dafne educator programme (dep) version 11 - dep... · practical use of the glycaemic index ......
TRANSCRIPT

DAFNE © T01.002, Version 10 – October 2010
DAFNE Educator Programme (DEP)
Training Workshop Curriculum

DAFNE © T01.002, Version 10 – October 2010 1
CONTENTS DEP Training Workshop
Day 1 – (slide and handout) ................................................................................................. 6
Delegate List ........................................................................................................................ 7
Day 1: Welcome, Housekeeping and Introductions .................................................................... 8-10
DEP Training Workshop (slide) .................................................................................... 11
DEP “Steps” (slide) ....................................................................................................... 12
Aims in Step 4 (slide) .................................................................................................... 13
What should I collect in my DEP file? (slide and handout) ........................................... 14 Experiences of observing a DAFNE course ....................................................................... 15 Experiences of observing (slide) ......................................................................................... 16
Attitude 15 Questionnaire ......................................................................................... 17-19 The DAFNE philosophy ................................................................................................ 20-23
The DAFNE philosophy (handout – double side and stapled) .................................. 24-26
Aims of DAFNE (slide) .................................................................................................. 27
DAFNE beliefs and values (slide) ................................................................................. 28
What are the aims of the DAFNE philosophy (slide) ..................................................... 29
Educator behaviours (slide and handout) ..................................................................... 30
The DAFNE approach to food ...................................................................................... 31
DAFNE principles (slide) .............................................................................................. 32 Practical use of the glycaemic index ............................................................................. 33-34
Glycaemic Index (slides) ......................................................................................... 35-37
DEP glycaemic index game (laminate and cut) ....................................................... 38-47
The glycaemic index (slide) .......................................................................................... 48
The glycaemic index and DAFNE (slide) ...................................................................... 49 The DAFNE approach to food – Lunchtime CP counting .................................................... 50
DAFNE and food worksheet (handout) ......................................................................... 51
Estimating CHO food diary (handout as a booklet or double side and stapled) ............. 52-59 Estimating difficult carbohydrates ................................................................................. 60-61
Lunch CP counting exercise (slide) .............................................................................. 62
Workstation 1 guidelines (handout) ............................................................................... 63
Workstation 2 guidelines (handout) .............................................................................. 64
Food labels exercise (handout) .................................................................................... 65
Food labels exercise answers (slide) ............................................................................ 66
Workstation 3 guidelines (handout) .............................................................................. 67
Snacks and DAFNE exercise (handout – double side) ............................................ 68-69
Snacks and DAFNE exercise answers (slide) ......................................................... 70-71
Workstation 4 guidelines (handout) .............................................................................. 72

DAFNE © T01.002, Version 10 – October 2010 2
Starting and adjusting the DAFNE insulin regime ......................................................... 73-76
Commencing the DAFNE insulin regime (handout) ...................................................... 77
Long-acting insulin analogue and DAFNE (handout) ............................................... 78-79
Using the DAFNE dose adjustment examples (handout) ............................................. 80
Explanation of dose adjustment examples (slides and handout–double side) .......... 81-82 Unfolding case example 1 (slide and handout) .................................................................. 83 Unfolding case example 1 (slides) (page 91 only as handout) ...................................... 84-91 Unfolding case example 1 (trainer notes/discussion points) ....................................... 92-100 Unfolding case example 2 (slides) (page 108 only as handout) ................................ 101-108 Unfolding case example 2 (trainer notes/discussion points) ..................................... 109-117 Unfolding case example 3 (slides) (page 125 only as handouts) ............................... 118-125 Unfolding case example 3 (trainer notes/discussion points) ..................................... 126-134 Insulin Dose Reduction: Isophane/Levemir examples (slides & handouts–double side) . 135-140 Insulin Dose Escalation: Isophane/Levemir examples (slides & handouts–double side) 141-146 Insulin Dose Adjustment/Corrections (slides and handouts – double sided) .............. 147-149 Insulin Dose Reduction: Lantus examples (a] as slides and handouts – b] slides only) . 150-163 Insulin Dose Escalation: Lantus examples (a] as slides and handouts – b] slides only) .. 164-175 Homework task – day 1 .................................................................................................... 176
DAFNE © T01.002, Version 10 – October 2010 3
Day 2: Day 2 – (slide and handout) ............................................................................................... 177 Feedback from homework – day 2 ..................................................................................... 178 Therapeutic patient education and adult education theories ....................................... 179-183
Therapeutic patient education (slide) ............................................................................ 184
Cycle of experiential learning (slide) ............................................................................. 185
Adult learning theory (slide) .......................................................................................... 186
Social learning theory (slide) ........................................................................................ 187
An overview of educational theories underpinning DAFNE (handout) .......................... 188 The DAFNE curriculum and lesson planning .............................................................. 189-190
Basic principles of adult learning (slide) ....................................................................... 191
Checklist for preparing lesson plans (slide and handout) ............................................. 192
What is a curriculum? (slide) ........................................................................................ 193
DAFNE curriculum example (slides) ...................................................................... 194-196 Writing lesson plans: Getting some practise ...................................................................... 197
Blank lesson plan (handout – not stapled x 8 copies per delegate) ....................... 198-199
Example lesson plan (slide) ................................................................................... 200-202 Sharing ideas/strategies for specific sessions ............................................................ 203-204 DAFNE: Exercise Physiology – Educator Notes (handout) ......................................... 205-210
Workstation 1 - Sick day rules (slides) ................................................................... 211-213
Workstation 1 - Sick day rules examples (a] handouts, b] slides) .......................... 214-217
Workstation 2 - Alcohol scenarios 1 (handout) ............................................................. 218
Workstation 2 - Alcohol scenarios 1 answers (slide) .............................................. 219-220
Workstation 2 - Alcohol and DAFNE 2 (handout) ......................................................... 221
Workstation 2 - Alcohol and DAFNE 2 answers (slide) ................................................. 222
Workstation 2 - Alcohol scenarios 3 (handout) ............................................................. 223
Workstation 3 - DAFNE and Exercise (handout – double side) ............................. 224-225
Workstation 3 - DAFNE and Exercise answers (slide) .................................................. 226
Workstation 3 - Physical activities scenarios (handout) ................................................ 227
Workstation 3 - Physical activities scenarios answers (slide) ........................................ 228
Workstation 4 – Annual Review – Planning Difficult Sessions ...................................... 229
Workstation 4 – Annual Review Worksheet (handout) ................................................. 230 Therapeutic patient education and adult education theories ....................................... 179-183
Therapeutic patient education (slide) ............................................................................ 184
Cycle of experiential learning (slide) ............................................................................. 185
Adult learning theory (slide) .......................................................................................... 186
Social learning theory (slide) ........................................................................................ 187
An overview of educational theories underpinning DAFNE (handout) .......................... 188 Goal Setting and Action Planning ............................................................................... 231-334

DAFNE © T01.002, Version 10 – October 2010 4
Day 3: Day 3 – (slide and handout) ............................................................................................... 235 Managing groups: Tips/scenarios ................................................................................. 236-37
Strategies for effective group processes – use ground rules (slide) ............................. 238
Strategies for effective group processes – become a facilitator (slide) ......................... 239
Helping groups work more effectively (handout – double side) ................................... 240-241
10 Interventions for regaining control (handout – double side) .............................. 242-243
Dealing with difficult participants (handout) .................................................................. 244
Dealing with difficult participants (game – use at own discretion) .......................... 245-253
Coping with problem participants (game - use at own discretion) ......................... 254-255
Card game (cut and laminate) ............................................................................... 256-257 Preparation for peer review ......................................................................................... 258-260
DoH structured education criteria (slide) ...................................................................... 261
Who are the reviewers (slide) ....................................................................................... 262
Ground rules for the DEP reviewer (slide) .................................................................... 263
Peer reviewed course – our expectations (slide) .......................................................... 264
DEP review documentation (slides) ....................................................................... 265-274
Effective recruitment strategies .......................................................................................... 275
Patient recruitment criteria (slide) ................................................................................. 276
Sheffield recruitment strategy (slide) ............................................................................ 277 Pre-course appointment/data collection: practise ....................................................... 278-279
Pre-course appointment exercise (handout) ................................................................. 280
Blank pre-course core data collection form (handout) .................................................. 281
Standard operating procedure (handout – double side and stapled) ..................... 282-289
Blank pre-course full data collection form (handout – double side and stapled) .... 290-293
Standard operating procedure (handout – double side and stapled) ..................... 294-308
EQ-5D (handout – double side and stapled) ......................................................... 309-313
PAID (handout) .............................................................................................................. 314
HADS (handout) ........................................................................................................... 315
DSQoL ................................................................................................................... 316-320
SF12 ...................................................................................................................... 321-323
Follow-up and support from DAFNE ‘graduates’ ......................................................... 324-325
Initial follow-up (slide) ................................................................................................... 326
Recurring follow-up (slides) .......................................................................................... 327
Catering arrangements and DAFNE resources .......................................................... 328-331
Choose a venue (slide) ................................................................................................. 332
Catering arrangements (slide) ...................................................................................... 333
DAFNE resources (slide) .............................................................................................. 334
Local resources (slide) ................................................................................................. 335
DAFNE resources purchase requisition (slide) ............................................................. 336
Delivering DAFNE locally – personal plan ......................................................................... 337
Personal plan (handout – double side) .................................................................. 338-339
Summary/feedback/evaluation .................................................................................... 340-341
Evaluation form (handout – double side) ............................................................... 342-343
DAFNE © T01.002, Version 10 – October 2010 5
1-Day Follow-Up Workshop Programme – (slide and handout) ..................................................................................... 344 Delegate List ...................................................................................................................... 345 Welcome, Housekeeping and Introductions ....................................................................... 346
Follow-up Workshop (slide) .......................................................................................... 347 Learning from Each Other’s Experiences .......................................................................... 348
Learning From Each Other’s Experiences (slide) ........................................................ 349 Unresolved Issues/Prioritising Issues for Day .................................................................... 350 DAFNE Curriculum Revisited ............................................................................................. 351
DEP Timetabling Exercise (handout) ....................................................................... 352-53 The DAFNE database – whose responsibilities? ............................................................... 354 Promoting DAFNE Awareness in Your Service ................................................................. 355
DAFNE Awareness Workshop and Case Study (handout–double side and stapled) . 356-358
DAFNE Awareness Workshop and Case Study Answers (slide) .................................. 359
DEP Guidelines for DAFNE Educators (handout–double side and stapled) .......... 360-368
DEP Reviewers Buddy List (handout after September 2009 – double side) .......... 369-370 Quality Assurance for DAFNE ........................................................................................... 371
DoH Structured Education Criteria (slide) ..................................................................... 372
Quality Assurance (Internal – ongoing) (slide) ................................................................ 373
Quality Assurance (External) (slide) ............................................................................. 374 Future Contribution to DAFNE Collaborative ...................................................................... 375
Remit of the DAFNE Collaborative (slide) ..................................................................... 376 Evaluation of DEP and Personal Plan ................................................................................ 377
1-Day Follow-Up Evaluation Form (handout – double side) .................................. 378-379
Personal Plan following Peer Reviewed Course (handout – double side) ............. 380-381

DAFNE © T01.002, Version 10 – October 2010 6
DAFNE Educator Programme (DEP)
Training Workshop
Day 1
08:45 ARRIVE and TEA / COFFEE
09:00 Welcome, ‘housekeeping’ and introductions Aims and expectations of the workshop 09.30 Experiences of observing a DAFNE course
10:00 TEA / COFFEE
10:15 The DAFNE Philosophy: ‘Can you tell what it is yet….?’
11:00 The DAFNE approach to food Practical use of the Glycaemic Index
12:30 LUNCH
13.15 Estimating difficult CHOs; advice for snacks; working out CPs
from food labels
14:45 TEA / COFFEE
15:00 Starting and adjusting the DAFNE insulin regime: Case studies and curriculum dose adjustment examples 17:00 ‘Homework’ tasks
DAFNE © T01.002, Version 10 – October 2010 7
DEP TRAINING WORKSHOP (venue) (date)
Delegate list
Name Profession Hospital

DAFNE © T01.002, Version 10 – October 2010 8
WELCOME, HOUSEKEEPING AND INTRODUCTIONS LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should…. Be informed of location of toilets, fire exits, etc. Feel welcomed and valued and able to contribute to the programme.
Describe location of toilets and fire escapes. Explain procedure if fire alarm sounds (also if any alarm tests expected on the day). Welcome of participants by trainers and introduction of trainers/guests. Illustrate outline of DEP and explain how the training workshop fits into programme. Thank participants for attending observation weeks and completing the tasks as directed. Explain we are all continuing to learn from DAFNE and current Educators are excited about receiving feedback and experience from trainees to further develop the programme. Ask participants to contribute/question/comment through the workshop to gain as much as they need to in preparing to teach DAFNE themselves. Stress that materials used in the DEP workshop have been specifically developed to train Educators and may not be suitable/appropriate to use in DAFNE (patient) courses.
OHP and title acetate Acetate – DEP outline
Get to know each other.
Ask participants to introduce themselves to the rest of the group, indicating their profession, place of work and how they became interested/involved in DAFNE.
Name badges/sticker

DAFNE © T01.002, Version 10 – October 2010 9
WELCOME, HOUSEKEEPING AND INTRODUCTIONS LEARNING GOALS METHODS MATERIALS/MEDIA
Share individual expectations of the DEP training workshop. Identify sessions that they would like to spend time discussing during the 3 day DEP.
Ask participants in pairs (or 3’s) to discuss their expectations of the training workshop and feedback to the rest of the group. Ask, were there any sessions that you feel you would like to spend time discussing during the DEP? Collect onto flipchart-stick on wall for later (Day 2) Explain that these will be kept on the wall to come back to later.
Flip chart and pens Flip chart and pens
Be aware of the aims and structure of the training workshop.
Illustrate and discuss the aims of ‘Step 4’. Outline the programme: Day 1, Day 2 and Day 3 (copy of the full programme is included in the DEP files). Explain that there will be homework tasks to allow us to get the most out of the 3 days. Explain Day 1 consolidates experiences from observation week and develops core DAFNE skills: Day 2 enables sharing ideas and practising lesson planning: day 3 prepares for peer reviewed course and looks at strategies for setting up DAFNE in new centres.
Acetate – Aims (page 28 DEP file) Acetates/handouts
Explain the evidence/paperwork they should be accumulating in their DEP file. Explain the importance of continuing to deliver DAFNE as a 5-day out-patient course at present.
‘What should I collect in my DEP file?’

DAFNE © T01.002, Version 10 – October 2010 10
WELCOME, HOUSEKEEPING AND INTRODUCTIONS LEARNING GOALS METHODS MATERIALS/MEDIA
Feel able to discuss unresolved issues from their preparatory work and observation week.
Ask participants to list any issues noted on their forms 2.10 2.11 and 3.6 in DEP file and stick onto prep-prepared flip chart.
Flip chart Post-it notes
Be made aware that they will be asked to complete a detailed evaluation form at the end of the 3 days to help.
Ask participants to look in their folders and find the evaluation forms. Sections of this form can be filled in at the end of each day or the whole form can be completed at the end of the 3 days. Stress how crucial feedback is to developing and improving the DEP process.
NOTE FOR TRAINERS PLEASE COLLECT OBSERVATION COURSE FEEDBACK FORMS FROM DELEGATES
DEP folders DEP evaluation form

DAFNE © T01.002, Version 10 – October 2010 11
DAFNE EDUCATOR PROGRAMME (DEP)
TRAINING WORKSHOP

DAFNE © T01.002, Version 10 – October 2010 12
DEP “steps”
1. Orientation
2. Background reading
3. Observational course
4. Training workshop
5. Personal preparation time
6. Peer-reviewed course
7. Follow up workshop
DAFNE © T01.002, Version 10 – October 2010 13
Aims in Step 4
Review and consolidate knowledge of nutrition and develop
competencies in applying this to DAFNE.
Review and consolidate knowledge of insulin regime and develop competencies in applying this to DAFNE.
Anticipate the demands of being a DAFNE educator and have plans for meeting these.
Reflect upon adult learning and patient empowerment skills.
Prepare for peer-reviewed course.

DAFNE © T01.002, Version 10 – October 2010 14
“What should I collect in my DEP File?”
Evidence of pre-course reading: Completed pages:
Signed copy of The Learning Contract (1.7)
“Questions to consider to help assimilate the reading material” (2.10)
“Remaining questions and issues” (2.11)
Evidence from observation week: Completed forms:
Observation sheets for all relevant sessions (3.7)
“Issues arising from observation week” (3.6)
“DAFNE Attitude 15 Questionnaire” Case study based on guidelines in DEP File (3.4) Additional notes taken during week
Evidence from training workshop: Notes and supporting materials from sessions and workshops Additional resources / materials collected Personal Plan for delivering DAFNE locally
Evidence from peer-supported course: Personal lesson plans for all relevant sessions Copies of DEP Reviewer’s completed documentation:
Evidence Forms
Learning Outcomes Forms
Summary Forms Additional notes of self-evaluation
Evidence from follow up workshop: Notes and supporting materials from workshop Additional resources collected Personal plan for development
Continuous Professional Development: Evidence from peer-supported course (as above) “Internal” Quality Assurance review documentation

DAFNE © T01.002, Version 10 – October 2010 15
EXPERIENCES OF OBSERVING A DAFNE COURSE LEARNING GOALS METHODS MATERIALS/MEDIA
Have the opportunity to share experiences of observing a DAFNE course. Become familiar with a range of attitudes to DAFNE.
Pairs / small groups to discuss their observation week:
What went well?
What didn’t go well?
Was there anything that made you feel uncomfortable?
Have your perceptions of attitudes to DAFNE changed? Large group feedback. Perceptions / changes of note listed on flipchart.
Acetate of guidelines for discussion of observation week DAFNE Attitude 15 Questionnaires Flip chart and pens

DAFNE © T01.002, Version 10 – October 2010 16
Experiences of observing a
DAFNE course
What went well?
What didn’t go well?
Was there anything that made you feel uncomfortable?
Have your perceptions or attitudes to DAFNE changed?
DAFNE © T01.002, Version 10 – October 2010 17
DAFNE ATTITUDE 15 QUESTIONNAIRE
Whilst much of the DEP is focused on knowledge and skills, to become competent (as a DAFNE Educator) it also helps to consider attitude. This was a key part of the early preparation of the original DAFNE Educators after the visit to Germany and their many visits to us. Unfortunately there is little time for long discussion about attitudes during the DEP. For this reason we have developed the DAFNE Attitude 15 Questionnaire which is designed to help you express your thoughts. There are no right and wrong answers as each can be qualified or pre-empted by an argument. The important part of the DEP is that you have at least given these issues some thought.
AIM To explore beliefs about DAFNE Please answer each question by saying how much you agree or disagree, and then use the explanation line to qualify your response if it feels necessary. 1 Patients just need support and encouragement to improve their diabetes control.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
.......................................................................................................................................... 2 Most Health Care Professionals know more about controlling blood sugar levels than
most people with Type 1 diabetes.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
3 People learn more when they feel safe, and free of criticism.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
4 People differ in how quickly they learn.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................

DAFNE © T01.002, Version 10 – October 2010 18
5 It is better to listen to patients than achieve all the objectives in the DAFNE programme.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
6 Learning in groups will always mean that people do better.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
7 After attending a DAFNE course, a patient should need significantly less help in subsequent clinics.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
8 Having explicit learning objectives stops you from being patient centred.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
9 If a person picks up knowledge quickly, then they will acquire a skill quickly.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
10 It will be possible to predict which patients do well, and which have difficulty with DAFNE.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................

DAFNE © T01.002, Version 10 – October 2010 19
11 You can teach attitudes (good, bad, like, dislike) through providing information.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
12 If you can’t count carbohydrates, you cannot do DAFNE.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
13 After two months of DAFNE people should know all that is necessary to control blood sugar levels.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
14 It is more important to concentrate on objectives than enthusiasm during the DAFNE programme.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
15 DAFNE has been developed over several years – it is as good as it gets.
Disagree Partly disagree Partly agree Strongly agree Explanation: ....................................................................................................................
..........................................................................................................................................
DAFNE © T01.002, Version 10 – October 2010 20
THE DAFNE PHILOSOPHY: CAN YOU TELL WHAT IT IS YET…? LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should…. Be clear about the aims of a philosophy.
Introduce the session to the group (5 mins) When DAFNE was developed it was implicit to the researchers that DAFNE had a clear philosophy. The DAFNE philosophy underpins everything we do, as a whole collaborative and as individuals, it is important that we all understand what the philosophy is and why it is important. Hopefully the reason why we are all here is that we share this philosophy! Since rolling DAFNE out and with the advent of the “DoH/NICE guidelines on structured education programmes for people with diabetes, it has become clear that the original philosophy was getting lost and a decision was made to make this much more explicit. Why have philosophies?( 10 mins) Ask the group:
“What do you think a philosophy is?”
“Why do you think a philosophy is important?” Work in pairs for 5 minutes and collate group answers. Using the group’s responses discuss: A philosophy is a something that determines our core beliefs, attitudes and values and as such will influence our behaviour, thoughts and ideas. The importance of a philosophy is to underpin the content, process and care that shapes the delivery and ongoing development of DAFNE and in theory all education programmes. DAFNE philosophy is drawn from Therapeutic Patient
Blue tack Post- it notes Flipchart paper and pens
DAFNE © T01.002, Version 10 – October 2010 21
Education (in line with the Berger and Assal models) and from Person Centered philosophy.
THE DAFNE PHILOSOPHY: CAN YOU TELL WHAT IT IS YET…? LEARNING GOALS METHODS MATERIALS/MEDIA
Be familiar with the DAFNE philosophy. To have reflected and considered how this will affect their own behaviour as educators delivering DAFNE
What are the aims of the DAFNE philosophy?(10 mins) Discuss the aims of the DAFNE philosophy using acetate with excerpt from philosophy. Ask the group: “how might this be different from traditional methods of education in type 1 diabetes”. Collate the answers, which might include the following:
Autonomy and self management
Confidence and competence
Skills based training
Carbohydrate counting to facilitate insulin dose adjustment
Flexible lifestyle
Experiential learning
Decisions made by the person with diabetes
Responsibility lies with the person with diabetes
Ultimately improved outcomes Facilitate a discussion around these issues, particularly if there are any areas of concern expressed by DEP trainees. Educator behaviours (20mins) Discuss the “Beliefs and Values” from the DAFNE philosophy. Using an acetate. Ask people to spend a moment reading and considering the
Copies of the philosophy Acetate: ‘Aims of DAFNE’ Flipchart and pens Acetate: ‘DAFNE Beliefs and Values’
DAFNE © T01.002, Version 10 – October 2010 22
beliefs and values and ask if there are any areas of concern or anything they disagree with? Lead a short discussion.
THE DAFNE PHILOSOPHY: CAN YOU TELL WHAT IT IS YET…? LEARNING GOALS METHODS MATERIALS/MEDIA
In groups of 3 ask them to list the behaviours that educators might exhibit if they were trying to implement the philosophy. Ask each person to write each comment on a post it note and transfer to flipchart. Answers might include: (option to use pre-prepared acetate)
Use of open questions
Use of reflection to seek clarification and demonstrate empathy
Acknowledging each members contribution
Trying to avoid saying “no”
Allowing opportunities for reflection
Time to practice new skills and gain feedback
Providing space for DAFNE participants to work things out for themselves (problem solving)
Using active learning methods
Avoiding a high percentage of “educator” talk
Providing options rather than absolute answers
Involving all the participants
Non- judgmental attitudes
Honest, accurate and up to date content
Demonstrating Empathy and warmth
Encouraging individuals to set their own goals
Providing support and encouragement
Pace of learning is flexible and fits to the learner
Pre-prepared flipcharts Post-it notes pens

DAFNE © T01.002, Version 10 – October 2010 23
Acknowledging previous experience and expertise
THE DAFNE PHILOSOPHY: CAN YOU TELL WHAT IT IS YET…? LEARNING GOALS METHODS MATERIALS/MEDIA
Allowing participants to be responsible for their own learning Ensuring participants have as much control as possible over the process and decisions made
Non threatening, relaxed and enjoyable
Positive encouragement of group/individuals
Responds to the group atmosphere
The DEP trainer discussed that these behaviours are important and reflect style of delivery of a DAFNE course. Much of this forms part of what is assessed in DEP peer review.
DAFNE © T01.002, Version 10 – October 2010 24
The DAFNE Philosophy The philosophy is the foundation upon which the DAFNE programme is based. The philosophy makes explicit the core beliefs, values and attitudes of the members of the DAFNE Collaborative. The DAFNE philosophy is drawn from Therapeutic Patient Education from which the DAFNE programme was derived (1, 2,) and person-centred philosophy that promotes active behaviour change (3). The philosophy underpins the content and processes of diabetes care that guides and shapes the DAFNE programme, its delivery and ongoing development.
Aims The principal aim of the DAFNE programme is to facilitate autonomy, competency and
confidence in the self- management of diabetes by providing skills- based training in the areas of carbohydrate counting and insulin dose adjustment in a comprehensive range of situations. This includes the development of problem solving skills, that ultimately leads to improvement in biomedical and quality of life outcomes in people with type 1 diabetes and eventual improvements in long-term health outcomes
The DAFNE programme aims to enable individuals with type 1 diabetes the ability to have a flexible lifestyle, as it teaches skills that encourages insulin doses to be adapted according to lifestyle choices, using algorithms which can ensure more predictable blood glucose levels and subsequently the experience of a greater sense of personal control.
Through experiential learning the DAFNE programme encourages individuals to become activated self- managers, building on their own experience and expertise within the framework of skills and guidance that DAFNE principles provide.
The DAFNE programme acknowledges that the person with diabetes drives the decision- making process, but aims to encourage the seeking of support when necessary and from whoever is most appropriate to the individual, that will help sustain behaviour change.
The responsibility of DAFNE clinicians is to provide optimal therapeutic educational care so that choices are fully informed, whilst recognising that ultimate responsibility and choice rests with the person with diabetes.
Beliefs and Values The philosophy of DAFNE is essentially person-centred and recognises that responsibility
for self-management lies within the individual with diabetes.
DAFNE philosophy recognises that clinicians have responsibility to but not for people with type 1 diabetes.
The DAFNE philosophy holds the view that human nature is basically constructive and that people aim to maximise their quality of life via the choices given their interpersonal and external circumstances.

DAFNE © T01.002, Version 10 – October 2010 25
In accordance with person-centred philosophy DAFNE clinicians communicate empathy and non-judgemental support for all those who participate in the programme regardless of the decisions they make. These core qualities underpin the conditions that provide open and honest dialogue regarding optimising self-management.
DAFNE clinicians have responsibility to facilitate optimal exploration of values, beliefs and barriers each individual has in relation to his/her diabetes and to provide honest and accurate information about risks and eventualities.
DAFNE philosophy recognises that the sharing of ideas between people with diabetes and health care professionals is a two way process that can facilitate improvements in both service delivery and outcomes for people with diabetes
DAFNE clinicians will act as a resource, facilitating and supporting the process of life-long change in individuals with type 1 diabetes.
Skills and Processes The DAFNE programme provides structured therapeutic education which provides a
problem-solving environment that teaches knowledge and skills in the management of diabetes and builds confidence in making informed choices.
The DAFNE programme is delivered using adult education principles that includes: o being learner- centred through acknowledgement of each individual’s personal
experience and expertise o offering a structured framework for the development of practical therapeutic skills in
dose adjustment and carbohydrate counting, allowing opportunity for practise and experiential learning
o use of open questions and reflections that encourages active participation, personal awareness and the application and practise of new skills
o facilitation of active group participation, in particular, valuing peer group support and the role- modelling of problem solving skills within the group
o encouraging a problem solving approach to personal barriers and consideration of treatment options
o use of goal setting to create personally relevant action plans thereby promoting meaningful involvement of individuals with type 1 diabetes in their own self care
The DAFNE programme has a responsibility to provide the highest standard of content and delivery by adhering to the 4 key criteria that fulfils the NICE requirements (4) (a structured curriculum, trained educators, quality assurance and audit) and by ensuring that all aspects of care discussed is evidence based and accurate.

DAFNE © T01.002, Version 10 – October 2010 26
References 1. Muhlhauser, I, Jorgens V, Berger M et al., Bicentric evaluation of a teaching and treatment
programme for Type 1 (insulin-dependent) diabetic patients: improvement of metabolic control and other measures of diabetes care for up to 22 months. Diabetologia, 1983. 25: (6) : 470-476.
2. Muhlhauser I, Berger M. Evidence-based patient information in diabetes. Diabetic
Medicine. 2000. 17 (12):823-829 3. Anderson RM, Funnell MM. The Art of Empowerment Stories and Strategies for Diabetes
Educators. 2nd Edition. (2005) American Diabetes Association. Virginia 4. Structured patient education working group: Report from the Patient Education Working
Group. Department of Health. 2005

DAFNE © T01.002, Version 10 – October 2010 27
Aims of DAFNE
The principal aim of the DAFNE programme is to facilitate autonomy, competency and confidence in the self- management of diabetes by providing skills- based training in the areas of carbohydrate counting and insulin dose adjustment in a comprehensive range of situations. This includes the development of problem solving skills that ultimately leads to improvement in biomedical and quality of life outcomes in people with type 1 diabetes and eventual improvements in long-term health outcomes.
The DAFNE programme aims to enable individuals with type 1 diabetes the ability to have a flexible lifestyle, as it teaches skills that encourage insulin doses to be adapted according to lifestyle choices, using algorithms which can ensure more predictable blood glucose levels and subsequently the experience of a greater sense of personal control.
Through experiential learning the DAFNE programme encourages individuals to become activated self- managers, building on their own experience and expertise within the framework of skills and guidance that DAFNE principles provide.
The DAFNE programme acknowledges that the person with diabetes drives the decision- making process, but aims to encourage the seeking of support when necessary and from whoever is most appropriate to the individual, that will help sustain behaviour change.
The responsibility of DAFNE clinicians is to provide optimal therapeutic educational care so that choices are fully informed, whilst recognising that ultimate responsibility and choice rests with the person with diabetes.
DAFNE © T01.002, Version 10 – October 2010 28
DAFNE Beliefs and Values
The philosophy of DAFNE is essentially person-centred and recognises that responsibility for self-management lies within the individual with diabetes.
DAFNE philosophy recognises that clinicians have responsibility to but not for people with type 1 diabetes.
The DAFNE philosophy holds the view that human nature is basically constructive and that people aim to maximise their quality of life via the choices given their interpersonal and external circumstances.
In accordance with person-centred philosophy DAFNE clinicians communicate empathy and non-judgemental support for all those who participate in the programme regardless of the decisions they make. These core qualities underpin the conditions that provide open and honest dialogue regarding optimising self-management.
DAFNE clinicians have responsibility to facilitate optimal exploration of values, beliefs and barriers each individual has in relation to his/her diabetes and to provide honest and accurate information about risks and eventualities.
DAFNE philosophy recognises that the sharing of ideas between people with diabetes and health care professionals is a two way process that can facilitate improvements in both service delivery and outcomes for people with diabetes.
DAFNE clinicians will act as a resource, facilitating and supporting the process of life-long change in individuals with type 1 diabetes.

DAFNE © T01.002, Version 10 – October 2010 29
What are the aims of the DAFNE philosophy
Autonomy and self management
Confidence and competence
Skills based training
Carbohydrate counting to facilitate insulin dose adjustment
Flexible lifestyle
Experiential learning
Decisions made by the person with diabetes
Responsibility lies with the person with diabetes
Ultimately improved outcomes

DAFNE © T01.002, Version 10 – October 2010 30
Educator behaviours
Use of open questions
Use of reflection to seek clarification and demonstrate empathy
Acknowledging each members contribution
Trying to avoid saying “no”
Allowing opportunities for reflection
Time to practice new skills and gain feedback
Providing space for DAFNE participants to work things out for themselves (problem solving)
Using active learning methods
Avoiding a high percentage of “educator” talk
Providing options rather than absolute answers
Involving all the participants
Non- judgmental attitudes
Honest, accurate and up to date content
Demonstrating Empathy and warmth
Encouraging individuals to set their own goals
Providing support and encouragement
Pace of learning is flexible and fits to the learner
Acknowledging previous experience and expertise
Allowing participants to be responsible for their own learning
Ensuring participants have as much control as possible over the process and decisions made
Non threatening, relaxed and enjoyable
Positive encouragement of group/individuals Responds to the group atmosphere

DAFNE © T01.002, Version 10 – October 2010 31
THE DAFNE APPROACH TO FOOD LEARNING GOALS METHODS MATERIALS/MEDIA
Understand and feel comfortable about the DAFNE approach to food.
Ask - Participants to summarise DAFNE approach to food and compare this to previous advice on food in Type 1 Diabetes.
Ask - Group to list pros/cons of DAFNE and food.
Debate the above issues as a group and aim to deal with any outstanding concerns.
Summarise the principles of DAFNE and food:
Insulin is the treatment for Type 1 Diabetes.
Insulin can be matched to lifestyle (not lifestyle to insulin).
Estimating carbohydrate allows an appropriate insulin dose to be given. This allows dietary freedom.
DAFNE is about blood glucose management so does not deal in any depth with healthy eating.
Reflective sheet “DAFNE and food”
Flipchart and pens Acetate “DAFNE principles”
Reflect upon and practise skills in carbohydrate estimation.
Discuss - Carbohydrate estimation is a key skill in DAFNE that requires practise. Like DAFNE participants, DEP trainers will be undergoing the same process of learning how to count carbohydrate. Ask - Group to reflect on observed DAFNE course and some of the difficulties they have seen in learning to estimate carbohydrate. Ask-What methods did you see used to teach CHO counting skills? Collect answers.
Flipchart and pens

DAFNE © T01.002, Version 10 – October 2010 32
DAFNE Principles
Insulin is the treatment for Type 1 diabetes. Insulin can be matched to lifestyle (not lifestyle to insulin). Estimating carbohydrate allows an appropriate insulin dose to be given. This allows dietary freedom. DAFNE is about blood glucose management so does not deal in any depth with healthy eating.

DAFNE © T01.002, Version 10 – October 2010 33
PRACTICAL USE OF THE GLYCAEMIC INDEX LEARNING GOALS METHODS MATERIALS/MEDIA
Understand the concept of Glycaemic Index and its role in DAFNE
Discuss – DAFNE is based on counting CPs to calculate a suitable insulin dose. Do all types of carbohydrate have the same effect on blood glucose? Evidence from research on the Glycaemic Index shows different carbohydrates have a different effect on blood glucose which is mainly related to the physical structure of the food and/or its accompanying ingredients. Presentation on basics of GI to explain concept Ask group in groups of 2-4 to sort carbohydrate foods into rapid, fast, medium and slow acting and those that have little on blood glucose. Discuss and feedback answers. Ask - What are the implications of the Glycaemic Index for DAFNE? Summarise The Glycaemic Index
Demonstrates the most effective hypo treatments.
Dispels the myth that sweet foods such as chocolate/cake cannot be eaten in Type 1 Diabetes.
Can explain unexpected blood results.
Acetates / Power Point Glycaemic index game Flipchart and pens Refer to Glycaemic Index table in Course Handbook Acetates “Practical use of the GI” “Glycaemic Index”
DAFNE © T01.002, Version 10 – October 2010 34
PRACTICAL USE OF THE GLYCAEMIC INDEX LEARNING GOALS METHODS MATERIALS/MEDIA
The main messages for DAFNE participants are:
Rapid acting carbohydrate is a hypo treatment.
Fast, medium and slow carbohydrates should be counted as CPs.
Carbohydrates with little or no effect usually require no insulin (unless taken in large quantities).
Acetate “Glycaemic Index and DAFNE” Pg 28 of workbook

DAFNE © T01.002, Version 10 – October 2010 35
Glycaemic Index
This theory was first investigated by Dr Jenkins in 1981
0
2
4
6
8
10
12
14
Time
Pasta
Glucose

DAFNE © T01.002, Version 10 – October 2010 36
Methodology
50g of CHO (test food) is given to an individual
Blood sugars are measured: 1st hr - every 15 min 2nd hr - every 30 min 3rd hr (diabetes only) every 30min Results are compared with glucose or white bread

DAFNE © T01.002, Version 10 – October 2010 37
Simple vs complex CHO
NNoo lloonnggeerr ttrruuee
NNoott bbaasseedd oonn cchheemmiiccaall aannaallyyssiiss ooff tthhee ffoooodd bbuutt rraatthheerr tthhaann
eeffffeeccttss ooff tthhee ffoooodd oonn tthhee bbooddyy wwhheenn eeaatteenn
Think LOW, MEDIUM and HIGH GI

DAFNE © T01.002, Version 10 – October 2010 38
High GI very rapid effect
(hypo treatment)

DAFNE © T01.002, Version 10 – October 2010 39
Medium GI CHO that can be matched by
insulin
DAFNE © T01.002, Version 10 – October 2010 40
Low GI little to no effect
(unless eaten in large quantities)

DAFNE © T01.002, Version 10 – October 2010 41

DAFNE © T01.002, Version 10 – October 2010 42

DAFNE © T01.002, Version 10 – October 2010 43
DAFNE © T01.002, Version 10 – October 2010 44

DAFNE © T01.002, Version 10 – October 2010 45
DAFNE © T01.002, Version 10 – October 2010 46

DAFNE © T01.002, Version 10 – October 2010 47

DAFNE © T01.002, Version 10 – October 2010 48
The Glycaemic Index
Demonstrates the most effective hypo treatments Contradicts the myth that sweet foods, e.g. chocolate should be avoided May explain unexpected blood glucose results
DAFNE © T01.002, Version 10 – October 2010 49
The Glycaemic Index and DAFNE
Rapid Acting CHO Hypo treatment
Fast / Med / Slow Count CPs
Acting CHO Match with insulin
CHO with little No insulin
effect

DAFNE © T01.002, Version 10 – October 2010 50
THE DAFNE APPROACH TO FOOD – INTRODUCTION OF LUNCHTIME CP COUNTING
LEARNING GOALS METHODS MATERIALS/MEDIA
Explain - Actively counting CPs is the best way to learn this skill. Participants will count CPs in their own food and drink throughout the 3-day workshop and as homework and will document this. They will be supervised at lunchtimes. This enables participants to:
Assess their current skills in CP estimation and therefore identify training needs.
Appreciate how it feels to have to count all CPs taken.
Understand what it is like to be supervised at mealtimes.
Carbohydrate portion estimation booklet

DAFNE © T01.002, Version 10 – October 2010 51
DAFNE and Food
How would you summarise the DAFNE approach to food?
How does this compare with your previous approach to food for Type 1 diabetes?
Having observed a DAFNE course, how do you feel now about food and DAFNE?
Pros: Cons:
General Comments:

DAFNE © T01.002, Version 10 – October 2010 52
CARBOHYDRATE
PORTION
ESTIMATION

DAFNE © T01.002, Version 10 – October 2010 53
Practising CP estimation
Please note down your CP estimates for each meal, snack and drink (including alcohol) you have throughout the next 3 days. This will enable you to: Assess your current CP estimation skills.
Identify future training needs.
Understand how it feels to have to count CPs each time you
eat/drink. Appreciate how DAFNE participants feel when being supervised
at mealtimes.

DAFNE © T01.002, Version 10 – October 2010 54
Date Time Food / Drink CP value
Comments:

DAFNE © T01.002, Version 10 – October 2010 55
Date Time Food / Drink CP value
Comments

DAFNE © T01.002, Version 10 – October 2010 56
Date Time Food / Drink CP value
Comments
DAFNE © T01.002, Version 10 – October 2010 57
Date Time Food / Drink CP value
Comments

DAFNE © T01.002, Version 10 – October 2010 58
Date Time Food / Drink CP value
Comments

DAFNE © T01.002, Version 10 – October 2010 59 59
DAFNE Educator Programme (DEP) 3-day Training Workshop

DAFNE © T01.002, Version 10 – October 2010 60
ESTIMATING DIFFICULT CHOs; SNACKS; FOOD LABELS LEARNING GOALS METHODS MATERIALS/MEDIA
Demonstrate an ability to assess “difficult to estimate” carbohydrates.
DISCUSS – PEOPLE’S EXPERIENCES OF COUNTING CPS AT LUNCHTIME.
Flipchart and pens
Consider strategies to help DAFNE participants with CP estimation.
Ask What was difficult?” How did it feel to be supervised? What information did you use for difficult CHO foods? How could you help DAFNE participants with these issues? Practical activities Set up workstations for each activity and divide group into teams of 3-4 people to visit each workstation. Station 1 Provide selection of plated CP foods that are difficult to estimate, eg pasta, chips, cereal, rice, jacket potatoes. Ask team to guess CPs and compare with answers then reflect on how to help DAFNE participants develop their CP counting skills with these foods.
Workstation instructions CP list Plated food Scales
Demonstrate an ability to calculate CPs from labels and consider strategies to help course participants with these. Understand and practice DAFNE advice regarding snacks
Station 2 Provide a selection of pre-packaged foods. Ask teams to estimate CP value of their personal serving size using the nutritional information on the label. Reflect on the difficulties and how these could be overcome. Station 3
Provide a selection of scenarios that involve having a snack and ask the group to use DAFNE approach to these scenarios (they may need to refer to the Course Handbook).
Workstation instructions Food packets Calculator Answer List Workstation instructions Snack scenarios and answers CP list Food models / photos Course Handbook

DAFNE © T01.002, Version 10 – October 2010 61
ESTIMATING DIFFICULT CHOs; SNACKS; FOOD LABELS LEARNING GOALS METHODS MATERIALS/MEDIA
Become familiar with DAFNE resources and consider their use within a DAFNE course.
Feedback – Reconvene to main group to debrief and summarise 1. What difficulties did they encounter with estimating
difficult CPs. How could these be overcome? 2. What are the difficulties when calculating CPs from labels.
How can you help DAFNE participants with these? 3. What are the main points of advice in the DAFNE
approach to snacks? Station 4 Set up a workstation with a selection of plate models, food models and a recipe book. Ask group to work through estimating the CHO in the plate models and food models and using their CHO portion guide, calculate the CP’s in a recipe. What key issues around nutrition does this exercise help DAFNE graduates with, and consider how they could include this in their lesson planning, eg the effect of portion size on CPs, that savoury foods often contain more CHO than sweet foods, the difference between using a dry weight ingredient and a cooked weight ingredient to calculate CHO. Summarise
Carbohydrate estimation skills are the cornerstone of DAFNE. DEP trainees will need to continue to practice CP counting beyond the 2-day workshop to continue to develop their skills.
Flipchart and pens Plate models, food models, recipe book
DAFNE © T01.002, Version 10 – October 2010 62
Lunch – CP counting
Estimate your CPs
o What was difficult? o How did it feel to be supervised? o What information did you use for difficult CHO foods? o How could you help DAFNE participants with these
issues?

DAFNE © T01.002, Version 10 – October 2010 63
WORKSTATION 1
Carbohydrate Portion Estimation
Visually estimate the CP value of the CHO on each plate.
Discuss and compare your answers with your colleagues.
What advice could you give to your DAFNE participants when estimating these foods?

DAFNE © T01.002, Version 10 – October 2010 64
WORKSTATION 2
Carbohydrate Portion Estimation from Labels
For each of these foods, decide how much you would eat in a serving and calculate the CP value.
Discuss and compare your answers with your colleagues.
Discuss any difficulties you think DAFNE participants may have when reading labels. How could you help?

DAFNE © T01.002, Version 10 – October 2010 65
Food Labels Workstation List which ingredients would need to be counted as CPs when looking at food labels, e.g. corn starch, wheat, sucrose, etc…. How many CPs of the following would you eat?:
Food Serving Size CPs
Chicken noodle soup
Custard mix
Chicken and mushroom pie
Pasta ‘N Sauce
Garlic bread
Yoghurt
Milk drink Noodles
Sweet ‘n’ sour sauce
Treacle pudding
What is misleading / confusing about the labels?
Where could mistakes easily slip in?
Formatted: DAFNE Header 1
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm

DAFNE © T01.002, Version 10 – October 2010 66
Food Labels Workstation Answers List which ingredients would need to be counted as CPs when looking at food labels, e.g. corn starch, wheat, sucrose, etc…. How many CPs of the following would you eat?
Food Serving Size CPs
Chicken noodle soup
3 per can
Custard mix 5½-6 per packet
Chicken and mushroom pie
14 per pie
Pasta ‘N Sauce 8½ per packet (+ 1 for milk)
Garlic bread 3 (for ½ baguette)
Yoghurt 2½
Milk drink 5
Noodles 6 *whole packet
Sweet ‘n’ sour sauce
6 ½ per can
Treacle pudding 15 per can
What is misleading / confusing about the labels?
Where could mistakes easily slip in?
Formatted: DAFNE Header 1
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
Formatted: DAFNE Header 1, Tabstops: Not at 7.32 cm + 14.65 cm
DAFNE © T01.002, Version 10 – October 2010 67
WORKSTATION 3
Snacks and DAFNE
Here are some scenarios that involve eating a ‘snack’
Use DAFNE snack guidelines to suggest a way of managing these scenarios.
Discuss your ideas with your colleagues.
How do DAFNE participants feel about the approach to snacks? What are the main issues?

DAFNE © T01.002, Version 10 – October 2010 68
Snacks and DAFNE Exercise Workstation 1. Your QA:CP ratios are: Breakfast 2:1 Midday 1:1 Evening 1:1
You are in a meeting at work. There is a coffee break at 11am and you fancy a custard cream biscuit. Lunch is scheduled for 12.30pm. How much insulin will you take and when? 2. Your QA:CP ratios are: Breakfast 1½:1 Midday 1:1 Evening 1:1 It is 12.15pm and you eat a Snickers bar on the way to meet a friend for lunch. Your BG before lunch at 1pm is 11mmol/l. You have ½ a thin 9” pizza, salad and a glass of apple juice. How much insulin will you take and when? 3. Your QA:CP ratios are: Breakfast 3:1 Midday 2:1 Evening 2:1 Background insulin 14u am, 14u pm You have a very busy day at work and end up working late, but managed to eat something at 6pm. On your way home at 11pm you decide to call at a burger bar. Your BG is 14.5mmol/l. You order a standard burger in a bun, regular fries and a milkshake. How much insulin will you take and when?
DAFNE © T01.002, Version 10 – October 2010 69
4. Your QA:CP ratios are: Breakfast 2:1 Midday 1½:1 Evening 1:1 Your lunch break is 12.30-1pm. Your friend has a later lunch break (1-1.30pm) and is going to bring you your favourite jam doughnut from the bakers in the High Street. You have a Pot Noodle and diet cola for your lunch. How much insulin will you take and when? 5. Your QA:CP ratios are: Breakfast 2:1 Midday 1½:1 Evening 1½:1 Background insulin 10u am, 10u pm You get up at 8am and your BG is 7.2mmol/l. You decide to skip breakfast, but feel peckish at 10.30am so you eat a Cornish pasty. How much insulin will you take and when?

