current endovascular management of ischemic stroke cuellar/endovascular management of... · current...
TRANSCRIPT

Current endovascular management of ischemic stroke
Hugo Cuellar, MD, PhDAssociate Professor of Neurosurgery
and RadiologyDirector of Neuronterventional Surgery
Disclosures
• Nothing to disclose

Objectives
• Evaluate latest technology for intracranial thrombectomy.
• Analize the results of latest endovascular trials for acute ischemic stroke.
Ischemic stroke
• Ischemic stroke usually results when an artery to the brain is blocked by a thrombotic or embolic occlusion and is more common than hemorrhagic stroke.
• If the clot breaks up spontaneously within less than 15 to 30 minutes, brain cells do not die and people's symptoms resolve. Such cases are called a transient ischemic attack (TIA).
• 20% mortality – 40% moderate to severe deficits.
Ischemic stroke
• Stroke is the leading cause of disability and the fourth leading cause of death in the United States.
• 82-92% of strokes in the United States are ischemic.
• Approximately 795,000 people in the United States experience new (610,000 people) or recurrent (185,000 people) stroke.
Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, et al. Heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. Jan 3 2012;125(1):e2-e220

Ischemic stroke
• Major risk factors: Atherosclerosis, High cholesterol, HTA, Diabetes, Smoking
• Consider stroke in any patient presenting with acute neurologic deficit or any alteration in level of consciousness.
• Initial goals: Confirm presence of stroke (CT-CTA), establish a baseline, establish severity (NIHSS), determine time of onset if possible.
Treatment
• IV- tPA
• 1996 FDA approved 0-3 hrs
• 2006 extend to 4.5 hrs
• AHA advisory.
• FDA had no position since 2008
• IV tPA 3-4.5hrs FDA approved with additional exclusions.
• In NINDS trial only 8% had favorable outcome if NIHSS> 20.

IV thrombolysis
• Rapid administration
• Greatest benefit in 60-90 minute window
• Efficacy decreases with time
• Efficacy decreases with burden of thrombus.
• 33% distal MCA
• 15% proximal MCA
• 24% tandem ICA/MCA
• 25% basilar artery
• 0% ICA ‘T’ occlusion
Stroke 2007. 38:948-952

Treatment
• Neurointerventional stroke rescue has grown rapidly over the last years.
• In addition to the oldest techniques that use IA tPA, we have a new expanding field of mechanical devices for fast revascularization.
• Time remains the most important part of stroke rescue.
Mazighi M, et al. Comparison of intravenous alteplase with a combined intravenous-endovascular approach in patients with stroke and confirmed arterial occlusion. Stroke 2009.
Evolution
• Intraarterial tPA -1998
• Mechanical embolus removal in cerebral ischemia (MERCI) FDA 2004.
• CATCH device 2005-EU
• PENUMBRA aspiration-2009 FDA
• SOLITAIRE-TREVO stent retrievers- 2012 FDA

MRCLEAN Study overview
Source: http://www.mrclean-trial.org/index.html, accessed 05Jun2014
Study MR CLEAN
Enrollment Period December 2010 – March 2014
Study Design Prospective, multi-center, randomized, controlled, blinded-endpoint trial
Tx Window 6 hrs
NIHSS 2 or more
Study ArmEndovascular treatment: intra-arterial thrombolysis (urokinase or alteplase), mechanical treatment (retraction or aspiration of the thrombus with a catheter guided device, or stenting) or both
Control Arm Medical management
Target Vessels Distal ICA, middle (M1/M2) or anterior (A1/A2) cerebral artery
Sample Size/Sites 500 pts, 18 sites in Netherlands
Primary EndpointsmRS at 90 daysRankin Shift
Secondary Endpoints NIHSS at 24 hours, vessel patency at 24 hours, infarct size at day 5-7, and the occurrence of major bleeding
Follow-up 24 hrs, 5-7 days, discharge, 90 days
Key In/ExclusionCriteria
• Intracranial occlusion of the distal intracranial ICA, middle (M1/M2) or anterior (A1/A2) cerebral artery, demonstrated with CTA, MRA, DSA or transcranial Doppler/duplex (TCD).
