cytomegalovirus infection after liver transplantation incidence, risks, and benefits of prophylaxis
TRANSCRIPT
CR
KP
Ctpainmstatrw
0d
2
ytomegalovirus Infection After Liver Transplantation Incidence,isks, and Benefits of Prophylaxis
. Weigand, P. Schnitzler, J. Schmidt, F. Chahoud, D. Gotthardt, P. Schemmer, W. Stremmel, and
. Sauer
ABSTRACT
Background. Cytomegalovirus (CMV) infection and related disease is a feared compli-cation after liver transplantation. Antiviral prophylaxis is recommended in clinical practiceguidelines depending on the CMV status of both donor and recipient as well as theindividual risk profile.Methods. We retrospectively analyzed 211 liver transplant recipients with respect to theincidence of CMV infection after transplantation, the influence of donor and recipientCMV status, and the effect of antiviral prophylaxis. In addition, the underlying liver diseaseand immunosuppressive regimen were compared with the incidence of CMV infection.Patients were divided into 4 groups according to CMV donor/recipient (D/R) profile:group A (D�/R�) 28 patients (13.3%), group B (D�/R�) 64 patients (30.3%), group C(D�/R�) 79 patients (37.4%), and group D (D�/R�) 40 patients (19.0%).Results. CMV infection was observed in 17.9%, 29.7%, 24.1%, and 22.5% of thepatients, respectively, with no significant difference in infection rates between the groups.CMV infection occurred in 5 patients (17.9%) in the presumed low-risk profile (group A),despite an antiviral prophylaxis in 4 out of these 5 patients. In contrast, CMV infectionoccurred in only 9/40 patients (22.5%) in the presumed high-risk profile (group D). Themost frequent infection rates were found in groups B and C (R� groups). After successfultreatment of CMV infection, no recurrence was detected. Underlying liver disease orimmunosuppressive protocol had no influence on CMV infection.Conclusion. Approximately one fourth of patients will acquire CMV infection after livertransplantation independent of donor/recipient status. Surprisingly, antiviral prophylaxisdoes not seem to be sufficient to reduce this proportion of patients, either in presumed
high-risk or in presumed low-risk situations.lltms
((U
mH
YTOMEGALOVIRUS (CMV) infection is among themost common complications after liver transplanta-
ion.1,2 It is a cause of great concern because it canotentially lead to cytopenia, fever, hepatitis, malaise,rthralgias, and tissue-invasive disease.3 In such tissue-nvasive disease, mucosal lesions, colitis, hepatitis, pneumo-itis, and meningoencephalitis can also occur.1,4,5 Further-ore, CMV infection bears the risk of bacterial or fungal
uperinfection. It has also been reported that CMV infec-ion is associated with higher rejection rates.6,7 Withoutntiviral prophylaxis, the overall incidence of CMV infec-ion independent of donor/recipient (D/R) profile has beeneported to reach 50%–60%.2,8 At present, it is unclear
hich patients are likely to suffer from CMV infection after m041-1345/10/$–see front matteroi:10.1016/j.transproceed.2010.04.025
634
iver transplantation. Some risk profiles are recognized, butong-term data are missing. There is also a lack of informa-ion as to whether the occurrence of CMV infection,easured by anti-CMV immunoglobulin (Ig)M or pp65 (a
pecific CMV regulation protein for viral replication), is
From the Department of Gastroenterology and HepatologyK.W., F.C., D.G., W.S., P.Sau.) the Department of VirologyP.Schn.) and the Department of General Surgery (J.S., P.Sche.),niversity Hospital Heidelberg, Heidelberg, Germany.Address reprint requests to Dr. med. Kilian Weigand, Depart-ent of Gastroenterology and Hepatology, University Hospitaleidelberg, Im Neuenheimer Feld 410, 69120 Heidelberg, Ger-
any. E-mail: [email protected]© 2010 by Elsevier Inc. All rights reserved.360 Park Avenue South, New York, NY 10010-1710
Transplantation Proceedings, 42, 2634–2641 (2010)

citrsCrwcOtfriThoAustgmubertmwlicvtofOdbraaf
PS
A2rapat2s2
dtmic
C
Tdtrcuph1
D
A(rcm
iaGoPatTCrmmBt(2TomGCpaaaav
ataafbp
POST LIVER TRANSPLANT CMV INFECTION 2635
aused by a new infection or the reactivation of a latentnfection. Although the transmission of infection via bloodransfusion during or after transplantation is possible,9,10
eactivation is considered more relevant.4,5 The CMV D/Rtatus at transplantation is a known risk predictor.11–13 TheMV mismatch with a positive donor and a negative
ecipient (D�/R�) is considered a high-risk constellationhile D�/R� is considered low risk.6,14,15 The 2 remainingonstellations are often regarded as intermediate risk.ther factors influencing a CMV infection after liver
ransplantation are reported to be low creatinine clearance,emale gender, and allograft rejection.16,17 It also has beeneported that there may be an association between themmunosuppressive regimen used and CMV infection.herapy with mycophenolate mofetil (MMF), for example,as been associated in some studies with an increased ratef CMV infections in kidney transplant recipients.18,19
ntiviral prophylaxis with ganciclovir or valganciclovir,sed depending on clinical practice and/or CMV D/Rtatus, has been shown to reduce the risk of CMV infectiono 20%–30% overall.13,20 Valganciclovir and oral or IVanciclovir are similarly effective as prophylaxes and treat-ent according to published data.13,21 At the moment, it is
nclear whether a preemptive or prophylactic approach isetter.8 A current study found both therapeutic regimensqually effective in renal transplantation.22 However, aecent survey showed that most liver transplant centers inhe United States and Canada prefer the prophylaxis regi-en.23 This most likely reflects the situation in Europe asell. It remains to be discussed whether antiviral prophy-
axis really reduces CMV infection rates or if it just turns itnto a so-called delayed-onset CMV infection with oc-urrence after antiviral prophylaxis is ended.13,24–26 Anti-iral prophylaxis itself is associated with several complica-ions.5,21 It may induce leukopenia and low platelet countsr renal dysfunction, to mention a couple of its mostrequent side effects. In addition, it is very cost intensive.verall, many questions remain unresolved and additional
ata are necessary to figure out if (and if so, which) patientsenefit from antiviral prophylaxis and to determine furtherisk factors. In the present long-term retrospective analysisfter liver transplantation, we evaluated the impact ofntiviral prophylaxis and the influence of assumed riskactors.
