dealer's greatest assets, inc. · dealer's greatest assets, inc. dear ... the rates and...
TRANSCRIPT

Benefit Booklet
July 1, 2017 - June 30, 2018
Dealer's Greatest Assets, Inc.

Dear Employee,
Once again, thank you for your commitment and dedication.
GBS Customer Service Rep Karen Munn (443) 589-1273 [email protected]
GBS Customer Service Rep Tonya Fowlkes (443) 589-1263 [email protected]
GBS Customer Service Rep Brianna Mistler (443) 589-1206 [email protected]
Life / AD&D The Hartford (860) 547-5000 www.thehartford.com
Medical CareFirst (888) 567-9155 www.carefirst.com
Dental CareFirst (866) 891-2802 www.carefirst.com
Welcome to Your Resources
We appreciate all of the hard work and effort that you put forth each and every day at Dealer's Greatest
Assets, Inc.. It's the dedication of our employees that separates us from our competitors. That's why we
offer a comprehensive employee benefits program so that, in addition to your paycheck, you and your
family may be relieved of some of the financial burdens of health care expenses.
We hope this employee benefit booklet helps you to better understand your benefits.
Benefit Name (Carrier/Rep) Phone Website/Email
Vision NVA Vision Program (443) 589-1240 www.e-nva.com

•Breast-feeding support, supplies & counseling •Domestic violence screening & counseling
•Contraception methods & counseling •Sexually transmitted disease counseling
•Gestational diabetes screening •Well-woman visits
•HIV screening & counseling
IRS Section 125 allows employees to make contributions for benefit costs on a pre-tax basis through salary reductions.
The employee will save Federal, State, Local, and Social Security/Medicare Tax on all of their tax-free premium
contributions. Depending on their income tax bracket, these savings could range anywhere from 30% to 55%.
PRE-TAX
(Household)
$40,000
$60,000
$80,000
$100,000
$120,000 $3,000
$2,500
$2,000
$1,500
$1,000
2016 & 2017- 2.5%
$2,400
$2,000
Health Care Reform Updates
Effective 2014, most individuals must be covered by a Qualified Health Insurance Plan that meets Minimum Essential
Coverage guidelines according to the Affordable Care Act (ACA). The chart below is an example of tax penalties in
2015 for non-compliance.
•Tax penalty for non-qualified HSA withdrawal
increased from 10% to 20%
INDIVIDUAL MANDATE
•Over-the-Counter medications no longer treated as
non-taxable unless prescribed by a doctor
•Medical Flexible Spending Account (FSA)
contributions are capped at $2,600 per employee,
per year (amount subject to change)
WOMEN'S PREVENTIVE CARE
The following list of women's preventive care services is an extension of the existing preventive care services that
went into effect under the health reform law dated Sept 23, 2010.
•Adult children coverage allowed to age 26
•No charge for preventive care
NOTE: This is meant to be an overview only. Please contact your HR administrator, broker, or GBS representative with more detailed questions.
GENERAL OVERVIEW
Beginning in 2011, several changes in health care regulations affected the way certain aspects of the health care
industry are treated. It is important that, as an employee, you understand these changes and how they impact your
health insurance benefits.
•Unlimited Lifetime Maximum
Adjusted Gross Income Annual Tax Penalty
$1,600
$1,200
$800
2015 - 2%

•Marriage or divorce
•Death of a spouse or child
•Loss of coverage
•Loss of dependent child status
Eligibility & Enrollment
Eligible Dependents
•Your unmarried child who, before the age of 19, became disabled by a mental or physical
handicap and is incapable of self-support
•Your children (until the last day of the month of their 26th birthday)
•Your spouse
Employees or dependents that choose not to
participate in the benefit program at time of initial
eligibility will be considered late applicants, subject
to the next open enrollment.
ELIGIBILITY & ENROLLMENT GUIDELINES
•Newborn or adopted dependents and newly eligible
grandchildren can be added within 31 days of birth,
adoption, or legal custody (proper documentation is
required to support adoption or legal custody)
•A dependent who loses coverage through a former
employer
•A newly married spouse can apply for coverage
within thirty (30) days of the date of marriage
All full-time employees (30+ hours per week) and their dependents are eligible to enroll in the company benefits. New
employees will become eligible for coverage on the 1st of the month following 60 days. All elections will remain in
effect and cannot be changed until the next open enrollment period (usually 12 months) unless a qualifying life event
occurs.
Qualifying Events Exceptions
•Termination of a spouse's employment or
significant change in health coverage (cost)
attributable to the spouse's employment

Enrollment TierEmployee Only $68.46 $120.59 $151.92
Employee/Spouse $290.93 $410.83 $482.91
Employee/Child(ren) $213.92 $310.36 $368.33
Family $417.57 $576.05 $671.31
HB Adv CDH Opt. E-S HSA
$2000BC Adv Opt.4-S $2000 BC Adv Opt.2-S $500
Benefits In-Network In-Network In-Network
Deductible (Ind/Fam) $2,000/$4,000 $2,000/$4,000 $500/$1,000
Out-of-Pocket Max (Ind/Fam) $4,500/$6,550 $6,850/$13,700 $4,500/$9000
Co-Insurance 100% 100% 100%
Primary Care No Charge after ded $20 $10
Specialist $30 after ded $40 $20
Inpatient Hospital $300/day after ded up to 5 days $300/day after ded up to 5 days $300/day after ded up to 5 days
Mental Health Inpatient $300/day after ded up to 5 days $300/day after ded up to 5 days $300/day after ded up to 5 days
Outpatient Facility $300 after ded FS -$100/H-$200 after ded FS-$100/H-$200 after ded
Lab/X-RayLab-FS-No charge after ded / H-
$100 after ded; X-Ray-FS $50 after
ded / H-$150 after ded
Lab-FS-$20 / H-$100 after ded; X-
Ray-FS $40 / H-$150 after ded
Lab-FS-$10 / H-$100 after ded; X-
Ray-FS $20 / H-$150 after ded
Mental Health Outpatient No Charge after ded $80 $60
Emergency Room$200 (waived if admitted)
after ded
$200 (waived if admitted)
after ded
$200 (waived if admitted)
after ded
Urgent Care $50 after ded $60 $40
Prescription Drugs 0/25/45/int ded 10/30/60/$0 10/30/60/$0
Medical Plans
The rates and benefits in this report are for presentation purposes only and do not constitute an offer of insurance.
Each eligible employee will be able to choose from the available medical plans. For an overview of each medical plan,
please refer to this page. To find a provider, go to www.carefirst.com and utilize the 'Find a Provider' feature, or call
(888) 567-9155 for a list of providers near you.
Per Pay Deduction: 26 Pays - Bi-Weekly
Legend: Generic/Preferred Brand/Non-Preferred Brand/Deductible
Cost Share Information
Office Visits
Inpatient Services
Outpatient Services
Emergency Care
Prescription Drugs

HealthyBlue Advantage HSA/HRA Integrated Deductible Summary of Benefits
Services In-Network You Pay1,2 Out-of-Network You Pay1,3
Visit www.carefirst.com/doctor to locate providers and facilities
FIRSTHELP—24/7 NURSE ADVICE LINE
Free advice from a registered nurse. Visit www.carefirst.com/needcare to learn more about your options for care.
When your doctor is not available, call FirstHelp at 800-535-9700 to speak with a registered nurse about your health questions and treatment options.
BLUE REWARDS
Visit www.carefirst.com/bluerewards for more information
Blue Rewards is an incentive program where you can earn up to $300 for taking an active role in getting healthy and staying healthy.
ANNUAL MEDICAL DEDUCTIBLE (Benefit Period)4
Individual $2,000 $4,500
Family $4,000 $9,000
ANNUAL OUT-OF-POCKET MAXIMUM (Benefit Period)5
Medical6 $4,500 Individual/$6,550 Family $6,000 Individual/$12,000 Family
Prescription Drug6 Combined with in-network out-of-pocket maximum
All drug costs are subject to in-network out-of-pocket maximum
PREVENTIVE SERVICES
Well-Child Care (including exams & immunizations)
No charge* No charge* after deductible
Adult Physical Examination (including routine GYN visit)
No charge* No charge* after deductible
Breast Cancer Screening No charge* No charge*
Pap Test No charge* No charge* after deductible
Prostate Cancer Screening No charge* No charge* after deductible
Colorectal Cancer Screening No charge* No charge* after deductible
PCP AND SPECIALIST SERVICES
FACILITY CHARGE7—In addition to the physician copays/coinsurances listed below, if a service is rendered on a hospital campus, ADD facility charge if applicable
Deductible, then $200 per visit Deductible, then $500 per visit
Office Visits for Illness—PCP7,8 No charge* after deductible Deductible, then $50 per visit
Convenience Care (retail health clinics such as CVS MinuteClinic or Walgreens Healthcare Clinic)
No charge* after deductible Deductible, then $50 per visit
Office Visits for Illness—Specialist7,8 Deductible, then $30 per visit Deductible, then $50 per visit
Allergy Testing7 No charge* after deductible PCP/Deductible, then $30 per Specialist visit
Deductible, then $50 per visit
Allergy Shots7 No charge* after deductible PCP/Deductible, then $30 per Specialist visit
Deductible, then $50 per visit
Physical, Speech, and Occupational Therapy7,9 (limited to 30 visits/injury/benefit period)
Deductible, then $30 per visit Deductible, then $50 per visit
Chiropractic Services7 (limited to 20 visits/benefit period)
Deductible, then $30 per visit Deductible, then $50 per visit
Acupuncture7 (limited to 20 visits/benefit period)
Deductible, then $30 per visit Deductible, then $50 per visit
EMERGENCY SERVICES
Urgent Care Center10 (such as Patient First or Express Care)
Deductible, then $50 per visit In-network deductible, then $50 per visit
Hospital Emergency Room Services10
■ FacilityDeductible, then $200 per visit (waived if admitted)
In-network deductible, then $200 per visit (waived if admitted)
■ Physician No charge* after deductible No charge* after in-network deductible
Ambulance10 (if medically necessary) Deductible, then $50 per service In-network deductible, then $50 per service
SUM3342-1P (3/17) ■ MD ■ 51+ Option E-S (Smart Selections)

