cutting edge topics in ibd surgery - static.livemedia.gr · st mark's hospital and academic...
TRANSCRIPT

St Mark's Hospital
and Academic Institute
Cutting edge topics in IBD surgery
Janindra Warusavitarne
Consultant Colorectal Surgeon and Lead IBD Surgeon,
St Mark’s Hospital, London, UK.
17th Panhellenic IBD Congress Thessaloniki May 2018
St Mark's Hospital
and Academic Institute
Perceptions of surgeons
• Cutting edge = Playing with toys

St Mark's Hospital
and Academic Institute
But is that all that’s new in IBD surgery?
The Thinking Surgeon

St Mark's Hospital
and Academic Institute
How is IBD surgery evolving
• The pastI think I have done
all I can now its your
turn to sort it out
boy!!

St Mark's Hospital
and Academic Institute
What is cutting edge now
• Joint clinics
• IBD MDT
• Patient in the centre of decision making

St Mark's Hospital
and Academic Institute
IBD Surgery
• IBD surgery is a sub speciality in its own right
• Requires an understanding of the disease process
• The aim is to restore quality of life
• An adjunct to optimise response to treatments
• Develop and maintain high quality standards in surgery

St Mark's Hospital
and Academic Institute
Why are standards important in IBD
Surgery

St Mark's Hospital
and Academic Institute
Why are IBD patients different
• Sepsis/abscess
• Albumin
• Medications
– Steroids anti TNF, vedolizumab,etc
• Fistula at the time of surgery
• Bowel anatomy
• Recurrent disease
• QUALITY OF LIFE !!!!!

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
Low Surgeon
Volume
• Associated with
high re-
hospitalisations
• Poor outcomes

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
Setting the standards can make a
difference
Involving patients can also make a
huge difference

St Mark's Hospital
and Academic Institute
Defining Key Performance Indicators for the surgical
management of Inflammatory Bowel Disease
Aims
To achieve an expert consensus on the development of
KPIs that will be used to measure quality of service
provision in IBD surgery