DAFNE © T01.002, Version 10 – October 2010 70
Snacks and DAFNE Exercise Workstation 1. Your QA:CP ratios are: Breakfast 2:1 Midday 1:1 Evening 1:1
You are in a meeting at work. There is a coffee break at 11am and you fancy a custard cream biscuit. Lunch is scheduled for 12.30pm. How much insulin will you take and when? 1 CP – no action required. Record in diary and correct at lunchtime if required. 2. Your QA:CP ratios are: Breakfast 1½:1 Midday 1:1 Evening 1:1 It is 12.15pm and you eat a Snickers bar on the way to meet a friend for lunch. Your BG before lunch at 1pm is 11mmol/l. You have ½ a thin 9” pizza, salad and a glass of apple juice. How much insulin will you take and when? CPs = Snicker 3½, apple juice 2, half 9” pizza 4½ = total 10 Inject for total of 10 CPs at 1.00 pm, but don’t correct the 11 mmol/l 3. Your QA:CP ratios are: Breakfast 3:1 Midday 2:1 Evening 2:1 Background insulin 14u am, 14u pm You have a very busy day at work and end up working late, but managed to eat something at 6pm. On your way home at 11pm you decide to call at a burger bar. Your BG is 14.5mmol/l. You order a standard burger in a bun, regular fries and a milkshake. How much insulin will you take and when? CPs = Burger and bun 3, regular fries 3, regular shake 6½ = total 12½ In theory using a 2:1 ratio = 25 units and blood glucose level of 14.5 = +2-3 correction in theory = 27/28 units of insulin ? suggest use 1:1 ratio and be cautious about correction initially

DAFNE © T01.002, Version 10 – October 2010 71
4. Your QA:CP ratios are: Breakfast 2:1 Midday 1½:1 Evening 1:1 Your lunch break is 12.30-1pm. Your friend has a later lunch break (1-1.30pm) and is going to bring you your favourite jam doughnut from the bakers in the High Street. You have a Pot Noodle and diet cola for your lunch. How much insulin will you take and when? Pot noodle = 5½ CPs Doughnut = 3½ CPs Option 1 – 2 separate injections using a 1½ ratio Option 2 – have injection after lunch/before snack Option 3 – or before snack 5. Your QA:CP ratios are: Breakfast 2:1 Midday 1½:1 Evening 1½:1 Background insulin 10u am, 10u pm You get up at 8am and your BG is 7.2mmol/l. You decide to skip breakfast, but feel peckish at 10.30am so you eat a Cornish pasty. How much insulin will you take and when? Cornish pastie = 6½ CPs ? retest blood glucose, ? may need correction Inject with pastie using 2:1 or 1½ ratio

DAFNE © T01.002, Version 10 – October 2010 72
WORKSTATION 4
Familiarising yourself with DAFNE resources Estimate the CPs in the plate models and food models and using the CHO portion guide, calculate the CP’s in a chosen recipe.
What key issues around nutrition does this exercise help DAFNE graduates with?
Consider how you would include this in your lesson planning.

DAFNE © T01.002, Version 10 – October 2010 73
STARTING AND ADJUSTING THE DAFNE INSULIN REGIME LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should ….. Understand how and when to transfer DAFNE participants from their existing insulin regime to a DAFNE regime
Ask participants to refer to their case study from observation week and discuss in pairs / small groups:
What was the pre-DAFNE regime?
When did the participant change regime?
What were their starting doses on DAFNE regime? Collect (selection of) answers – note on flip chart. Discuss pro’s/con’s; any ‘right’ or ‘wrong’ way? Discuss the origins of DAFNE and the ‘Berger’ model. NB evidence in terms of background insulin is for bd isophane, so use of analogues (Lantus/Levemir) is according to local preferences and long-term evidence will be collected on the DAFNE database.
Case studies Flip chart and pens DEP handout ‘Commencing the DAFNE insulin regime’
Understand how insulin is used in DAFNE
In small groups discuss the purpose of QA and BI in DAFNE.
Flipchart and pens
Consider any differences between how insulin is used in DAFNE and traditional care.
Reflect and discuss the differences between how QA and BI is used in the DAFNE regimen and traditional care. Discuss pros and cons of DAFNE insulin regime compared to other/previous regimen.
Reflect on the DAFNE insulin regime and algorithms
Discuss any challenges you think this may represent for you as a DAFNE educator, for patients and for the wider diabetes MDT. Ask group for feedback, collect responses on flipchart. Feedback key/common discussion points and list on flipchart.
Flipchart and pens

DAFNE © T01.002, Version 10 – October 2010 74
STARTING AND ADJUSTING THE DAFNE INSULIN REGIME LEARNING GOALS METHODS MATERIALS/MEDIA
Each group to be provided with insulin action posters (1 each group, concentrating on basal/bolus illustrations only). Discuss how would they explain it to their course participants. Trainer note: It is important that trainee Educators are able to explain that bd isophane and meal-time soluble is the evidence base for the ‘Düsseldorf’ regime, but should also be able to discuss the relative pros and cons of both QA and long-acting analogues.
DAFNE Insulin Action Posters
Large group feedback on each poster. Discuss how these could be used within course week. (NB useful to relate to insulin production in non-diabetic).
Understand the format and process of individual insulin dose adjustment sessions during a DAFNE week
Centre teams / small groups to discuss how the individual (patient) insulin dose adjustment sessions were delivered on their course(s) and how the patients in their case studies progressed through the week Feedback and list key points, eg:
Time of day / where on timetable
Group discussion
Acetate diary pages
Each person feeding back their results in turn
Use of Step-Wise approach by Educators
Who lead the session(s)
What changes were actually made to doses during the week etc
Course timetables Observation sheets Case studies

DAFNE © T01.002, Version 10 – October 2010 75
STARTING AND ADJUSTING THE DAFNE INSULIN REGIME LEARNING GOALS METHODS MATERIALS/MEDIA
Demonstrate ability to problem-solve ‘real life’ examples
Discuss what did / didn’t work well. Provide advice from the point of view of an experienced Educator, including common ‘problems’ Provide groups with ‘unfolding’ case examples (3) – there are 8 pages to each example, looking at each stage of the week’s course that their diary would be discussed. Facilitators of the DEP may wish to role play these examples for the participants.
‘Unfolding’ case examples (3)
Reflect on DAFNE insulin dose adjustment theory/principles.
For each example (page), consider the following questions:
What is the problem (if any)?
What are the possible causes (NB CP estimation)?
What questions would you ask (NB CP estimation)?
Is there a clear pattern / have you got enough information to make/suggest any changes?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage?
What was actually done? Was it by pt or Educator?
What would you have done differently? Why? Large group feedback / discussion of key issues. Emphasis on the fact that there is often no absolute ‘right’ or ‘wrong’ and that following DAFNE guidelines should mean no disasters occur. Ask participants how they observed the insulin dose adjustment examples being used on their course.
Observation sheets/timetables
DAFNE © T01.002, Version 10 – October 2010 76
STARTING AND ADJUSTING THE DAFNE INSULIN REGIME LEARNING GOALS METHODS MATERIALS/MEDIA
Understand the structured approach to insulin dose adjustment within the DAFNE programme
Discuss the learning goals and step-wise approach relating to insulin dose adjustment from curriculum and their importance in the DAFNE programme as a whole
DEP handout ‘Using the DAFNE Dose Adjustment examples’
Explain the format of the Dose Adjustment examples, ie:
Heading relates to curriculum section
(a) is the ‘problem’
(b) is the suggested solution Show example page of curriculum, emphasising discussion points provided for each example. Demonstrate the systematic (step-wise) approach to using an example, by using ‘problem’ (a), followed by ‘solution’ (b).
Explain that these are provided in Essential Curriculum Resources file and must be reproduced on acetate in preparation for course.
Dose adjustment example acetates (Insulin Dose Reduction 12.3 Example 1(a) and 1(b)) Example curriculum page 85 (12.3 ‘Insulin Dose Reduction Example 1)
DAFNE © T01.002, Version 10 – October 2010 77
DAFNE Educator Programme (DEP) Commencing the DAFNE Insulin Regime
The ‘Berger Model’ is based on twice daily isophane (NPH): at bedtime and in the morning, plus soluble insulin matched to carbohydrate portions (CPs). The majority of DAFNE course participants will still be using bd isophane, with either soluble or rapid-acting analogue to cover CPs, however a significant number of people (or DAFNE Centres) use Lantus insulin, therefore the following guidelines should help you to advise your course participants about their insulin prior to commencing the course. Bear in mind that many people seem to be ‘over-insulinised’ and do require quite dramatic reductions in their overall insulin doses when doing DAFNE! Changing from a bd pre-mixed insulin regime: Option 1 (standard):
‘Berger regime’: 12u isophane at bedtime and 12u isophane in the morning. Soluble or rapid-acting analogue 1u per 1 CP (1:1 ratio) Continue usual pre-mixed insulin up to and including Sunday evening and commence ‘DAFNE regime’ on Monday morning. (Educator to estimate breakfast CPs and advise QA dose for Monday morning).
Option 2 (‘resistant’ or ‘sensitive’):
If insulin resistant (e.g. >1u/kg total daily dose) and high HbA1c: Commence ‘Berger regime’, but using 14u-16u isophane twice daily Consider 1½:1 or possibly 2:1 QA:CP ratios If insulin sensitive (e.g. <30u total daily dose): Commence ‘Berger regime’, but using 6u-8u isophane twice daily Consider ½:1 QA:CP ratios
Changing from a ‘conventional’ basal/bolus regime: Option 1 (isophane or Levemir): ‘Berger regime’: 12u at bedtime and 12u in the morning, as above. Starting from Sunday bed-time, with a suggested QA dose for Monday morning (approx 1u QA ; 1 CP) Adapt starting doses according to insulin sensitivity. Option 2 (Lantus):
Consider leaving dose of Lantus unchanged, or approx 24u/24hrs (adapt according to sensitivity). Main benefits from Lantus (ie reduced fasting BG) may be achieved from taking it at bedtime, rather than in the morning. If planning to convert from Lantus to isophane or Levemir, consider the ‘washout’ period for Lantus and plan to change 2-3 days prior to the course.
Considerations Views and reasons for doing DAFNE
Views about BG monitoring and extra insulin injections
How do they feel about taking insulin at bedtime?
Are there any issues around nocturnal hypos?
What is their hypo awareness like?
What is their current HbA1c?

DAFNE © T01.002, Version 10 – October 2010 78
Long-acting insulin analogues and DAFNE These are suggested guidelines for people who come to a DAFNE course using long acting insulin analogues as their background insulin.
Once per day long acting insulin analogues: Commonly Glargine has been used more often as a once per day basal insulin than
Detemir.
The dose of once per day long acting insulin analogues should be in keeping with the current DAFNE guidelines, and most patients are recommended to reduce their dose to between 24 and 28 units at bedtime.
The time of administration may have been determined by the pattern of previous hypoglycaemia or for concordance reasons. These reasons need to be explored and addressed on an individual basis.
The time of administration will impact upon the ratios of rapid-acting insulin. Bedtime administration may result in better basal insulin cover through the morning, but poorer basal cover during the following afternoon and evening-this may mean that a higher evening meal ratio Is required.
Ratios for rapid-acting insulin: The time action profile for once daily long acting insulin analogues differs from twice
daily NPH insulin, and may impact upon the ratios of rapid-acting insulin.
It is recommended to start with the usual DAFNE ratios, incorporating the impact of the dawn phenomenon, with a higher ratio at breakfast time than at meals later in the day.
People using once daily long acting insulin analogues at bedtime may require a lower breakfast ratio (less than 2:1) and a higher ratio with their evening meal (greater than 1:1), reflecting the wearing off of Glargine over the final few hours of the 24 hour period.
Dose of long acting insulin analogues:
Patients using long acting insulin analogues are often over-insulinised, and require a review and reduction of their dose.
People on less than 24 units per 24 hrs of long acting insulin analogues may have had problems with hypoglycaemia on higher doses, and should continue on their usual dose at the start of the DAFNE course week.
Changes to long acting insulin analogue dose through the DAFNE week are made using the DAFNE blood glucose targets, taking into account any episodes of hypoglycaemia.
Duration of action of long acting insulin analogues is dose dependent, a reduction in dose may highlight shortcomings in the duration see below.
Frequency of long acting insulin analogues
People using once daily insulin glargine may find that their basal insulin is wearing out over the final few hours of a 24 hour period.
In this case Insulin Glargine can be switched from once daily to twice daily, one dose before bed and the second first thing in the morning. This results in a conventional

DAFNE © T01.002, Version 10 – October 2010 79
DAFNE-type basal bolus insulin regimen, using both rapid-acting and long-acting insulin analogues.
The use of twice daily Insulin Glargine may permit more flexibility in basal dosing to accommodate exercise, although Insulin Detemir maybe a better option in this circumstance.
Switching to a different basal insulin:
On occasions the indication for use of Insulin Glargine may not be readily apparent, and there maybe a more appropriate basal insulin, although this will invariably lead to a switch to twice daily basal insulin dosing..
The best example is the patient who exercises on a frequent basis, and thus has variable insulin requirements. If there are problems with glycaemia relating to exercise, then twice daily NPH insulin or Insulin Detemir should be considered.
There remains uncertainty as to the safety of Insulin Glargine in pregnancy, and our practice is for the pregnancy session to incorporate the pros and cons of using Glargine in the context of pregnancy (this also tends to feature in the Questions and Answers session). Again a switch to twice daily NPH insulin or Insulin Detemir should be considered.

DAFNE © T01.002, Version 10 – October 2010 80
DAFNE Educator Programme (DEP) Using the DAFNE Dose Adjustment Examples
Encourage participants to use a systematic analysis for each example (and for their own BG results!)
What is the (main) problem?
(which BG reading(s) is(are) outside of target range?)
Exclude all possible causes. (rule out CP miscalculation; snacks; more/less exercise than usual; accidentally given wrong dose/insulin; injection site/technique; over-treated hypo; over/under-corrected; etc)
Wait 24-48 hours (except night-time hypos) Is there a clear pattern?
Which insulin(s) may be responsible? (remember onset, peak and duration of both insulins used)
Adjust relevant dose (only 1 at a time)
QA:CP ratio by ½ or
BI by 1-2 units (~10%-20%)
Review

DAFNE © T01.002, Version 10 – October 2010 81
DAFNE Educator Programme (DEP)
Using the DAFNE Dose Adjustment Examples
What Are The Learning Outcomes? (see: T02.002, Version 10. September 2010 Course Curriculum)
“Principles”: Understand that insulin dose adjustment requires a systematic approach (E)
State the stages of the step-wise approach to insulin dose adjustment (E) “Reduction”: State the causes and risk factors for hypoglycaemia (E)
Know when the insulin dose should be reduced (E)
Understand that they should first rule out the causes of hypoglycaemia (E)
Understand that for hypos that occur during the day, they should wait 24 hours to see if the same pattern occurs before adjusting insulin dose (E)
Understand that they should identify the insulin responsible for the hypoglycaemia (E)
Understand that the QA:CP ratio is adjusted by about ½ a ratio, or BI by about 10%, i.e. 1-2 units (E)
Understand that they should only change one dose at a time (E)
Demonstrate use of the step-wise approach in relation to the dose adjustment reduction examples provided (E)
Remember that the dose has to be reduced if BG values are repeatedly too low (E)
Understand why you may need less insulin (E)
State what long-term situations may cause insulin sensitivity to be improved (E)
NB Please note that any reference to the old DUK campaign of “4’s the floor” has been removed from the DAFNE curriculum. Please do not refer to this within the context of DAFNE as it is confusing and does not reflect the DAFNE targets. It is recommended that a discussion around when to “treat” (a hypo-BG less than 3.5mmol/l) and when one might need to “eat”( if BG is below the pre meal target of 4.5mmol/l but above hypo) is more appropriate.

DAFNE © T01.002, Version 10 – October 2010 82
Insulin Dose Adjustment Examples Educator Reference Notes / Discussion Points
Reduction Examples:
Section Example Specific Learning Outcomes? Discussion Points Solution
12.3
Isophane/Levemir Reduction 1
Hypo 2 – 2½ hrs after breakfast BI starting to kick in More likely to be due to QA
Morning QA:CP ratio reduced from 2:1 to 1½:1 Lantus
Reduction 1
Hypo 1½ - 2 hrs after breakfast BI is working More likely to be due to QA
12.4
Isophane/Levemir Reduction 2
Hypo 2hrs after evening meal Very little BI around then QA has to be the cause
Evening QA:CP ratio reduced from 1½:1 to 1:1 Lantus
Reduction 2
Hypo 1 – 1½ hrs after evening meal BI not yet having much effect More likely to be due to QA
12.5
Isophane/Levemir Reduction 3
Understand that in the case of night-time hypos, the relevant BI dose has to be reduced the next evening (E)
Remember to recheck night-time BG following change to BI (E)
Hypo during the night All possible causes considered and ruled out No QA since evening meal Only BI working in the night Don’t wait for a pattern
Reduce BI the next evening Recheck BG at 3am (should be >4.5mmol/l)
Lantus Reduction 3
12.6
Isophane/Levemir Reduction 4 Understand that in the case of night-time
hypo and high morning BG, the morning BG should not be corrected with extra QA (D)
Hypo during the night; High morning BG Same discussion as above (e.g. 3) If BG raised following a hypo, there is a risk of repeated hypos if it is corrected with QA, so do not correct BG at next mealtime following a hypo (night-time or daytime)
Do not correct high morning BG Reduce BI the next evening Recheck BG at 3am (should be >4.5mmol/l)
Lantus Reduction 4

DAFNE © T01.002, Version 10 – October 2010 83
Reduction Examples:
Section Example Specific Learning Outcomes? Discussion Points Solution
12.7
Isophane/Levemir Reduction 5
Hypo 2 – 2½ hrs after lunch 6hrs into action of morning BI Cause could be either QA or BI, but more likely at peak of QA
Lunchtime QA:CP ratio reduced from 2:1 to 1½:1
Lantus Reduction 5
Hypo 1½ - 2 hrs after lunch BI is working Cause could be either QA or BI, but more likely at peak of QA
12.8
Isophane/Levemir Reduction 6
Understand how having a CHO-free meal can aid decision-making in dose adjustments (E)
Hypo 4 – 5 hrs after lunch (beyond action of QA) 9 –10 hrs into action of BI Lunch ratio 1:1 – unlikely to need less than 1:1 Try having CP-free lunch and test BG If BG still drops, BI is causing the problem
Morning BI reduced
Lantus Reduction 6(i)
Hypo 4 –5 hrs after lunch (beyond action of QA) BI working (taken am) All BG at lower end of range Lunch ratio 1:1 – unlikely to need less than 1:1 More likely due to BI than QA
BI reduced
Lantus Reduction 6(ii)
Understand how having a CHO-free meal can aid decision-making in dose adjustments (E)
Hypo 4 –5 hrs after lunch (beyond action of QA) All BG at lower end of range, with marked drop overnight Lunch ratio 1:1 – unlikely to need less than 1:1 Try having CP-free lunch and test BG If BG still drops, BI is causing the problem
BI reduced Check BG at 3am following BI change

DAFNE © T01.002, Version 10 – October 2010 84
“Escalation”: State the causes of high blood glucose levels (E)
Know when the insulin dose should be increased (E)
Understand that they should first rule out the reasons for high BG levels (E)
Know that they should wait 24 hours to see if the same pattern occurs before adjusting an insulin dose (E)
Understand that they should identify the insulin responsible for the high BG(E)
Understand that the QA dose is increased by about ½ a ratio, or the BI dose is increased by about 10%, i.e. 1-2 units (E)
Understand they should only change one dose at a time (E)
Demonstrate use of the step-wise approach in relation to the dose adjustment examples provided (E)

DAFNE © T01.002, Version 10 – October 2010 85
Escalation Examples:
Section Example Specific Learning Outcomes? Discussion Points Solution
13.3
Isophane/Levemir Escalation 1
High BG before lunch QA finished working BI kicking in More likely that BG rose after breakfast, so QA:CP ratio not high enough Morning QA:CP ratio
increased from 1½:1 to 2:1
Lantus Escalation 1
High BG before lunch QA finished working BI working All other BG in target range and stable overnight More likely that BG rose after breakfast, so QA:CP ratio not high enough
13.4
Isophane/Levemir Escalation 2
High BG at bedtime Very little BI around after 16hrs Must need higher QA:CP ratio with evening meal
Evening QA:CP ratio increased from 1:1 to 1½:1 Lantus
Escalation 2
High BG at bedtime and morning BI still working – 16hrs into action Bedtime corrective dose having predictable effect, so BI looks OK Evening QA:CP ratio must be too low
13.5 Isophane/Levemir Escalation 3
High BG before evening meal 6hrs after lunch Morning BI still working QA finished working but BG could have gone up after lunch Increasing morning BI may cause lunch BG to be too low Try increased QA:CP ratio
Lunch QA:CP ratio increased from 1:1 to 1½: 1

DAFNE © T01.002, Version 10 – October 2010 86
Escalation Examples:
Section Example Specific Learning Outcomes? Discussion Points Solution
13.5 Lantus Escalation 3
Understand how having a CHO-free meal can aid decision-making in dose adjustments (E)
High BG before evening meal 6hrs after lunch BI still working – 10hrs into action All other BG in target and stable overnight QA finished working but BG could have gone up after lunch Increasing BI may cause lunch BG to be too low Try a CP-free lunch and test BG; stable BG indicates BI is OK
Lunch QA:CP ratio increased from 1:1 to 1½: 1
13.6
Isophane/Levemir Escalation 4
Understand how having a CHO-free meal can aid decision-making in dose adjustments (E)
High BG before evening meal Similar to previous e.g. (3) – could be either QA or BI Perhaps an increased QA:CP ratio had caused afternoon hypos More leeway with lunch BG Try CP-free lunch and test BG; rising BG indicates BI too low
Morning BI increased
Lantus Escalation 4
High BG before evening meal Similar to previous e.g. (3) – could be either QA or BI BI 20hrs into action Lunch QA:CP ratio already 3:1; Perhaps an increased QA:CP ratio had caused afternoon hypos BG drifting down overnight, so little leeway for increasing it
Split BI to get better 24-hr coverage Consider bd Isophane or Levemir
13.7 Isophane/Levemir Escalation 5
High BG in the morning Evening BI taken at tea-time instead of bed-time (maybe mixing QA and BI doses together for 1 less injection, or trying to space BI doses 12hrs apart) Tail end of BI in the morning not strong enough to counteract Dawn Phenomenon Generally better to have evening BI as late as possible, i.e. at bed-time
Evening BI moved to bed-time Check 3am BG following change to BI (should be >4.5mmol/l)

DAFNE © T01.002, Version 10 – October 2010 87
Escalation Examples:
Section Example Specific Learning Outcomes? Discussion Points Solution
13.7 Lantus Escalation 5
High BG in the morning BI taken in the morning (maybe due to previous hypos at night) BI at tail end of action, not strong enough to counteract Dawn Phenomenon BG in target range the rest of the day and at bed-time
Check 3am BG to rule out night-time hypos (should be >4.5mmol/l)Move BI to bed-time Recheck 3am BG May need less than 3:1 ratio in the morning with better BI coverage
13.8
Isophane/Levemir Escalation 6
Understand that in the case of high BG in the morning, the BG should be checked in the night (E)
Remember not to increase bed-time BI dose without checking 3am BG first (E)
BG in target at bed-time but high in the morning Probably not enough BI to counteract Dawn Phenomenon Essential to rule out night-time hypos before increasing BI BG should always be >4.5mmol/l at 3am (although natural to dip)
BG tested at 3am is safely above hypo range Evening BI increased Recheck 3am BG
Lantus Escalation 6
BG in target at bed-time but high in the morning Corrective QA has reasonable effect BG all at upper end of target range QA:CP ratios all 2:1 More likely to need increased BI but need to rule out night-time hypos BG should always be >4.5mmol/l at 3am (although natural to dip)
BG tested at 3am is safely above hypo range BI increased Recheck 3am BG

DAFNE © T01.002, Version 10 – October 2010 88
“Corrections”:
Know the DAFNE guideline for BG correction (E)
Understand that by self-monitoring their BG it is possible predict the effect of 1
unit of QA insulin (E)
Know that when blood glucose levels are above 11mmol/l, the “2-3mmol/l
guideline” does not apply (E)
Be aware of other possible causes of a raised BG level (E)
Know when it is appropriate to increase the insulin dose (E)
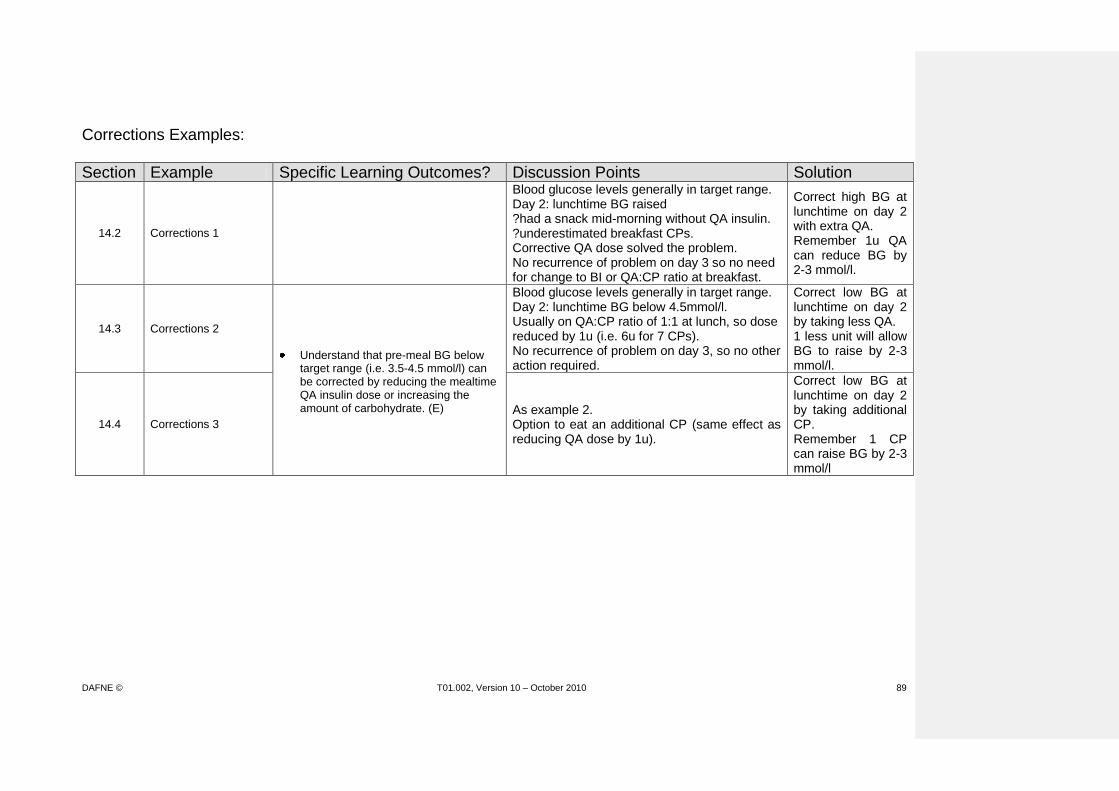
DAFNE © T01.002, Version 10 – October 2010 89
Corrections Examples:
Section Example Specific Learning Outcomes? Discussion Points Solution
14.2 Corrections 1
Blood glucose levels generally in target range. Day 2: lunchtime BG raised ?had a snack mid-morning without QA insulin. ?underestimated breakfast CPs. Corrective QA dose solved the problem. No recurrence of problem on day 3 so no need for change to BI or QA:CP ratio at breakfast.
Correct high BG at lunchtime on day 2 with extra QA. Remember 1u QA can reduce BG by 2-3 mmol/l.
14.3 Corrections 2
Understand that pre-meal BG below target range (i.e. 3.5-4.5 mmol/l) can be corrected by reducing the mealtime QA insulin dose or increasing the amount of carbohydrate. (E)
Blood glucose levels generally in target range. Day 2: lunchtime BG below 4.5mmol/l. Usually on QA:CP ratio of 1:1 at lunch, so dose reduced by 1u (i.e. 6u for 7 CPs). No recurrence of problem on day 3, so no other action required.
Correct low BG at lunchtime on day 2 by taking less QA. 1 less unit will allow BG to raise by 2-3 mmol/l.
14.4 Corrections 3
As example 2. Option to eat an additional CP (same effect as reducing QA dose by 1u).
Correct low BG at lunchtime on day 2 by taking additional CP. Remember 1 CP can raise BG by 2-3 mmol/l

DAFNE © T01.002, Version 10 – October 2010 90
Number = eg in curriculum section
(a) example gives the ‘problem’
(b) example gives the ‘solution’
Insulin Dose Reduction 12.3 Example 1(a)
Date
Time 07:30 10:00 12:00 18:00 22:00 Comments
CP 6 +2 3 5
Blood glucose 6.0 2.7 5.7 7.3 7.7
Quick-acting 12 3 8
Background 12 12
Date Time 07:30 09:30 12:00 18:00 22:00 Comments
CP 3 +2 9 4
Blood glucose 8.3 3.3 5.0 6.0 6.7
Quick-acting 6 9 6
Background 12 12
Date Time Comments
CP
Blood glucose
Quick-acting
Background
DEP Workshop
What is the main problem in this example?
Hypo during the morning Are there any specific Learning Outcomes attached to this example? (list)
No What are the possible discussion points? (see p85 of Curriculum)
2-2 ½ hrs after breakfast BI will be starting to kick in, but BG more likely to have dropped due to action of QA (whether it is soluble or analogue) What is the suggested solution? (p86 of Curriculum)
Reduce morning QA:CP ratio from 2:1 to 1½:1
Refers to curriculum section

DAFNE © T01.002, Version 10 – October 2010 91
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 Comments
CP 3 4 Taking Insulatard 15u bd
Mon BG 3.6 7.3 Starting ratios 1:1
QA 4 4
BI 15
Time Comments
CP
Tue BG
QA
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Monday afternoon)?
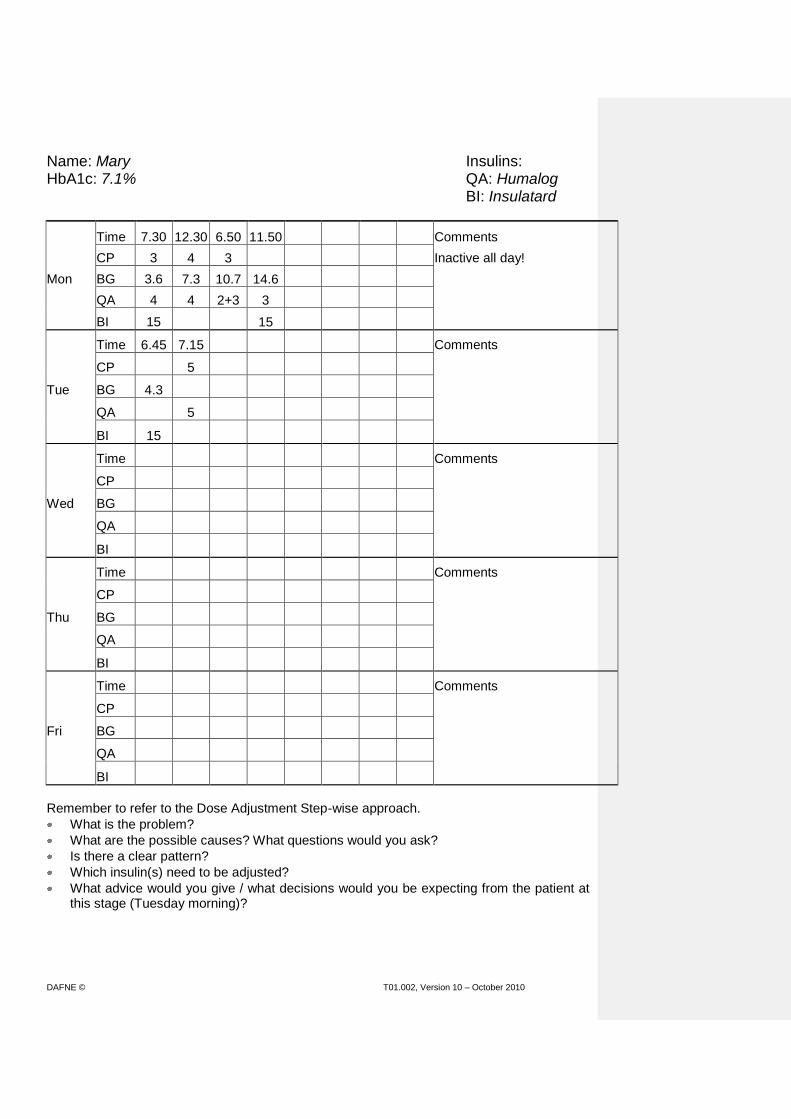
DAFNE © T01.002, Version 10 – October 2010 92
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3 Inactive all day!
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 Comments
CP 5
Tue BG 4.3
QA 5
BI 15
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Tuesday morning)?

DAFNE © T01.002, Version 10 – October 2010 93
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3 Inactive all day!
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 Comments
CP 5 2
Tue BG 4.3 6.0
QA 5 2
BI 15
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Tuesday afternoon)?

DAFNE © T01.002, Version 10 – October 2010 94
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2 Check night-time BGL
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 Comments
CP 2
Wed BG 13.7 13.5
QA 2+3
BI 15
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Wednesday morning)?
What would you have done differently? Why?
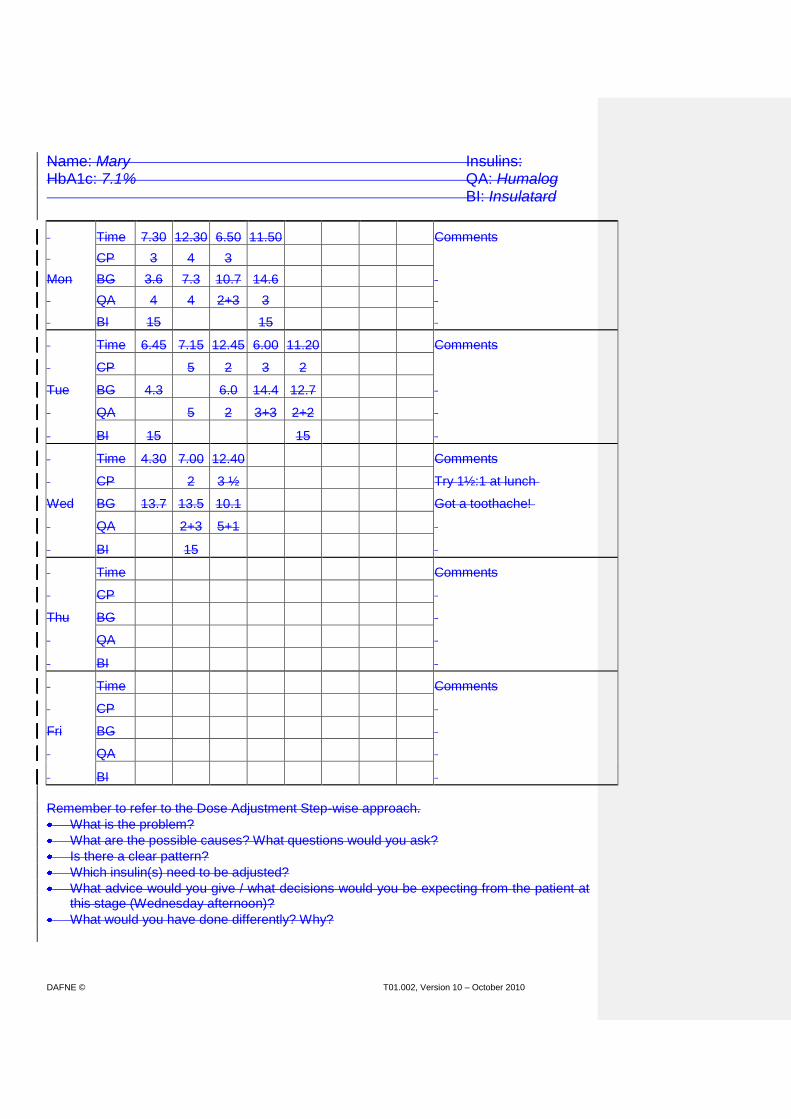
DAFNE © T01.002, Version 10 – October 2010 95
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 Comments
CP 2 3 ½ Try 1½:1 at lunch
Wed BG 13.7 13.5 10.1 Got a toothache!
QA 2+3 5+1
BI 15
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Wednesday afternoon)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 96
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 5.30 7.00 11.30 Comments
CP 2 3½ 2½
Wed BG 13.7 13.5 10.1 9.5 10.3 11.4
QA 2+3 5+1 4+2 2
BI 15 15
Time 4.30 7.15 Comments
CP 1½ 3½ Mary decided to try 1½ :1 at tea
Thu BG 2.5 5.6 and at breakfast
QA 5 She also wants to try 2:1 at lunch
BI 15
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Thursday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 97
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 5.30 7.00 11.30 Comments
CP 2 3½ 2½
Wed BG 13.7 13.5 10.1 9.5 10.3 11.4
QA 2+3 5+1 4+2 2
BI 15 15
Time 4.30 7.15 12.30 4.15 Comments
CP 1½ 3½ 5 1½ Reduce night BI to 13u (due to hypo
Thu BG 2.5 5.6 8.0 2.8 last night)
QA 5 10
BI 15
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Thursday afternoon)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 98
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 5.30 7.00 11.30 Comments
CP 2 3½ 2½
Wed BG 13.7 13.5 10.1 9.5 10.3 11.4
QA 2+3 5+1 4+2 2
BI 15 15
Time 4.30 7.15 12.30 4.15 6.00 10.40 Comments
CP 1½ 3½ 5 1½ 2+3
Thu BG 2.5 5.6 8.0 2.8 2.9 9.7
QA 5 10 4 1
BI 15 13
Time 3.00 7.00 Comments
CP 2+4 Mary thinks she may need to
Fri BG 8.4 3.3 reduce her BI further (?am as well as
QA 6 pm)
BI 15
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Friday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 99
Unfolding Case Example 1 Mary
Mary is a 40 year old occupational therapist, diagnosed 4 years ago. Weight 75.7kg Height 166cm BMI 27.5 HbA1c 7.1% Has lipohypertrophy, but no DKA/no severe hypos Has performed 42 capillary BG tests in 2 weeks prior to DAFNE course, but doesn’t record in a diary Has altered hypo awareness (<3mmol/l) Has been waiting almost 2 years to do the DAFNE course. On PAID questionnaire, the majority of items are ‘Not a Problem’, with a couple of ‘Minor Problems.

DAFNE © T01.002, Version 10 – October 2010 100
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 Comments
CP 3 4 Taking Insulatard 15u bd
Mon BG 3.6 7.3 Starting ratios 1:1
QA 4 4
BI 15
Time Comments
CP
Tue BG
QA
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Obviously started off low this morning – need to watch this – is it a pattern or just ‘1st day phenomenon’? (Actually had 2u QA at bedtime last night as BG 8.9mmol/l!). Can’t draw any conclusions at present. What is she having for tea tonight? How will she work it out? What has she got to help (ie CP list)? Does she/you envisage any difficulties? Explain about 1u QA per CP and to continue on 15u Insulatard bd for now. Emphasise BG targets (especially bed-time) and correct treatment of hypos/corrective QA.

DAFNE © T01.002, Version 10 – October 2010 101
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3 Inactive all day!
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 Comments
CP 5
Tue BG 4.3
QA 5
BI 15
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Give encouragement – has recorded BGs at appropriate times -> helpful information. What were her 3 CPs at evening meal? How did she work them out? How accurate was she? How did she decide on her QA dose? Was this 2u for CPs + 3 corrective? – no, should have written 3+2. Mary feels her BGs were too high yesterday because she was sitting all day, hence needing corrective QA. She is happy that her BG is OK this morning. Discuss BG targets again – 4.3mmol/l is too low at breakfast – did she over-correct at bed-time (again), or is night BI too high? – watch both of these

DAFNE © T01.002, Version 10 – October 2010 102
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3 Inactive all day!
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 Comments
CP 5 2
Tue BG 4.3 6.0
QA 5 2
BI 15
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
BG was within target at lunch. Nothing to be too concerned about at this stage. What is she eating /doing this evening? How will she estimate CPs? Does she need any guidance? Is she confident to use her CP list? Was there anything from today’s hypo session that she needs to take on board? (Vigilance with reduced hypo warnings.) Continue on 1:1 ratios and 15u bd, but be cautious with corrective QA. Perform a 3am test to check night BI.
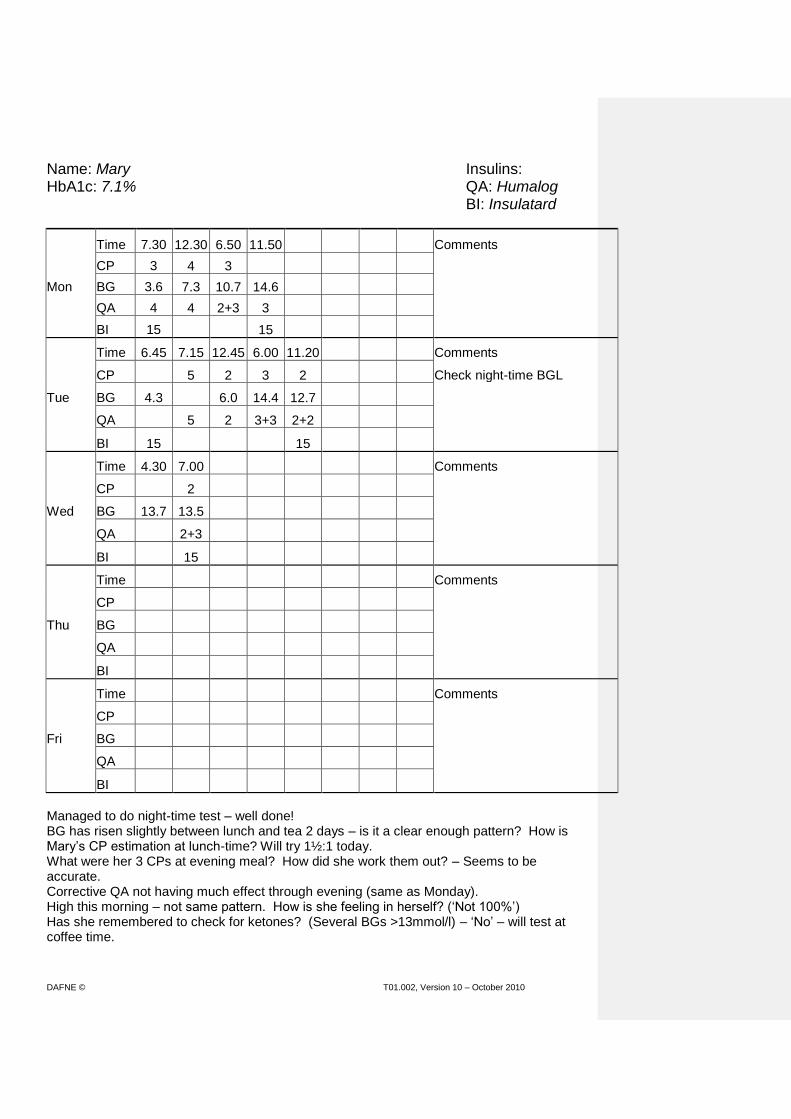
DAFNE © T01.002, Version 10 – October 2010 103
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2 Check night-time BGL
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 Comments
CP 2
Wed BG 13.7 13.5
QA 2+3
BI 15
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Managed to do night-time test – well done! BG has risen slightly between lunch and tea 2 days – is it a clear enough pattern? How is Mary’s CP estimation at lunch-time? Will try 1½:1 today. What were her 3 CPs at evening meal? How did she work them out? – Seems to be accurate. Corrective QA not having much effect through evening (same as Monday). High this morning – not same pattern. How is she feeling in herself? (‘Not 100%’) Has she remembered to check for ketones? (Several BGs >13mmol/l) – ‘No’ – will test at coffee time.

DAFNE © T01.002, Version 10 – October 2010 104
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 Comments
CP 2 3 ½ Try 1½:1 at lunch
Wed BG 13.7 13.5 10.1 Got a toothache!
QA 2+3 5+1
BI 15
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Ketones negative, but has now got a toothache. Discuss using ‘minor illness’ rules, i.e. use corrective QA and continue to check for ketones if BG >13mmol/l. May make it difficult to ascertain patterns for now. How confident is she to estimate her CPs tonight? Is she planning anything different? Continue on 15u bd and 1:1, 1½:1, 1:1.
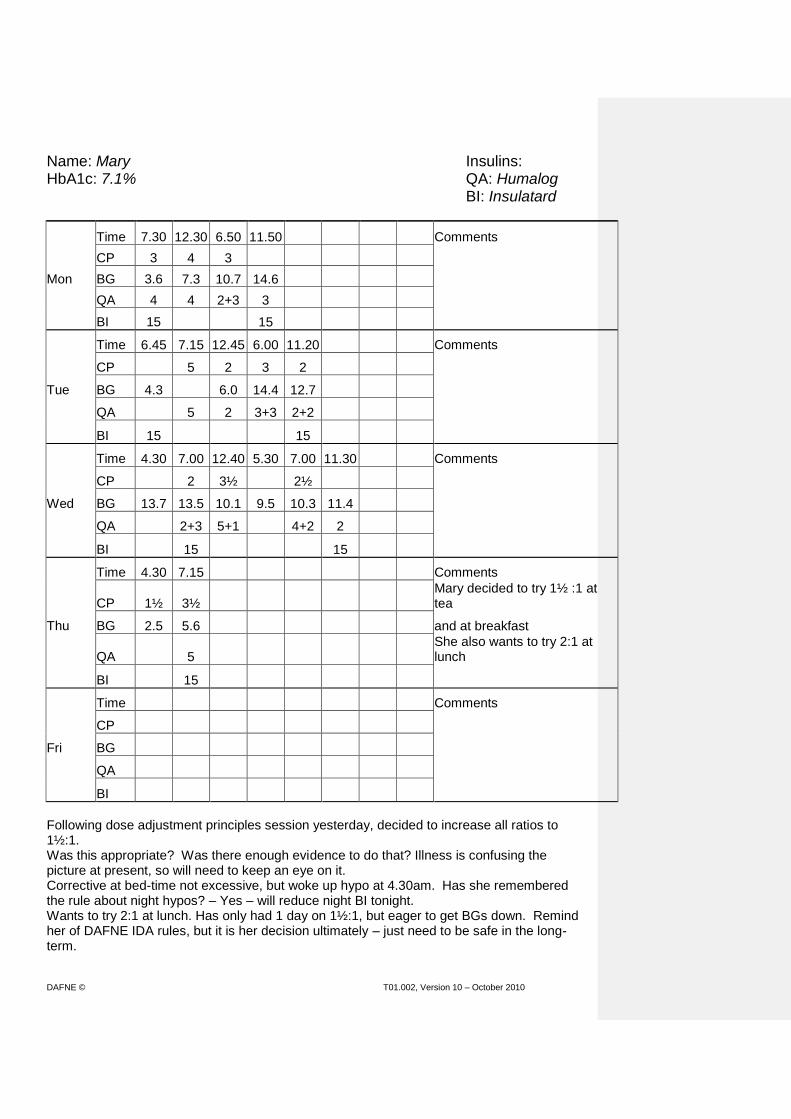
DAFNE © T01.002, Version 10 – October 2010 105
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 5.30 7.00 11.30 Comments
CP 2 3½ 2½
Wed BG 13.7 13.5 10.1 9.5 10.3 11.4
QA 2+3 5+1 4+2 2
BI 15 15
Time 4.30 7.15 Comments
CP 1½ 3½ Mary decided to try 1½ :1 at tea
Thu BG 2.5 5.6 and at breakfast
QA 5 She also wants to try 2:1 at lunch
BI 15
Time Comments
CP
Fri BG
QA
BI
Following dose adjustment principles session yesterday, decided to increase all ratios to 1½:1. Was this appropriate? Was there enough evidence to do that? Illness is confusing the picture at present, so will need to keep an eye on it. Corrective at bed-time not excessive, but woke up hypo at 4.30am. Has she remembered the rule about night hypos? – Yes – will reduce night BI tonight. Wants to try 2:1 at lunch. Has only had 1 day on 1½:1, but eager to get BGs down. Remind her of DAFNE IDA rules, but it is her decision ultimately – just need to be safe in the long-term.