Services In-Network You Pay1 Out-of-Network You Pay1
DIAGNOSTIC SERVICES
Labs11
■ Non-Hospital/Freestanding Facility No charge* after deductible Deductible, then $50 per visit
■ Hospital Deductible, then $100 per visit Deductible, then $200 per visit
X-ray
■ Non-Hospital/Freestanding Facility Deductible, then $50 per visit Deductible, then $50 per visit
■ Hospital Deductible, then $150 per visit Deductible, then $200 per visit
Imaging
■ Non-Hospital/Freestanding Facility Deductible, then $100 per visit Deductible, then $200 per visit
■ Hospital Deductible, then $200 per visit Deductible, then $500 per visit
HOSPITALIZATION—(Members are responsible for both physician and facility fees)
Outpatient Surgical Center Services ■ Facility Deductible, then $100 per visit Deductible, then $500 per visit ■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
Outpatient Hospital Surgical Services ■ Facility Deductible, then $300 per visit Deductible, then $500 per visit ■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
Inpatient Hospital Services
■ FacilityDeductible, then $300 per day ($1,500 maximum per admission)
Deductible, then $500 per day ($2,500 maximum per admission)
■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
HOSPITAL ALTERNATIVES
Home Health Care Deductible, then $30 per visit Deductible, then $50 per visit
Hospice (Inpatient—limited to 30 days; Outpatient—unlimited during Hospice eligibility period)
Deductible, then $30 per visit Deductible, then $50 per visit
Skilled Nursing Facility (limited to 60 days/benefit period)
Deductible, then $30 per admission Deductible, then $50 per admission
MATERNITY
Preventive Prenatal and Postnatal Office Visits No charge* Deductible, then $50 per visit
Delivery and Facility Services Deductible, then $300 per day ($1,500 maximum per admission)
Deductible, then $500 per day ($2,500 maximum per admission)
Artificial and Intrauterine Insemination7,12 (limited to 6 attempts per live birth)
Deductible, then $30 per visit Deductible, then $50 per visit
In Vitro Fertilization Procedures7,12 (limited to 3 attempts per live birth up to $100,000 lifetime maximum)
Deductible, then $30 per visit Deductible, then $50 per visit
MENTAL HEALTH AND SUBSTANCE ABUSE—(Members are responsible for both physician and facility fees)
Office Visits No charge* after deductible Deductible, then $50 per visit
Outpatient Services
■ Facility No charge* after deductible Deductible, then $50 per visit
■ Physician No charge* after deductible Deductible, then $50 per visit
Inpatient Services
■ Facility Deductible, then $300 per day ($1,500 maximum per admission)
Deductible, then $500 per day ($2,500 maximum per admission)
■ Physician Deductible, then $30 per visit Deductible, then $50 per visit
MEDICAL DEVICES AND SUPPLIES
Durable Medical Equipment No charge* after deductible Deductible, then 20% of Allowed Benefit
Hearings Aids for ages 0-18 (limited to one hearing aid per hearing-impaired ear every 3 years)
No charge* after deductible Deductible, then 20% of Allowed Benefit
VISION
Routine Exam (limited to 1 visit/benefit period)
$10 per visit at participating vision provider Total charge minus $33 Allowed Benefit
Eyeglasses and Contact Lenses Discounts from participating vision centers Not covered
SUM3342-1P (3/17) ■ MD ■ 51+ Option E-S (Smart Selections)

Note: Allowed Benefit is the fee that participating, in-network providers have agreed to accept for a particular covered service. The provider cannot charge the member more than this amount for any covered service. Example: Dr. Carson charges $100 to see a sick patient. To be part of CareFirst’s network, he has agreed to accept $50 for the visit. The member will pay their copay/coinsurance and deductible (if applicable) and CareFirst will pay the remaining amount up to $50.
* No copayment or coinsurance.1 When multiple services are rendered on the same day by more than one provider, Member payments are required for each provider.2 In-Network: When covered services are rendered in Maryland, Washington D.C. and/or Northern Virginia, collectively known as the CareFirst BlueChoice service area, by a
provider in the CareFirst BlueChoice Provider network, care is reimbursed at the in-network level. In-network benefits are based on the CareFirst BlueChoice Allowed Benefit. The CareFirst BlueChoice Allowed Benefit is generally the contracted rates or fee schedules that CareFirst BlueChoice providers have agreed to accept as payment for covered services. These payments are established by CareFirst BlueChoice, Inc., however, in certain circumstances, an allowance may be established by law. Outside of the CareFirst BlueChoice service area, when covered services are rendered by a provider in the preferred provider network, care is also covered at the in-network level. These in-network benefits are based on the contracted rates or fee schedules that preferred providers have agreed to accept as payment for covered services that are established by the local Blue Cross and Blue Shield Plan, however, in certain circumstances, an allowance may be established by law.
3 Out-of-Network: When covered services are rendered by a provider that is not in the CareFirst BlueChoice network in Maryland, Washington D.C. or Northern Virginia, or isnot in the preferred provider network outside of CareFirst BlueChoice service area, the care is reimbursed as out-of-network. Out-of-network benefits are based on the Allowed Benefit. The Allowed Benefit is generally the contracted rates or fee schedules that are established by CareFirst BlueChoice, or the local Blue Cross and Blue Shield Plan, however, in certain circumstances, an allowance may be established by law.
4 For family coverage only: The family deductible must be met before any member starts receiving benefits. The deductible may be met by one member or any combination of members.
5 For family coverage only: The family out-of-pocket maximum must be met before any member's services will be covered at 100% up to the Allowed Benefit. The out-of-pocket maximum may be met by one member or any combination of members.
6 Plan has an integrated medical and prescription drug out-of-pocket maximum.7 If a service is rendered on a hospital campus you could receive two bills, one from the physician and one from the facility.8 “Telemedicine services” refers to the use of a combination of interactive audio, video, or other electronic media used for the purpose of diagnosis, consultation, or treatment. Use
of audio-only telephone, electronic mail message (e-mail), or facsimile transmission (FAX) is not considered a telemedicine service.9 There are no limits for children until the end of the month in which the insured or enrollee turns 19 years of age when Physical, Speech or Occupational Therapy is included as
part of Habilitative Services.10 If the out-of-network benefit is listed as contributing toward the in-network deductible, then it also contributes toward the in-network out-of-pocket maximum.11 Members accessing laboratory services inside the CareFirst Service area (Maryland, D.C., Northern Virginia) must use LabCorp as their Lab Test facility and a non-hospital/
freestanding facility for X-rays and specialty Imaging for In-Network benefits. Services performed by any other provider, while inside the CareFirst Service area will be considered Out-of-Network. Members accessing laboratory, X-rays, and specialty Imaging services outside of Maryland, D.C. or Northern Virginia, may use any participating BlueCard PPO facility and receive in-network benefits.
12 Members who are unable to conceive have coverage for the evaluation of infertility services performed to confirm an infertility diagnosis, and some treatment options forinfertility. Preauthorization required
Not all services and procedures are covered by your benefits contract. This summary is for comparison purposes only and does not create rights not given through the benefit plan.
The benefits described are issued under form numbers: MD/CFBC/GC (R. 1/13); MD/CFBC/HBADV/EOC (7/12); MD/CFBC/DOL APPEAL (R. (9/11); MD/CFBC/LG/POS/DOCS (6/16); MD/CFBC/LG/POS/SOB (6/16); MD/BV/OON/VISION (3/12); MD/CFBC/RX (R. 1/16); MD/CFBC/INCENT (1/16); MD/CFBC/ELIG (R. 10/10) and any amendments.
SUM3342-1P (3/17) ■ MD ■ 51+ Option E-S (Smart Selections)
www.carefirst.com
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst MedPlus is the business name of First Care, Inc. CareFirst BlueCross BlueShield, First Care, Inc., and CareFirst BlueChoice, Inc., are independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.

Pharmacy ProgramIntegrated Deductible
See Annual Deductible on Medical Summary of Benefits $0/0/25/45 Retail Copays n 50% Injectables Coinsurance
Summary of BenefitsPlan Feature Amount DescriptionDeductible See medical summary
of benefit for annual deductible amount
If you meet your combined medical and drug deductible, you will pay a different copay or coinsurance depending on the drug tier. Drugs not subject to any medical or drug deductible are noted below.
Out-of-Pocket Maximum See medical summary of benefit for annual out‑of‑pocket amount
If you reach your out‑of‑pocket maximum, CareFirst BlueChoice will pay 100% of the applicable allowed benefit for most covered services for the remainder of the year. All deductibles, copays, coinsurance, and other eligible out‑of‑pocket costs count toward your out‑of‑pocket maximum except balanced billed amounts.
Preventive Drugs (Affordable Care Act) (up to a 34‑day supply)
$0 (Not subject to deductible)
A preventive drug is a prescribed medication or item on CareFirst’s Preventive Drug List (ACA)* (examples: Folic Acid, Fluoride, and FDA approved contraceptives for women).
Oral Chemotherapy Drugs Diabetic Supplies (up to a 34‑day supply)
$0 (Not subject to deductible except for HSA plans)
Diabetic supplies include needles, lancets, test strips and alcohol swabs.
Generic Drugs (Tier 1) – HealthyBlue Select Generics (up to a 34‑day supply)
$0 (Not subject to deductible)
See complete list of HealthyBlue Select generic drugs at www.carefirst.com/hbselectgenerics or call 800-241-3371.
Generic Drugs (Tier 1) (up to a 34‑day supply)
$0 Generic drugs (except Preventive Drugs) are covered at this level.
Preferred Brand Drugs (Tier 2) (up to a 34‑day supply)
$25 All preferred brand drugs are covered at this copay level.
Non-preferred Brand Drugs (Tier 3) (up to a 34‑day supply)
$45 All non‑preferred brand drugs on this copay level are not on the Preferred Drug List.* Discuss using alternatives with your physician or pharmacist.
Self-administered Injectable (excluding insulin) (Tier 4) (up to a 34‑day supply)
50% coinsurance up to a maximum payment of $75
All self‑administered injectable drugs (excluding insulin) are covered at this payment level. Insulin is covered at appropriate copay level.
Maintenance Drugs (up to a 90‑day supply)
Generic: $0 Preferred Brand: $50 Non‑preferred Brand: $90 Self‑Administered Injectables: 50% coinsurance, up to a maximum payment of $150
Maintenance drugs of up to a 90‑day supply are available for twice the copay through Mail Service Pharmacy or a retail pharmacy. Injectables (excluding insulin) are covered at 50% coinsurance up to a maximum payment of $150.
Restricted Generic Substitution Yes If a provider prescribes a non‑preferred brand drug when a generic is available, you will pay the non‑preferred brand copay or coinsurance PLUS the cost difference between the generic and brand drug up to the cost of the prescription. If a generic version is not available, you will only pay the copay or coinsurance. Also, if your prescription is written for a brand‑name drug and DAW (dispense as written) is noted by your doctor, you will only pay the copay.
Visit www.carefirst.com/rx for the most up-to-date Preferred Drug List and Formulary (list of covered drugs), including the prescription guidelines. Prescription guidelines indicate drugs that require your doctor to obtain prior authorization from CareFirst before they can be filled and drugs that can be filled in limited quantities.
This plan summary is for comparison purposes only and does not create rights not given through the benefit plan.
Policy Form Numbers: MD/CFBC/RX (R. 1/15)
SUM1861-1P (1/17) n MD
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst of Maryland, Inc., Group Hospitalization and Medical Services, Inc., and CareFirst BlueChoice, Inc. are independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association.

