definition of dementia a global impairment of higher cortical functions including memory, capacity...
TRANSCRIPT

Definition of Dementia
• A global impairment of higher cortical functions including memory, capacity to solve problems of daily living, performance of learned perceptuomotor skills, correct use of social skills and control of emotional reactions. No clouding of consciousness. The course is often irreversible and progressive.
Royal College of Physicians, 1980

Dementia Diagnoses in the US
55%
14%
2%
13%
15%1%
Alzheimer's Disease
Vascular Dementia
Lewy Body Dementia
Mixed (AD + VAD)
Mild CognitiveImpairmentOther


Classification of Dementia
Subcortical• Presence of motor symptoms
Hypo- or hyperkinetic Dysarthria
• Slow motor speed and information processing
• Impaired planning and problem solving
• Depression, apathy, withdrawal• No aphasia, apraxia, agnosia• Basal ganglia, mesencephalon,
thalamus affectedExamples: Parkinson’s disease;
Huntington’s disease
Cortical• No motor symptoms (early)
• Processing speed normal (early)
• Amnesia, aphasia, apraxia, agnosia
• Impaired new learning
• Mood usually unaffected
• Behavior can be odd or unusual (FLD or later in AD)
• Involvement of basal forebrain, hippocampus and cortex
Examples: Alzheimer’s disease; Pick’s disease; Lewy Body dementia




18FDOPA-PET, Brooks 1993
PD: Progression of disease with decrease in striatal 18FDOPA uptake


Huntington’s disease
• Autosomal dominantly inherited
• Unstable and expanded CAG trinucleotide repeat in the IT15 gene on chromosome 4
• Symptoms are movement disorder and dementia
• Slowly progressive, resulting in death 10-20 years after symptom onset


Dopaminergic function in Huntington’s
Turjanski, 2000
18F- dopa 11C-raclopride

Huntington’s disease
Symptomaticcarrier
Asymptomaticcarrier
Asymptomaticcarrier
PSI, 1997
CMRglc
D2/D3

HD - Asymptomatic gene carrier
PSI, 1997
18F-FDG 11C-Raclopride
1. Scan
2. Scan(30 Months)

MOVEMENT DISORDER ATLAS






Pick Bodies







1992AHCPR
develops screening guidelines
for AD
7th century BC
Age-related mental
deterioration recognized
~200 AD
Galen associates “morosis” (dementia)
with old age
700 BC
2000 AD
1980Alzheimer
’sAssociatio
nestablishe
d
Early 1960sAwareness of AD as a
single disease
1907AD first
described by Dr. Alois
Alzheimer
AD—History TimelineAD—History Timeline
1978?Single entity established—
senile dementia of
the Alzheimer’s type (SDAT)
1983Cholinergi
cdeficit
identified
1991APOE
implicated
1994Brain
inflammatory response identified
as pathogenet
ic
Research into
treatments
continues
1993First
cholinesterase inhibitor approved


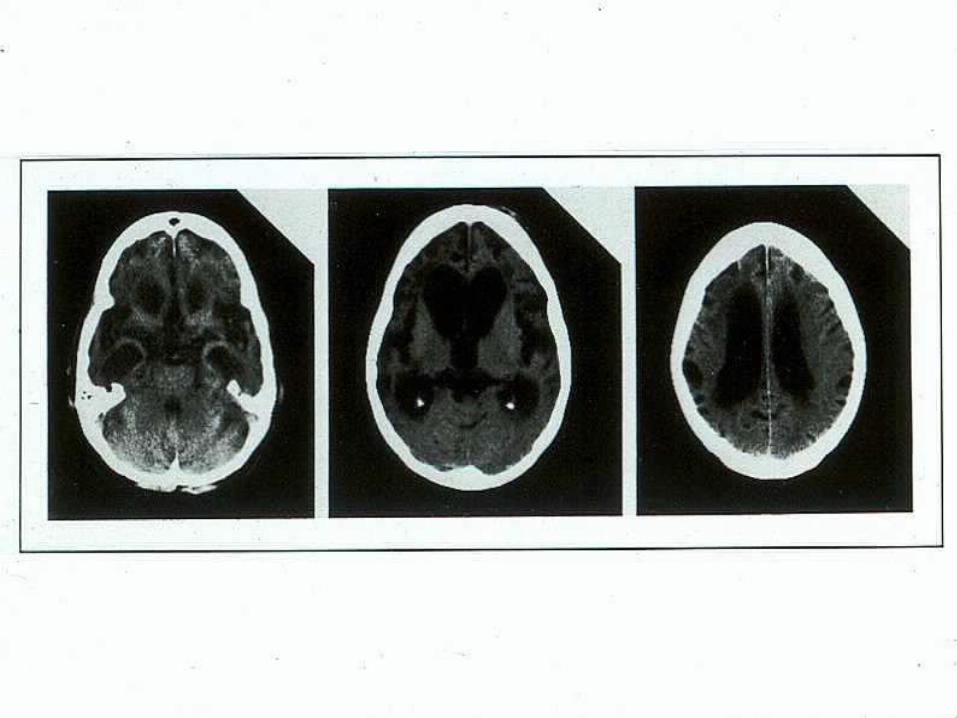
•Gross atrophy
shrinkage of brain
thinning of gyri
widened sulci
Macro Pathology of the Alzheimer Brain

