death certification. confirming death palpation for an arterial pulse (e.g. carotid) for at least...
TRANSCRIPT
Death Certification
Confirming death
• Palpation for an arterial pulse (e.g. carotid) for at least one minute.
• Auscultation of the heart for heart sounds for at least one minute
• Auscultation for breath sounds for at least one minute • Inspection of the pupils and examining for pupillary
reflexes (i.e. for fixed dilated pupils)(Note! that with some types of poisons (e.g. opiates) the pupils may be pinpoint)
• You may consider examining for reflexes including the corneal, gag and/or vestibulo-ocular reflexes.
• External appearance of the deceased
Confirming Death
– Pupils fixed and dilated
– No heart sounds for 30s
– No respiratory effort– No pulse at carotid for 30s
Document the above as well as date and time of death
Clearly identify yourself
Death Certification
• You can write a death certificate if:
– You provided care during the deceased’s last illness AND
– You have seen the person within 14 days of death OR after death
• i.e. practically speaking, in hospital you must have seen the patient before death
Talk to the Coroner if….• Death <24 hours after admission to hospital• no doctor has seen the patient in the last 14 days• the certifying doctor has not seen the body after death• the cause of death is unknown;• the death was violent or unnatural or suspicious;• the death may be due to an accident (whenever it occurred);• the death may be due to self-neglect or neglect by others;• the death may be due to an industrial disease or related to the deceased’s• employment;• the death may be due to an abortion; Doubtful stillbirth• the death occurred during an operation or before recovery from the effects of• an anaesthetic;• the death may be a suicide;• the death occurred during or shortly after detention in police or prison custody.• Unknown identity of deceased• Sudden suspicious death (homicide, suicide, accident)• Death due to drugs / alcohol
• Avoid abbreviations• Cause of death – if unsure seek advice
from senior – registrar, consultant• Part 1a – state the disease or pathology
eg MI, not the mode eg cardiac arrest• Part 1b – state the underlying disease• Part 2 – contributory cause, not part of the
main cause• Seal the certificate in an envelope
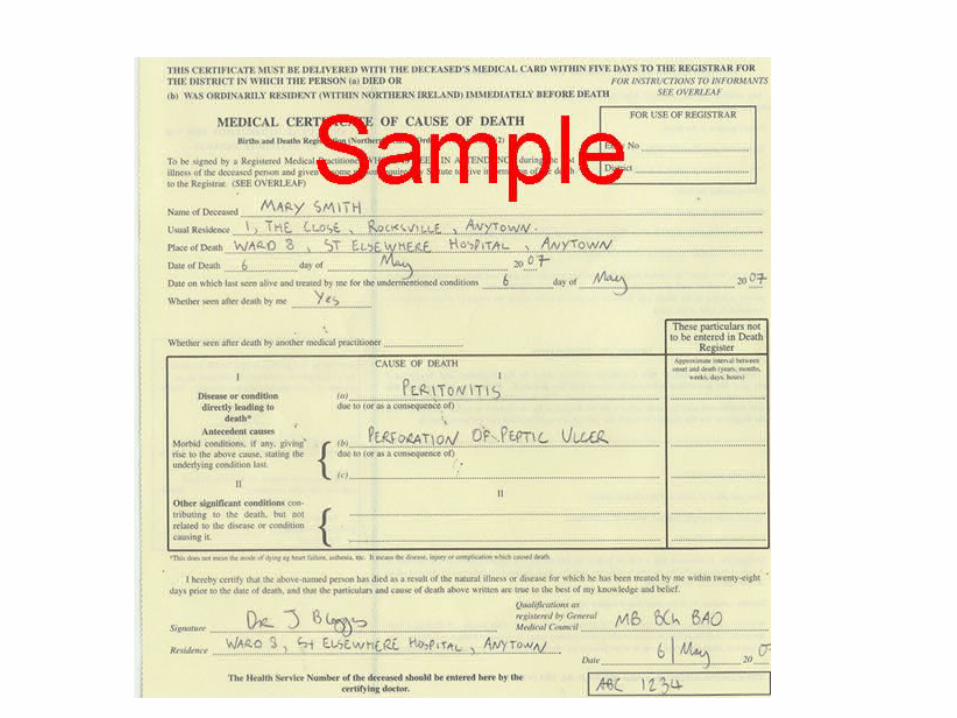
Medical Certificate of Cause of Death (MCCD)
• Name and place of death of deceased
• Date of death
• Age in years
• Date last seen alive
• Then circle1 The certified cause of death takes account of
information obtained from post mortem
2 Information from post mortem may be available later
3 Post mortem not being held
4 I have reported this death to the coroner for further action
• Then circlea seen after death by me
b seen after death by another medical practitioner but not me
c not seen after death by a medical practitioner
Cause of Death
• The tricky bit!
