deep cnn for segmentation of myocardial asl … › files › talks ›...
TRANSCRIPT
Deep CNN for Segmentation of Myocardial ASL Short-Axis Data:
Accuracy, Uncertainty, and Adaptability
Hung P. Do1, Yi Guo2, Andrew J. Yoon3, and Krishna S. Nayak4
1Canon Medical Systems USA, Inc.
2Snap Inc.
3Long Beach Memorial Medical Center, University of California Irvine
4University of Southern California
ISMRM Workshop on Machine Learning, Washington DC, Oct 26-28, 2018

Speaker Name: Hung Do
Company Name: Canon Medical Systems USA, Inc. (formerly Toshiba Medical)
Type of Relationship: Employee
Declaration of
Financial Interests or Relationships
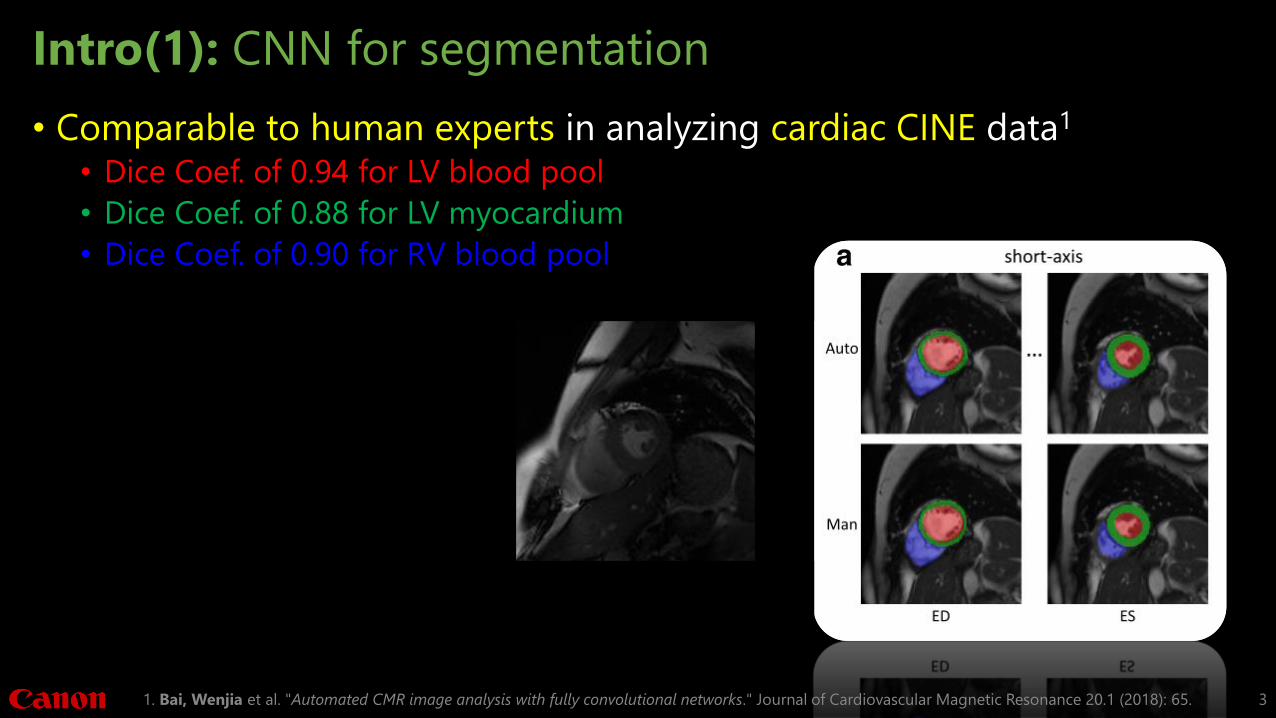
Intro(1): CNN for segmentation
• Comparable to human experts in analyzing cardiac CINE data1
• Dice Coef. of 0.94 for LV blood pool
• Dice Coef. of 0.88 for LV myocardium
• Dice Coef. of 0.90 for RV blood pool
1. Bai, Wenjia et al. "Automated CMR image analysis with fully convolutional networks." Journal of Cardiovascular Magnetic Resonance 20.1 (2018): 65. 3

