decreasing the impact of diabetes in the adult and older
TRANSCRIPT

Jacksonville State University Jacksonville State University
JSU Digital Commons JSU Digital Commons
Doctor of Nursing Practice Projects Theses, Dissertations & Graduate Projects
Summer 2021
Decreasing the Impact of Diabetes in the Adult and Older Adults Decreasing the Impact of Diabetes in the Adult and Older Adults
Rural Health Population Utilizing Phone Calls as Part of the Rural Health Population Utilizing Phone Calls as Part of the
Chronic Care Management Program Chronic Care Management Program
Adrienne Shambray [email protected]
Follow this and additional works at: https://digitalcommons.jsu.edu/etds_nursing
Part of the Nursing Commons
Recommended Citation Recommended Citation Shambray, Adrienne, "Decreasing the Impact of Diabetes in the Adult and Older Adults Rural Health Population Utilizing Phone Calls as Part of the Chronic Care Management Program" (2021). Doctor of Nursing Practice Projects. 48. https://digitalcommons.jsu.edu/etds_nursing/48
This Final DNP Paper is brought to you for free and open access by the Theses, Dissertations & Graduate Projects at JSU Digital Commons. It has been accepted for inclusion in Doctor of Nursing Practice Projects by an authorized administrator of JSU Digital Commons. For more information, please contact [email protected].

Jacksonville State University Graduate Studies
700 Pelham Rd N., 320 Angle Hall, Jacksonville, AL 36265 Phone: (256) 782-5348
http://www.jsu.edu/graduate/index.html
DNP Manuscript Defense Approval
First Name: Last Name: Student ID:
Date:
Choose your DNP program:
Manuscript Title:
Date of Manuscript Approval:
Student Signature Electronically signed by Adrienne Shambray on 06/28/2021 9:34:41 PM
Chair, DNP Manuscript Signature
Electronically signed by Laura Barrow on 06/29/2021 9:49:04 AM
DNP Clinical Coordinator Signature
Electronically signed by Lori McGrath on 06/29/2021 10:01:48 AM
DNP Program Coordinator Signature
Electronically signed by Donna Dunn on 06/29/2021 10:38:22 AM
Director of Online & Graduate Nursing Programs Signature
Electronically signed by Kimberly Helms on 07/01/2021 11:11:39 AM
Dean of Graduate Studies Signature
Electronically signed by Channing Ford on 07/22/2021 4:50:19 PM
Adrienne* Shambray* *
06/28/2021*
nmlkj Adult-Gerontology Acute Care Nurse Practitioner (Doctor of Nursing Practice) nmlkj Family Nurse Practitioner (Doctor of Nursing Practice) nmlkji Post-Master's DNP (Doctor of Nursing Practice)
*
Decreasing the Impact of Diabetes in the Adult and Elderly Rural Health Population Utilizing Phone Calls as Part of the Chronic Care Management Program *
06/29/2021*
ii
DECREASING THE IMPACT OF DIABETES IN THE ADULT AND OLDER
ADULTS RURAL HEALTH POPULATION UTILIZING PHONE CALLS AS PART
OF THE CHRONIC CARE MANAGEMENT PROGRAM
A DNP Project Submitted to the Graduate Faculty
of Jacksonville State University in partial Fulfillment of the
Requirements for the Degree of Doctor of Nursing Practice
By
ADRIENNE SLAUGHTER SHAMBRAY
Jacksonville, Alabama
June 28, 2021

iii
Copyright 2021
All Rights Reserved
_______________________________________________
Adrienne Slaughter Shambray June 28, 2021

iv
ABSTRACT
This quantitative study was developed in order to evaluate the impact of phone calls on
patient outcomes using the Chronic Care Management program (CCM). In January 2015,
the Centers for Medicare and Medicaid Services (CMS) implemented the (CCM), with
the goal of improving health and quality of care for high-risk patients. The administration
and physicians at the clinic of focus for this project recognized a need for the facility to
help improve and manage these patients’ care to prevent issues such as hospital
readmission. This project aimed at following patients in the program with the chronic
condition of diabetes mellitus and tracked previous glycated hemoglobin (A1C) prior to
program and compared the result to the A1C three months into the program. After
participation in the program for a minimum of three months, a quantitative analysis was
completed from the data collected. Results showed the probability of an individual’s A1C
to decrease was 61.8%, which is clinically significant. Nursing has a strong foundation
based in promoting quality of life for patients. This project reflects that goal and has
potential to advance nursing’s mission to promote quality of life moving into the future.
Keywords: Chronic care management, Chronic care protocols, Chronic care, diabetes,
Type 2 diabetes, diabetes management, telehealth
v
ACKNOWLEDGEMENTS
Throughout this process of completing this DNP Manuscript I have received a
great deal of support and assistance. Firstly, I would like to thank my DNP Chair, Dr.
Laura Barrow, and Dr. Crystal Fuller, whose expertise and insight pushed me to sharpen
my thinking and brought my work to a higher level. I would also like to thank Dr. Keith
for her encouragement and assistance to push our class to greater expectations. Secondly,
I would like to thank my colleagues from my internship and preceptor, Dr. Ilinca
Prisacaru for the wonderful collaboration and assistance with my project. Additionally, I
like to thank God, my family, especially my husband for his support and wise counsel.
You are always there for me and assist me with anything I may need. I would like to
thank my parents for their continued support. And finally, my children, Sebastian and
Nicholas, for giving me the drive I needed to complete this project.

