day care specialty books - superior receipt book … · day care specialty books ... tuition paym...
TRANSCRIPT
PLEASE LIST QUANTITY NEXT TO BOOK CHOICE
BEST SELLER! ________ OUCH REPORT ________ CHILD BEHAVIOR REPORT
________ DAILY DIAPER LOG AFTER HOURS LATE ________ FEE RECEIPT
________ TOTAL NUMBER OF BOOKS ORDERED (2 Book Minimum)
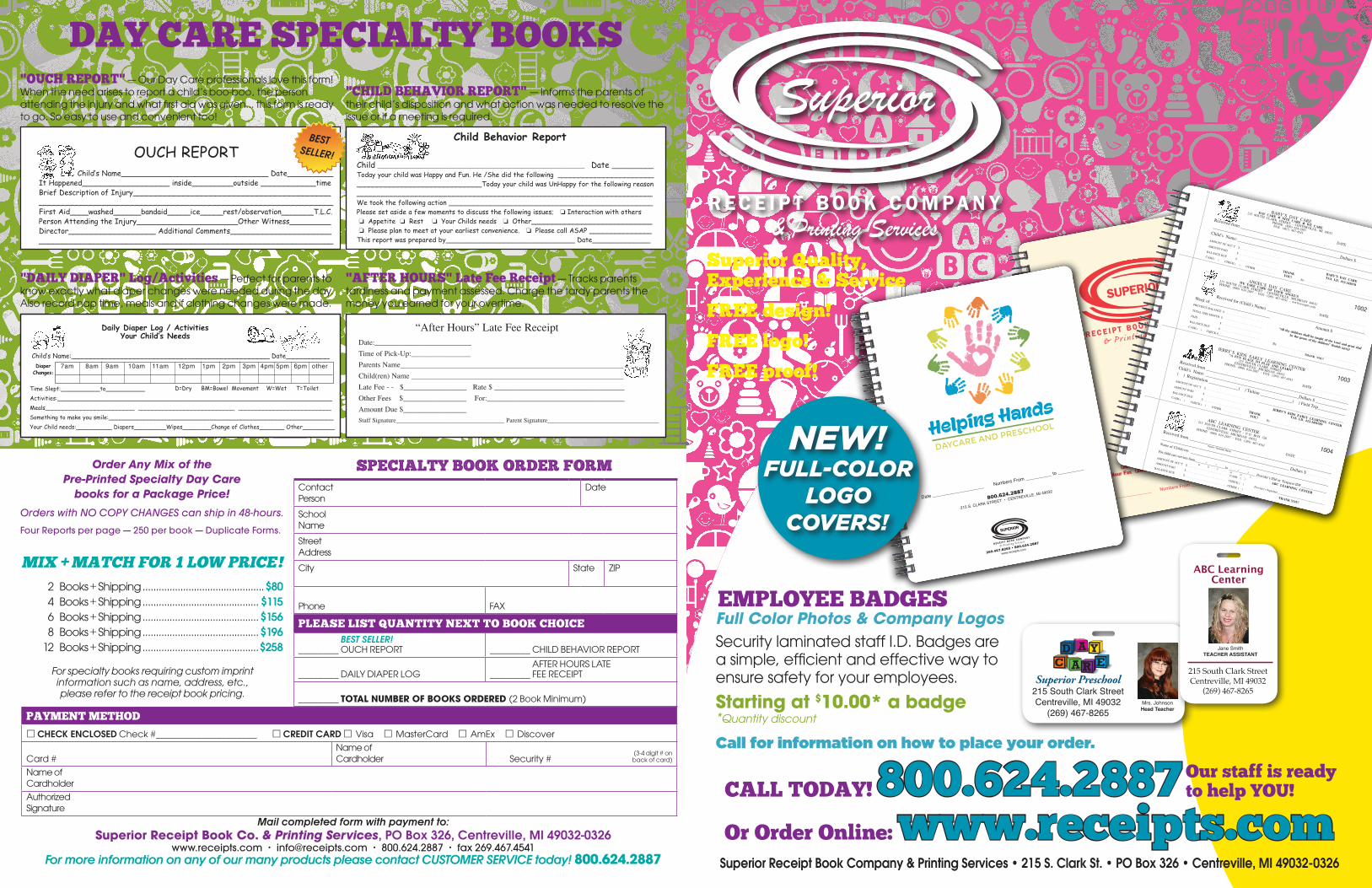
Superior Quality, Experience & Service
FREE design!