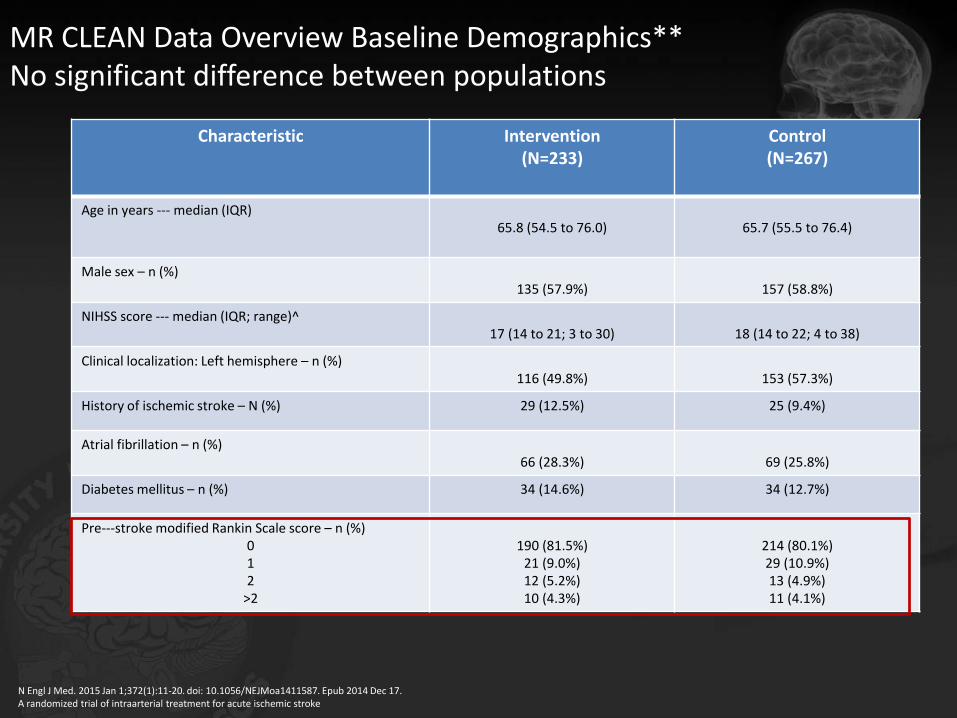
MR CLEAN Data Overview Baseline Demographics** No significant difference between populations
Characteristic Intervention(N=233)
Control(N=267)
Age in years --‐ median (IQR)65.8 (54.5 to 76.0) 65.7 (55.5 to 76.4)
Male sex – n (%)135 (57.9%) 157 (58.8%)
NIHSS score --‐ median (IQR; range)^17 (14 to 21; 3 to 30) 18 (14 to 22; 4 to 38)
Clinical localization: Left hemisphere – n (%)116 (49.8%) 153 (57.3%)
History of ischemic stroke – N (%) 29 (12.5%) 25 (9.4%)
Atrial fibrillation – n (%)66 (28.3%) 69 (25.8%)
Diabetes mellitus – n (%) 34 (14.6%) 34 (12.7%)
Pre--‐stroke modified Rankin Scale score – n (%)012
>2
190 (81.5%)21 (9.0%)12 (5.2%)10 (4.3%)
214 (80.1%)29 (10.9%)13 (4.9%)11 (4.1%)
N Engl J Med. 2015 Jan 1;372(1):11-20. doi: 10.1056/NEJMoa1411587. Epub 2014 Dec 17.A randomized trial of intraarterial treatment for acute ischemic stroke
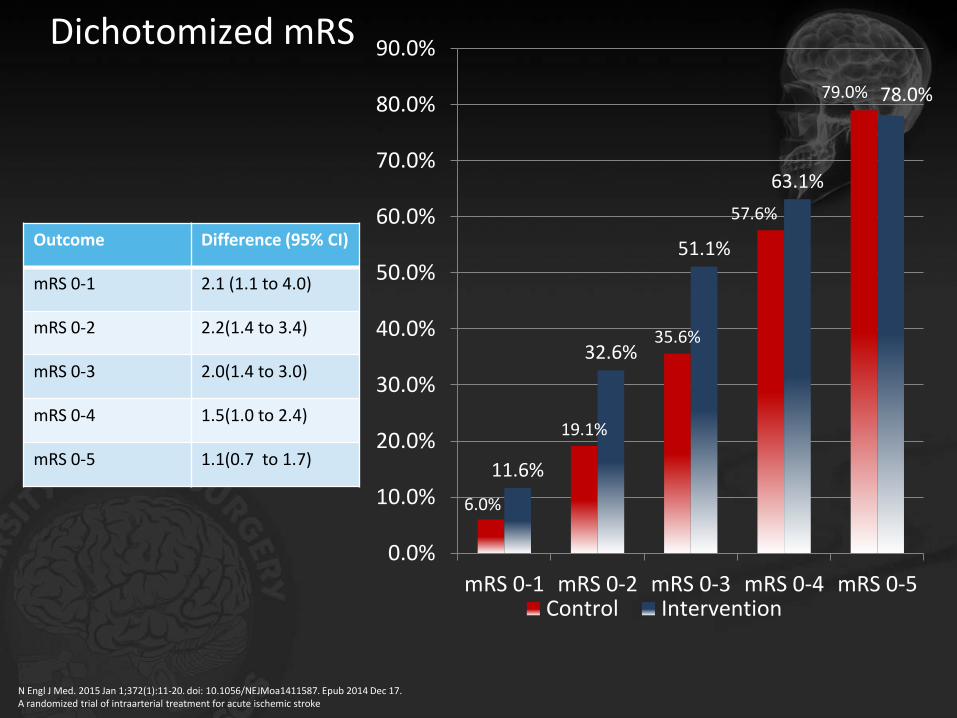
Dichotomized mRS
Outcome Difference (95% CI)
mRS 0-1 2.1 (1.1 to 4.0)