BlueChoice Advantage Non-Integrated Deductible Summary of Benefits
Services In-Network You Pay1,2 Out-of-Network You Pay1,3
Visit www.carefirst.com/doctor to locate providers and facilities
FIRSTHELP—24/7 NURSE ADVICE LINE
Free advice from a registered nurse. Visit www.carefirst.com/needcare to learn more about your options for care.
When your doctor is not available, call FirstHelp at 800-535-9700 to speak with a registered nurse about your health questions and treatment options.
BLUE REWARDS
Visit www.carefirst.com/bluerewards for more information
Blue Rewards is an incentive program where you can earn up to $300 for taking an active role in getting healthy and staying healthy.
ANNUAL MEDICAL DEDUCTIBLE (Benefit Period)4
Individual $2,000 $4,000
Family $4,000 $8,000
ANNUAL OUT-OF-POCKET MAXIMUM (Benefit Period)5
Medical6 $6,850 Individual/$13,700 Family $7,850 Individual/$15,700 Family
Prescription Drug6 Combined with in-network out-of-pocket maximum
All drug costs are subject to in-network out-of-pocket maximum
PREVENTIVE SERVICES
Well-Child Care (including exams & immunizations)
No charge* No charge*
Adult Physical Examination (including routine GYN visit)
No charge* No charge* after deductible
Breast Cancer Screening No charge* No charge*
Pap Test No charge* No charge* after deductible
Prostate Cancer Screening No charge* No charge* after deductible
Colorectal Cancer Screening No charge* No charge* after deductible
PCP AND SPECIALIST SERVICES
FACILITY CHARGE7—In addition to the physician copays/coinsurances listed below, if a service is rendered on a hospital campus, ADD facility charge if applicable
$200 per visit Deductible, then 20% of Allowed Benefit
Office Visits for Illness—PCP7,8 $20 per visit Deductible, then 20% of Allowed Benefit
Convenience Care (retail health clinics such as CVS MinuteClinic or Walgreens Healthcare Clinic)
$20 per visit Deductible, then 20% of Allowed Benefit
Office Visits for Illness—Specialist7,8 $40 per visit Deductible, then 20% of Allowed Benefit
Allergy Testing7 $40 per visit Deductible, then 20% of Allowed Benefit
Allergy Shots7 $40 per visit Deductible, then 20% of Allowed Benefit
Physical, Speech, and Occupational Therapy7,9
(limited to 30 visits/benefit period)$40 per visit Deductible, then 20% of Allowed Benefit
Chiropractic Services7
(limited to 20 visits/benefit period)$40 per visit Deductible, then 20% of Allowed Benefit
Acupuncture7,9
(limited to 20 visits/benefit period)$40 per visit Deductible, then 20% of Allowed Benefit
EMERGENCY SERVICES
Urgent Care Center10
(such as Patient First or Express Care)$60 per visit $60 per visit
Hospital Emergency Room Services10
■ Facility Deductible, then $200 per visit (waived if admitted)
In-network deductible, then $200 per visit (waived if admitted)
■ Physician No charge* after deductible No charge* after in-network deductible
Ambulance10 (if medically necessary) Deductible, then $50 per service In-network deductible, then $50 per service
SUM3270-1P (3/17) ■ MD ■ 51+ Option 4-S (Smart Selections)

Services In-Network You Pay1,2 Out-of-Network You Pay1,3
DIAGNOSTIC SERVICES
Labs11
■ Non-Hospital/Freestanding Facility $20 per visit Deductible, then 20% of Allowed Benefit ■ Hospital Deductible, then $100 per visit Deductible, then 20% of Allowed Benefit
X-ray ■ Non-Hospital/Freestanding Facility $40 per visit Deductible, then 20% of Allowed Benefit ■ Hospital Deductible, then $150 per visit Deductible, then 20% of Allowed Benefit
Imaging ■ Non-Hospital/Freestanding Facility $80 per visit Deductible, then 20% of Allowed Benefit ■ Hospital Deductible, then $200 per visit Deductible, then 20% of Allowed Benefit
HOSPITALIZATION—(Members are responsible for both physician and facility fees)
Outpatient Surgical Center Services ■ Facility $100 per visit Deductible, then 20% of Allowed Benefit ■ Physician $40 per visit Deductible, then 20% of Allowed Benefit
Outpatient Hospital Surgical Services ■ Facility Deductible, then $200 per visit Deductible, then 20% of Allowed Benefit ■ Physician Deductible, then $40 per visit Deductible, then 20% of Allowed Benefit
Inpatient Hospital Services
■ FacilityDeductible, then $300 per day ($1,500 maximum per admission)
Deductible, then 20% of Allowed Benefit
■ Physician Deductible, then $40 per visit Deductible, then 20% of Allowed Benefit
HOSPITAL ALTERNATIVES
Home Health Care No charge* Deductible, then 20% of Allowed Benefit
Hospice (Inpatient—limited to 30 days; Outpatient—unlimited during Hospice eligibility period)
No charge* Deductible, then 20% of Allowed Benefit
Skilled Nursing Facility (limited to 60 days/benefit period)
Deductible, then $200 per admission Deductible, then 20% of Allowed Benefit
MATERNITY
Preventive Prenatal and Postnatal Office Visits No charge* Deductible, then 20% of Allowed Benefit
Delivery and Facility Services Deductible, then $300 per day ($1,500 maximum per admission)
Deductible, then 20% of Allowed Benefit
Artificial and Intrauterine Insemination7,12
(limited to 6 attempts per live birth)Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
In Vitro Fertilization Procedures7,12
(limited to 3 attempts per live birth up to $100,000 lifetime maximum)
Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
MENTAL HEALTH AND SUBSTANCE ABUSE—(Members are responsible for both physician and facility fees)
Office Visits $20 per visit Deductible, then 20% of Allowed Benefit
Outpatient Services
■ Facility $80 per visit Deductible, then 20% of Allowed Benefit
■ Physician $40 per visit Deductible, then 20% of Allowed Benefit
Inpatient Services
■ Facility Deductible, then $300 per day ($1,500 maximum per admission)
Deductible, then 20% of Allowed Benefit
■ Physician Deductible, then $40 per visit Deductible, then 20% of Allowed Benefit
MEDICAL DEVICES AND SUPPLIES
Durable Medical Equipment Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
Hearings Aids for ages 0-18 (limited to one hearing aid per hearing-impaired ear every 3 years)
No charge* Deductible, then 20% of Allowed Benefit
VISION
Routine Exam (limited to 1 visit/benefit period)
$10 per visit at participating vision provider Total charge minus $33 Allowed Benefit
Eyeglasses and Contact Lenses Discounts from participating vision centers Not covered
SUM3270-1P (3/17) ■ MD ■ 51+ Option 4-S (Smart Selections)

Note: Allowed Benefit is the fee that participating, in-network providers have agreed to accept for a particular covered service. The provider cannot charge the member more than this amount for any covered service. Example: Dr. Carson charges $100 to see a sick patient. To be part of CareFirst’s network, he has agreed to accept $50 for the visit. The member will pay their copay/coinsurance and deductible (if applicable) and CareFirst will pay the remaining amount up to $50.
* No copayment or coinsurance.1 When multiple services are rendered on the same day by more than one provider, Member payments are required for each provider.2 In-Network: When covered services are rendered in Maryland, Washington D.C. and/or Northern Virginia, collectively known as the CareFirst BlueChoice service area, by a
provider in the CareFirst BlueChoice Provider network, care is reimbursed at the in-network level. In-network benefits are based on the CareFirst BlueChoice Allowed Benefit. The CareFirst BlueChoice Allowed Benefit is generally the contracted rates or fee schedules that CareFirst BlueChoice providers have agreed to accept as payment for covered services. These payments are established by CareFirst BlueChoice, Inc., however, in certain circumstances, an allowance may be established by law. Outside of the CareFirst BlueChoice service area, when covered services are rendered by a provider in the preferred provider network, care is also covered at the in-network level. These in-network benefits are based on the contracted rates or fee schedules that preferred providers have agreed to accept as payment for covered services that are established by the local Blue Cross and Blue Shield Plan, however, in certain circumstances, an allowance may be established by law.
3 Out-of-Network: When covered services are rendered by a provider that is not in the CareFirst BlueChoice network in Maryland, Washington D.C. or Northern Virginia, or isnot in the preferred provider network outside of CareFirst BlueChoice service area, the care is reimbursed as out-of-network. Out-of-network benefits are based on the Allowed Benefit. The Allowed Benefit is generally the contracted rates or fee schedules that are established by CareFirst BlueChoice, or the local Blue Cross and Blue Shield Plan, however, in certain circumstances, an allowance may be established by law.
4 For Family coverage only: When one family member meets the individual deductible, they can start receiving benefits. Each family member cannot contribute more than the individual deductible amount. The family deductible must be met before the remaining family members can start receiving benefits.
5 For Family coverage only: When one family member meets the individual out-of-pocket maximum, their services will be covered at 100% up to the Allowed Benefit. Each family member cannot contribute more than the individual out-of-pocket maximum amount. The family out-of-pocket maximum must be met before the services for all remaining family members will be covered at 100% up to the Allowed Benefit.
6 Plan has separate out-of-pocket maximums for medical and drug expenses which accumulate independently.7 If a service is rendered on a hospital campus you could receive two bills, one from the physician and one from the facility.8 “Telemedicine services” refers to the use of a combination of interactive audio, video, or other electronic media used for the purpose of diagnosis, consultation, or treatment. Use
of audio-only telephone, electronic mail message (e-mail), or facsimile transmission (FAX) is not considered a telemedicine service.9 There are no limits for children until the end of the month in which the insured or enrollee turns 19 years of age when Physical, Speech or Occupational Therapy is included as
part of Habilitative Services.10 If the out-of-network benefit is listed as contributing toward the in-network deductible, then it also contributes toward the in-network out-of-pocket maximum.11 Members accessing laboratory services inside the CareFirst Service area (Maryland, D.C., Northern Virginia) must use LabCorp as their Lab Test facility and a non-hospital/
freestanding facility for X-rays and specialty Imaging for In-Network benefits. Services performed by any other provider, while inside the CareFirst Service area will be considered Out-of-Network. Members accessing laboratory, X-rays, and specialty Imaging services outside of Maryland, D.C. or Northern Virginia, may use any participating BlueCard PPO facility and receive in-network benefits.
12 Members who are unable to conceive have coverage for the evaluation of infertility services performed to confirm an infertility diagnosis, and some treatment options forinfertility. Preauthorization required
Not all services and procedures are covered by your benefits contract. This summary is for comparison purposes only and does not create rights not given through the benefit plan.
The benefits described are issued under form numbers: MD/CFBC/GC (R. 1/13); MD/CFBC/HPN/EOC (R. 6/10); MD/CFBC/DOL APPEAL (R. 9/11); MD/CFBC/LG/POS/DOCS (6/16); MD/CFBC/LG/POS/SOB (6/16); MD/CFBC/ELIG (R. 7/09); MD/CFBC/RX (R. 1/16); MD/CFBC/INCENT (1/16) and any amendments.
SUM3270-1P (3/17) ■ MD ■ 51+ Option 4-S (Smart Selections)
www.carefirst.com
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst MedPlus is the business name of First Care, Inc. CareFirst BlueCross BlueShield, First Care, Inc., and CareFirst BlueChoice, Inc., are independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.

