
• Biopsychosoziale „Transduktionstheorien“ der Depression postulieren einen Zusammenhang zwischen (epi-)genetisch veränderter ZNS-Immuno- bzw. hormoneller Interaktion und Umwelt bei der Entstehung/Aufrechterhaltung der Depression.
• Depressionen sind mit bestimmten funktionellen und strukturellen Netzwerken/Veränderungen im Gehirn assoziiert.
• „Kognitive Signatur“ der Depression : Aufmerksamkeit, Gedächtnis, geistiges Tempo, mentale Kontrolle.
• Kognitive Störungen wirken sich auf das Alltagsleben (u. Produktivität) der Betroffenen aus.
• Kognitive Störungen können dem “klinischen Eindruck” entgehen. Pat. sollten gezielt untersucht werden.
Take home...