ATIENTS AND METHODStudy Population
ll patients who underwent liver transplantation from January 1,004, to December 31, 2006, were screened for inclusion in thisetrospective analysis. All patients who died within the first 4 weeksfter liver transplantation were excluded from the study. Foratients who experienced acute graft failure after transplantationnd were retransplanted within 2 weeks, only their second liverransplantation periods were included in the analysis. We screened53 patients for inclusion; 211 remained after applying the exclu-ion criteria. From these selected patients, 3 received a split liver,
underwent living-donor liver transplantation, and 1 patient was a womino liver recipient. The remaining patients received liverransplants from deceased donors. For the additional review ofortality and CMV infection, all 253 patients were analyzed. All
ncluded patients, parents, or legal guardians provided writtenonsent for the review of the liver recipients’ medical records.
linical Follow-Up
he medical records of the included patients were reviewed foremographic data, underlying disease that led to liver transplanta-ion, immunosuppressive regimen, and possible changes in theegimen, CMV infection, antiviral prophylaxis, and treatment,ause of infection, outcome, and death. All patients were followedntil death or December 31, 2007. With the exception of thoseatients who died or moved, a follow-up time of �12 months waseld. The median follow-up time of the whole cohort was 24.5 �3.5 months (range, 2–47).
efinition and Detection of Acute CMV Infection
cute CMV infection was defined as the detection of pp65phosphoprotein 65 kDa, specific CMV regulation protein for viraleplication) or anti-CMV IgM (see below).5 There were only 2ases in which IgM was detected but where the more sensitivearker of pp65 was not observed.DNA Extraction and Polymerase Chain Reaction Amplificat-
on. CMV DNA was extracted from 200 �L EDTA blood samplesnd purified using the QIAamp blood kit (QIAGEN, Hilden,ermany). A nested polymerase chain reaction (PCR) consisting
f 2 successive sets of 35 cycles each was performed in a Gene AmpCR System 2400 thermocycler (Perkin Elmer, Norwalk, Conn) tomplify the CMV IE-1 gene DNA. After an initial step of dena-uration for 5 minutes at 94 °C, the outer primers CMV-1 5= ACACT TTC TCG GGG TTC TCG TTG C 3= and CMV-2 5= GTCTC TGC CAA GAG AAA GAT GGA C 3= were used for the first
ound of amplification (1 min at 94 °C, 2 minutes at 65 °C, and 1inute at 72 °C with an additional time extension delay of 10inutes at 72 °C). Specific CMV primers were synthesized on aeckman Oligo 1000 mol/L oligonucleotide synthesizer. The reac-
ion mix consisted of 10 �L extracted DNA and 90 �L master mix10 mmol/L Tris-HCl [pH 8.3], 50 mmol/L KCl, 1.5 mmol/L MgCl2,00 �mol/L of each dNTP, 0.2 �mol/L of each primer and 2.5 Uaq DNA polymerase (Perkin Elmer). A nested PCR was carriedut with a 2-�L aliquot of the first PCR reaction, the PCR masterix, and the inner primers CMV-3 5= TTG AGG GAT TCT TCGCC AAC TCT G 3= and CMV-4 5= TCT CCT GTA TGT GACCA TGT GCT T 3= for further amplification to yield a PCRroduct of 170 bp.27 Reaction conditions and thermal cycling weres above. All DNA extraction and amplification reactions carriedppropriate parallel negative controls to detect contamination atny stage in the procedure. PCR products were electrophoresed in2% agarose gel containing 0.5 �g/mL ethidium bromide and
isualized under ultraviolet illumination.CMV pp65 Antigen Detection. For the quantitative CMV pp65
ntigenemia assay, about 8 mL of EDTA blood samples were usedo isolate leukocytes and 500,000 leukocytes were spun carefully onslide using a cytospin centrifuge. Cells were fixed and stained withn anti-CMV pp65 mouse monoclonal antibody, washed andurther incubated with an anti-mouse IgG FITC-labeled anti-ody.28 Slides were analyzed with ultraviolet microscopy and CMVp65 antigen positive cells were counted.Detection of CMV-Specific Antibodies. CMV-specific antibodies
ere determined in serum samples using the Enzygnost Anti-CMV

Iawfiwtgmiiaim
A
AwaaadaDdrbc
dmtJsa
I
Tn2gt2s1tcm
S
Dartc.