FREE logo!
FREE proof!
PAYMENT METHOD
CHECK ENCLOSED Check #____________________ CREDIT CARD Visa MasterCard AmEx Discover
Card #Name of Cardholder
(3-4 digit # on Security # back of card)
Name of CardholderAuthorized Signature
Contact Person
Date
School NameStreet AddressCity State ZIP
Phone FAX
2 Books + Shipping .............................................$80 4 Books + Shipping ........................................... $115 6 Books + Shipping ...........................................$156 8 Books + Shipping ...........................................$196 12 Books + Shipping ...........................................$258
Order Any Mix of the Pre-Printed Specialty Day Care
books for a Package Price!Orders with NO COPY CHANGES can ship in 48-hours.Four Reports per page — 250 per book — Duplicate Forms.
SPECIALTY BOOK ORDER FORM
For specialty books requiring custom imprint information such as name, address, etc., please refer to the receipt book pricing.
Mail completed form with payment to: Superior Receipt Book Co. & Printing Services, PO Box 326, Centreville, MI 49032-0326
www.receipts.com • [email protected] • 800.624.2887 • fax 269.467.4541For more information on any of our many products please contact CUSTOMER SERVICE today! 800.624.2887
DAY CARE SPECIALTY BOOKS
OUCH REPORTChild’s Name________________________________ Date__________
It Happened___________________ inside_________outside ____________timeBrief Description of Injury___________________________________________________________________________________________________________First Aid____washed______bandaid_____ice_____rest/observation_______T.L.C.Person Attending the Injury______________________Other Witness_________Director___________________ Additional Comments______________________________________________________________________________________
"OUCH REPORT" — Our Day Care professionals love this form! When the need arises to report a child’s boo-boo, the person attending the injury and what first aid was given... this form is ready to go. So easy to use and convenient too!
"CHILD BEHAVIOR REPORT" — Informs the parents of their child’s disposition and what action was needed to resolve the issue or if a meeting is required.
Daily Diaper Log / Activities Your Child’s Needs
7am 8am 9am 10am 11am 12pm 1pm 2pm 3pm 4pm 5pm 6pm otherDiaper Changes:
D=Dry BM=Bowel Movement W=Wet T=ToiletTime Slept:___________to___________Activities:_____________________________________________________________________________Meals_________________________ ___________________________ __________________________Something to make you smile:_______________________________________________________________Your Child needs:__________ Diapers_________Wipes________Change of Clothes_______ Other_________
Child’s Name:__________________________________________________ Date___________
Date:__________________________Time of Pick-Up:________________Parents Name____________________________________________________________Child(ren) Name _________________________________________________________Late Fee - - $_________________ Rate $ ___________________________________Other Fees $_________________ For:_____________________________________Amount Due $_________________Staff Signature___________________________________ Parent Signature____________________________________
“After Hours” Late Fee Receipt
"DAILY DIAPER" Log/Activities — Perfect for parents to know exactly what diaper changes were needed during the day. Also record nap time, meals and if clothing changes were made.
"AFTER HOURS" Late Fee Receipt — Tracks parents tardiness and payment assessed. Charge the tardy parents the money you earned for your overtime.
Child ___________________________________________________ Date __________Today your child was Happy and Fun. He /She did the following _____________________________________________________Today your child was UnHappy for the following reason_______________________________________________________________________We took the following action _________________________________________________Please set aside a few moments to discuss the following issues; � Interaction with others � Appetite � Rest � Your Childs needs � Other_____________________________� Please plan to meet at your earliest convenience. � Please call ASAP _______________
This report was prepared by_______________________________ Date______________
Child Behavior Report
MIX + MATCH FOR 1 LOW PRICE!
BEST SELLER!