DAFNE © T01.002, Version 10 – October 2010 106
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 5.30 7.00 11.30 Comments
CP 2 3½ 2½
Wed BG 13.7 13.5 10.1 9.5 10.3 11.4
QA 2+3 5+1 4+2 2
BI 15 15
Time 4.30 7.15 12.30 4.15 Comments
CP 1½ 3½ 5 1½ Reduce night BI to 13u (due to hypo
Thu BG 2.5 5.6 8.0 2.8 last night)
QA 5 10
BI 15
Time Comments
CP
Fri BG
QA
BI
Breakfast 1½:1 ratio seemed to work OK – continue. What were her CPs at lunch? How accurate was she? She feels she jumped in with the ratio increase too early and will go back to 1½:1 tomorrow. Confident to estimate CPs tonight and staying on 1½:1 for tea. Reducing BI to 13u tonight.

DAFNE © T01.002, Version 10 – October 2010 107
Name: Mary Insulins: HbA1c: 7.1% QA: Humalog BI: Insulatard
Time 7.30 12.30 6.50 11.50 Comments
CP 3 4 3
Mon BG 3.6 7.3 10.7 14.6
QA 4 4 2+3 3
BI 15 15
Time 6.45 7.15 12.45 6.00 11.20 Comments
CP 5 2 3 2
Tue BG 4.3 6.0 14.4 12.7
QA 5 2 3+3 2+2
BI 15 15
Time 4.30 7.00 12.40 5.30 7.00 11.30 Comments
CP 2 3½ 2½
Wed BG 13.7 13.5 10.1 9.5 10.3 11.4
QA 2+3 5+1 4+2 2
BI 15 15
Time 4.30 7.15 12.30 4.15 6.00 10.40 Comments
CP 1½ 3½ 5 1½ 2+3
Thu BG 2.5 5.6 8.0 2.8 2.9 9.7
QA 5 10 4 1
BI 15 13
Time 3.00 7.00 Comments
CP 2+4 Mary thinks she may need to
Fri BG 8.4 3.3 reduce her BI further (?am as well as pm)
QA 6
BI 15
BG stayed low through yesterday evening - ? due to too much QA at lunch, or is morning BI too high now ‘illness’ has settled down – Mary considering both. Treating hypos appropriately – good! Discuss safety issues re correcting raised BG following hypos (bed-time last night) – discourage this practice. Rechecked night BG – OK at 3am, but woke up hypo at 7am! Could be that relatively high dose of Insulatard having prolonged action/peak. Has lipohypertrophy – re-emphasise injection sites! Mary wants to reduce her BI anyway in anticipation of going back to work.

DAFNE © T01.002, Version 10 – October 2010 108
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 Comments
CP 3½ 8 Taking Glargine 12-14u nocte
Mon BG 12.9 10.4 8.6 Starting ratios 1:1
QA 6 8
BI
Time Comments
CP
Tue BG
QA
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Monday afternoon)?

DAFNE © T01.002, Version 10 – October 2010 109
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 Comments
CP 5
Tue BG 11.2
QA 5
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Tuesday morning)?

DAFNE © T01.002, Version 10 – October 2010 110
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 Comments
CP 5 3
Tue BG 11.2 7.4
QA 5 3
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Tuesday afternoon)?

DAFNE © T01.002, Version 10 – October 2010 111
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 Comments
CP 1½ +2 10
Wed BG 2.0 8.5
QA 10
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Wednesday morning)?
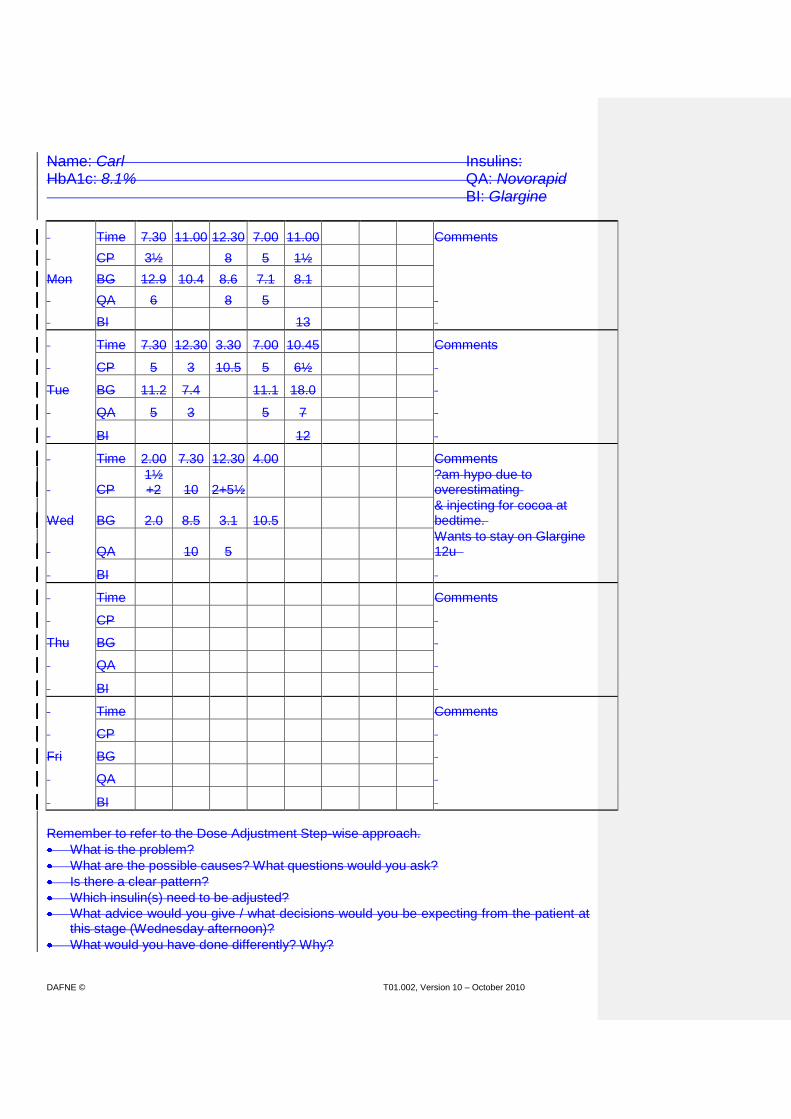
DAFNE © T01.002, Version 10 – October 2010 112
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 Comments
CP 1½ +2 10 2+5½
?am hypo due to overestimating
Wed BG 2.0 8.5 3.1 10.5 & injecting for cocoa at bedtime.
QA 10 5 Wants to stay on Glargine 12u
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Wednesday afternoon)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 113
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 9.15 12.00 Comments
CP 1½ +2 10 2+5½ 2 2
Wed BG 2.0 8.5 3.1 10.5 21.1 6.0
QA 10 5 4+6
BI 12
Time 3.30 7.30 Comments
CP 4½ Carl tried 2:1 at teatime
Thu BG 8.3 10.4 Wants to try 1½:1 at lunch
QA 5+1
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Thursday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 114
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 9.15 12.00 Comments
CP 1½ +2 10 2+5½ 2 2
Wed BG 2.0 8.5 3.1 10.5 21.1 6.0
QA 10 5 4+6
BI 12
Time 3.30 7.30 12.45 3.45 Comments
CP 4½ 5½ Considering 1½:1 for all meals
Thu BG 8.3 10.4 7.5 12.5
QA 5+1 8
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Thursday afternoon)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 115
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 9.15 12.00 Comments
CP 1½ +2 10 2+5½ 2 2
Wed BG 2.0 8.5 3.1 10.5 21.1 6.0
QA 10 5 4+6
BI 12
Time 3.30 7.30 12.45 3.45 6.30 11.00 Comments
CP 4½ 5½ 4 2
Thu BG 8.3 10.4 7.5 12.5 11.0 10.3
QA 5+1 8 6 2+1
BI 12
Time 8.00 Comments
CP 3 Thinking he may need to increase
Fri BG 8.7 Glargine
QA 5
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Friday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 116
Unfolding Case Example 2 Carl
Carl is a 62 year old who works 5am-2pm as a cleaner in a supermarket. He was diagnosed 50 years ago. He has treated angina, hypertension and hypercholesterolaemia. He has retinopathy, treated with laser 19 years ago. He has slight lipohypertrophy, but no DKA and has had 1 severe hypo (with paramedic assistance) in last 5 years. Hypo awareness is generally good (>3mmol/l). Weight 62.8kg Height 160cm BMI 24.5 HbA1c 8.1% (has been stable for at least past 2 yrs) He has performed 56 capillary BG tests in past 2 weeks prior to DAFNE course – does not record in a diary. On PAID questionnaire, Feeling discouraged with your diabetes treatment plan and worrying about low blood sugar reactions are ‘Somewhat serious problem’. Uncomfortable social situations related to your diabetes care, Worrying about the future and the possibility of serious complications, Feelings of guilt or anxiety when getting off track with diabetes management, Coping with complications of diabetes and Feeling ‘burned out’ by the constant effort needed to manage diabetes are ‘Moderate Problem’
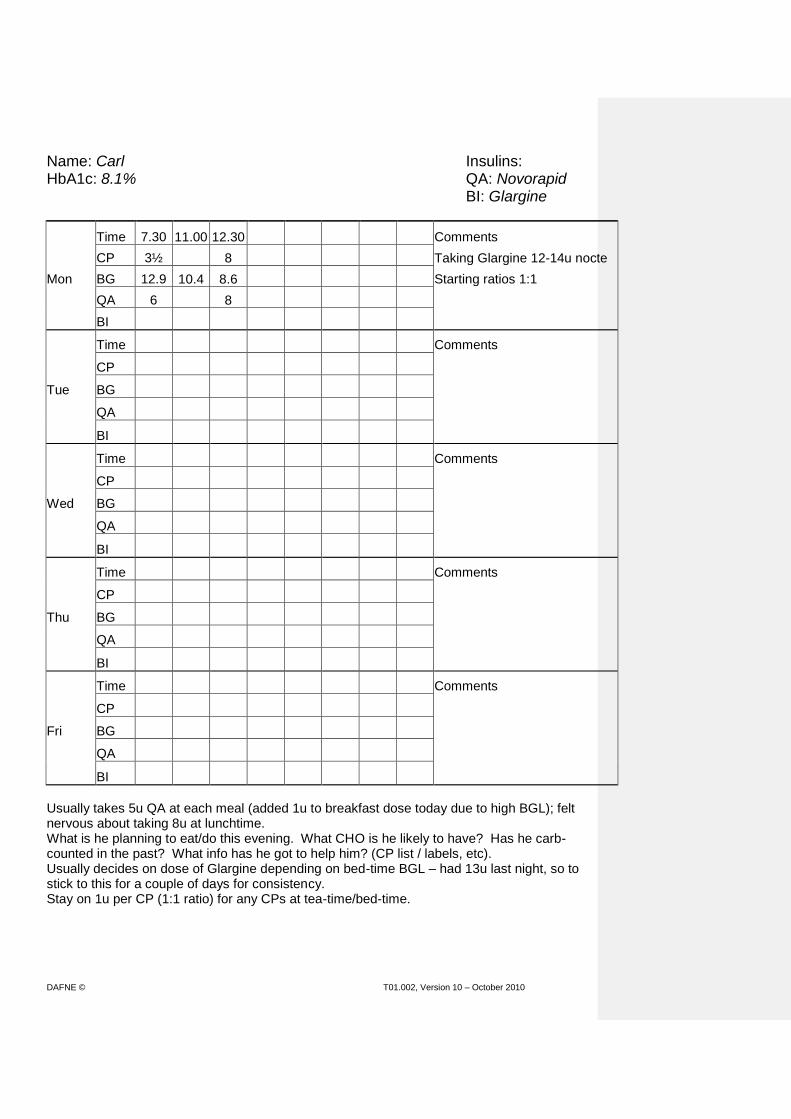
DAFNE © T01.002, Version 10 – October 2010 117
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 Comments
CP 3½ 8 Taking Glargine 12-14u nocte
Mon BG 12.9 10.4 8.6 Starting ratios 1:1
QA 6 8
BI
Time Comments
CP
Tue BG
QA
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Usually takes 5u QA at each meal (added 1u to breakfast dose today due to high BGL); felt nervous about taking 8u at lunchtime. What is he planning to eat/do this evening. What CHO is he likely to have? Has he carb-counted in the past? What info has he got to help him? (CP list / labels, etc). Usually decides on dose of Glargine depending on bed-time BGL – had 13u last night, so to stick to this for a couple of days for consistency. Stay on 1u per CP (1:1 ratio) for any CPs at tea-time/bed-time.
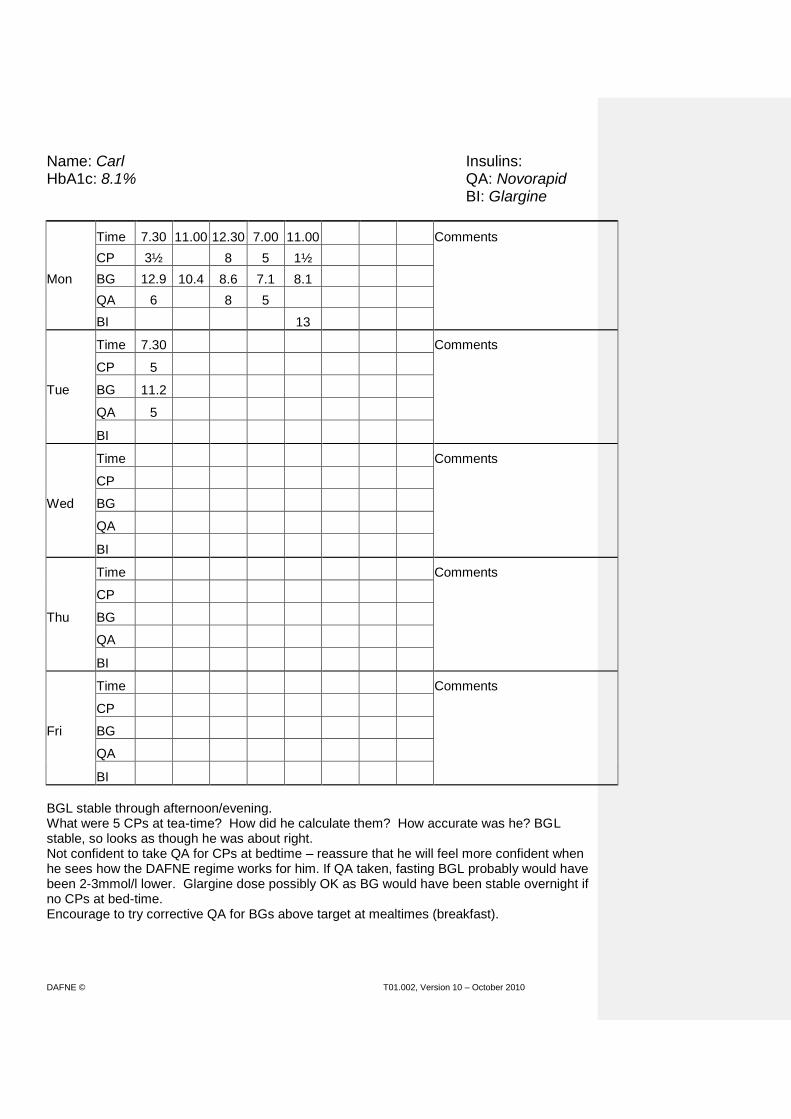
DAFNE © T01.002, Version 10 – October 2010 118
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 Comments
CP 5
Tue BG 11.2
QA 5
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
BGL stable through afternoon/evening. What were 5 CPs at tea-time? How did he calculate them? How accurate was he? BGL stable, so looks as though he was about right. Not confident to take QA for CPs at bedtime – reassure that he will feel more confident when he sees how the DAFNE regime works for him. If QA taken, fasting BGL probably would have been 2-3mmol/l lower. Glargine dose possibly OK as BG would have been stable overnight if no CPs at bed-time. Encourage to try corrective QA for BGs above target at mealtimes (breakfast).

DAFNE © T01.002, Version 10 – October 2010 119
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 Comments
CP 5 3
Tue BG 11.2 7.4
QA 5 3
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
BG did come down significantly during the morning. What were 5 CPs at breakfast? How did he calculate them? How accurate was he? – Could be over-estimation of breakfast CPs, or possibly Glargine is too high. Need another day to see pattern as different to Monday. What is he doing this evening? Does he need any advice / help with working out CHO? Following hypo session this afternoon, Carl knows he needs to check his BGL before driving home.
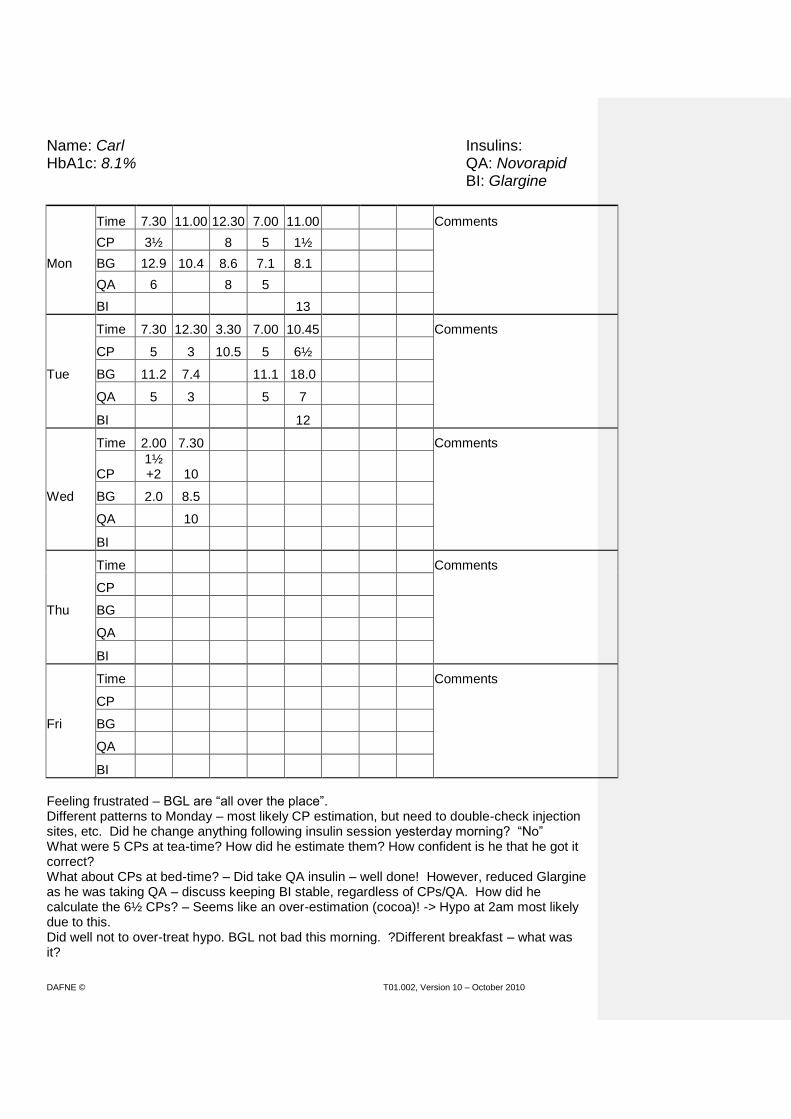
DAFNE © T01.002, Version 10 – October 2010 120
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 Comments
CP 1½ +2 10
Wed BG 2.0 8.5
QA 10
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Feeling frustrated – BGL are “all over the place”. Different patterns to Monday – most likely CP estimation, but need to double-check injection sites, etc. Did he change anything following insulin session yesterday morning? “No” What were 5 CPs at tea-time? How did he estimate them? How confident is he that he got it correct? What about CPs at bed-time? – Did take QA insulin – well done! However, reduced Glargine as he was taking QA – discuss keeping BI stable, regardless of CPs/QA. How did he calculate the 6½ CPs? – Seems like an over-estimation (cocoa)! -> Hypo at 2am most likely due to this. Did well not to over-treat hypo. BGL not bad this morning. ?Different breakfast – what was it?

DAFNE © T01.002, Version 10 – October 2010 121
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 Comments
CP 1½ +2 10 2+5½
?am hypo due to overestimating
Wed BG 2.0 8.5 3.1 10.5 & injecting for cocoa at bedtime.
QA 10 5 Wants to stay on Glargine 12u
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
BG drop between breakfast and lunch - re-visit breakfast CPs – it was actually the same as other days and he had got confused using scales to check weights (following Tuesday afternoon nutrition session). Remind that weight of food is not the same as CHO value. Found this morning’s dose adjustment theory session useful – wants to try a different QA:CP ratio at tea-time. Has he got enough evidence for this? (Mon and Tue different) Better to wait another day (according to DAFNE guidelines). Wants to stay on 12u Glargine after night-time hypo.

DAFNE © T01.002, Version 10 – October 2010 122
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 9.15 12.00 Comments
CP 1½ +2 10 2+5½ 2 2
Wed BG 2.0 8.5 3.1 10.5 21.1 6.0
QA 10 5 4+6
BI 12
Time 3.30 7.30 Comments
CP 4½ Carl tried 2:1 at teatime
Thu BG 8.3 10.4 Wants to try 1½:1 at lunch
QA 5+1
BI
Time Comments
CP
Fri BG
QA
BI
BGL at tea-time very high – different again to other days, but ?due to 2 hypos in 1 day? Decided to try 2:1 ratio at tea-time – not disastrous due to high BGL, but not clear that this is indicated. What were the 2 CPs? Did he eat less because he wasn’t hungry, or because BG was high? If necessary, remind that with DAFNE it’s OK to eat to your appetite and inject the appropriate amount of QA – no need to ‘fast’ to get BG down! Also remind of safe corrective strategy and that 1u reducing BG by 2-3mmol/l is less predictable >11mmol/l; limit to 4u until sure of sensitivity. Remembered target BG for bed-time and didn’t inject QA for CPs as they were to correct below-target BG. Also remembered to re-check night-time BG.

DAFNE © T01.002, Version 10 – October 2010 123
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 9.15 12.00 Comments
CP 1½ +2 10 2+5½ 2 2
Wed BG 2.0 8.5 3.1 10.5 21.1 6.0
QA 10 5 4+6
BI 12
Time 3.30 7.30 12.45 3.45 Comments
CP 4½ 5½ Considering 1½:1 for all meals
Thu BG 8.3 10.4 7.5 12.5
QA 5+1 8
BI
Time Comments
CP
Fri BG
QA
BI
A bit happier with BGL today. Feels 2:1 may have been too high for tea-time ratio yesterday, so will try 1½:1 tonight. Increased lunch ratio today to 1½:1 as BG has risen between lunch and tea on 2 days – seems like an appropriate decision. Actually feels that 1½:1 would be better for all meals. Investigate his reasoning behind this. Point out that 1:1 at breakfast seems to be working fine. Confident to calculate CPs tonight and will be more cautious with corrective QA if needed. Staying on 12u Glargine tonight.
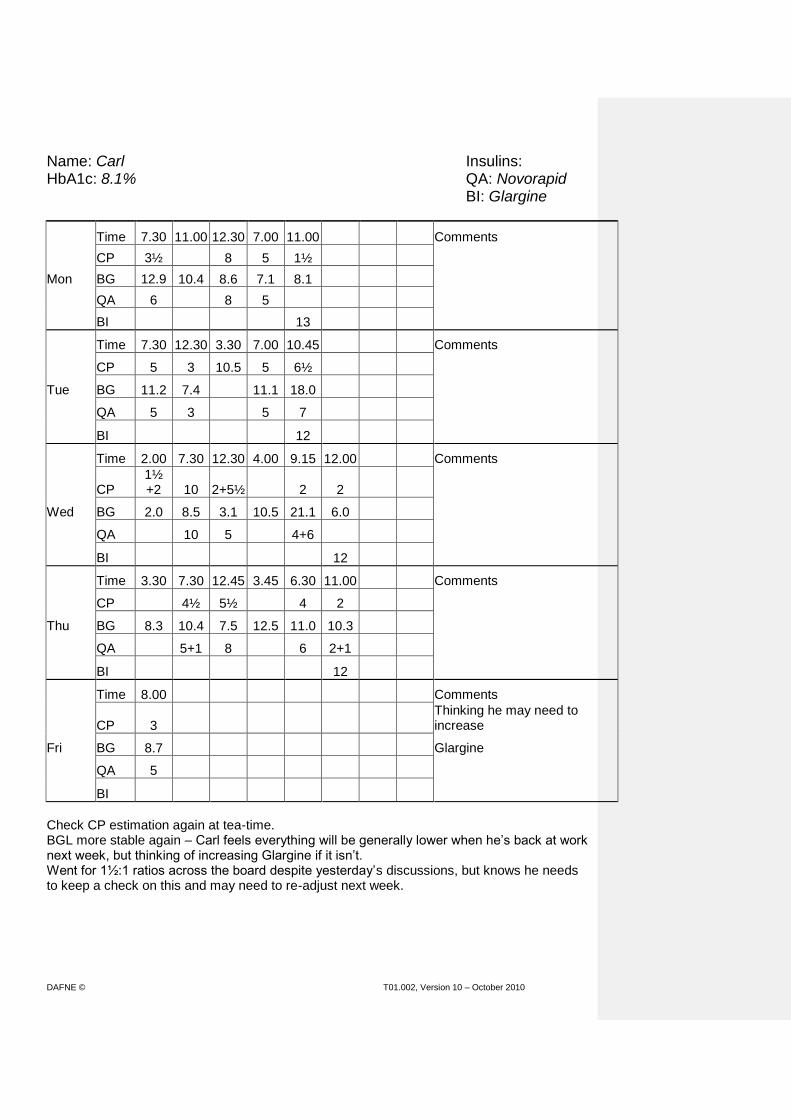
DAFNE © T01.002, Version 10 – October 2010 124
Name: Carl Insulins: HbA1c: 8.1% QA: Novorapid BI: Glargine
Time 7.30 11.00 12.30 7.00 11.00 Comments
CP 3½ 8 5 1½
Mon BG 12.9 10.4 8.6 7.1 8.1
QA 6 8 5
BI 13
Time 7.30 12.30 3.30 7.00 10.45 Comments
CP 5 3 10.5 5 6½
Tue BG 11.2 7.4 11.1 18.0
QA 5 3 5 7
BI 12
Time 2.00 7.30 12.30 4.00 9.15 12.00 Comments
CP 1½ +2 10 2+5½ 2 2
Wed BG 2.0 8.5 3.1 10.5 21.1 6.0
QA 10 5 4+6
BI 12
Time 3.30 7.30 12.45 3.45 6.30 11.00 Comments
CP 4½ 5½ 4 2
Thu BG 8.3 10.4 7.5 12.5 11.0 10.3
QA 5+1 8 6 2+1
BI 12
Time 8.00 Comments
CP 3 Thinking he may need to increase
Fri BG 8.7 Glargine
QA 5
BI
Check CP estimation again at tea-time. BGL more stable again – Carl feels everything will be generally lower when he’s back at work next week, but thinking of increasing Glargine if it isn’t. Went for 1½:1 ratios across the board despite yesterday’s discussions, but knows he needs to keep a check on this and may need to re-adjust next week.

DAFNE © T01.002, Version 10 – October 2010 125
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 Comments
CP 3½ 0 Taking Detemir 10-12u bd
Mon BG 9.7 11.5 9.9 9.9 and Metformin 500mg bd
QA 10 0 Starting ratios 1:1
BI 10 Feeling unwell pm – home early
Time Comments
CP
Tue BG
QA
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Monday afternoon)?

DAFNE © T01.002, Version 10 – October 2010 126
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 Comments
CP 3½ Has always taken 9u at breakfast
Tue BG 10.0 (always has the same thing)
QA 9
BI 12
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Tuesday morning)?
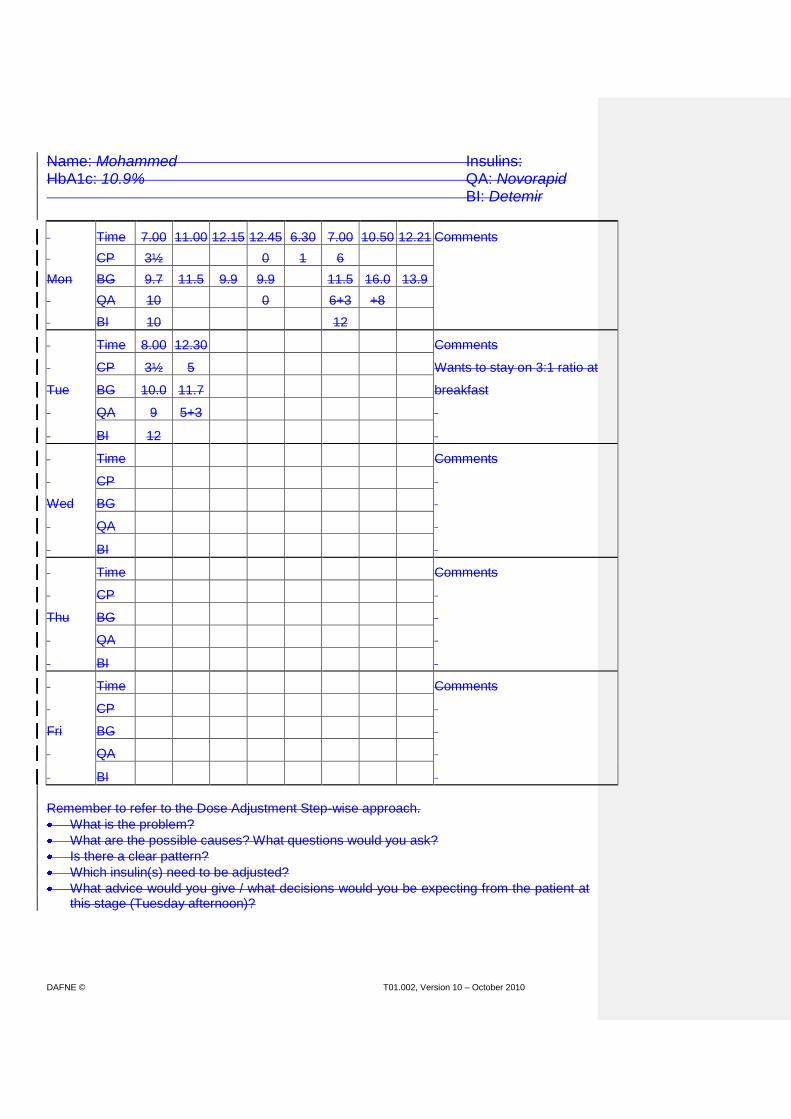
DAFNE © T01.002, Version 10 – October 2010 127
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 Comments
CP 3½ 5 Wants to stay on 3:1 ratio at
Tue BG 10.0 11.7 breakfast
QA 9 5+3
BI 12
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Tuesday afternoon)?
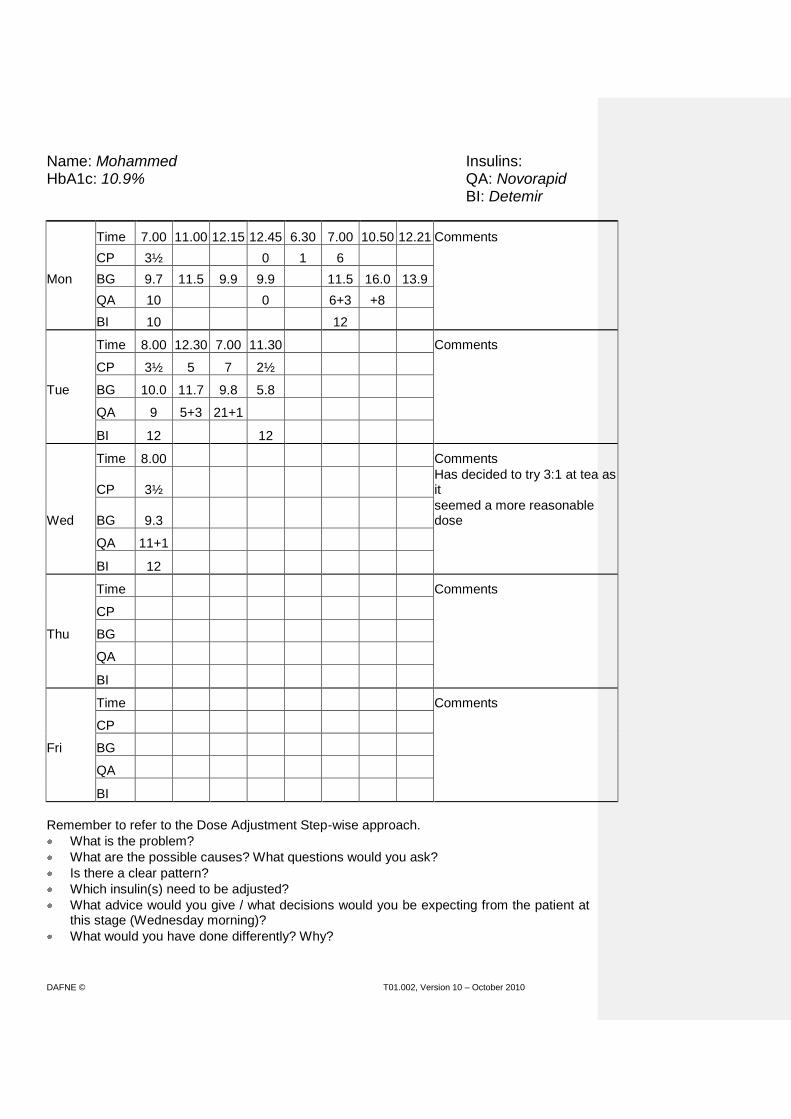
DAFNE © T01.002, Version 10 – October 2010 128
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 Comments
CP 3½ Has decided to try 3:1 at tea as it
Wed BG 9.3 seemed a more reasonable dose
QA 11+1
BI 12
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Wednesday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 129
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 Comments
CP 3½ 3 Has decided on 3:1, 1½:1, 3:1
Wed BG 9.3 9.3 ratios
QA 11+1 5+2
BI 12
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Wednesday afternoon)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 130
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 7.00 1.20 Comments
CP 3½ 3 4
Wed BG 9.3 9.3 8.9 9.4
QA 11+1 5+2 12+1
BI 12 12
Time 8.00 Comments
CP 3½
Thu BG 8.7
QA 12
BI 12
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Thursday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 131
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 7.00 1.20 Comments
CP 3½ 3 4
Wed BG 9.3 9.3 8.9 9.4
QA 11+1 5+2 12+1
BI 12 12
Time 8.00 12.45 3.45 Comments
CP 3½ 4 He is thinking about 3:1 for all
Thu BG 8.7 5.7 11.9 meals
QA 12 6
BI 12
Time Comments
CP
Fri BG
QA
BI
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Thursday afternoon)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 132
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 7.00 1.20 Comments
CP 3½ 3 4
Wed BG 9.3 9.3 8.9 9.4
QA 11+1 5+2 12+1
BI 12 12
Time 8.00 12.45 3.45 6.50 10.15 11.00 Comments
CP 3½ 4 3 2 He is thinking about 3:1 for all
Thu BG 8.7 5.7 11.9 8.8 5.2 9.8 meals
QA 12 6 9
BI 12 12
Time 8.00 Comments
CP 3½
Fri BG 8.4
QA 11
BI 12
Remember to refer to the Dose Adjustment Step-wise approach.
What is the problem?
What are the possible causes? What questions would you ask?
Is there a clear pattern?
Which insulin(s) need to be adjusted?
What advice would you give / what decisions would you be expecting from the patient at this stage (Friday morning)?
What would you have done differently? Why?

DAFNE © T01.002, Version 10 – October 2010 133
Unfolding Case Example 3 Mohammed
Mohammed is a 43-yr-old consultant surgeon. Diagnosed 3yrs ago. Treated initially as type 2 – put on sulphonylurea and metformin, but progressed quickly to insulin (probably LADA). Weight 79.5kg, Height 182cm = BMI 24 HbA1c 10.9% No lipohypertrophy / no DKA / no severe hypos. Has performed 1 capillary BG test in past 2 weeks prior to DAFNE course – not recorded in diary. Has general medical knowledge about diabetes, but little understanding about carbohydrates and insulin. Worried about hypos, especially at work and frequently over-treats, or over-eats to avoid them. On PAID questionnaire, most items are ‘Not a Problem’ or ‘Minor Problem’, with Worrying about low blood sugar reactions and Feelings of guilt or anxiety when getting off track with diabetes management being ‘Moderate Problems’

DAFNE © T01.002, Version 10 – October 2010 134
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 Comments
CP 3½ 0 Taking Detemir 10-12u bd
Mon BG 9.7 11.5 9.9 9.9 and Metformin 500mg bd
QA 10 0 Starting ratios 1:1
BI 10 Feeling unwell pm – home early
Time Comments
CP
Tue BG
QA
BI
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Will miss whole afternoon session (monitoring and dose adjustment planning). Is he fed up with it, or is he planning to return tomorrow? How confident is he to estimate any CPs tonight and tomorrow morning? Refer to CP list and ‘common’ foods to him. Advise 1u QA per CP. Record BGs, CPs, QA and BI in diary.

DAFNE © T01.002, Version 10 – October 2010 135
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 Comments
CP 3½ Has always taken 9u at breakfast
Tue BG 10.0 (always has the same thing)
QA 9
BI 12
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Encouragement – has done BG testing (doesn’t usually) and recorded everything! What exactly were his 1 CP at 6.30pm and his 6 CPs at 7pm? How did he work them out? How accurate was he? What was his reasoning behind the 8u corrective at 10.50pm? Perhaps wasn’t disastrous as he was unwell and maybe had underestimated tea-time CPs. Discuss safe corrective practice as in front of diary. Discuss 1:1 starting ratios and ask about trying it at breakfast-time (Mohammed not keen as he’s certain it won’t be enough and would rather try 3:1) NB 3 x 3½ = 10.5u.

DAFNE © T01.002, Version 10 – October 2010 136
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 Comments
CP 3½ 5 Wants to stay on 3:1 ratio at
Tue BG 10.0 11.7 breakfast
QA 9 5+3
BI 12
Time Comments
CP
Wed BG
QA
BI
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Higher breakfast ratio seems to have worked OK. ?Has he over-corrected lunch-time BG – will know at tea-time, or if testing BG before driving home. What is he having for evening meal? How will he work out CPs? What ratio will he take? Is he doing anything different (e.g. exercise) this evening? Discuss ‘rounding up’ QA at breakfast tomorrow. Perhaps double-check how he’s arrived at 3½ CPs.

DAFNE © T01.002, Version 10 – October 2010 137
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 Comments
CP 3½ He decided to try 3:1 at tea as it
Wed BG 9.3 seemed a more reasonable dose
QA 11+1
BI 12
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Has continued to test and record – good! Lunch-time corrective wasn’t excessive. Not a pattern yet, but ?morning BI or lunch ratio. What were his 7 CPs at evening meal? How did he work them out? Decided himself to have 3:1 for evening meal. Worked well, but point out that insulin adjustment principles will be discussed this morning and it is usually advised to increase by only ½ ratio. Did well to remember to have CPs as BG below target at bed-time, maybe didn’t need as much as 2½ - that’s why BG above target this morning.

DAFNE © T01.002, Version 10 – October 2010 138
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 Comments
CP 3½ 3 Has decided on 3:1, 1½:1, 3:1
Wed BG 9.3 9.3 ratios
QA 11+1 5+2
BI 12
Time Comments
CP
Thu BG
QA
BI
Time Comments
CP
Fri BG
QA
BI
Following session on dose adjustment principles, decided himself to try 1½:1 at lunch-time. Having corrective QA all the time – still not clear whether it’s QA:CP ratios or BI that need increasing. Breakfast 3:1 ratio still looks OK, better ‘rounded up’. Watch corrective QA doses – he could be over-doing it when he gets his BI and ratios right. What is he eating/doing tonight? How will he estimate CPs?