R
Dw
TpviDi
psptld(pCoR(iw
T
A
G
I
C
I
n
b
2636 WEIGAND, SCHNITZLER, SCHMIDT ET AL
gG and Enzygnost Anti-CMV IgM enzyme linked immunosorbentssays (Dade Behring, Marburg, Germany). Microtitration platesere coated with inactivated CMV antigen from CMV-infectedbroblasts. CMV-specific IgG or IgM antibodies in serum samples,hich bind to these CMV-derived antigens, could be detected after
he addition of peroxidase-conjugated rabbit anti-human IgG oroat anti-human IgM, whereby the peroxidase reacts with a chro-ogen solution. To avoid false-positive results owing to rheumatic
nterference, pretreatment with rheumatic factor absorbent wasmplemented. The amount of bound CMV-specific IgG or IgMntibodies was analyzed photometrically at 450 nm. Enzyme-linkedmmunosorbent assays (ELISA) were performed according to the
anufacturer’s instructions.
nti-CMV Prophylaxis and Treatment
ntiviral prophylaxis, when applied, was performed in accordanceith the current guidelines by ganciclovir regarding body weightnd renal adapted concentration. Valganciclovir was also used asntiviral prophylaxis regimen after July 2004 when it becamevailable as an oral medication. Valganciclovir became the stan-ard medication in January 2005.13,29,30 Antiviral prophylaxis wasdministered in consideration of the following criteria: high-risk/R status, retransplantation, or clinical decision. The standard
ose was 900 mg/d, but it was adapted to renal function whenequired. The duration of antiviral prophylaxis was three monthsut this was expanded to 6 months in some cases owing to clinicalonsiderations or CMV infection during prophylaxis.
Antiviral therapy was introduced when a CMV infection wasiagnosed. In the beginning of the study, IV ganciclovir was theedication of choice, whereas valganciclovir became the first-line
herapy after January 2005. However, IV. ganciclovir was used afteranuary 2005 in several cases owing to clinical decision or nonre-ponse. In these cases, it was used for 2 weeks, followed by andditional valganciclovir prophylaxis for 1–6 months.
mmunosuppressive Regimen
he immunosuppressive regimen was always based on methylpred-isolon. This was given in a high dose during surgery and the firstdays postsurgery. Then it was reduced as recommended in the
uidelines of the transplant center to 40 mg/d with further reduc-ion every second week. Methylprednisolon was tapered down to.5 mg or none after 6–12 months. Maintenance immunosuppres-ion consisted of cyclosporine or tacrolimus. Of the study cohort,41 patients were started on cyclosporine and 70 patients onacrolimus. At the beginning azathioprine was often combined withyclosporine for 6 months. Later, MMF became a frequently usededication in addition to cyclosporine or tacrolimus.
tatistical Analysis
escriptive statistics were used to characterize demographic datand clinical variables. The chi-square test was used to assess theelationships between the underlying liver disease and CMV infec-ion, the immunosuppressive regimen and CMV infection, or ahange of immunosuppressive regimen and CMV infection. P �05 was considered significant.
ESULTS
uring the 3-year study period, 253 liver transplantations
ere performed; 211 patients were included in the study.cr
he mean age of the patients was 47.5 � 14.5 years; 138atients (65.4%) were male. Demographic data and clinicalariables are shown in Table 1. The CMV serostatus of thencluded patients was CMV D�/R� in 28 cases (13.3%),�/R� in 64 (30.3%), D�/R� in 79 (37.4%), and D�/R�
n 40 (19.0%; Fig 1).CMV infections were observed in 24.6% of the study
atients. No significant differences between the 4 D/Rubgroups were detected. In the D�/R� subgroup, with aresumed low-risk profile, we found 17.9% of CMV infec-ions after liver transplantation. Although this rate wasower compared with the other subgroups, the differenceid not reach significance. The rate of CMV infectionsCMV�) in the 4 subgroups in total numbers and inercentage is shown in Figure 1. The subgroup with theMV D/R high-risk status had the second lowest incidencef CMV infection (22.5%), whereas the 2 subgroups with a� situation suffered more often from CMV infection
24.1% and 29.7%; Fig 1). Antiviral prophylaxis was admin-stered to 51.7% of patients in this study. Of the patientsho acquired a CMV infection, 67.3% had no prophylaxis.
Table 1. Demographic and Clinical Characteristics of 211 Liverransplant Recipients From January 2004 to December 2006 at
the University Hospital of Heidelberg
Variable Value (N � 211)
ge (y)Mean (SD) 47.5 (14.5)Median 51Range 1–66enderMale 138 (65.4%)Female 73 (34.6%)
ndications for transplantation*Hepatitis C 34 (16.1%)Hepatitis B 19 (9.0%)Alcoholic liver disease 62 (29.4%)Wilson’s disease 3 (1.4%)Autoimmune hepatitis 10 (4.7%)Hemochromatosis 4 (1.9%)Others 46 (21.8%)Hepatocellular carcinoma 63 (29.9%)MV status (D/R)D�/R� 28 (13.3%)D�/R� 64 (30.3%)D�/R� 79 (37.4%)D�/R� 40 (19.0%)
mmunosuppressive regimen#
Cyclosporine 21Cyclosporine and Azathioprine 85Tacrolimus 50Cyclosporine and MMF 35Tacrolimus and MMF 20
Abbreviations: CMV, cytomegalovirus; D/R, donor/recipient; MMF, Mycophe-olate mofetil.*Cumulative incidences. If �2 underlying diseases were found in 1 patient,
oth diseases are represented in the statistic above.#Immunosuppressive regimen started with the liver transplantation; for
hanges in the follow-up time due to various reasons, see main text. Everyegimen included additional methylprednisolon in decreasing dosage over time.