St Mark's Hospital
and Academic Institute
Outcome measure for Crohn’s
surgery

St Mark's Hospital
and Academic Institute
Outcome measures specific to case adjusted Crohn's small bowel or ileocolonic
surgery include:-
Likert ratings
(median; interquartile
range)
Round 1 Round 2
➢ the proportion of patients who require re-operations within 30 days secondary to
intra-abdominal septic complications.5; 0.5 5, 0
➢ the proportion of patients who develop enterocutaneous fistulae within 90 days. 4; 1 5, 1
➢ the proportion of cases performed laparoscopically without conversion to open. 3; 0 3, 0
➢ the proportion of patients who are stoma free after 12 months. 4; 1 4, 2
➢ the proportion of patients who develop clinical recurrence within 12 months. 4; 1 4,1
➢ the proportion of patients who develop surgical recurrence within 36 months. 3; 1 3, 1
➢ the proportion of patients who receive preoperative nutritional optimization where
indicated.4; 1 4, 1
➢ the proportion of patients who develop subsequent short bowel. 5; 1 5, 1
➢ the proportion of patients who are started on prophylactic immunomodulatory
therapy within 6 months after surgery.4; 1 4, 1
➢ quality of life measures at 6 month postoperatively using the Crohn's Life Impact
Questionnaire (CLIQ).4; 2 4, 1
St Mark's Hospital
and Academic Institute
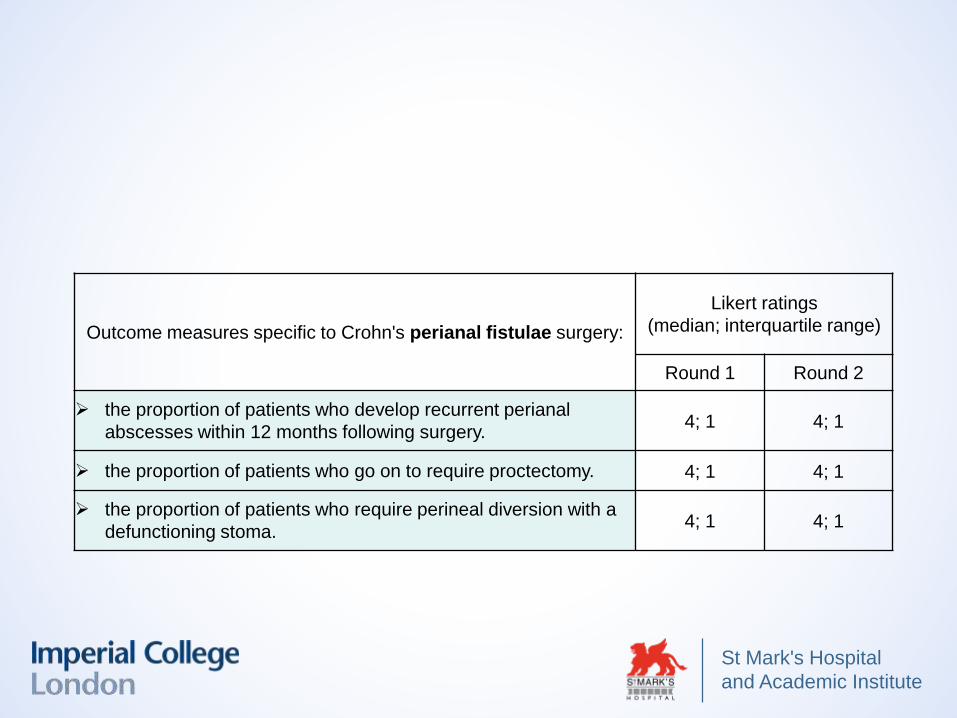
Outcome measures specific to Crohn's perianal fistulae surgery:
Likert ratings
(median; interquartile range)
Round 1 Round 2
➢ the proportion of patients who develop recurrent perianal
abscesses within 12 months following surgery.4; 1 4; 1
➢ the proportion of patients who go on to require proctectomy. 4; 1 4; 1
➢ the proportion of patients who require perineal diversion with a
defunctioning stoma.4; 1 4; 1
St Mark's Hospital
and Academic Institute
Outcome measure for UC
surgery

St Mark's Hospital
and Academic Institute
Outcome measures specific to subtotal colectomy with end ileostomy:-
Likert ratings
(median; interquartile range)
Round 1 Round 2
➢ 30 day mortality rates in patients aged over 70. 5; 1 5; 0
➢ 90 day mortality rates in patients aged over 70. 5; 1 5; 0
➢ the proportion of cases performed laparoscopically without conversion to
open.3; 1 3; 1
➢ the proportion of patients who develop rectal stump blowouts. 4.5; 2 4; 1
➢ the proportion of patients who undergo re-operation within 30 days after
surgery.5; 1

St Mark's Hospital
and Academic Institute
Outcome measures specific to proctocolectomy include:-
Likert ratings
(median; interquartile range)
Round 1 Round 2
➢ the proportion of cases that are performed laparoscopically
without conversion to open.3; 1 3; 1
➢ the proportion that develop perineal sinus formation. 4; 2 4; 0
➢ the proportion of patients who have concomitant ileoanal
pouch formation out of the total number of
proctocolectomies.
4; 2 4; 1
➢ the proportion of patients who develop sexual dysfunction. 5; 1 5; 1

St Mark's Hospital
and Academic Institute
Outcome measures specific to ileoanal pouch formation
include:-
Likert ratings
(median; interquartile
range)
Round 1 Round 2
➢ the proportion of patients who undergo re-operations within
30 days secondary to intra-abdominal septic complications.5; 1 5; 0
➢ the proportion of patients who develop pelvic septic
complications within 30 days following surgery.5; 1 5; 0
➢ the proportion of patients who require permanent faecal
diversion with an ileostomy for long term pouch-related
complications (including pouchitis, fistulae or pouch failure).
5; 1 5; 1
➢ the proportion of patients who require pouch salvage
surgery in the long term for pouch failure.4; 2 4; 1