DAFNE © T01.002, Version 10 – October 2010 139
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 7.00 1.20 Comments
CP 3½ 3 4
Wed BG 9.3 9.3 8.9 9.4
QA 11+1 5+2 12+1
BI 12 12
Time 8.00 Comments
CP 3½
Thu BG 8.7
QA 12
BI 12
Time Comments
CP
Fri BG
QA
BI
All BGs <10mmol/l yesterday! – That’s great – will have an impact on HbA1c if maintained! Check CP estimation for evening meal – seems accurate enough. Corrective QAs still not having much effect. Likely that morning BI needs increasing, but Mohammed would rather concentrate on QA:CP ratios as he feels his BGs may be lower when he goes back to work next week (fair/good decision). BG stable overnight, so good indicator that night BI is OK. Could have safely corrected by 1u at bedtime. ?12u QA this morning – 11 + 1 corrective.
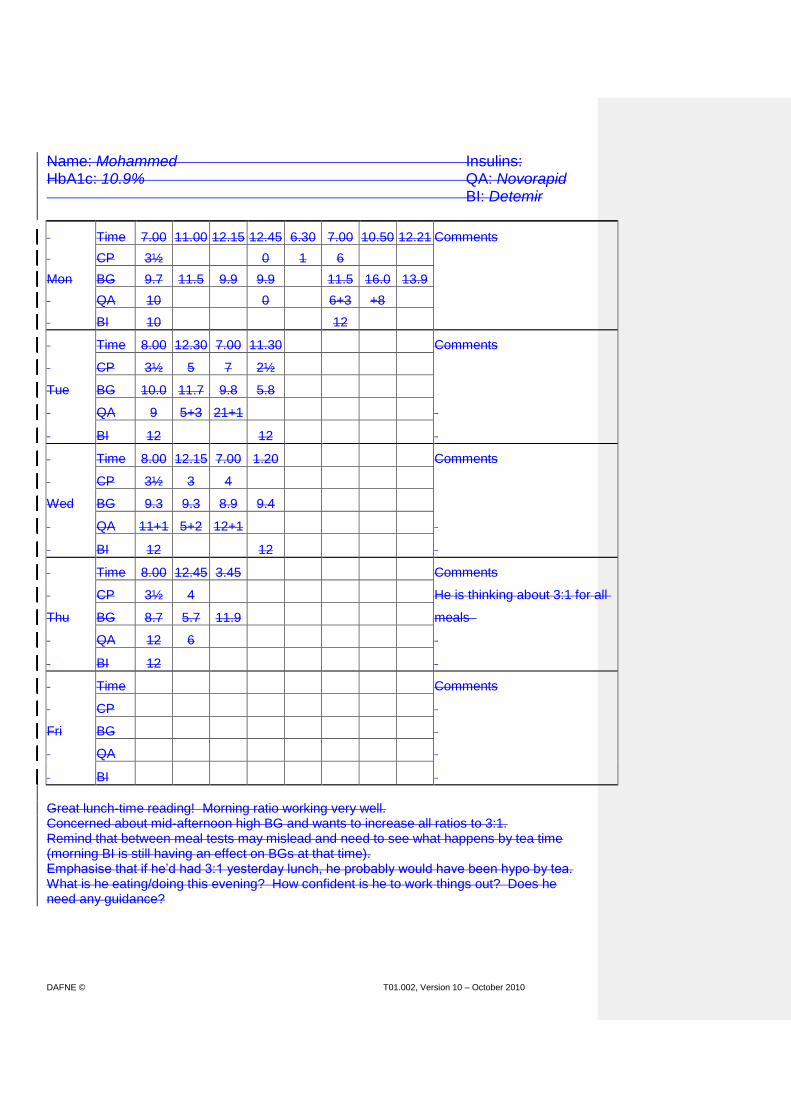
DAFNE © T01.002, Version 10 – October 2010 140
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 7.00 1.20 Comments
CP 3½ 3 4
Wed BG 9.3 9.3 8.9 9.4
QA 11+1 5+2 12+1
BI 12 12
Time 8.00 12.45 3.45 Comments
CP 3½ 4 He is thinking about 3:1 for all
Thu BG 8.7 5.7 11.9 meals
QA 12 6
BI 12
Time Comments
CP
Fri BG
QA
BI
Great lunch-time reading! Morning ratio working very well. Concerned about mid-afternoon high BG and wants to increase all ratios to 3:1. Remind that between meal tests may mislead and need to see what happens by tea time (morning BI is still having an effect on BGs at that time). Emphasise that if he’d had 3:1 yesterday lunch, he probably would have been hypo by tea. What is he eating/doing this evening? How confident is he to work things out? Does he need any guidance?
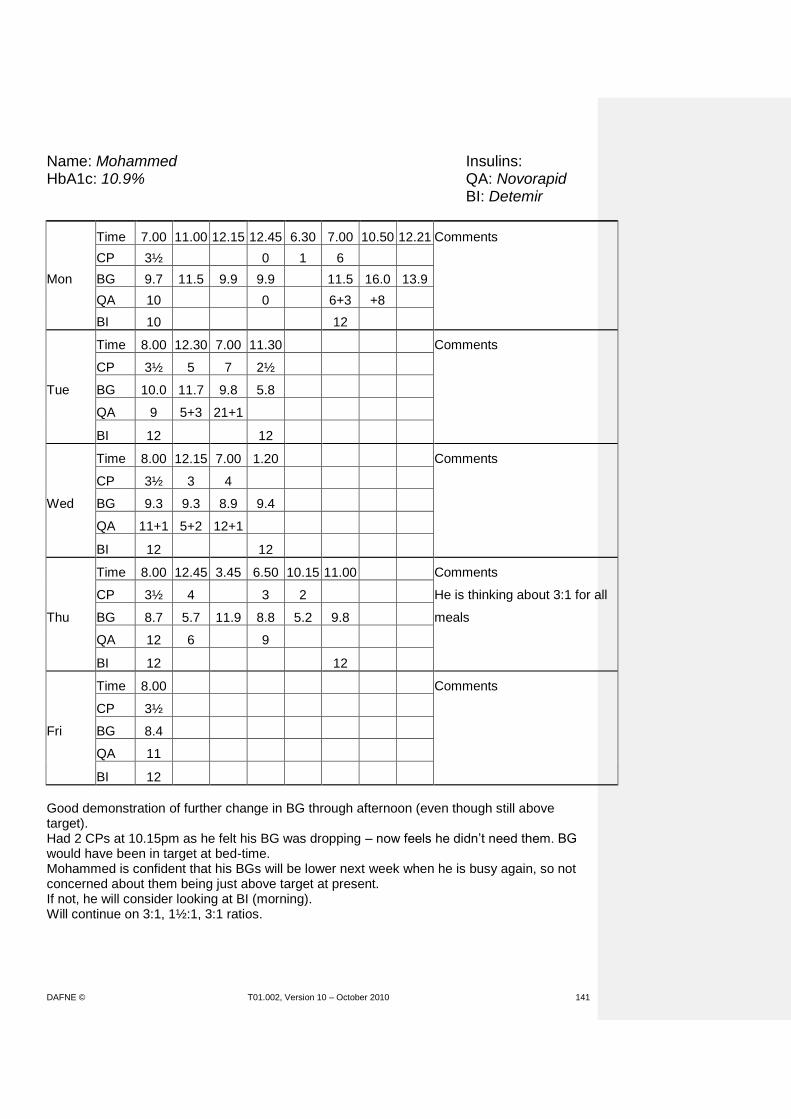
DAFNE © T01.002, Version 10 – October 2010 141
Name: Mohammed Insulins: HbA1c: 10.9% QA: Novorapid BI: Detemir
Time 7.00 11.00 12.15 12.45 6.30 7.00 10.50 12.21 Comments
CP 3½ 0 1 6
Mon BG 9.7 11.5 9.9 9.9 11.5 16.0 13.9
QA 10 0 6+3 +8
BI 10 12
Time 8.00 12.30 7.00 11.30 Comments
CP 3½ 5 7 2½
Tue BG 10.0 11.7 9.8 5.8
QA 9 5+3 21+1
BI 12 12
Time 8.00 12.15 7.00 1.20 Comments
CP 3½ 3 4
Wed BG 9.3 9.3 8.9 9.4
QA 11+1 5+2 12+1
BI 12 12
Time 8.00 12.45 3.45 6.50 10.15 11.00 Comments
CP 3½ 4 3 2 He is thinking about 3:1 for all
Thu BG 8.7 5.7 11.9 8.8 5.2 9.8 meals
QA 12 6 9
BI 12 12
Time 8.00 Comments
CP 3½
Fri BG 8.4
QA 11
BI 12
Good demonstration of further change in BG through afternoon (even though still above target). Had 2 CPs at 10.15pm as he felt his BG was dropping – now feels he didn’t need them. BG would have been in target at bed-time. Mohammed is confident that his BGs will be lower next week when he is busy again, so not concerned about them being just above target at present. If not, he will consider looking at BI (morning). Will continue on 3:1, 1½:1, 3:1 ratios.
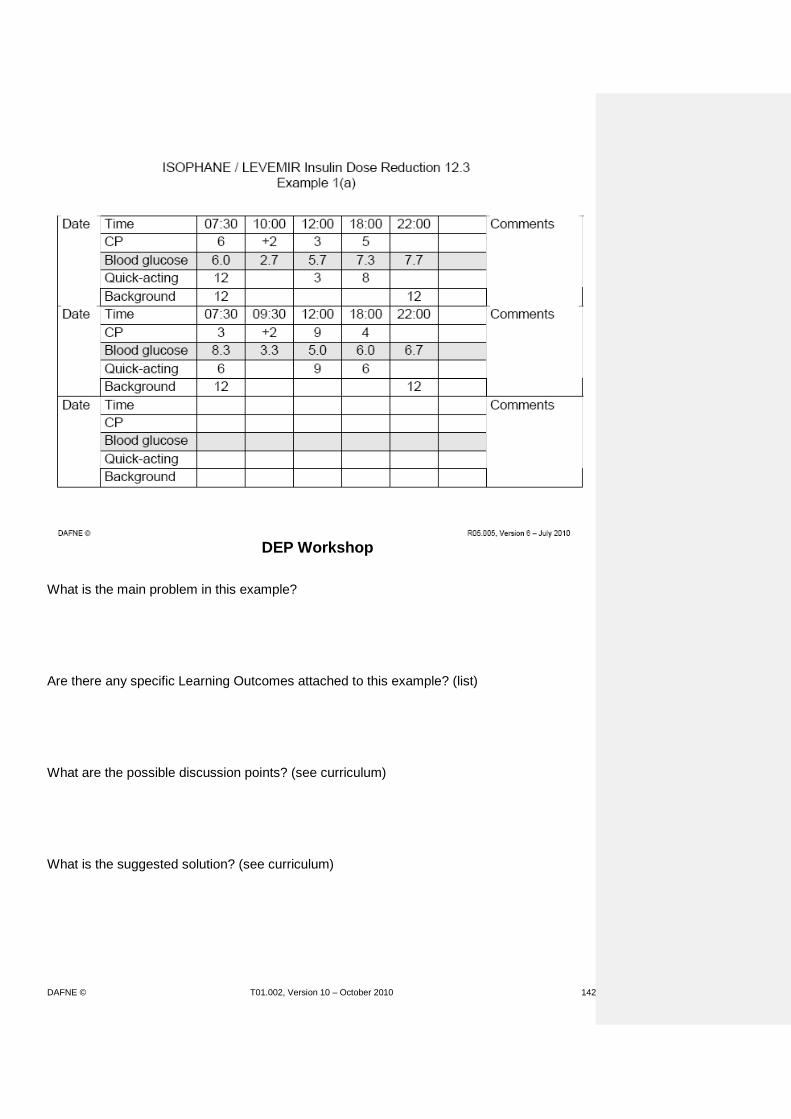
DAFNE © T01.002, Version 10 – October 2010 142
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 143
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 144
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)
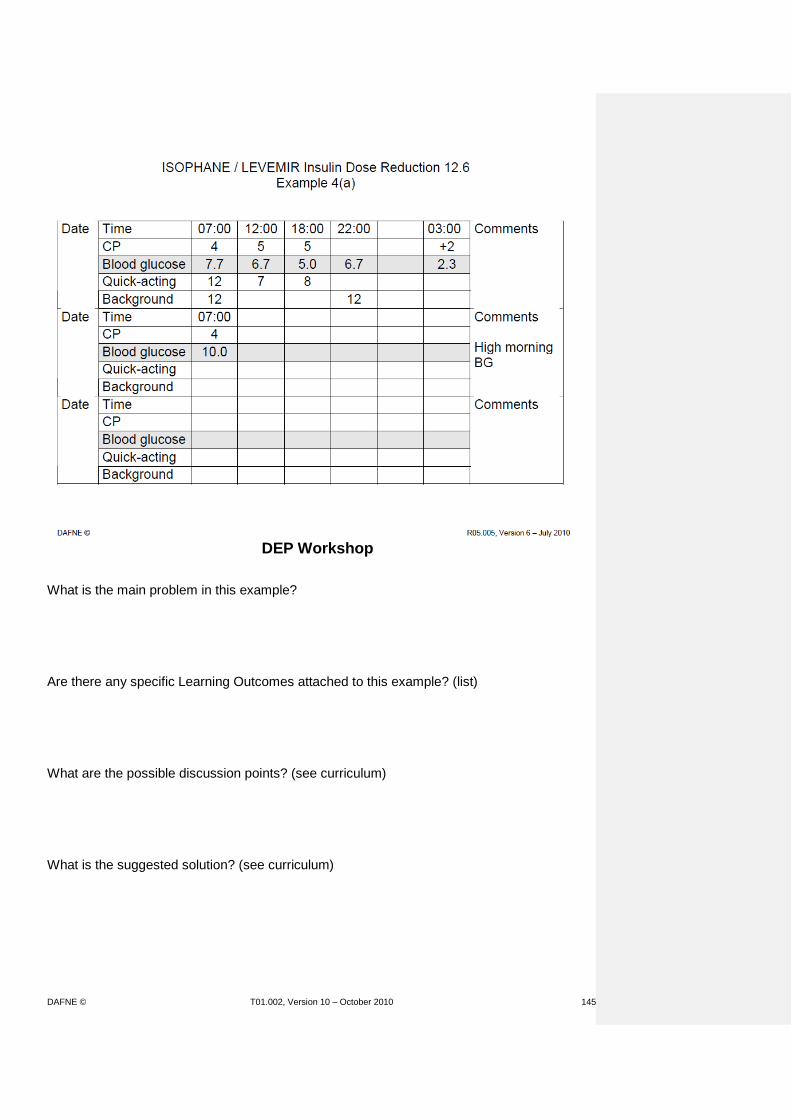
DAFNE © T01.002, Version 10 – October 2010 145
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)
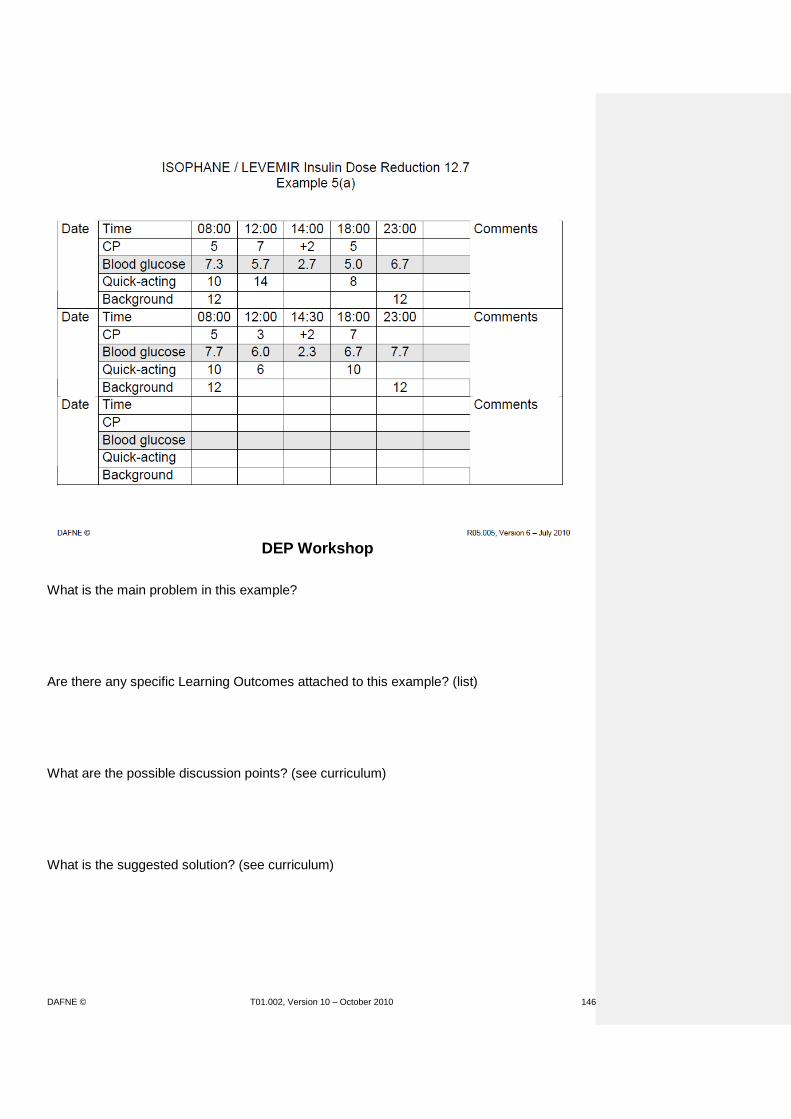
DAFNE © T01.002, Version 10 – October 2010 146
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 147
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)
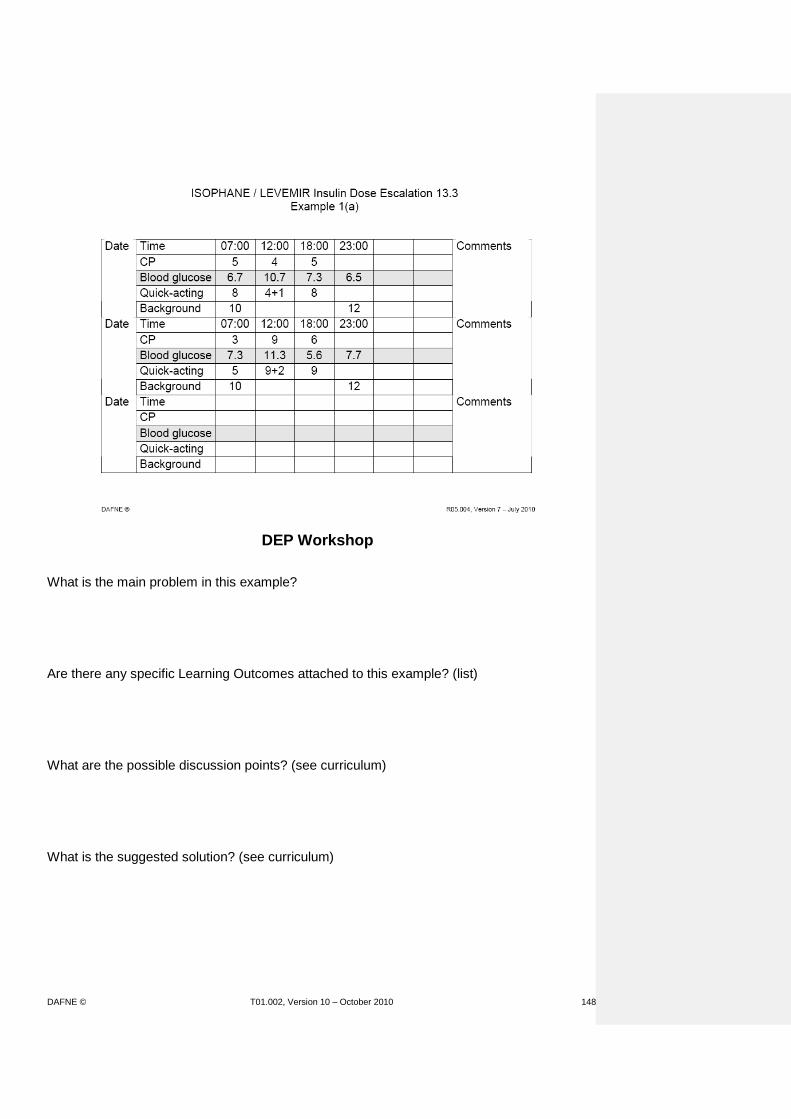
DAFNE © T01.002, Version 10 – October 2010 148
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 149
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 150
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)
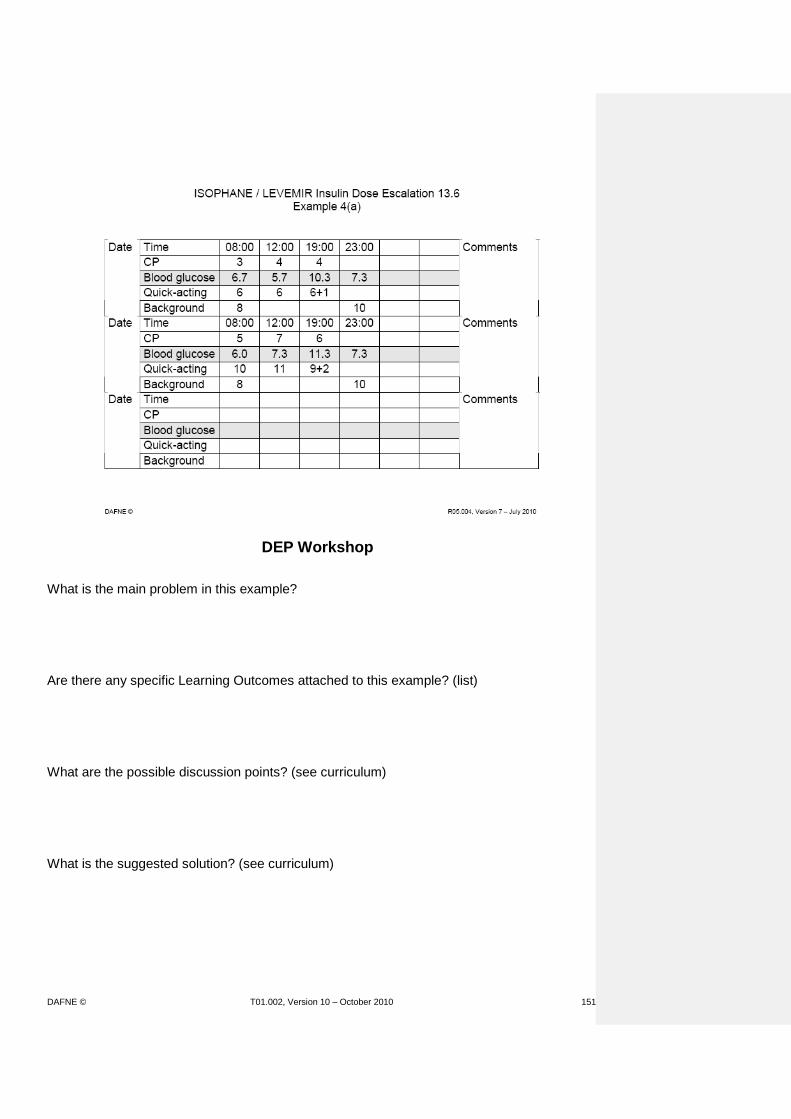
DAFNE © T01.002, Version 10 – October 2010 151
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 152
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 153
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 154
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)
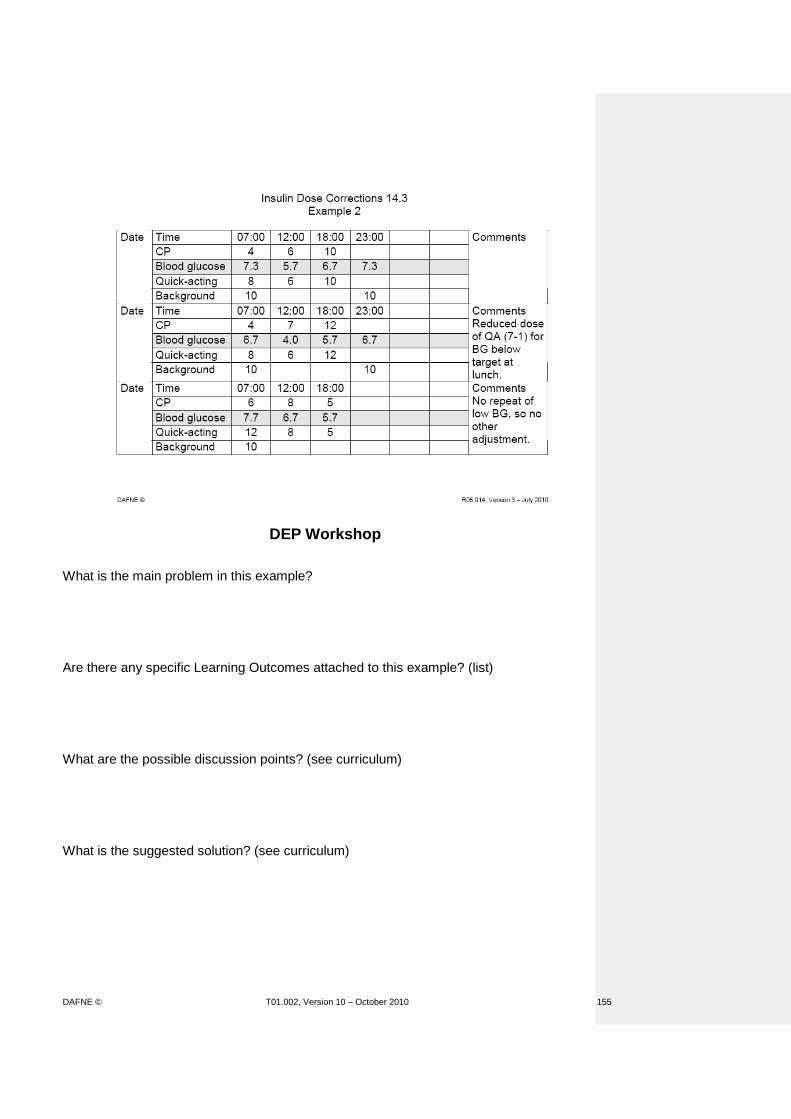
DAFNE © T01.002, Version 10 – October 2010 155
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 156
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 157
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 158
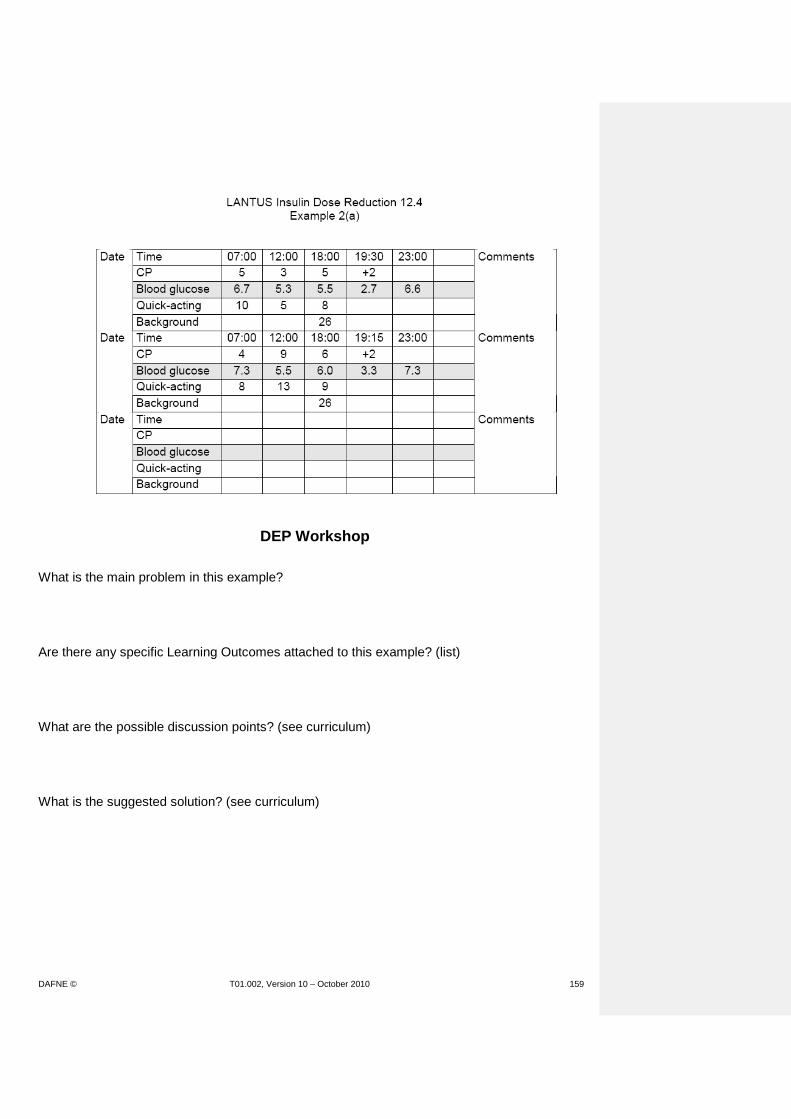
DAFNE © T01.002, Version 10 – October 2010 159
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 160

DAFNE © T01.002, Version 10 – October 2010 161
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 162

DAFNE © T01.002, Version 10 – October 2010 163
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 164
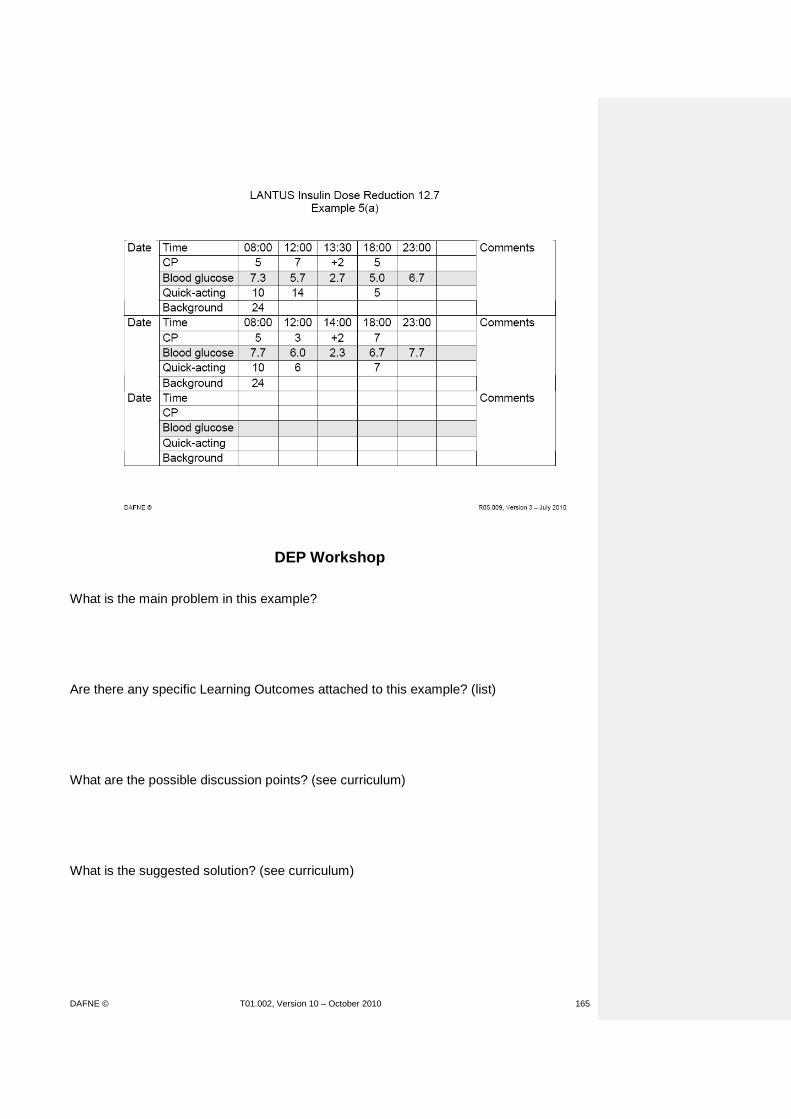
DAFNE © T01.002, Version 10 – October 2010 165
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)
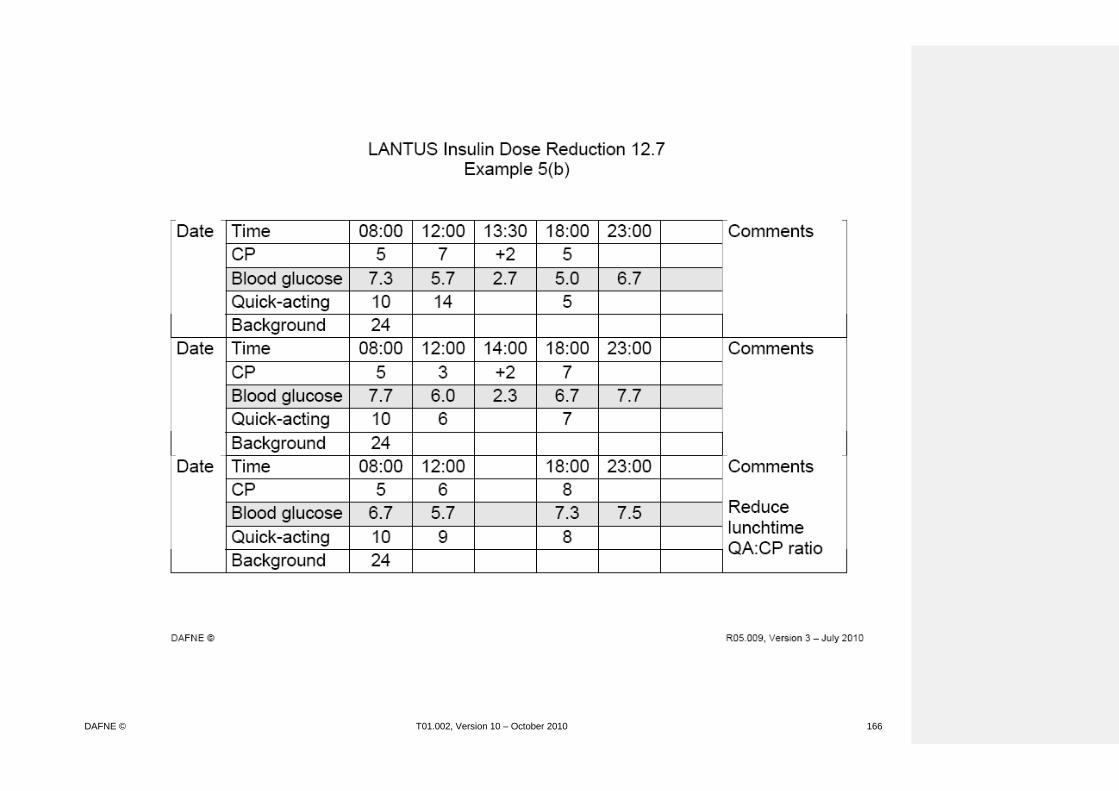
DAFNE © T01.002, Version 10 – October 2010 166

DAFNE © T01.002, Version 10 – October 2010 167
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 168

DAFNE © T01.002, Version 10 – October 2010 169
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 170

DAFNE © T01.002, Version 10 – October 2010 171
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 172
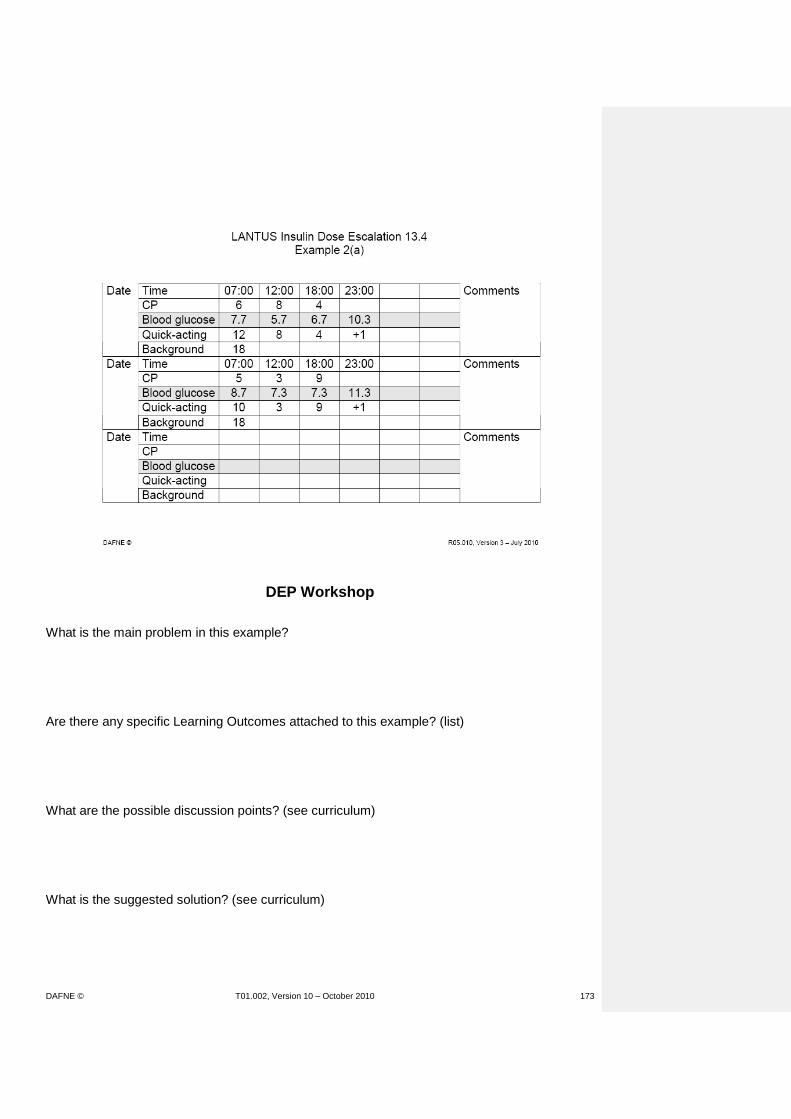
DAFNE © T01.002, Version 10 – October 2010 173
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 174

DAFNE © T01.002, Version 10 – October 2010 175
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 176

DAFNE © T01.002, Version 10 – October 2010 177
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 178

DAFNE © T01.002, Version 10 – October 2010 179
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 180

DAFNE © T01.002, Version 10 – October 2010 181
DEP Workshop
What is the main problem in this example? Are there any specific Learning Outcomes attached to this example? (list) What are the possible discussion points? (see curriculum) What is the suggested solution? (see curriculum)

DAFNE © T01.002, Version 10 – October 2010 182

DAFNE © T01.002, Version 10 – October 2010 183
HOMEWORK TASK – DAY 1 LEARNING GOALS METHODS MATERIALS/MEDIA
Practise theory of DAFNE insulin dose adjustment
Each centre pair to work through the dose adjustment examples in the DAFNE workbook be provided with one set of worksheets on the insulin dose adjustment examples to be completed as ‘homework’. If the Centre is likely to use primarily Lantus, they should review just the Lantus examples, but answer the same questions for each, ie:
What is the main problem in this example?
Are there any specific Learning Outcomes attached to this example? (list from Curriculum)
What are the possible discussion points? (see Curriculum)
What is the suggested solution? (in Curriculum) The following examples should be worked through sufficiently for feedback tomorrow:
12.6, Reduction Example 4
12.8, Reduction Example 6
13.5, Escalation Example 3
13.7, Escalation Example 5
13.8, Escalation Example 6
Dose adjustment example handouts / worksheets. DAFNE course curriculum.

DAFNE © T01.002, Version 10 – October 2010 184
DAFNE Educator Programme (DEP)
Training Workshop
Day 2
09:00 Feedback from ‘homework’ 09:45 Therapeutic Patient Education Adult Education / Learning Theories
10:1530 TEA / COFFEE
10:3045 The DAFNE curriculum and lesson planning 11:15 Writing lesson plans: getting some practise
12.0030 LUNCH
12.453:15 Sharing ideas / strategies for specific sessions, eg Sick Day Rules Exercise Alcohol Annual Review
14.4515.30 TEA / COFFEE
15.00 Therapeutic Patient Education Adult Education / Learning Theories 15:45 Goal Setting and Action Planning 17:00 Close

DAFNE © T01.002, Version 10 – October 2010 185
FEEDBACK FROM HOMEWORK – DAY 2 LEARNING GOALS METHODS MATERIALS/MEDIA
Demonstrate an understanding of DAFNE insulin dose adjustment theory Practise using the DAFNE dose adjustment examples in the workbook Have an opportunity to discuss any concerns or misunderstandings regarding the regime and/or adjustments
Each group to feed back on 1 example (chosen by DEP trainer from 12.6, Reduction Example 4; 12.8, Reduction Example 6; 13.5, Escalation Example 3; 13.7, Escalation Example 5; 13.8, Escalation Example 6) explaining discussion points and rationale for answer(s) Discuss the DAFNE workbook and how it can be used during the DAFNE course Discussion of key points, e.g.:
Only using pre-meal readings
Night time hypos
Not correcting high BG following hypo
Ways of evaluating BI (overnight profile; missing meal, etc)
Examples same whether pt on soluble QA or analogue QA
Questions and answers / suggestions Suggest Centres/individuals consider how they will use the examples in their own course(s) and to plan time to work through all the examples before delivering their first course.
Dose adjustment example handouts / worksheets. DAFNE course curriculum. DAFNE workbook Dose Adjustment Example Acetates (questions(a) and solutions(b) for Levemir/Isophane and Lantus)

DAFNE © T01.002, Version 10 – October 2010 186
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
Know the aim of the session is to discuss the educational theories that underpin DAFNE Know the 4 learning models that underpin DAFNE/TPE 1. Experiential learning model 2. Adult Learning Theory 3. Social Learning Theory
Introduction Explain - The aim of this session is to provide an opportunity to discuss the educational theories underpinning DAFNE. Ask group if they know the origins of the Düsseldorf Model. Discuss responses and explain Assal’s Therapeutic Patient Education (TPE) Model: Developed in Switzerland by a physician (Jean-Philippe Assal), who has diabetes himself. Several recognised theories are likely to have contributed to development of TPE: Experiential Learning Model (Kolb 1984) David Kolb (1984) sees learning as a core process of human development. Development results from learning that is gained through experience, and this is the basis of the ‘experiential learning model. Essentially experiential learning uses concrete experiences to inform decisions and actions, through a process of reflection and reformulation and retesting, people can learn and develop. This can be a very powerful tool in learning and is likely to be much more credible than any information given by a healthcare professional.
Acetate: “Therapeutic Patient Education” Acetate “Cycle of Experiential Learning”

DAFNE © T01.002, Version 10 – October 2010 187
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
There are four stages in this process: 1. Concrete experience. The person must immerse
themselves fully and openly in new experiences. 2. Reflective observation. The person must observe and
reflect on concrete experiences from a variety of perspectives.
3. Abstract conceptualisation. The person integrates their observations with and reformulates theories.
4. Active experimentation. The person must apply and retest these theories in decision-making and problem-solving. (cited in Quinn 3rd ed 1995)
This cycle repeats and repeats to allow for experimentation and learning. Examples of this on DAFNE – ask the group if they can recount any incidents of this during their DAFNE course Examples might include treating of hypos, trying sweet foods for the first time, eating a CHO free meal, testing out the algorithms for alcohol. Summary The DAFNE model allows for experiential learning by giving people a clear framework around CHO counting and insulin dose adjustment within which to experiment. Adult Learning Theory (Knowles 1990) Education systems for adults should be different to educational systems for children.
Acetate “Table of Adult Learning Theory”

DAFNE © T01.002, Version 10 – October 2010 188
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING
THEORIES
LEARNING GOALS METHODS MATERIALS/MEDIA
Traditional education (‘chalk and talk’) does not equip the learner with skills which are transferable in life long learning. Adult learning should promote self enquiry and autonomy. Ask the group to consider a positive learning experience they have had and compare it to an unhelpful learning experience. Ask them to list the qualities of the positive learning experience and of the unhelpful learning experience on post it notes. Collate post it notes onto flipchart paper and discuss. Now refer to the acetate ‘Table of Adult Learning Theory’ and reflect on key points that adult learning should be ‘learner centred’ and its core qualities will include:
Personal relevance
Active and task/problem based
Involved in the learning
Based on personal experiences
Self directed/self motivated Social Learning Theory (Bandura 1977) Social learning theory is to support people in becoming active self managers and includes helping people in terms of their self esteem and confidence.
Post it notes Flipchart Acetate “Social Learning diagram” Flipchart Pens Post-its

DAFNE © T01.002, Version 10 – October 2010 189
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
There are 4 core aspects to social learning theory: Mastery
This draws on peoples previous positive experiences and tries to transfer these skills to new situations
This will include building on small successes
Performing practical tasks that builds on personal skills Modelling/vicarious learning
This includes observing an appropriate role model, trying or testing something out
Learning from the suggestions of peers Emotional management
Coping with emotions/anxieties
Supporting individuals who show distress Action planning
Setting concrete plans
Developing specific strategies for situations or eventualities
In pairs, ask “can you think of an example during your observation week where social learning theory was evident?” Examples might include:
Mastery – asking people about their previous experiences as part of the lesson, congratulating people who make small change to their insulin, congratulating people who manage without a bedtime snack for the first time in 10 years.

DAFNE © T01.002, Version 10 – October 2010 190
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
Modelling/vicarious learning – seeing someone else try a small carton of fruit juice to treat a hypo, someone during the dose adjustment session suggesting someone should have a corrective dose before bed.
Emotional management – supporting individuals who are upset, acknowledging and reflecting on people’s anxieties around dose adjustment.
Action planning – recording the instructions for dose adjustment, in future goal setting.
Summary – The next session is around lesson planning, it would be worth you considering how you are going to provide opportunities for all of the above during the planning of your sessions.
Handout summarising the key learning theories
DAFNE © T01.002, Version 10 – October 2010 191
Therapeutic Patient Education
Enables patients to gain and maintain abilities for optimal
management of their diabetes
Provides information, practical learning and psychosocial support
Should help patients and their families to better co-operate with health care providers
Should be a continuous and systematic process integrated into the healthcare system
Jean-Philippe Assal et al, 2000. www.desg.org

DAFNE © T01.002, Version 10 – October 2010 192
Cycle of Experiential Learning
Concrete experience
Testing implications of concepts in new Observations and reflections situations
Formation of abstract concepts and generalisations
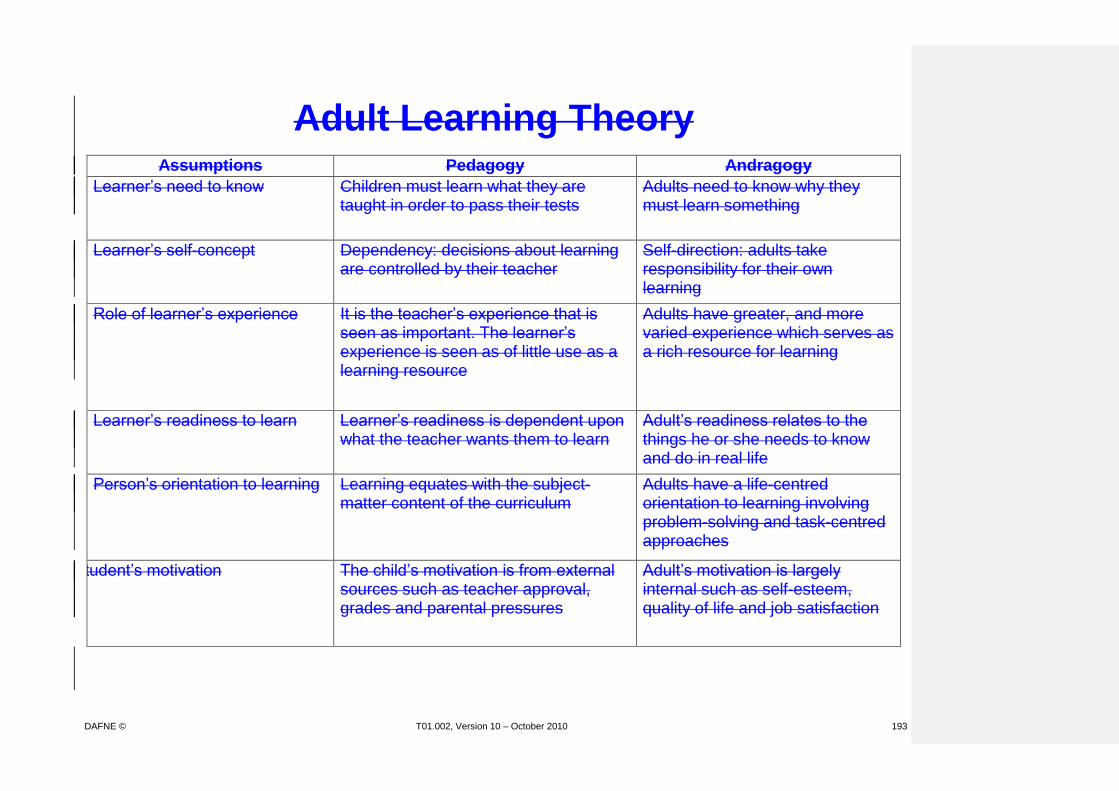
DAFNE © T01.002, Version 10 – October 2010 193
Adult Learning Theory
Assumptions Pedagogy Andragogy
Learner’s need to know Children must learn what they are taught in order to pass their tests
Adults need to know why they must learn something
Learner’s self-concept Dependency: decisions about learning are controlled by their teacher
Self-direction: adults take responsibility for their own learning
Role of learner’s experience It is the teacher’s experience that is seen as important. The learner’s experience is seen as of little use as a learning resource
Adults have greater, and more varied experience which serves as a rich resource for learning
Learner’s readiness to learn Learner’s readiness is dependent upon what the teacher wants them to learn
Adult’s readiness relates to the things he or she needs to know and do in real life
Person’s orientation to learning Learning equates with the subject-matter content of the curriculum
Adults have a life-centred orientation to learning involving problem-solving and task-centred approaches
Student’s motivation The child’s motivation is from external sources such as teacher approval, grades and parental pressures
Adult’s motivation is largely internal such as self-esteem, quality of life and job satisfaction
DAFNE © T01.002, Version 10 – October 2010 194
Social Learning Theory
Observation
Environment
DAFNE © T01.002, Version 10 – October 2010 195
Therapeutic Patient Education An overview of educational theories underpinning DAFNE
1. Therapeutic Patient Education (Jean-Philippe Assal 2000 www.desg.org)
Enables people to gain and maintain abilities for optimal management of their diabetes
Provides information, practical learning and psychological support.
Should help people to co-operate with health care providers
Should be a continuous and systematic process integrated into the healthcare system 2. Experiential Learning model (Kolb 1984) Essentially experiential learning uses concrete experiences to inform decisions and actions,
through a process of reflection and reformulation and retesting, people can learn and develop.
This can be a very powerful tool in learning and is likely to be much more credible than any
information given by a healthcare professional. Development results from learning that is gained through experience. Four stages:
Concrete experience-the person must engage fully and openly in new experiences
Reflective observation-the person must observe and reflect on their experiences from different perspectives
Abstract conceptualisation-the person thinks about how their observations could be applied to their own lives and develops a theory or plan
Active experimentation-the person applies their theory or plan to test it out This is a repetitive cycle of experimentation and learning. 3. Adult learning theory (Knowles 1990) See table. Education systems should be different for adults and children. Adult learning should be learner centred:
Personally relevant-what the person needs to know and do in their lives
Active, task and problem based
The person is involved in the learning-they can influence what is covered and take responsibility for their own learning
Based on personal experience
Self directed and self motivated
4. Social learning theory (Bandura 1977) Supports people to self manage, looks at self esteem and confidence Four key aspects
Mastery-draws on previous positive experience. Builds on small successes, develop personal skills through performing small practical tasks.
Modelling/vicarious learning-observing others, trying and testing things out, learning from the actions and suggestions of peers.
Emotional management-coping with emotions and anxieties, being supported.
Action planning-making concrete plans, developing strategies

DAFNE © T01.002, Version 10 – October 2010 196
THE DAFNE CURRICULUM and LESSON PLANNING LEARNING GOALS METHODS MATERIALS/MEDIA
Understand what a curriculum is Understand the format of the DAFNE curriculum Reflect on Adult Education Theories Be able to design and plan teaching sessions using the principles of adult education
Ask group what they understand about the term ‘curriculum’ Collect responses and correct/elaborate, using acetate Illustrate an example session from curriculum, emphasising:
‘Essential’ and ‘Desirable’ learning goals
Suggested ‘methods’ / explanations / evidence
Resources Discuss how it relates to Adult Education / Learning Theories. Emphasise that the order of topics within a session may be flexible, i.e. it is up to Educator to decide how to meet the learning goals. (Provide a personal example if possible) Ask – What is your experience of lesson planning? When planning a session, what should you take into consideration? A lesson plan is a personal plan of how you will deliver a session. It should contain all the elements on the handout ‘checklist for preparing lesson plans. What kind of teaching methods would you wish to use? Give an example of a teaching method, eg brainstorm and gather a list of other teaching methods from group, eg discussion, lecture, group activities, case study, simulation.
Acetate ‘What is a curriculum?’ Acetate(s) of eg curriculum session Flipchart and pens Acetates Handout – Checklist for preparing lesson plans

DAFNE © T01.002, Version 10 – October 2010 197
THE DAFNE CURRICULUM and LESSON PLANNING LEARNING GOALS METHODS MATERIALS/MEDIA
Discuss - Different teaching methods seen on observed DAFNE courses and how they fulfilled the principles of Adult Education. Show group an example of the DAFNE Curriculum and discuss its structure. Compare this with a lesson plan of the same session. Explain - The curriculum gives guidelines on the learning outcomes and content and the lesson plan focuses more on how this can be achieved, eg teaching methods and how long it will take.
DAFNE © T01.002, Version 10 – October 2010 198
Basic Principles of Adult Education
Participants experience should be incorporated into the programme.
Different teaching methods are needed to allow participants to gain appropriate knowledge and skills.
Participants are responsible for their own learning. Teaching should start with what participants know and are interested in.
Participants will learn from each other.
People need opportunities to develop understanding, experiment, practise and reflect on what has happened.
People should have as much control as possible in the education process.
DAFNE will constantly go through a process of development, participants will inform this.
Effective learning climate is non-threatening, relaxed and enjoyable.