mRS 0-2 2.2(1.4 to 3.4)
mRS 0-3 2.0(1.4 to 3.0)
mRS 0-4 1.5(1.0 to 2.4)
mRS 0-5 1.1(0.7 to 1.7)
6.0%
19.1%
35.6%
57.6%
79.0%
11.6%
32.6%
51.1%
63.1%
78.0%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
mRS 0-1 mRS 0-2 mRS 0-3 mRS 0-4 mRS 0-5Control Intervention
N Engl J Med. 2015 Jan 1;372(1):11-20. doi: 10.1056/NEJMoa1411587. Epub 2014 Dec 17.A randomized trial of intraarterial treatment for acute ischemic stroke

Almost exclusively stent thrombectomy used
190 (97%)
1 (0%)5 (3%) Devices Used
Stent Retrievers
Thrombolysis
Other MechanicalDevices
N= 196 patients
N Engl J Med. 2015 Jan 1;372(1):11-20. doi: 10.1056/NEJMoa1411587. Epub 2014 Dec 17.A randomized trial of intraarterial treatment for acute ischemic stroke
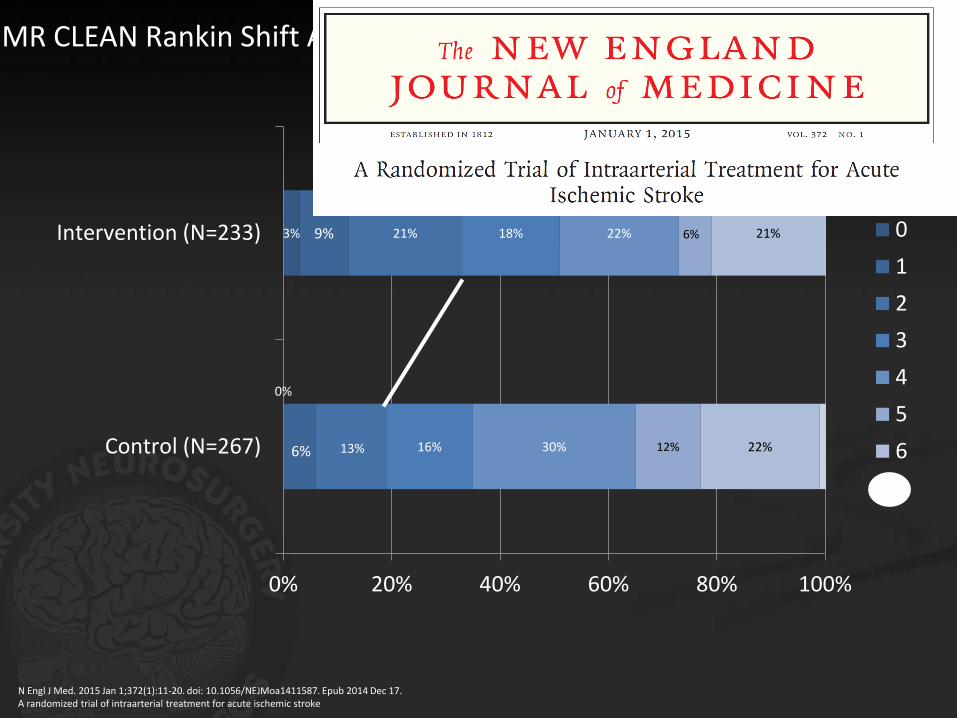
MR CLEAN Rankin Shift Analysis**
0%
3%
6%
9%
13%
21%
16%
18%
30%
22%
12%
6%
22%
21%
0% 20% 40% 60% 80% 100%
Control (N=267)
Intervention (N=233) 0
1
2
3
4
5
6
7
N Engl J Med. 2015 Jan 1;372(1):11-20. doi: 10.1056/NEJMoa1411587. Epub 2014 Dec 17.A randomized trial of intraarterial treatment for acute ischemic stroke

MR CLEAN (EU) SWIFT PRIME (Global) EXTEND IA (AUS, NZ) REVASCAT (Spain) ESCAPE (Global) Therapy (Global)
Randomization of patients to IV TPA vs. IV TPA + Endovascular
Time Window Studied Onset to 6 hours Onset to 6 hours Onset to 6 hours Onset to 8 hours Onset to 12 hours Onset to 5 hours
Trial FundingSupport
Funded by Dutch Heart
Foundation with small support from industry
Funded by CovidienFunded by Covidien
Investigator InitiatedFunded by Covidien
Investigator InitiatedFunded by Covidien
Investigator InitiatedFunded by Penumbra
Number of Patients 500 196 70 ~195 314 ~105
Analysis of Primary Endpoint
Rankin Shift Rankin ShiftReperfusion at 24 hrs
without sICH <72 hours
Rankin ShiftNIHSS 0-2 or mRS 0-2
at 90 daysmRS 0-2 at 90 days
Trial status Presented Trial haltedEfficacy endpoint
metTrial Stopped
Study stopped.Data with DSMB for
analysis.
Efficacy endpoint metTrial Stopped
DSMB reviewed data.Trial ongoing but not
recruiting.