Pharmacy Program$0 Deductible n $0/10/30/60 Retail Copays
50% Injectables Coinsurance
Summary of BenefitsPlan Feature Amount DescriptionIndividual Deductible None Your benefit does not have a deductible.
Family Deductible None Your benefit does not have a family deductible.
Out-of-Pocket Maximum See medical summary of benefits for annual out‑of‑pocket amount
If you reach your out‑of‑pocket maximum, CareFirst or CareFirst BlueChoice will pay 100% of the applicable allowed benefit for most covered services for the remainder of the year. All deductibles, copays, coinsurance and other eligible out‑of‑pocket costs count toward your out‑of‑pocket maximum, except balance billed amounts.
Preventive Drugs (Affordable Care Act) (up to a 34‑day supply)
$0 (not subject to deductible)
A preventive drug is a prescribed medication or item on CareFirst’s Preventive Drug List (ACA).* (Examples: Folic Acid, Fluoride and FDA approved contraceptives for women.)
Oral Chemotherapy Drugs Diabetic Supplies (up to a 34‑day supply)
$0 (not subject to deductible except for HSA Plans)
Diabetic supplies include needles, lancets, test strips and alcohol swabs.
Generic Drugs – (Tier 1) (up to a 34‑day supply)
$10 Generic drugs are covered at this copay level.
Preferred Brand Drugs (Tier 2) (up to a 34‑day supply)
$30 All preferred brand drugs are covered at this copay level.
Non-preferred Brand Drugs (Tier 3) (up to a 34‑day supply)
$60 All non‑preferred brand drugs on this copay level are not on the Preferred Drug List.* Discuss using alternatives with your physician or pharmacist.
Self-administered Injectable (excluding insulin) (Tier 4) (up to a 34‑day supply)
50% coinsurance up to a maximum payment of $150
All self‑administered injectable drugs (excluding insulin) are covered at this payment level. Insulin is covered at appropriate copay level.
Maintenance Drugs (up to a 90‑day supply)
Generic: $20 Preferred Brand: $60 Non‑preferred Brand: $120 Self‑Administered Injectables: 50% coinsurance, up to a maximum payment of $300
Maintenance drugs of up to a 90‑day supply are available for twice the copay through Mail Service Pharmacy or a retail pharmacy. Injectables (excluding insulin) are covered at 50% coinsurance up to a maximum payment of $300.
Restricted Generic Substitution Yes If a provider prescribes a non‑preferred brand drug when a generic is available, you will pay the non‑preferred brand copay or coinsurance PLUS the cost difference between the generic and brand drug up to the cost of the prescription. If a generic version is not available, you will only pay the copay or coinsurance. Also, if your prescription is written for a brand‑name drug and DAW (dispense as written) is noted by your doctor, you will only pay the copay.
Visit www.carefirst.com/rx for the most up-to-date Preferred Drug List and Formulary (list of covered drugs), including the prescription guidelines. Prescription guidelines indicate drugs that require your doctor to obtain prior authorization from CareFirst before they can be filled and drugs that can be filled in limited quantities.
This plan summary is for comparison purposes only and does not create rights not given through the benefit plan.
Policy Form Numbers: MD/CFBC/RX (R. 7/12) • MD/CF/RX (R. 7/12) • CFMI/51+/RX (R. 7/12)
SUM3400-1P (1/17) n MD n (Smart Selections)
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst of Maryland, Inc., Group Hospitalization and Medical Services, Inc., and CareFirst BlueChoice, Inc. are independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association.

BlueChoice Advantage Non-Integrated Deductible Summary of Benefits
Services In-Network You Pay1,2 Out-of-Network You Pay1,3
Visit www.carefirst.com/doctor to locate providers and facilities
FIRSTHELP—24/7 NURSE ADVICE LINE
Free advice from a registered nurse. Visit www.carefirst.com/needcare to learn more about your options for care.
When your doctor is not available, call FirstHelp at 800-535-9700 to speak with a registered nurse about your health questions and treatment options.
BLUE REWARDS
Visit www.carefirst.com/bluerewards for more information
Blue Rewards is an incentive program where you can earn up to $300 for taking an active role in getting healthy and staying healthy.
ANNUAL MEDICAL DEDUCTIBLE (Benefit Period)4
Individual $500 $1,000
Family $1,000 $2,000
ANNUAL OUT-OF-POCKET MAXIMUM (Benefit Period)5
Medical6 $4,500 Individual/$9,000 Family $6,500 Individual/$13,000 Family
Prescription Drug6 Combined with in-network out-of-pocket maximum
All drug costs are subject to in-network out-of-pocket maximum
PREVENTIVE SERVICES
Well-Child Care (including exams & immunizations)
No charge* No charge*
Adult Physical Examination (including routine GYN visit)
No charge* No charge* after deductible
Breast Cancer Screening No charge* No charge*
Pap Test No charge* No charge* after deductible
Prostate Cancer Screening No charge* No charge* after deductible
Colorectal Cancer Screening No charge* No charge* after deductible
PCP AND SPECIALIST SERVICES
FACILITY CHARGE7—In addition to the physician copays/coinsurances listed below, if a service is rendered on a hospital campus, ADD facility charge if applicable
$200 per visit Deductible, then 20% of Allowed Benefit
Office Visits for Illness—PCP7,8 $10 per visit Deductible, then 20% of Allowed Benefit
Convenience Care (retail health clinics such as CVS MinuteClinic or Walgreens Healthcare Clinic)
$10 per visit Deductible, then 20% of Allowed Benefit
Office Visits for Illness—Specialist7,8 $20 per visit Deductible, then 20% of Allowed Benefit
Allergy Testing7 $20 per visit Deductible, then 20% of Allowed Benefit
Allergy Shots7 $20 per visit Deductible, then 20% of Allowed Benefit
Physical, Speech, and Occupational Therapy7,9
(limited to 30 visits/benefit period)$20 per visit Deductible, then 20% of Allowed Benefit
Chiropractic Services7
(limited to 20 visits/benefit period)$20 per visit Deductible, then 20% of Allowed Benefit
Acupuncture7,9
(limited to 20 visits/benefit period)$20 per visit Deductible, then 20% of Allowed Benefit
EMERGENCY SERVICES
Urgent Care Center10
(such as Patient First or Express Care)$40 per visit $40 per visit
Hospital Emergency Room Services10
■ Facility Deductible, then $200 per visit (waived if admitted)
In-network deductible, then $200 per visit (waived if admitted)
■ Physician No charge* after deductible No charge* after in-network deductible
Ambulance10 (if medically necessary) Deductible, then $50 per service In-network deductible, then $50 per service
SUM3268-1P (3/17) ■ MD ■ 51+ Option 2-S (Smart Selections)

Services In-Network You Pay1,2 Out-of-Network You Pay1,3
DIAGNOSTIC SERVICES
Labs11
■ Non-Hospital/Freestanding Facility $10 per visit Deductible, then 20% of Allowed Benefit ■ Hospital Deductible, then $100 per visit Deductible, then 20% of Allowed Benefit
X-ray ■ Non-Hospital/Freestanding Facility $20 per visit Deductible, then 20% of Allowed Benefit ■ Hospital Deductible, then $150 per visit Deductible, then 20% of Allowed Benefit
Imaging ■ Non-Hospital/Freestanding Facility $60 per visit Deductible, then 20% of Allowed Benefit ■ Hospital Deductible, then $200 per visit Deductible, then 20% of Allowed Benefit
HOSPITALIZATION—(Members are responsible for both physician and facility fees)
Outpatient Surgical Center Services ■ Facility $100 per visit Deductible, then 20% of Allowed Benefit ■ Physician $20 per visit Deductible, then 20% of Allowed Benefit
Outpatient Hospital Surgical Services ■ Facility Deductible, then $200 per visit Deductible, then 20% of Allowed Benefit ■ Physician Deductible, then $20 per visit Deductible, then 20% of Allowed Benefit
Inpatient Hospital Services
■ FacilityDeductible, then $300 per day ($1,500 maximum per admission)
Deductible, then 20% of Allowed Benefit
■ Physician Deductible, then $20 per visit Deductible, then 20% of Allowed Benefit
HOSPITAL ALTERNATIVES
Home Health Care No charge* Deductible, then 20% of Allowed Benefit
Hospice (Inpatient—limited to 30 days; Outpatient—unlimited during Hospice eligibility period)
No charge* Deductible, then 20% of Allowed Benefit
Skilled Nursing Facility (limited to 60 days/benefit period)
Deductible, then $200 per admission Deductible, then 20% of Allowed Benefit
MATERNITY
Preventive Prenatal and Postnatal Office Visits No charge* Deductible, then 20% of Allowed Benefit
Delivery and Facility Services Deductible, then $300 per day ($1,500 maximum per admission)
Deductible, then 20% of Allowed Benefit
Artificial and Intrauterine Insemination7,12
(limited to 6 attempts per live birth)Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
In Vitro Fertilization Procedures7,12
(limited to 3 attempts per live birth up to $100,000 lifetime maximum)
Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
MENTAL HEALTH AND SUBSTANCE ABUSE—(Members are responsible for both physician and facility fees)
Office Visits $10 per visit Deductible, then 20% of Allowed Benefit
Outpatient Services
■ Facility $60 per visit Deductible, then 20% of Allowed Benefit
■ Physician $20 per visit Deductible, then 20% of Allowed Benefit
Inpatient Services
■ Facility Deductible, then $300 per day ($1,500 maximum per admission)
Deductible, then 20% of Allowed Benefit
■ Physician Deductible, then $20 per visit Deductible, then 20% of Allowed Benefit
MEDICAL DEVICES AND SUPPLIES
Durable Medical Equipment Deductible, then 25% of Allowed Benefit Deductible, then 45% of Allowed Benefit
Hearings Aids for ages 0-18 (limited to one hearing aid per hearing-impaired ear every 3 years)
No charge* Deductible, then 20% of Allowed Benefit
VISION
Routine Exam (limited to 1 visit/benefit period)
$10 per visit at participating vision provider Total charge minus $33 Allowed Benefit
Eyeglasses and Contact Lenses Discounts from participating vision centers Not covered
SUM3268-1P (3/17) ■ MD ■ 51+ Option 2-S (Smart Selections)