DAFNE © T01.002, Version 10 – October 2010 199
Checklist for Preparing Lesson Plans
Your lesson plan should contain:
DAFNE learning outcomes
Content with appropriate teaching methods
Resources needed for each section
Appropriate timings for each part of session The content should include:
An introduction to the aims/content of session
Using participant’s current knowledge and experience
Opportunities for them to learn from each other
A range of teaching methods
Methods which allow participants to practise their skills and reflect
Opportunities for participants to have their say
A summary of main principles at the end The style of delivery should:
Be relaxed and non-judgemental
Encourage participation from the group and individuals
Respond effectively to the group’s atmosphere
Encourage a problem solving approach
Include clear explanations and language that is appropriate to the group
Encourage reflection

DAFNE © T01.002, Version 10 – October 2010 200
What is a Curriculum? Curriculum is a process that includes:
Setting goals for learning, based on needs assessment
Selecting subject matter and methods appropriate to the participants
Developing materials and activities for learning
Evaluating the results
Understanding Curriculum Development in the Workplace. A Resource for Educators.
Belfiore, M.E. (1996)
DAFNE © T01.002, Version 10 – October 2010 201
1.0 Introduction and Organisation
Resources: Session - Introduction and Organisation
1. Patient pack including:
Course Handbook
Diary(ies)
CP list
Name badge
Pencil with rubber
Timetable
2. Lesson plan
3. Timetables for Educators and guests
4. Register of patients
5. Flipchart/whiteboard
6. Pens
7. DAFNE title flipchart
8. Flipchart: “Expectations of the DAFNE course”
9. ‘Post-it’ notes
10. Hypo treatment box
Learning goals: The patient should … 1.1 Welcome and Housekeeping Resources Get to know the training team. (E) Be aware of the guest observers (if any). (E) Know essential housekeeping arrangements, ie fire escape, toilet etc. (E) Be aware of the background to DAFNE courses locally and internationally. (E) Know that they can reduce the risks of acute and long term diabetic complications. (E)
Welcome the patients to the DAFNE course and introduce Educators and guest
observers (if any). Explain any housekeeping for the week including room changes (if any),
catering/refreshments arrangements including availability of hypo treatment, location of toilets, fire exits, etc. Explain:
DAFNE is based on the principles of a course run successfully in Germany since 1980’s. Courses started in the UK in 2000. Thousands of people with Type 1 Diabetes in the UK and Republic of Ireland have now been trained in the DAFNE skills. Evidence shows that DAFNE has been shown to reduce short and long term complications and improve QoL .
DAFNE title flipchart

DAFNE © T01.002, Version 10 – October 2010 202
Understand that the DAFNE course teaches the skills of insulin dose adjustment to support self-management of their diabetes. (E) Understand that active participation is essential for the acquisition of new skills. (E)
DAFNE course teaches you the skills needed to adjust you own insulin day to day. Learning these skills enables you to take over this major part of your treatment in order to successfully manage your diabetes. This will also enable you to become more independent of health care professionals. Define: Dose Adjustment For Normal Eating Encourage participants to play an active role during the sessions and feel free
to ask questions at any time if anything is unclear.
Learning goals: The patient should … 1.2 Introductions and Expectations Resources
Understand the value of discussing previous experiences of living with diabetes. (E)
To become familiar with all other patients. (E)
Identify their personal expectations of DAFNE. (E)
Identify and agree to work within their group ground rules. (E)
Ask the participants to introduce themselves (name badges if applicable), to
discuss when their diabetes had been diagnosed, what their previous treatment had been, who had invited them to attend this training, why they came to this training and what problems they have with their diabetes. Invite the participants to list their expectations of the training week. Collect and discuss the various expectations on the flipchart.
Invite the participants to identify the ground rules for the training week.
Collect the ground rules on the flipchart.
Name badges Flipchart “Expectations of the DAFNE course” Pens and ‘post-it’ notes Flipchart and pens
Learning goals: The patient should … 1.3 Timetable Resources
Understand the structure and contents of the week (course timetable). (E)
Understand that it may be beneficial to invite a guest to some of the sessions. (E)
Illustrate and discuss:
The topics to be covered during the training course using the timetable. Emphasise:
Participation of relatives/partners/friends is particularly desirable for the session on hypoglycaemia as they may be of assistance in the recognition and management of hypoglycaemic episodes.
Timetable
DAFNE © T01.002, Version 10 – October 2010 203
Know that the contents of the course are summarised in the handbook. (E)
Explain:
The contents of course may be looked up in the Course Handbook and you may make your own additional notes in your handbook if you wish to.
Course Handbook
Learning goals: The patient should … 1.4 Blood Testing and Hypoglycaemia Resources
Understand the importance of blood glucose measurements prior to meals, snacks and treating hypos. (E)
Be aware that hypos may occur during the week and that there is specific advice for their treatment which they should familiarise themselves with. (E)
Emphasise:
The importance of testing their blood glucose level before eating (lunch), before having snacks, and if feeling hypo. Explain:
Hypos are not uncommon during the week (1-2 mild hypos per week can be expected). Please check your blood glucose level if you feel low. The advice for treating a hypo is slightly different on DAFNE to what you may have been previously taught, please familiarise yourself with this and do not hesitate to ask if you are unsure. Identify the recommended hypo treatments and where the box will be kept during the week.
Hypo treatments box
Learning goals: The patient should … 1.5 Quiz and Summary Resources
Understand the purpose of the quiz. (E)
Be aware that the week is an introduction to the skills. They will be responsible for implementing on a daily basis, and review and update their own practice. (E)
Explain:
You will be asked to work through the quiz during the training week. The quiz helps the Educators find out whether the sessions have truly met your requirements and what information needs to be refreshed. Explain:
You should not expect perfect blood glucose control by the end of the training week. The DAFNE skills need to be implemented on a daily basis. Keeping a record of your blood sugars, food and insulin in the DAFNE diary will help you identify patterns and make appropriate dose adjustments in the future for life long good glycaemic control.
Quiz Pencil with rubber

DAFNE © T01.002, Version 10 – October 2010 204
WRITING LESSON PLANS : GETTING SOME PRACTISE LEARNING GOALS METHODS MATERIALS/MEDIA
Understand how a lesson plan is different to a curriculum. Participants will be able to write a lesson plan using the DAFNE curriculum.
Ask group for their thoughts on the differences between a curriculum and a lesson plan. Discuss:
Personal plan of how you will meet learning outcomes
Identify where session will be located within the course
Prior consideration of timing for individual topics within a session
Plan of methods / strategies and how core or personally developed resources will be used
Effective way of getting to know the content of curriculum (look at it in detail).
Explain that DAFNE Educators should develop their own lesson plans and may use different teaching methods from those observed (if they wish), as long as they cover the content of the whole curriculum, use a varied range of teaching methods and meet the learning outcomes. Divide into smaller groups 3-4 people (if any have previously produced lesson plans, try to place them with participants who have not). Ask each group to write a lesson plan using part of the DAFNE curriculum. Groups present their lesson plans and ideas. Feedback and discussion.
Lesson plan pro forma Acetates of blank lesson plan (Copied section of) Curriculum OHP pens

DAFNE © T01.002, Version 10 – October 2010 205
DAFNE LESSON PLAN
Session Title: Curriculum pages: (T02.002 – Issue 8. October 2004) Day: Time: Key aims of the session:

DAFNE © T01.002, Version 10 – October 2010 206
Session:
Learning Outcomes Method Resources Time
DAFNE © T01.002, Version 10 – October 2010 207
DAFNE LESSON PLAN
Session Title: Individual Dose Adjustment Practise Curriculum pages: 133-136 (T02.002 – Issue 8. October 2004)
Day: Tuesday - Friday Time: 9-10am and 4.00-5.00pm Key aims of the session:
To enable individual participants to reflect on what they have learned in relation to CP estimation and insulin dose adjustment so that they can demonstrate application of the principles to their own blood glucose management.

DAFNE © T01.002, Version 10 – October 2010 208
Session:
Learning Outcomes Method Resources Time Understand the benefits of
sharing their BG results with the other group members (E)
Understand that before
adjusting insulin doses, they should check the accuracy of their CP estimation (E)
Be able to reflect on insulin
dose adjustment theory using the systematic step-wise approach (E)
Be aware that hypoglycaemia
should be treated with 1½-2 CPS of rapid-acting CHO (E)
Be aware that a BG reading
below target range at a mealtime can be corrected by injecting less QA insulin than required for CHO eaten (E)
1st session / day: Explanation of the purpose and format of the session. Emphasise importance of everyone listening to each other.
--- Each person in turn to ‘display’ and discuss their diary, explaining: Which QA and BI they are using Their doses and ratios Their BG target ranges What CHO they have had and how they calculated the
CPs Any challenges / difficulties
Highlight and emphasise ‘step-wise’ approach to dose adjustment to encourage safe practice and prevent ‘tail-chasing’
--- Address specific issues as required, eg: Hypoglycaemia / BG below target range Can they identify cause(s)? Recognition / symptoms Appropriate treatment? Insulin adjustment / correction CHO (e.g. at bedtime)
Diary on acetate OHP Pens Posters – BG target ranges, Insulin actions Course Handbook p24 Poster – Treating a hypo
2 mins 5 – 10 mins each

DAFNE © T01.002, Version 10 – October 2010 209
Session:
Learning Outcomes Method Resources Time Be aware that a BG reading
below target range at bedtime can be corrected by eating additional CPs (E)
Be aware that a BG reading
above target range can be corrected with extra QA insulin (but used cautiously until sensitivity known) (E)
Know that, apart from during
illness, high BG should not be corrected in between meals (E)
Be aware that if BG is more
than 13mmol/l on more than 1 occasion, or a one-off reading of more than 17mmol/l, with no clear cause, they should test for ketones
Hyperglycaemia Can they identify any cause(s)? Appropriate use of correction dose When is adjustment to BI or QA:CP ratio appropriate? Recurrent high readings Screening for ketones
Poster – Guidelines for corrections
DAFNE © T01.002, Version 10 – October 2010 210
SHARING IDEAS / STRATEGIES FOR SPECIFIC SESSIONS - WORKSTATIONS LEARNING GOALS METHODS MATERIALS/MEDIA
Understand the aims of the session
Note: This session can be quite flexible in its delivery and needs to be based on the issues that were highlighted by the DAFNE trainees on Day 1. It may be necessary to alter the content and provide additional resources dependent on the trainee’s requirements. Introduce session - this is an opportunity to share ideas on some of the sessions that might be more challenging to deliver. Refer to flipchart collected yesterday for sessions the group wanted to spend more time on. Discuss with group that there are 4 workstations:
Sick day rules
Alcohol
Physical activity
Annual review/planning difficult sessions Given the time available they will be able to do 3 out of 4 of these. Workstation 1 – Sick Day Rules Ask group what difficulties they anticipate in delivering this session. Ask group to outline the main areas to be covered in this session. Demonstrate the order and flow that you, as an educator, would use to deliver this session. Using handouts, discuss minor and severe sick day rules. Use examples and encourage reference to DAFNE handbook.
Pens flipcharts post-it’s

DAFNE © T01.002, Version 10 – October 2010 211
SHARING IDEAS / STRATEGIES FOR SPECIFIC SESSIONS - WORKSTATIONS LEARNING GOALS METHODS MATERIALS/MEDIA
Workstation 2 – Alcohol NB This session needs careful facilitation. The key points covered should be; Long acting insulin analogues, how educators feel about advising participants to take QA with alcoholic drinks containing CPs. This workstation needs to be semi-supervised. Ask the trainees to work their way through the worksheets: Alcohol and DAFNE principles (No 1) Alcohol and DAFNE (No 2) Alcohol Scenarios (No 3) Workstation 3 – Physical Activity DAFNE and Exercise Physical activity scenarios Workstation 4 – Annual Review/Planning Difficult Sessions The group are asked to identify sessions other than the above which they would like some support in planning to make as interactive as possible. The DEP trainer facilitates a session looking at lesson planning and methods used and may wish to use the annual review session as an example using the Leicester model.

DAFNE © T01.002, Version 10 – October 2010 212
DAFNE: Exercise Physiology Educator Notes
The DAFNE Curriculum sets out to teach patients with Type 1 Diabetes how to remove diabetes as a limiting factor to being more active, and to normalise function. By increasing the patient’s understanding of exercise physiology a greater confidence in his/her own training and performance can be instilled. It is important that the individual with Type 1 diabetes knows that the greatest advantage of exercise is its cardioprotective effect, rather than improved glycaemic control1,2; the latter of which is more pronounced in Type 2 Diabetes and overweight individuals with Type 1 Diabetes by improving insulin sensitivity. However, by demonstrating the levels of commitment required by rigorous BG monitoring before and after exercise, and adjusting insulin or CP intake accordingly as per DAFNE guidance, the risk of hypos, or decline in BGs can be minimised1,3. Exercise Physiology
During exercise working muscles demand more oxygen; this is met by increased cardiac and respiratory output. Adequate amounts of oxygen need to be delivered to prevent premature fatigue. In addition to this there needs to be rapid mobilisation and redistribution of metabolic fuels to ensure there is adequate energy available for the working muscles. The provision of fuel in the blood is dependent on the effects of the sympathetic nervous system (SNS) and hormones on the liver and adipose tissue1,2,4. Blood glucose levels can rise or fall depending on the type, duration and intensity of activity an individual takes part in, these factors also influence whether the activity is anaerobic or aerobic in nature, or a mixture of the two. Oxygen consumption
There is a linear relationship between aerobic metabolism and maximal exercise intensity in most forms of exercise, whereby when walking, cycling or running faster, our oxygen consumption (VO2) increases in parallel. This consumption of oxygen will continue to increase until it reaches a maximum rate (VO2max) this is shown by the plateau on the graph below. Exercise can only be continued for a short while at this level as there is no further increase in oxygen uptake. An individual’s VO2max is determined by several factors including weight, height, age, sex, habitual activity levels and inherited factors1. It is generally considered the best indicator of cardiorespiratory endurance and aerobic fitness. Definition: Exercise intensity
Intensity Mild Moderate Intense %VO2 max 25 50 75
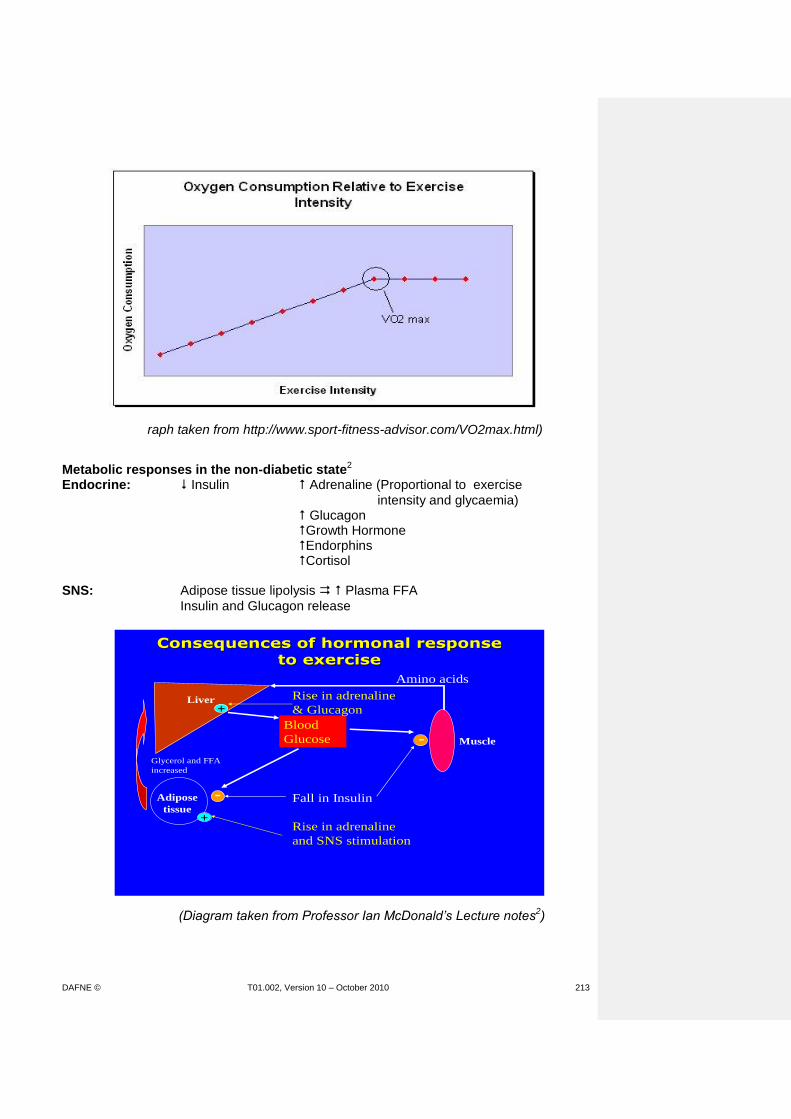
DAFNE © T01.002, Version 10 – October 2010 213
(Graph taken from http://www.sport-fitness-advisor.com/VO2max.html)
Metabolic responses in the non-diabetic state2
Endocrine: Insulin Adrenaline (Proportional to exercise
intensity and glycaemia) Glucagon Growth Hormone Endorphins Cortisol SNS: Adipose tissue lipolysis Plasma FFA
Insulin and Glucagon release
(Diagram taken from Professor Ian McDonald’s Lecture notes2)
Consequences of hormonal response Consequences of hormonal response
to exerciseto exercise
Liver
Adipose
tissue
Muscle
Glycerol and FFA
increased
Amino acids
Blood
Glucose
Fall in Insulin
Rise in adrenaline
and SNS stimulation
-
-
+
Rise in adrenaline
& Glucagon+
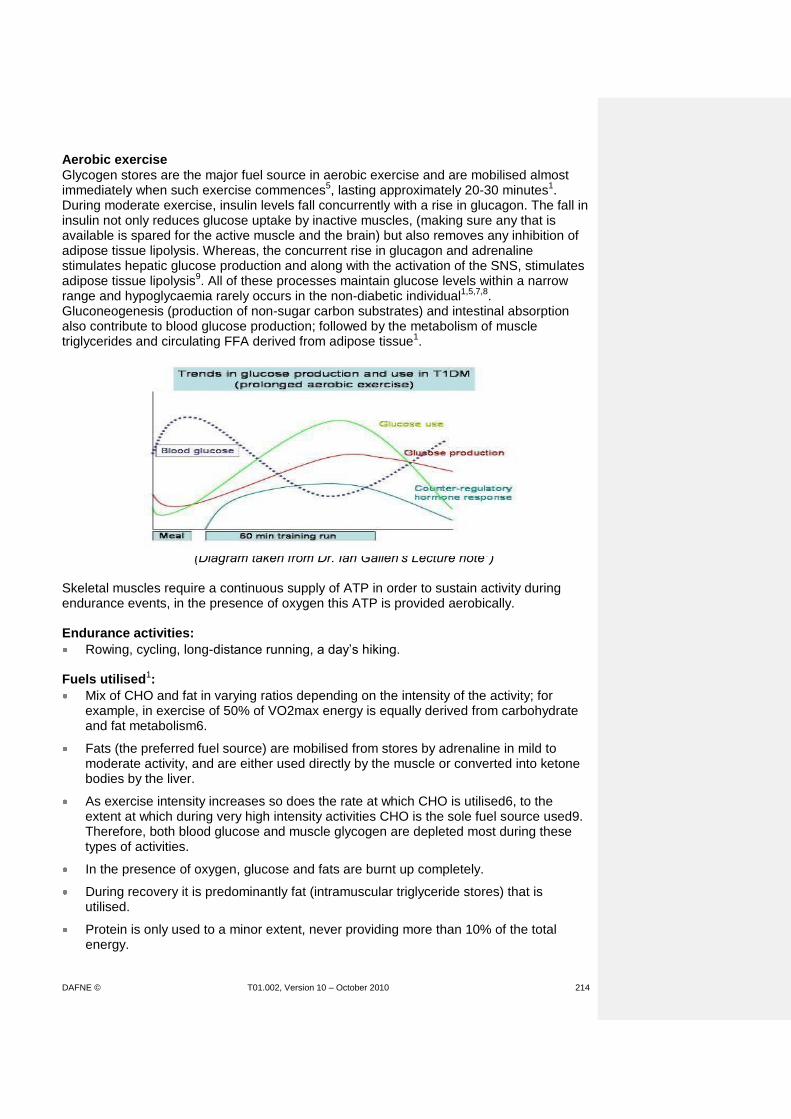
DAFNE © T01.002, Version 10 – October 2010 214
Aerobic exercise
Glycogen stores are the major fuel source in aerobic exercise and are mobilised almost immediately when such exercise commences5, lasting approximately 20-30 minutes1. During moderate exercise, insulin levels fall concurrently with a rise in glucagon. The fall in insulin not only reduces glucose uptake by inactive muscles, (making sure any that is available is spared for the active muscle and the brain) but also removes any inhibition of adipose tissue lipolysis. Whereas, the concurrent rise in glucagon and adrenaline stimulates hepatic glucose production and along with the activation of the SNS, stimulates adipose tissue lipolysis9. All of these processes maintain glucose levels within a narrow range and hypoglycaemia rarely occurs in the non-diabetic individual1,5,7,8. Gluconeogenesis (production of non-sugar carbon substrates) and intestinal absorption also contribute to blood glucose production; followed by the metabolism of muscle triglycerides and circulating FFA derived from adipose tissue1.
(Diagram taken from Dr. Ian Gallen’s Lecture note3) Skeletal muscles require a continuous supply of ATP in order to sustain activity during endurance events, in the presence of oxygen this ATP is provided aerobically. Endurance activities:
Rowing, cycling, long-distance running, a day’s hiking. Fuels utilised1:
Mix of CHO and fat in varying ratios depending on the intensity of the activity; for example, in exercise of 50% of VO2max energy is equally derived from carbohydrate and fat metabolism6.
Fats (the preferred fuel source) are mobilised from stores by adrenaline in mild to moderate activity, and are either used directly by the muscle or converted into ketone bodies by the liver.
As exercise intensity increases so does the rate at which CHO is utilised6, to the extent at which during very high intensity activities CHO is the sole fuel source used9. Therefore, both blood glucose and muscle glycogen are depleted most during these types of activities.
In the presence of oxygen, glucose and fats are burnt up completely.
During recovery it is predominantly fat (intramuscular triglyceride stores) that is utilised.
Protein is only used to a minor extent, never providing more than 10% of the total energy.
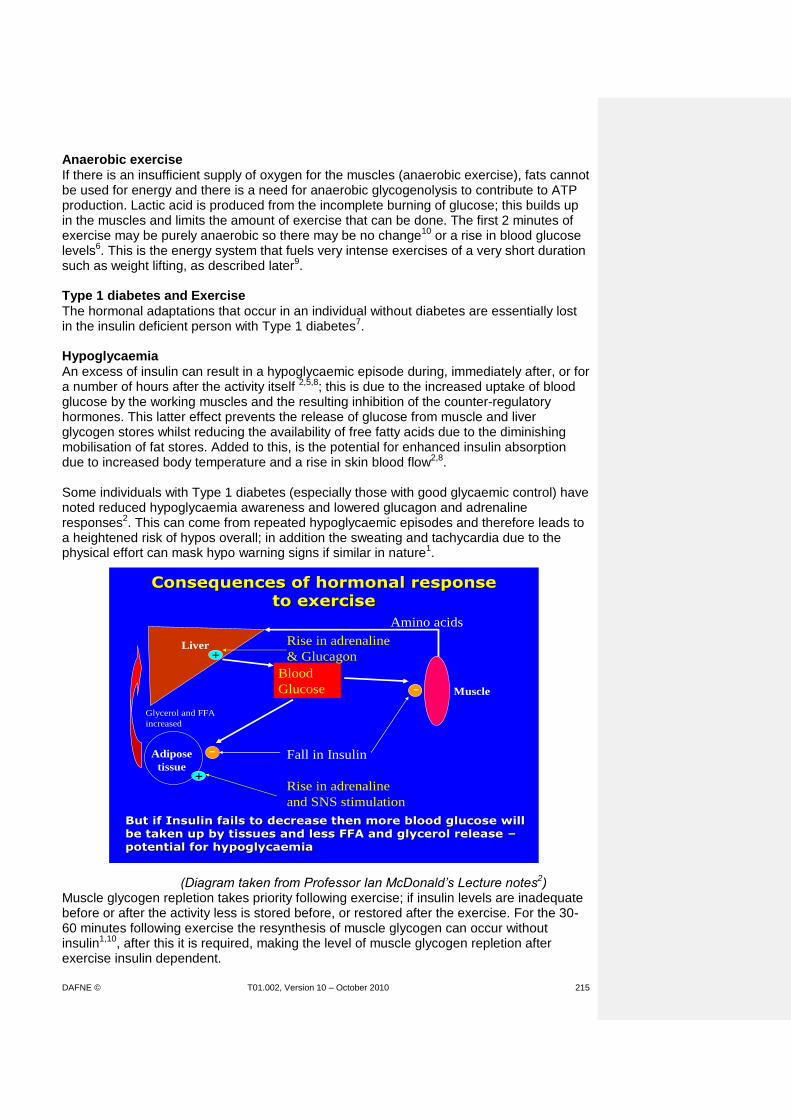
DAFNE © T01.002, Version 10 – October 2010 215
Anaerobic exercise
If there is an insufficient supply of oxygen for the muscles (anaerobic exercise), fats cannot be used for energy and there is a need for anaerobic glycogenolysis to contribute to ATP production. Lactic acid is produced from the incomplete burning of glucose; this builds up in the muscles and limits the amount of exercise that can be done. The first 2 minutes of exercise may be purely anaerobic so there may be no change10 or a rise in blood glucose levels6. This is the energy system that fuels very intense exercises of a very short duration such as weight lifting, as described later9. Type 1 diabetes and Exercise
The hormonal adaptations that occur in an individual without diabetes are essentially lost in the insulin deficient person with Type 1 diabetes7. Hypoglycaemia
An excess of insulin can result in a hypoglycaemic episode during, immediately after, or for a number of hours after the activity itself 2,5,8; this is due to the increased uptake of blood glucose by the working muscles and the resulting inhibition of the counter-regulatory hormones. This latter effect prevents the release of glucose from muscle and liver glycogen stores whilst reducing the availability of free fatty acids due to the diminishing mobilisation of fat stores. Added to this, is the potential for enhanced insulin absorption due to increased body temperature and a rise in skin blood flow2,8. Some individuals with Type 1 diabetes (especially those with good glycaemic control) have noted reduced hypoglycaemia awareness and lowered glucagon and adrenaline responses2. This can come from repeated hypoglycaemic episodes and therefore leads to a heightened risk of hypos overall; in addition the sweating and tachycardia due to the physical effort can mask hypo warning signs if similar in nature1.
(Diagram taken from Professor Ian McDonald’s Lecture notes2) Muscle glycogen repletion takes priority following exercise; if insulin levels are inadequate before or after the activity less is stored before, or restored after the exercise. For the 30-60 minutes following exercise the resynthesis of muscle glycogen can occur without insulin1,10, after this it is required, making the level of muscle glycogen repletion after exercise insulin dependent.
Consequences of hormonal response Consequences of hormonal response
to exerciseto exercise
Liver
Adipose
tissue
Muscle
Glycerol and FFA
increased
Amino acids
Blood
Glucose
Fall in Insulin
Rise in adrenaline
and SNS stimulation
-
-
+
Rise in adrenaline
& Glucagon+
But if Insulin fails to decrease then more blood glucose will But if Insulin fails to decrease then more blood glucose will
be taken up by tissues and less FFA and glycerol release be taken up by tissues and less FFA and glycerol release ––
potential for hypoglycaemiapotential for hypoglycaemia
DAFNE © T01.002, Version 10 – October 2010 216
Therefore, if higher intensity exercise is undertaken following this, larger amounts of blood glucose need to be utilised as the muscle glycogen stored is limited, which results in both fatigue and a faster drop in blood glucose levels. Hepatic glycogen stores are more slowly replenished. The time it takes for repletion of glycogen stores explains why the hypoglycaemic episode may occur a number of hours following the exercise. Hyperglycaemia
Raised blood sugars following activity may also occur in the individual with Type 1 diabetes, either because:
1) The individual is insulin deficient. OR
2) Following extremely intense exercise. 1a) Pre-exercise high blood glucose levels with ketones
If there is a severe lack of circulating insulin an excessive hormonal response occurs resulting in hyperglycaemia and the production of ketones; this is due to an increase in hepatic glucose production and reduced glucose disposal by the working muscle. The release of counter regulatory hormones as a response to exercise itself will further elevate blood glucose levels and cause metabolic disturbance. Therefore, hyperglycaemia during activity can lead to lesser use of muscle glycogen and a greater use of blood glucose1,6. Hyperglycaemia (>13mols/l) with ketonuria is a contraindication to exercise, as suggested in the DAFNE curriculum this needs to be corrected with QA insulin, blood glucose levels decline and urinary ketones disappear before exercise can be resumed. 1b) High blood glucose levels without ketones
This occurs if there is a relative or mild deficiency in insulin, perhaps due to an excess of CPs at the last meal, exercising soon after eating (which can occur during the DAFNE week if going for a walk in the exercise session soon after having lunch), or a consequence of stress. There is no need to abstain from the activity but to monitor blood glucose levels before and after exercise as usual and keep well hydrated. It is more than likely that BG levels will fall6 if they do not fall extra QA insulin may be required1. 2) Very short intense exercise with normal blood glucose levels
The first 10-20 seconds of exercise is powered by creatine phosphate and ATP and is anaerobic (without oxygen) in nature10. Glucose is not involved in the energy production and therefore it is not likely that blood glucose levels will fall following very intense/short duration activities such as weight lifting, pole vaulting, and sprint racing. In fact blood glucose will rise due to the release of counter-regulatory hormones such as adrenaline1,8,9. causing hepatic glucose output to exceed the rate of glucose uptake6. The state of insulin resistance created may last a few hours following the activity itself. In which case, the individual with diabetes would need to take additional insulin to bring their blood glucose levels down after the activity. Exercise can remain solely anaerobic for up to the first 2 minutes10. Summary
There are a number of physiological changes (cardiac, respiratory, neural and hormonal) that occur during exercise that can affect glycaemia and therefore performance of the individual with Type 1 diabetes. The action of manipulating insulin doses before, during and after the event, and adapting CP intake according to blood glucose levels are a learned skill that come with perseverance and dedication. Suggestions of which are outlines in the DAFNE curriculum for physical activity and exercise.

DAFNE © T01.002, Version 10 – October 2010 217
DAFNE Educators Reading List: Diabetes and Exercise
1. Nagi D (ed). Exercise and Sport In Diabetes. Wiley, 2005 2. MacDonald IA. Lecture notes: What is different about “diabetic physiology”? Royal
Society of Medicine, June 2005
3. Gallen I. Lecture notes: Diabetes and Sport. Royal Society of Medicine, June 2005
4. Wilmore JH and Costill DL. (2005) Physiology of Sport and Exercise: 3rd Edition. Champaign, IL: Human Kinetics
5. www.runsweet.com 2007
6. Maughan R (ed) Nutrition in Sport: Volume VII. 2002: Blackwell Science
7. American Diabetes Association: Diabetes mellitus and exercise; position statement. Diabetes Care 2004; 27(1): 58-62
8. Riddell M. Lecture notes: Blood glucose control during and after exercise in Type 1 diabetes: Is it at all possible. IDF Congress, December 2006
9. Marliss E and Vranic M. Intense exercise has unique effects on both insulin release and its roles in glucoregulation. Diabetes 2002; 51 (1): 271-283
10. Colberg S. The Diabetic Athlete. Human Kinetics, 2001
Websites
www.steveredgrave.com
www.runsweet.com
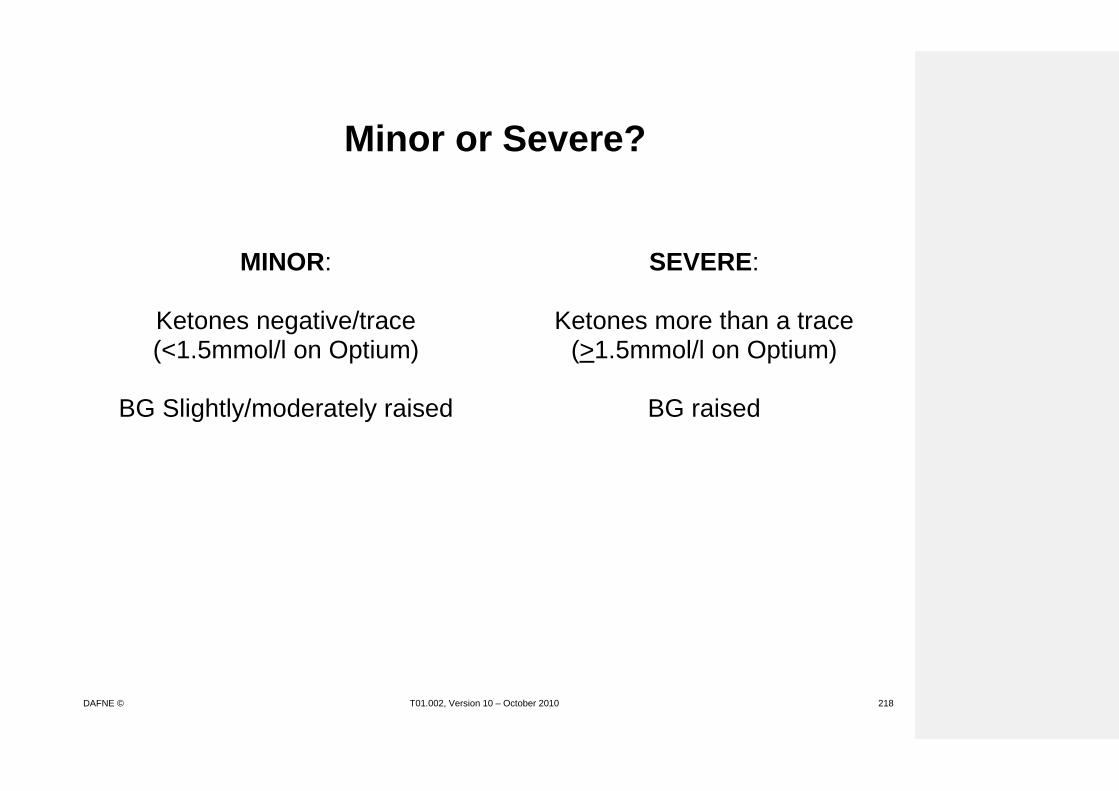
DAFNE © T01.002, Version 10 – October 2010 218
Minor or Severe?
MINOR:
SEVERE:
Ketones negative/trace (<1.5mmol/l on Optium)
Ketones more than a trace
(>1.5mmol/l on Optium)
BG Slightly/moderately raised
BG raised
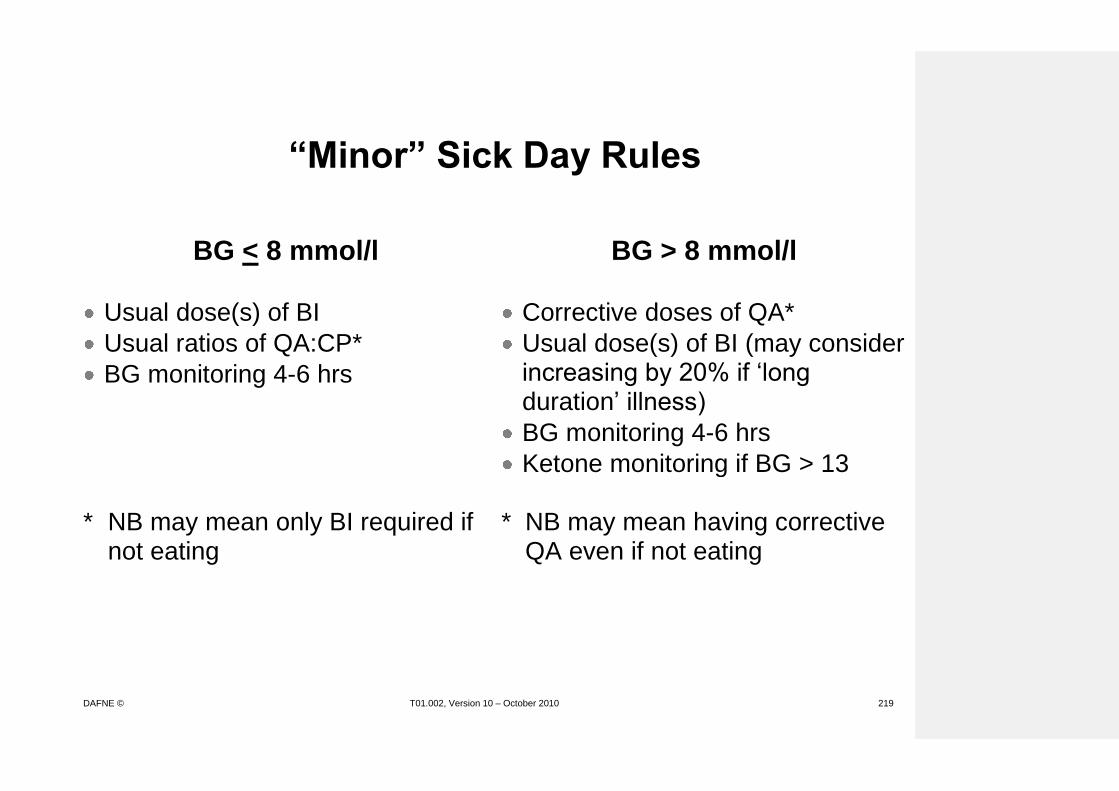
DAFNE © T01.002, Version 10 – October 2010 219
“Minor” Sick Day Rules
BG < 8 mmol/l BG > 8 mmol/l
Usual dose(s) of BI
Usual ratios of QA:CP*
BG monitoring 4-6 hrs
Corrective doses of QA*
Usual dose(s) of BI (may consider increasing by 20% if ‘long duration’ illness)
BG monitoring 4-6 hrs
Ketone monitoring if BG > 13 * NB may mean only BI required if
not eating
* NB may mean having corrective
QA even if not eating

DAFNE © T01.002, Version 10 – October 2010 220
“Severe” Sick Day Rules
BG > 13 mmol/l Ketones mod-large
(>3mmol/l on Optium)
BG 10-13 mmol/l Ketones small-mod
(1.5 - 3mmol/l on Optium)
Calculate previous day’s total insulin dose: tdd (BI and QA)
Continue usual dose(s) of BI
QA dose = 20% of tdd
BG and ketone monitoring 2 hourly
Repeat additional QA doses
(20% of tdd) as required
Drink >100ml fluid per hour
CHO will help to stop ketones
Calculate previous day’s total insulin dose: tdd (BI and QA)
Continue usual dose(s) of BI
QA dose = 10% of tdd
BG and ketone monitoring 2 hourly
Repeat additional QA doses
(10% of tdd) as required
Drink >100ml fluid per hour
CHO will help to stop ketones
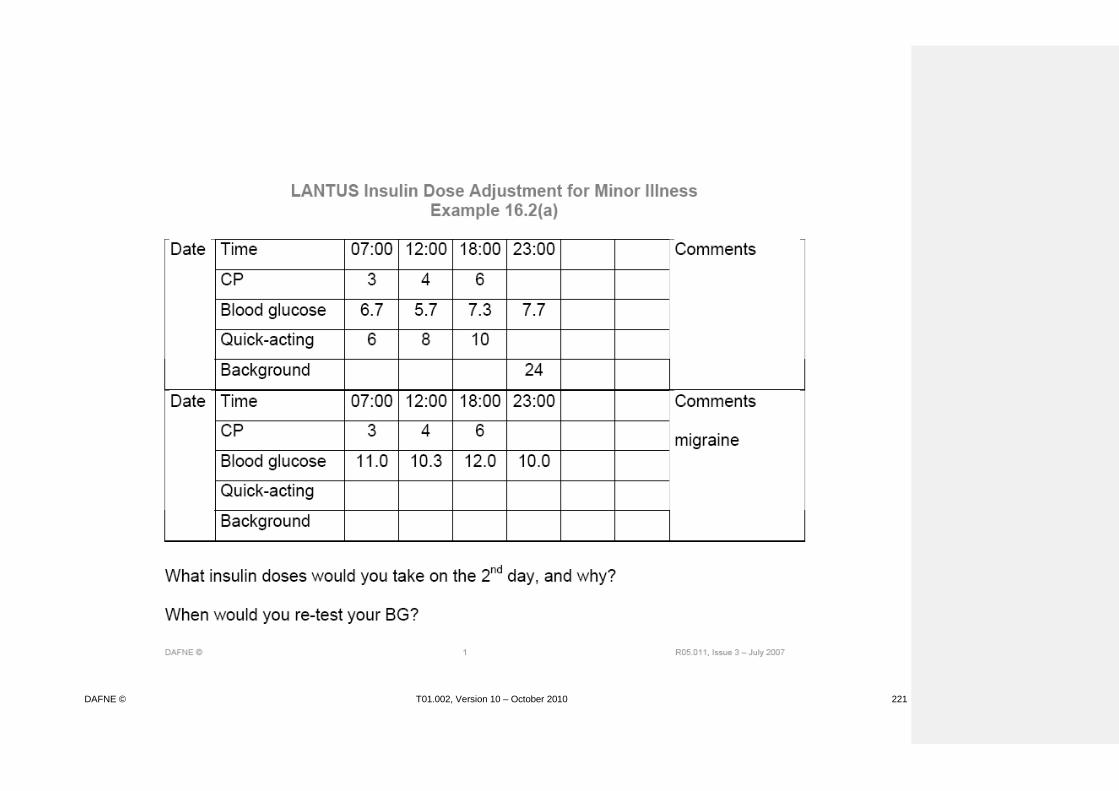
DAFNE © T01.002, Version 10 – October 2010 221
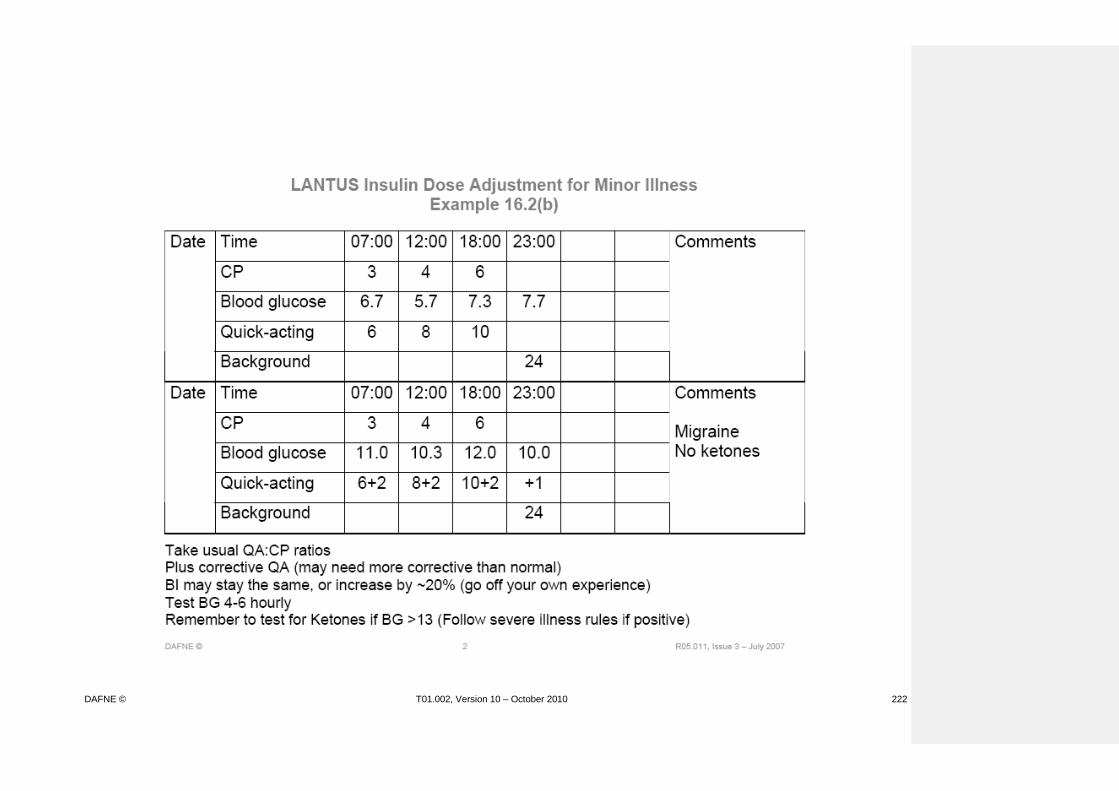
DAFNE © T01.002, Version 10 – October 2010 222

DAFNE © T01.002, Version 10 – October 2010 223

DAFNE © T01.002, Version 10 – October 2010 224

DAFNE © T01.002, Version 10 – October 2010 225
Workstation 2 Alcohol Scenarios (No 1)
What are the core messages about alcohol and DAFNE? When considering what action to take in relation to alcohol, what foods need to be considered? How would you categorise these drinks: Lager Whiskey Gin and tonic Bacardi breezer Cider Port Sherry White wine with soda Baileys Stout Champagne What are the core dose adjustment rules for carbohydrate and non carbohydrate containing drinks?

DAFNE © T01.002, Version 10 – October 2010 226
Workstation 2 Alcohol Scenarios (No 1)
Answers What are the core messages about alcohol and DAFNE? Alcohol can contribute to delayed hypoglycaemia and the key issue is that of safety and avoidance of severe hypos. Different types of alcohol have different effects on BG dependent on their CP and alcohol content and dose adjustment principles will vary according to this. DAFNE algorithms for alcohol are not rigorously scientifically tested and so need to be used with caution. When considering what action to take in relation to alcohol, what foods need to be considered? The type of alcohol (carbohydrate/alcoholic strength) The quantity The timing in relation to food Any additional snacks or meals Any physical activity Previous experiences How would you categorise these drinks: Lager Whiskey Gin and tonic Bacardi breezer Cider Port Sherry White wine with soda Baileys Stout Champagne (Those with and without carbohydrate: refer to handbook)

DAFNE © T01.002, Version 10 – October 2010 227
What are the core dose adjustment rules for carbohydrate and non carbohydrate containing drinks? Alcohol with no carbohydrate requires dose reduction of background insulin or/and extra CPs. Alcohol containing carbohydrate needs the above plus the addition of a dose of QA insulin (but not at the usual ratio.

DAFNE © T01.002, Version 10 – October 2010 228
Workstation 2 Alcohol and DAFNE (No 2)
For which of the following alcoholic drinks may you need to consider injecting QA insulin?
½ bottle of wine 5 bottles (330ml) of 5% bitter 4 small (120ml) glasses of red wine 1 pint of cider 3 gin and slimline tonics 4 Tia Maria and Diet Coke 1 liqueur coffee 5 pints of bitter How much QA might you suggest having? What factors would you consider when making this decision? Would you make any changes to BI?

DAFNE © T01.002, Version 10 – October 2010 229
Workstation 2 Alcohol and DAFNE (No 2)
Answers / Discussion Points
½ bottle of wine No, but 3-5 units of alcohol so may consider having CPs
before bed, depending on BGL 5 bottles (330ml) of 5% bitter = 3 pints of strong bitter Yes, 2u QA (4½ CPs) and as 6½ units of alcohol consider
dropping BI at bedtime (Isophane/Levemir) or having CPs (Lantus)
4 small (120ml) glasses of red wine No, but 6 units of alcohol so may consider having CPs
before bed depending on BGL 1 pint of cider No action required 3 gin and slimline tonics No action required as long as BGL within range – if doubles = 6 units alcohol have some CPs before bed or less BI 4 Tia Maria and Diet Coke Yes, 1u QA (2 CPs). 1 liqueur coffee Depends on amount of sugar added to coffee, but usually no action required 5 pints of bitter Yes, 2-3u QA (5 CPs) and as 10 units of alcohol drop BI at bedtime (isophane/Levemir) or have CPs (Lantus)

DAFNE © T01.002, Version 10 – October 2010 230
Workstation 2 Alcohol Scenarios (No 3)
1. Rosie is having a night out with friends.
She has her evening meal at 6pm and meets her friends in the pub at 7:30pm. In the pub she plans to drink 4 pints of standard lager. How should Rosie prepare for this night out?
2. Dave is going to a wedding. The service is at noon and the meal is arranged for 4pm. Prior to the meal, and whilst the photographs are being taken, champagne is served. Dave unexpectedly drinks 3 glasses of champagne before the meal. What should Dave do to ensure he does not hypo due to the
unexpected champagne? 3. Katie goes out clubbing with her boyfriend.
She drinks 5 alcopops and dances until 3am. What does she have to think about in order to avoid going hypo?

DAFNE © T01.002, Version 10 – October 2010 231
Workstation 3 DAFNE and Exercise
1. Helen goes shopping in town every Thursday morning and she usually
has a hypo mid-morning. Recently she has put on 2kg and she is keen to lose weight.
How could she deal with this problem?
a) Always stop for coffee and a cake mid-morning b) Reduce her BI by 10% on shopping days c) Reduce her QA at breakfast by 10-20% on shopping days d) Take some toffees to suck while she’s shopping 2. George has been asked to come to school on Monday evening to help
set up the hall for concerts that will start the next day. He will go after his evening meal and will be lifting and moving chairs and tables around for at least an hour.
How could he prepare for this?
3. Pete has recently taken up playing squash. His friend phones him
unexpectedly at 7.30pm to ask him to play a game. He has already had his evening meal and his QA at 6pm.
How could he handle this situation?
4. Liz is reasonably fit and has decided to start training for a 10k run. The
easiest time for her to fit in the running is first thing in the mornings before breakfast. Her fasting BGL is usually around 10-13mmol/l and it rises to 15-17mmol/l after the run; she doesn’t feel like she is running as well as usual. Her BGL is in range at bedtime and when she has tested during the night it is 5-6mmol/l.
How could she handle this problem?