BpKlCplAca1pwi
RtPilmdpwtw
(ltswiwi(
tibnipswddRt(i2
Fstw ). He
POST LIVER TRANSPLANT CMV INFECTION 2637
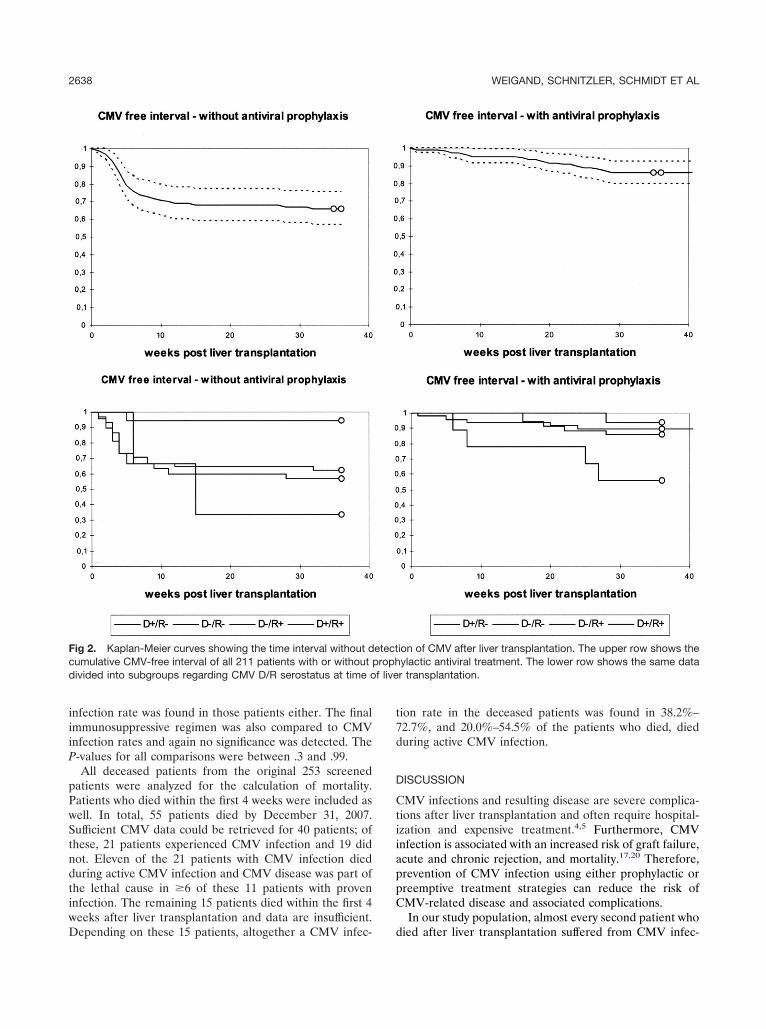
y contrast, a CMV infection was detected in 32.7% ofatients with antiviral prophylaxis. Figure 2 shows theaplan-Meier curves of patients with and without prophy-
axis. It demonstrates the time interval without detection ofMV after liver transplantation. With the exception ofatients with a D�/R� situation, CMV infections after
iver transplantation were reduced by antiviral prophylaxis.ltogether, 17 patients in our study population who re-
eived antiviral prophylaxis experienced a CMV infection; 7cquired the infection during the prophylactic course and0 after the prophylaxis was stopped. In 8 of these 10ostprophylaxis cases, CMV infection occurred within 8eeks after the end of antiviral prophylaxis. In the remain-
ng 2 patients, pp65 was found positive at a later time point.Of the 5 patients in the presumed low-risk group (D�/�) who acquired a CMV infection after liver transplan-
ation, 4 patients (80%) received antiviral prophylaxis.rophylaxis was administered because of retransplantation
n 3 cases. Two of the 4 patients who had antiviral prophy-axis developed CMV infections during prophylactic treat-
ent. One died during the infection. The remaining 2eveloped CMV infections 2 and 4 months after antiviralrophylaxis was ended. With the exception of the patientho died, all others recovered from the CMV infection. In
he presumed high-risk group (D�/R�), 66.7% of patients
ig 1. Distribution of screened and enrolled patients. The thirderostatus. Shown are absolute numbers and percentage (in bracransplantation related to the serostatus. Again, absolute numberith antiviral prophylaxis (P�) or without antiviral prophylaxis (P�
ho acquired a CMV infection had an antiviral prophylaxis b
6/9). The subgroups with the highest infection rates afteriver transplantation were the R� groups (Fig 1). However,he overall rate of prophylactic therapy in these groups wasomewhat lower than in the D�/R� group. In accordanceith earlier published data, women suffered from CMV
nfection more often than men. Twenty out of the 73omen in our study population (37.7%) acquired a CMV
nfection, whereas 32 out of 138 male patients (30.2%) didP � .7).