Goals
1. To apply CNN for segmentation of myocardial Arterial Spin Labeled (ASL) data
2. To measure model uncertainty using Monte Carlo dropout
3. To adapt the CNN model to the desired trade-off between false positive (FP) and false negative (FN) using Tversky loss function
4
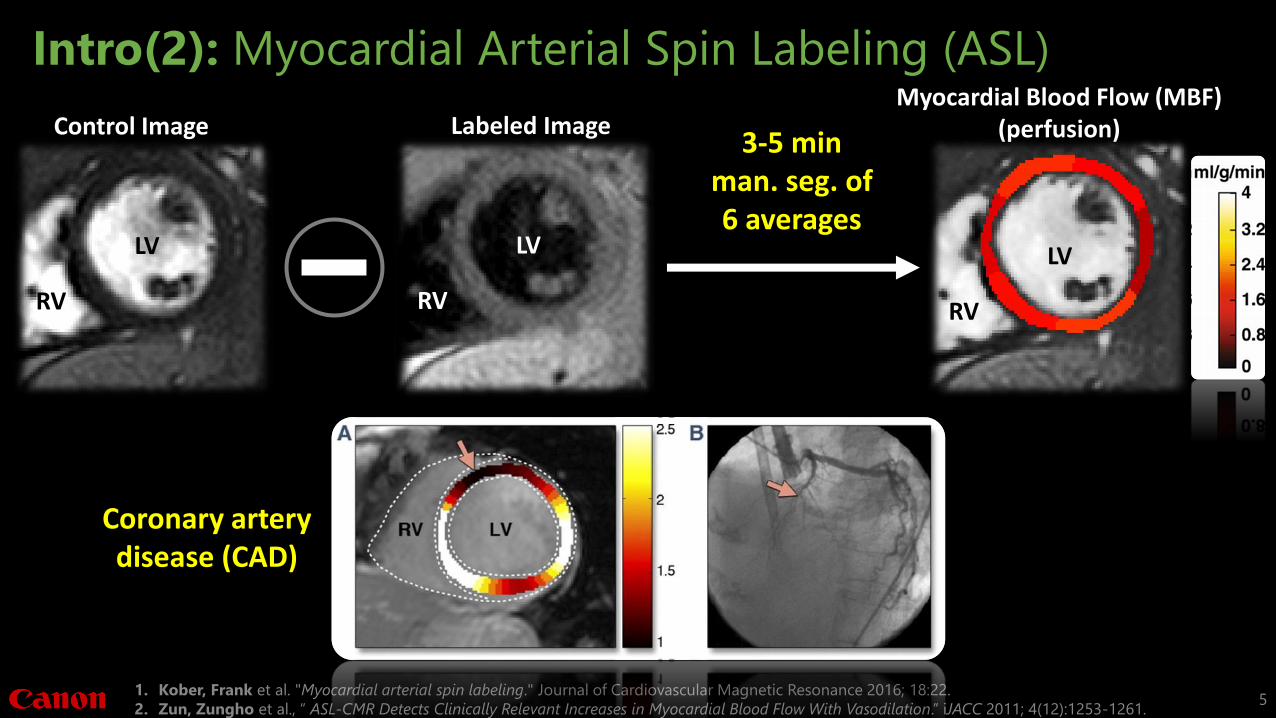
Intro(2): Myocardial Arterial Spin Labeling (ASL)
1. Kober, Frank et al. "Myocardial arterial spin labeling." Journal of Cardiovascular Magnetic Resonance 2016; 18:22.
2. Zun, Zungho et al., “ ASL-CMR Detects Clinically Relevant Increases in Myocardial Blood Flow With Vasodilation.” iJACC 2011; 4(12):1253-1261.5
3-5 minman. seg. of6 averages
Coronary artery disease (CAD)
Control Image
LV
RV
Labeled Image
LV
RV
Myocardial Blood Flow (MBF)(perfusion)
LV
RV

Intro(3): Characteristics of ASL data
• Low resolution
• Low SNR and CNR
• Varying SNR and CNR
6
LV
RV
Labeled images Control images
CINE images