DAFNE © T01.002, Version 10 – October 2010 232
5. Becky goes out to a club for the night with friends. They share a couple of bottles of wine – she has about 4 glasses. They dance for 2 hours. While she is out she has some crisps (about 2 CPs), but no QA insulin. As she goes to bed at 2am she tests her BGL and it is 10.8mmol/l.
What insulin should she take at bedtime?

DAFNE © T01.002, Version 10 – October 2010 233
Workstation 3 DAFNE and Exercise
Answers / Discussion Points
1. Reduce QA insulin at breakfast
Better to reduce insulin than eat more to help weight loss 2. Consider:
Reduce QA by 10-20% at evening meal
Reduce bedtime BI (10%) if a particularly strenuous session
If supper eaten, reduce QA by 20%
Remember hypo treatment 3. Can’t reduce QA as it is unplanned, so:
Pre-exercise BGL is likely to be raised post-prandially
Take 2-3 CPs before the game (think about type of CHO)
Consider additional CPs after the game if it is strenuous
Consider dropping bedtime BI by 10%, or have additional CPs (Lantus)
Remember hypo treatment 4. Likely that night-time BI not covering ‘Dawn Phenomenon’ (may be
less of an issue on Levemir or Lantus). Try:
Take additional 1u QA prior to exercise (possibly with 1 CP)
Reduce QA at next mealtime by 20%.
Remember hypo treatment
?consider reducing morning BI if it is a long run 5. Combination of exercise and alcohol!
Do not correct high BG at bedtime with QA insulin
Reduce bedtime BI by 20% or have additional CPs (Lantus)
If on bd BI, do not give next dose until after 9am, or reduce dose if this isn’t possible

DAFNE © T01.002, Version 10 – October 2010 234
Workstation 3 Physical Activity Scenarios
1. You plan to decorate all day (painting, wall papering). How would you plan to avoid hypos?
2. You decide to go swimming at 3:30pm for half an hour. Your blood glucose is 6.9 mmol/l. What should you do?
3. You are going to the gym for 1½ hours after work. You have not eaten since 12 noon and it is now 7:30pm. Your blood glucose is 13.5 mmol/l. What would you do before and after exercising to manage your blood sugars?
4. You have your evening meal at 6pm and plan to go cycling for an hour later on. What should you do?
5. Sunday afternoon you decide to mow the lawn. What would you do?
6. You are taking the dog out for a walk before breakfast for 20 minutes. Your blood glucose is 9.4 mmol/l. What do you do?
7. You help a friend move some furniture after tea. It takes 3 hours and turns out to be very strenuous. What would you do?
8. You plan to play badminton for 1½ hours after lunch. At lunchtime your blood glucose is 10.3 mmol/l. You have 6 CP's. Using your current ratio at lunch, how much insulin would you take?

DAFNE © T01.002, Version 10 – October 2010 235
Workstation 3 Physical Activity Scenarios Answers/discussion points
You plan to decorate all day (painting, wall papering). How would you plan to
avoid hypos? background + quick acting insulin at breakfast 30-50%, + quick acting at lunch by 30-50% +? at tea depending. You decide to go swimming at 3.30 pm for half an hour. Your blood glucose is 6.9 mmol/l. What would you do? Take 2-3 CPs depending how serious the activity - ? combination short + long. You are going to the gym for 1½ hours after work. You have not eaten since 12 noon and it is now 7.30 pm. Your blood glucose is 13.5 mmol/l. What would you do before and after exercising to manage your bg? Check for ketones if present, inject extra QA - ? 2 units. If not You have your evening meal at 6 pm and plan to go cycling for an hour later
on. What would you do? teatime actrapid by 30%. Sunday afternoon you decide to mow the lawn. What would you do? Check BS. ? eat CPs according to the level, or just carry hypo remedy. You are taking the dog out for a walk before breakfast for 20 minutes. Your blood glucose is 9.4. What do you do? Carry a hypo remedy. You help a friend move some furniture after tea. It takes 3 hours and turns out
to be very strenuous. What would you do? QA insulin at tea by 50% eat
extra CPs. background at night by 20%. You plan playing badminton for 1½ hours after lunch. At lunchtime your blood glucose is 10.3 mmol/l. You have 6 CPs. Using your current ratio at lunch how much insulin would you take? Based on a 1:1 ratio. 6 units for CPs = 6 +
1 corrective by 30-50%.
DAFNE © T01.002, Version 10 – October 2010 236
ANNUAL REVIEW LEARNING GOALS METHODS MATERIALS/MEDIA
Reflect on activities and methods used during the “Annual Review session. Become familiar with some suggested activities/scenarios that can be used for the Annual Review sessions. Share ideas of how to develop resources to support the delivery of the session. Practise, talk through and discuss new ideas for the delivery of this session.
What methods did you see used to deliver this session?
List and share.
Debate the pros and cons (what was helpful, what could have worked better?)
Model or discuss local (to DEP trainer) methods used to deliver this session. What other ideas might be suggested to deliver this session, that are in keeping with DAFNE philosophy and TPE. The group should use any remaining time to debate, discuss or work through or practise their ideas for delivering this session.
Annual Review curriculum Worksheet Local curriculum, lesson plans and resources for Annual Review sessions
DAFNE © T01.002, Version 10 – October 2010 237
WORKSTATION 4
Annual Review
What methods did you see used to deliver this session? List and share. Debate the pros and cons (what was helpful, what could have worked better?)
What other ideas might be suggested to deliver this session, which are in keeping with DAFNE philosophy and TPE? Use any remaining time to debate, discuss or work through or practise your ideas for delivering this session.
DAFNE © T01.002, Version 10 – October 2010 238
Use any remaining time to debate, discuss or work through or practise your ideas for delivering this session.
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA

DAFNE © T01.002, Version 10 – October 2010 239
Know the aim of the session is to discuss the educational theories that underpin DAFNE Know the 4 learning models that underpin DAFNE/TPE 1. Experiential learning model 2. Adult Learning Theory 3. Social Learning Theory
Introduction Explain - The aim of this session is to provide an opportunity to discuss the educational theories underpinning DAFNE. Ask group if they know the origins of the Düsseldorf Model. Discuss responses and explain Assal’s Therapeutic Patient Education (TPE) Model: Developed in Switzerland by a physician (Jean-Philippe Assal), who has diabetes himself. Several recognised theories are likely to have contributed to development of TPE: Experiential Learning Model (Kolb 1984) David Kolb (1984) sees learning as a core process of human development. Development results from learning that is gained through experience, and this is the basis of the ‘experiential learning model. Essentially experiential learning uses concrete experiences to inform decisions and actions, through a process of reflection and reformulation and retesting, people can learn and develop. This can be a very powerful tool in learning and is likely to be much more credible than any information given by a healthcare professional.
Acetate: “Therapeutic Patient Education” Acetate “Cycle of Experiential Learning”
DAFNE © T01.002, Version 10 – October 2010 240
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
There are four stages in this process: 1. Concrete experience. The person must immerse
themselves fully and openly in new experiences. 2. Reflective observation. The person must observe and
reflect on concrete experiences from a variety of perspectives.
3. Abstract conceptualisation. The person integrates their observations with and reformulates theories.
4. Active experimentation. The person must apply and retest these theories in decision-making and problem-solving. (cited in Quinn 3rd ed 1995)
This cycle repeats and repeats to allow for experimentation and learning. Examples of this on DAFNE – ask the group if they can recount any incidents of this during their DAFNE course Examples might include treating of hypos, trying sweet foods for the first time, eating a CHO free meal, testing out the algorithms for alcohol. Summary The DAFNE model allows for experiential learning by giving people a clear framework around CHO counting and insulin dose adjustment within which to experiment. Adult Learning Theory (Knowles 1990) Education systems for adults should be different to educational systems for children.
Acetate “Table of Adult Learning Theory”

DAFNE © T01.002, Version 10 – October 2010 241
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING
THEORIES
LEARNING GOALS METHODS MATERIALS/MEDIA
Traditional education (‘chalk and talk’) does not equip the learner with skills which are transferable in life long learning. Adult learning should promote self enquiry and autonomy. Ask the group to consider a positive learning experience they have had and compare it to an unhelpful learning experience. Ask them to list the qualities of the positive learning experience and of the unhelpful learning experience on post it notes. Collate post it notes onto flipchart paper and discuss. Now refer to the acetate ‘Table of Adult Learning Theory’ and reflect on key points that adult learning should be ‘learner centred’ and its core qualities will include:
Personal relevance
Active and task/problem based
Involved in the learning
Based on personal experiences
Self directed/self motivated Social Learning Theory (Bandura 1977) Social learning theory is to support people in becoming active self managers and includes helping people in terms of their self esteem and confidence.
Post it notes Flipchart Acetate “Social Learning diagram” Flipchart Pens Post-its
DAFNE © T01.002, Version 10 – October 2010 242
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
There are 4 core aspects to social learning theory: Mastery
This draws on peoples previous positive experiences and tries to transfer these skills to new situations
This will include building on small successes
Performing practical tasks that builds on personal skills Modelling/vicarious learning
This includes observing an appropriate role model, trying or testing something out
Learning from the suggestions of peers Emotional management
Coping with emotions/anxieties
Supporting individuals who show distress Action planning
Setting concrete plans
Developing specific strategies for situations or eventualities
In pairs, ask “can you think of an example during your observation week where social learning theory was evident?” Examples might include:
Mastery – asking people about their previous experiences as part of the lesson, congratulating people who make small change to their insulin, congratulating people who manage without a bedtime snack for the first time in 10 years.

DAFNE © T01.002, Version 10 – October 2010 243
THERAPEUTIC PATIENT EDUCATION and ADULT EDUCATION / LEARNING THEORIES LEARNING GOALS METHODS MATERIALS/MEDIA
Modelling/vicarious learning – seeing someone else try a small carton of fruit juice to treat a hypo, someone during the dose adjustment session suggesting someone should have a corrective dose before bed.
Emotional management – supporting individuals who are upset, acknowledging and reflecting on people’s anxieties around dose adjustment.
Action planning – recording the instructions for dose adjustment, in future goal setting.
Summary – The next session is around lesson planning, it would be worth you considering how you are going to provide opportunities for all of the above during the planning of your sessions.
Handout summarising the key learning theories

DAFNE © T01.002, Version 10 – October 2010 244
Therapeutic Patient Education
Enables patients to gain and maintain abilities for optimal
management of their diabetes
Provides information, practical learning and psychosocial support
Should help patients and their families to better co-operate with health care providers
Should be a continuous and systematic process integrated into the healthcare system
Jean-Philippe Assal et al, 2000. www.desg.org
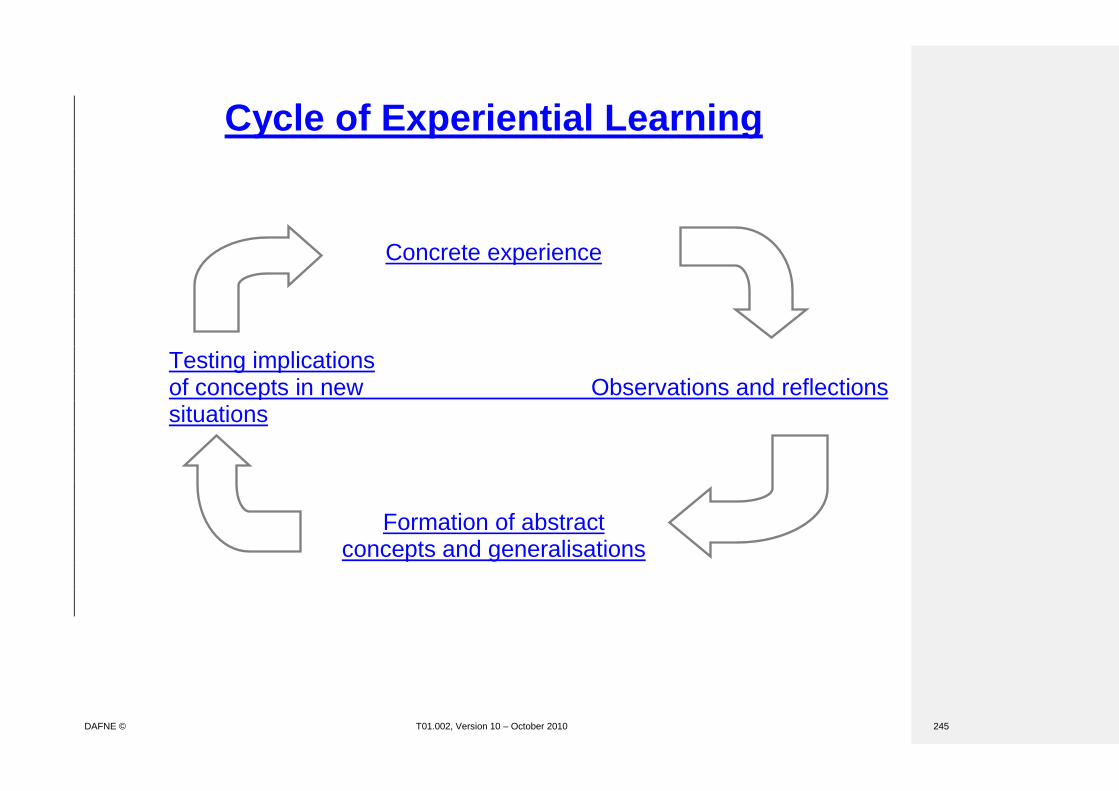
DAFNE © T01.002, Version 10 – October 2010 245
Cycle of Experiential Learning
Concrete experience
Testing implications of concepts in new Observations and reflections situations
Formation of abstract concepts and generalisations

DAFNE © T01.002, Version 10 – October 2010 246
Adult Learning Theory
Assumptions Pedagogy Andragogy
Learner’s need to know Children must learn what they are taught in order to pass their tests
Adults need to know why they must learn something
Learner’s self-concept Dependency: decisions about learning are controlled by their teacher
Self-direction: adults take responsibility for their own learning
Role of learner’s experience It is the teacher’s experience that is seen as important. The learner’s experience is seen as of little use as a learning resource
Adults have greater, and more varied experience which serves as a rich resource for learning
Learner’s readiness to learn Learner’s readiness is dependent upon what the teacher wants them to learn
Adult’s readiness relates to the things he or she needs to know and do in real life
Person’s orientation to learning Learning equates with the subject-matter content of the curriculum
Adults have a life-centred orientation to learning involving problem-solving and task-centred approaches
Student’s motivation The child’s motivation is from external sources such as teacher approval, grades and parental pressures
Adult’s motivation is largely internal such as self-esteem, quality of life and job satisfaction

DAFNE © T01.002, Version 10 – October 2010 247
Social Learning Theory
Observation
Environment

DAFNE © T01.002, Version 10 – October 2010 248
Therapeutic Patient Education An overview of educational theories underpinning DAFNE
1. Therapeutic Patient Education (Jean-Philippe Assal 2000 www.desg.org)
Enables people to gain and maintain abilities for optimal management of their diabetes
Provides information, practical learning and psychological support.
Should help people to co-operate with health care providers
Should be a continuous and systematic process integrated into the healthcare system 2. Experiential Learning model (Kolb 1984) Essentially experiential learning uses concrete experiences to inform decisions and actions,
through a process of reflection and reformulation and retesting, people can learn and develop.
This can be a very powerful tool in learning and is likely to be much more credible than any
information given by a healthcare professional. Development results from learning that is gained through experience. Four stages:
Concrete experience-the person must engage fully and openly in new experiences
Reflective observation-the person must observe and reflect on their experiences from different perspectives
Abstract conceptualisation-the person thinks about how their observations could be applied to their own lives and develops a theory or plan
Active experimentation-the person applies their theory or plan to test it out This is a repetitive cycle of experimentation and learning. 3. Adult learning theory (Knowles 1990) See table. Education systems should be different for adults and children. Adult learning should be learner centred:
Personally relevant-what the person needs to know and do in their lives
Active, task and problem based
The person is involved in the learning-they can influence what is covered and take responsibility for their own learning
Based on personal experience
Self directed and self motivated
4. Social learning theory (Bandura 1977) Supports people to self manage, looks at self esteem and confidence Four key aspects
Mastery-draws on previous positive experience. Builds on small successes, develop personal skills through performing small practical tasks.
Modelling/vicarious learning-observing others, trying and testing things out, learning from the actions and suggestions of peers.
Emotional management-coping with emotions and anxieties, being supported.
Action planning-making concrete plans, developing strategies
DAFNE © T01.002, Version 10 – October 2010 249

DAFNE © T01.002, Version 10 – October 2010 250
INTRODUCTION TO GOAL SETTING AND ACTION PLANNING LEARNING GOALS METHODS MATERIALS/MEDIA
Understand why and how goal setting is part of the has been introduced in DAFNE curriculum and workbook To consider what it is we are trying to achieve by using goal setting and action planning Be able to identify DAFNE related long term goals Be able to identify specific DAFNE behaviours
Introduction Goal setting is now part of DAFNE curriculum and has been introduced to ensure we continue to meet NICE criteria. Educators have only just been trained (Autumn 2006), therefore you have observed first courses incorporating goal setting. “What is it we are trying to help people achieve using goal setting and action planning?”
Getting people to think about their future and their long term goal for their diabetes.
Getting people to think about this as being about a process of small steps (mini goals and action plans).
Reflecting that DAFNE is the beginning of this journey.
Ultimately setting behaviour based action plans that increase the likelihood of them implementing their intentions and that are focused on their long-term goals.
Ask participants “Where in course did you observe goal setting taking place?” Pairs/small group work What were the goals? (that participants wanted to achieve). What were the specific behaviours identified to enable participants to achieve their goals? Room continuum exercise Ask four volunteers from the group to stand against a wall at one end of the room facing another wall.
Flipchart and pens

DAFNE © T01.002, Version 10 – October 2010 251
GOAL SETTING AND ACTION PLANNING LEARNING GOALS METHODS MATERIALS/MEDIA
To develop and overview of short term action planning, short and long term goals and how they fit together
Ask each person to think of a personal goal that they might set for themselves in the future (6 months – 1 year). Using the room continuum exercise to model the overall process of goal setting. Breaking it down into What is their long term goal for the future and how important is it for them and how will they know when they’ve got there? Facilitator lists on flipchart Note: It is important that you record the individuals own words not your interpretation of what they have said. Ask them to take one step forward – what is that first step? This is their first mini goal. Ask them to list what it is they need to do in order to achieve their mini goal? – This is their first action plan. Facilitator lists on flipchart. The facilitator then reflects back the action plan and asks questions like:
When you do this how long will it take?
What’s going to stop you from doing it?
How confident are they? Note to educator ensure that they identify?
Specific behaviour
When will they do it
How will they know when they have achieved their goal
How will they keep it going
Is it realistic for them

DAFNE © T01.002, Version 10 – October 2010 252
GOAL SETTING AND ACTION PLANNING LEARNING GOALS METHODS MATERIALS/MEDIA
Understand the process of goal setting for a DAFNE participant Reflect on the key component of action planning and so the competencies of educators
Repeat the mini goal setting and steps using one or two of the four individuals until their long term goal is reached and they get to the opposite wall. In groups of 4, using DAFNE case study, state:
long term goals
one priority goal
what behaviour they focused on
what barriers existed
strategies to overcome barriers Share 1-2 examples. Discuss any issues that arise. If time: Ask the group to spend 5 minutes in pairs considering the key components or skills for educators in this process (what are you doing as an educator). Emphasise you are asking questions to get them to explore their goals and action plans but you are not telling them what to do. Discuss the key components/competencies
eliciting goal setting(long-term)
facilitating identification of the short term goals (series of steps)
exploring the options in terns of behaviours
checking out action plans in terms of being behaviour based/SMART
exploring barriers
checking out confidence and importance

DAFNE © T01.002, Version 10 – October 2010 253
GOAL SETTING AND ACTION PLANNING LEARNING GOALS METHODS MATERIALS/MEDIA
To observe a demonstration of Action Planning session To practice and discuss how they will deliver the curriculum and use the DAFNE workbook.
using reflections, open/probing questions and encouraging problem solving
summary and discussion The two trainers then demonstrate how to fill in the final action plan using the example from the trainers day, with one trainer taking the role of the educator recording on the wipe clean resource and the other trainer taking the role of the patient; using the following example. In pairs practice completing the goal setting and action planning section of the workbookaction plan using their case study from a DAFNE course they have observed. Take turns at being the educator/DAFNE participant. Summary Final thoughts on goal setting/action planning. As a new addition to curriculum this will be reviewed via educator feedback and evaluation forms. If this is a very new skill for individuals, consider accessing local course(s) on, for eg behaviour change.
Goal setting wipe board My Plan booklet (reference) Resource for trainer of worked completed action plan

DAFNE © T01.002, Version 10 – October 2010 254
DAFNE Educator Programme (DEP)
Training Workshop
Day 3
09:00 Managing Groups Tips/scenarios for discussion 10.00 Preparation for peer reviewed course: Your expectations ‘Our’ expectations Role of the DEP Reviewer (who’s yours?) Review documentation
11:15 TEA / COFFEE
11.30 Recruitment strategies 12:00 Pre-course appointment / data collection: Getting some practise
12.45 LUNCH
13.30 Follow up and support for DAFNE ‘graduates’ 14.00 Catering arrangements and DAFNE resources 14:45 Delivering DAFNE locally – Personal Plan 15:15 Summary / feedback / evaluation 15:45 Depart
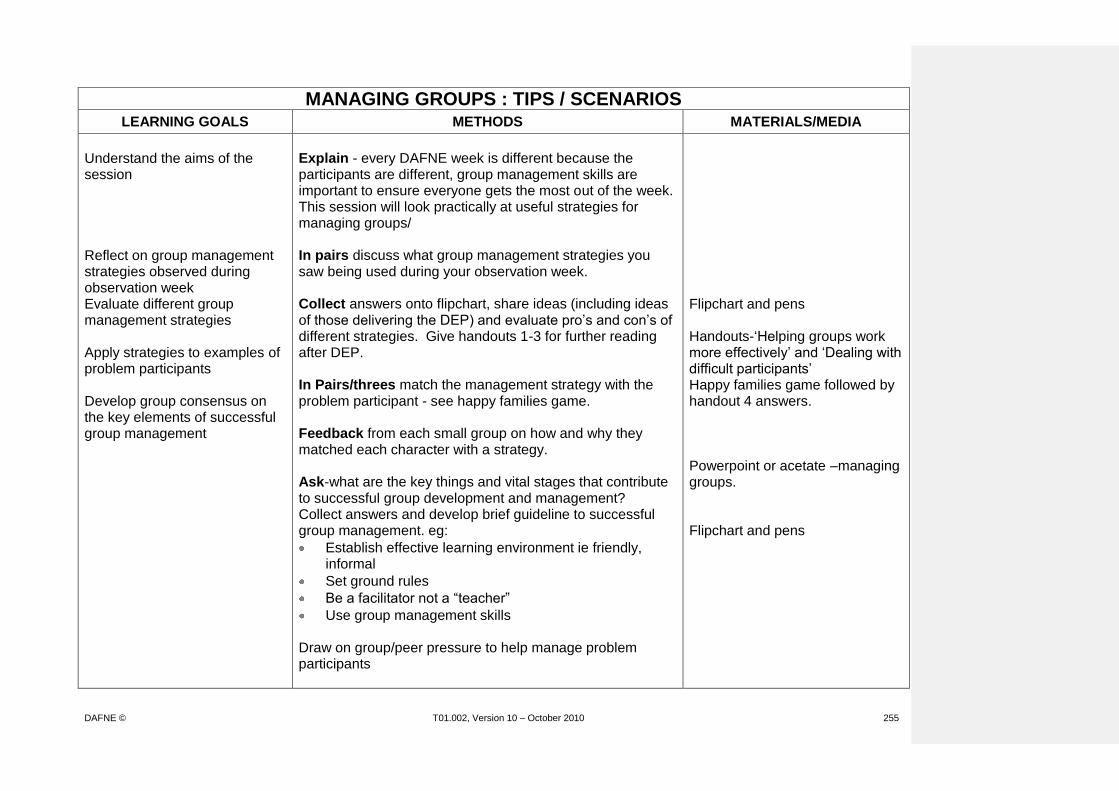
DAFNE © T01.002, Version 10 – October 2010 255
MANAGING GROUPS : TIPS / SCENARIOS LEARNING GOALS METHODS MATERIALS/MEDIA
Understand the aims of the session Reflect on group management strategies observed during observation week Evaluate different group management strategies Apply strategies to examples of problem participants Develop group consensus on the key elements of successful group management
Explain - every DAFNE week is different because the participants are different, group management skills are important to ensure everyone gets the most out of the week. This session will look practically at useful strategies for managing groups/ In pairs discuss what group management strategies you saw being used during your observation week. Collect answers onto flipchart, share ideas (including ideas of those delivering the DEP) and evaluate pro’s and con’s of different strategies. Give handouts 1-3 for further reading after DEP. In Pairs/threes match the management strategy with the problem participant - see happy families game. Feedback from each small group on how and why they matched each character with a strategy. Ask-what are the key things and vital stages that contribute to successful group development and management? Collect answers and develop brief guideline to successful group management. eg:
Establish effective learning environment ie friendly, informal
Set ground rules
Be a facilitator not a “teacher”
Use group management skills Draw on group/peer pressure to help manage problem participants
Flipchart and pens Handouts-‘Helping groups work more effectively’ and ‘Dealing with difficult participants’ Happy families game followed by handout 4 answers. Powerpoint or acetate –managing groups. Flipchart and pens

DAFNE © T01.002, Version 10 – October 2010 256
MANAGING GROUPS : TIPS / SCENARIOS LEARNING GOALS METHODS MATERIALS/MEDIA
Apply group management strategies to scenarios
Activity: In pairs draw scenarios from a hat and discuss how they would use group management skills discussed previously to control the DAFNE situation. Feedback to whole group for discussion and evaluation.
Pre-prepared group management scenarios.
DAFNE © T01.002, Version 10 – October 2010 257
Strategies For Effective Group Processes
Use Ground Rules
• Grounds rules are guidelines for interaction – “norms”
• Encourage positive functional behaviors
• Solicit guidelines from the group itself – don’t impose
• POST the guidelines and refer to as needed
• Include additional norms on an ongoing basis as needed

DAFNE © T01.002, Version 10 – October 2010 258
Strategies For Effective Group Processes
Become a Facilitator• Manage interaction and participation that helps groups
become more effective
• Choose appropriate instructional methods and
techniques
• Help the group
– Define goals and objectives
– Create an open climate
– Facilitate problem solving
– Evaluate results

DAFNE © T01.002, Version 10 – October 2010 259
Helping Groups Work More Effectively – Handout 1 Groups are effective when they pay attention to both what they are doing (the task at hand) and how they are doing it (processes used to maintain an effective group). Many groups focus mainly on the task and ignore the process. As a result, effectiveness at achieving the group's goals is lowered. If one uses a car as an analogy, the task might be defined as providing transportation for someone in order to get from point A to point B. Any driver could do this (well, most drivers anyway) as long as the car functions properly. If, however, the auto's inner workings are not maintained -- oil and gas added, brakes checked, water pressure examined -- the car may have some trouble reaching its destination, not reach it at all, or it may in fact arrive, but only with serious damage to its internal mechanisms. The exact same phenomenon is true for groups. If maintenance functions are minimal, the results could be graphic. The group may not perform well, flounder and find itself irreparably split. Or, the results may be more subtle - a lack of group cooperation, some resources may remain untapped, a weak product is generated, a feeling may emerge that time has been wasted. One other harmful impact sometimes results when ineffective group maintenance produces conflict which is assumed to be related to the actual task. For example, an individual may disagree with someone else in the group because he/she has been unable to enter the discussion. The disagreement may have nothing to do with the task itself. This can often take the group off in irrelevant directions. There are specific functions that a group can perform which will increase the group's effectiveness. They are grouped into two categories of MAINTENANCE FUNCTIONS and TASK FUNCTIONS. The assumption is not that any given group will have all of these functions happening at the same time, but that a productive group will have a healthy and conscious mix of functions at appropriate times.
Group Task Functions Initiating: Getting the group started on the task. Offering new suggestions, topics for discussion, plans, etc. Clarifying: Probing for meaning; defining terms, clearing up confusion, working to get the task clear. Asking a question or repeating a point, in different words to make it clear to all. Explaining: Giving practical examples to make a point clear. Reaching Task Agreement: Discussing and deciding the best way to proceed with the task given the time constraints; agreeing on time/task management process. Focusing: Staying on target; avoiding topic jumping or going off on tangents. Seeking Useful Information: Asking for facts, opinions or beliefs; asking for feelings or values. Drawing out resources of the group and identifying information that needs to be found elsewhere.

DAFNE © T01.002, Version 10 – October 2010 260
Giving Useful Information: Offering facts or opinions; stating beliefs or ideas; making feelings known appropriately; making suggestions, sharing relevant experiences. Summarising: Stating briefly the main points made so far. Checking Consensus: Seeing if everyone, especially the silent members agree on a point. Moving Towards Action: Reviewing; bringing related ideas together; restating - suggestions and positions; checking if group is ready to decide, suggesting a process for decision making.
Group Maintenance Functions Gate Keeping: Inviting others to talk; suggesting time limits or other procedures to permit wide participation; keeping talk flowing; avoiding domination by one person. Mediating: Harmonizing; conciliating differences in points of view, suggesting compromises; disagreeing comfortably. Listening: Going along with the group; being a good listener; demonstrating that other's statements are heard; avoiding inappropriate interruptions. Diagnosing Difficulties: Addressing lack of information needed in order to make a decision or the fear of consequences of a decision that is blocking the group from reaching one. Harmonising: Helping those in conflict to understand one another’s views. Evaluating: Creating an opportunity for people to express feelings and reactions towards the working of the group. Encouraging: Being friendly, warm, responsive through words or facial expressions; being supportive even when disagreeing, building on suggestions made by others, showing acceptance and appreciation of others and their ideas. Relieving Tension: Using humor; throwing oil on troubled waters; asking for a "cooling-off" period, making a well timed joke, bringing problem out into the open.

DAFNE © T01.002, Version 10 – October 2010 261
10 Interventions for Regaining Control of the Group – Handout 2
Using active-training techniques tends to minimize the problems that often plague trainers who rely too heavily on lecture and full-group discussion. Nonetheless, difficulties such as monopolizing, distracting, and withdrawal still may occur. Below are interventions you can use; some work well with individual participants while others work with the entire group. 1. Signal nonverbaIly. Make eye contact with or move closer to participant when they
hold private conversations, start to fall asleep, or hide from participation. Press your fingers together to signal for a wordy participant to finish what he or she is saying. Make a "T" (for time out) sign with your fingers to stop unwanted behavior.
2. Listen actively. When participants monopolize discussion, go off on a tangent, or
argue with you, interject with a summary of their views and then ask others to speak. Or acknowledge the value of their viewpoints and invite them to discuss their views with you during a break.
3. Encourage new volunteers. When a few participants repeatedly speak in class
while others hold back, pose a question or problem and then ask how many people have a response to it. You should see new hands go up. Call on one of them. The same technique might work when trying to obtain volunteers for role playing.
4. Invoke participation rules. From time to time, tell participants that you would like to
use rules such as the following: a. No one may laugh during a role play. b. Only participants who have not yet spoken can participate. c. Each new comment must build on a previous idea. d. Speak for yourself, not for others.
5. Use good-natured humor. One way to deflect difficult behavior is to use humor. Be
careful, however, not to be sarcastic or patronizing. Gently protest the inappropriate behavior ("Enough, enough for one day!") or humorously put yourself down instead of the participant (“I guess I'm being stubborn, but...").
6. Connect on a personal level. Even if the problem participants are hostile or
withdrawn, make a point of getting to know them during breaks or lunch. It is unlikely that people will continue to give you a hard time or remain distant if you have taken an interest in them.
7. Change the method of participation. Sometimes, you can control the damage done
by difficult participant by inserting new formats, such as using pairs or smaIl groups rather than full-class activities.
8. Ignore mildly negative behaviors. Try to pay little or no attention to behaviors that
are small nuisances. These behaviors may disappear if you simply continue the session.
DAFNE © T01.002, Version 10 – October 2010 262
9. Discuss very negative behaviors in private. You must call a stop to behaviors that you find detrimental to the training session. Arrange a break and firmly request, in private, a change in behavior of those participants who are disruptive. Or create small-group activities and call aside the problem participants. If the entire group is involved, stop the session and explain clearly what you need from participants to conduct the training effectively.
10. Do not take personally the difficulties you encounter. Remember that many
problem behaviors have nothing to do with you. Instead, they are due to personal fears and needs or displaced anger. Try to determine if this is the case and ask whether participants can put aside the conditions affecting their positive involvement in the training session.
Reproduced from 101 Ways To Make Training Active by M. Silberman. Copyright 1995 by Pfeiffer and Company, San Diego, CA
DAFNE © T01.002, Version 10 – October 2010 263
Dealing with Difficult Participants – Handout 3 by Robert W. Pike, CSP
We all have them from time to time, but no one spends much time in a train-the-trainer session talking about how to handle them.
Over the years I've done research with my participants asking them to identify the most common types of difficult participants. I ended up with fifteen that came up more than all the others. Among them are the know-it-all, the latecomer, the shy, the sceptic, the dominator, etc. For each we identified from 6 to 15 strategies that could be used to help deal with that person.
We also identified some strategies that could prevent difficult participants from surfacing at all. Here are some of the key thoughts from our book, Dealing with Difficult Participants, by Bob Pike and Dave Arch.
1. There are two goals in dealing with a difficult participant: a. to get them on board b. to minimize their impact on others
2. Whenever possible use small groups of 5-7 for your preferred seating arrangement. Five is large enough for the group to have power enough to moderate most difficult behaviour. Seven is small enough to insure that people (even the shy) will have an opportunity to participate.
3. Divide your content into 20 minute blocks (for maximum retention) and seek to involve participants some way every 8 minutes. Involvement might be discussing something with a partner, doing something as a group, creating a flip chart that is posted on the wall, reflecting on the content and coming up with action ideas, etc.
4. For activities that involve the small groups always have a group leader.
5. Have a variety of ways to choose group leaders and rotate the leadership. Some methods for choosing group leaders include: the seven people in the group point a finger in the air; on the count of three they point at the person they want to lead; the person with the most fingers pointed at them leads, the person with the most (or least ) experience in the subject, the person with the most (or least) years with the organization, the person with the most (or least) letters in the first name as printed on their name tag or tent, etc.
6. Start with a value-added activity five minutes before the scheduled starting time. This activity should be done in small groups with people encouraging others that arrive to quickly join the group so that they can help. You can choose to let this run a couple of minutes into the formal class time. This will help people begin to understand that despite corporate norms or personal habits your sessions start and end on time and you expect to respect their time.
DAFNE © T01.002, Version 10 – October 2010 264
Hesitant Hanna: Shy reluctant, silent most of the time, easy to overlook, melts into the background
Arguing Arthur - the voice of experience: Constantly looking for opportunities to disagree or to show others up, can be annoying and disruptive

DAFNE © T01.002, Version 10 – October 2010 265
Monopolizing Mike: Big talker gobbles up all the discussion time if allowed
Not-listening Norma: Tends to interrupt, cut off and leap into the fray before others have had their say, can be because she is too eager and wants to advance her ideas
DAFNE © T01.002, Version 10 – October 2010 266
Rigid Roberta: Not obnoxious-but staunchly takes a stand on an issue and rarely moves
Angry Arnie: Behaviour ranges from total silence to constant complaining he’s mad at the world and nothing is right

DAFNE © T01.002, Version 10 – October 2010 267
Charlie the clown. Doesn’t take anything seriously, life’s a joke
Complaining Chester: Blames, faults gripes shares endless pet peeves

DAFNE © T01.002, Version 10 – October 2010 268
Show off Sandra: Parades knowledge-big words name dropping
Idea Stealing Ida: A master at putting down other peoples ideas, offers an endless barrage of suggestions to anything new or different-it’ll never work: we’ve tried it before. This is dangerous because it may inhibit others creativity.

DAFNE © T01.002, Version 10 – October 2010 269
Tangent Tony: Constantly talks about topics that are not relevant to the session. Repeatedly discusses individual issues which are not relevant to the session or other group members.
Unwilling Ursula: Neither a volunteer nor a willing attendee-nurse sent her!
DAFNE © T01.002, Version 10 – October 2010 270
Negative Nellie: Down about everything, nothing will work for her, she can’t do it.

DAFNE © T01.002, Version 10 – October 2010 271
Management: Must figure out ways to draw her out, Smaller groups, pair work, ask easy questions that relate to their experiences, socialise with them at breaks, offer encouragement. Management: Let him know you appreciate his input but on a more selective basis. We haven’t heard from….yet, can we discuss that further at the break, rely on peer pressure, do not put them down! Use a rationing technique. Management: Let the group deal with them-anyone want to respond to that? Say ok I understand your position, can we agree to disagree. Remember no trainer ever wins an argument with a participant! (they will side together in the end!) Management: Insist on sharing the discussion time, ask them to restate what someone else has said to help them listen. Ask for a comparative analysis-how does your idea compare with John’s? Help them to see to incorporate others views. Refer to ground rules. Offer them a toffee! Management: Rescue the idea-ask what the rest of the group think about the idea. Ask them to come up with and idea of their own in lieu of the one they just trashed. Ask the group to come up with possibilities. Refer to ground rules. Management: Force them to problem solve-ask for solutions. Encourage exploration of the other side of the argument. Say “You have identified everything that’s bad, perhaps that makes you the ideal person to tell us one good thing about it?” Management: Get them to admit there is another side of the story and acknowledge their points loudly (even on a flipchart). Management: Try to eliminate threats, ensure the environment is friendly, and consider a role play to let them vent in a positive manner, individual conference, refer to ground rules, consider clinical psychology referral.

DAFNE © T01.002, Version 10 – October 2010 272
Management: Ask them for a positive comment, just listen, ignore at times. Management: Deal with if hindering the group’s progress. Compliment them for worthwhile serious contributions, do not reinforce humour attempts, ask to rephrase- I’m sorry I didn’t get your point…… Management: Stifle them, give them a recording job, wait for peer pressure. Management: Ignore, defer until a later more appropriate time, canvas the group for agreement to move on of defer until later. Ask to discuss their issues later/individually. Explain why it is necessary to stick with the timetable. Refer to ground rule if relevant. Management: Acknowledge, you are here under duress! But you still have a choice as to how much you get out of this now that you are here. Work through/highlight what might be most appropriate for them. Make sure the sessions are not dull or boring. Find out what interests them and relate to their experiences.
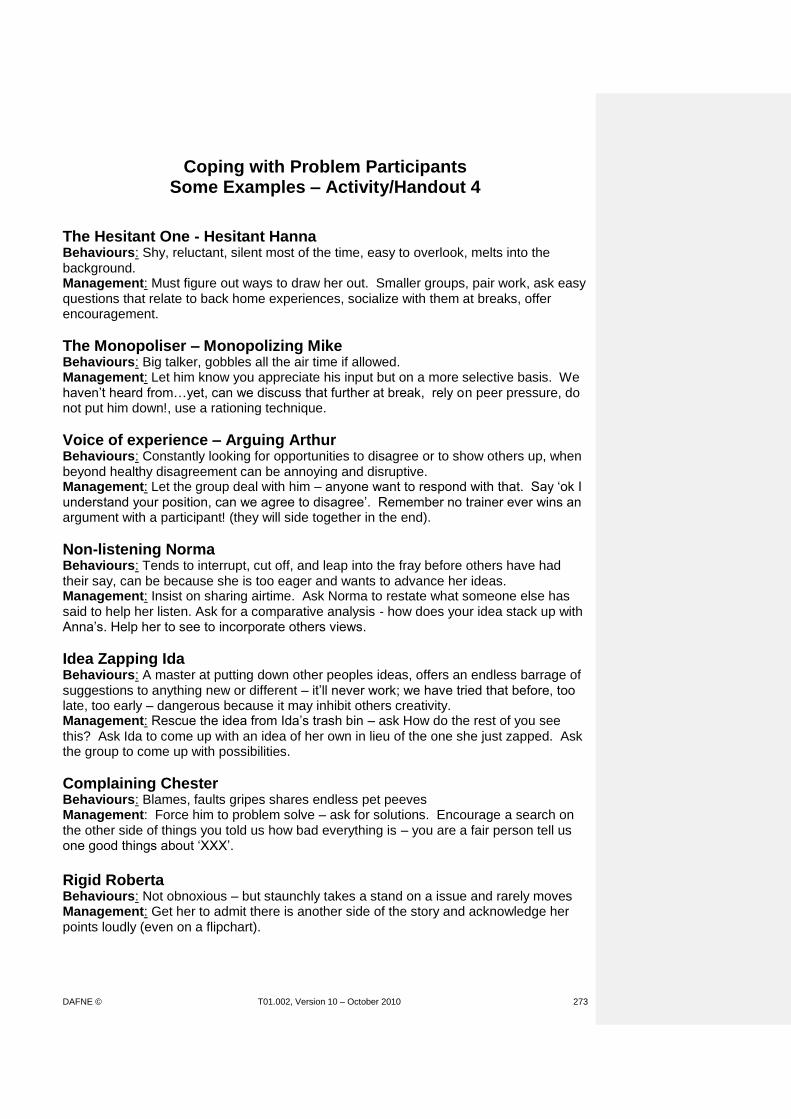
DAFNE © T01.002, Version 10 – October 2010 273
Coping with Problem Participants Some Examples – Activity/Handout 4
The Hesitant One - Hesitant Hanna Behaviours: Shy, reluctant, silent most of the time, easy to overlook, melts into the background. Management: Must figure out ways to draw her out. Smaller groups, pair work, ask easy questions that relate to back home experiences, socialize with them at breaks, offer encouragement.
The Monopoliser – Monopolizing Mike Behaviours: Big talker, gobbles all the air time if allowed. Management: Let him know you appreciate his input but on a more selective basis. We haven’t heard from…yet, can we discuss that further at break, rely on peer pressure, do not put him down!, use a rationing technique.
Voice of experience – Arguing Arthur Behaviours: Constantly looking for opportunities to disagree or to show others up, when beyond healthy disagreement can be annoying and disruptive. Management: Let the group deal with him – anyone want to respond with that. Say ‘ok I understand your position, can we agree to disagree’. Remember no trainer ever wins an argument with a participant! (they will side together in the end).
Non-listening Norma Behaviours: Tends to interrupt, cut off, and leap into the fray before others have had their say, can be because she is too eager and wants to advance her ideas. Management: Insist on sharing airtime. Ask Norma to restate what someone else has said to help her listen. Ask for a comparative analysis - how does your idea stack up with Anna’s. Help her to see to incorporate others views.
Idea Zapping Ida Behaviours: A master at putting down other peoples ideas, offers an endless barrage of suggestions to anything new or different – it’ll never work; we have tried that before, too late, too early – dangerous because it may inhibit others creativity. Management: Rescue the idea from Ida’s trash bin – ask How do the rest of you see this? Ask Ida to come up with an idea of her own in lieu of the one she just zapped. Ask the group to come up with possibilities.
Complaining Chester Behaviours: Blames, faults gripes shares endless pet peeves Management: Force him to problem solve – ask for solutions. Encourage a search on the other side of things you told us how bad everything is – you are a fair person tell us one good things about ‘XXX’.
Rigid Roberta Behaviours: Not obnoxious – but staunchly takes a stand on a issue and rarely moves Management: Get her to admit there is another side of the story and acknowledge her points loudly (even on a flipchart).

DAFNE © T01.002, Version 10 – October 2010 274
Hostile Harry Management: Best to keep you cool, rephrase in milder terms, get the group to respond to him.
Angry Arnie Behaviours: Behaviour ranges from total silence to constant complaining, he is mad at the world, nothing is right. Management: Try to eliminate threats, ensure the environment is friendly, and consider a role play to let him vent in a positive manner, individual conference, recommend to his company removal and/or professional help.
Negative Nellie Management: Ask her for something positive, just listen, ignore at times
Charlie the Clown Management: Deal with if hindering the group progress. Compliment him for worthwhile serious contributions, do not reinforce humour attempts, ask for rephrasement – I am sorry I did not get your point…
Show Off Sandra Behaviours: Parades knowledge –big words, name dropping. Management: Stifle her, give her a recording job, wait for peer pressure.
Tangent Tanya Management: Ignore, defer until a later more appropriate time, canvas the group for agreement, individual counselling – explaining why it is necessary to stick with the program.
The Unwilling Participant Behaviours: Those who are neither volunteers nor willing attendees. Boss sent them Management: Acknowledge, you are here against your will but you still have a choice – you can stonewall the program or get the most out of it while you are here; work through what might be most appropriate for participant, make certain training is not dull or boring, provide just in time training, stress what is in it for me; introduce job relevant situations.

DAFNE © T01.002, Version 10 – October 2010 275
On the second day of the course one of the group says they won’t be coming back as they don’t feel this treatment regime is suitable for them. Suggest possible ways to handle this. One of the participants breaks down during the ‘complications’ session and leaves the room in tears. How would you deal with this without disrupting the rest of the group? A participant is clearly over-confident with CP estimation and consistently underestimates CP values of meals. What could you do to begin to resolve this?
One of the participants has an HbA1c of 11.8%, they are very concerned about weight gain and express this concern during one of the discussions.
Suggest ways of dealing with this.
One of the participants is very dominant and constantly interrupts you during sessions.
How could you deal with this?
A participant discusses their alcohol intake; it is far in excess of healthy normal limits and they often binge-drink at weekends.
How could you deal with this?

DAFNE © T01.002, Version 10 – October 2010 276
A participant asks if they could arrive late and leave early for the duration of the course due to family commitments.
How would you deal with this? One of the participants has changed from a bd mixture to DAFNE regime and they are disappointed that their BG levels are higher than they have experienced before. How would you help them? One of the participants feels that the other group members are making fun of them and they mention this to you at coffee break. How would you deal with this?