Comparing the underlying liver diseases that led to liverransplantation with the number of patients acquiring CMVnfection, we found no significant differences (P-valuesetween .22 and .99). It has been reported that immu-osuppressive therapy using mycophenolate mofetil may
ncrease the risk of CMV infection after solid organ trans-lantation. In our population, we compared the immuno-uppressive regimen after liver transplantation (Table 1)ith the risk of acquiring a CMV infection and found noifferences. The immunosuppressive regimen was changeduring the follow-up time in 44 out of the 211 patients.easons for changing the immunosuppressants were cen-
ral or peripheral neurologic symptoms (n � 18), rejectionn � 10), addition of azathioprine or MMF (n � 10),nadequate response to primary immunosuppressant (n �), and renal failure (n � 1). In 3 cases, the reason could not
hows the distribution of the donors’ (D) and recipients’ (R) CMV). The fourth row shows the incidence of CMV infection post liver
relative percentages are shown. The last row identifies patientsre also, absolute numbers and relative percentages are shown.
row sketss and
e determined; however, no significant increase in the
iiiP
pPwStndtiwD
t7d
D
CtiiappC
Fcd f live
2638 WEIGAND, SCHNITZLER, SCHMIDT ET AL
nfection rate was found in those patients either. The finalmmunosuppressive regimen was also compared to CMVnfection rates and again no significance was detected. The-values for all comparisons were between .3 and .99.All deceased patients from the original 253 screened
atients were analyzed for the calculation of mortality.atients who died within the first 4 weeks were included asell. In total, 55 patients died by December 31, 2007.ufficient CMV data could be retrieved for 40 patients; ofhese, 21 patients experienced CMV infection and 19 didot. Eleven of the 21 patients with CMV infection dieduring active CMV infection and CMV disease was part ofhe lethal cause in �6 of these 11 patients with provennfection. The remaining 15 patients died within the first 4eeks after liver transplantation and data are insufficient.
ig 2. Kaplan-Meier curves showing the time interval without dumulative CMV-free interval of all 211 patients with or without pivided into subgroups regarding CMV D/R serostatus at time o
epending on these 15 patients, altogether a CMV infec- d
ion rate in the deceased patients was found in 38.2%–2.7%, and 20.0%–54.5% of the patients who died, dieduring active CMV infection.
ISCUSSION
MV infections and resulting disease are severe complica-ions after liver transplantation and often require hospital-zation and expensive treatment.4,5 Furthermore, CMVnfection is associated with an increased risk of graft failure,cute and chronic rejection, and mortality.17,20 Therefore,revention of CMV infection using either prophylactic orreemptive treatment strategies can reduce the risk ofMV-related disease and associated complications.In our study population, almost every second patient who
ion of CMV after liver transplantation. The upper row shows theylactic antiviral treatment. The lower row shows the same datar transplantation.
etectroph
ied after liver transplantation suffered from CMV infec-

tsdi
p(rtmitcbtCaItftree
costsadpbitspmwprapndmm
codaadop
gt
imHhssgtp
whcbgtiliiTaeoaNfnHimhclph
iprbp(psslbrrrea
POST LIVER TRANSPLANT CMV INFECTION 2639
ion. CMV disease was identified as the cause of death inome cases (�10%), which lends support to the concept ofiligent prevention of CMV infection. The obvious problem
s identifying those patients at risk for infection.Practices regarding CMV prophylaxis vary among trans-
lant centers and generally accepted recommendationse.g., whether all liver recipient or only those with increasedisk should be treated, the optimal duration of prophylacticreatment) are not well-established. Prophylactic treatmentay be associated with adverse events. Antiviral medication
tself may cause problems such as cytopenia and renaloxicity5,19 and, in addition, is cost intensive. In mostenters, the decision to provide prophylactic treatment isased on the recipient and donor risk profiles. Liverransplant recipients who were initially seronegative forMV but who received a graft from a CMV-positive donorre presumed to be at the greatest risk for CMV infection.12
n addition, the use of antithymocyte globulin, retransplan-ation, and gender are thought to be additional risk factorsor CMV infection in posttransplant patients.16 However,he indication for prophylactic treatment in the individualecipient in relation to risk profile has not been wellvaluated. In our population, for example, females did notxperience CMV infection more often.
An association between immunosuppressive regimen (in-luding MMF) and higher CMV infection rates has beenbserved in renal transplant recipients.18 In contrast, othertudies have demonstrated MMF to be protective againsthe long-term consequences of CMV disease on grafturvival and to have synergistic antiviral effects for patientsfter kidney transplantation.31,32 There is a lack of suchata for liver transplant recipients, however. In our studyopulation of 211 patients, we observed no correlationetween immunosuppressive regimen or the necessity of an
mmunosuppressant change and CMV infection after liverransplantation. Cumulative methylprednisolon dose is con-idered a possible risk factor for CMV infection.33,34 Allatients in our study cohort were injected with high-doseethylprednisolone during transplantation in accordanceith our institutional guidelines. These guidelines are com-arable to most transplant centers worldwide. They eacheceived 80 mg methylprednisolone IV for the first 2 daysfter surgery. Then they were set on weight-based methyl-rednisolone. Methylprednisolone was tapered over for theext 6–9 months. All patients in our cohort had a maximumosage of 2.5 mg methylprednisolone after 9 months. Theajority of our patients (�90%) were steroid free after 12onths.Although there might be a slight uncertainty in the
alculation of exact cumulative methylprednisolone dosagewing to the retrospective character of our study, noifference was observed in the comparison of patients withnd without CMV infection after liver transplantation. Inddition to the mentioned risk factors, underlying liverisease has been thought to correlate with an increased riskf CMV infection after transplantation.35 In our study
opulation, however, we found no difference between the aroups regarding underlying liver disease and CMV infec-ion after liver transplantation.