SUPERIOR
R EC E I PT B OO K C O M PA N Y
& P r int ing S e r v i c e s
Date ____________________ Numbers From __________ to __________
215 South Clark Street, P.O. Box 326
Centreville, MI 49032
(269) 467-8265 • (800) 624-2887
24-Hour Fax (269) 467-4541 • www.receipts.com
800.624.2887
215 S. CLARK STREET • CENTREVILLE, MI 49032
SUPERIOR
R EC E I PT B OO K C O M PA N Y
& P r int ing S e r v i c e s
Date ____________________ Numbers From __________ to __________
269.467.8265 • 800.624.2887
www.receipts.com
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ____________________________________________________________________
____________________________________________________________Dollars $ . . . . . . . . . . . . . . . . . . .
Child’s Name: ____________________________________________________________________
AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .______________________________________________________________
AMOUNT PAID$ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE$ . . . . . . . . . . . . . . . . . . . . . . . . . . .
THANK
CASH ( ) CHECK ( ) OTHER . . . . . . . . . . . . YOU!By . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BABY’S DAY CARE
DAY CARE � NITE CARE � WE CARE
215 SOUTH CLARK STREET - CENTERVILLE, MI 49032
PHONE: (800) 624-2887FAX: (467) 467-4541
BABY’S DAY CARETAX I.D. #12-345678
1001
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received for (Child’s Name) _______________________________________________
Week of ____________________________ Amount $ . . . . . . . . . . . . . . . . . . . . . .
TOTAL THIS MONTH $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PAID
$ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE$ . . . . . . . . . . . . . . . . . . . . . . . . . . .
CASH ( ) CHECK #_______________________
THANK YOU!
ANGEL’S DAY CARE
WE TAKE CARE OF YOUR ANGEL’S
215 SOUTH CLARK STREET - CENTREVILLE, MICHIGAN 49032
PHONE: (800) 624-2887 - FAX: (269) 467-4541 - www.receipts.com
“All thy children shall be taught of the Lord and great shall
be the peace of thy children” (Isaiah 54:13)
PREVIOUS BALANCE $ . . . . . . . . . . . . . . . . . . . . . . . . . .
By. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1002
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ____________________________________________________________________
Child’s Name: ____________________________________________Dollars $ ________________
( ) Registration ______________( ) Tuition _______________( ) Field Trip______________
AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .______________________________________________________________
AMOUNT PAID$ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE$ . . . . . . . . . . . . . . . . . . . . . . . . . . .
THANK
CASH ( ) CHECK ( ) OTHER . . . . . . . . . . . . YOU!By . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
JERRY’S KIDS EARLY LEARNING CENTER
“A FUN PLACE TO PLAY AND LEARN”
215 SOUTH CLARK STREET
CENTREVILLE, MICHIGAN 49032
PHONE: (800) 624-2887 - FAX: (269) 467-4541
JERRY’S KIDS EARLY LEARNING CENTER
TAX I.D. #12-3456789
1003
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ____________________________________________________________________
____________________________________________________________ Dollars $ . . . . . . . . . . . . . . . . . .
Name of Child(ren): __________________________________________________________________
For child care services from______/_____/_____to _____/_____/____ Provider’s SS# or Taxpayer ID# _______________
AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . CASH ( )
AMOUNT PAID$ . . . . . . . . . . . . . . . . . . . . . . . . . . . . CHECK ( )
Provider’s Signature__________________________________
BALANCE DUE$ . . . . . . . . . . . . . . . . . . . . . . . . . . . . OTHER ( )
THANK YOU!
ABC LEARNING CENTER
215 SOUTH CLARK STREET - P. O. BOX 326
CENTREVILLE, MICHIGAN 49032
PHONE: (800) 624-2887 - FAX: (269) 467-4541
ABC LEARNING CENTER
Parent / Guardian Name
M D Y M D Y
1004
Superior Preschool215 South Clark StreetCentreville, MI 49032
(269) 467-8265Mrs. Johnson Head Teacher
EMPLOYEE BADGESFull Color Photos & Company Logos Security laminated staff I.D. Badges are a simple, efficient and effective way to ensure safety for your employees.
Starting at $10.00* a badge *Quantity discount
Call for information on how to place your order.
800.624.2887800.624.2887CALL TODAY! Our staff is ready to help YOU!