DAFNE © T01.002, Version 10 – October 2010 277
PREPARATION FOR PEER-REVIEW 60 min LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Explain after this 3-day workshop the next stage of your DAFNE training is to teach a DAFNE course which will be peer reviewed. Question in pairs, make a list of your concerns and questions about peer review. Write each individual comment on a separate post it note and pin these to a blank flipchart at the front. The educator then themes these questions and gradually through the session deals with all of the issues.
Understand the purpose of peer-review
Why is peer review important? Educator discusses importance of peer review to DAFNE. Discuss responses as appropriate. Purpose of peer review:
Be able to demonstrate an understanding and application of the DAFNE core principles and adult education methods
Be able to demonstrate competence to run DAFNE courses independently in their own service
Have agreed areas for ongoing professional development and improvement of the programme to ensure continued quality assurance of DAFNE
Go on to successfully complete step 6 of the DEP and have their name entered on a register of DAFNE educators.
Explain the importance of Quality Assurance and how the model is based on that in Germany (Fulda). Who are the reviewers? Refer to list provided by Central DAFNE
Acetate: ‘DoH Structured Education Criteria’ Acetate – ‘Who are the Reviewers?’
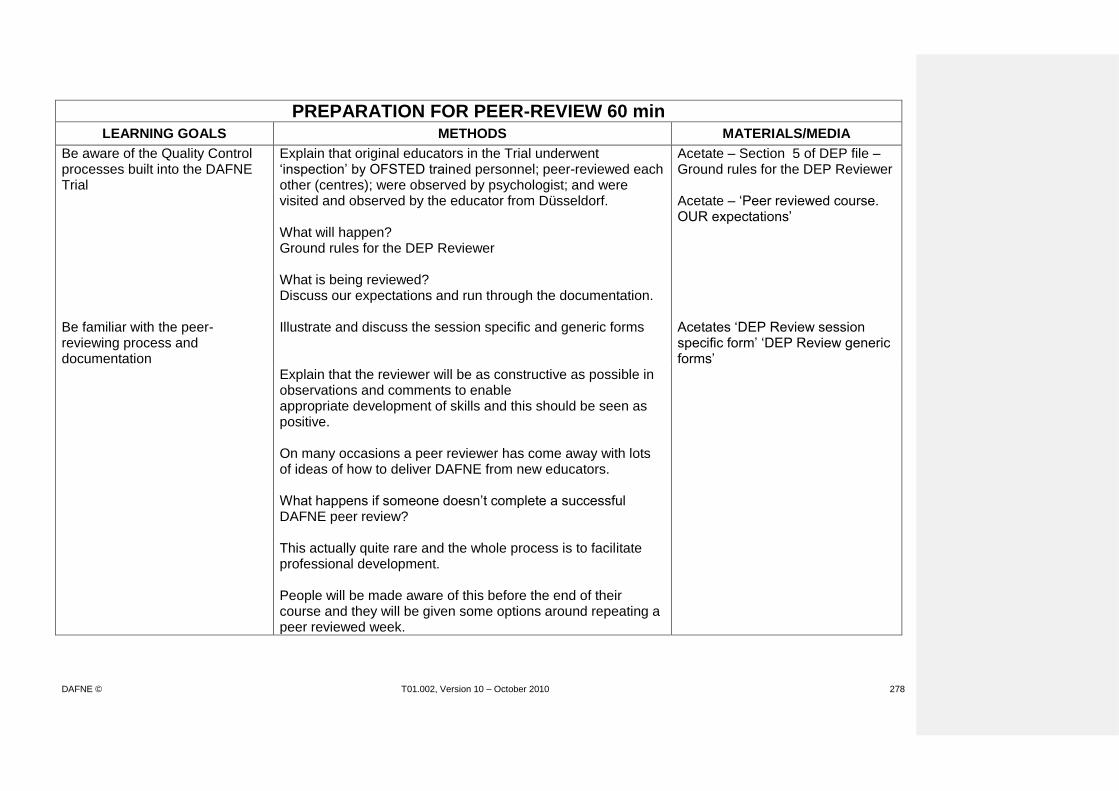
DAFNE © T01.002, Version 10 – October 2010 278
PREPARATION FOR PEER-REVIEW 60 min LEARNING GOALS METHODS MATERIALS/MEDIA
Be aware of the Quality Control processes built into the DAFNE Trial
Explain that original educators in the Trial underwent ‘inspection’ by OFSTED trained personnel; peer-reviewed each other (centres); were observed by psychologist; and were visited and observed by the educator from Düsseldorf. What will happen? Ground rules for the DEP Reviewer What is being reviewed? Discuss our expectations and run through the documentation.
Acetate – Section 5 of DEP file – Ground rules for the DEP Reviewer Acetate – ‘Peer reviewed course. OUR expectations’
Be familiar with the peer-reviewing process and documentation
Illustrate and discuss the session specific and generic forms
Acetates ‘DEP Review session specific form’ ‘DEP Review generic forms’
Explain that the reviewer will be as constructive as possible in observations and comments to enable appropriate development of skills and this should be seen as positive. On many occasions a peer reviewer has come away with lots of ideas of how to deliver DAFNE from new educators. What happens if someone doesn’t complete a successful DAFNE peer review? This actually quite rare and the whole process is to facilitate professional development. People will be made aware of this before the end of their course and they will be given some options around repeating a peer reviewed week.

DAFNE © T01.002, Version 10 – October 2010 279
PREPARATION FOR PEER-REVIEW 60 min LEARNING GOALS METHODS MATERIALS/MEDIA
Understand that trainers and reviewers also had to ‘start somewhere’, and can help them empathetically to develop their confidence and skills
Stress again that this process should be seen as a positive experience, more like a ‘mentorship’ and that the learning experience will be 2 way, ie the reviewer will also learn a lot from them. This will enable DAFNE to continue to develop. Discuss any concerns or issues as appropriate. Before you come back for the follow-up day for the DEP (day 4) you will be asked to complete a feedback form on your peer review experience. This is one of the ways that the standards for peer reviewers is maintained.
DEP Peer-review schedule
DAFNE © T01.002, Version 10 – October 2010 280

DAFNE © T01.002, Version 10 – October 2010 281
Who are the Reviewers?
Experienced DAFNE educators (minimum 4 courses).
Attended 1 day’s peer review training on documentation and giving feedback.
People who are committed to DAFNE and the aim to increase the number of DAFNE centres.

DAFNE © T01.002, Version 10 – October 2010 282
Ground Rules for the DEP Reviewer – The Peer Supported Course
They should seek agreement with the DEP Trainee at the beginning of the course regarding their preferred method and timing of the feedback from sessions (at least daily).
They should arrive on time for each session.
They should sit at the back of the room/out of the way and be as unobtrusive as possible.
They should not interrupt or attempt to participate in any of the sessions unless invited to do so by the DEP Trainee.
If the DEP Reviewer observes a serious error they will get the attention of the DEP Trainee and arrange to speak (in confidence) in a way that does not undermine the DEP Trainee (after the session).
Give feedback according to the principles.
DAFNE © T01.002, Version 10 – October 2010 283
Peer-reviewed course OUR Expectations
Delivery of a 5-day DAFNE course
Achieving learning outcomes from DAFNE curriculum
Appropriate use of DAFNE resources
Use of adult learning principles
Appropriate advice on “core skills” (ie CP estimation and insulin dose adjustment)
Effective group management skills
Appropriate recruitment/preparation of participants
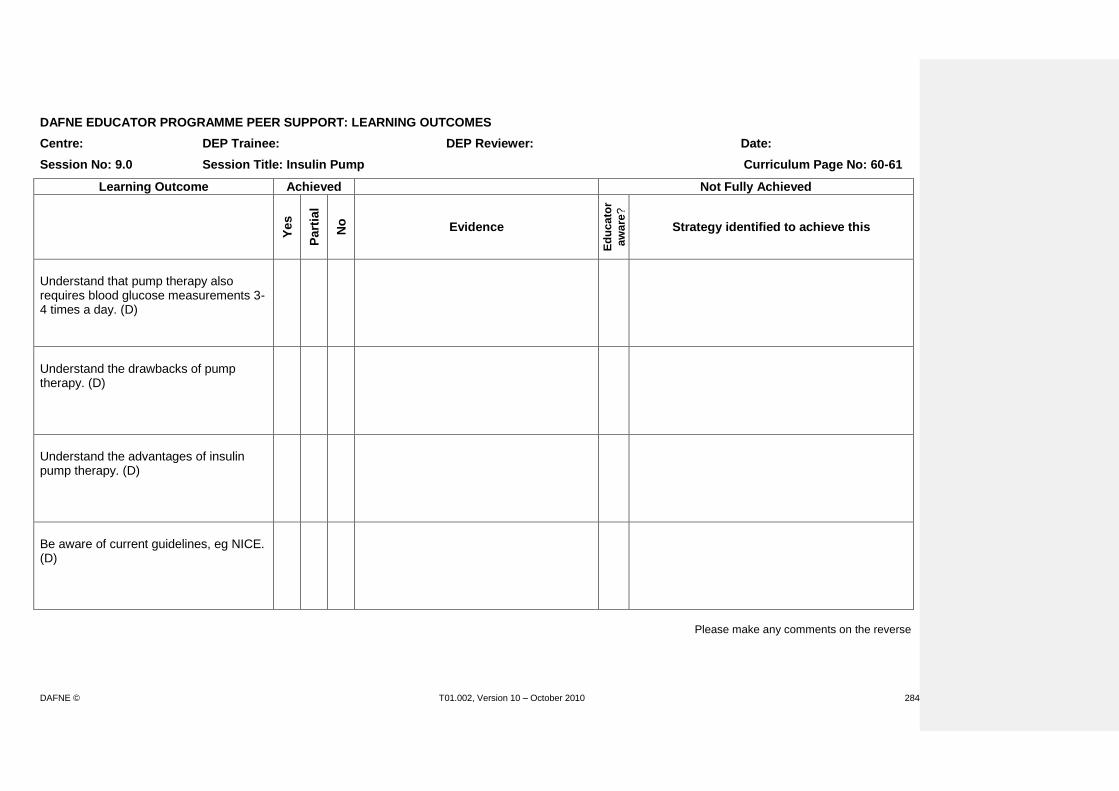
DAFNE © T01.002, Version 10 – October 2010 284
DAFNE EDUCATOR PROGRAMME PEER SUPPORT: LEARNING OUTCOMES
Centre: DEP Trainee: DEP Reviewer: Date:
Session No: 9.0 Session Title: Insulin Pump Curriculum Page No: 60-61
Learning Outcome Achieved Not Fully Achieved
Yes
Part
ial
No
Evidence
Ed
uc
ato
r
aw
are
?
Strategy identified to achieve this
Understand that pump therapy also requires blood glucose measurements 3-4 times a day. (D)
Understand the drawbacks of pump therapy. (D)
Understand the advantages of insulin pump therapy. (D)
Be aware of current guidelines, eg NICE. (D)
Please make any comments on the reverse

DAFNE © T01.002, Version 10 – October 2010 285

DAFNE © T01.002, Version 10 – October 2010 286

DAFNE © T01.002, Version 10 – October 2010 287

DAFNE © T01.002, Version 10 – October 2010 288

DAFNE © T01.002, Version 10 – October 2010 289
DAFNE © T01.002, Version 10 – October 2010 290

DAFNE © T01.002, Version 10 – October 2010 291

DAFNE © T01.002, Version 10 – October 2010 292
DAFNE © T01.002, Version 10 – October 2010 293

DAFNE © T01.002, Version 10 – October 2010 294
EFFECTIVE RECRUITMENT STRATEGIES LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Be familiar with the existing criteria for appropriate recruitment to the DAFNE programme
Explain and discuss the criteria
Acetate/Centre Manual (section 6.1)
Be aware of different recruitment methods and identify an appropriate strategy for their service
Ask participants how they plan to recruit patients to courses in their service OR (in established centre) ask if they are aware of or involved in the recruitment process. Discuss the pro’s and con’s of various approaches. Discuss one example of (local) recruitment strategy.
Flip chart and pens Acetate: DAFNE Recruitment Strategy (Sheffield)
Understand the importance of appropriate patient information to enable informed choice and commitment to the programme
Discuss what information is required/essential in order to fully inform patients.
DAFNE information leaflets DAFNE Posters

DAFNE © T01.002, Version 10 – October 2010 295
CRITERIA FOR PEOPLE WHO COULD BE SUITABLE/BENEFIT FROM DAFNE
Type 1 diabetes for at least 6 months (and/or post ‘honeymoon’)
Over 17 years old
HbA1c <12%
Motivated to improve diabetes control
Need for flexibility of eating/insulin regime
Willing to inject and test at least 5 times a day
Able to speak/understand/read English
Absence of ‘end-stage’ diabetes complications, ie renal failure
Able to attend for a full 5 days course (supporting information is available for employers) and follow-up sessions

DAFNE © T01.002, Version 10 – October 2010 296
DAFNE Recruitment Strategy
(Sheffield)
Letter to referrer
copied to patient
Reply:
Not Interested.
Remove from
waiting list.
Appointment with
Educator 1:1
Plan pre-course
appointment
Allocate course date.
Mail:
Confirmation letter
Employer letter
Recruitment meeting
Reply:
Interested.
Need to establish
commitment!
Mailing:
Letter
DAFNE leaflet
reply slip
Referral to
DAFNE waiting list
Existing
Type 1 Diabetes:
ROUTINE
Newly diagnosed T1
or unplanned pregnancy:
FAST TRACK
Patient identified according
to DAFNE criteria

DAFNE © T01.002, Version 10 – October 2010 297
PRE-COURSE APPOINITMENT / DATA COLLECTION : GETTING SOME PRACTISE LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Understand that there are two levels of data collection and their centre will collect either core or full data sets. Be familiar with the DAFNE Data Collection Form and ‘Standard Operating Procedure’ appropriate to their centre. Know the importance of ongoing Quality Assurance Practise completing a data collection form Be familiar with quality of life questionnaires appropriate to their centre.
Explain that in order to support smaller centres who may not have admin support, centres will collect a core data set. The full data set collected by participating centres will be used for DAFNE research for the benefit of the whole DAFNE collaborative. Briefly demonstrate the DAFNE Pre-Course Data Collection form (current issue). Explain this and the SOP are provided in the Centre Manual. Discuss the importance of ongoing Quality Assurance in relation to current DoH recommendations, etc. Provide (centre) pairs with DEP pre-course appointment exercise handout and blank data collection form and ask them to complete as much of the form as they can, with the information provided. Discuss what can/cannot be recorded on the form and discuss what further information would be required at pre-course appointment. Discuss queries arising from exercise. If appropriate, provide handouts of HADS, PAID, EQ-5D, DSQoL and SF12
Data Collection Form Centre Manual DEP Pre-course Appointment Exercise handout. Blank pre-course data collection form. HADS, PAID, EQ-5D, DSQoL, SF12
Identify who will carry out data collection within their service and the time required.
Reflect on strategies for commencing DAFNE insulin regime and discuss when this will take place within their centre. Pairs to identify and allocate time scales for arranging appointments prior to their peer-reviewed course.

DAFNE © T01.002, Version 10 – October 2010 298
PRE-COURSE APPOINITMENT / DATA COLLECTION : GETTING SOME PRACTISE LEARNING GOALS METHODS MATERIALS/MEDIA
Understand what information should be given to the patient at their pre-course appointment so that they arrive on the course prepared and informed
Ask group what information they think they would need to give their patients. Discuss and list on flipchart, eg:
Venue
Times
Catering arrangements
Parking
Relatives/partners
What to bring (monitoring equipment, insulin, questionnaires, etc)
Etc. Explain examples of letters are provided in Centre Manual.
Centre Manual Flipchart and pens

DAFNE © T01.002, Version 10 – October 2010 299
DEP DAFNE Pre-course Appointment Exercise
John Smith Dob 20.02.1965 Type 1 diabetes since age 9 At annual review 5 months ago: Background diabetic retinopathy Reduced sensation (monofilament) in both feet HbA1c 8.9% Creatinine 110 umol/l Cholesterol 4.6 mmol/l BP 128/72
Weight 82kg Currently on:
Humulin I 30 units at bedtime Humulin S 8 units at breakfast, 12 units at lunch, 20 units at tea. Atorvastatin and Lisinopril
Has hypoglycaemia unawareness and has had 2 severe hypos in the past year. Has discussed insulin pump therapy with Consultant.

DAFNE © T01.002, Version 10 – October 2010 300

DAFNE © T01.002, Version 10 – October 2010 301
DAFNE © T01.002, Version 10 – October 2010 302

DAFNE © T01.002, Version 10 – October 2010 303

DAFNE © T01.002, Version 10 – October 2010 304
DAFNE © T01.002, Version 10 – October 2010 305

DAFNE © T01.002, Version 10 – October 2010 306

DAFNE © T01.002, Version 10 – October 2010 307
DAFNE © T01.002, Version 10 – October 2010 308

DAFNE © T01.002, Version 10 – October 2010 309
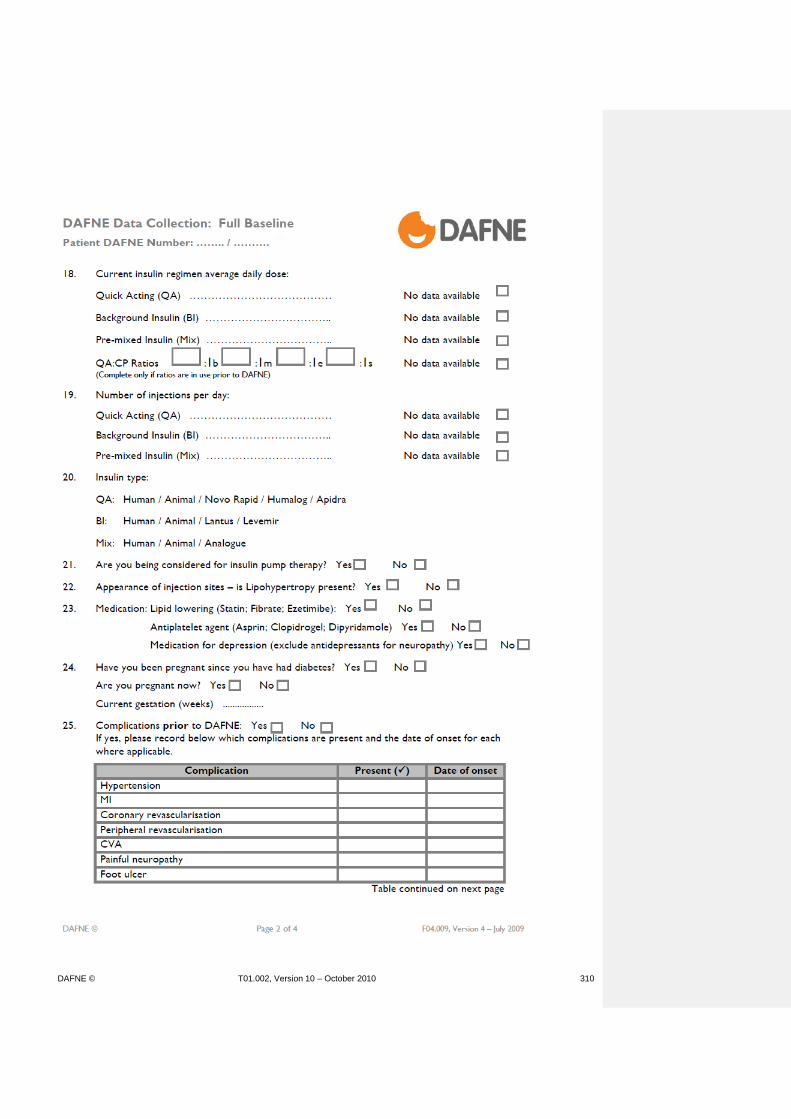
DAFNE © T01.002, Version 10 – October 2010 310

DAFNE © T01.002, Version 10 – October 2010 311
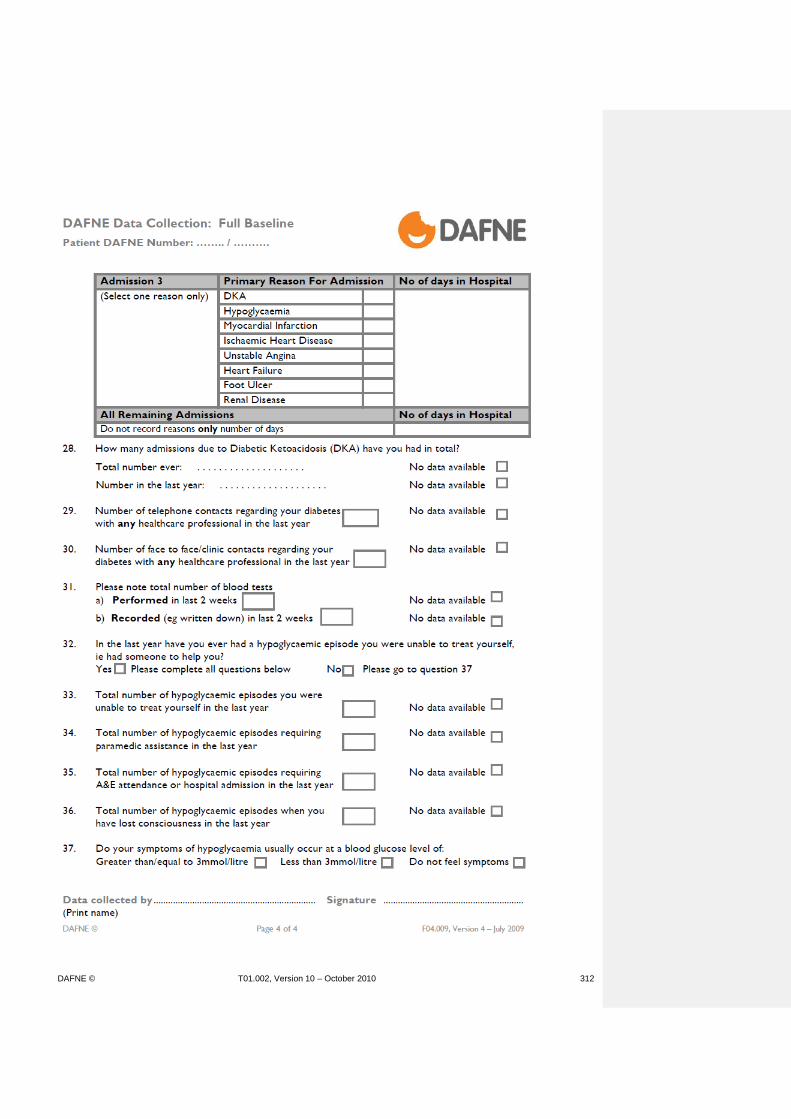
DAFNE © T01.002, Version 10 – October 2010 312

DAFNE © T01.002, Version 10 – October 2010 313

DAFNE © T01.002, Version 10 – October 2010 314
DAFNE © T01.002, Version 10 – October 2010 315

DAFNE © T01.002, Version 10 – October 2010 316

DAFNE © T01.002, Version 10 – October 2010 317

DAFNE © T01.002, Version 10 – October 2010 318
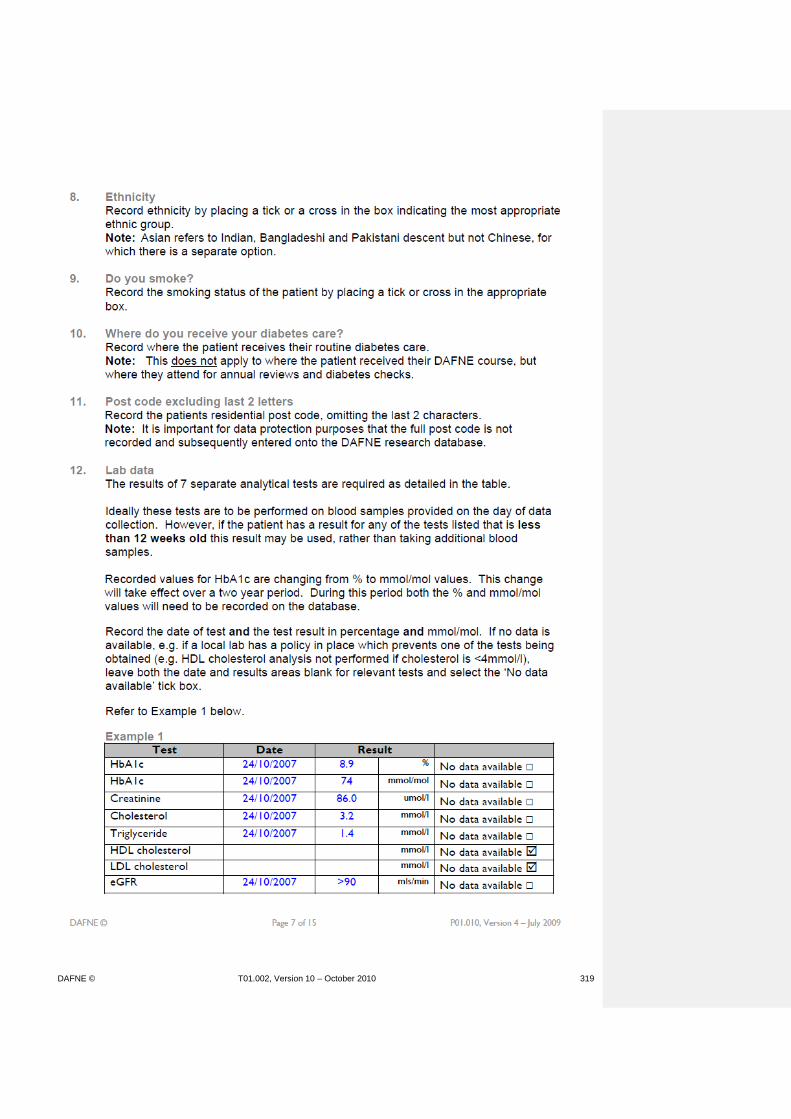
DAFNE © T01.002, Version 10 – October 2010 319
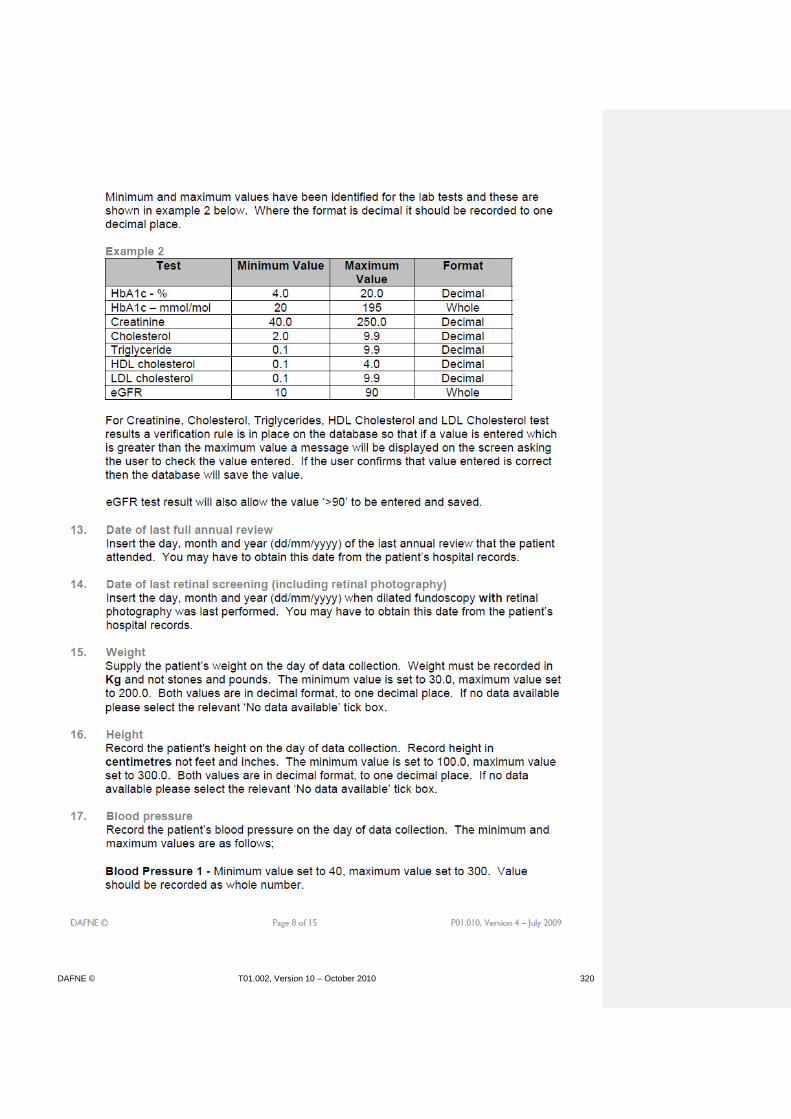
DAFNE © T01.002, Version 10 – October 2010 320

DAFNE © T01.002, Version 10 – October 2010 321

DAFNE © T01.002, Version 10 – October 2010 322

DAFNE © T01.002, Version 10 – October 2010 323

DAFNE © T01.002, Version 10 – October 2010 324

DAFNE © T01.002, Version 10 – October 2010 325

DAFNE © T01.002, Version 10 – October 2010 326

DAFNE © T01.002, Version 10 – October 2010 327

DAFNE © T01.002, Version 10 – October 2010 328
EQ-5D Pre/Post Course* (delete where applicable) DAFNE No ……/……..
Health Questionnaire
(English version for the UK) (validated for use in Eire)

DAFNE © T01.002, Version 10 – October 2010 329
By placing a tick in one box in each group below, please indicate which
statements best describe your own health state today.
Mobility
I have no problems in walking about
I have some problems in walking about
I am confined to bed
Self-Care
I have no problems with self-care
I have some problems washing or dressing myself
I am unable to wash or dress myself
Usual Activities (e.g. work, study, housework, family or
leisure activities)
I have no problems with performing my usual activities
I have some problems with performing my usual activities
I am unable to perform my usual activities
Pain/Discomfort
I have no pain or discomfort
I have moderate pain or discomfort
I have extreme pain or discomfort
Anxiety/Depression
I am not anxious or depressed
I am moderately anxious or depressed
I am extremely anxious or depressed
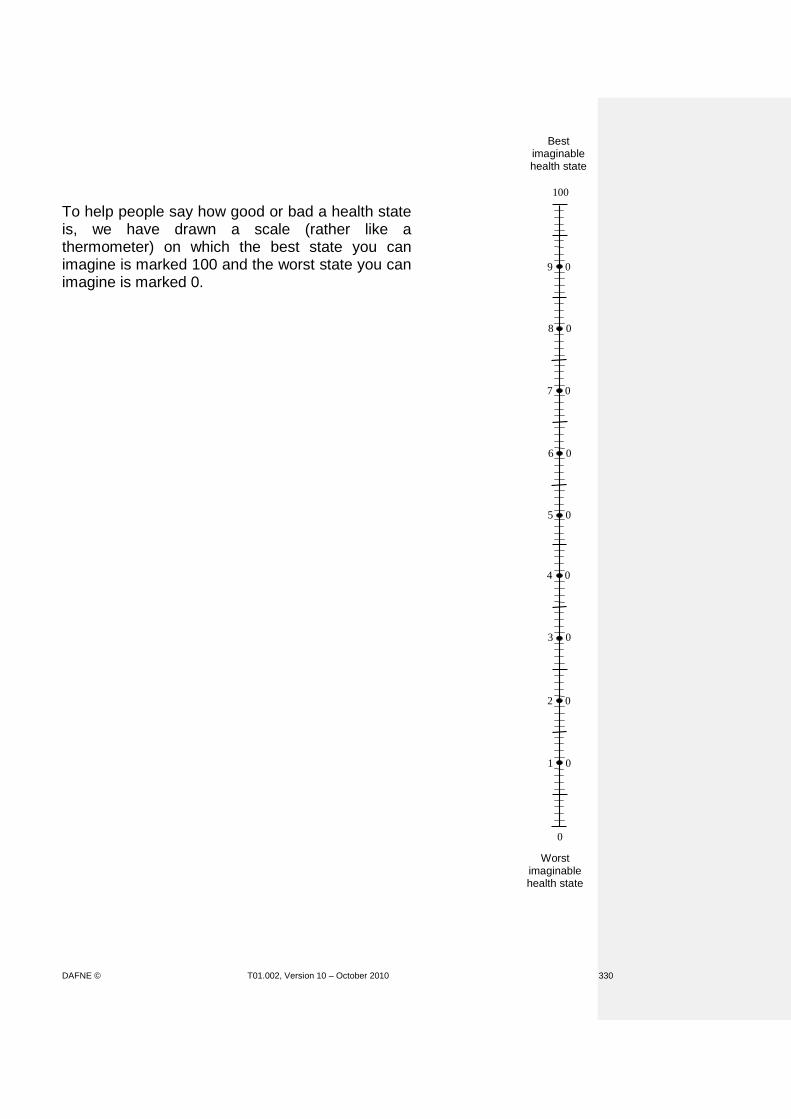
DAFNE © T01.002, Version 10 – October 2010 330
To help people say how good or bad a health state is, we have drawn a scale (rather like a thermometer) on which the best state you can imagine is marked 100 and the worst state you can imagine is marked 0.
9 0
8 0
7 0
6 0
5 0
4 0
3 0
2 0
1 0
100
Worst imaginable health state
0
Best imaginable health state

DAFNE © T01.002, Version 10 – October 2010 331
We would like you to indicate on this scale how good or bad your own health is today, in your opinion. Please do this by drawing a line from the box below to whichever point on the scale indicates how good or bad your health state is today.
Your own health state
today

DAFNE © T01.002, Version 10 – October 2010 332
Because all replies are anonymous, it will help us to understand your answers better if we have a little background data from everyone, as covered in the following questions.
1. Have you experienced serious illness? Yes No
in you yourself
in your family
in caring for others
2. What is your age in years ?
3. Are you: Male Female
4. Are you:
a current smoker
an ex-smoker
a never smoker
5. Do you now, or did you ever, work in Yes No
health or social services?
If so, in what capacity? .....................................................................
6. Which of the following best describes
your main activity?
in employment or self employment
retired
housework
student
seeking work
other (please specify) .........................................
7. Did your education continue after Yes No
the minimum school leaving age?
8. Do you have a Degree or equivalent Yes No
professional qualification?
9. If you know your postcode, would you please write it here
PLEASE TICK APPROPRIATE
BOXES
PLEASE TICK APPROPRIATE
BOX
PLEASE TICK APPROPRIATE
BOX
PLEASE TICK APPROPRIATE
BOX
PLEASE TICK APPROPRIATE
BOX
PLEASE TICK APPROPRIATE
BOX
PLEASE TICK APPROPRIATE
BOX

DAFNE © T01.002, Version 10 – October 2010 333
Problem Areas in Diabetes (PAID) Questionnaire Pre/Post Course* (delete where applicable) DAFNE No ……/…….. INSTRUCTIONS: Which of the following diabetes issues are currently a problem for you? Circle the number that gives the best answer for you. Please provide an answer for each question.
Not a
problem Minor
problem Moderate problem
Somewhat serious problem
Serious problem
Not having clear and concrete goals for your diabetes care?
0 1 2 3 4
Feeling discouraged with your diabetes treatment plan?
0 1 2 3 4
Feeling scared when you think about living with diabetes?
0 1 2 3 4
Uncomfortable social situations related to your diabetes care (eg people telling you what to eat)?
0 1 2 3 4
Feelings of deprivation regarding food and meals?
0 1 2 3 4
Feeling depressed when you think about living with diabetes?
0 1 2 3 4
Not knowing if your mood or feelings are related to your diabetes?
0 1 2 3 4
Feeling overwhelmed by your diabetes? 0 1 2 3 4
Worrying about low blood sugar reactions? 0 1 2 3 4
Feeling angry when you think about living with diabetes?
0 1 2 3 4
Feeling constantly concerned about food and eating?
0 1 2 3 4
Worrying about the future and the possibility of serious complications?
0 1 2 3 4
Feelings of guilt or anxiety when you get off track with your diabetes management?
0 1 2 3 4
Not “accepting” your diabetes? 0 1 2 3 4
Feeling unsatisfied with your diabetes physician?
0 1 2 3 4
Feeling that diabetes is taking up too much of your mental and physical energy every day?
0 1 2 3 4
Feeling alone with your diabetes? 0 1 2 3 4
Feeling that your friends and family are not supportive of your diabetes management efforts?
0 1 2 3 4
Coping with complications of diabetes? 0 1 2 3 4
Feeling “burned out” by the constant effort needed to manage diabetes?
0 1 2 3 4
1999 Joslin Diabetes Center

DAFNE © T01.002, Version 10 – October 2010 334
The Hospital Anxiety and Depression Scale (HADS)
Pre/Post Course* (delete where applicable) DAFNE No ……/……..
This questionnaire is designed to help us know how you are feeling emotionally. Read each statement and
place a tick in the box by the reply that comes closest to how you have been feeling in the past week. Don’t
take too long over your replies; an immediate reaction to each item will probably be more accurate.
I feel tense or ‘wound up’: I feel as if I am slowed down:
Most of the time .......................................................... Nearly all the time ........................................................
A lot of the time .......................................................... Very often ......................................................................
From time to time, occasionally ............................... Sometimes ......................................................................
Not at all ........................................................................ Not at all .........................................................................
I get a sort of frightened feeling like ‘butterflies’
I still enjoy the things I used to enjoy: in the stomach:
Definitely as much ....................................................... Not at all ........................................................................
Not quite so much ...................................................... Occasionally ..................................................................
Only a little ................................................................... Quite often ...................................................................
Hardly at all ................................................................... Very often .....................................................................
I get a sort of frightened feeling as if something
awful is about to happen: I have lost interest in my appearance:
Very definitely and quite badly .................................. Definitely ........................................................................
Yes, but not too badly ................................................ I don’t take as much are as I should .........................
A little, but it doesn’t worry me .............................. I may not take quite as much care ............................
Not at all ........................................................................ I take just as much care as ever ................................
I can laugh and see the funny side of things: I feel restless as if I have to be on the move:
As much as I always could ......................................... Very much indeed ........................................................
Not quite so much now ............................................. Quite a lot ......................................................................
Definitely not so much now ...................................... Not very much ..............................................................
Not at all ........................................................................ Not at all ........................................................................
Worrying thoughts go through my mind: I look forward with enjoyment to things:
A great deal of the time ............................................. As much as ever I did ..................................................
A lot of the time .......................................................... Rather less than I used to ...........................................
From time to time but not too often ..................... Definitely less than I used to ......................................
Only occasionally ......................................................... Hardly at all ....................................................................
I feel cheerful: I get sudden feelings of panic:
Not at all ........................................................................ Very often indeed .........................................................
Not often ....................................................................... Quite often ....................................................................
Sometimes ..................................................................... Not very often ..............................................................
Most of the time .......................................................... Not at all ........................................................................
I can enjoy a good book or radio or TV
I can sit at ease and feel relaxed: programme:
Definitely ....................................................................... Often ...............................................................................
Usually ............................................................................ Sometimes ......................................................................
Not often ....................................................................... Not often ........................................................................
Not at all ........................................................................ Very seldom ...................................................................
HADS copyright © R.P.Snaith and A.S.Zigmond, 1983, 1992, 1994. Record forms originally published in Acta Psychiatrica Scandinavica, 67, 361-70,
copyright Munksgaard International Publishers Ltd, Copenhagen 1983. Reproduced by permission of the Publishers, nferNelson Publishing Company
Ltd., of The Chiswick Centre, 414 Chiswick High Road, London W4 5TF UK. All rights reserved including translation. nferNelson is a division of
Granada Learning Limited.

DAFNE © T01.002, Version 10 – October 2010 335

DAFNE © T01.002, Version 10 – October 2010 336

DAFNE © T01.002, Version 10 – October 2010 337

DAFNE © T01.002, Version 10 – October 2010 338

DAFNE © T01.002, Version 10 – October 2010 339

DAFNE © T01.002, Version 10 – October 2010 340

DAFNE © T01.002, Version 10 – October 2010 341

DAFNE © T01.002, Version 10 – October 2010 342

DAFNE © T01.002, Version 10 – October 2010 343
FOLLOW UP AND SUPPORT FOR DAFNE ‘GRADUATES’ LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Be willing to discuss the significance of the DAFNE Trial results in relation to the ’12 month drift in HbA1c’. Be aware that follow up strategies were not systematically studied during the trial. Identify factors that may affect patients’ learning needs and motivation to continue to use the DAFNE approach. Understand that patients’ learning needs to be encouraged and consolidated for it to become habitual and confident
Ask group if they can remember the results of the DAFNE RCT. Reflect on the HbA1c data and discuss the possible reasons for the ‘drift’ at 12 months. Explain that participants in the RCT were deliberately not offered any follow up support or advice following the course (unless they asked for it), as we naively believed that the patients in Germany only got the 5 day course and were ‘sorted’ for life. Participants in the RCT returned to traditional diabetes clinics where staff (particularly doctors) were either unaware of or did not support DAFNE principles/philosophy. Outside of the group, many patients may have felt very alone when faced with negative responses from HCPs, unless they were assertive enough to stand up for what they had been trained to do. Research on how adults learn suggests that people require practise, reflection and reinforcement of skills for these to be maintained in the long term. Relate to other group support examples (e.g. Weight Watchers; smoking cessation) and how people tend to ‘lapse’ when not attending group / receiving ongoing support.
DAFNE © T01.002, Version 10 – October 2010 344
FOLLOW-UP AND SUPPORT FOR DAFNE ‘GRADUATES’ LEARNING GOALS METHODS MATERIALS/MEDIA
Be aware of existing models for educational and clinical follow up for DAFNE ‘graduates’ and begin to identify appropriate strategies for their service.
Describe the aims of and suggested methods of follow up: Initial Follow Up Recurring Follow Up
Discuss other methods, e.g. telephone helplines, drop-in clinics, etc. Explain the usefulness of collecting data on who attends / does not attend follow up so we can audit outcomes and develop a system which best meets the needs of patients. Suggest centre pairs meet to discuss a follow-up / support plan post DAFNE for their own service.
Acetates: ‘Initial Follow Up’ and ‘Recurring Follow Up’

DAFNE © T01.002, Version 10 – October 2010 345
Initial Follow Up
• Within 8 weeks of completion of course
• Same group / Educator(s)
• 2 – 2½ hours
• Review CP estimation & dose adjustment
• Diaries / acetates
• Discussion of other relevant issues / concerns
• Opportunity for 1:1

DAFNE © T01.002, Version 10 – October 2010 346
Recurring Follow Up
• Every 12-18 months following completion of course
• Same, or mixed groups. 8-10 participants
• 1-2 Educator(s) & Dr availability
• 3 – 3½ hours
• Reinforcement of core DAFNE principles (group), via
structured curriculum & resources
• Data collection (1:1) – biomedical & psychometric

DAFNE © T01.002, Version 10 – October 2010 347
CATERING ARRANGEMENTS AND DAFNE RESOURCES LEARNING GOALS METHODS MATERIALS/MEDIA
Know the aim of the session is to discuss the planning required to ensure all the facilities are available to run a DAFNE course
INTRODUCTION Explain - The aim of this session is to provide an opportunity to discuss your ongoing planning for running the DAFNE courses in terms of the catering arrangements, resources and equipment required. The DAFNE Centre Handbook will be essential for this planning.
DAFNE Centre Manual Flipchart and pens DAFNE flipchart Curriculum Insulin action charts Food models Food plates Folder of ‘Essential Curriculum Resources’ Patient folder containing:
Diary
CP booklet
Course Handbook
Quiz
Pencil
Timetable
Individual Dose Adjustment Acetate
Know the requirements of a suitable venue for a DAFNE course
VENUE Ask – From your observation week, what do you think are the requirements of a suitable venue for a DAFNE course?
Collect the various suggestions on the flipchart. Discuss – Acetate – venue. Ask – Do any centres have concerns about finding suitable venues? Collect and discuss concerns
Flip chart and pens Acetate - Venue
DAFNE © T01.002, Version 10 – October 2010 348
CATERING ARRANGEMENTS AND DAFNE RESOURCES LEARNING GOALS METHODS MATERIALS/MEDIA
Know the catering arrangements may vary between centres due to the facilities and finance available.
CATERING Explain – Each centre has different catering arrangements. These vary due to factors such as the cost of the food and the facilities available. Describe – The various options for catering arrangements. Emphasise – Each approach has pros and cons and each centre needs to find a system that works for them.
Acetate – Catering arrangements
Know the key considerations when planning local catering arrangements.
Explain – Key considerations when making local catering arrangements for acetate Meal times are a learning opportunity, therefore a range of CHO foods should be available through the week for practise of CP estimation. There should be time and space for a discussion around the CP estimation and insulin doses. Participants should be able to eat together. Requirements for special diets should be established at the pre course assessment and planned for. Ask – What arrangements are centres considering and why? Split into groups of 4-5. Collect and discuss – Feedback from small groups.
Acetate – Catering arrangements Flipchart and pens

DAFNE © T01.002, Version 10 – October 2010 349
CATERING ARRANGEMENTS AND DAFNE RESOURCES LEARNING GOALS METHODS MATERIALS/MEDIA
Explain – In addition to meals, refreshments also need to be available and purchased out of the catering budget. These include drinks, snacks and hypo treatments. Discuss – A choice of healthy and high fat, snacks and desserts should be available where possible.
Acetate – Catering arrangements
Know the resources required for the week and where they should be obtained from. Know which resources they need to obtain and purchase themselves. Be aware of additional resources that may need to be collected/developed for sessions
RESOURCES Explain – There are many resources used during the DAFNE week. It is important to familiarise yourself with these. The DAFNE centre manual provides a comprehensive list of what is required for the week and where to obtain the various items from (see Section 1). Discuss – Locally funded and supplied resources – DAFNE Centre Manual, section 11.2, and clarify queries. Emphasise – When lesson planning, there will be some sessions that require additional resources to be collected, ie food packets, recipes and takeaway information for the nutrition sessions. You should also feel free to develop further local resources to help meet the learning outcomes of the sessions. Many of the 3 centres original ideas have now been incorporated into the handbook but we continue to develop and share new ideas all the time. You have examples of such additional resources that you can use should you wish.
DAFNE Centre Manual Acetate – Locally funded and supplied resources

DAFNE © T01.002, Version 10 – October 2010 350
CATERING ARRANGEMENTS AND DAFNE RESOURCES LEARNING GOALS METHODS MATERIALS/MEDIA
Know the resources that are produced and supplied by the Central Office
CENTRALLY FUNDED AND SUPPLIED RESOURCES Explain – Centrally funded and supplied resources – DAFNE Centre Manual 11.1
Acetate: “DAFNE Resource Purchase Requisition”
Know that the DAFNE resources are essential to meet the learning outcomes of the course.
Show and discuss – The key DAFNE resources.
Be aware f how the resources have been developed and that there is further scope for development.
Emphasise – The development of these. Translated from German originally. Since been further revamped. Scope for further development through the Collaborative. Explain – The resources are specific to the learning outcomes and are therefore essential, not optional.