St Mark's Hospital
and Academic Institute
Outcome measure for overall
quality

St Mark's Hospital
and Academic Institute
Outcome measures required in measuring the overall quality of an
IBD surgical service include:-
Likert ratings
(median; interquartile
range)
Round 1 Round 2
➢ the proportion of readmissions within the six month postoperative
period, relative to the length of initial postoperative inpatient stay.4; 1 4; 1
➢ the length of postoperative inpatient stay. 4; 2 4; 2
➢ the proportion of patients that return to work normal activities
within a six month postoperative period.4; 1 4; 1
➢ distribution of patient satisfaction surveys (through IBD specific
patient panels, departmental open days, or patient opinion
websites).
4; 2 4; 1
➢ overall case adjusted 30 day postoperative morbidity (as graded
by the Clavien-Dindo classification).4; 1 4; 1
➢ overall mortality rates within 90 days after surgery. 5; 1 5; 0
➢ quality of life measures 12 months postoperatively by use of the
Inflammatory Bowel Disease Questionnaire (IBDQ).4; 1 4; 1

St Mark's Hospital
and Academic Institute
Structural necessities for an
IBD surgical service provision

St Mark's Hospital
and Academic Institute
Quality assurance mechanisms for the delivery of a high quality IBD surgical
service should include:-
Likert ratings
(median; interquartile range)
Round 1 Round 2
➢ an IBD team meeting discussion for all IBD deaths within 12 months of surgery
with the outcome of the discussion recorded and submitted to national data
collection.
5;1 5; 0
➢ an IBD team meeting discussion in the event of significant postoperative
morbidity (Clavien-Dindo grade 3) and mortality with the outcome of the
discussion recorded and submitted to national data collection.
4; 1 5; 1
➢ an IBD team meeting discussion in the event of all IBD-related postoperative
readmissions.4; 2
4; 0➢ an IBD team meeting discussion considering the length of postoperative
inpatient stay is greater than 14 days. 4; 14; 1
➢ discussion in the surgical Morbidity & Mortality meeting in the event of surgical
deaths within 30 days of surgery.5; 0
5; 0➢ open publication or registry reporting for case adjusted morbidity and mortality. 4; 2 4; 0
➢ a process of credentialing from a national or international governing body for
the IBD unit to deliver surgical services. 4; 2 4; 1
➢ submission of surgical outcome data into national IBD audits or registries
(including the IBD audit, ileal pouch registry, IBD registry). 5; 1 5; 1
➢ a local registry of surgical IBD patients. 5; 1

St Mark's Hospital
and Academic Institute
An individual consultant colorectal surgeon should be performing the following number of IBD major
resections per year (including proctocolectomy, subtotal colectomy, ileoanal pouch formation &
ileocolonic/small bowel Crohn's surgery):
Round 1 Round 2
Consensus following round two: 85.7%
> 16

St Mark's Hospital
and Academic Institute
An institution delivering a high quality surgical service should be performing the following minimum
number of IBD major resections per year (including proctocolectomy, subtotal colectomy, ileoanal pouch
formation and ileocolonic/small bowel Crohn's surgery):
Round 1 Round 2

St Mark's Hospital
and Academic Institute
The IBD team members required to deliver a high quality IBD surgical service,
include:-
Likert ratings
(median; interquartile
range)
Round 1 Round 2
➢ a consultant colorectal surgeon trained and experienced in laparoscopic
surgery.
5; 1 5; 0
➢ a consultant colorectal surgeon who is a core member of the IBD
multidisciplinary team.
5; 0 5; 0
➢ a consultant colorectal surgeon who is on a dedicated IBD on-call rota
providing emergency IBD surgery when required.
4; 2 4; 2
➢ a consultant radiologist who is a core member of the IBD multidisciplinary
team.
5; 1 5; 1
➢ a consultant gastroenterologist who is a core member of the IBD
multidisciplinary team.
5; 0 5; 0
➢ a clinical nurse specialist with a special interest and competency in stoma
therapy and ileoanal pouch surgery.
5; 1 5; 1
➢ a consultant histopathologist who is a core member of the IBD multidisciplinary
team.
4; 1 4; 1
4; 2 4 ;1
St Mark's Hospital
and Academic Institute
Multidisciplinary team
• Essential to good working of a IBD
unit
• Joint clinics enhance the patient
experience and decision making
• For the surgeon – understanding the
medications and its impact pre and
post operatively
• For the gastroenterologist –
understanding the surgery and its
impact on patients