Note: Allowed Benefit is the fee that participating, in-network providers have agreed to accept for a particular covered service. The provider cannot charge the member more than this amount for any covered service. Example: Dr. Carson charges $100 to see a sick patient. To be part of CareFirst’s network, he has agreed to accept $50 for the visit. The member will pay their copay/coinsurance and deductible (if applicable) and CareFirst will pay the remaining amount up to $50.
* No copayment or coinsurance.1 When multiple services are rendered on the same day by more than one provider, Member payments are required for each provider.2 In-Network: When covered services are rendered in Maryland, Washington D.C. and/or Northern Virginia, collectively known as the CareFirst BlueChoice service area, by a
provider in the CareFirst BlueChoice Provider network, care is reimbursed at the in-network level. In-network benefits are based on the CareFirst BlueChoice Allowed Benefit. The CareFirst BlueChoice Allowed Benefit is generally the contracted rates or fee schedules that CareFirst BlueChoice providers have agreed to accept as payment for covered services. These payments are established by CareFirst BlueChoice, Inc., however, in certain circumstances, an allowance may be established by law. Outside of the CareFirst BlueChoice service area, when covered services are rendered by a provider in the preferred provider network, care is also covered at the in-network level. These in-network benefits are based on the contracted rates or fee schedules that preferred providers have agreed to accept as payment for covered services that are established by the local Blue Cross and Blue Shield Plan, however, in certain circumstances, an allowance may be established by law.
3 Out-of-Network: When covered services are rendered by a provider that is not in the CareFirst BlueChoice network in Maryland, Washington D.C. or Northern Virginia, or isnot in the preferred provider network outside of CareFirst BlueChoice service area, the care is reimbursed as out-of-network. Out-of-network benefits are based on the Allowed Benefit. The Allowed Benefit is generally the contracted rates or fee schedules that are established by CareFirst BlueChoice, or the local Blue Cross and Blue Shield Plan, however, in certain circumstances, an allowance may be established by law.
4 For Family coverage only: When one family member meets the individual deductible, they can start receiving benefits. Each family member cannot contribute more than the individual deductible amount. The family deductible must be met before the remaining family members can start receiving benefits.
5 For Family coverage only: When one family member meets the individual out-of-pocket maximum, their services will be covered at 100% up to the Allowed Benefit. Each family member cannot contribute more than the individual out-of-pocket maximum amount. The family out-of-pocket maximum must be met before the services for all remaining family members will be covered at 100% up to the Allowed Benefit.
6 Plan has separate out-of-pocket maximums for medical and drug expenses which accumulate independently.7 If a service is rendered on a hospital campus you could receive two bills, one from the physician and one from the facility.8 “Telemedicine services” refers to the use of a combination of interactive audio, video, or other electronic media used for the purpose of diagnosis, consultation, or treatment. Use
of audio-only telephone, electronic mail message (e-mail), or facsimile transmission (FAX) is not considered a telemedicine service.9 There are no limits for children until the end of the month in which the insured or enrollee turns 19 years of age when Physical, Speech or Occupational Therapy is included as
part of Habilitative Services.10 If the out-of-network benefit is listed as contributing toward the in-network deductible, then it also contributes toward the in-network out-of-pocket maximum.11 Members accessing laboratory services inside the CareFirst Service area (Maryland, D.C., Northern Virginia) must use LabCorp as their Lab Test facility and a non-hospital/
freestanding facility for X-rays and specialty Imaging for In-Network benefits. Services performed by any other provider, while inside the CareFirst Service area will be considered Out-of-Network. Members accessing laboratory, X-rays, and specialty Imaging services outside of Maryland, D.C. or Northern Virginia, may use any participating BlueCard PPO facility and receive in-network benefits.
12 Members who are unable to conceive have coverage for the evaluation of infertility services performed to confirm an infertility diagnosis, and some treatment options forinfertility. Preauthorization required
Not all services and procedures are covered by your benefits contract. This summary is for comparison purposes only and does not create rights not given through the benefit plan.
The benefits described are issued under form numbers: MD/CFBC/GC (R. 1/13); MD/CFBC/HPN/EOC (R. 6/10); MD/CFBC/DOL APPEAL (R. 9/11); MD/CFBC/LG/POS/DOCS (6/16); MD/CFBC/LG/POS/SOB (6/16); MD/CFBC/ELIG (R. 7/09); MD/CFBC/RX (R. 1/16); MD/CFBC/INCENT (1/16) and any amendments.
SUM3268-1P (3/17) ■ MD ■ 51+ Option 2-S (Smart Selections)
www.carefirst.com
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst MedPlus is the business name of First Care, Inc. CareFirst BlueCross BlueShield, First Care, Inc., and CareFirst BlueChoice, Inc., are independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.

Pharmacy Program$0 Deductible n $0/10/30/60 Retail Copays
50% Injectables Coinsurance
Summary of BenefitsPlan Feature Amount DescriptionIndividual Deductible None Your benefit does not have a deductible.
Family Deductible None Your benefit does not have a family deductible.
Out-of-Pocket Maximum See medical summary of benefits for annual out‑of‑pocket amount
If you reach your out‑of‑pocket maximum, CareFirst or CareFirst BlueChoice will pay 100% of the applicable allowed benefit for most covered services for the remainder of the year. All deductibles, copays, coinsurance and other eligible out‑of‑pocket costs count toward your out‑of‑pocket maximum, except balance billed amounts.
Preventive Drugs (Affordable Care Act) (up to a 34‑day supply)
$0 (not subject to deductible)
A preventive drug is a prescribed medication or item on CareFirst’s Preventive Drug List (ACA).* (Examples: Folic Acid, Fluoride and FDA approved contraceptives for women.)
Oral Chemotherapy Drugs Diabetic Supplies (up to a 34‑day supply)
$0 (not subject to deductible except for HSA Plans)
Diabetic supplies include needles, lancets, test strips and alcohol swabs.
Generic Drugs – (Tier 1) (up to a 34‑day supply)
$10 Generic drugs are covered at this copay level.
Preferred Brand Drugs (Tier 2) (up to a 34‑day supply)
$30 All preferred brand drugs are covered at this copay level.
Non-preferred Brand Drugs (Tier 3) (up to a 34‑day supply)
$60 All non‑preferred brand drugs on this copay level are not on the Preferred Drug List.* Discuss using alternatives with your physician or pharmacist.
Self-administered Injectable (excluding insulin) (Tier 4) (up to a 34‑day supply)
50% coinsurance up to a maximum payment of $150
All self‑administered injectable drugs (excluding insulin) are covered at this payment level. Insulin is covered at appropriate copay level.
Maintenance Drugs (up to a 90‑day supply)
Generic: $20 Preferred Brand: $60 Non‑preferred Brand: $120 Self‑Administered Injectables: 50% coinsurance, up to a maximum payment of $300
Maintenance drugs of up to a 90‑day supply are available for twice the copay through Mail Service Pharmacy or a retail pharmacy. Injectables (excluding insulin) are covered at 50% coinsurance up to a maximum payment of $300.
Restricted Generic Substitution Yes If a provider prescribes a non‑preferred brand drug when a generic is available, you will pay the non‑preferred brand copay or coinsurance PLUS the cost difference between the generic and brand drug up to the cost of the prescription. If a generic version is not available, you will only pay the copay or coinsurance. Also, if your prescription is written for a brand‑name drug and DAW (dispense as written) is noted by your doctor, you will only pay the copay.
Visit www.carefirst.com/rx for the most up-to-date Preferred Drug List and Formulary (list of covered drugs), including the prescription guidelines. Prescription guidelines indicate drugs that require your doctor to obtain prior authorization from CareFirst before they can be filled and drugs that can be filled in limited quantities.
This plan summary is for comparison purposes only and does not create rights not given through the benefit plan.
Policy Form Numbers: MD/CFBC/RX (R. 7/12) • MD/CF/RX (R. 7/12) • CFMI/51+/RX (R. 7/12)
SUM3400-1P (1/17) n MD n (Smart Selections)
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst of Maryland, Inc., Group Hospitalization and Medical Services, Inc., and CareFirst BlueChoice, Inc. are independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association.

BlueDental PlusIncludes access to a National Provider Network
CareFirst BlueCross BlueShield (CareFirst) offers BlueDental Plus coverage, which allows you the freedom to see any dentist you choose.
Advantages of the plan■■ Freedom of choice, freedom to save—With■BlueDental■Plus,■you■can■
see■any■dentist■you■choose.■However,■this■plan■also■gives■you■the■option■to■reduce■your■out-of-pocket■expenses■by■visiting■a■dentist■who■participates■in■our■Preferred■Provider■Network.■It’s■your■choice!
■■ Comprehensive coverage—Benefits■include■regular■preventive■care,■X-rays,■dental■surgery■and■more.■A■summary■of■your■benefits■is■available■on■the■following■page.
■■ Nationwide access to participating dentists—You■have■access■to■one■of■the■nation’s■largest■dental■networks,■with■participating■dentists■throughout■the■United■States.■BlueDental■Plus■gives■you■coverage■for■the■dental■services■you■need,■whenever■and■wherever■you■need■them.
Three options for care■■ Option■1—By■choosing■a■dentist■in■the■Preferred■Provider■
Network,■you■incur■the■lowest■out-of-pocket■costs.■These■dentists■accept■CareFirst’s■allowed■benefit■as■payment■in■full,■which■means■no■balance■billing■for■you.■You■are■responsible■for■deductibles■and■coinsurance,■and■also■have■the■convenience■of■your■provider■being■reimbursed■directly.
■■ Option 2—By■choosing■a■dentist■who■participates■with■CareFirst,■but■not■through■the■Preferred■Provider■Network,■you■incur■slightly■higher■out-of-pocket■costs.■Similar■to■Option■1,■there■is■no■balance■billing.■You■are■responsible■for■deductibles■and■coinsurance,■and■also■have■the■convenience■of■your■provider■being■reimbursed■directly.
■■ Option 3—You■can■receive■out-of-network■coverage■from■a■dentist■who■has■no■relationship■with■CareFirst.■With■this■option,■you■may■experience■higher■out-of-pocket■costs■since■you■pay■your■provider■directly.■You■can■be■balance■billed■and■must■pay■your■deductible■and■coinsurance■as■well.■
Using your plan
How do I find a preferred dentist?
Visit■www.carefirst.com/doctor■to■access■our■online■directory■24■hours■a■day. Click■on■the■Dental■tab■and■then■select■BlueDental■Plus■from■the■Plan■drop-down■menu.■
How much will I have to pay for dental services?
The■chart■on■the■following■page■gives■you■an■overview■of■many■of■the■covered■services■along■with■the■percentage■of■what■you■will■pay■for■each■class■of■services,■both■in■and■out-of-network.■
Is there a lot of paperwork?
There■is■no■paperwork■when■you■see■a■participating■dentist,■you■are■free■from■filing■claims.■However,■if■you■use■a■non-participating■dentist,■you■may■be■required■to■pay■all■costs■at■the■time■of■care,■and■then■submit■a■claim■form■in■order■to■be■reimbursed■for■covered■services.
Who can I call with questions about my dental plan?
Call■Dental■Customer■Service■toll■free■at:■866-891-2802 between■8:30■am■and■5:00■pm■ET,■Monday–Friday.

