de novo reciprocal translocation t(4;20) (q28;q11) associated in a child with developmental delay:...
TRANSCRIPT
De novo reciprocal translocation t(4;20) (q28;q11) associated in a child with developmental delay:
Case report

ww.sciencedirect.com
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3
Available online at w
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
Case Report
De novo reciprocal translocation t(4;20) (q28;q11)associated in a child with developmental delay:Case report
Kavitha Eppa a,*, Iravathy Goud Kalal b, Pranathi Reddy Guttala c,Sakina Aneeb d
a Consultant, Department of Cytogenetics & Molecular Biology, Apollo Health City, Jubilee Hills, Hyderabad,
Andhra Pradesh 500033, Indiab HOD, Consultant, Department of Cytogenetics & Molecular Biology, Apollo Health City, Jubilee Hills, Hyderabad,
Andhra Pradesh 500033, Indiac Consultant, Department of Internal Medicine, Apollo Health City, Jubilee Hills, Hyderabad, Andhra Pradesh
500033, Indiad Technologist, Department of Cytogenetics & Molecular Biology, Apollo Health City, Jubilee Hills, Hyderabad,
Andhra Pradesh 500033, India
a r t i c l e i n f o
Article history:
Received 25 January 2014
Accepted 18 July 2014
Available online xxx
Keywords:
Developmental delay
Translocation
Cytogenetic analysis
Karyotype
* Corresponding author. Tel.: þ91 9491226E-mail addresses: matamkavitha@gmail.
Please cite this article in press as: Eppadevelopmental delay: Case report, Apollo
http://dx.doi.org/10.1016/j.apme.2014.07.0040976-0016/Copyright © 2014, Indraprastha M
a b s t r a c t
The common cause of mental impairment and the wide range of physical abnormalities is
balanced chromosome rearrangement. As such, it is difficult to interpret, posing as a
diagnostic challenge in human development. We present a unique case report with a
denovo autosomal-balanced reciprocal translocation involving chromosomal regions 4q
and 20q.The etiology of the translocation, i.e. 46,XX,t (4;20)(q28;q11) was detected by con-
ventional high-resolution Giemsa-Trypsin-Giemsabanding technique. Parents non-
consanguineous, with 2 healthy children. To the best of our knowledge this is the first
case reported so far with the balanced reciprocal translocation involving 4q and 20q
associated with the delayed milestone development.
Conclusion: The reason likely may be due to the rearrangement of genetic material at these
breakpoints having a crucial relationship and thus manifesting developmental delay in the
proband.
Copyright © 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
In humans the incidence of balanced chromosomal trans-
locations is approximately 1 in 500.1 In cytogenetic evaluation,
119, þ91 040 23607777x40com, kavitha_e@apolloho
K, et al., De novo reciprMedicine (2014), http://
edical Corporation Ltd. A
balanced chromosome translocations are defined as those
rearrangements where no loss or gain of genetic material is
observed. Most of the balanced chromosome rearrangements
(BCRs) are not considered to be associated with the clinical
12; fax: þ91 040 23608050.spitals.com (K. Eppa).
ocal translocation t(4;20) (q28;q11) associated in a child withdx.doi.org/10.1016/j.apme.2014.07.004
ll rights reserved.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e32
(phenotype) abnormalities. But, they are of concern, as the
carriers of BCRs offer a greater risk to their descendants with
congenital anomalies or recurrent miscarriages. On the basis
of a few evaluation procedures, it is estimated that 6.7% of the
carriers of de novo BCRs have the risk of phenotypic abnor-
malities.2 In the present paper, we describe de novo
autosomal-balanced reciprocal translocation involving chro-
mosomes 4 and 20 in a child associated with delayed mile-
stone development.
2. Case report
The proband is a 7 months boy, the third male child of a
healthy, young, non-consanguineous couple with 2 other
healthy children. No family history. Pregnancy and delivery at
38 weeks were normal. Birth weight was 3.2 kgs. Length was
44 cm and head circumference (HC) was 34 cm. The child was
neither focusing nor following the object at 3 months did not
attain social smile and has delayed mile stones. At 7 months
there was no head control, and was not recognizing the
parents.
Examination revealed hypotonia (frog posture) with facial
asymmetry and microcephaly, HC below 3rd centile. There
was no plagiocephaly with closed anterior fontanel. Some
dysmorphic features (low set ears, high arched palate, single
palmer crease and hypoplastic toe nails) were seen. He was
not following and there was no startle. He had horizontal
nystagmus. There was axial hypotonia with limbs spasticity
and brisk deep tendon reflexes. There was no clonus. He had
no organomeghaly.