Antiviral prophylaxis seems to be effective. The risk ofnfection can be reduced from 50%–60%2,8 to approxi-
ately 25%, as seen in our study population (Figs 1 and 2).owever, this treatment exposes patients, many of whom
ave no need of antiviral prophylaxis, to potentially seriouside effects. New interesting approaches including the mea-urement of immunologic parameters, such as the pro-rammed death 1 receptor, may be of predictive value inhe future, but at present they remain experimental ap-roaches.36
The decision to apply antiviral prophylaxis in our studyas based on the following criteria: patients with D/Righ-risk status, patients undergoing retransplantation, andlinical decisions. Clinical decisions included severe comor-idity with assumed high-risk profile, impaired or reducedraft function due to other causes, and biliary complica-ions. Although prophylactic therapy was diligently admin-stered in these patients, CMV infection occurred nonethe-ess in a substantial number. This was observed particularlyn the D/R low-risk subgroup, of whom 80% of patients withnfection had received prophylaxis (4 out of 5 patients).hus, patients with D�/R� status seem not to profit fromntiviral prophylaxis. This conclusion may be limited, how-ver, owing to the low number of patients. With exceptionf the patients with a presumed low-risk profile (D�/R�),ntiviral prophylaxis was efficient in all subgroups (Fig 2).evertheless, an average 1 out of 4 patients still suffered
rom CMV infection in these subgroups. Any problems withonadherence to the medication can only be speculated on.owever, it seems that some patients experience CMV
nfection independent of antiviral prophylaxis. Further-ore, it has been shown recently that, at least for the
igh-risk D/R population, lengthening the prophylacticourse merely delays the onset of CMV infection .25,37 Aonger course, however, may be useful in improving theatient’s overall immunogenic state and better preparingim to deal with the infection.In contrast with the risk profiles, the highest rate of CMV
nfection was observed in the R� groups and not in theresumed high-risk subgroup D�/R�. The high infectionate in patients with the D�/R� situation may be explainedy the antiviral prophylaxis rate of only 25% in theseatients. In comparison, 90% of the high-risk patientsD�/R�) received prophylactic treatment. However, pro-hylaxis was also applied to 62% of the patients in theecond R� subgroup (D�/R�) and they suffered theecond most frequently from CMV infections. Neverthe-ess, the high rate of prophylaxis in the high-risk group muste taken into account, because it may relativize theseesults. Even so, Hughes et al38 recently published similaresults in kidney recipients. In their cohort, a seropositiveecipient status also had a high impact on CMV antigen-mia after renal transplantation.38 These data led to thessumption that patients in R� situation should be set on
ntiviral prophylaxis more frequently. However, around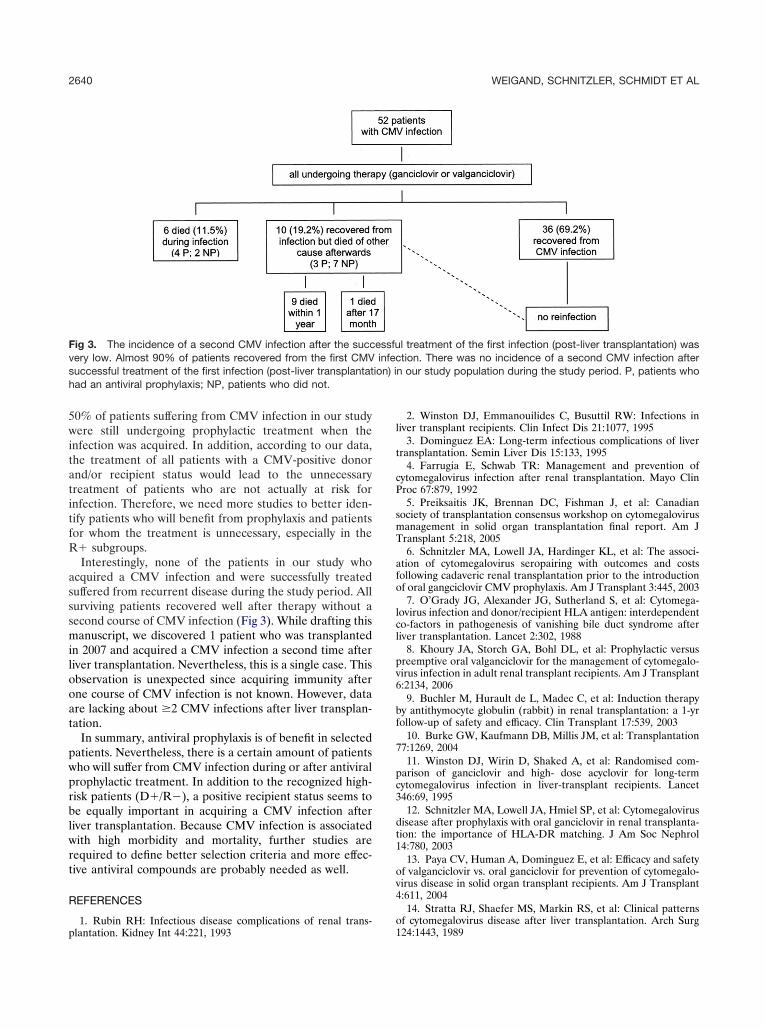
5witatitfR
asssmilooat
pwprblwrt
R
p
l
t
cP
smT
afo
lcl
pv6
bf
7
pc3
dt1
ov4
Fvsh
2640 WEIGAND, SCHNITZLER, SCHMIDT ET AL
0% of patients suffering from CMV infection in our studyere still undergoing prophylactic treatment when the
nfection was acquired. In addition, according to our data,he treatment of all patients with a CMV-positive donornd/or recipient status would lead to the unnecessaryreatment of patients who are not actually at risk fornfection. Therefore, we need more studies to better iden-ify patients who will benefit from prophylaxis and patientsor whom the treatment is unnecessary, especially in the� subgroups.Interestingly, none of the patients in our study who
cquired a CMV infection and were successfully treateduffered from recurrent disease during the study period. Allurviving patients recovered well after therapy without aecond course of CMV infection (Fig 3). While drafting thisanuscript, we discovered 1 patient who was transplanted
n 2007 and acquired a CMV infection a second time afteriver transplantation. Nevertheless, this is a single case. Thisbservation is unexpected since acquiring immunity afterne course of CMV infection is not known. However, datare lacking about �2 CMV infections after liver transplan-ation.