St Mark's Hospital
and Academic Institute
The road map:
Radiologist who understands
IBD
• CT enterography
• Barium Follow through
• MR enterography
stricture
abscess
fistula

St Mark's Hospital
and Academic Institute
Thinking outside the box

St Mark's Hospital
and Academic Institute
How do we decide on the surgical approach?

St Mark's Hospital
and Academic Institute
To Join or Not to Join
• Sepsis/abscess
• Albumin
• Medications
– Steroids ? Infliximab
• Fistula at the time of surgery
• Risk of anastomotic leak
– 50% with all 4 risk factors, 29% with 3 14% -16% with 2 or 1 risk
factor and 5% with none

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
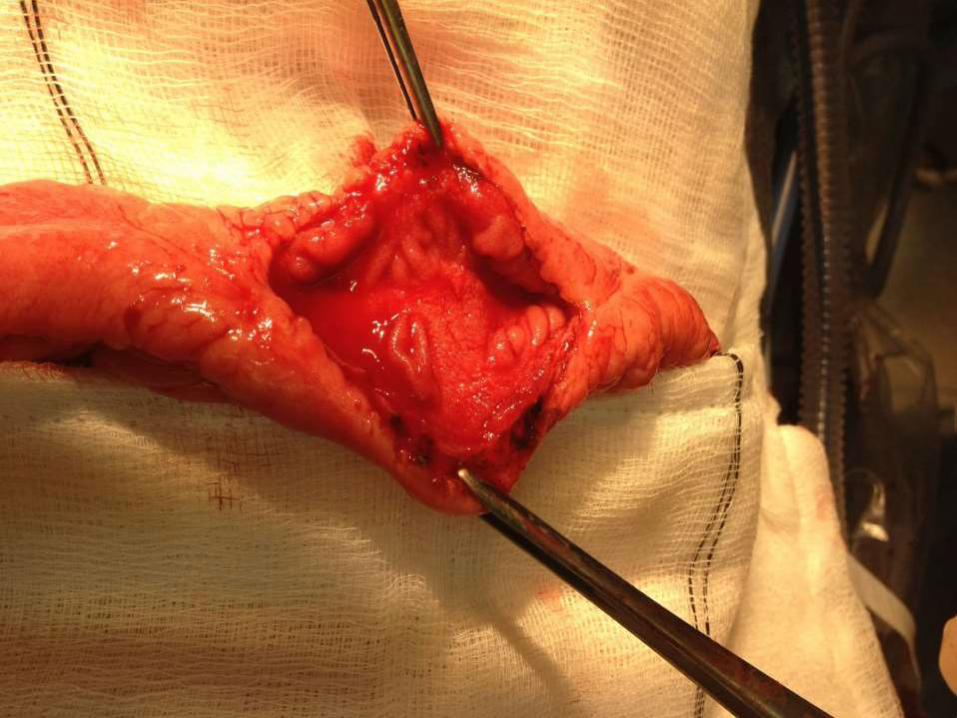
Hazards in Crohn’s surgery
The mesentery and risk of bleeding
Undetected fistula
State of small bowel- do not
miss a stricture

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
Types of strictureplasty

St Mark's Hospital
and Academic Institute
St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
`

St Mark's Hospital
and Academic Institute
strictureplasty is safe
• 1112 patients (1975-2005)
• 3259 strictureplasties– 81% Heineke-Mikulicz
– 10% Finney
– 5% Michelassi
• Surgical recurrence rate 23% – Site specific 3%
• 4 % septic complications (leak, abscess, fistula)
Yamamoto DCR 2007