Data Status
Presented at WSC; Data
published in NEJM
Presentation:Feb 11, ISC
publication pending
Presentation:Feb 11, ISC
publication pendingPresentation &
publication pending
Presentation:Feb 11, ISC
publication pending
No presentation or publication of data
scheduled
Primary Device Studied
Not Available Solitaire™ Device Solitaire™ Device Solitaire™ Device Solitaire™ DevicePenumbra™* Aspiration
System
Data will ONLY support evidence
for
All stent retrievers
Solitaire™ DeviceONLY
Solitaire™ DeviceONLY
Solitaire™ DeviceONLY
Solitaire™ DeviceONLY
Penumbra™* Aspiration System
Leading Investigator
DiederikDippel
(Netherlands)
Jeff Saver(USA)
Stephen Davis(Australia)
Tudor Jovin(USA)
Mayank Goyal(Canada)
Jay Mocco(USA)
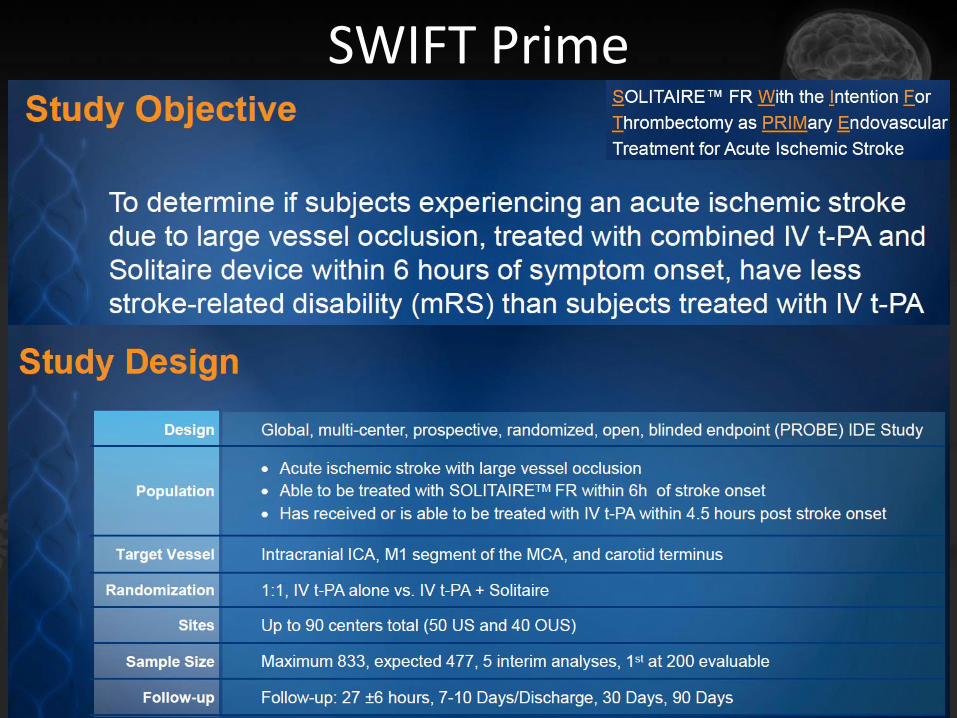
SWIFT Prime
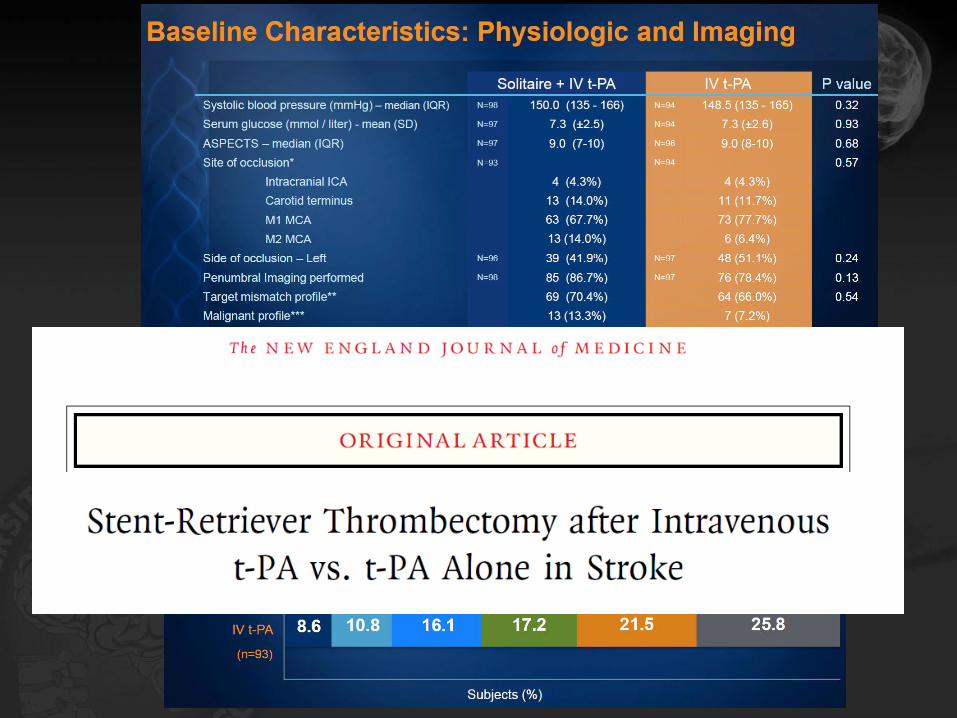
Reperfusion TICI 2b/3: 88%

EXTEND IA