• List causes in order of immediacy
• Should be as specific as possible
• Causes not Modes of death
• Part II is not for all PMH, just relevant conditions
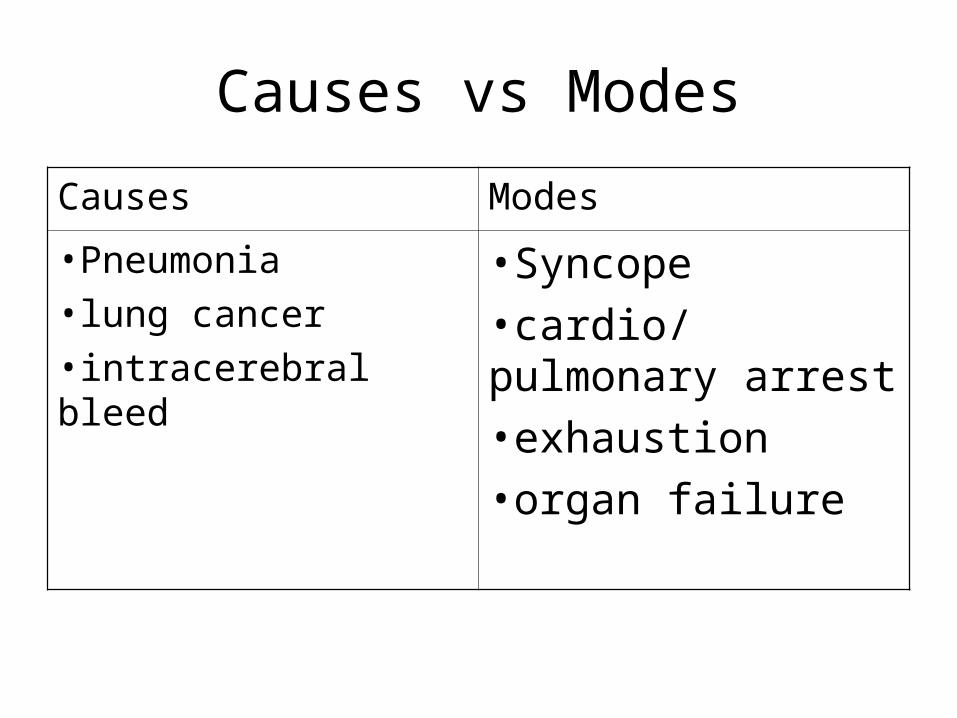
Causes vs Modes
Causes Modes
•Pneumonia •lung cancer •intracerebral bleed
•Syncope
•cardio/pulmonary arrest
•exhaustion
•organ failure
• If felt to be related to industrial disease tick the box on the front of the MCCD
• Sign, date and Print your name
• Give the name of the Consultant in charge of the patient
• Fill in the counterfoil in the book
• Example• A 76yr old retired school teacher was admitted with
collapse and hypotension. Her medical history included a hiatus hernia and recurrent indigestion. On examination she was hypotensive with generalized guarding and abdominal tenderness. An erect chest x-ray showed free gas under the diaphragm. A diagnosis of peritonitis secondary to a perforated peptic ulcer was made but her condition did not improve sufficiently to enable surgical intervention and she died four hours after admission.