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
Michelassi strictureplasty

St Mark's Hospital
and Academic Institute
Michellassi strictureplasty
-results
• Length of diseased bowel 20-68 cm
• Anastomotic haemorrhage 2%
• Anastomotic leak 1%
• Bowel obstruction 1%
• Enteric fistula from site of strictureplasty 20%
• 22% needed surgery for recurrent disease
– 7.7% of these for disease at site of previous
strictureplasty
• Average time to surgery after strictureplasty 35 months
• 5 year recurrence free survival 77%

St Mark's Hospital
and Academic Institute
Courtesy Andree D’Hoore UZ Leuven
Michelassi strictureplasty over the IC
valve provides ultimate bowel preservation

St Mark's Hospital
and Academic Institute
Isoperistaltic strictureplasty
extending over ilecaecal valve

St Mark's Hospital
and Academic Institute
caecum
Opened terminal ileum
Proximal diseased segment

St Mark's Hospital
and Academic Institute
Deep Ulcerations
IC valve

St Mark's Hospital
and Academic Institute
The Kono-S anastomosis

St Mark's Hospital
and Academic Institute
Kono-s Anastomosis

St Mark's Hospital
and Academic Institute
The mesentery as an organ
What is its role in Crohn’s disease ?
Are we heading to more radical
surgery for Crohn’s?
St Mark's Hospital
and Academic Institute
Crossroads in decision making
Medications Surgery

St Mark's Hospital
and Academic Institute
Laparoscopic Ileocolic Resection
or !nfliximab treatment of distal
ileitis in Crohn’s disease

St Mark's Hospital
and Academic Institute
No participation
Randomisation (N=130)
Laparoscopic ileocolic
resection (N=65)
Infliximab treatment
(N=65)
Follow-up for 12 months by trial nurse with
questionnaires
Analysis: quality of life, costs, morbidity
and mortality
Patients with Crohn´s disease
located in terminal ileum
Flow chart
LIR!C trial

St Mark's Hospital
and Academic Institute
LIR!C Trial
• 143 patients – after exclusions
– 65 for Infliximab and 70 for surgery
• No difference in Quality of Life after 1 year –
laparoscopic surgery non inferior
• 21 (31%) had to stop infliximab and 13 went on to
surgery
• 4% started infliximab after surgery
• Cheaper to have surgery but is this true in the era of
biosimilars?

St Mark's Hospital
and Academic Institute
• Is there a paradigm shift
• Move to reducing recurrence
• Role of medications and surgical complications
• Or are surgeons just losing touch with reality?
• Should we operate earlier?

St Mark's Hospital
and Academic Institute
Ulcerative colitis

St Mark's Hospital
and Academic Institute
Pouch procedures
and outcomes
• Only 26 surgeons in the UK
carried out more than 15
pouches in 5 years
• But 126 Surgeons perform
one pouch procedure in 5
years
• The concept of the occasional
pouch surgeon

St Mark's Hospital
and Academic Institute
Laparoscopic pouch surgery

St Mark's Hospital
and Academic Institute
Adhesions
• Significant reduction in adhesion related admission
attributed to laparoscopic surgery
Faiz et al 2011

St Mark's Hospital
and Academic Institute
Fecundity

St Mark's Hospital
and Academic Institute
fecundity
• Definite increase in time to first pregnancy after
laparoscopic pouch surgery
Bemelman et al 2010 Annals of Surgery

St Mark's Hospital
and Academic Institute
TATME
• Established as an alternative approach to rectal excision
• Overcomes some of the issues associated with
laparoscopic excision
• There is a learning curve
• How can we adopt to benign disease

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute

St Mark's Hospital
and Academic Institute
What additional benefits can we achieve for benign
disease
• Low anastomosis
• No need for multiple firings
• Double purse string
• ? Reduced leak rate
• Single port technique for proctectomy

St Mark's Hospital
and Academic Institute
Consequences of leak UC

St Mark's Hospital
and Academic Institute
No Leak
St Mark's Hospital
and Academic Institute
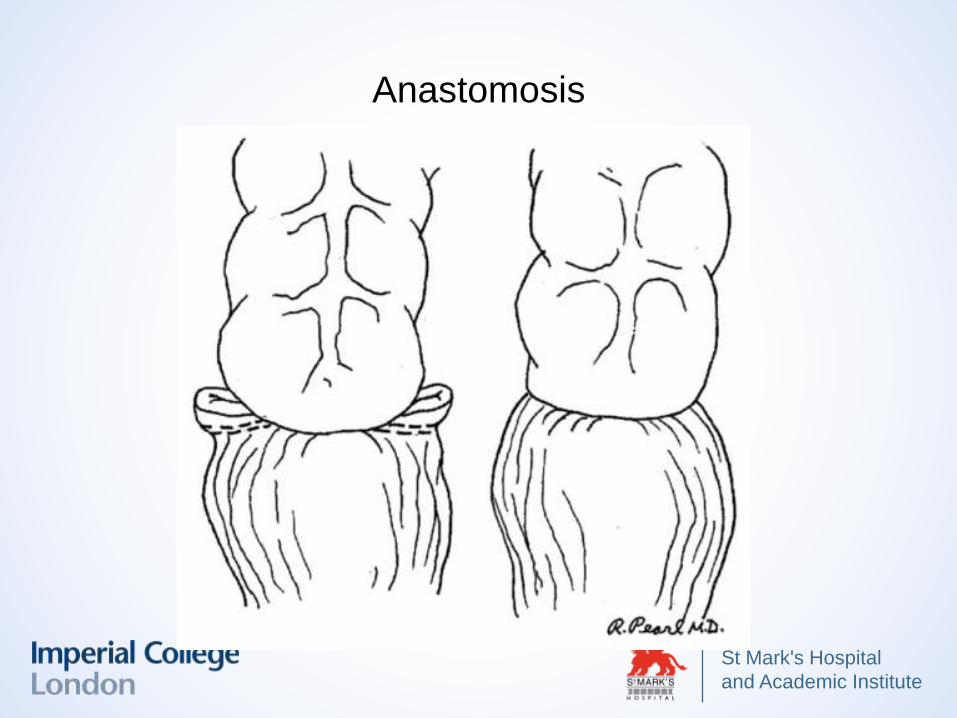
Anastomosis

St Mark's Hospital
and Academic Institute
Ileoanal Pouch: 2014 April to 2017
• SILS & TATME IPAA Cases: 32
• Not defunctioned: 6
• Complications: 8 (29.6%)
• Anastomotic stricture
– Simple dilatation: 5 (18.5%)
– ileostomy not reversed: 2 (7.4%)
• Pouch leak: 2 (6.25%)

St Mark's Hospital
and Academic Institute
Evolution of the Technique
• Males only to start
• Hand sewn anastomosis
• Stapled anastomosis with reinforcing
• Change of stapler and method of anastomosis
• No defunctioning

St Mark's Hospital
and Academic Institute
Quality of Life
• 47 patients St Mark’s and Milan with 12 month follow up
• Significant improvement in the 24h bowel frequency and
nocturnal frequency
• 80% of patients having 6 to 8 bowel movements
• 80% of patients reporting absence of nocturnal
frequency. A positive trend was also found in relation to
social, work, dietary and sexual activity during the 12
month follow up.

St Mark's Hospital
and Academic Institute
Quality of life assessment
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0 2 4 6 8 10 12 14
CGQL

St Mark's Hospital
and Academic Institute
Back to the future
• Is the appendix making a resurgence

St Mark's Hospital
and Academic Institute
Will these hold the key?

St Mark's Hospital
and Academic Institute
• IBD surgery is cutting edge
• Requires a different mind set with very much a
multidisciplinary approach
• Do not underestimate the value of the joint clinic