In summary, antiviral prophylaxis is of benefit in selectedatients. Nevertheless, there is a certain amount of patientsho will suffer from CMV infection during or after antiviralrophylactic treatment. In addition to the recognized high-isk patients (D�/R�), a positive recipient status seems toe equally important in acquiring a CMV infection after
iver transplantation. Because CMV infection is associatedith high morbidity and mortality, further studies are
equired to define better selection criteria and more effec-ive antiviral compounds are probably needed as well.
EFERENCES
ig 3. The incidence of a second CMV infection after the succery low. Almost 90% of patients recovered from the first CMVuccessful treatment of the first infection (post-liver transplantatad an antiviral prophylaxis; NP, patients who did not.
1. Rubin RH: Infectious disease complications of renal trans-lantation. Kidney Int 44:221, 1993
o1
2. Winston DJ, Emmanouilides C, Busuttil RW: Infections iniver transplant recipients. Clin Infect Dis 21:1077, 1995
3. Dominguez EA: Long-term infectious complications of liverransplantation. Semin Liver Dis 15:133, 1995
4. Farrugia E, Schwab TR: Management and prevention ofytomegalovirus infection after renal transplantation. Mayo Clinroc 67:879, 19925. Preiksaitis JK, Brennan DC, Fishman J, et al: Canadian
ociety of transplantation consensus workshop on cytomegalovirusanagement in solid organ transplantation final report. Am Jransplant 5:218, 20056. Schnitzler MA, Lowell JA, Hardinger KL, et al: The associ-
tion of cytomegalovirus seropairing with outcomes and costsollowing cadaveric renal transplantation prior to the introductionf oral gangciclovir CMV prophylaxis. Am J Transplant 3:445, 20037. O’Grady JG, Alexander JG, Sutherland S, et al: Cytomega-
ovirus infection and donor/recipient HLA antigen: interdependento-factors in pathogenesis of vanishing bile duct syndrome afteriver transplantation. Lancet 2:302, 1988
8. Khoury JA, Storch GA, Bohl DL, et al: Prophylactic versusreemptive oral valganciclovir for the management of cytomegalo-irus infection in adult renal transplant recipients. Am J Transplant:2134, 20069. Buchler M, Hurault de L, Madec C, et al: Induction therapy
y antithymocyte globulin (rabbit) in renal transplantation: a 1-yrollow-up of safety and efficacy. Clin Transplant 17:539, 2003
10. Burke GW, Kaufmann DB, Millis JM, et al: Transplantation7:1269, 200411. Winston DJ, Wirin D, Shaked A, et al: Randomised com-
arison of ganciclovir and high- dose acyclovir for long-termytomegalovirus infection in liver-transplant recipients. Lancet46:69, 199512. Schnitzler MA, Lowell JA, Hmiel SP, et al: Cytomegalovirus
isease after prophylaxis with oral ganciclovir in renal transplanta-ion: the importance of HLA-DR matching. J Am Soc Nephrol4:780, 200313. Paya CV, Human A, Dominguez E, et al: Efficacy and safety
f valganciclovir vs. oral ganciclovir for prevention of cytomegalo-irus disease in solid organ transplant recipients. Am J Transplant:611, 200414. Stratta RJ, Shaefer MS, Markin RS, et al: Clinical patterns
l treatment of the first infection (post-liver transplantation) wastion. There was no incidence of a second CMV infection after
n our study population during the study period. P, patients who
essfuinfec
ion) i
f cytomegalovirus disease after liver transplantation. Arch Surg24:1443, 1989

cra
ci1
r(p1
mt
pws
ird
nmT
vr
p8
oc6
pT
cr
hDr
mc
agtt
og
nT
mdc
msT
tr
mo8
di
cv
C
POST LIVER TRANSPLANT CMV INFECTION 2641
15. Singh N, Dummer JS, Kusne S, et al: Infections withytomegalovirus and other herpesviruses in 121 liver transplantecipients: transmission by donated organ and the effect of OKT3ntibodies. J Infect Dis 158:124, 1988
16. Freeman RB, Paya CV, Pescovitz MD, et al: Risk factors forytomegalovirus viremia and disease developing after prophylaxisn high-risk solid-organ transplant recipients. Transplantation 78:765, 200417. Razonable RR, Rivero A, Rodriguez A, et al: Allograft