2.1. Materials & methods
Tandem mass: Normal, elevated liver enzymes: ALT-55IU/
L(0e41), AST:86 U/L(0e38). CT brain: smooth brain surface
with thick cortex, absent corpus callosum and asymmetry in
the lateral ventricles. MRI brain: polymicrogyria and double
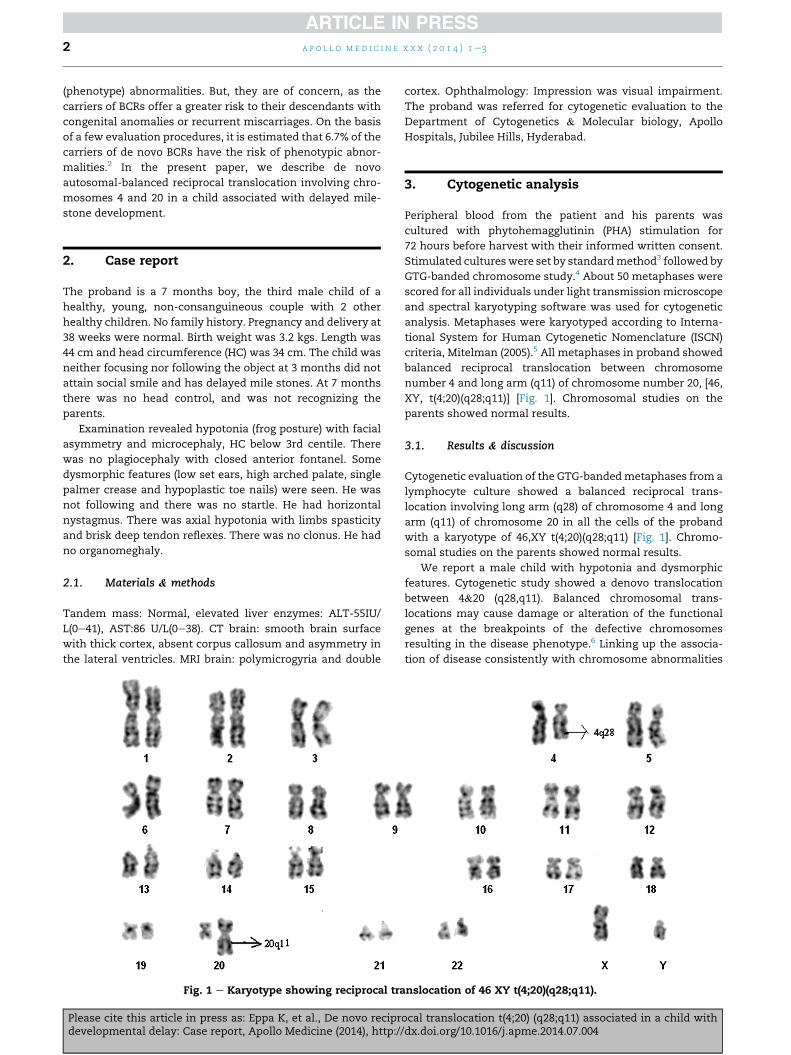
Fig. 1 e Karyotype showing reciprocal tra
Please cite this article in press as: Eppa K, et al., De novo reciprdevelopmental delay: Case report, Apollo Medicine (2014), http:/
cortex. Ophthalmology: Impression was visual impairment.
The proband was referred for cytogenetic evaluation to the
Department of Cytogenetics & Molecular biology, Apollo
Hospitals, Jubilee Hills, Hyderabad.
3. Cytogenetic analysis
Peripheral blood from the patient and his parents was
cultured with phytohemagglutinin (PHA) stimulation for
72 hours before harvest with their informed written consent.
Stimulated cultureswere set by standardmethod3 followed by
GTG-banded chromosome study.4 About 50 metaphases were
scored for all individuals under light transmissionmicroscope
and spectral karyotyping software was used for cytogenetic
analysis. Metaphases were karyotyped according to Interna-
tional System for Human Cytogenetic Nomenclature (ISCN)
criteria, Mitelman (2005).5 All metaphases in proband showed
balanced reciprocal translocation between chromosome
number 4 and long arm (q11) of chromosome number 20, [46,
XY, t(4;20)(q28;q11)] [Fig. 1]. Chromosomal studies on the
parents showed normal results.
3.1. Results & discussion
Cytogenetic evaluation of the GTG-bandedmetaphases from a
lymphocyte culture showed a balanced reciprocal trans-
location involving long arm (q28) of chromosome 4 and long
arm (q11) of chromosome 20 in all the cells of the proband
with a karyotype of 46,XY t(4;20)(q28;q11) [Fig. 1]. Chromo-
somal studies on the parents showed normal results.
We report a male child with hypotonia and dysmorphic
features. Cytogenetic study showed a denovo translocation
between 4&20 (q28,q11). Balanced chromosomal trans-
locations may cause damage or alteration of the functional
genes at the breakpoints of the defective chromosomes
resulting in the disease phenotype.6 Linking up the associa-
tion of disease consistently with chromosome abnormalities
nslocation of 46 XY t(4;20)(q28;q11).