vi
TABLE OF CONTENTS
Abstract…………………………………………………………………………………... iv
Introduction………………………………………………………………………………. 1
Background……………………………………………………………………………. 1
Problem Statement..……………………………………………………………………3
Organizational Description of Project Site…………………………………………… 4
Review of Literature………………………………………………………………........... 4
Evidence-Based Practice: Verification of Chosen Option………....…………………..8
Theoretical Framework………………………………........................................................9
Goals, Objectives, & Expected Outcomes…………………………………………... 11
Project Design…………………………………………………………………………… 12
Project Site and Population………………………………………………………….. 13
Setting Facilitators and Barriers……………………………………………………... 14
Implementation Plan/Procedures………………………………………………………... 15
Measurement Instruments…………………………………………………………….15
Data Collection Procedure……………………………………………………………15
Data Analysis…………………………………………………………………………16
Results………………………………………………………………………………...19
Interpretation/discussion…………………………………………………………………20
Cost-Benefit Analysis/Budget…………………………………………………………...22
Timeline………………………………………………………………………………….22
Ethical Considerations/Protection of Human Subjects ………………………………….23
Conclusion……………………………………………………………………………….23
References……………………………………………………………………………….25

ii
Appendices………..……………………………………………………………………...29
Appendix A…………………………………………………………………………....... 29
Appendix B………………………………………………………………………………30
Appendix C………………………………………………………………………………31
Appendix D……………………………………………………………………………... 34

1
Decreasing the Impact of Diabetes in the Adult and Older Adults Rural Health Population
Utilizing Phone Calls as Part of the Chronic Care Management Program
Introduction
The older adult population is continuing to grow and will soon triple in the next
few decades to come. Based on current trends, the population of people greater than 79
years of age will expand from approximately 126.5 million to approximately 446.6
million by 2050. When aging, the population tends to accumulate multiple deficits in
their life that makes them more vulnerable and require more assistance in healthcare. It is
predicted that the growing population will see a decline in daily functions, have
unfavorable health outcomes, and have frequent hospital admissions (Aranha,
Smitherman, Patel, & Patel, 2020). Hospital admissions are costly and can cost insurance
companies and patients millions to billions of dollars yearly. With proper quality of care,
hospital admissions and readmissions can be reduced and occasionally prevented (Chen
& Grabowski, 2019).
Background
Healthcare providers have a responsibility of providing quality care to patients
and preventing hospital admissions and readmissions. Hospitalizations are a burden on
healthcare systems and individuals financially and physically. This may cause
depression, poor social support, and/or polypharmacy for patients; therefore, linking to
patients getting readmitted to the hospital. Another factor of hospital readmission is poor
discharge planning processes where hospital staff may fail to have adequate
2
communication with primary care physicians or patients fail to utilize follow-up visits
(Shih, Buurman, Tynan-McKiernan, Tinetti, & Jenq, 2015). Adequate follow-up with
patients who have been hospitalized is lacking in primary care.
This lack of follow-up care can be costly. Readmissions among Medicare
beneficiaries account for 56% of three0-day readmissions in the United States and cost
$26 billion (Jung, DuGoff, Smith, Palta, Gilmore-Bykovskyi, & Mullahy, 2020).
Approximately, one-quarter of patients develop an adverse effect and half of those events
are preventable. It was estimated about 19.6% of Medicare fee-for-service patients are
re-hospitalized within 30 days of discharge. This accumulates extreme costs; for
example, 3.3 million adults were readmitted to the hospital within three0 days and
resulted in a cost of $41.3 billion. Each year, avoidable hospital readmissions cost
approximately $12 billion (Hudali, Robinson, & Bhattarai, 2017). These statistics prove
the need for interventions to reduce hospital admissions and subsequent costs.
According to Scott (2018), one intervention to reduce these statistics is the
implementation of the Chronic Care Management (CCM) program. CCM services are
provided by a physician or non-physician practitioner such as a nurse practitioner or
physician assistant. The service is provided per calendar month for patients with multiple
chronic conditions. The conditions must meet the expected criteria lasting at least a year,
placing the patient at risk of death, acute exacerbation, or functional decline. The chronic
condition may include Alzheimer’s disease, arthritis, asthma, cancer, chronic obstructive
pulmonary disease, diabetes, heart failure, hypertension, heart disease, or depression
(Scott, 2018). This study will focus on patients with diabetes in the CCM program.

3
Diabetes mellitus is associated with a two to three-fold increase in the likelihood
of contracting cardiovascular diseases. Managing diabetes appropriately and lowering
the glycated hemoglobin (HbA1C) by at least 1% reduces microvascular complications
(Gorina, Limonero, & Alvarez, 2018). The use of an interdisciplinary care team for
diabetes care when combined with self-management diabetic education and glucose-
lowering therapies helps prevent comprehensive lifelong complications. The CCM
program allows a team effort between staff and patients to develop goals for the patient’s
health and manage individual goals that have been set (Del Valle & McDonnell, 2018).
With proper education, patients feel better by increasing their knowledge and experience
and they are protected from possible side effects by controlling the disease. Telephone
reminders are effective in creating behavior change in patients with diabetes in
performing self-management activities (Eroglu & Sabuncu, 2021).
Problem Statement
The adult and older adult population with multiple chronic conditions need
adequate quality of care and follow-up to ensure proper compliance and treatment. The
patient, intervention, comparison, and outcome (PICO) question for this DNP project is
as follows: among the insured adult to older adult patients ages 25 and older, how
effective are monthly telephone calls as part of the CCM program in ensuring adequate
A1C control, compared to patients’ A1C prior to entering the program? The author will
address the PICO question by utilizing monthly phone calls to evaluate a newly
implemented program within a primary care clinic.

4
Organizational Description of Project Site
The population with diabetes continues to rise and is partially due to the lack of
education, patient self-management, and/or patient understanding of the disease. The
help of education and continued follow-up causes an increase in patient’s managing their
care and achieving the goals created for his/her treatment. The project site needed a
protocol to assure providers and staff had the ability to assure proper diabetic education
and counseling as well as giving the patient more access to express one’s needs,
concerns, questions, and understanding (Eroglu & Sabuncu, 2021). According to Eroglu
& Sabuncu (2021), studies show there is a direct link between education and metabolic
control.
Review of Literature
According to Westphal (2019), healthcare and medicine have made great
advances over the decades and have resulted in longevity in human life. This results in
humans living longer with chronic conditions such as heart disease, chronic obstructive
pulmonary disease (COPD), Alzheimer’s disease, stroke, cancer, and diabetes. These
conditions account for two-thirds of deaths and $1.5 trillion of healthcare spending
(Westphal, 2019). According to Cohen et al. (2020), the United States and other
developed nations enjoyed large gains in life expectancy at birth, however, the United
States began to lag behind other nations starting in the 1960s. This poor performance has
been studied and documented to find the proper solution to enhance care. Studies have
shown that patients with insurance versus patients without insurance have improved
5
survival and achieved better outcomes due to access to earlier diagnoses and treatment,
especially individuals with diabetes (Cohen et al., 2020).
According to the Centers for Disease Control and Prevention (CDC) (2021),
diabetes is the seventh leading cause of death in the United States. Approximately
three4.2 million adults in the US have diabetes, and 20% of those people are unaware
they have the diagnosis. In the last twenty years, adults diagnosed with diabetes have
more than doubled (CDC, 2021). Rodriguez et al., (2021) stated providers should follow
recommendations by the American Diabetes Association (ADA) and screen individuals
aged 45-70 years of age who are overweight/obese, individuals with a family history of
diabetes, and individuals with a history of gestational diabetes or polycystic ovarian
syndrome. According to the ADA (2021), if individuals present to the clinical setting
complaining of polyuria, polydipsia, polyphagia, fatigue, blurry vision, slow healing
wounds, weight loss, or paresthesia; the provider should screen the individual for
diabetes. Early detection of diabetes can decrease the risk of developing diabetic
complications (ADA, 2021).
Hospital readmissions have been on the rise for decades due to chronic diseases,
which are one of the most significant challenges the United States healthcare system
confronts. The majority of Medicare beneficiaries have two or more chronic health
conditions. These beneficiaries have more hospitalizations, physician visits, and
emergency room visits when compared to patients with one or no chronic conditions.
Primary care practices provide the majority of the beneficiaries’ care; although, these
practices often receive inadequate funding and infrastructure support. In January 2015,
the Centers for Medicare and Medicaid Services (CMS) implemented a new policy to pay

6
providers or chronic care management services. The goal was to improve health and
quality of care for high-need patients. This program allowed eligible providers to bill
CMS for up to 20 min of non-face-to-face care services in a three0-day period (Wilson,
O’Malley, Bozzolo, McCall, & Ma, 2019).
As stated above, one study estimated that approximately 19.6% of Medicare
patients are hospitalized within thirty days of hospital discharge (Hudali, Robinson, &
Bhattari, 2017). Rehospitalizations also caused an increase in costs in the hospital
setting. In 2011, approximately 3.3 million adults were readmitted to the hospital which
cost about $41.3 billion (Hudali, Robinson, & Bhattari, 2017). By 2016, the three0-day
readmission rate had increased to over 4 million (Bailey, Weiss, Barrett, & Jiang, 2019).
The goal of researchers, hospitals, and policymakers is to reduce preventable patient
readmissions. Billions of dollars are wasted each year due to avoidable hospital
readmission costs. When attempting to reduce readmission rates, the readmission of
high-risk patients was significantly reduced with adequate one-week follow-up
appointments after discharge. Patients who do not receive timely follow-up appointments
with their primary care provider have readmission rates ten times higher than those who
do. This article presented a study that followed a transition of care clinic after discharge.
The study focused on the care for patients in a 30-day window and with the policy and
procedure of follow-up care, the clinic succeeded in reducing the rehospitalization rate
from 11.7% to 3.8%. One method used to help reduce rehospitalization was through
enhancing communication with patients after discharge. This includes post-discharge
phone calls along with community-based education and information through easily

7
accessible electronic health records among inpatient and outpatient providers (Hudali,
Robinson, & Bhattari, 2017)
Xing, Goehring, & Mancuso (2015) study demonstrated that having well-
designed care coordination after discharge can reduce healthcare costs and manage
chronic conditions. Care coordination improves communication among patients and
healthcare providers. This study also showed high-risk patients who benefitted from care
coordination by having a Chronic Care Management program. In this program, a nurse
care manager coordinated the long-term care services, educated patients to better
understand signs of worsening health, and supported patients’ efforts to achieve self-
management goals (Xing, Goehring, & Mancuso, 2015). The program included an initial
comprehensive assessment, an individualized health action plan, and meetings with the
nurse care manager occurring at least once a month. Health action plans were reviewed
and updated every six weeks (Xing, Goehring, & Mancuso, 2015).
Implementing this program can be difficult for clinical practices due to a lack of
infrastructure. The Chronic Care Management (CCM) program was developed by The
Centers for Medicare and Medicaid Services (CMS). It was developed to provide care
coordination activities outside of office visits. A 2015 article by Hodach, addressed the
challenges of the CCM program. One challenge is finding ways to promote greater
patient engagement with the comprehensive care plans required by CMS. Without the
care plan in place, there is a risk for a negative impact on the success of the patient’s
condition. Another challenge was reconfiguring and adapting electronic health records to
be more aligned with CCM. The support of Healthcare Information Technology (IT) can
help ease these challenges (Hodach, 2015).

8
After literature review, the evidence reveals the continued rise of hospitalizations
due to worsening of an individual’s chronic conditions (Aranha, Smitherman, Patel, &
Patel, 2020; Bailey, Weiss, Barrett, & Jiang, 2019). This has caused a strain for patients
physically, emotionally, and financially. Insurance companies have more responsibilities
to manage financially as well. One study found that patients were not receiving the
education needed at hospital discharge which resulted in a decrease in patients’ abilities
to manage their care properly and therefore, returned to the hospital within the 30-day
window (Bailey, Weiss, Barrett, & Jiang, 2019). Another study found that a nurse who
took time to educate a patient and his/her family, establish a care plan, and meet with the
patient often significantly decreased the likelihood the of rehospitalization. Barriers to
this type of program exist, such as patient and staff participation. Therefore, proactive
measures may be needed to mediate these barriers (Chen & Grabowski, 2019).
The CCM program was implemented to help decrease hospitalizations, however,
research shows a lack of information regarding specific chronic conditions such as
diabetes. Because the system is newly introduced, there is a lack of evidence regarding
its impact on diabetic complications and management. More evidence is also needed
regarding the impact of providers counseling patients regularly and the impact on
meeting diabetic goals.
Evidence-Based Practice: Verification of Chosen Option
After a thorough literature review, the program intervention chosen for
implementation focused on patients with diabetes to improve their A1C by adjusting the
CCM program that was established at the rural primary clinic chosen for this study. This

9
intervention focused solely on patients with diabetes with a goal to reduce diabetic
complications; therefore, reducing diabetic-related hospitalizations. The intervention
included close follow-up with these patients through phone calls regarding their self-
management. The phone calls included the needed education and counseling to impact
the desired goals.
Theoretical Framework
This DNP project is based on two theories. One is the interpersonal relations in
nursing theory by Hildegard Peplau which focuses on observations. The second theory is
Neuman’s systems model by Betty Neuman which focuses on examining patients as a
system.
Hildegard Peplau developed the theory of interpersonal relations in nursing, in
which she discussed her belief nursing concepts should come from observations in
nursing. Peplau developed a system combining inductive and deductive reasoning. This
was based on observation (inductive) and known concepts (deductive). She used methods
to examine phenomena of interest and to test an intervention targeted at the problem
(Peplau, 1991). Peplau’s interpersonal model examines the process between the nurse
and patient that works toward a mutual goal. The DNP project will follow this process
when developing goals with the patient at the beginning of the program to help prevent
hospitalization or rehospitalization. The first phase of Peplau’s theory is orientation, in
which the nurse gathers healthcare and other information about the client, and an auto
10
diagnosis is developed regarding the illness/disorder. A nurse may function as a resource
person by giving specific information that aids the patient to understand the situation
(Peplau, 1991). In this concept, introductions are made, questions are asked, and issues
are clarified. Trust and rapport are developed between provider and patient. This phase
also includes contracting, establishing a plan of care, and time limits for visits are
clarified and agreed upon (Peplau, 1991). Initially in the program, the provider discusses
the program and the chronic conditions with the patient. Then, the patient gives consent
to join the CCM program and establish a plan of care. The second core concept of this
model is identification. In this step, the nurse and patient clarify expectations and
determine how to work together. In this phase, the patient’s first impression is clarified;
one feels that he/she knows what the situation can offer; and then responds to persons
who seem to offer the help one needs (Peplau, 1991). The third phase is exploitation, in
which the patient uses the services offered by the nurse and attempts to accept full value
from the relationship that has been established (Peplau, 1991). The final core concept is
resolution. In this step, the patient’s needs have been met and the patient moves toward
independence due to the gradual freeing from being a person that needs help to having
the strength and ability to stand more or less alone (Peplau, 1991). The patient may
reduce interaction times, issues are summarized, and the patient has a health maintenance
plan (Peplau, 1991).
Betty Neuman’s system model states an individual or group is a client system.
Each system is unique but composed of common characteristics. It further states that
nursing interventions can affect the client’s move toward health on several levels. The

11
goal is to promote the system’s stability by assessing the impact of stressors and helping
the client adjust to the environment. Neuman’s systems model focuses on three types of
prevention: primary, secondary, and tertiary prevention, which promote wellness
(Neuman, 1982).
The DNP project used primary prevention by promoting health and wellness to
reduce risk factors and prevent possible medical events. Secondary prevention was
practiced in the CCM program by helping patients amid chronic conditions when a
stressor has occurred. Then tertiary prevention maintained wellness after an event by
continuing to monitor patients monthly (Neuman, 1982). In this project, each patient was
seen and treated as individuals and not as a generic group of individuals with diabetes,
although that was the common characteristic of the project population. Each patient had
time to discuss interventions to improve or stabilize their health and work towards a goal.
Stressors were also discussed, and the relationship was built between the patient and the
provider to assess the stressor and help the patient adjust to his/her environment
(Neuman, 1982).
Goals, Objectives, and Expected Outcomes
The purpose of this project was to establish monthly phone calls to follow patients
in the program with the chronic condition of diabetes and tracked previous A1C prior to
entry compared to A1C three months into the program. Phone calls included a review of
daily glucose readings as well as medication reconciliation. This information is
verbalized to the provider by the patient or caregiver. This allowed the provider to assess
patient/caregiver competency with both glucose monitoring and medication compliance.

12
The provider adjusted medications as needed and provided patient medication education,
also as needed. Data analysis compared A1C prior to entry to A1C three months after
phone calls were initiated and measured any differences for statistical significance. In
addition, any medication administration errors (e.g. patient reports taking incorrect
medication or dosage) from first phone call to last phone call were noted and month one
was compared to month three to analyze for statistically significant changes. The
expected outcome was to show a decrease in A1C in patients that have an A1C greater
than 7% or to stabilize patients who have an A1C less than or equal to 7%.
Project Design
This project was a quantitative, quasi-experimental design and purposive
sampling was used in data collection. It focused on implementing a program to help
reduce hospitalizations and rehospitalizations in Medicare patients with chronic
conditions. Every month a provider contacted the patient for close follow-up on diabetes.
If the patient had complications or questions regarding intervention, medication, or diet;
the phone calls were more frequent such as weekly or bi-monthly. A detailed protocol
was implemented to create a system for consistent care in a rural clinic. The protocol for
the project was developed to help staff continue the program for longevity. Post-surveys
were completed by patients via telephone on the usefulness of the program. Quantitative
data were collected on the percentage of A1Cs and hospitalizations or lack thereof during
the program.
13
Project Site and Population
The project took place at a family practice clinic in an urban area. This
community has a small-town feel but is continuing to develop and grow each year. The
population is approximately 14,000 as of 2019. Of those residents, 86% are Caucasian
and 14% identify as minorities. Approximately 14% lived in poverty (U.S. Census
Bureau, 2019). Only two medical clinics reside in this area. The participants of this
project included patients with Medicare as their primary insurance and had at least two
chronic conditions. They participated by answering the calls every month and
communicating with the staff regularly. The provider was responsible for calling the
patients for follow-up care. Patients were able to contact our staff if they had any
medical questions or problems and the staff were aware of the protocol to help assist with
clerical needs or to notify the provider of the patient’s concern regarding treatment or
his/her condition. Clinical staff for the program included a nurse practitioner who was
the main source of communication with the patients. Medical assistants helped manage
any incoming calls and direct messages to the nurse practitioner for any patient calls that
needed immediate attention and/or had questions outside of the monthly calls.
Recruitment for the program included discussing the project with a patient with diabetes
during his/her lab visit and obtaining the written consent if the patient wanted to join.
When patients decided to join, the next contact via telephone included developing a care
plan with the patient.
14
The practice offers services ranging from newborns to older adults. Service
ranges from wellness visits to acute care visits. Procedures performed at the clinic may
include suturing, ear irrigation, cryotherapy, joint injections, trigger point injections,
incision and drainage, and casting. Each physician has three to four medical assistants,
and each nurse practitioner has one to two medical assistants. Communication between
the author and staff included messages through the charting system and direct
communication.
Setting Facilitators and Barriers
The resources included a guideline from Medicare used when the program was
implemented. Office resources included a provider, medical assistants, lab technicians,
phones, computers, a charting system, and paper. Constraints included time management
of regular clinic visits and managing the program each month. Barriers included patients
not answering phone calls or not wanting to participate with the program after a few
months of being enrolled in the program. Some patients did not want to spend time on
the phone discussing their daily or weekly blood glucose logs. Other patients were not
checking their blood glucose level appropriately or found a pattern of knowing when they
would receive a phone call and check their blood sugar at that time. Another barrier
included lack of proper documentation of staff members if they discussed anything with
the patients regarding diabetes. Having bi-monthly meetings with staff helped reiterate
the need for proper documentation and prevented any burnout or staff becoming lax to
ensure close follow-up, program accuracy and continued care.

15
Implementation Plan/Procedures
Measurement Instruments
The CCM program was established prior to the implementation of the DNP
project but was used as the basis for the patient selection for the project. When
measuring the outcomes of this DNP Project the following instruments were used: the
patient list, the patient information form was used during each phone call to document
data collection and log glucose levels, and the data spreadsheet for results. Approaching
the end of the three months, a phone survey was given to evaluate the project. A
spreadsheet was created for the A1C data entry.
Data Collection Procedures
Pre-intervention consisted of getting the approval for the project from the
Institutional Review Board (IRB) (see Appendix A). The agency was selected for the
project and permission was given to allow the investigator to perform the study for the
project (See Appendix B). Pre-intervention also consisted of developing the protocol for
the continuation of the chronic care program. A list was provided of all Medicare
patients in the office from each physician in the clinic and the investigator sorted the
patients with diabetes from those patients not diagnosed with diabetes. The patients on
16
the list were contacted and made aware of the project and provided with needed
information for enrolling in the program. They gave verbal consent to enroll in the
program and then signed a consent form in the clinic prior to participation (see Appendix
C). For the first data collection, the intervention included obtaining the initial A1C of the
patient from the initiating month or within three months of the start of the project. Then,
each patient was contacted via phone call or in the office to develop a care plan and
develop appropriate goals. For three months, the project investigator called the patient
every month and occasionally called patients weekly due to medication changes and to
discuss any questions the patient had regarding diabetes. A patient information
(Appendix D) form was kept for tracking purposes to monitor patient progress from visit
to visit. Post-intervention included collecting the second A1C for each patient, evaluating
the effectiveness of the program such as evaluating the patient’s second A1C and blood
sugar logs.
Data Analysis
Twenty participants were selected for the study. The participants were between
the ages of 26-8three. The objectives and design have been described in detail elsewhere.
Briefly, the study recruited adults with a diagnosis of diabetes from a rural primary clinic
in the US. Recruitment began in January of 2021 and participants were followed until
April 2021. For data analysis, the participants were divided into four groups by age for
comparison. Group 1 consisted of individuals less than 45 years of age, group 2 included
ages 46-55 years old, group three included ages 56-65 years, and group 4 included
17
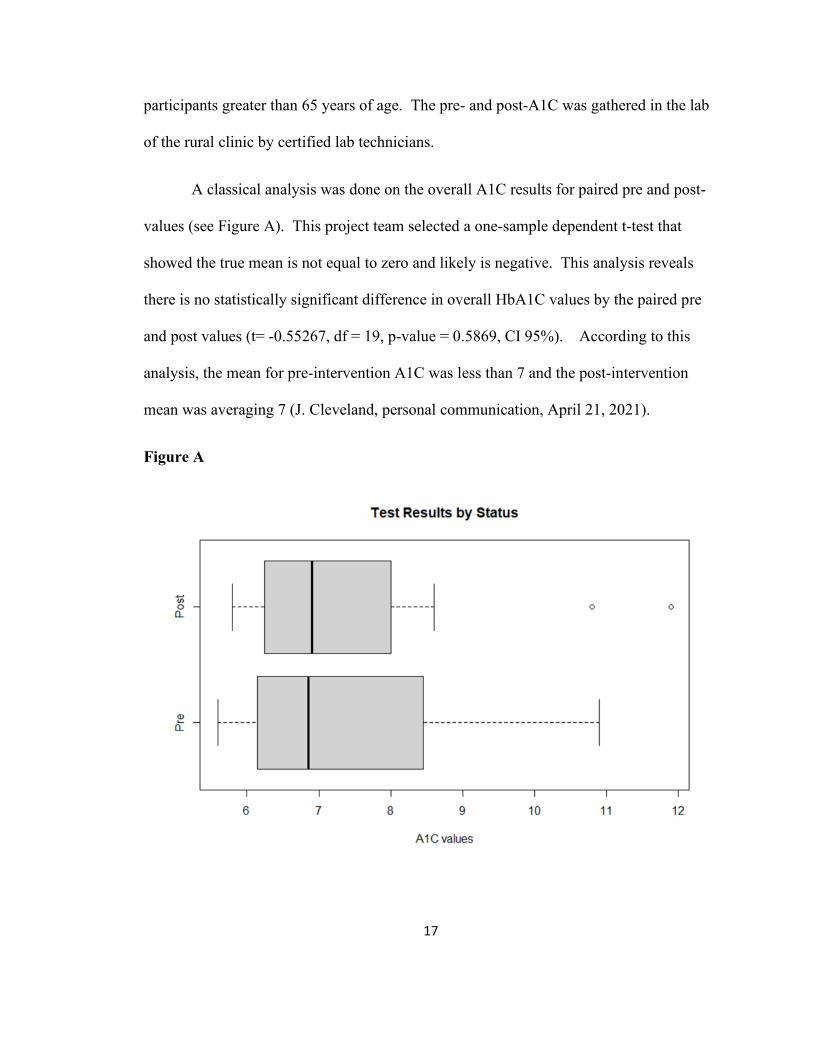
participants greater than 65 years of age. The pre- and post-A1C was gathered in the lab
of the rural clinic by certified lab technicians.
A classical analysis was done on the overall A1C results for paired pre and post-
values (see Figure A). This project team selected a one-sample dependent t-test that
showed the true mean is not equal to zero and likely is negative. This analysis reveals
there is no statistically significant difference in overall HbA1C values by the paired pre
and post values (t= -0.55267, df = 19, p-value = 0.5869, CI 95%). According to this
analysis, the mean for pre-intervention A1C was less than 7 and the post-intervention
mean was averaging 7 (J. Cleveland, personal communication, April 21, 2021).
Figure A

18
A Bayesian Analysis (see Figure B) was run to provide further information about
the data. It shows the overall HbA1C to compare the pre- and post-HbA1C mean. It
shows there is no statistically significant difference in overall A1C values by paired pre
and post results. Since the credible interval includes zero, it could be possible that there
was no difference between pre- and post-status results for A1C. However, based on the
data, the probability that an individual’s HbA1C would decrease is 61.8% (J. Cleveland,
personal communication, April 21, 2021).
Figure B
A Bayesian analysis was also used to reveal the results of each age group
mentioned previously (see Figure C). It does present that there is no statistically

19
significant difference in overall HbA1C values (by paired pre and post and by age range
category). Since the confidence interval includes zero, it could be possible that there was
no difference between pre and post and age-range status results for HbA1C (J. Cleveland,
personal communication, April 21, 2021).
Figure C
Results
Although each analysis shows no statistically significant difference, the study has
practical differences. The breakdown of the groups shows there was a decrease in
HbA1C in the group ages 56-65 over a three-month period. The age group of 46-55
remained about the same with an average mean of pre-HbA1C 7.20 and decreased to

20
HbA1C 7.17 during the three-month period. The other two groups showed a slight
increase in the HbA1C over the three-month period. Due to short duration of the study,
any decrease in HbA1C was significant. If the study is continued over the duration of a
year, the overall probability of potential decrease (61.8%) may increase and show
statistical significance (J. Cleveland, personal communication, April 21, 2021).
Interpretation/Discussion
Most society guidelines incorporate recommendations for hemoglobin A1C
monitoring and routine primary care visits in an effort to reduce the burden of diabetes
complications. In a 2018 national database study, patients who regularly received all the
recommended preventative measures, due to close follow-up, experienced a 20% risk
reduction in hospitalization (Albright & Fleischer, 2021). The participants in this study
state in the post-telephone survey that they did not have any hospitalizations during the
duration of this project. The results listed state the overall mean of A1C increased. A
few factors impacted this result. Multiple participant’s A1Cs remained the same. For
example, the pre-A1C was 7.2 and the post-A1C was 7.2. This is still a positive result
because the patient followed the protocol of taking medication regularly, continuing a
diabetic diet, and participating in monthly phone calls. Patients that showed a slight
increase in A1C in Group 1 had trouble accepting every phone call each month due to
work, appointments, or life events. Some of these patients did not always have weekly
glucose logs to present but would state they checked their glucose regularly. Group 4
included patients that had trouble recalling their diabetic medications and some found out
21
they were taking their medication incorrectly. When the patient would have an
appointment at the doctor's office, they would tell the provider that they were taking the
medications on file. For one participant, when asked specifically about each medication
on the initial phone call, the patient stated one could not afford the medicine prescribed
and was taking an old prescription found in the cabinet. The patient stated fear of
disappointing his/her doctor if the truth was told. Education was provided on the harmful
effects this could cause and the ways we could improve this situation.
One limitation of this study is the diabetic maturity of the participants. One
cannot ascertain that the length of time a participant has been a diabetic affects the
attitude towards the project and manner of one’s behavior. A participant who has been a
diabetic for a decade may be inflexible to change if they present with bad eating habits
and not taking their medication and vice versa a participant who has his/her regimen in
place with good habits may skew the results to look better. Another limitation is the
primary exposures and outcome variables such as blood glucose levels, diet, and
medication are self-reported. Self-reporting can be subject to bias among the
participants. Lastly, the data analysis was set to zero although the A1C will never be
zero. With adjustments, the data could change in the future.
The results help one to see the issues that occur in the primary care setting with
patients that do not improve and the reasons for their actions. It is important to see the
patients' improvements but it is also important to see the patients whose A1C did not
decrease. When reflecting on future recommendations, studies should include a larger
sample size in each age group to obtain more data. The data could include race/ethnicity,

22
financial status, and diabetic maturity (timeline since diagnosed with diabetes). Another
recommendation for further studies is a longer duration; the study should continue for at
least one year for more accurate data collection since three months is the recommended
amount of time to obtain an HbA1C. Future studies should consider including a
continuous glucose monitor to obtain more accurate readings from patients.
Cost-Benefit Analysis/Budget
No financial cost was obtained by the office for the project, but time was utilized
from providers and medical staff. If patients are in the CCM program, they were already
aware that their insurance is billed and there was a possibility of obtaining a bill that the
patient will bear if extra services were provided. Patients did not report any additional
fees incurred. This study did not charge any extra finances for the participants. Obtaining
cost or the lack thereof does not affect or benefit this project to monitor their diabetes.
Timeline
The project was originally developed beginning in the summer of 2020 and
implementation began the fall of 2020. Data collection lasted from January 2021 to April
2021, and the analysis was completed in April 2021. When considering the timeline from
start to finish, the project lasted 10 months.

23
Ethical Considerations/Protection of Human Subjects
The Jacksonville State University Institutional Review Board (IRB) approval
(Appendix A) was obtained before initiating the DNP project. All participants were
protected by the Health Insurance Portability and Accountability Act of 1996 (HIPAA).
All patients were coded to protect privacy and all identifiable criteria were removed from
any public reports. The author and personnel followed the standards of care for practice
in the clinical setting. All electronic files containing identifiable information were
password-protected to prevent access by unauthorized users. The project coordinator had
a personal login to electronic health records and all patient information were kept in the
office separate from anything submitted to JSU or taken to another location. No further
risks were introduced to patients other than the usual risks from receiving standard care.
Conclusion
Chronic conditions in the primary care setting must have close follow-up by
healthcare providers. Continuing to follow-up with patients can help decrease further
complications with these conditions, reduce hospitalizations, and ensure continuity of
care. This study showed that close follow-up with individuals with diabetes has the
potential to help decrease hemoglobin A1C in the adult population; therefore, decreasing
both current and future complications, and increasing the cooperation of patients with
their care. Nursing has a strong foundation based on promoting quality of life for
patients. This project reflects that goal and has potential to advance it within the

24
profession moving into the future. In addition, programs such as this can be used for
other chronic diseases. They will be essential moving into a time when chronic diseases
are on the rise and will likely continue to be due to a larger aging population.

25
REFERENCES
Albright, R. H., & Fleischer, A. E. (2021). Association of select preventative services and
hospitalization in people with diabetes. Journal of Diabetes & Its
Complications, three5(5), N.PAG.
https://doi.org/10.1016/j.jdiacomp.2021.10790three
American Diabetes Association. (2021). Diabetes symptoms. Retrieved from
https://www.diabetes.org/diabetes/type-2/symptoms
Aranha, A., Smitherman, H., Patel, D., & Patel, P. (2020). Association of hospital
readmissions and survivability with frailty and palliative performances scores
among long-term care residents. American Journal of Hospice & Palliative
Medicine, three7(9) 716-720. doi: 10.1177/1049909120907602
Bailey, M., Weiss, A., Barrett, M., Jiang, J. (2019). Characteristics of three0-day all-
cause hospital readmissions, 2010-2016. Agency for Healthcare Research and
Quality. Retrieved from https://www.hcup-us.ahrq.gov/reports.
Centers for Disease Control and Prevention (2021). What is diabetes? U.S. Department
of Health and Human Services. Retrieved from
https://www.cdc.gov/diabetes/basics/diabetes.html
Chen, M., & Grabowski, D. (2019). Hospital readmissions reduction program: Intended
and unintended effects. Medical Care Research and Review, 76(6) 643-660. doi:
10.1177/1077558717744611
Cleveland, J. (2021, April 21). Personal communication [Personal communication].

26
Cohen, B., Goldman, D., Ho, J., McFadden, D., Ryan, M., Tysinger, B. (2020). Improved
survival for individuals with common chronic conditions in the medicare
population. Health Economics, 1-12. doi:10.1002/hec.4168
Del Valle, K. L., & McDonnell, M. E. (2018). Chronic care management services for
complex diabetes management: a practical overview. Current Diabetes
Reports, 18(12), N.PAG. https://doi.org /10.1007/s11892-018-1118-x
Eroglu, N., & Sabuncu, N. (2021). The effect of education given to type 2 diabetic
individuals on diabetes self-management and self-efficacy: Randomized
controlled trial. Primary Care Diabetes, 15(3), 451–458. https://doi.org
/10.1016/j.pcd.2021.02.011
Gorina, M., Limonero, J. T., & Álvarez, M. (2018). Effectiveness of primary healthcare
educational interventions undertaken by nurses to improve chronic disease
management in patients with diabetes mellitus, hypertension and
hypercholesterolemia: A systematic review. International Journal of Nursing
Studies, 86, 139–150. https://doi.org /10.1016/j.ijnurstu.2018.06.016
Hodach, R. (2015). Making medicare’s chronic care management program work in
practice. Hfm (Healthcare Financial Management), 69(8), 112.
Hudali, T., Robinson, R., & Bhattari, M. (2017). Reducing three0-day rehospitalization
rates using a transition of care clinic model in a single medical center. Advances
in Medicine. doi:10.1155/2017/5132536
Jung, D., DuGoff, E., Smith, M., Palta, M., Gilmore-Bykovskyi, A., & Mullahy, J.
(2020). Likelihood of hospital readmission in medicare advantage and fee-for-

27
service within same hospital. Health Services Research, 55, 587-595. doi:
10.1111/1475-6773.13315
Neuman, B. (1982). The neuman systems model. Application to nursing education and
practice. Norwalk, CT: Appleton-Century Crofts.
Peplau, H. E. (1991). Interpersonal relations in nursing: A conceptual frame of reference
for psychodynamic nursing. Ukraine: Springer Publishing Company.
Rodriguez, L. A., Bradshaw, P. T., Shiboski, S. C., Fernandez, A., Vittinghoff, E.,
Herrington, D., Ding, J., & Kanaya, A. M. (2021). Examining if the relationship
between BMI and incident type 2 diabetes among middle–older aged adults varies
by race/ethnicity: evidence from the multi‐ethnic study of atherosclerosis
(MESA). Diabetic Medicine, 38(5), 1–8. https://doi.org/10.1111/dme.14377
Scott, N. (2018). Effective documentation and billing for chronic care management
according to the latest CMS guidelines. Briefings on APCs, 19(9), 6–8.
Shih, A. F., Buurman, B. M., Tynan, M. K., Tinetti, M. E., & Jenq, G. (2015). Views of
primary care physicians and home care nurses on the causes of readmission of
older adults. Journal of the American Geriatrics Society, 63(10), 2193–2196.
https://doi.org /10.1111/jgs.13681
U.S. Census Bureau. (2019). Quick Facts. Retrieved from
https://www.census.gov/quickfacts/pellcitycityalabama
Westphal, E. (2019). Managing chronic disease in an evolving healthcare environment:
Community-based organizations increasingly are addressing social determinants
of health, and preventing more expensive medical interventions. Generations, 4-7.

28
Wilson, C., O’Malley, A. S., Bozzolo, C., McCall, N., & Ma, S. (2019). Patient
experiences with chronic care management services and fees: A qualitative
study. JGIM: Journal of General Internal Medicine, 34(2), 250–255.
https://doi.org /10.1007/s11606-018-4750-x
Xing, J., Goehring, C., & Mancuso, D. (2015). Care coordination program for
Washington state Medicaid enrollees reduced inpatient hospital costs. Health
Affairs, 34(4), 653–661. https://doi.org /10.1377/hlthaff.2014.0655
29
APPENDIX A
October 30, 2020
Dear Adrienne Shambray:
Your proposal submitted for review by the Human Participants Review Protocol for the project titled: “Decreasing the Impact of Diabetes in the Adult and Elderly Rural Health Population Utilizing Phone Calls as Part of the Chronic Care Management Program” has been approved as exempt. If the project is still in process one year from now, you are asked to provide the IRB with a renewal application and a report on the progress of the research project.
Sincerely
Walsh ecutive Secretary, IRB
30
APPENDIX B
October 20, 2020 To whom it may concern:
Adrienne Shambray, Doctor of Nursing Practice (DNP), student at Jacksonville State University has permission to conduct a Quality Improvement DNP Project, titled — Decreasing the Impact of Diabetes in The Adult and Elderly' Rural Health Population Utilizing the Chronic Care Management Program. This DNP Project may be conducted at this facility.
Sincerely,
«?
Practice Administrator
31
APPENDIX C
CONSENT FOR PARTICIPATION IN A STUDY
Title of Project: Decreasing the Impact of Diabetes in the Older adults Rural Health
Population Utilizing Phone Calls as Part of the Chronic Care Management
Program
Investigator Names: Adrienne Shambray & Laura E. Barrow
E-Mail Contact Information: [email protected] , [email protected]
You are being asked to participate in a research study. Before you give your
consent to volunteer, it is important that you read the following information
and ask as many questions as necessary to be sure you understand what you
are being asked to do.
Investigators
Adrienne Shambray, MSN, CRNP, FNP-C
Laura E. Barrow, PhD, RN
Purpose of the Research
This project identifies patients who quality for the Chronic Care Management Program
(CCM) using criteria from of the Centers for Medicare and Medicaid Services and
who are currently diagnosed with Diabetes Mellitus. The project will utilize
monthly phone calls in order to better assist patients in managing their Diabetes.
Identifying any complications of this disease early may help reduce complications
and improve your overall quality of life.
32
Procedures
If you volunteer to participate in this study, you will be asked to agree to monthly phone
calls lasting approximately 20 to three0 minutes. These calls will focus on your
current illnesses, and specific questions about your Diabetes will be asked. You
will be asked to provide information about your daily blood glucose levels and
your daily medication.
Potential Risks or Discomforts
There are no foreseeable risks, however, you may experience positive or negative
feelings as you respond to questions. The phone calls will be scheduled during
business hours and at your convenience. There are no costs associated with your
participation in the study. You have the right to discontinue participation,
temporarily or permanently, without any consequence.
Potential Benefits of the Research
There are personal benefits for participating in the study. Your participation may identify
complications of your diabetes and lead to earlier treatment. The nursing
profession and clinical practice standards may increase due to the knowledge
obtained in this study.
Confidentiality and Data Storage
Identifying information will be confidential and not be shared with anyone outside the
study.
Data, specific to the study, will be stored in the researchers’ offices on a password-
protected computer. Following the completion of the project, the forms will be
destroyed six months after the study.

33
Questions, Participation, and Withdrawal
Your participation in this research study is voluntary. As a participant, you may refuse to
participate at any time. To withdraw from the study, please contact the researchers
at 205-201-three111, 256-490-three625, [email protected], or
Reasons for Exclusion from this Study
The exclusion criteria for this study include patients with the inability to speak English,
not qualifying for the CCM program, or with no diagnosis of diabetes mellitus 2.
34
APPENDIX D
Participate Information Form
Name:
Age:
Gender:
Self-identified ethnic identification:
A1C prior to entering program and initiating phone calls: ________________________
Self- reported glucose scores:
Any notes needed regarding glucose:
Self-reported medication reconciliation:
No problems identified: ______
Problems identified: ______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

35
Any actions taken by provider:
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
If this is month three, follow up A1C result:
______________