Or Order Online: www.receipts.com
ABC LearningCenter
215 South Clark StreetCentreville, MI 49032
(269) 467-8265
Jane Smith TEACHER ASSISTANT
Superior Receipt Book Company & Printing Services • 215 S. Clark St. • PO Box 326 • Centreville, MI 49032-0326
SELECT FROM AVAILABLE LOGOS (Please check the correct box)
CUSTOM LOGO SUPPLIED: Enclosed with Order Form Sent via Email to [email protected]
1 2 4 5 6
1910987
24
from this
CALL800.624.2887
RECEIPT BOOK ORDER FORM
SELECT QUANTITY AND TYPE (Please check the correct boxes)NOW OFFERING CUSTOM COVERS! Quantity Discounts available. Call 800.624.2887
2 books $132.24 Add logo cover + $11.12
8 books $307.44 Add logo cover + $22.24
16 books $511.20 Add logo cover + $27.36
4 books $181.96 Add logo cover + $20.60
12 books $395.64 Add logo cover + $26.21
24 books $727.44 Add logo cover + $32.64
6 books $242.22 Add logo cover + $21.30
DUPLICATE (250/book) TRIPLICATE (180/book)
TOTAL THIS ORDER $_______________
Format: DC1002
Format: DC1003
Format: DC1004
Format: DC1005
Format: DC1006
AVAILABLE FORMATSFormats can be customized with your changes at NO CHARGE!
Format: DC1001
PROOF REQUIRED (Please check the correct box)
1st and 2nd Proofs are free — additional are $7 per revision
YES! Email to: No proof neededContact Person
Date
Business NameSlogan
Street AddressCity State ZIP
Phone FAX
Starting @ Number:____________________________(IF LEFT BLANK, 1001)
CHOOSE FROM ONE OF SIX FORMATS:
Receipt books come with 4 receipts per page, are available as duplicate (250 per book) or triplicate (180 per book), measure 7 5/8" x 2 3/4"
and have a 7/8" bound tear-off on the left.
Mail completed form with payment to: SUPERIOR RECEIPT BOOK CO. & Printing Services
PO Box 326, Centreville, MI 49032-0326www.receipts.com • [email protected] • 800.624.2887 • fax 269.467.4541
SELECT FORMAT (Please check the correct box)
DC1001 DC1002 DC1003 DC1004 AT1005 DC1006 DCIN1007 (Custom Format or provide your own sample)
PAYMENT METHOD
CHECK ENCLOSED Check #____________________
CREDIT CARD Visa MasterCard AmEx Discover
Card #
Expiration Date(3-4 digit # on
Security # back of card)
Name of CardholderAuthorized Signature
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ________________________________________________________________________________________________________________________________Dollars $ . . . . . . . . . . . . . . . . . . .
Child’s Name: ____________________________________________________________________AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . ______________________________________________________________
AMOUNT PAID $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . . THANKCASH ( ) CHECK ( ) OTHER . . . . . . . . . . . . YOU! By . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BABY’S DAY CAREDAY CARE � NITE CARE � WE CARE
215 SOUTH CLARK STREET - CENTERVILLE, MI 49032PHONE: (800) 624-2887
FAX: (467) 467-4541
BABY’S DAY CARETAX I.D. #12-345678
1001
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received for (Child’s Name) _______________________________________________Week of ____________________________ Amount $ . . . . . . . . . . . . . . . . . . . . . .
TOTAL THIS MONTH $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PAID $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . .
CASH ( ) CHECK #_______________________ THANK YOU!
ANGEL’S DAY CAREWE TAKE CARE OF YOUR ANGEL’S
215 SOUTH CLARK STREET - CENTREVILLE, MICHIGAN 49032PHONE: (800) 624-2887 - FAX: (269) 467-4541 - www.receipts.com
“All thy children shall be taught of the Lord and great shallbe the peace of thy children” (Isaiah 54:13)
PREVIOUS BALANCE $ . . . . . . . . . . . . . . . . . . . . . . . . . .
By. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1002
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ____________________________________________________________________Child’s Name: ____________________________________________Dollars $ ________________( ) Registration ______________( ) Tuition _______________( ) Field Trip______________AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . ______________________________________________________________
AMOUNT PAID $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . . THANKCASH ( ) CHECK ( ) OTHER . . . . . . . . . . . . YOU! By . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
JERRY’S KIDS EARLY LEARNING CENTER“A FUN PLACE TO PLAY AND LEARN”
215 SOUTH CLARK STREETCENTREVILLE, MICHIGAN 49032
PHONE: (800) 624-2887 - FAX: (269) 467-4541
JERRY’S KIDS EARLY LEARNING CENTERTAX I.D. #12-3456789
1003
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ________________________________________________________________________________________________________________________________ Dollars $ . . . . . . . . . . . . . . . . . .
Name of Child(ren): __________________________________________________________________For child care services from______/_____/_____to _____/_____/____ Provider’s SS# or Taxpayer ID# _______________
AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . CASH ( )
AMOUNT PAID $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . CHECK ( ) Provider’s Signature__________________________________
BALANCE DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . OTHER ( ) THANK YOU!
ABC LEARNING CENTER215 SOUTH CLARK STREET - P. O. BOX 326
CENTREVILLE, MICHIGAN 49032PHONE: (800) 624-2887 - FAX: (269) 467-4541
ABC LEARNING CENTER
Parent / Guardian Name
M D Y M D Y
1004
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ________________________________________________________________________________________________________________________________Dollars $ . . . . . . . . . . . . . . . . . . .
In re: __________________________________________________________________________AMOUNT OF ACC’T $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . ______________________________________________________________
AMOUNT PAID $ . . . . . . . . . . . . . . . . . . . . . . . . . . . .
BALANCE DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . . THANKCASH ( ) CHECK ( ) OTHER . . . . . . . . . . . . YOU! By . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CENTREVILLE COMMUNITY DAYCARE215 SOUTH CLARK STREET - P. O. BOX 326
CENTREVILLE, MICHIGAN 49032PHONE: (800) 624.2887 - FAX: (269) 467-4541