ocal translocation t(4;20) (q28;q11) associated in a child with/dx.doi.org/10.1016/j.apme.2014.07.004

a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3 3
such as deletions, duplications and translocations would be
the simple way of mapping disease genes. Molecular charac-
terization of chromosomal breakpoints in carriers of balanced
translocation would be one of the vital strategies to be
implemented. Thus, disease-associated chromosome rear-
rangements that truncate, delete or otherwise inactivate
specific genes have been instrumental in the positional clon-
ing of many disease genes.7
In thispaper,wereportan interestingcasewithapparentlyde
novo reciprocal-balanced translocation that has resulted in
delayed development of milestones. Delayed milestones or
developmental delays are defined as a lag in the child's devel-
opment compared to theestablished standardnormal ranges for
hisorherage. Frombirth to6yearsofage, 8%ofall childrenshow
delays in one or more areas of development. The present report
indicates that the proband had developmental lags in the first
year of his life. At the age of 7months hehadnohead control, no
hand regards andwas not recognizingparents. The present case
report, however, is the first report of denovo balanced trans-
location involving chromosomes 4 and 20 at their respective
breakpoint, which shows an association with delayed mile-
stones andwhichhasnot been reported previously. On the basis
of thechromosomes involvedandonthe locationofbreakpoints,
the production of normal, balanced or unbalanced gametes is
decided.8 In carriers of balanced translocation, the possible
reason for the association of malformations could be gene
inactivation or disruption at the breakpoint or a position effect.9
The gene PRSS12 that maps at 4q28 encodes a extracellular
multidomain serine protease associated with neural devel-
opment and plasticity and studies in mouse suggest that the
encoded enzyme may be involved in structural re-
organizations associated with learning and memory. Molinari
et al.,10 reviewed the molecular pathogenesis of autosomal
recessive mental retardation caused by neurotrypsin muta-
tions. Another important gene NNAT mapped to 20q11 en-
codes a proteolipid which participate in the maintenance of
segment identity in the hindbrain and pituitary development,
and maturation or maintenance of the overall structure of the
nervous system, also as a regulatory subunit of ion Channels.
Hence, disruption of the gene or group of genes at this
breakpoint might suggest a cause for delayed developmental
milestones. The possible reason leading to delayedmilestones
may be due to the consequence of the abnormality described
in the patient. Hence, further analysis of the breakpoints and
molecular characterization of these genes might help in un-
derstanding the basis of delayed development of milestones.
Moreover, it is known that the modification or inactivation of
specific disease genes at chromosomal breakpoints have been
very phenomenal in identifying genes that are associatedwith
a variety of disorders, mostly early-onset disorders.7
4. Conclusion
These findings suggest that cytogenetic analysis is useful in
the investigation of children with genetic disorders of un-
Please cite this article in press as: Eppa K, et al., De novo reciprdevelopmental delay: Case report, Apollo Medicine (2014), http://
known origin to confirm clinical diagnosis and in view of an
increased risk of having congenitally abnormal children, car-
riers of balanced reciprocal translocation should, therefore, be
advised to seek genetic counseling.
Conflicts of interest
All authors have none to declare.
Acknowledgements
The authors acknowledge the parents of the child for
accepting to give the consent and samples, technical support
of Mr. V. Ravi for cytogenetics and the Management of Apollo
Hospitals for their support.
r e f e r e n c e s
1. Hook EB, Hamerton JL. The frequency of chromosomeabnormalities detected in consecutive newborn studies -differences between studies - results by sex and by severity ofphenotypic involvement, population cytogenetics. In:Hook EB, Porter IH, eds. New York: Academic Press;1977:63e79.
2. Warburton D. De novo balanced chromosomerearrangements and extra marker chromosomes identifiedat prenatal diagnosis: clinical significance and distributionof breakpoints. Am J Hum Genet. 1991;49:995e1013.
3. Moorehead PS, Nowell PC, Mellman WJ, Battips DM,Hungerford DA. Chromosome preparation of leukocytescultured from human peripheral blood. Exp Cell Res.1960;20:613e616.
4. Seabright M. A rapid banding technique for humanchromosomes. Lancet. 1971;2:971e972.
5. Mitelman F. ISCN. An International System for Human CytogeneticNomenclature. Basel: Karger; 2005:1e115.
6. Fryns JP, Kleczkowska A, Kubien E, Van den Berghe H.Excess of mental retardation and/or congenitalmalformation in reciprocal translocations in man. HumGenet. 1986;72:1e8.
7. Bugge M, Bruun-Petersen G, Brondum-Nielsen K, et al.Disease associated balanced chromosome rearrangements: aresource for large-scale genotype-phenotype delineation inman. J Med Genet. 2000;37:858e865.
8. Burns JP, Koduru PR, Alonso ML, Chaganti RS. Analysis ofmeiotic segregation in a man heterozygous for two reciprocaltranslocations using the hamster in vitro penetration system.Am J Hum Genet. 1986;38:945e964.
9. Buhler EM. Unmasking of heterozygosity by inheritingbalanced translocations. Implications for prenataldiagnosis and gene mapping. Ann Genet. 1983;26:133e137.
10. Molinari F, Rio M, Meskenaite V, et al. Truncatingneurotrypsin mutation in autosomal recessivenonsyndromic mental retardation. Science.2002;298:1779e1781.
ocal translocation t(4;20) (q28;q11) associated in a child withdx.doi.org/10.1016/j.apme.2014.07.004

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/