Cremation Forms
• 2 doctors needed to sign• 1 should be someone who looked after the
patient, ideally whoever filled out the MCCD• 1 should have at least 5 years full GMC
registration and be unconnected with the patient• You must have seen the patient after death• You might have to go and retrieve pacemaker or
defibrillator

Post Mortems
2 types:• Coroners PM
– This is a legal requirement– Coroners officer will arrange a pathologist and
talk to the family
• Hospital PM– Very rare now– Team have to arrange a pathologist– Must also gain detailed consent from family
Case Studies
Case 1 – Mr Barry Ventricle
• You are the F1 doctor on a medical ward. Yesterday a 76 year old man was transferred to your care from CCU following an anterior myocardial infarction for which he received thrombolysis. He has a history of type 2 diabetes and hypertension. He was seen on the ward round by you and your consultant in the morning.
• Unfortunately that afternoon he suffers a VF arrest on the ward and dies despite the resuscitation efforts of yourself and the cardiac arrest team.
• The ward clerk asks you to fill in a death certificate and cremation form.
Case 2 – Mrs Phoebe Bleed
• You were on of the team on medical admissions on call yesterday evening. One of the patients you saw was a 65 year old woman with a history of poorly controlled hypertension who was admitted via A&E unconscious with a GCS of 3. A CT scan confirmed a massive intracerebral haemorrhage which wasn’t amenable to surgical intervention. She wasn’t expected to survive and was made “not for CPR”.
• The lady died overnight and was confirmed dead by one of the night team who hadn’t previously seen her.
• Today you are back on your own ward but you are bleeped by the ward clerk on MAU who asks you if you can fill in a death certificate
Case 3 – Mrs Sheila Cough • You are the F1 doctor on the ITU. You have been treating a 45 year
old lady, with a history of rheumatoid arthritis, on the unit for the past week who was originally admitted via the MAU with a severe community acquired pneumonia and multiple organ failure. Despite full supportive therapy, including renal support and broad spectrum antibiotics, she develops DIC and inotrope requirements are escalating.
• She is seen on the ward round by the consultant intensivist who decides to withdraw treatment after discussion with the family. She dies several hours later on the ITU after her ventilator is switched off.
• The family enquire of the patient’s nurse about a death certificate and cremation form who asks you to complete it.
Case 4 – Mr Thomas Shuffle
• You are the F2 doctor on the trauma ward. You admit an 85 year old man with Parkinson’s disease from a residential home after he falls and fractures his hip
• Unfortunately he develops pneumonia while waiting for an operating slot and dies.
• The ward sister asks you to complete a death certificate and cremation form quickly as the family are threatening to lodge a complaint.
Case 5 – Miss Amy Frail
• You are the F1 doctor on an elderly care ward. You have been looking after this 96 year old woman with a previous history of strokes and cognitive impairment for the past 2 weeks. She was originally admitted from her residential home with decreased mobility and treated successfully for a UTI. She has been waiting for a nursing home bed for the past week as her care needs have increased lately.
• Unfortunately she was found cold and dead in bed this morning by the morning nursing shift.
• You are asked to write a death certificate and cremation form by nursing staff
Case 6 – Mr James Bottle
• You are the F1 doctor on the gastroenterology ward. Two days ago you admitted from endoscopy a 56 year old publican with alcoholic cirrhosis who presented to A&E with haematemesis. The OGD demonstrated varices which were banded.
• Unfortunately he bled again overnight and died despite an urgent rescope.
• The ward clerk asks you if you will be able to complete a death certificate and cremation form as the family are enquiring.
Case 7 – Mr William Crab
• You are an F1 doctor on the acute assessment ward. Yesterday morning you admitted a 51 year old man with metastatic renal carcinoma and a history of angina. He had been complaining of significantly increased breathlessness over the past few days. A chest x-ray had shown only the established metastatic deposits and further investigations are awaited.
•• Unfortunately this afternoon he arrests and dies while
still on the AAU.• A member of his family approaches you and asks
whether you will be able to complete a death certificate.
Case 8 – Mrs Edna Muddle
• You are still the F1 doctor on the AAU. You admit a confused 80 year old from home but are unable to get much history from her as she is very disorientated.
• Unfortunately she arrests and dies shortly after you see her, although she had had bloods taken by the nursing staff prior to your assessment.
• You are asked to complete a death certificate and cremation form by nursing staff. You check her bloods and you notice a Troponin T of 9.34.
Any Questions?