• Extending the Time for Thrombolysis in Emergency Neurological Deficits – IntraArterial
• An investigator-initiated, multi-center, prospective, randomized, open-label, blinded-endpoint (PROBE) study in ischemic stroke patients receiving intravenous alteplase within 4.5h of stroke onset
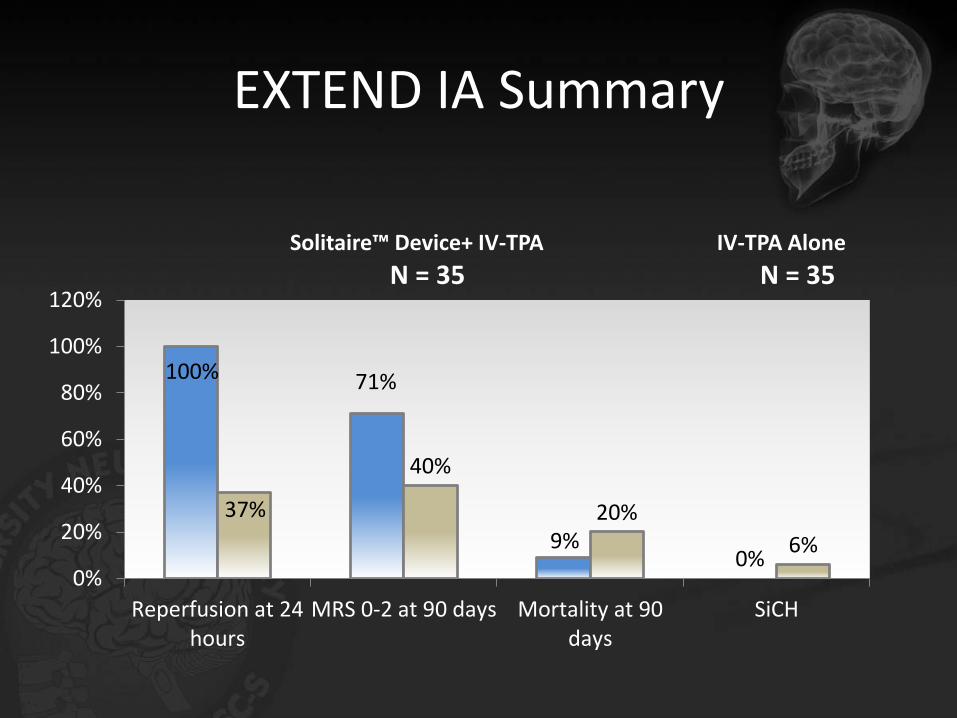
EXTEND IA Summary
100% 71%
9%0%
37%
40%
20%
6%
0%
20%
40%
60%
80%
100%
120%
Reperfusion at 24hours
MRS 0-2 at 90 days Mortality at 90days
SiCH
Solitaire™ Device+ IV-TPA IV-TPA Alone
N = 35 N = 35
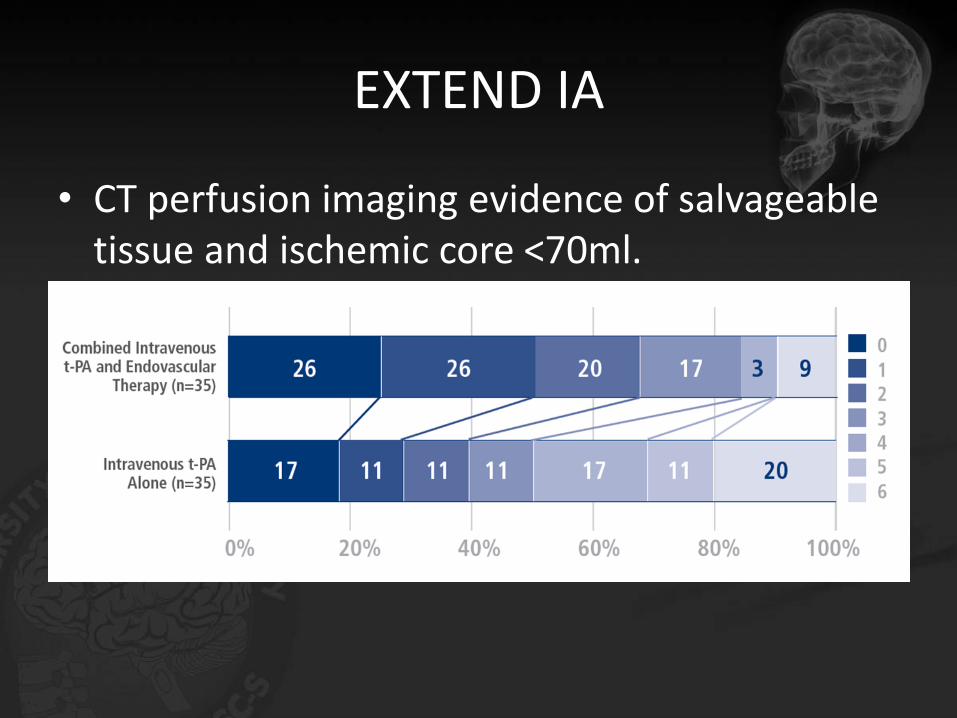
EXTEND IA
• CT perfusion imaging evidence of salvageable tissue and ischemic core <70ml.

ESCAPE
• Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke.
• Patients were included up to 12 hours from symptom onset. Computed Tomography (CT) and CT Angiography were used to exclude patients with large infarct core or poor collaterals, and document anterior circulation, proximal intracranial occlusion.