Rate of brain atrophy in Alzheimer’s disease
+ 11 months
MRI, Fox 1996
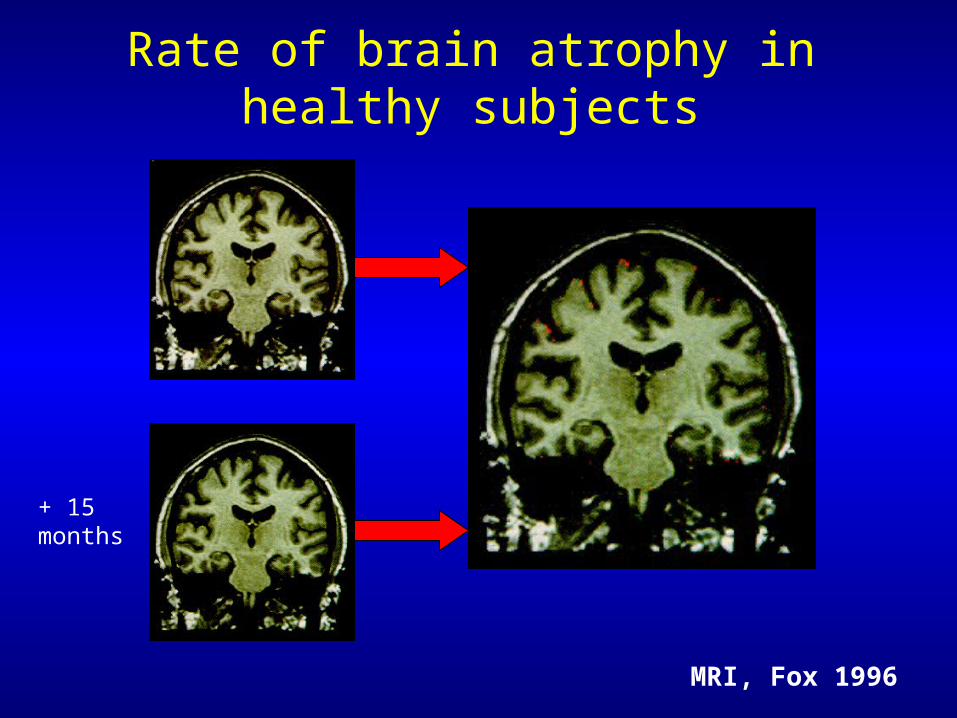
Rate of brain atrophy in healthy subjects
MRI, Fox 1996
+ 15 months


Normal AD
Temporal-Parietal Hypofunction in AD
Temporal-Parietal Hypofunction in AD

Micro Pathology of the Alzheimer Brain
Senile Plaque
Contain A peptide
Neuron with Neurofibrillary Tangles
Selkoe





Disease Gene vs Risk-factor Gene
Age at onset Genetic Component of Disease Mutation frequency Inheritance Individual effect Population effect
Early onset Mutation associated with the disease Rare Mendelian Major Weak
Late onset Mutation associated with increased risk Frequent Complex Weak Major
Interaction with environmental factors
Weak Major
Disease Gene Risk-factor Gene