DAFNE © T01.002, Version 10 – October 2010 351
Choosing a Venue
Consider
Access
Size
Availability of same room for whole week
Availability of toilets, telephones
Storage and transportation of resources
Equipment required
Temperature – fans, blinds etc

DAFNE © T01.002, Version 10 – October 2010 352
Catering Arrangements
1. Consider Hospital catering
Outside catering
Hospital canteen
Participants bring own food All options have pros and cons
2. Meal Times Learning opportunity
Range of CHO foods available
Time and space for discussion
All eat together
Plan for special diets
3. Snacks and Refreshments Drinks
Choice of snacks
Hypo treatment – lucozade, fruit juice

DAFNE © T01.002, Version 10 – October 2010 353
DAFNE Resources
Patient Resources Handbook (1) Diary (4 per year) CP list (1) My Plan (1) Folder (1) Eraser-tip pencil (1) Quiz (1) Note paper (10 pg) Folder (1)
Core Course Resources DAFNE flipchart Food photographs Replica food set Insulin action charts My Plan wipe board Curriculum and manual Dose adjustment examples Dose adjustment template for OHP

DAFNE © T01.002, Version 10 – October 2010 354
‘Local’ Resources
Name badges BG meters and strips Timetable Lesson plans Nutrition text books Pencil sharpener Tissues Blu-tac/pins Food scales (<£36)
Room, table and chairs Flipcharts and pens OHP Acetates and pens Hypo treatments Food packets Evaluation forms Additional ‘handouts’ Catering (>£12.50/pt/wk)

DAFNE © T01.002, Version 10 – October 2010 355

DAFNE © T01.002, Version 10 – October 2010 356
DELIVERING DAFNE LOCALLY – PERSONAL PLAN LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Identify, by means of their ‘Personal Plan’, what further preparation they and their team must undertake prior to their first DAFNE course. Have an opportunity to discuss any further training issues or concerns.
Individuals/centre pairs to complete their own Personal Plan following completion of the training workshop. (this may be done during the workshop, if time allows, or in trainees’ own time) Individuals should be encouraged to discuss with trainer(s) any issues which may need to be addressed prior to the peer-reviewed week.
Handout ‘Personal Plan’

DAFNE © T01.002, Version 10 – October 2010 357
Personal Plan
What do I personally need to do between now and my peer-reviewed course? Consider: Time required:
Patient recruitment and preparation:
Room/catering organisation:
Preparation of resources:
PTO

DAFNE © T01.002, Version 10 – October 2010 358
Preparation of lesson plans:
‘Team’ organisation:
Any unresolved issues/training needs:

DAFNE © T01.002, Version 10 – October 2010 359
SUMMARY / FEEDBACK / EVALUATION LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Reflect on their expectations of the training workshop and identify if these have been met
Refer to flip charts from Day 1 Discuss each expectation in turn. Has it been met/achieved? If not, why not? Could it have been achieved? Is it more appropriate for Follow up day etc?
Flip charts
Reflect on their experience of keeping a CP Diary and being ‘scrutinised’ in their CP estimation Reflect on homework tasks
Ask for experiences. How does this relate to what will happen on their ‘patient’ courses?
Have an opportunity to discuss any unresolved issues and identify issues to take forward to Doctor’s training day or Follow up day Contribute to future DEP workshops
Refer to flip chart of ‘unresolved issues from preparatory work/observation week’. Is there anything still outstanding? Does anything need to be taken forward to Doctor training day or Follow up day? (REMEMBER TO SAVE THESE FOR FOLLOW UP WORKSHOP) Ask individuals to write on a separate post-its:
1 thing that they thought was really good about the 3 day DEP
1 thing that they think we should change Include planning and organisation prior to DEP as well as the last 3 days.
Flip charts Post-it notes Flipcharts and pens
DAFNE © T01.002, Version 10 – October 2010 360
SUMMARY / FEEDBACK / EVALUATION LEARNING GOALS METHODS MATERIALS/MEDIA
Complete a workshop evaluation form
Place post-its on pre-prepared flipcharts. Feedback to group and clarify any points. Participants each complete evaluation sheet.
DEP Training Workshop Evaluation
Leave feeling prepared for their tasks and course delivery over the following weeks
Check/ask if anything further to discuss either as a group or individually.
Know where to find contact details for Trainers, Reviewers and other Educators for ongoing support
Refer to Centre Manual
Centre Manual

DAFNE © T01.002, Version 10 – October 2010 361
DAFNE © T01.002, Version 10 – October 2010 362
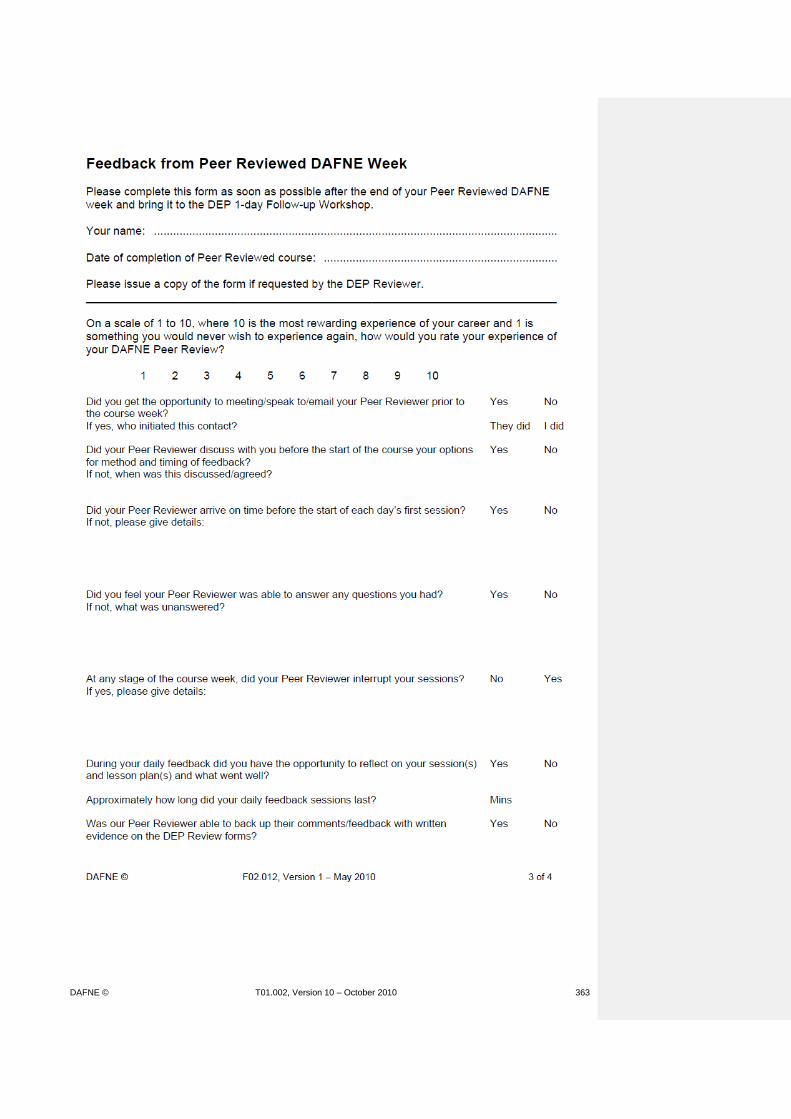
DAFNE © T01.002, Version 10 – October 2010 363

DAFNE © T01.002, Version 10 – October 2010 364
DAFNE © T01.002, Version 10 – October 2010 365
DEP Training Workshop Date / venue
Evaluation form
It would really help us if you could complete this form as honestly and constructively as possible to help us further develop DEP.
The aims of the workshop are to develop your competencies in CP estimation and DAFNE insulin regime, and to prepare for delivering DAFNE in your own service. On reflection do you feel the workshop met these aims?
Yes Partly No (please comment) (please comment)
Are there any sessions you would like to make particular comments on? Day 1:
(Experiences of observing a DAFNE course; The DAFNE Philosophy; The DAFNE approach to food; Estimating difficult CHOs; snacks; labelling; Practical use of the glycaemic index; Starting and adjusting the DAFNE insulin regime; Homework) Day 2:
(Therapeutic Patient Education and Adult Education / Learning Theories; The DAFNE curriculum and lesson planning; Sharing ideas / strategies for specific sessions; Managing groups: tips / scenarios; Homework)
PTO

DAFNE © T01.002, Version 10 – October 2010 366
Day 3: (Preparation for peer-reviewed course; Pre-course appointment / data collection; The DAFNE database; Recruitment strategies; Follow up and support for DAFNE ‘graduates’; Catering arrangements and DAFNE resources; Delivering DAFNE locally – personal plan)
Do you have any suggestions for future changes to the workshop programme (if required)?
Name: ..............................................................................................................................
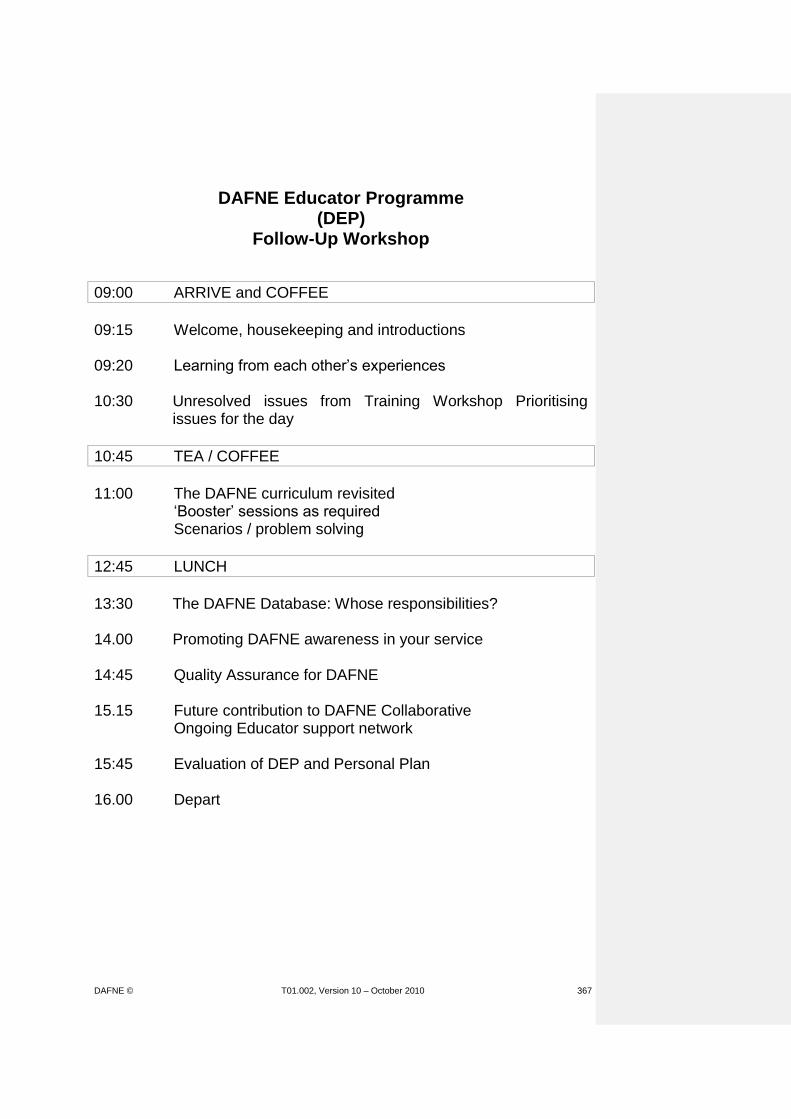
DAFNE © T01.002, Version 10 – October 2010 367
DAFNE Educator Programme (DEP)
Follow-Up Workshop
09:00 ARRIVE and COFFEE
09:15 Welcome, housekeeping and introductions 09:20 Learning from each other’s experiences 10:30 Unresolved issues from Training Workshop Prioritising
issues for the day
10:45 TEA / COFFEE
11:00 The DAFNE curriculum revisited ‘Booster’ sessions as required Scenarios / problem solving
12:45 LUNCH
13:30 The DAFNE Database: Whose responsibilities? 14.00 Promoting DAFNE awareness in your service 14:45 Quality Assurance for DAFNE 15.15 Future contribution to DAFNE Collaborative Ongoing Educator support network 15:45 Evaluation of DEP and Personal Plan 16.00 Depart

DAFNE © T01.002, Version 10 – October 2010 368
DEP FOLLOW-UP WORKSHOP (Venue) (Date)
Delegate list
Name Profession Hospital

DAFNE © T01.002, Version 10 – October 2010 369
WELCOME, HOUSEKEEPING AND INTRODUCTIONS LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should…. Be informed of location of toilets, fire exits, etc. Feel welcomed and valued and able to contribute to the programme Be informed about the agenda for the workshop
Describe location of toilets and fire escapes. Explain procedure if fire alarm sounds (also if any alarm tests expected on the day) Welcome of new Educators by trainers and introduction of trainers / guests. Congratulate all Educators for completing their peer-reviewed first DAFNE course Illustrate outline of DEP follow up workshop. Explain arrangements for breaks / lunch. Explain that the workshop agenda is flexible, depending on their needs – to be identified shortly.
OHP and title acetate Handout: DEP follow up workshop agenda
Be re-acquainted with each other / meet new members.
Ask participants to introduce themselves to the rest of the group, indicating their profession, place of work and when they completed their peer reviewed DAFNE course. (this can be brief if it is exactly the same group as attended the 3-day training workshop)
Name badges/sticker
DAFNE © T01.002, Version 10 – October 2010 370
DAFNE EDUCATOR PROGRAMME (DEP)
FOLLOW-UP WORKSHOP
DAFNE © T01.002, Version 10 – October 2010 371
LEARNING FROM EACH OTHER’S EXPERIENCES LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should….
Have the opportunity to share their experiences of teaching their first DAFNE course Identify areas for further development that can be addressed in the workshop
Small groups of ~4 (e.g. 2 centre pairs) to discuss their first course:
What went well
Lessons learned
Which aspects require further development
Etc Each centre (pair) to feedback:
1 ‘Highlight’ of the week
1 ‘Low point’ of the week
1 priority for further development Topics for further development listed on flipchart
Acetate: ‘Learning from each other’s experiences’ Flipchart and pens
DAFNE © T01.002, Version 10 – October 2010 372
LEARNING FROM EACH OTHER’S EXPERIENCES
Discuss your first DAFNE course with your neighbours:
What went well?
Lessons learned
Which aspects require further development? (refer to your peer review documentation)
Each Centre (pair) feed back:
1 ‘highlight’ of the week
1 ‘lowlight’ of the week
1 priority for further development
DAFNE © T01.002, Version 10 – October 2010 373
UNRESOLVED ISSUES / PRIORITISNG ISSUES FOR DAY LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should….
Identify unresolved issues from training workshop that still need to be addressed. Identify and agree priorities for the follow up workshop
Pre-prepared flipchart of issues / questions still unresolved / unanswered at end of training workshop. Ask group to identify any that have not been answered / resolved by teaching first course (delete those that have) Referring to this flipchart and the one of ‘topics for further development’, identify common / popular themes. Ask group to decide on what can be covered in time allocated (1 hour 45 minutes prior to lunch). (Frequently these issues will be naturally resolved with experience of running more courses and Educators should be reassured / encouraged to have self-confidence).
Flipchart of unresolved issues / questions from training workshop Flipchart of areas for further development (from 1st session) Highlight / list on flipchart
DAFNE © T01.002, Version 10 – October 2010 374
THE DAFNE CURRICULUM REVISITED ‘BOOSTER’ SESSIONS / SCENARIOS / PROBLEM-SOLVING
LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should….
Participate in group session(s) appropriate to their learning priorities for the day.
Either: A) Facilitate a whole group session covering the priority topics for the day Or: B) Consider splitting into smaller groups to address specific topics as appropriate to individuals. Common topics / themes have been:
Alcohol session
Exercise session
Annual review / complications session
Use of (long acting) analogues
Patient cases from peer reviewed week Use their experiences / ideas as well as trainers’ own to help discussions. Aim for them to solve these issues by themselves as far as possible. If no specific issues arise, use pre-prepared strategies, eg:
Timetabling exercise Physiological explanations – in small groups develop simple explanations for the following:
Hypo unawareness
Development of ketones
Insulin profile in someone without diabetes
DAFNE course curriculum Course Handbook CP list DAFNE / DEP teaching resources as required DEP timetabling exercise handouts
DAFNE © T01.002, Version 10 – October 2010 375
DEP Timetabling Exercise
Using the blank timetable outline provided, arrange the curriculum sessions in a fluent, logical order.
Think carefully about the time of day, participants’/Educators’ concentration/energy levels, etc., as well as the time needed to deliver the session.
Session: Title on timetable:
Eg: 6. Individual Dose Adjustment Practise Discussion of daily goals, BG results & insulin
doses 4. Lunchtime CP Estimation Practise and Insulin Dose Adjustment Lunch. Discussion of individual BG results & Insulin doses 1. Introduction & Organisation 2. What is Diabetes? 3. Nutrition 1: DAFNE and Food 5. Diabetes Control and Targets 7. Insulin Action and Injection Technique 8. Insulin Pump 9. Nutrition 2: Carbohydrate Portions 10. Hypoglycaemia 11. Nutrition 3: Estimating CHO in a Range of Situations 12a /13a Principles of Insulin Dose Adjustment 12. Insulin Dose Adjustment/Reduction 13. Insulin Dose Adjustment/Escalation 14. Insulin Dose Adjustment/Corrections 15. Nutrition 4: Eating Out, Alcohol, Healthy Eating, Weight Management 16. Illness and Sick Day Rules 17. Physical Activity & Exercise 18. The Theory of Goal Setting & Action Planning 19. Diabetes Annual Review and Complications 20. Social Aspects 21. Quiz, Action Planning, Evaluation and Follow-Up Doctor’s Q&A session (not a curriculum session)
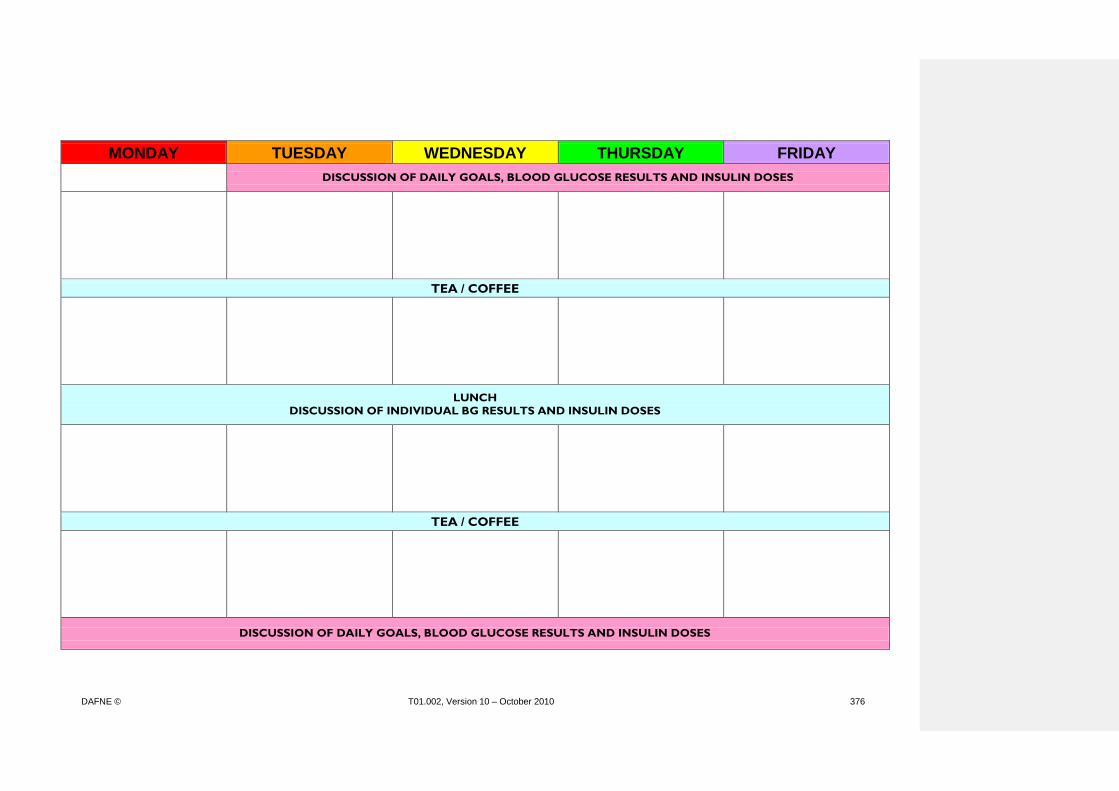
DAFNE © T01.002, Version 10 – October 2010 376
MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY
DISCUSSION OF DAILY GOALS, BLOOD GLUCOSE RESULTS AND INSULIN DOSES
TEA / COFFEE
LUNCH
DISCUSSION OF INDIVIDUAL BG RESULTS AND INSULIN DOSES
TEA / COFFEE
DISCUSSION OF DAILY GOALS, BLOOD GLUCOSE RESULTS AND INSULIN DOSES

DAFNE © T01.002, Version 10 – October 2010 377
DAFNE DATABASE – WHOSE RESPONSIBILITY IS IT? LEARNING GOALS METHODS MATERIALS/MEDIA
Know the aim of the session is to discuss the data collection and data entry onto the DAFNE database for core and full datasets Know that Quality assurance is a key part of delivering structured education Know that baseline data (incl quality of life questionnaires for centres collecting full data set) needs to be collected prior to the course. Know that post course data (incl quality of life questionnaires for centres collecting full data set) needs to be collected annually. Know that it is the lead educator’s responsibility that the DAFNE database is kept up to date and the information is accurately entered.
INTRODUCTION Explain - The aim of this session is to provide an opportunity to discuss the data collection and data entry onto the DAFNE database for full and core datasets. The DAFNE collaborative has an expectation of each DAFNE centre to collect data for audit as well as R&D purposes on an ongoing basis. Some centres will be collecting the full data set, the majority of centres will collect core datasets. This is all part of the Quality assurance programme that DAFNE runs and is one of the key criteria for structured education laid down by the DOH. Reflect back on session before tea break and remind DEP trainees of the data that is collected prior to the course. Describe the post course data that should be collected annually. Discuss – It is the centre’s lead educator’s responsibility to ensure that the data is being collected and added to the database. Ideally only one person should add the data to ensure that it is standardised (ideally an admin person). The centres data will be assessed as part of the 3 yearly external QA visit. Demonstrate the database and discuss how it works, passwords and access levels.
DAFNE Centre Manual – section 11 Acetate DOH key criteria for structured education Baseline Data Collection Form Quality of life questionnaires for centres collecting full dataset Acetate Post course Data Collection Form Quality of life questionnaires for centres collecting full dataset

DAFNE © T01.002, Version 10 – October 2010 378
PROMOTING DAFNE AWARENESS IN YOUR SERVICE LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should….
Identify potential needs for awareness training within their service. Consider ways in which other HCPs may be trained to know more about DAFNE
Ask group who they can think of in primary care / secondary care / elsewhere who may need to know more about DAFNE. List responses on flipchart.
Discuss & list what exactly these individuals / groups would need to know, with particular reference to other members of the team & the tensions that may arise initially. Emphasise that only HCPs who have undergone complete DEP/DDP can teach on DAFNE courses, but course participants will need ongoing support from both the diabetes team and general practitioners who will need to have some basic understanding. Small groups / centre pairs to discuss strategies for promoting DAFNE awareness to particular groups of HCPs. Discuss one model, used successfully in primary care (in Sheffield), but which could be adapted & used in other settings. Observation of courses is the best way for others to learn what DAFNE is about. Explain that awareness training may not be a priority to begin with, but the need will escalate as they train more patients.
Flipchart and pens DAFNE Awareness Workshop handouts Handouts: ‘DEP Guidelines for Educators’ ‘The observation of DAFNE courses’
DAFNE © T01.002, Version 10 – October 2010 379
DAFNE Awareness Workshop Agenda
Introduction
Case Study (in pairs/groups)
Feedback from case study
What is DAFNE?
(Participants’ experiences)
Case Study revisited (CHO counting and insulin calculation workshop)
Discussion
Summary

DAFNE © T01.002, Version 10 – October 2010 380
Case Study
Mike is a 35 year old, a sales rep who lives alone. He has had Type1 Diabetes for 12 years. He really enjoys all types of sport and has a busy social life. Following an assessment by the Diabetes Nurse it was agreed that a basal bolus insulin regimen would best suit his erratic lifestyle, but despite using this system for 3 years his HbA1c has never been below 8.5% and he has problems with night-time hypos or high blood sugars on rising. At a recent out patient appointment he was found to have developed background retinopathy.
His current insulin regimen is: Breakfast Novorapid 12 units Lunch Novorapid 12 units Tea Novorapid 12 units Bed Insulatard 25 units He saw a Dietitian at diagnosis but has not seen one since. Mike monitors his blood glucose levels once a day before breakfast; he would be willing to monitor more often but can only get 50 strips per month on his repeat prescription. He does alter his insulin doses sometimes; if he feels high he takes extra insulin. A typical day: 7.30am Black Coffee with 1 tsp sugar 11.00am 1 cereal bar and small carton of orange juice 1.30pm Regular cheeseburger with fries and chocolate milkshake 5.30pm Gym for 2 hours 8.00pm Ready Meal: Chicken curry, pilau rice, naan bread, onion bhaji Raspberry cheesecake 11.30pm Bed
Discuss how he could improve his blood glucose control and prevent further complications developing.

DAFNE © T01.002, Version 10 – October 2010 381
Mike’s DAFNE insulin regime
Background insulin: Morning 12 units Night 12 units Quick Acting Insulin: Breakfast 2 unit per carbohydrate portion (CP) Lunch 1 unit per CP Tea 1 unit per CP
TIME 7.30 11.00 1.30 5.30 7.30 8.00 11.30
Carbohydrate Portions
Blood Glucose
9.0 6.4 7.3 8.2 8.5 7.6
Quick Acting Insulin
Background Insulin
Using the information for Mike’s ‘typical day’ and the resources provided (CP lists, food photos, food packets, etc), calculate Mike’s CPs, work out the insulin doses that he should take and fill in the diary above

DAFNE © T01.002, Version 10 – October 2010 382
Answers
TIME 7.30 11.00 1.30 5.30 7.30 8.00 11.30
Carbohydrate Portions
½ 4 12½ 0 11½
Blood Glucose
9.0 6.4 7.3 8.2 8.5 7.6
Quick Acting Insulin
+1 8 13 12
Background Insulin
12 10*
*reduced night BI to prevent nocte hypo following exercise

DAFNE © T01.002, Version 10 – October 2010 383
DAFNE Awareness Workshop Educator guidelines
Case Study (in pairs/groups): Provide copies of p1 of the case study. Allow 10-15 mins for pairs/groups to work through case.
Feedback from case study: Take feedback from groups. Notes on flipchart (with particular emphasis on ‘common’ misconceptions / responses such as healthy eating, cardiovascular risks, etc.
What is DAFNE?: Acetates / PowerPoint presentation. Describe background to DAFNE and results of trial. Discuss importance of glycaemic control in type 1 diabetes and how it’s matching insulin to CHO that will achieve this, not ‘healthy eating’ alone. (Contrast with T2DM if appropriate.) DAFNE timetable – emphasise key sessions / skills.
Participants’ experiences (optional): Invite previous participants to attend and talk about their experiences of DAFNE & answer questions. (Choose them carefully)
Case Study revisited: Provide copies of p2 of case study. Have appropriate resources available (based on ‘Mike’s typical day’), i.e. CP list(s), cereal bar, fruit juice, burger food photo plate, Indian food photo plate, cheesecake food model, etc.
Allow 15 mins for pairs/groups to work out CPs and insulin doses for the case. Discuss responses and provide ‘answers’ (p3).
DAFNE © T01.002, Version 10 – October 2010 384
DEP Guidelines for DAFNE Educators (when being observed by trainee centres/educators) The observation course is a pivotal part of the DEP and DDP. It is therefore essential that DEP/DDP Trainees are able to maximise the benefit by observing a high quality course. In order to ensure that this occurs this document outlines the learning outcomes for the DEP /DDP Trainees during their observation week and what you as experienced DAFNE Educators must do in order to ensure that DEP/DDP Trainees achieve these learning outcomes. Trainee Educator(s) Details Course date:
Centre:
Lead Educator 1:
Educator 2:
Doctor: Learning Outcomes of the observation week for the DEP trainee(s)
Observe the delivery of the DAFNE course curriculum.
Know how lesson plans are used to relate to the learning outcomes from the curriculum.
Become familiar with the resources used during a DAFNE course, and know the importance of these in achieving the learning outcomes.
Understand how adult learning principles are used to achieve a person centred and empowering style.
Observe the important individual and group processes and understand what behaviours of the Educators can promote or inhibit these.
Understand the key DAFNE principles of carbohydrate estimation and insulin regime / dose adjustment.
Prior to the observation week The DEP/DDP Trainees have been provided with your contact details in their Personal Training Plan. DEP Trainees have been advised to contact the DAFNE Educator(s) delivering the patient course that they will observe at least 1 week prior to the course to confirm venue / times, etc. They have also been instructed to arrive around 30 minutes before the start of day 1 to undergo a briefing session with you. Central DAFNE Administration will send the following resources to your centre for the DEP/DDP Trainee(s) that will be observing your course, which are to be handed to the trainees before the patient course commences on day 1:
DAFNE Patient Course Curriculum (DEP Trainees only, not DDP Trainees)
A folder containing a DAFNE Handbook, CP booklet, Diary, Quiz and DAFNE Attitude 15 Questionnaire.
At the beginning of the week – Briefing Session When you meet the DEP/DDP Trainees on the morning of day 1 (as organised prior to the observation week) please provide the trainees with a:
Curriculum (if appropriate) and folder as mentioned above.
Timetable for the course they are about to observe.

DAFNE © T01.002, Version 10 – October 2010 385
Note: If during the week the timetable is changes (eg schedule of sessions altered, sessions dropped) you must inform the Trainees why this has occurred. If a session has been dropped (eg pregnancy in an all male group of patients) the Trainees must be allowed to ask questions about the missed session and see lesson plans. Likewise if the timing of a session over or under runs, the Trainees should be made aware of why this has occurred.
Copy of a dose adjustment form. Check that Trainees have brought their DEP File and have:
Sufficient copies of the observation sheets (section 3.7 of the DEP file) and remind them that they must complete these for every session relevant to their discipline and all lunch time and dose adjustment sessions.
Case study guidelines (section 3.4 of the DEP file). Ensure that Trainees have access to your lesson plans to compare with their curriculum (but not to copy). Inform the trainee(s) that they:
Will be introduced to the group as observers (observing you, not the participants).
Should observe all timetabled sessions, including individual dose adjustments and lunchtimes and complete observation sheets for all these.
Should remain quiet during sessions and not interrupt/ participate in any way.
Will be allowed time in between sessions, when participants are out of the room, to make comments, ask questions or give general feedback. Agree with the trainees’ times throughout each day when they will be able to ask questions. It is essential that trainees have ample opportunity to ask you any questions they may have on a daily basis throughout the course.
Should pick a participant for their case study at random from the list, and follow guidelines in section 3.4 of DEP file.
Please insert the following into each of the DAFNE folders:
Timetable for the course that will be observed.
A copy of the dose adjustment forms that your patients will be using during the week.

DAFNE © T01.002, Version 10 – October 2010 386
The observation of DAFNE courses
Introduction Your DAFNE patient courses will often be observed by a variety of healthcare professionals. These observers will fall into1of 3 categories: 1. Trainee DAFNE educators and doctors observing the patient courses as part of the DAFNE
Educator Programme (DEP) and DAFNE Doctor Programme (DDP).
The philosophy underpinning the DAFNE Collaborative is the spread of DAFNE throughout the UK. It is therefore expected that all DAFNE centres open their patient courses to individuals completing the DEP and DDP.
2. Peer review as part of your centre’s 3 yearly Quality Assurance audit.
During your audit peer review, there should be no other observers on your patient course. You will be informed by Central DAFNE Administration at least 3 months in advance, which of your patient courses will be audited.
3. Casual observers, these may be either
Local colleagues to increase DAFNE awareness.
HCP from other centres that have shown an interest in DAFNE, but who are not training to become DAFNE educators.
Priority We request that QA peer review and individuals completing the DEP/DDP have priority over scheduled casual observers for observation places. Casual observers must be made aware at the time of booking their observation course that this may be cancelled at short notice should the observation places be required for the DEP/DDP. General Information It is essential that all DAFNE centres and educators are aware of what is expected of them when a DAFNE course is being observed. Regardless of why the individual(s) is observing your course it is essential that the following factors are considered and acted upon. Patient needs are paramount All observers must be reminded that they are there merely to observe and not to participate in the course. Observers should not interrupt/create a disturbance/ask questions during the sessions. Any questions can be fielded at break-times or at the end of the day. Patients should also be made aware of who the observers are and their reason for being there. It is essential that the patients are aware that the observers are not there to observe them. Educator needs It is essential that the educators delivering the observation course are experienced and comfortable being observed by their peers. It is unreasonable to expect newly trained educators to be observed when they have only delivered a few patient courses themselves. For this reason we recommend that, other than the purpose of peer review/audit, the first 4 courses that an educator delivers should not be observed by others.

DAFNE © T01.002, Version 10 – October 2010 387
Educators delivering the observation course must be informed of the number, names and reason for the observers’ presence. The number of observers on any particular session of the course should be kept to a minimum so as not to affect the patient/educator group dynamics. It is recommended that the number of observers does not exceed 3. The following pages give further details of what is to be provided for the various individuals that might observe a course.

DAFNE © T01.002, Version 10 – October 2010 388
Individuals observing as part of the DEP/DDP The first part of the training for new DAFNE educators and Doctors involves observing a full 5-day patient course delivered by experienced DAFNE educators in an established DAFNE centre. All DAFNE centres are expected to open their patient courses for observation. Central DAFNE Administration is responsible for the booking of observation courses for individuals completing the DEP and DDP and will liaise with the local DAFNE Administrator and/or unit lead DAFNE educator when booking the courses and will provide names and contact details of the scheduled observers. Each DAFNE centre should notify Central DAFNE Administration of: 1. Dates of all planned DAFNE courses. 2. Names of the educators scheduled to deliver each course and whether they have delivered
>4 patient courses. 3. Details of courses scheduled to be observed by casual observers. Central DAFNE Administration will try to avoid using these courses for the DEP/DDP when at all possible. However in certain circumstances (e.g. shortage of patient courses for observation, last minute trainee recruitment) it may be unavoidable to use courses that have already allocated for casual observation. Prior to observation week Observers have been advised to contact educator(s) at least 1 week prior to the course to confirm venue/times, etc. It is recommended that they arrive around ½ hour before the start of day 1 to undergo a briefing session. Central DAFNE Administration will forward to you resources that the observers will require for the observation week. You will receive the following resources 2-4 weeks before the observation course for each observer: Trainee educators: 1 x copy of the DAFNE patient course curriculum 1 x DAFNE folder containing: 1 x DAFNE patient workbook, including quiz 1 x DAFNE CP booklet 1 x DAFNE patient blood glucose monitoring diary 1 x Attitude 15 Questionnaire Trainee doctors 1 x DAFNE folder containing: 1 x DAFNE patient workbook, including quiz 1 x DAFNE CP booklet 1 x DAFNE patient blood glucose monitoring diary 1 x Attitude 15 Questionnaire When these resources are received, please insert the following into each of the DAFNE folders:
Timetable for the course that will be observed.
A copy of the dose adjustment forms that your patients will be using during the week.
DAFNE © T01.002, Version 10 – October 2010 389
At beginning of the week Check that observers have brought their DEP file including the case study guidelines and have photocopied sufficient observation sheets for each session of the course. Supply each observer with the resources mentioned above.
Observers should have access to your lesson plans to compare (not to copy) with their curriculum.
Briefing
Explain that they will be introduced to the group as observers (observing YOU, not the participants).
They should observe all timetabled sessions, including individual dose adjustments and lunchtimes and complete observation checklists for all these.
They should complete their photocopied observation sheets (page 24 – 25 of their DEP file) for each session of the course; these will be required during the 2-day workshop.
They should remain quiet during sessions.
They will be allowed time in between sessions, when participants are out of the room, to make comments, ask questions or give general feedback.
Observers should pick a participant for their case study at random from the list, and follow guidelines on page 22 of their DEP file.

DAFNE © T01.002, Version 10 – October 2010 390
Quality Assurance Peer Review All DAFNE centres are subjected to a quality assurance audit every three years, the first audit being 3 years after you diabetes unit commenced offering DAFNE courses. If you are at all unsure when your first or next audit is due please contact Central DAFNE Administration office. The audit currently involves: 1. Peer review of a full 5-day patient course by an experience DAFNE educator from another
DAFNE centre. 2. Completion of the Quality Assurance Audit questionnaire.
Prior to observation week You will be contacted approximately 3 months prior to your audit visit by Central DAFNE Administration to confirm which of your patient courses will be peer reviewed and to obtain details of the venue. Central DAFNE will also confirm the name of your peer reviewer. There should be no additional observers during the peer review course. The peer reviewer is not there to assess the educators delivering the course, but to ensure that the DAFNE curriculum is being delivered by your centre. The peer reviewer will not interrupt and participate in the DAFNE course at all. At beginning of the week Please ensure that the peer reviewer receives a copy of the timetable for the course being reviewed at the start of the course. The educators delivering the course should have their lesson plans available for the peer reviewer to refer to as requested. The peer reviewer does not require, and will not remove, any resources from your centre. Briefing At the end of end of the 5-day course the peer reviewer will feedback their observations to the educators/DAFNE team.
DAFNE © T01.002, Version 10 – October 2010 391
Casual observers - DAFNE awareness. Casual observers may be either local colleagues or healthcare professionals from other units who want to increase their DAFNE awareness, but who are not training to become DAFNE educators. The observation by casual observers will organised at a local level. However you will need to inform Central DAFNE Administration of any casual observers so that, if at all possible, they can avoid using these courses for observation courses for DEP/DDP. In certain circumstances (e.g. shortage of patient courses for observation, last minute trainee recruitment) Central DAFNE Administration may request the use a course for DEP/DDP observation that you have already allocated to colleagues. It is therefore recommended that you make casual observers fully aware when booking their observation course that you may have to cancel this at short notice and the reason why this may happen. Central DAFNE Administration will however try to minimise such disruption. Casual observers are not to be provided with any DAFNE resources. Central DAFNE Administration have provide each DAFNE centre with 2 copies of the following reference resources which observers may use during the observation week.
DAFNE patient handbook
DAFNE patient quiz
DAFNE CP booklet
DAFNE patient blood glucose monitoring diary It is essential that the educators delivering the course ensure that these resources are not removed from the classroom or photocopied and are returned by observers at the end of the session/day. All casual observers must be made aware that they observing a DAFNE course do not make them DAFNE educators. Should any of your casual observers decide to complete the DEP/DDP at a later stage, they should be aware that they will need to observe a further 5-day course as part of the DEP. Under no circumstances will casual observation qualify as completion of the DEP observation course. Central DAFNE Administration has provided each centre with 6 copies of an information sheet aimed at casual observers outlining the points above. Further copies can be obtained from Central DAFNE. Casual observers should be provided with a copy of the information sheet when they book their observation course. They should be provided with a further copy at the beginning of their observation course.

DAFNE © T01.002, Version 10 – October 2010 392
DEP REVIEWERS BUDDY LIST
DEP REVIEWERS
Surname First name Email Telephone
Adcock Judy [email protected] 020 8333 3091
Ashton-Cleary Siobhan [email protected] 0115 924 9924 x 37317
Baillie Jane [email protected] 01223 586761
Barrass Jean [email protected] 01892 633943
Beckwith Anita [email protected] 0203 299 1812
Bennion Jane [email protected] 0161 627 8268
Bhachu Pavita [email protected] 0208 522 9859 07535647709
Breen Cathy [email protected] 00353 1 2115156
Callaby Karen [email protected] 01223 586668
Cassidy Sharon [email protected] 01482 675373 07909527738
Chandrasekharan Lakshmi [email protected] 01702 385331
Clark Susan [email protected] 0191 333 2705
Cowling Pauline [email protected] 0114 271 4162
Dewhurst Anne-Marie [email protected] 01304 865443
Donald Sarah [email protected] 01223 216655
Doran Lynn [email protected] 01236 713129
Gandham Sri [email protected] 01745 534058
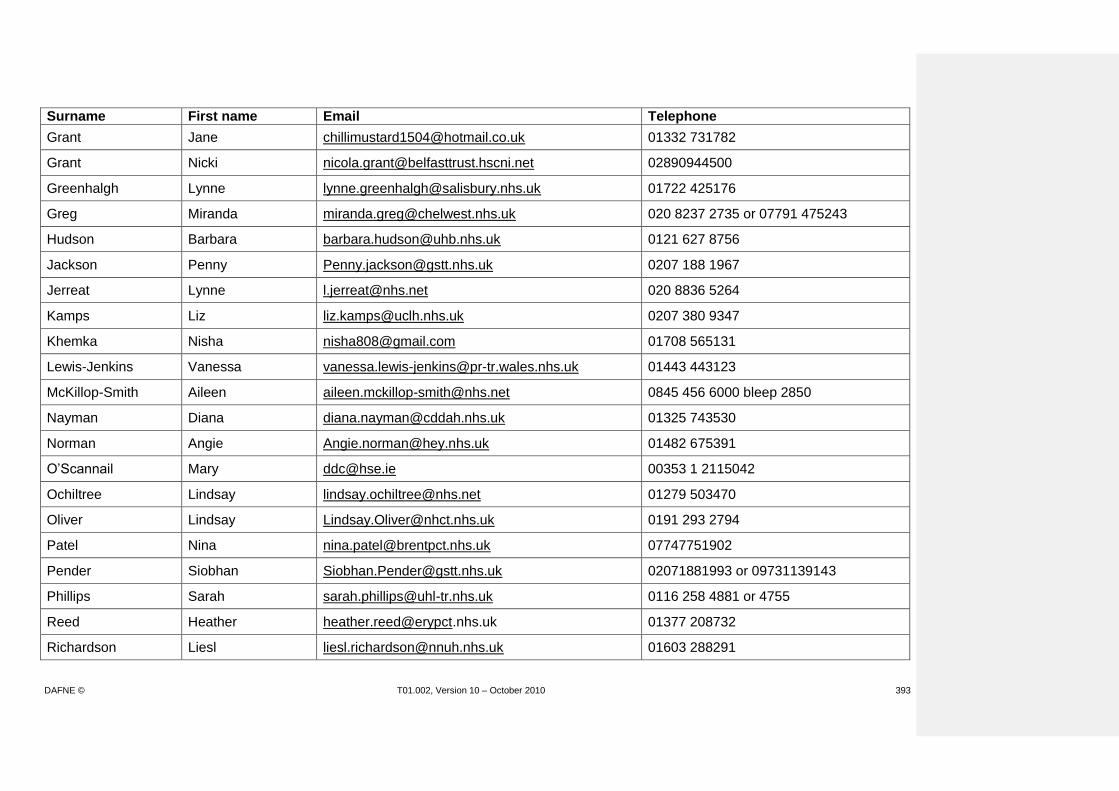
DAFNE © T01.002, Version 10 – October 2010 393
Surname First name Email Telephone
Grant Jane [email protected] 01332 731782
Grant Nicki [email protected] 02890944500
Greenhalgh Lynne [email protected] 01722 425176
Greg Miranda [email protected] 020 8237 2735 or 07791 475243
Hudson Barbara [email protected] 0121 627 8756
Jackson Penny [email protected] 0207 188 1967
Jerreat Lynne [email protected] 020 8836 5264
Kamps Liz [email protected] 0207 380 9347
Khemka Nisha [email protected] 01708 565131
Lewis-Jenkins Vanessa [email protected] 01443 443123
McKillop-Smith Aileen [email protected] 0845 456 6000 bleep 2850
Nayman Diana [email protected] 01325 743530
Norman Angie [email protected] 01482 675391
O’Scannail Mary [email protected] 00353 1 2115042
Ochiltree Lindsay [email protected] 01279 503470
Oliver Lindsay [email protected] 0191 293 2794
Patel Nina [email protected] 07747751902
Pender Siobhan [email protected] 02071881993 or 09731139143
Phillips Sarah [email protected] 0116 258 4881 or 4755
Reed Heather [email protected] 01377 208732
Richardson Liesl [email protected] 01603 288291

DAFNE © T01.002, Version 10 – October 2010 394
Surname First name Email Telephone
Rogers Helen [email protected] 020 3299 1717
Smith Fiona [email protected] 01709 307910
Smith Julie [email protected] 01262 423154
Taylor Carolin [email protected] 0114 271 4445 / 07977007118
Thompson Thea H = [email protected] W = [email protected]
W = 0208 4532482 M= 079313 05009
Valette Marielle [email protected] 01234 792313
Wardynec Carol [email protected] 01946 523009
Williams Lis [email protected] or [email protected]
07957202886
Wood Liz [email protected] 0191 333 2551
Woolgar Sally [email protected] 01723 342415

DAFNE © T01.002, Version 10 – October 2010 395
QUALITY ASSURANCE FOR DAFNE LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should….
DISCUSS ACETATES AND ANSWER ANY QUESTIONS / QUERIES.
Understand the purpose and process of Quality Assurance in the DAFNE programme Understand that all registered Educators must be involved in QA at least at an internal level. Know that they can train to become peer reviewers
Discuss role of Lead Educator. Explain requirement for continued ‘registration’ is to teach at least 1 course every 6 months. Emphasise that they will need to contribute to internal QA and PDP development. At least 1 Educator in each centre will need to be trained in the process/documentation, this is often the lead Educator, but it is ultimately everyone’s responsibility. It is essential for everyone to take part in internal QA and it is recommended that you try to do some each time you deliver a course. Explain that internal QA needs to be ongoing and that each centre will be externally Quality Assured every 3 years. The auditor will need to look at their observation sheets from their internal QA. Explain that having completed 4 DAFNE courses they can train to become peer reviewers in order to train their educator colleagues for internal peer review and take part in the external peer review programme Explain that internal peer review is done using the same paperwork that the peer reviewer used for new educators.
Acetates: ‘DoH Structured Education Criteria’ ‘Quality Assurance (Internal-ongoing)’ ‘Quality Assurance (External)’
DAFNE © T01.002, Version 10 – October 2010 396

DAFNE © T01.002, Version 10 – October 2010 397
Quality Assurance
(Internal - ongoing)
• Educator (&Dr) PDPs (based on peer-reviewed course
documentation)
• Local 3-yearly programme of ‘colleague review’ using P-R
documentation (additional training in use of paperwork)
• Involve all Educators in local reviewing (not just
responsibility of Lead Educator)
• Minimum requirement of each Educator teaching 1 course
every 6 months
DAFNE © T01.002, Version 10 – October 2010 398
Quality Assurance
(External)
• 3-yearly Centre ‘Report’ and ‘Review’
Report Questionnaire (Lead Educator / Physician):
• Outcome data (database)
• Courses run / patients trained
• DEP & Training commitments
Review (visit from external Auditor):
• Observe & report on ½ day of course re planning and running of course(s)
• Use P-R paperwork & compare to internal QA
• Meeting with Lead Educator to review progress with individual PDPs
FUTURE CONTRIBUTION TO DAFNE COLLABORATIVE ONGOING EDUCATOR SUPPORT NETWORK
LEARNING GOALS METHODS MATERIALS/MEDIA

DAFNE © T01.002, Version 10 – October 2010 399
Participants should….
Understand the remit of the DAFNE Collaborative Be aware of the Educator support network
DISCUSS ACETATE Explain that the Collaborative Meeting (2nd Friday in July each year) is open to anyone, but usually only space for 2 representatives from each centre each year. Explain that all Educator and Dr details can be found in the Centre Manual and that Educators should feel able to contact others as required. Discuss the proposed (local) networks of Educators and the roles of the groups (when agreed / available).
Acetate: ‘Remit of the DAFNE Collaborative’ Centre Manual Acetate (when agreed / available)
DAFNE © T01.002, Version 10 – October 2010 400
Remit of the DAFNE Collaborative
Full remit presented in Section 3 of the DAFNE Centre Manual:
• Ensure DAFNE successfully implemented in all DAFNE centres
• Training new DAFNE centres via the DEP and DDP
• Patient courses available as observation courses
• DAFNE Trainers, Peer Reviewers and Auditors
• Implement the DAFNE QA programme.
• Audit
• ‘Unpacking' DAFNE, what does and does not work (further research).
• Development of DAFNE programme and resources
• Promotion of DAFNE to colleagues

DAFNE © T01.002, Version 10 – October 2010 401
EVALUATION OF DEP AND PERSONAL PLAN LEARNING GOALS METHODS MATERIALS/MEDIA
Participants should …..
Reflect on their priorities for the follow up workshop and identify if these have been met
Refer to flip charts from Introduction / Unresolved Issues sessions Discuss each priority topic in turn. Has it been met/achieved? If not, why not? Could it have been achieved?
Flip charts
Complete a DEP evaluation form
Participants each complete evaluation form.
DEP Evaluation
Leave feeling prepared for their tasks and course delivery over the following weeks / months
Check/ask if anything further to discuss either as a group or individually. Provide ‘Personal Plan’ for each participant to complete in their own time.
Personal Plan (following peer reviewed course) handouts
DAFNE © T01.002, Version 10 – October 2010 402
DAFNE EDUCATOR PROGRAMME (DEP) 1-DAY FOLLOW-UP
Date and venue Evaluation form
Having completed the DEP, how would you rate it overall (circle 1)?
Excellent Very Good Good Poor Please comment: Are there any parts you would like to make particular comments on (ie what worked/went well, what did not work/go well)? Pre-course preparation and reading: Observation week: Training workshop:

DAFNE © T01.002, Version 10 – October 2010 403
Peer-reviewed course: Follow-up workshop: Do you have any suggestions for future changes to the workshop (if required)?
Thank you very much and good luck with your DAFNE courses!
Name: ...................................................................................

DAFNE © T01.002, Version 10 – October 2010 404
Personal Plan Following Peer-Reviewed Course
What do I personally need to do between now and my next DAFNE courses? Consider: Time required:
Patient recruitment and preparation:
Room / catering organisation:
Preparation of resources:
PTO
DAFNE © T01.002, Version 10 – October 2010 405
Preparation of lesson plans:
‘Team’ organisation:
Any unresolved issues / training needs: