d & h cross roads
DESCRIPTION
cardiologyTRANSCRIPT
Hypertension
Diab
etes
Hypertension &DiabetesCross Roads

• 42% of people with diabetes had normal BP • 56% of people with hypertension had normal glucose tolerance
A prospective cohort study in the United States reported that type 2 diabetes mellitus was almost 2.5 times as likely to develop in subjects with hypertension as in subjects with normal blood pressure

Etiology
DYSLIPIDEMIA DIABETES HYPERTENSION
Increased FFA & triglycerides, Apo B-100 , CETP, MTP,HL, LPL
High leptin,low adiponectin,low vislatin,omentin,vaspin, Increased TNF-alpha & IL-6, high retinol binding protein-4,FFA(via DAG & ceramides
VLDL, triglycerides, sdLDL, HDL, Apo -A1
Incresed FFA, DecreasedNO , RAS activation & aldosterone
Glucotoxicity,lipotoxicity,Inflamtion, endoplasmic reticulum stress
vasoconstriction
leptin, insulin, aldosterone, RAS
Systemic sympathetic activityImpaired Beta cell fuction&
decreases insulin resistance

Genetic FactorsAcquired factorsCentral adiposeEctopic lipid
Environmental factorsDietExercise
Inflammatory oxidative Stress Insulin resistance
Hyperglycemia Dyslipidemia Hyperinsulinemia
RAASVascular dysfunction Sodium
retention SNS
Hypertension

5.5 million people died of stroke in 2002
50% of these were from ASIA (Pakistan, India , China)
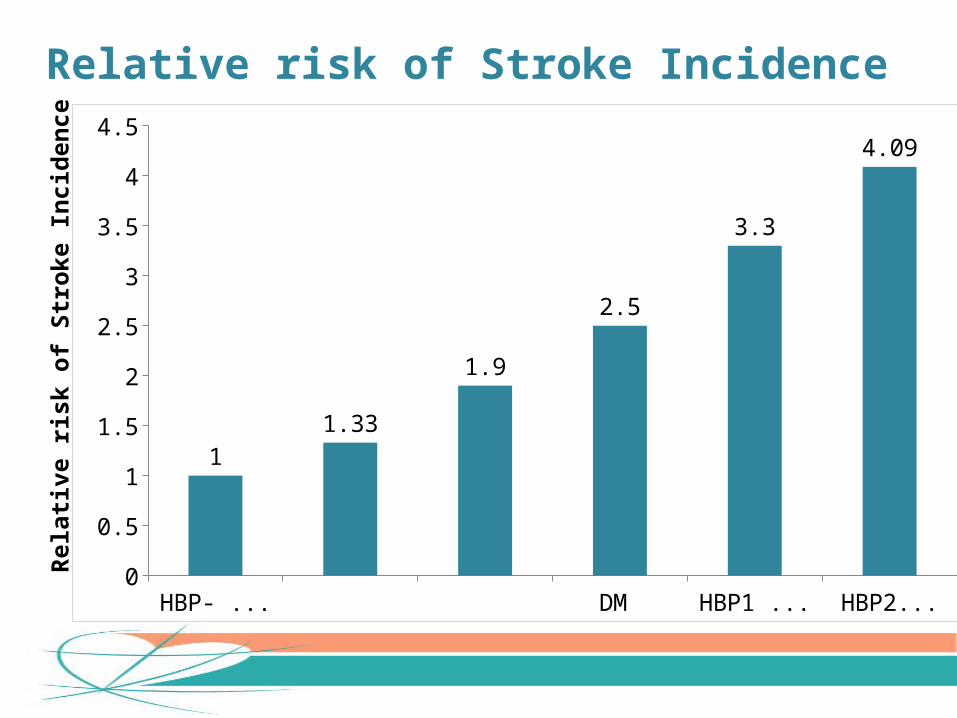
HBP- & DM HBP1 HBP2 DM only HBP1 & DM HBP2 &DM0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
11.33
1.9
2.5
3.3
4.09
Rela
tive
risk
of S
trok
e In
cide
nce
Relative risk of Stroke Incidence

<120 120-139 140-159 160-170 180-190 >2000
50
100
150
200
250
300
No daibetesDiabetes
Double jeopardy: Diabetes & Hypertension and Cardiovascular Risk

23.1%
76.8%
0
20
40
60
80
100
Patients with no cardiovascular disease co-morbidities
Patients with diabetes
Hypertension and Diabetes often coexist
Wong et al. Arch Intern Med 2007; 167:2431-2436

0
5
10
Major CV Events
Incidence per 1000 patients
Hypertension without diabetes (n=17,289)Hypertension with diabetes (n=1501)
Stroke CV Mortality
15
CV Mortality
J Hypertens 2001
Co-morbid diabetes significantly increases the risk of CV events in patients with Hypertension:HOT Study
Men Women0
5
10
15
20
25
30
35
40
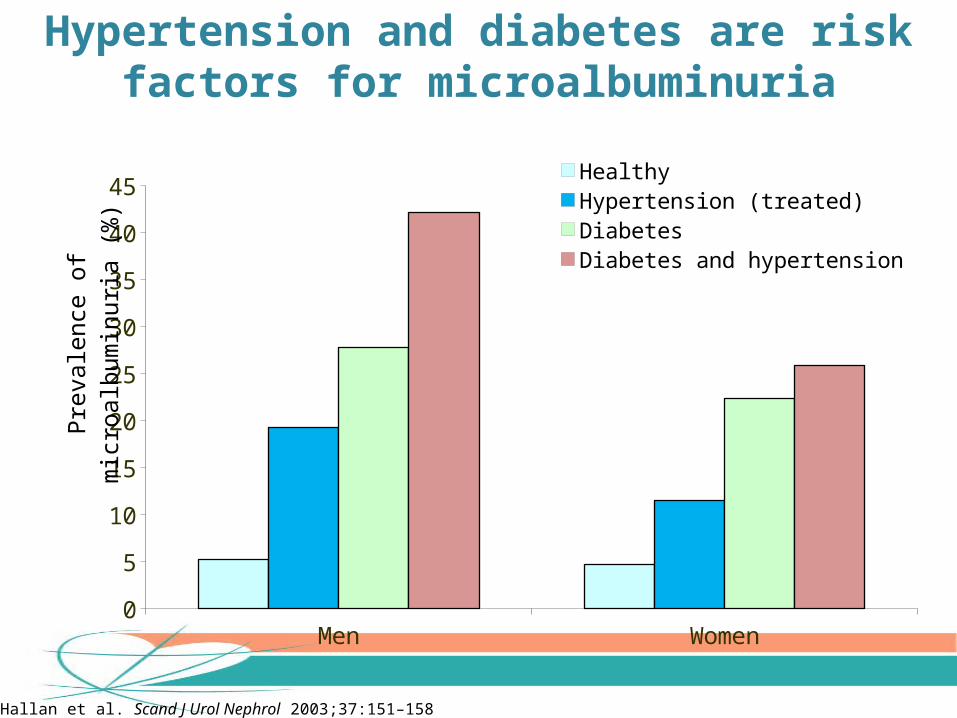
45HealthyHypertension (treated)DiabetesDiabetes and hypertension
Pre
vale
nce
of m
icro
albu
min
uria
(%
)
Hallan et al. Scand J Urol Nephrol 2003;37:151–158
Hypertension and diabetes are risk factors for microalbuminuria

36.7%
43.5%
0
20
40
60
<140/90 mmHg
Proportion of patients achieving BP goal (%)
13.2%
20.8%
10.5%
14.1%
Hypertension without diabetes (n=3156)Hypertension with diabetes (n=853)
<130/85 mmHg <140/90 mmHg
Cross Road of HTN & DM and likelihood of achieving BP control rates
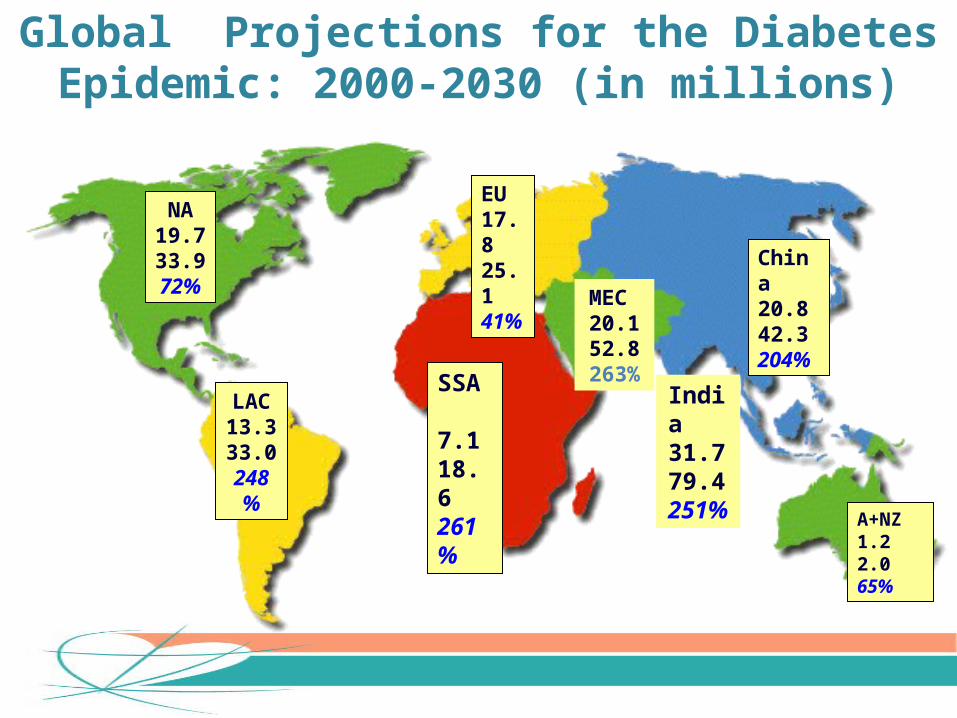
NA19.733.972%
LAC13.333.0248%
SSA 7.118.6261%
EU17.825.141%
MEC20.152.8263%
India31.779.4251%
China20.842.3204%
A+NZ1.22.065%
Global Projections for the Diabetes Epidemic: 2000-2030 (in millions)
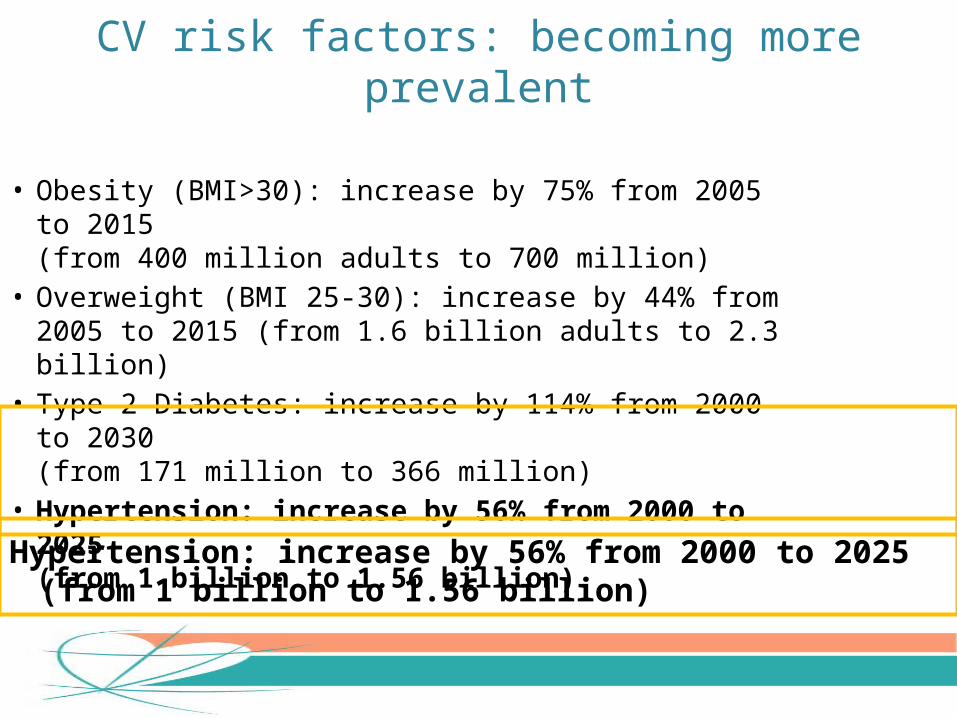
• Obesity (BMI>30): increase by 75% from 2005 to 2015 (from 400 million adults to 700 million)
• Overweight (BMI 25-30): increase by 44% from 2005 to 2015 (from 1.6 billion adults to 2.3 billion)
• Type 2 Diabetes: increase by 114% from 2000 to 2030 (from 171 million to 366 million)
• Hypertension: increase by 56% from 2000 to 2025 (from 1 billion to 1.56 billion)
Hypertension: increase by 56% from 2000 to 2025 (from 1 billion to 1.56 billion)
CV risk factors: becoming more prevalent

Blood Pressure Reduction of 2 mmHg Decreases the Risk of Cardiovascular Events by 7–10%
7% reduction in risk of ischaemic heart disease mortality
10% reduction in risk of stroke mortality
2 mmHg decrease in mean SBP
Lewington et al. Lancet 2002;360:1903–13
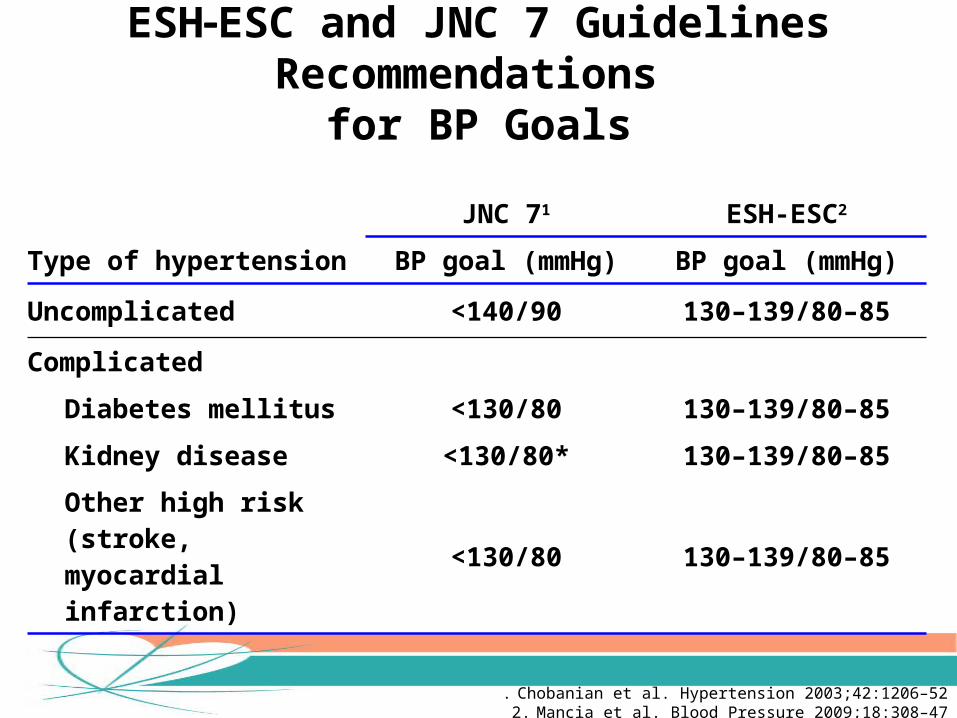
JNC 71 ESH-ESC2
Type of hypertension BP goal (mmHg) BP goal (mmHg)
Uncomplicated <140/90 130–139/80–85
Complicated
Diabetes mellitus <130/80 130–139/80–85
Kidney disease <130/80* 130–139/80–85
Other high risk (stroke, myocardial infarction)
<130/80 130–139/80–85
. Chobanian et al. Hypertension 2003;42:1206–522. Mancia et al. Blood Pressure 2009;18:308–47
ESHESC and JNC 7 Guidelines Recommendations for BP Goals

BP ClassificationLifestyle Modification
Initial Drug Therapy
Without Compelling Indication
With Compelling Indication
Normal<120/80 mm Hg
Prehypertension120-139/80-89 mm Hg
Stage 1 hypertension140-159/90-99 mm Hg
Stage 2 hypertension160/100 mm Hg
Encourage
Yes
Yes
Yes
No drug indicated Drug(s) for the compelling indications
Thiazide-type diuretics for most; may consider ACE-I, ARB, BB, CCB, or combination
2-drug combination for most (usually thiazide-type diuretic and ACE-I, ARB, BB, or CCB)
JNC VII: First line recommendations for antihypertensive

RAAS Blockade as Foundation Therapy in Hypertension

ARB Foundation
CCBAlpha
BlockersBeta
Blockers Diuretics Others
RAAS blockade with ARBs can be considered a Foundation of Antihypertensive Therapy
Weir. Am J Hypertens 1998;11:163S-9SDzau. J Hypertens 2005;23 (Suppl. 1): S9-S17
Sica et al. J Clin Hypertens 2002;4:52-7

Rationale for selective angiotensin type 1 receptor blockade
Bradykinin
Inactive fragments
ANGIOTENSIN I
ANGIOTENSIN II
ARB
AT1 RECEPTOR
VasoconstrictionSodium retention
SNS activationInflammation
Growth-promoting effects
AT2 RECEPTOR
VasodilationNatriuresis
Tissue regenerationInhibition of inappropriate
cell growth
Chymase, tPA, ‘Angiotensin II
escape’ACE inhibitor

RAAS
AtherosclerosisVasoconstrictionVascular hypertrophyEndothelial dysfunction
LVHFibrosisRemodeling
GFRProteinuriaAldosterone releaseGlomerular sclerosis
Stroke
Hypertension
Heart failureMyocardial infarction
Renal failure
DEATH
RAAS Plays an Important Role in Organ Damage & CV Outcomes
Willenheimer et al. Eur Heart J 1999;20:997–1008 Dahlöf et al. J Hum Hypertens 1995;9 (Suppl 5):S37–44
Fyhrquist et al. J Hum Hypertens 1995;9 (Suppl 5):S19 –24 Fogo. Am J Kidney Dis 2000;35:179–88
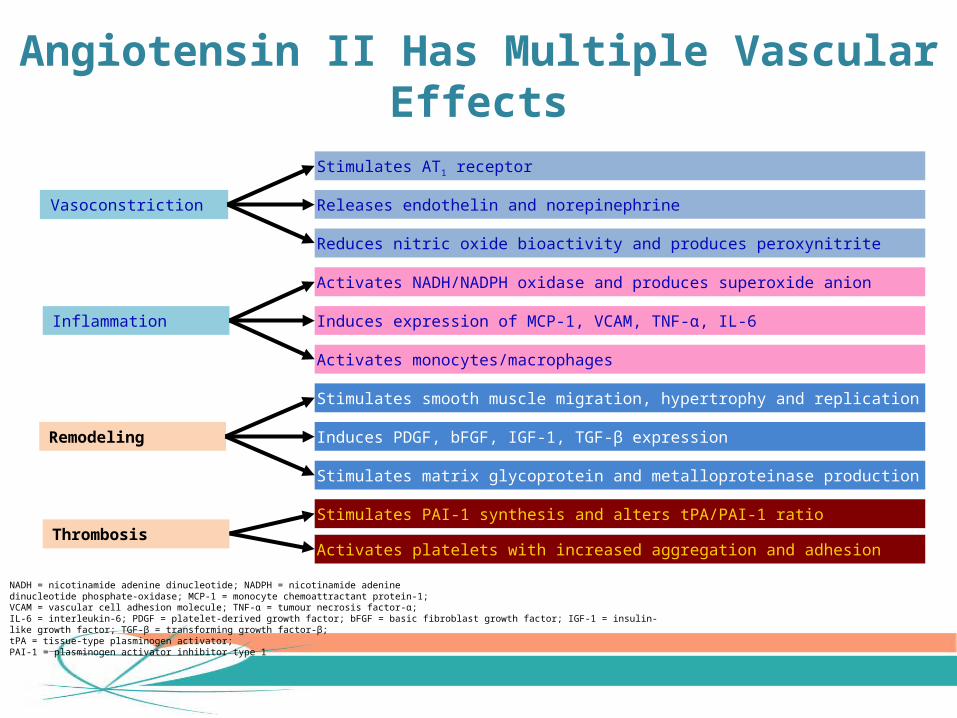
Vasoconstriction
Inflammation
Remodeling
Thrombosis
Stimulates AT1 receptor
Releases endothelin and norepinephrine
Reduces nitric oxide bioactivity and produces peroxynitrite
Activates NADH/NADPH oxidase and produces superoxide anion
Induces expression of MCP-1, VCAM, TNF-α, IL-6
Activates monocytes/macrophages
Stimulates smooth muscle migration, hypertrophy and replication
Induces PDGF, bFGF, IGF-1, TGF-β expression
Stimulates matrix glycoprotein and metalloproteinase production
Stimulates PAI-1 synthesis and alters tPA/PAI-1 ratio
Activates platelets with increased aggregation and adhesion
NADH = nicotinamide adenine dinucleotide; NADPH = nicotinamide adenine dinucleotide phosphate-oxidase; MCP-1 = monocyte chemoattractant protein-1; VCAM = vascular cell adhesion molecule; TNF-α = tumour necrosis factor-α;IL-6 = interleukin-6; PDGF = platelet-derived growth factor; bFGF = basic fibroblast growth factor; IGF-1 = insulin-like growth factor; TGF-β = transforming growth factor-β;tPA = tissue-type plasminogen activator;PAI-1 = plasminogen activator inhibitor type 1
Angiotensin II Has Multiple Vascular Effects

Price DA et al. Am J Hypertens (1999) 12, 348–355
RAAS activity in response to a high-salt diet and recumbent position
‡P<0.01 vs. healthy subjects
Hypertensive Diabetic Patients have an Inappropriately Activated RAAS
Healthy Non-Diabetic DiabeticSubjects Hypertensives Hypertensives
N=23 N=104 N=36
2.0
1.5
1.0
0.5
0
RAAS
Acti
vity
as
mea
sure
d by
PR
A (n
g/m
L/m
in)
‡

Hypertensive Diabetic Patients have an Exaggerated Vascular Response to Ang II
‡P<0.01 vs. healthy subjects* P<0.01 vs. non-diabetic hypertensives
Gordon et al. J Renin Angiotensin Aldosterone Syst. 2000;1(3):252-6
BP response to Ang II infusion
Healthy Non-Diabetic DiabeticSubjects Hypertensives Hypertensives
N=61 N=158 N=38
Chan
ge in
Mea
n Ar
teria
l Pr
essu
re (m
mH
g)
‡ *
‡
15
10
5
0

• ARBs provide a more specific and selective blockade of the effects of angiotensin II than ACE inhibitors
• ARBs tend to have more favourable tolerability than ACE inhibitors
• Unlike ACE inhibitors, ARBs do not disrupt bradykinin degradation, leading to a much lower incidence of treatment-related cough
McClellan KJ, Goa KL. Drugs 1998; 56: 847–869.
Benefits of ARBs over ACE inhibitorsBenefits of ARBs over ACE inhibitors

ARBs are Associated with Higher Adherence Rates Compared with Other Antihypertensive
Drug ClassesA retrospective cohort study analysing claims from
62,754 patients in the German Sickness Fund
Adapted from Höer A et al. J Hum Hypertens 2007;21:744–6
Adhe
renc
e (m
edic
ation
po
sses
sion
ratio
)
ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; CCB = calcium channel blocker; MPR = medication possession ratioMean (95%CI) MPR: ARBs 0.697 (95%CI:0.686–0.707); ACEIs 0.556 (0.550–0.562); beta-blockers 0.385 (0.382–0.388); CCBs 0.540 (0.531–0.548); diuretics 0.533 (0.525–0.541)
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
ARB ACEI CCB Diuretic Beta blocker

Study nFollow Up
Period BP (mmHG) Drugs Tested Impact on Outcome
Years
UKPDS 510220 Tight Goal150/85 versus
<180/105 Captopril /Atenolol Favors tight control
HOT 187903.8 DSP goal 80 Vs < 90
CCB + others Favors tight control
HOPE,MICRO HOPE 9297 (3577 with
diabetes)
3.5 Mean BP for Both 139/79
Ramipril Vs placebo
Ramipril decreased Mortality & morbidity
ALLHAT42418 (13101) with daibetes)
4.9 Mean BP 146/83 aat baseline Amlodipine Vs Lisinopril
Increased heart failure with amlodipine
ABCD 4705 DSP Intensive 75 Vs moderate
<80-89Nisoldipine Vs enapril
Intensive group decreased death
ACCORD BP 47334.7 SBP <120 Vs <140 Stepped care tp reach
goal
No difference in mortality & morbidity
ON TARGET
25620 (6392 with Diabetes & Organ
Damage)
5.5 141.8±17.4/82.1±10.4 on baseline
Telmesartan Vs Ramipril
Equal in Outcomes but safety is better with telmesartan
Clinical Trials of BP Medication in Patients with Diabetes

ARB CV outcome studies in hypertensive patients – evidence unclear
LIFE• Losartan reduced incidence of stroke compared with atenolol in
patients with severe hypertension and LVH1
• However, atenolol is a weak comparator since it provides poor CV protection compared with all other antihypertensive classes2
VALUE• Valsartan was not better than amlodipine in reducing CV risk in
patients with hypertension and risk factors3
• Valsartan was significantly worse than amlodipine on the incidence of MI
1. Dahlöf B et al. Lancet 2002; 359:995-10032. Carlberg et al. Lancet 2004;364:1684–93. Julius S, et al. Lancet. 2004;363:2022-31
ARB CV outcome studies in hypertensive patients – evidence unclear

ARB CV outcome studies demonstrate effectiveness in heart failure
• Three key ARB trials have shown the effectiveness of ARBs in patients with heart failure
– Val-HeFT and VALIANT showed that valsartan is effective in patients with heart failure or patients with heart failure/LV dysfunction after a recent MI*, respectively
– CHARM showed candesartan is also effective in heart failure
1. Pfeffer MA, et al. N Engl J Med 2003;349:1893-906; 2. Cohn JN, et al. N Engl J Med 2003;345;1667-75;3. Pfeffer MA, et al. Lancet 2003 362: 759–66;
* VALIANT (VALsartan In Acute myocardial iNfarction Trial) was conducted in clinically stable patients with symptomatic heart failure or asymptomatic left ventricular systolic dysfunction after a recent (12 hours – 10 days) myocardial infarction.
ARB CV outcome studies demonstrate effectiveness in heart failure
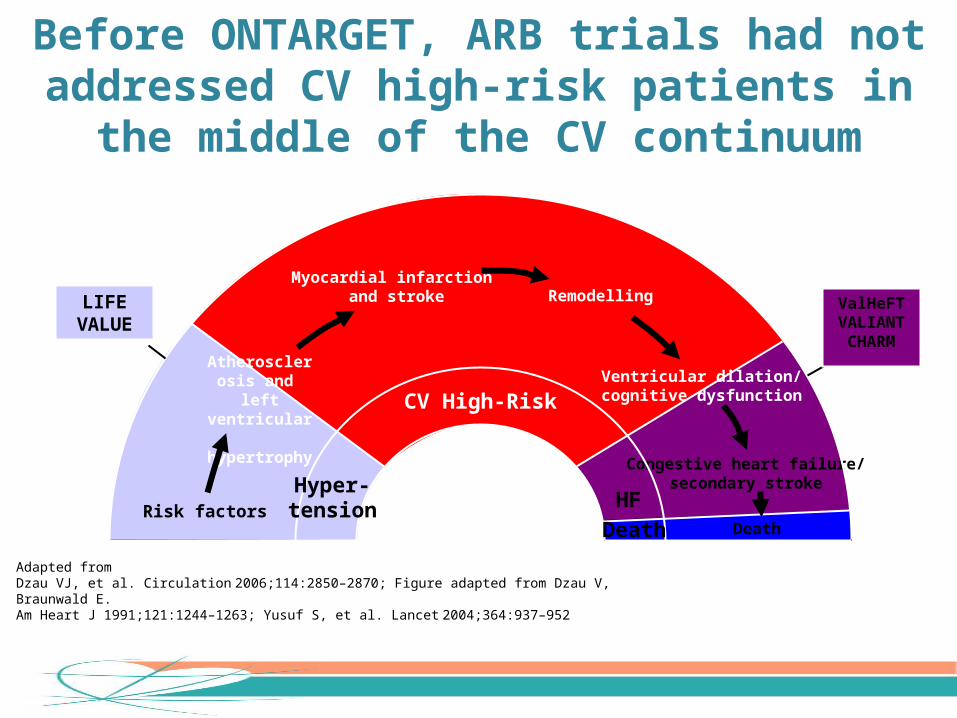
CV High-Risk
Death
Remodelling
Congestive heart failure/secondary stroke
Myocardial infarction and stroke
Hyper-tension
Atherosclerosis and
left ventricular hypertrophy
HFDeath
Ventricular dilation/cognitive dysfunction
Risk factors
LIFEVALUE
ValHeFTVALIANTCHARM
Before ONTARGET, ARB trials had not addressed CV high-risk patients in the middle of the CV continuum
Adapted fromDzau VJ, et al. Circulation 2006;114:2850–2870; Figure adapted from Dzau V, Braunwald E. Am Heart J 1991;121:1244–1263; Yusuf S, et al. Lancet 2004;364:937–952

Which ARB to reduce events in CV high-risk patients?
• Before ONTARGET, no ARB had been tested for protective
effects in CV high-risk patients
• To demonstrate effectiveness equal to the gold-standard
ramipril, an ARB with the optimal pharmacology was selected
• Telmisartan has a unique pharmacology among ARBs
• This translates to meaningful clinical benefit over other ARBs
Burnier M. JIMR 2009;37(6) e-publish ahead of print
Which ARB to reduce events in CV high-risk patients?

Telmesartan stands out in crowded contest
Burnier M. & Brunner H.R., Lancet 2000;355:637–645; Brunner H.R., J Hum Hypertens 2002;16(Suppl 2):S13–S16; Kakuta H., et al. Int J Clin Pharmacol Res 2005;25:41–46; Wienen W., et al. Br J Pharmacol 1993;110:245-252; Song J.C. & White C.M., Formulary 2001;36:487–499; Asmar,R., Int J Clin Pract. 2006;60:315-320; Israili,Z.H., J Hum.Hypertens. 2000;14 Suppl 1: S73-S86; Benson S.C. et al. Hypertension 2004;43:993–1002
Longest plasma half life Highest receptor affinity
0
20
40
60
80
100
Most lipophilic (high tissue penetration)
0
6
12
18
24Longest Plasma half life
Plas
ma
half
life
(h)
range
Epro-sartan
Lo-sartan
Val-sartan
Olme-sartan
Irbe-sartan
Telmi-sartan
0
50
100
150
200
250 † Active metabolite EXP 3174
Rece
ptor
dis
soci
ation
ha
lf lif
e (m
in)
†
Lo-sartan
Val-sartan
Olme-sartan
Telmi-sartan
Olme-sartan
Val-sartan
Lo-sartan
Irbe-sartan
Epro-sartan
Telmi-sartan
Volu
me
of d
istr
ibuti
on (L
)500
range
PPARg
fold
acti
vatio
n0
5
10
15
20
25
30
EXP 3174(Losartan)
Val-sartan
Olme-sartan
Telmi-sartan
Epro-sartan
Irbe-sartan
Longest half life, Highest receptor affinity, Highest tissue penetration and selective PPARg activation
Highest selective PPARg activation
Highest receptor Affinity

Telmisartan’s unique pharmacology translates to meaningful clinical benefit
0 13 26 39 521300
1500
1700
1900
2100Telmisartan 80 mg (n = 407)
Losartan 100 mg (n = 420)
Week
gMea
n U
PC (m
g/g
crea
tinin
e)
P = 0.03
Bakris et al. Kidney Int 2008; DOI:10.1038/ki.2008.204
n=860
39% more
proteinuria reduction with telmisartan

ONTARGET trial –CV High-Risk patients

n=8,502 Telmisartan 80 mg + Ramipril 10 mg
The ONTARGET Trial in CV High-Risk patients* – the largest ARB outcomes trial
n=8,542 Telmisartan 80 mg
n=8,576 Ramipril 10 mg
5.5 yearsFollow-up at 6 weeks and every 6 months
Teo K, et al. Am Heart J 2004;148:52–61; The ONTARGET Investigators. N Engl J Med 2008;358:1547–1559
*Age 55 years at high risk of a CVD event (i.e. with a history of: coronary artery disease, peripheral arterial occlusive disease (PAD), cerebrovascular event, or diabetes mellitus with end-organ damage)
The ONTARGET Trial in CV High-Risk patients* – the largest ARB outcomes trial

Years of follow-up
0.20
0.15
0.05
0.10
00 1 2 3 4 5
Cum
ulati
ve H
azar
d Ra
tio
8,4528,576
8,1778,214
7,7787,832
7,4207,472
7,0517,093
1,6871,703
No. at riskTelmisartanRamipril
TelmisartanRamipril
Telmisartan 80mg reduces devastating CV events similar to ramipril 10mg in CV High-Risk patients
Reduction in composite CV risk (Primary endpoint: cardiovascular mortality, non-fatal myocardial infarction, hospitalisation for congestive heart failure, non-fatal stroke)The ONTARGET Investigators. N Engl J Med 2008;358:1547–1559
Reduction in composite CV risk
‡p< 0.01 vs. non-inferiority margin (1.13)

Telmisartan is better tolerated than ramipril (ONTARGET study)
n at riskTelmisartanRamipril
8,5428,576
7,9547,796
7,3847,165
6,9096,681
6,4786,254
Ramipril (10 mg)
Telmisartan (80 mg)
Data on File (Boehringer Ingelheim GmbH)
Years offollow-up0 1 2 3 4 5
0.0
0.1
0.2
0.3
0.4
Cum
ulati
ve h
azar
d ra
tes
(dis
conti
nuati
on fr
om tr
eatm
ent)
(%)

Telmisartan is the only ARB indicated in CV high-risk patients – representing the majority of the patients
typically seen in clinical practice
Product information provided by EMA (http://www.emea.europa.eu) and eMC (http://emc.medicines.org.uk)
Lo-sartan
Epro-sartan
Irbe-sartan
Olme-sartan
Val-sartan
Telmi-sartan
Hypertension Renal disease with hypertension and T2DM
Prevention of stroke in hypertensive patients with LVH
CV High-Risk Type 2 diabetes with target organ damage Coronary Heart Disease Peripheral Vascular Disease Stroke
Heart Failure (or LV dysfunction)