ejection predicts the occurrence of late- onset cytomegalovirusCMV) disease among CMV-mismatched solid organ transplantatients receiving prophylaxis with oral ganciclovir. J Infect Dis84:1461, 200118. Song AT, Abdala E, Bonazzi PR, et al: Does mycophenolateofetil increase the risk of cytomegalovirus infection in solid organ
ransplant recipients? A mini-review. Braz J Infect Dis 10:132, 200619. Moreso F, Seron D, Morales JM, et al: Incidence of leuko-
enia and cytomegalovirus disease in kidney transplants treatedith mycophenolate mofetil combined with low cyclosporine and
teroid doses. Clin Transplant 12:198, 199820. Hodson EM, Jones CA, Webster AV, et al: Antiviral med-
cations to prevent cytomegalovirus disease and early death inecipients of solid-organ transplants: a systematic review of ran-omised controlled trials. Lancet 365:2105, 200521. Asberg A, Humar A, Rollag H, et al: Oral valganciclovir is
oninferior to intravenous ganciclovir for the treatment of cyto-egalovirus disaese in solid organ transplant recipients. Am Jransplant 7:2106, 200722. Reischig T, Jindra P, Hes O, et al: Valacyclovir prophylaxis
ersus preemptive valganciclovir therapy to prevent cytomegalovi-us disease after renal transplantation. Am J Transplant 8:69, 2008
23. Levitsky J, Singh N, Wagener MM, et al: A survey of CMVrevention strategies after liver transplantation. Am J Transplant:158, 200824. Brennan DC, Garlock KA, Singer GG, et al: Prophylactic
ral ganciclovir compared with deferred therapy for control ofytomegalovirus in renal transplant recipients. Transplantation4:1843, 199725. Arthurs SK, Eid AJ, Pedersen RA, et al: Delayed-onset
rimary cytomegalovirus disease after liver transplantation. Liverranspl 13:1703, 200726. Limaye AP, Bakthavatsalam R, Kim HW, et al: Impact of
ytomegalovirus in organ transplant recipients in the era of antivi-
al prophylaxis. Transplantation 81:1645, 2006 a27. Mangano MF, Hodinka RL, Spivack JG: Detection ofuman cytomegalovirus by polymerase chain reaction. In Becker Y,arai G, eds: Diagnosis of human viruses by polymerase chain
eaction technology. New York: Springer; 199228. Landry ML, Ferguson D: Comparison of quantitative cyto-egalovirus antigenemia assay with culture and correlation with
linical disease. J Clin Microbiol 31:2851, 199329. Singh N, Paterson DL, Gayowski T, et al: Cytomegalovirus
ntigenemia directed preemptive prophylaxis with oral versus i.v.anciclovir for the prevention of cytomegalovirus disease in liverransplant recipients: a randomized, controlled trial. Transplanta-ion 70:717, 2000
30. Razonable RR, Cruijsen HvH, Brown RA, et al: Dynamicsf cytomegalovirus replication during preemptive therapywith oralanciclovir. J Infect Dis 187:1801, 2003
31. Allison AC, Eugui EM: Mechanisms of action of mycophe-olate mofetil in preventing acute and chronic allograft rejection.ransplantation 15:S181, 200532. Giral M, Nguyen JM, Daguin P, et al: Mycophenolateofetil does not modify the incidence of cytomegalovirus (CMV)
isease after kidney transplantation but prevents CMV-inducedhronic graft dysfunction. J Am Soc Nephrol 12:1758, 2001
33. Moench C, Barreiros AP, Schuchmann M, et al: Tacrolimusonotherapy without steroids after liver transplantation: a pro-
pective randomized double-blinded placebo-controlled trial. Am Jransplant 7:1616, 200734. Eason JD, Loss GE, Blazek J, et al: Steroid-free liver
ransplantation using rabbit antithymocyte globuline induction:esults of a prospective randomized trial. Liver Transpl 7:693, 2001
35. Burak KW, Kremers WK, Batts KP, et al: Impact of cyto-egalovirus infection, year of transplantation, and donor age on
utcomes after liver transplantation for hepatitis C. Liver Transpl:362, 200236. La Rosa C, Krishnan A, Longmate J, et al: Programmed
eath-1 expression in liver transplant recipients as a prognosticndicator of cytomegalovirus disease. J Infect Dis 197:25, 2008
37. Limaye AP, Bakthavatsalam R, Kim HW, et al: Late-onsetytomegalovirus disease in liver transplant recipients despite anti-iral prophylaxis. Transplantation 78:1390, 2004
38. Hughes D, Hafferty J, Fulton L, et al: Donor and recipientMV serostatus and antigenemia after renal transplantation: an
nalysis of 486 patients. J Clin Virol 41:92, 2008