BlueDental Plus
Summary of Benefits YOU PAY
DEDUCTIBLE APPLIES TO ALL BASIC AND MAJOR SERVICES* $25■Ind./$75■Family—in-network■$50■Ind./$150■Family—out-of-network
ANNUAL MAXIMUM APPLIES TO ALL BASIC AND MAJOR SERVICES* Plan■pays■$1,500■Maximum
PREVENTIVE & DIAGNOSTIC SERVICES
■■ Oral■Exams■(two■per■benefit■period)■■ Prophylaxis■(two■cleanings■per■benefit■period)
■■ Bitewing■X-rays■■ Full■mouth■X-ray■or■panograph■and■bitewing■X-ray■combination■and■one■cephalometric■X-ray■(once■per■36■months)
■■ Palliative■emergency■treatment
■■ Fluoride■treatments■(two■per■benefit■period■per■member,■until■the■end■of■the■year■the■member■reaches■the■age■19)
■■ Sealants■on■permanent■molars■(once■per■tooth■per■36■months■per■member,■until■the■end■of■the■year■the■member■reaches■the■age■19)
■■ Space■maintainers■(once■per■60■months)
No■charge■from■participating■dentist1
BASIC SERVICES AND MAJOR SERVICES—SURGICAL
■■ Direct■placement■fillings■using■approved■materials■(one■filling■per■surface■per■12■months)
■■ Periodontal■scaling■and■root■planing■(once■per■24■months,■one■full■mouth■treatment)
■■ Oral■surgery■(surgical■extractions,■treatment■for■cysts,■tumor■and■abscesses,■apicoectomy■and■hemi-section)
■■ Surgical■periodontic■services■including■osseous■surgery,■mucogingival■surgery■and■occlusal■adjustments■(once■per■60■months)
■■ Endodontics■(treatment■as■required■involving■the■root■and■pulp■of■the■tooth,■such■as■root■canal■therapy)
■■ General■anesthesia■rendered■for■a■covered■dental■service
■■ Simple■extractions
20%■of■Allowed■Benefit■after■deductible1
MAJOR SERVICES—RESTORATIVE
■■ Full■and/or■partial■dentures■(once■per■60■months)
■■ Fixed■bridges,■crowns,■inlays■and■onlays■(once■per■60■months)
■■ Denture■adjustments■and■relining■(limits■apply■for■regular■and■immediate■dentures)
■■ Recementation■of■crowns,■inlays■and/or■bridges■(once■per■12■months)
■■ Repair■of■prosthetic■appliances■as■required■(once■in■any■12■month■period■per■specific■area■of■appliance)
■■ Dental■implants,■subject■to■medical■necessity■review■(once■per■60■months)
50%■of■Allowed■Benefit■after■deductible1
HIGHER OUT-OF-NETWORK REIMBURSEMENT AVAILABLE. Talk■to■your■benefits■manager■about■our■90■fee■schedule■option.
1 CareFirst payments are based on the CareFirst Allowed Benefit. Participating and Preferred Dentists accept 100% of the CareFirst Allowed Benefit as payment in full for covered services. Non-participating dentists may bill the member for the difference between the Allowed Benefit and their charges.
* Deductible and Annual Maximum Combined In-network/Out-of-network.
Summary of Exclusions: Not■all■services■and■procedures■are■covered■by■your■benefits■contract.■This■plan■summary■is■for■comparison■purposes■only■and■does■not■create■rights■not■given■through■the■benefit■plan.■
MD Benefits issued under policy form numbers:■■CareFirst■of■Maryland,■Inc.:■■CFMI/BLUEDENTAL EOC (1/15); CFMI/BLUEDENTAL DOCS (1/15); CFMI/BLUEDENTAL SOB (1/15); CFMI/51+/GC (R. 1/13); CFMI/ELIG/D-V (7/09) and■any■amendments.
Group■Hospitalization■and■Medical■Services,■Inc.:■ MD/GHMSI/BLUEDENTAL EOC (1/15); MD/GHMSI/BLUEDENTAL DOCS (1/15); MD/GHMSI/BLUEDENTAL SOB (1/15); MD/CF/GC (R.1/13); MD/CF/ELIG (R. 1/08)■and■any■amendments.
DC Benefits issued under policy form numbers: DC/GHMSI/BLUEDENTAL EOC (1/15); DC/GHMSI/BLUEDENTAL DOCS (1/15); DC/GHMSI/BLUEDENTAL SOB (1/15); DC/CF/GC (1/14); DC/CF/ELIG (1/14) and■any■amendments.■■
The CareFirst BlueCross BlueShieldfamily of health care plans
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst BlueCross BlueShield and CareFirst BlueChoice, Inc. are both independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.
SUM2580-1P (6/15) ■ MD/DC Group ■ Plan 1

CareFirst BlueCross BlueShield is the business name of CareFirst of Maryland, Inc. which is an independent licensee of the Blue Cross and Blue Shield Association. The Blue Cross and Blue Shield Names and Symbols are registered trademarks
of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.
Blue Rewards Healthy Habits Can Earn You Money
At CareFirst BlueCross BlueShield (CareFirst), your health is important to us. That’s why we include our exclusive incentive program—Blue Rewards—as part of your
medical plan.
SUM3704-1N (9/16) ■ MD Fully insured
With Blue Rewards, you have the opportunity to earn financial incentives for taking an active role in your health. By completing four important steps and achieving certain health measures, you and your covered spouse/domestic partner can each earn up to $300.
How Blue Rewards works
Blue Rewards gives you the opportunity to be rewarded twice! First, you can earn a participation-based reward for completing four important steps. Then, you can also earn a results-based reward by meeting certain health measures.
Get started by logging in to My Account at carefirst.com/myaccount and clicking on Blue Rewards. To begin each step, click on Start. Once you’ve completed step one, you can finish the remainder of the steps in any order.
Steps to earn your reward
Select a Patient-Centered Medical Home (PCMH) PCP
Additional results-based reward
Provide e-consent for wellness
communicationsComplete a health
assessment
Go to selected PCMH PCP and complete a
health evaluation
Reward based on health
evaluation results
+ + +
Earn a participation-based reward when you:
Complete before the end of your benefit periodComplete within 120 days from the date your coverage begins

Participation-based reward
Blue Rewards encourages you and your covered spouse/domestic partner to select and visit primary care providers (PCPs) who participate in our Patient-Centered Medical Home (PCMH) program—a program that provides your PCP with resources and tools to coordinate all your health care; leading to better health, better communication and better results.
To earn your participation-based reward, complete these 4 steps within 120 days from the date your coverage begins.
■ Select a PCP who participates in our PCMH program
■ Agree to receive wellness emails
■ Complete an online health assessment
■ Visit your selected PCMH PCP and complete the Health and Wellness Evaluation Form
Results-based reward
You have until the end of your benefit period to achieve this additional reward.
■ The results from your Health and Wellness Evaluation will be measured against the following results-based goals. As long as your results fall within all of the recommended ranges, you will earn an additional reward.
Measure Results-based goals
Weight (Body Mass Index—BMI) BMI between 19 and less than 30
Flu vaccine Received within the last 18 months
Tobacco use Must be a “non-smoker/user” (never smoked/used or quit for more than 30 days)
Blood pressure ■ Less than 140/90 (ages <60) ■ Less than 150/90 (ages 60+)
Blood glucose Fasting blood glucose is less than 126
■ If you do not meet these health measures during the initial visit with your PCP, you will need to work with your doctor to develop a goal and a plan of action. You should schedule a rescreening visit with your PCP to check your progress before the end of the benefit period. If your rescreening results are within the range the doctor established, you will earn the results-based reward once you enter your new measures. To do so, log in to My Account before the end of your benefit period and enter the new measure along with the date of the rescreening appointment.
Incentive amounts
Participation-based reward
Results-based reward Total reward
$100 + $200 = $300
Note: If you have a PPO or Advantage Plan and you live outside Maryland, D.C. or Northern Virginia, you can select a provider from the BlueCard® PPO network who specializes in general practice, family practice, internal medicine, pediatrics or geriatrics. While PCP selection is not required as part of the plan, you must select a provider in these specialties to earn a reward.

CareFirst Blue Rewards Visa® Incentive Card
■ Once you complete the four participation-based steps, you will receive an incentive card in the mail. Only one card is issued to the policyholder but it can be used by everyone covered under your policy.
■ Incentive cards should be retained as long as you remain a CareFirst member. Incentive cards will be replenished with funds once you earn another Blue Reward.
■ You have until the end of your benefit period to use your incentive card toward annual deductibles and out-of-pocket costs like copays or coinsurance related to eligible expenses (medical, prescription drug, dental and vision) under your CareFirst health plan.
■ If you have a plan with a health savings account (HSA) option, typically you will receive the incentive card once you have met the Internal Revenue Service (IRS) minimum deductible for an HSA plan—$1,300 for an individual or $2,600 for a family. In some circumstances, you may be able to receive your card right away.
To receive the incentive card right away, you can choose to certify either:
■ No contributions will be made (by you or your employer) to the HSA for the current benefit period; or
■ The card will only be used for CareFirst dental and vision expenses until meeting the IRS minimum deductible.1
■ You should always save your receipts as proof of your expense. As long as the card is used correctly, there are no tax reporting obligations.
1 Once the IRS minimum deductible has been met, the card can be used for all qualified expenses (including medical) incurred after meeting the deductible.
The CareFirst Blue Rewards Visa Incentive Card is issued by The Bancorp Bank pursuant to a license from Visa U.S.A. Inc. This card may not be used everywhere Visa debit cards are accepted. No cash access permitted. The Bancorp Bank; Member FDIC.
Get started now by logging in to My Account at www.carefirst.com/myaccount.

View personalized information on your claims and out-of-pocket costs online with My Account. Simply log on to
www.carefirst.com/myaccount for real-time information about your plan. You will see it's easier than ever to find
your personalized health care information.
CareFirst - My Account - Online Access to Your Claims

Know Before You Go

Know Before You Go

ER versus Urgent Care or Doctor’s Office Settings
Symptom Doctors’ office setting Urgent care center
Animal bites √
Stitches √
Back pain √ √
Mild asthma √ √
Minor headache √ √
Sprain, strain √ √
Nausea, vomiting, diarrhea √ √
Bumps, cuts, scrapes √ √
Burning with urination √ √
Cough, sore throat √ √
Ear or sinus pain √ √
Eye swelling, irritation, redness or pain √ √
Minor allergic reactions √ √
Rash, minor bumps √ √
Vaccination √ √
Symptom Emergency Room
Sudden or unexplained loss of consciousness √
Signs of a heart attack, such as sudden/severe chest pain or pressure
√
Sign of stroke, such as numbness of the face, arm or leg on one side of the body; difficulty talking; sudden loss of vision
√
Sudden shortness of breath √
High fever with stiff neck, mental confusion and/or difficulty breathing
√
Coughing up or vomiting blood √
Cut or wound that won’t stop bleeding √
Possible broken bones √
Poisoning √
Stab wounds √
Sudden, severe abdominal pain √
Suicidal feelings √
Partial or total amputation of a limb √
It’s important to know ahead of time what to do when you need emergency or urgent care. The chart below can help you decide where and when to go for care.
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc.CareFirst BlueCross BlueShield and CareFirst BlueChoice, Inc. are both independent licensees of the Blue Cross and Blue Shield Association.
® Registered trademark of the Blue Cross and Blue Shield Association. ®’ Registered trademark of CareFirst of Maryland, Inc.
MBR4745 (8/13)
For a complete listing of Urgent Care Centers, visit www.carefirst.com/doctor and select your health plan. Then select Urgent Care under the Facilities section. Medical emergencies require a visit to the emergency room. If your situation
is a medical emergency, call 911 or go directly to the nearest emergency care facility.
This information is not intended as medical advice.

National Vision Administrators, L.L.C.
www.e-nva.com Page 1
Your NVA Vision Benefit Summary Dealers Greatest Assets, Inc. Effective 07/01/2017 Group Number# 8927 Schedule of Vision Benefits How Your Vision Care Program Works Eligible members and dependents are entitled to receive a vision examination and one (1) pair of lenses and a frame or contact lenses once every plan year. For your convenience, at the start of the program, you will receive two identification cards with participating providers in your zip code area listed on the back. At the time of your appointment, simply present your NVA identification card to the provider or indicate that your benefit is administered by NVA. The provider will contact NVA to verify eligibility. A vision claim form is not required at an NVA participating provider. Be sure to inform the provider of your medical history and any prescription or over-the-counter (OTC) medications you may be taking. To verify your benefit eligibility prior to calling or visiting your eye care provider, please visit our website at www.e-nva.com or contact NVA’s Customer Service Department toll-free at 1.800.672.7723 (TDD line 1-888-820-2990) or NVA’s Interactive Voice Response (IVR). Customer Service is available 24 hours a day, 7 days a week, 365 days a year. Any question any time. If you are not a registered subscriber, you can still search our providers online by selecting the “Find a Provider” link on our home page. Enter group number 8927000001 or the group number on the identification card and enter in your search parameters. It’s that easy! *Does not apply to Wal-Mart / Sam’s Club locations or for certain proprietary brands. **Does not apply to Wal-Mart/Sam’s Club, Contact Fill (NVA Mail Order) or certain locations at: Target, Sears, Pearle, & K-Mart and may be prohibited by some manufacturers. ***Pre-approval from NVA required.
�Additional professional services related to contact lenses (also known as fitting fees) would be included in the contact lens allowance shown above. Due to their everyday low prices (EDLP) the amounts listed below may not be applicable at Wal-Mart/Sam’s Club.
Lens options purchased from a participating NVA provider will be provided to the member at the amounts listed in the fixed option pricing list below: � $100 Progressive Lenses Premium* $50 Progressive Lenses Standard* � $75 Polarized $65 Transitions Single Vision Standard � $10 Standard Scratch-Resistant Coating $70 Transitions Multi-Focal Standard � $12 Ultraviolet Coating $25 Polycarbonate (Single Vision) 19 & over � $40 Standard Anti-Reflective $30 Polycarbonate (Multi-Focal) 19 & over � $20 Glass Photogrey (Single Vision) $30 Blended Bifocal (Segment) � $30 Glass Photogrey (Multi-Focal) $55 High Index *Fixed Pricing not available on certain brands Options not listed will be priced by NVA providers at their R&C retail price less 20%. In MD, members may be required to pay the full retail amount and not the negotiated discount amount at certain participating providers.
Participating providers are not contractually obligated to offer sale prices in addition to outlined coverage. Regardless of medical or optical necessity, vision benefits are not available more frequently than specified in your policy.
Benefit Frequency Participating
Provider Non-Participating
Provider Examination Once Every Plan Year � Covered 100% After $10 copay
Reimbursed Amount � Up to $45 Lenses Once Every Plan Year
� Single Vision � Bifocal � Trifocal � Lenticular � Polycarbonates (under age 19) � Oversized � Fashion Gradient Tints � Solid Tints
Standard Glass or Plastic
� Covered 100%
� Up to $50 � Up to $80 � Up to $100 � Up to $120
� Up to $25 (SV) � Up to $30 (Bi/Tri)
� Up to $5 � Up to $12 � Up to $10 Frame Once Every Plan Year Retail Allowance
� Up to $100 (20% discount off balance)*
� Up to $50
Contact Lenses Once Every Plan Year Elective Contact Lenses Medically Necessary*** In lieu of Lenses & Frame
� Up to $100 Retail� (15% discount (Conventional) or 10% discount (Disposable) off balance)** � Covered 100%
In lieu of Lenses & Frame
� Up to $100
� Up to $210

www.e-nva.com Page 2
Get a Better View Plan Specific Details Online: The NVA website is easy to use and provides the most up to date information for program participants: -Locate a nearby participating provider by name, zip code, or City/State, Verify eligibility for you or a dependent -View benefit program and specific detail, Review claims, Print ID cards (when applicable), Nominate a non-participating provider to join the NVA network Examinations: The comprehensive exam includes case history, examination for pathology or anomalies, visual acuity (clearness of vision), refraction, tonometry (glaucoma test) and dilation (if professionally indicated). Lenses: NVA provides coverage in full for standard glass or plastic eyeglass lenses.
Frames: Select any frame from the participating provider’s inventory. Any amount in excess of your plan allowance is the member’s responsibility. Frame choices vary from office to office. (Visit NVA’s website to view the Benefit maximizer Program) Contact Lenses: The contact lens benefit includes all types of contact lenses such as hard, soft, gas permeable and disposable lenses. Medically necessary contact lenses includes fitting and follow up and may be covered with prior authorization when prescribed for: post cataract surgery, correction of extreme visual acuity problems that cannot be corrected to 20/70 with spectacle lenses, Anisometropia or Keratoconus. Non-Participating Providers: You will be responsible for one hundred percent (100%) of the cost at the time of service at a non-participating provider. You can request a claim form from NVA via the website www.e-nva.com or you may submit receipts along with a letter containing the member’s full name, patient’s full name, address, ID# and sponsoring organization to NVA, P.O. Box 2187, Clifton, NJ 07015. Laser Eye Surgery: NVA has chosen The National LASIK Network to serve their members. This network was developed by LCA Vision in 1999 and is one of the largest panels of LASIK surgeons in the U.S. Members are entitled to significant discounts and a free initial consultation with all in-network providers. Discounts: In addition to your funded benefit you are eligible to access the EyeEssential® Plan discount (in Network Only) on additional purchases during the plan period. Please see table for more detail regarding NVA’s discount plan: *Discount is not applicable to mail order; however, you may get even better pricing on contact lenses through Contact Fill. In MD, members may be required to pay the full retail amount and not the negotiated discount amount at certain participating providers. Lens options purchased from a participating NVA provider will be provided to the member at the amounts listed in the fixed option price list above. Options not listed will be priced by NVA providers at their reasonable & customary retail price less 20%. Wal-Mart / Sam’s Club Stores: Due to their everyday low prices (EDLP) Wal-Mart / Sam’s Club stores do not provide additional discounts. At NVA, We Work Only for Our Clients. Insurance coverage provided by National Guardian Life Insurance Company (NGLIC), 2E Gilman, Madison, WI 53703. Policy NVIGRP 5/07. NGLIC is not affiliated with the Guardian Life Insurance Company of America, a/k/a The Guardian or Guardian Life. A full description of your coverage, its limitations, exclusions and conditions is contained in the Insurance Policy issued to your Plan Sponsor at its place of business. That full description in the form of a Certificate of Coverage can be made available to you by requesting it from your Plan Sponsor. Exclusions / Limitations: No payment is made for medical or surgical treatments / Rx drugs or OTC medications / non-prescription lenses / two pair of glasses in lieu of bifocals / subnormal visual aids / vision examination or materials required for employment / replacement of lost, stolen, broken or damaged lenses/ contact lenses or frames except at normal intervals when service would otherwise be available / services or materials provided by federal, state, local government or Worker's Compensation / examination, procedures training or materials not listed as a covered service / industrial safety lenses and safety frames with or without side shields / parts or repair of frame / sunglasses. National Vision Administrators, L.L.C. ▫ PO Box 2187 ▫ Clifton, NJ 07015 Web: www.e-nva.com ▫ Toll-Free: 1.800.672.7723 NVA® and EyeEssential® are registered marks of National Vision Administrators, L.L.C.
Your NVA EyeEssential® Plan Discount – In Network Only Service Participating Provider Lens Options Eye Examination: Contact Lens Fitting: Lenses: Single Vision Bifocal Trifocal or Lenticular Frame:
Member Cost: Retail Less $10 Retail Less 10% Glass or Plastic $35.00 $55.00 $70.00 Retail Less 35%
$12 Solid Tint/ Gradient Tint $50 Standard Progressive Lenses $75 Polarized Lenses $65 Transitions Single Vision Standard $70 Transitions Multi-Focal Standard $15 Standard Scratch Coating $12 UV Coating $35 Polycarbonate $45 Standard Anti-Reflective Contact Lenses*:
Conventional Disposable
Member Cost: Retail Less 15% Retail Less 10%
This document is intended as a program overview only and is not a certified document of the individual plan parameters.

•Employee determines the amount of pre-tax money they will contribute to their HSA account.
Tax Deductible: Contributions to the HSAs are 100% tax deductible (for the person making the contribution)
Tax-Deferred: Interest earnings accumulate tax-deferred
Tax Free: Withdrawals for qualified medical expenses are never taxed.
*Those individuals ages 55 and over may contribute an additional $1,000 for catch up
Daily Use of an HSA
An HSA (Health Savings Account) is an innovative tool for managing the cost of health benefits. Designed by the
federal government, HSA legislation allows individuals to save for future qualified medical and retiree health
expenses on a tax-free basis.
•HSA funds accrue and are available for reimbursement of qualified expenses and/or remain available for the future.
For a list of eligible expenses visit:
•Amounts contributed by the employee to an HSA belong to the employee, and are portable should their
employment terminate.
Health Savings Accounts (HSA)
$3,400
$1,300
•Employees may be free to choose from a wide range of investment options for the HSA, and earnings accumulate
tax-free.
•Funds distributed from the HSA are not taxed if they are used to pay for qualified medical expenses, and any unused
funds accumulate tax-free for future use.
www.irs.gov
HSA Benefits
Tax Benefits, Deductible Requirements, & Contribution Limits
$3,350
$1,300
2017
FamilyCurrent & Upcoming IRS Limits
Maximum Annual Contribution
Minimum Deductible
Maximum Annual Contribution
Minimum Deductible2016
$2,600
$6,750
$2,600
$6,750
Single
Doctor, Specialist, Hospital, Lab, etc.
Show ID card to provider and you will be asked to pay applicable copay for that service. Member will receive Explanation of Benefits (EOB) from carrier
showing the balance due. Member then pays facility directly. Member should use HSA Debit Card for all
IRS qualified medical costs.
Pharmacy
Always show ID card! Pharmacist will submit claim
to carrier and member will be responsible for discounted price while still meeting the deductible. After deductible, member is responsible for copay
only. Member should use HSA Debit Card for all qualified prescribed medication costs.
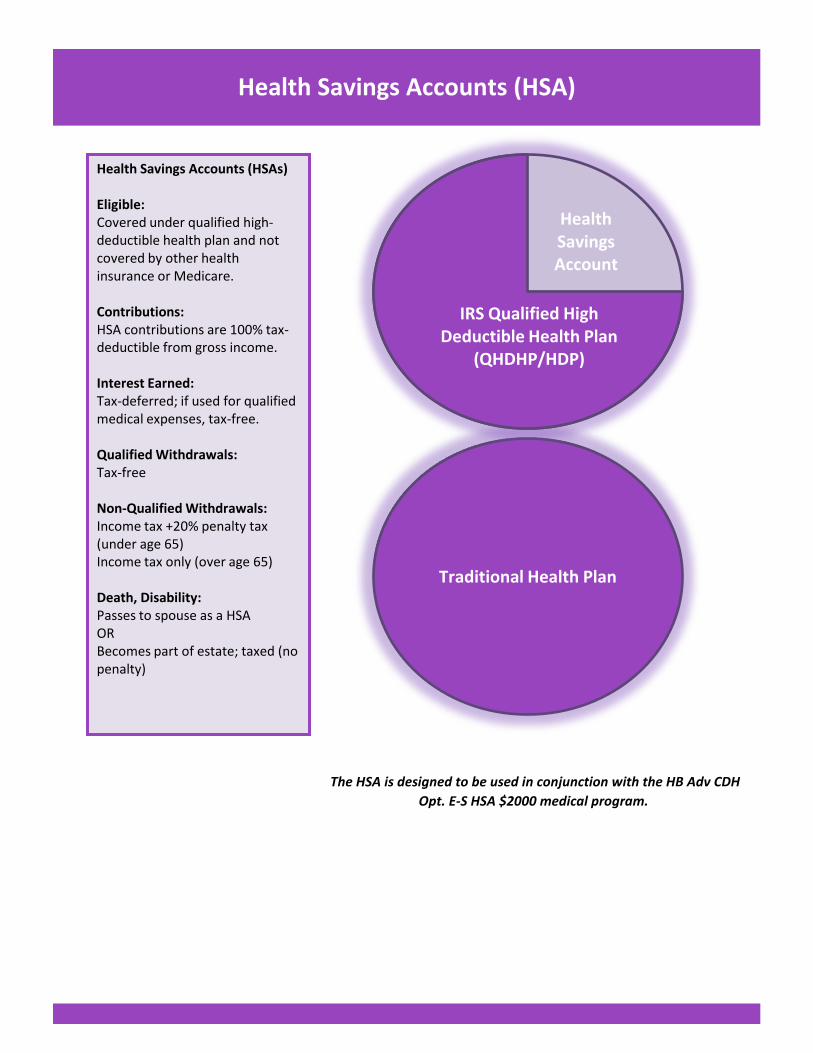
Health Savings Accounts (HSA)
The HSA is designed to be used in conjunction with the HB Adv CDH
Opt. E-S HSA $2000 medical program.
Health Savings Accounts (HSAs) Eligible: Covered under qualified high-deductible health plan and not covered by other health insurance or Medicare. Contributions: HSA contributions are 100% tax-deductible from gross income. Interest Earned: Tax-deferred; if used for qualified medical expenses, tax-free. Qualified Withdrawals: Tax-free Non-Qualified Withdrawals: Income tax +20% penalty tax (under age 65) Income tax only (over age 65) Death, Disability: Passes to spouse as a HSA OR Becomes part of estate; taxed (no penalty)
Traditional Health Plan
Health Savings Account
IRS Qualified High Deductible Health Plan
(QHDHP/HDP)

Consolidated Omnibus Budget Reconciliation Act (COBRA)
Employee Retirement Income Security Act (ERISA)
HIPAA Information Notice of Privacy Practices
Janet’s Law
v All stages of reconstruction of the breast on which the mastectomy was performed;
v Surgery and reconstruction of the other breast to produce a symmetrical appearance;
v Prostheses;
v Treatment of Physical complications of the mastectomy, including lymphedema.
Newborn’s Act
Disclosure Notices
Requires group health plans sponsored by employers with 20 or more employees in the prior year to offer employees
and eligible dependents a temporary extension of health coverage when group coverage would otherwise end. Under
COBRA, plans must provide covered employees and dependents with specific notices explaining their COBRA rights.
Coverage continues on a temporary basis due to various circumstances that initiate loss in coverage. If an employee
retires, a divorce occurs, employee joins another organization, are the types of circumstances that allow COBRA to
protect the employee.
Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any
hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a
vaginal delivery, or less than 96 hours following a cesarean section. However, Federal law generally does not prohibit
the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her
newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under Federal,
require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not
in excess of 48 hours (or 96 hours)
The Employee Retirement Income Security Act of 1974 (ERISA) is a federal law that sets minimum standards for
retirement and health benefit plans in private industry. ERISA covers retirement, health and other welfare benefit
plans (e.g., life, disability and apprenticeship plans). Among other things, ERISA provides that those individuals who
manage plans (and other fiduciaries) must meet certain standards of conduct. ERISA has also been expanded to
include health laws. For example, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) amended
ERISA to provide for the continuation of health care coverage for employees and their beneficiaries (for a limited
period of time) if certain events would otherwise result in a reduction in benefits. In addition, the Health Insurance
Portability and Accountability Act of 1996 (HIPAA) amended ERISA to make health care coverage more portable and
secure for employees.
The Health Insurance Portability and Accountability Act of 1996 (HIPAA) impacts a wide variety of features of the U.S.
health care system. The law establishes standards to protect individual’s medical records and personal information.
The regulation requires safeguards to protect the patient information, such as limiting the release of information
without authorization. The rule gives the patient total control over their information, as to who has rights over the
information and who can examine the information.
On October 21, 1998, Congress enacted the Women’s Health and Cancer Rights Act of 1998.The law protects
individuals post-mastectomy, and benefits must be provided to covered patients. The required coverage for the
individuals includes:
Under Janet’s Law, mastectomy benefits may be subject to annual deductibles and coinsurance consistent with those
established for other benefits under the plan or coverage.

Pre-Existing Condition Notification (HIPAA)
Premium Assistance Under Medicaid & The Children’s Health Insurance Program (CHIP)
Qualified Medical Child Support Order (QMCSO)
Special Enrollment Rights
Uniformed Services Employment and Reemployment Rights Act (USERRA)
In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may
be able to enroll yourself and your dependents. However, you must request enrollment within the specified period of
time after the marriage, birth, adoption, or placement of adoption. Contact Group Benefit Services in order request
special enrollment or for any other information regarding special enrollment rights.
Under federal law, the Uniformed Services Employment and Reemployment Rights Act (USERRA) provide employees
the right to be reemployed in their civilian job if they leave their job to perform service in the uniformed service.
Military employees have the right to elect to continue health plan coverage, including dependents, for up to 24
months of service. If elected to end health plan, you must be reinstated to your employer’s plan when reinstated;
with no waiting period or exclusion for pre-exiting conditions unless related to military service.
A QMCSO is a court order or an order issued by a state administrative agency in accordance with federal and state
laws that require an alternate beneficiary (for example, a child or stepchild) to be covered by a plan participant’s
group health plan. ERISA requires group health plans to provide health benefits coverage to children of a parent-
employee who is divorced, separated, or never married in accordance with the applicable requirements of any
qualified medical child support order (QMCSO) issued by a state court or agency. Each group health plan must
establish reasonable procedures to determine whether medical child support orders are qualified.
If you are declining enrollment for yourself or your dependents (including your spouse) because of the other health
insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or
your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your
dependents’ other coverage). However, you must request enrollment within the specified period within the plan,
after your dependent’s other coverage ends.
As part of the Health Care Reform law, employer-sponsored group health plans are no longer permitted to apply pre-
existing condition exclusion periods to individuals covered under the plan.
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer,
your state may have a premium assistance program that can help pay for coverage, using funds for their Medicaid or
CHIP programs. If you or your children aren’t eligible for these premium assistance programs but you may be able to
buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit
www.healthcare.gov.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your
dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-
KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that
might help you pay the premiums for an employer-sponsored plan.
Disclosure Notices

Benefits questions
ID Card issues
Prescription issues
Questions regarding billing and claim resolution
Provider network questions
HRA/FSA questions……….and much more!
Fax #: 443-541-1409
For your convenience, here are wallet size information cards
Fax #: 443-541-1409
Tonya Fowlkes (443) 589-1263
Brianna Mistler (443) 589-1206
Karen Munn (443) 589-1273
Fax #: 443-541-1409
Tonya Fowlkes
Brianna Mistler
Karen Munn
Brianna Mistler
(443) 589-1263
(443) 589-1206
(443) 589-1273
GBSVIP Customer Service Team
GBSVIP is a powerful, one-stop contact center staffed by licensed professionals who adhere to the strictest
standards of confidentiality. Your dedicated team of experienced benefit advocates are ready to help you
and your family members. GBSVIP can resolve claim issues through carriers and service providers 3-4 time
faster than members can on their own. We provide assistance with the following:
GBSVIP Customer Service Team
Monday - Friday,
7:30am - 6:00pm (EST)
Monday - Friday, 7:30am - 6:00pm (EST)
GBSVIP Customer Service TeamMonday - Friday, 7:30am - 6:00pm (EST)
For Services that's confidential and responsive, contact the GBSVIP team!
Tonya Fowlkes (443) 589-1263
(443) 589-1206
(443) 589-1273
GBS Customer Service Representative
GBS Customer Service Manager
GBS Customer Service Representative
Karen Munn