APOE 65%
? 30%
PS-2 0.1%
PS-1 3%
APP 0.4%
? 1%
Distribution of Alzheimer's disease forms and related genetic susceptibility factors
From Richard and, Amouyel, 2001
Autosomal Dominant mutation cases (<5%)
Sporadic cases (>95%



Possible Mechanismsin the Pathogenesis of AD
Tangles Plaques
Inflammatory response
Neuronal injury/death
Oxidativestress
Environmental and genetic factors
Dementia

INTERMISSION



What is MCI?• Common precursor to AD
• Emerging criteria– Memory test scores 1 SD below age-
adjusted normals– No significant objective loss of function– Do not meet diagnostic criteria for
dementia• 12% per year convert from MCI to AD in 4
years
• Treatments are under investigation
• Common precursor to AD
• Emerging criteria– Memory test scores 1 SD below age-
adjusted normals– No significant objective loss of function– Do not meet diagnostic criteria for
dementia• 12% per year convert from MCI to AD in 4
years
• Treatments are under investigation

MRI, NRU 2001
MCI-Cerebral atrophy
MCI patient, MMSE=27 Healthy volunteer
Age 83 years Age 65 years

Clinical Progression of AD and MCI
Clinical Progression of AD and MCI
Cognit
ive f
unct
ion
•Forgetfulness
•Repetitive questions
•Daily function impaired
•Progression of cognitive deficits
•Short-term memory loss
•Word-finding difficulties
•Agitation
•Altered sleep patterns
•Total dependence: dressing, feeding, bathing
MCIMMSE 24–30 Mild AD
MMSE 20–23
Moderate AD
MMSE 10–19
Severe ADMMSE 0–9
•Mild subjective/objective memory loss
•Normal function
10 y0 yTime (y)
Time?

Natural history of Alzheimer’s disease
1 2 3 4 5 6 7 8 9
0
5
10
15
20
25
30
Time (years)
Symptoms
Diagnosis
Loss of functional independence
Behavioural problems
Nursing home placement
Death
Min
i-M
enta
l Sta
te E
xam
inat
ion
(M
MS
E)
Early diagnosis Mild-to-moderate Severe
Reproduced from Feldman and Gracon, 1996
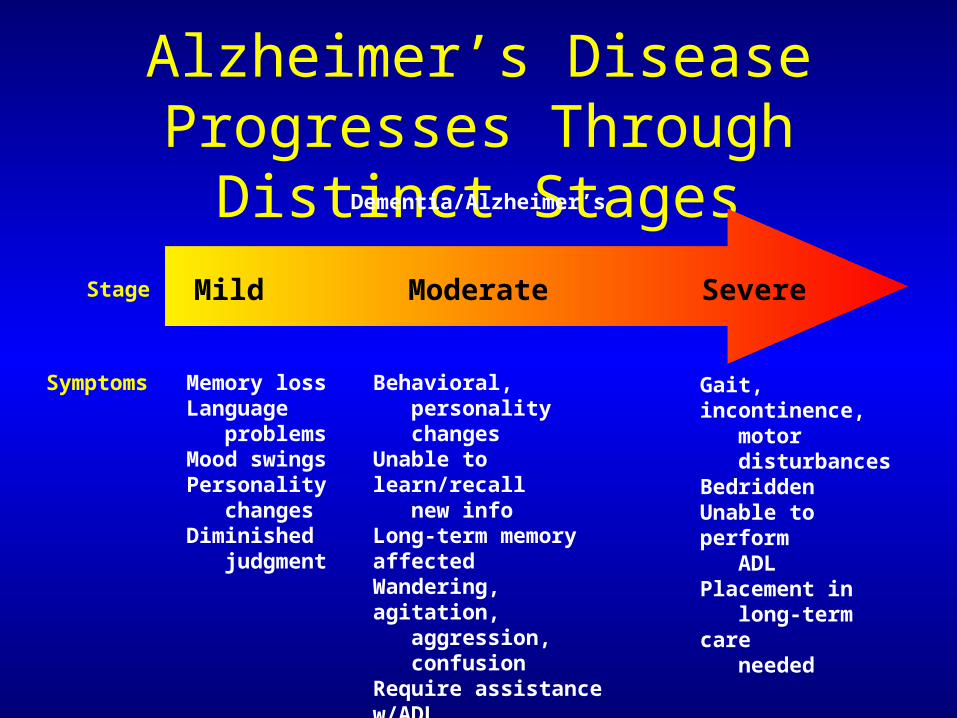
Alzheimer’s Disease Progresses Through Distinct Stages
Mild Moderate Severe
Memory lossLanguage problemsMood swingsPersonality changesDiminished judgment
Behavioral, personality changesUnable to learn/recall new infoLong-term memory affectedWandering, agitation, aggression, confusionRequire assistance w/ADL
Gait, incontinence, motor disturbancesBedriddenUnable to perform ADLPlacement in long-term care needed
Dementia/Alzheimer’s
Stage
Symptoms

Correlation between Correlation between Cognition and ADLsCognition and ADLs
MMSE score25 20 15 10 5 0
KEEP APPOINTMENTSKEEP APPOINTMENTS
TELEPHONETELEPHONE
OBTAIN MEAL / SNACKOBTAIN MEAL / SNACK
TRAVEL ALONETRAVEL ALONE
USE HOME APPLIANCEUSE HOME APPLIANCE
FIND BELONGINGSFIND BELONGINGS
SELECT CLOTHESSELECT CLOTHES
DRESSDRESS
GROOMGROOM
MAINTAIN HOBBYMAINTAIN HOBBY
DISPOSE LITTERDISPOSE LITTER
CLEAR TABLECLEAR TABLE
WALKWALK
EATEAT
Loss of optimal(independent) performance
25% 75%
AD
L
Each bar from left to
right represents the
range of MMSE
scores over which
25–75% of
Alzheimer’s
patients in one
study† showed loss
of optimal
(independent)
ADL performance
†Galasko et al. Alzheimer Dis Assoc Disord 1997;11(Suppl 2):S33–S39



Behavioral Disturbances in Alzheimer’s Disease and Other
Dementias
“Alzheimer’s disease is the most widely encountered cause of psychiatric pathology associated with a specific neuropathologic substrate”
Merriam et al, JAGS 36: 7-12, 1988

Behavioral Symptoms in Alzheimer’s Disease
• Most common reason for institutional placement
• In study by Cummings et al, only 12% of
patients did not have a behavioral problem.
• Most common reason for caregiver distress Caregiver distress ratings correlate highly (r
= .88) with behavioral disturbances

Behavioral Symptoms in Alzheimer’s Disease
Personality Changes:
Apathy: Most common behavioral change
Decreased motivation, indifference
Associated with frontal hypoperfusion (medial frontal, supraorbital, anterior frontal areas)
Not related to depressionCummings 1998

Behavioral Symptoms in Alzheimer’s Disease
Delusions:
Cross sectional studies: 20-50% Longitudinal studies: 50-70%
Common Delusions: theft, infidelity, Capgras, phantom boarder, picture sign
Associated with decreased metabolism in
frontal lobesCummings 1998

Psychotic symptoms in Alzheimer’s disease
• Delusions 44%• Persecutory 73%
• Reference 15%• Jealousy 9%
• Misidentification 30%• Not home 51%
• Strangers 29%
• Reflection is Someone Else 21%
• Hallucinations 24%• Visual 85%
• Auditory 45%
• Tactile 3%
Deutsch et al

Behavioral Symptoms in Alzheimer’s Disease
Depression: Depressive symptoms are frequent
Major depressive disorder (MDD) is uncommon
More common with positive family or personal history
MDD may precede diagnosis of Alzheimer’s disease or vascular dementia
Cummings 1998

Behavioral Symptoms in Alzheimer’s Disease
Agitation: Correlates with anxiety in mild patients
Correlates with psychosis in moderately demented
patients
Correlation unclear in severely demented patients
Associated with decrease in fronto-temporal metabolism on imaging studies
Cummings 1998





Cholinergic System of the Human Brain
Basal Forebrain
Hippocampus
Occipital Cortex
Parietal Cortex
Frontal Cortex

The Basal Forebrain Cholinergic System Enables or Gates Important CNS Functions
Cerebral Blood Flow
Cognitive Function
BF
Basal Forebrain Cholinergic
Neurons

Acetyl CoA+
Choline
Acetylcholine
N receptor
Action of ACh at pre- and postsynaptic nerve terminals and its removal by AChE
Presynaptic nerve terminal
Postsynaptic nerve terminal
CAT
CAT = choline acetyltransferase
AChE = acetylcholinesterase
N = nicotinic
M = muscarinic
N receptor
M receptor
M receptor
= acetylcholine
AChE AChE

VIDEO

Cholinergic deficits in Alzheimer’s disease
• Reduction in the activity of choline acetyltransferase, which synthesises ACh(1)
• Reduction in the number of cholinergic neurons in the basal forebrain(2)
• Reduction in the number of nicotinic receptors(3)
Refs: (1)Bartus et al, 1982 (2)Whitehouse et al, 1982 (3)Sihver et al, 1999

Nicotinic acetylcholine receptors (nAChR) in the brain
42 nAChR subtype-High affinity
• Pre- and postsynaptic nAChR(3)
• Major excitatory neuronal nAChR(3)
7 nAChR subtype-Low affinity
• Predominantly presynaptic nAChR(1)
• Generates fast calcium currents(1)
• Affects release of glutamate, 5HT, ACh(2)
(1)Albuquerque et al, 1997; Maelicke et al, 1998; Strange, 1992 (2)Alkondon et al, 1996
(3)Clarke et al, 1985

Acetylcholine activates pre- and postsynaptic 7 nicotinic receptor
Presynaptic nerve terminal
Postsynaptic nerve terminal
Glutamate
Acetylcholine
Glutamate receptor
7 nicotinic receptor
The 7 receptor, present at pre- synaptic termini, controls ACh release and mayalso modulate release of glutamate

Nicotinic cholinergic neuron density in different populations
Middle-agedcontrols
Age-matched controls
Patients with AD
Density of nicotinic cholinergic neurons/mm3
7600 4000 1000
0
1000
2000
3000
4000
5000
6000
7000
8000

Wevers et al, 1999
4 and 7 mRNA expressing neurons associated with -amyloid plaque
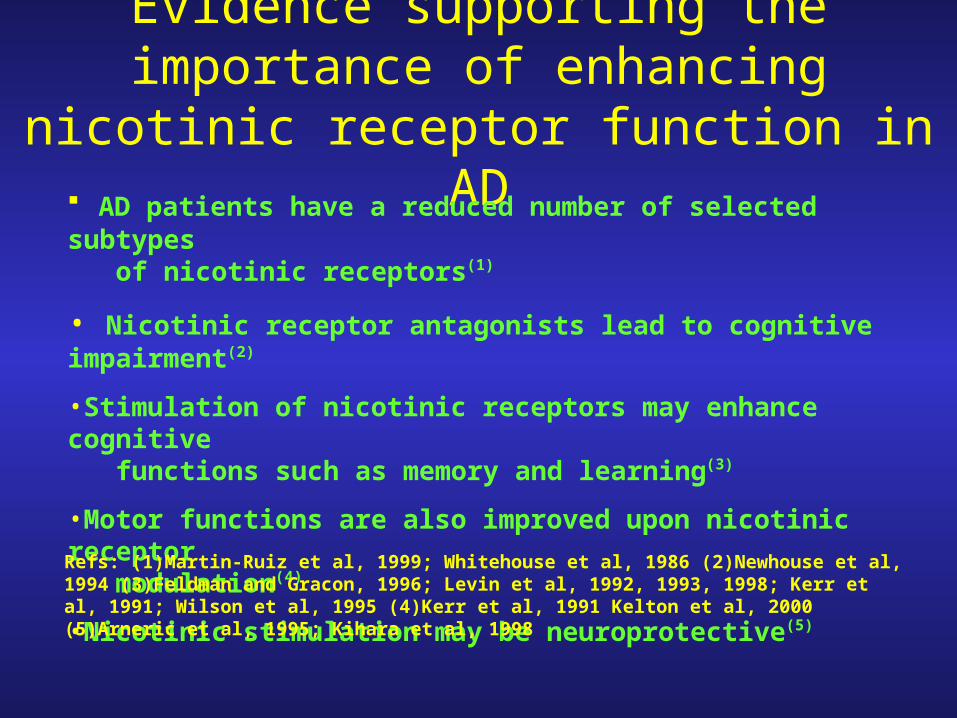
Evidence supporting the importance of enhancing nicotinic receptor function in AD
AD patients have a reduced number of selected subtypes of nicotinic receptors(1)
• Nicotinic receptor antagonists lead to cognitive impairment(2)
•Stimulation of nicotinic receptors may enhance cognitive functions such as memory and learning(3)
•Motor functions are also improved upon nicotinic receptor modulation(4)
•Nicotinic stimulation may be neuroprotective(5)
Refs: (1)Martin-Ruiz et al, 1999; Whitehouse et al, 1986 (2)Newhouse et al, 1994 (3)Feldman and Gracon, 1996; Levin et al, 1992, 1993, 1998; Kerr et al, 1991; Wilson et al, 1995 (4)Kerr et al, 1991 Kelton et al, 2000 (5)Arneric et al, 1995; Kihara et al, 1998

Acetyl CoA+
Choline
M receptor N receptor
Primary Strategy for increasing cholinergic function: block acetylcholinesterase
ACh
Presynaptic nerve terminal
Postsynaptic nerve terminal
CAT
Acetylcholinesterase
Choline +acetate
Acetylcholine (ACh) AChEI (donepezil, rivastigminegalantamine)
AChEI = acetylcholinesterase inhibitors

Primary medication treatment of AD (secondary prevention)
• Cholinesterase inhibitors are the mainstay of therapy
• Two drugs currently on the market (Aricept and Exelon); one about to be launched (Reminyl)
• Though some patients experience immediate improvement, most prominent effect is cognitive stabilization
• Functional improvement follows cognitive enhancement or stabilization
• Positive effects of these agents appear to be sustained

Pharmacological Comparison of Pharmacological Comparison of Aricept, ReminylAricept, Reminyl®® and Exelon and Exelon®®
Aricept Reminyl Exelon
Chemical class Piperidine Alkaloid Carbamate
Mechanism Reversible Reversible Pseudo-irreversible
Half-life ~70 h 5.8 h ~2 h*
Hepatic monitoring No No No
Dosing qd bid bid
*Apparent long duration of action (~10 h) due to slow-binding and time-dependent inhibitory kinetics of carbamates

Aricept 30-week, Phase III trials
ADAS-cog ResultsADAS-cog Results
Study week Placebowashout
Clinical improvement
Clinical decline
4.00
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
–0.5
–1.0
–1.5
–2.0
–2.5
6 12 18 30Endpoint
US Study† Multinational Study‡
Placebo
Aricept:
5 mg/day
10 mg/day
** ********
****
****
****
**
**
ITT-LOCF analysis; **p0.001 for Aricept versus placebo†Rogers et al. Neurology 1998;50:136–145; ‡Burns et al. Dement Geriatr Cogn Disord 1999;10:237–244
Le
ast
sq
ua
res
me
an
ch
an
ge
fro
mb
ase
line
(±S
E)
**

Raskind Trial: Mean (± SE) Change From Baseline in ADAS-cog
MonthsMonths
Mean (± SE) Mean (± SE) Change Change From From
Baseline in Baseline in ADAS-cogADAS-cog
ScoreScore
*P < .001 vs placebo.
Raskind et al. Neurology. 2000.
Placebo (n = 157)
Reminyl® 32 mg (n = 117)
Reminyl® 24 mg (n = 131)
3
2
1
0
–1
–2
–3
–4 ImprovementImprovement
DeteriorationDeterioration
1 2 4 5 63
4
**

Raskind et al. Neurology. 2000.
Raskind Trial: Mean (± SE) Change From Baseline in ADAS-cog
Open-ExtensionOpen-ExtensionDouble-blindDouble-blind
Reminyl® 24 mg/Reminyl® 24 mg(n = 212/116)
Historical placebo group
*P < .05 vs placebo/Reminyl®
and not statistically different from baseline.
ImprovementImprovement
DeteriorationDeterioration0 3 6 9 12
Mean (± SE)Mean (± SE)Change From Change From Baseline inBaseline inADAS-cogADAS-cog
ScoreScore
–4
–3
–2
–1
0
1
2
3
45
6
7
MonthsMonths
Placebo/Reminyl® 24 mg (n = 213/135)
*

Caregiver Time in AD• As AD progresses, caregivers provide more
assistance to patient with dressing, feeding, bathing and management of incontinence1
• Estimated time spent by caregivers of severe AD patients on caregiving activities2:– 10 hours per day– 290 hours per month
1. Mace et al; 2. Max, et al. 1995.

Mean Change in Daily Time Spent by Caregiver Assisting With ADL at 6 Months: The Wilcock
Study
*P < .05 vs baseline.
Placebo (n = 160)
Galantamine 24 mg/d(n = 165)
–50
–40
–30
–20
–10
0
10
20
30
Change From Change From Baseline in Baseline in Daily Time Daily Time
Spent Spent Assisting Assisting
With ADLWith ADLat 6 Months at 6 Months
(min)(min)
*

† Weeks from the beginning of the double-blind studyFriedhoff et al. Int J Neuropsychopharmacol 1999;2(Suppl 1):S175
Long-Term Open Label Treatment of AD
AD
AS
-Co
g M
ea
n c
ha
ng
e f
rom
b
ase
line
(±S
E)
Study week†
No. ofsubjects: 133 124 100 56 46 37 34 28 25
36
30
24
18
12
6
0
–6
0 26 50 74 98 122 146 170 194
Aricept-treated patients
95% confidence interval
Clinical improvement
Clinical decline
Decline in ADAS-cog score (9–11 pointsper year) based on the natural history of untreated patients with moderate AD†

12 mg/day (6 mg bid)
9 mg/day (4.5 mg bid)6 mg/day (3 mg bid)
4 mg/day (2 mg bid)
Anticholinesterase Dose Titration Anticholinesterase Dose Titration ScheduleSchedule
Aricept 5 mg/day (od)
4 mg bid
0 6 12 18Weeks
8 mg bid12 mg bid (optional)
10 mg/day (od) according to individual patient requirements
Exelon
Reminyl

Reminyl (galantamine) has an allosteric modulatingaction at nicotinic receptors
Postsynaptic nerve terminal
M receptor N receptor
Presynaptic nerve terminal
ACh
ACh
galantamine
N = nicotinic
M = muscarinic
ACh = acetylcholine

Summary of Cholinergic Pathology and Therapy in AD
• Alzheimer’s disease is associated with impairment of the cholinergic nervous system(1)
• This leads to: – decrease in ACh(1)
– decrease in specific subtypes of nicotinic cholinergic receptors(2)
•Targeting the cholinergic nervous system with:
• AchE inhibition and
• nicotinic stimulation/modulation may be the optimal cholinergic therapy (3)
Refs: (1)Bartus et al, 1982 (2)Feldman and Gracon, 1996; Martin-Ruiz et al., 1999 (3)Newhouse et al, 2001


Focus of Symptomatic Psychiatric Treatment of AD (secondary prevention)
• Psychic– Paranoia
– Delusion/hallucinations
– Anxiety/fear
– Agitation
– Confusion
– Depression
• Vegetative– Sleep disturbance– Over or under eating– Elimination difficulties
• Cognitive– Limiting impact of
cognitive dysfunction– Enhancing efficacy of
remaining cognitive skills

Psychotropic Drug Management of AD
• Goal: allow caregiver to manage problem behaviors at home as long as possible
Antidepressants
Depression, Anxiety, Agitation, Disinhibition
Antipsychotics
Psychosis, Anxiety, Agitation, Aggression
Anxiolytics
Anxiety (short-term)
Anticonvulsants (?) Agitation, aggression
Anticholinesterase (Primary Therapy)


PATHOPHYSIOLOGY OF AGGRESSIVITY IN ALZHEIMER’S DISEASE
Evidence of derangement of serotonergic system:
(1) Clinical response to serotonergic agents (trazodone, tryptophan, bupsirone, sertraline, fluoxetine) in dementia
(2) Depleted levels of serotonergic binding in neocortex (frontal & temporal) found in Alzheimer’s Disease
(3) Intense neurofibrillary tangle information found in dorsal raphe nucleus


Support/AidFor Caregiver
Competency
Treatment ofPsychiatricSymptoms
Screening and Diagnosis
The Roles of the Psychiatrist in AD
Psychiatrist
Long-Term CareConsultation

To View or Download this Presentation
Fletcher-Allen Server: Burlington17
Look in the following Folders:
Groups
Mental Health
Neurobiology Course
File is:
Psychopath Course Lecture-Dementia


AD: The Role of the Physician in the Community
Screening
Diagnosis
Treatment Medication
Therapy (PT and family)
Management
Behavior Cognitive Decline
Competency Placement
Primary MD