www.receipts.com - [email protected]
CENTREVILLE COMMUNITY DAYCARE
1005
DATE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Received from ______________________________________________________________________Name of Child(ren): __________________________________________________________________( ) Registration ________________ ( ) Tuition _________________ ( ) Drop-In ________________For child care services from______/_____/_____to _____/_____/____ Tax I.D. # 12-3456789AMOUNT DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . CASH ( )
AMOUNT PAID $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . CHECK ( ) Provider’s Signature__________________________________
BALANCE DUE $ . . . . . . . . . . . . . . . . . . . . . . . . . . . . OTHER ( ) THANK YOU!
MY FAMILY DAY CARE HOMEHOME AWAY FROM HOME
215 SOUTH CLARK STREET - P. O. BOX 326CENTREVILLE, MICHIGAN 49032
PHONE: (800) 624-2887 - FAX: (269) 467-4541
MY FAMILY DAY CARE HOME
Parent / Guardian Name
M D Y M D Y
1006
DATE:____________________________
Received from________________________________________________Dollars $_____________
Child’s Name:____________________________Class Name: ______________________________
Memo: __________________________________________________________________________
REGISTRATION FEE:TUITION PAYMENT FOR WEEK BEGINNING___________________________________ ENDING ______________________________
PAYMENT ON TUITION ACCOUNT____________________________________________ BAL DUE _____________________________
THANK YOU! By ___________________________________________________
SUPERIOR WEEKDAY PRESCHOOL215 SOUTH CLARK STREET - P. O. BOX 326
CENTREVILLE, MICHIGAN 49032PH: (800) 624-2887 - FAX: (269) 467-4541
www.receipts.com - [email protected]
� ��
Cus
tom
For
mat
Fo
rmat
: DC
1007
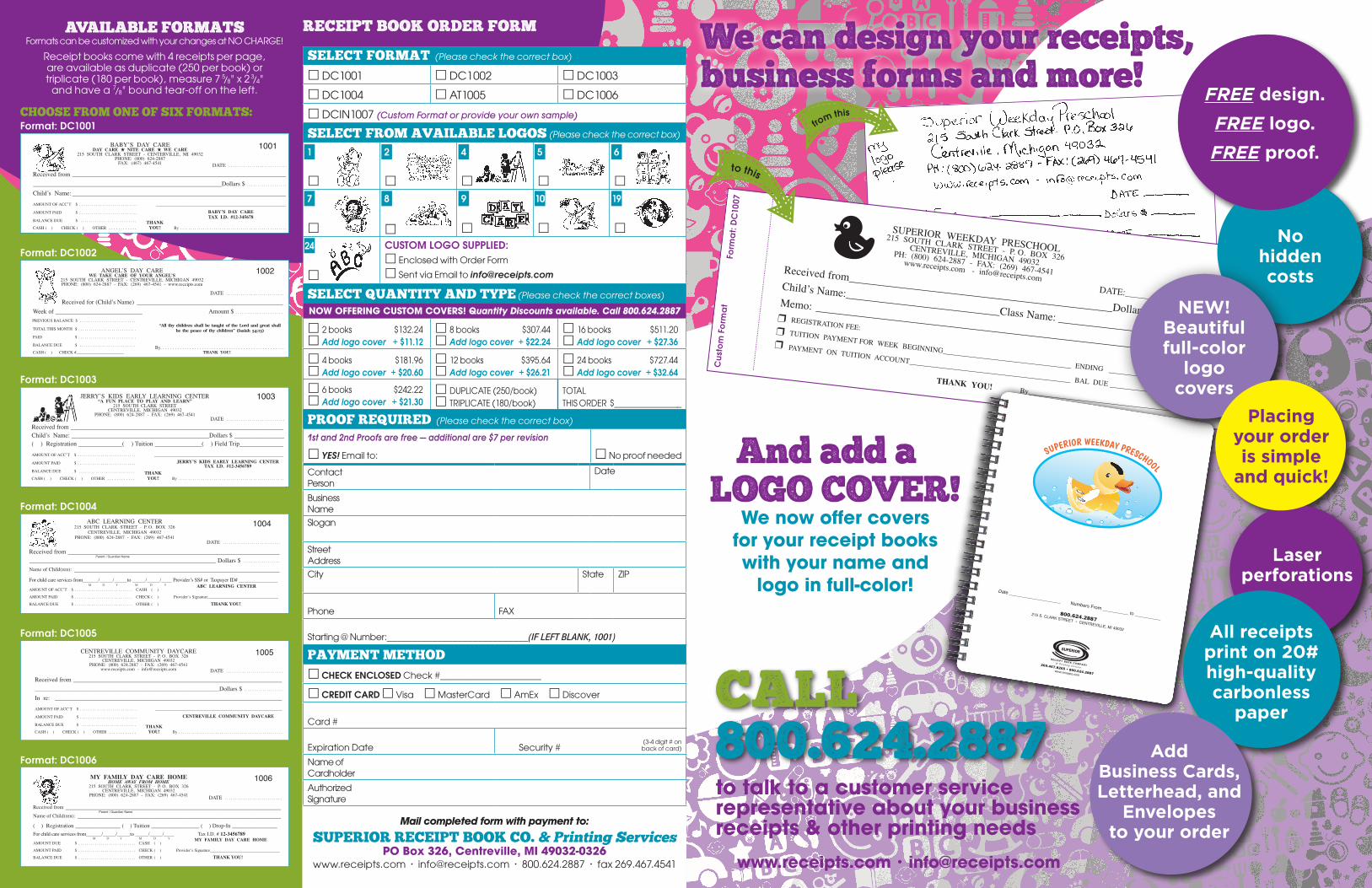
We can design your receipts, business forms and more!
to this
And add a …LOGO COVER!
We now offer covers for your receipt books with your name and
logo in full-color!800.624.2887
215 S. CLARK STREET • CENTREVILLE, MI 49032
SUPERIOR
R EC E I PT B OO K C O M PA N Y& P r int ing S e r v i c e s
Date ____________________ Numbers From __________ to __________
269.467.8265 • 800.624.2887www.receipts.com
SUPERIOR WEEKDAY PRESCHOOL
to talk to a customer service representative about your business receipts & other printing needs
www.receipts.com • [email protected]
No hidden costs
Laser perforations
FREE design.FREE logo.FREE proof.
NEW! Beautiful full-color
logo covers
Placing your order is simple
and quick!
All receipts print on 20# high-quality carbonless
paper
Add Business Cards, Letterhead, and
Envelopes to your order