Intro(4): Partial volume effects
• Ventricular blood and epicardial fat have different physical properties and spin history compared to myocardium.
1. Wikimedia Commons contributors, "File:Heart normal short axis section.jpg," Wikimedia Commons, the free media repository, (accessed October 11, 2018). 7
LVRV LV
RVFat
Fat
Myocardium
Myocardium
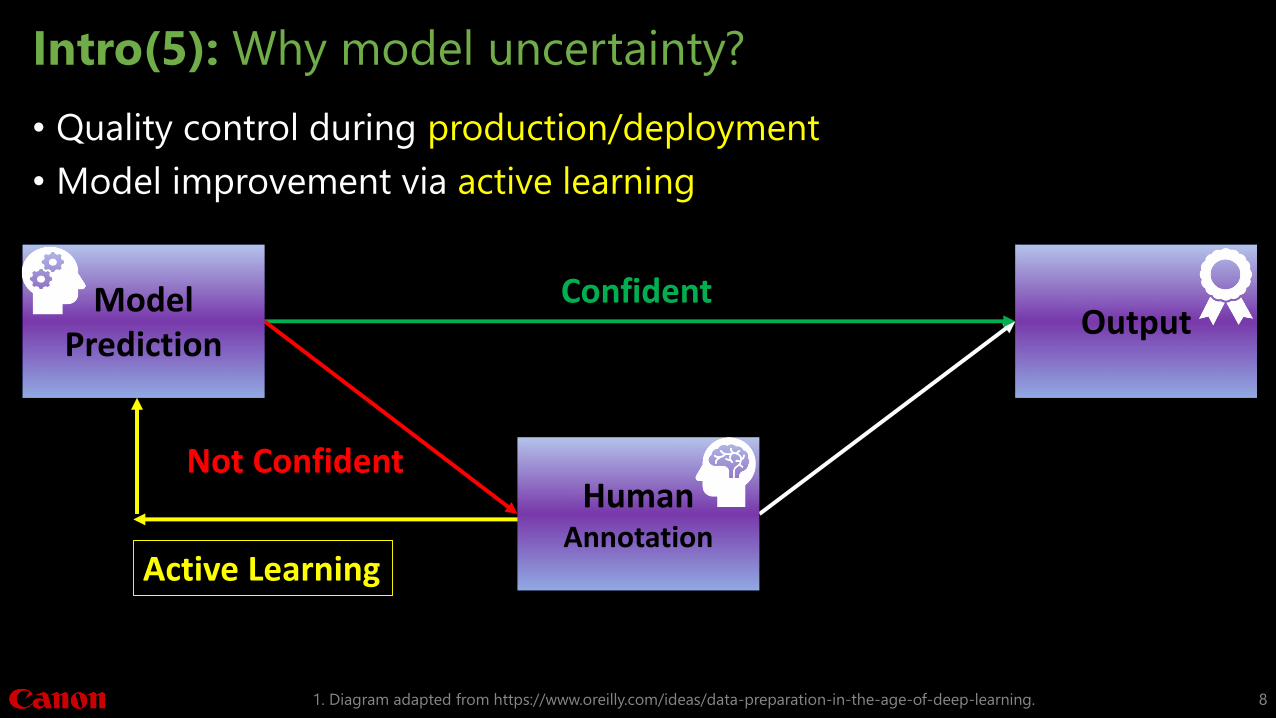
Intro(5): Why model uncertainty?
• Quality control during production/deployment
• Model improvement via active learning
1. Diagram adapted from https://www.oreilly.com/ideas/data-preparation-in-the-age-of-deep-learning. 8
HumanAnnotation
Active Learning
Confident
Not Confident
Model Prediction
Output

Methods(1): Network Architecture1
5x5 Conv+ReLU+BN 1x1 Conv+Sigmoid
C Channel Concatenation
Max Pooling UpsamplingMonte Carlo Dropout
C
C
C
CInput
Output
1. Ronneberger O et al., "U-net: Convolutional networks for biomedical image segmentation." 2015; arXiv:1505.04597. 9
loss = Binary Cross-Entropy or (1 – Soft-Dice) or (1 – Tversky Index)

Methods(2): Dataset and training parameters
• Training and validation data1:• From 22 subjects: 478 images – 438/40 images for training/validation
• Test data1:• From 6 “un-seen” heart transplant patients: 144 images (rest and during
Adenosine stress)
• Training parameters:• 150 epochs
• Learning rate: 1e-4
• Dropout rate: 0.5
• Batch size = 12
• Adam optimizer
1. Do, Hung et al, “Double-gated Myocardial ASL Perfusion Imaging is Robust to Heart Rate Variation.” Magn Reson Med 2017; 77(5):1975-1980. 10

Methods(4): Adaptability using Tversky loss
1. Tversky, Amos. "Features of similarity." Psychological Review 1977;84(4): 327-52.
2. Wikipedia contributors. "Jaccard index." Wikipedia, The Free Encyclopedia. Wikipedia, The Free Encyclopedia, 20 Sep. 2018. Web. 5 Oct. 2018.11
𝑫𝒊𝒄𝒆 =𝟐⋅|𝑨 ⋂𝑩|
𝑨 +|𝑩|
𝑫𝒊𝒄𝒆 =𝟐⋅𝑻𝑷
𝟐⋅𝑻𝑷+𝑭𝑷+𝑭𝑵=
𝑻𝑷
𝑻𝑷+𝟎.𝟓⋅𝑭𝑷+𝟎.𝟓⋅𝑭𝑵TPFP FN
Tversky loss = 1- Tversky Index1
𝑻𝒗𝒆𝒓𝒔𝒌𝒚 𝑰𝒏𝒅𝒆𝒙 =𝑻𝑷
𝑻𝑷 + (𝟏 − β) ⋅ 𝑭𝑷 + β ⋅ 𝑭𝑵
A: Predicted MaskB: Reference Mask
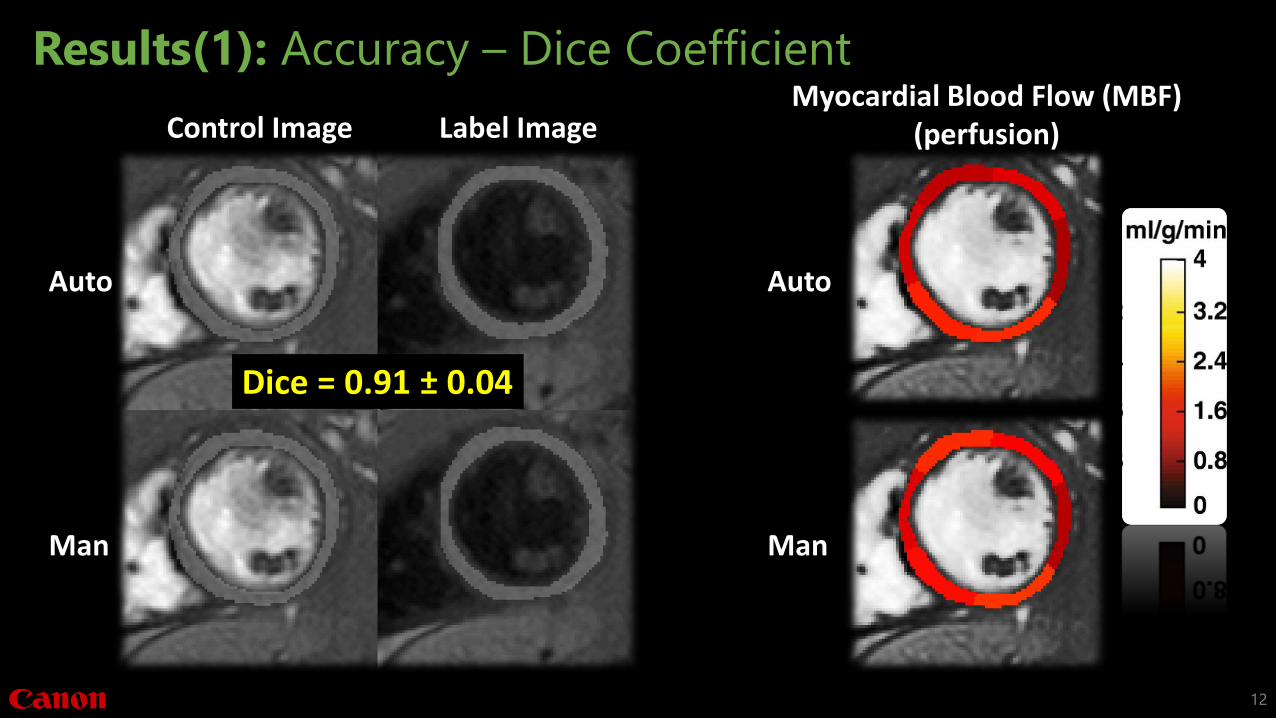
Results(1): Accuracy – Dice Coefficient
12
Auto
Man
Auto
Man
Myocardial Blood Flow (MBF)(perfusion)Control Image Label Image
Dice = 0.91 ± 0.04

Results(1): Accuracy – Myocardial Blood Flow (MBF)
13
y = 0.9877x + 0.0244R² = 0.9613
-2
0
2
4
6
8
10
-2 0 2 4 6 8 10
AU
TO S
EGM
ENTA
TIO
NMANUAL SEGMENTATION
Regional MBF (ml/g/min)
MBF measured using automatic segmentation is highly correlated to that measured using manual segmentation

Results(2): Uncertainty
14
y = 5.4434x + 0.0641R² = 0.637
0.05
0.1
0.15
0.2
0.25
0.3
0.0025 0.0075 0.0125 0.0175 0.0225 0.0275
NO
RM
ALI
ZED
MC
STD
DICE STD
Normalized MC STD vs. Dice STD
MC STD
Without manual segmentation
Given man. segmentation
Dice STD
1115 MC trials

y = 5.4434x + 0.0641R² = 0.637
0.05
0.1
0.15
0.2
0.25
0.3
0.0025 0.0075 0.0125 0.0175 0.0225 0.0275
NO
RM
ALI
ZED
MC
STD
DICE STD
Normalized MC STD vs. Dice STD
Auto: Dashed lines Man: White solid lines
Results(2): Uncertainty
15
MC STDMC STD
1115 MC trials

0.229 0.367 0.744 1.49 2.716
12
24
0
5
10
15
20
25
16 32 64 128 256 512 1024 2048INFE
REN
CE
TIM
E (S
ECO
ND
)
NUMBER OF MC TRIALS
Inference Time vs. # of MC trials
0
0.005
0.01
0.015
0.02
0.025
0.03
16 32 64 128 256 512 1024 2048
UN
CER
TAIN
TY
NUMBER OF MC TRIAL
Model Uncertainty
Results(2): Uncertainty – Time penalty per image
16
Batch Size = 64
~1.5s/image with 128 MC trials

Results(3): Adaptability – Partial volume effects
17
y = 1.0166x - 0.1445R² = 0.9523
-2
0
2
4
6
8
10
-2 0 2 4 6 8 10
THIN
SEG
MEN
TATI
ON
ORIGNIGAL SEGMENTATION
Regional MBF: Thin vs. Orig.
y = 0.9811x + 1.1951R² = 0.8266
-2
0
2
4
6
8
10
-2 0 2 4 6 8 10
THIC
K S
EGM
ENTA
TIO
N
ORIGNIGAL SEGMENTATION
Regional MBF: Thick vs. Orig.
Dice = 0.80 ± 0.04 Dice = 0.81 ± 0.02
FP = 0FN ~300 pixels/im
FP ~400 pixels/imFN = 0
Original/ManThin mask Thick mask
Significant overestimation due to partial volume effects
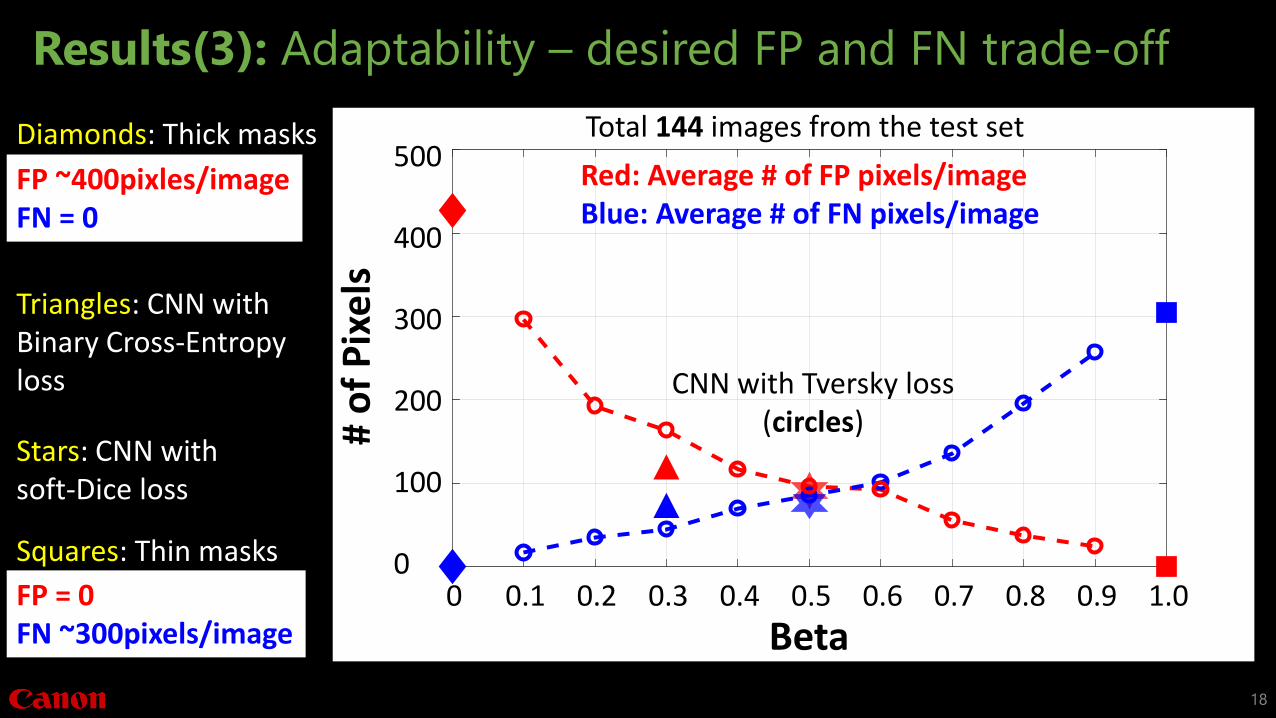
Results(3): Adaptability – desired FP and FN trade-off
18
Beta
# o
f P
ixe
ls200
100
400
300
500
00 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.00.1
Red: Average # of FP pixels/imageBlue: Average # of FN pixels/image
CNN with Tversky loss(circles)
Diamonds: Thick masks
FP ~400pixles/imageFN = 0
Stars: CNN with soft-Dice loss
Triangles: CNN with Binary Cross-Entropy loss
Total 144 images from the test set
FP = 0FN ~300pixels/image
Squares: Thin masks
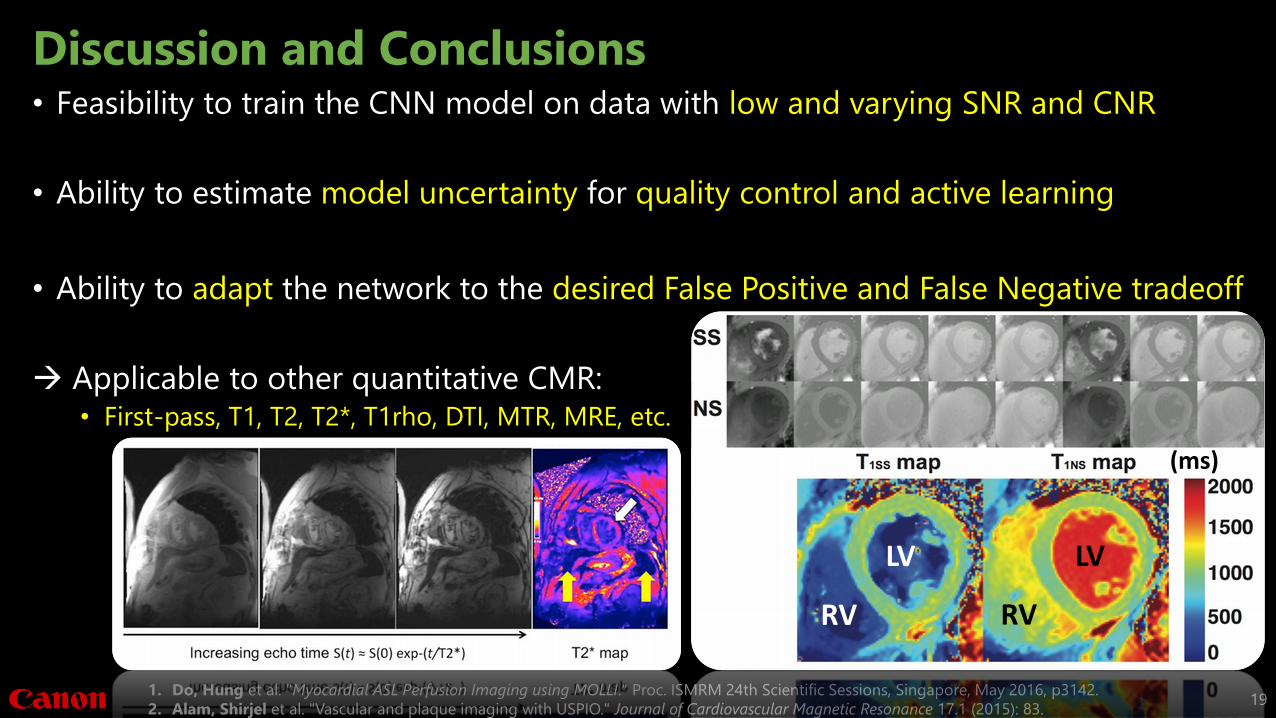
Discussion and Conclusions• Feasibility to train the CNN model on data with low and varying SNR and CNR
• Ability to estimate model uncertainty for quality control and active learning
• Ability to adapt the network to the desired False Positive and False Negative tradeoff
Applicable to other quantitative CMR: • First-pass, T1, T2, T2*, T1rho, DTI, MTR, MRE, etc.
191. Do, Hung et al. "Myocardial ASL Perfusion Imaging using MOLLI." Proc. ISMRM 24th Scientific Sessions, Singapore, May 2016, p3142.
2. Alam, Shirjel et al. "Vascular and plaque imaging with USPIO." Journal of Cardiovascular Magnetic Resonance 17.1 (2015): 83.
LV
RV
LV
RV
(ms)

Acknowledgements
• Funding:• Whittier Foundation
• NIH/NHLBI, #1R01HL130494-01A1
20

For over 100 years, the Canon Medical Systems `Made for Life’ philosophy prevails as our ongoing commitment
to humanity. Generations of inherited passion creates a legacy of medical innovation and service that
continues to evolve as we do. By engaging the brilliant minds of many, we continue to set the benchmark,
because we believe quality of life should be a given, not the exception.
Thank you for your attention!

Backup slides

77
49.537.4
22.914.4 12 10.1 9.65
16.5
0102030405060708090
1 2 4 8 16 32 64 128 256INFE
REN
CE
TIM
E (S
ECO
ND
)
BATCH SIZE
InferenceTime for 1024 MC trials
0
0.2
0.4
0.6
0.8
1 2 4 8 16 32 64 128 256MEA
N D
ICE
BATCH SIZE
Dice Mean
0
0.01
0.02
0.03
1 2 4 8 16 32 64 128 256
DIC
E ST
D
BATCH SIZE
Dice STD
Results(2): Uncertainty – Batch Size
23

Methods(3): dropout1
1. Srivastava et al., “Dropout: A simple way to prevent NN from overfitting.” JMLR 2014.
2. Animation is adapted from https://www.techemergence.com/what-is-machine-learning/24
Hidden Layer #1
HL #2 HL #3 HL #4
Output

Intro(3): Data characteristics of ASL
• Low SNR and contrast
1. Zungho Zun et al. “Assessment of myocardial blood flow in humans using arterial spin labeling: feasibility and SNR requirements.” MRM2009;62(4):975-83. 25
Control/Labeled Pulse Imaging
LV
RV

Methods(3): Uncertainty measure using MC dropout1
1. Gal, Yarin et al. "Dropout as a Bayesian approximation: Representing model uncertainty in deep learning." International conference on ML 2016; 1050-1059. 26
• Any NN, with dropout applied before every weight layer, is mathematically equivalent to an approximation of the Bayesian model.
• Model uncertainty can be estimated given the posterior distribution of the trained weights
Methods(3): Uncertainty measure using MC dropout1
1. Srivastava et al., “Dropout: A simple way to prevent NN from overfitting.” JMLR 2014.
2. Hinton, Geoffrey, “Lecture 10.5 – Dropout: An efficient way to combine neural nets.” COURSERA: Neural Networks for Machine Learning 2012: 33-41. 27
• “Use dropout of 0.5 in every hidden layer”
• “At test time, run the stochastic model several times on the same input”

0.229 0.367 0.744 1.49 2.716
12
24
0
5
10
15
20
25
16 32 64 128 256 512 1024 2048INFE
REN
CE
TIM
E (S
ECO
ND
)
NUMBER OF MC TRIALS
Inference Time vs. # MC trials
Results(2): Uncertainty – Time penalty
1. Srivastava et al., “Dropout: A simple way to prevent NN from overfitting.” JMLR 2014. 28
~1.5s/image with 128 MC trials
Batch Size = 64

Figure 2: worst and best
29