• ESCAPE assessed 316 patients and found that the addition of stent thrombectomy doubled patients’ rate of return to functional independence.

Rankin scale
• Among acute ischemic stroke patients with proximal vessel occlusion, small infarct core and good collaterals, rapid endovascular treatment [particularly with the Solitaire™ stent thrombectomy device as recommended primary technique] resulted in significant clinical benefit and reduced mortality.
REVASCAT
• Randomized trial of revascularization with Soilitaire versus best medical therapy in the treatment of acute stroke due to anterior circulation large vessel occlusion within 8 hrs.
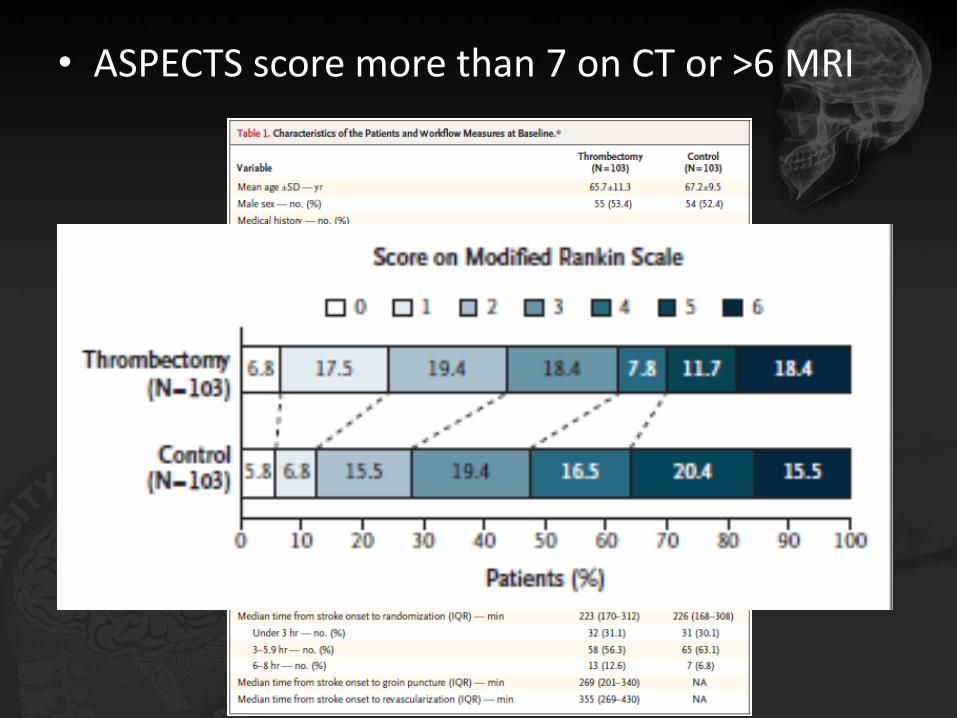
• ASPECTS score more than 7 on CT or >6 MRI
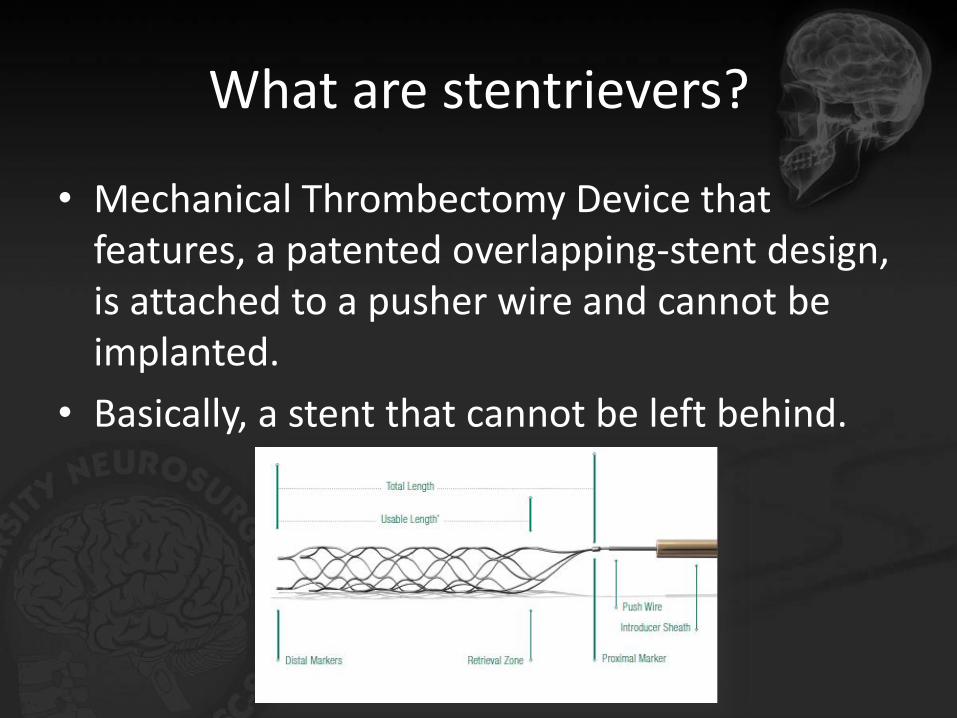
What are stentrievers?
• Mechanical Thrombectomy Device that features, a patented overlapping-stent design, is attached to a pusher wire and cannot be implanted.
• Basically, a stent that cannot be left behind.

• 2012 FDA approved, CE marked since Dec 2007.
• Up to 6 hrs or use with advanced imaging.
• Time is relative, we move towards physiologicselection.
• 75-90% TIMI 2-3 recanalization.
• 55 % mRS less than 2 at 90 days.
• Stroke. 2012 Oct;43(10):2699-705. Epub 2012 Jul 31.
Retrospective Multicenter Study of Solitaire FR for Revascularization in the Treatment of Acute Ischemic Stroke.
• Lancet. 2012 Oct 6;380(9849):1231-40. doi: 10.1016/S0140-6736(12)61299-9. Epub 2012 Aug 26.
Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions inacute ischaemic stroke (TREVO 2): a randomised trial.
Stentrievers (Solitaire-Trevo)
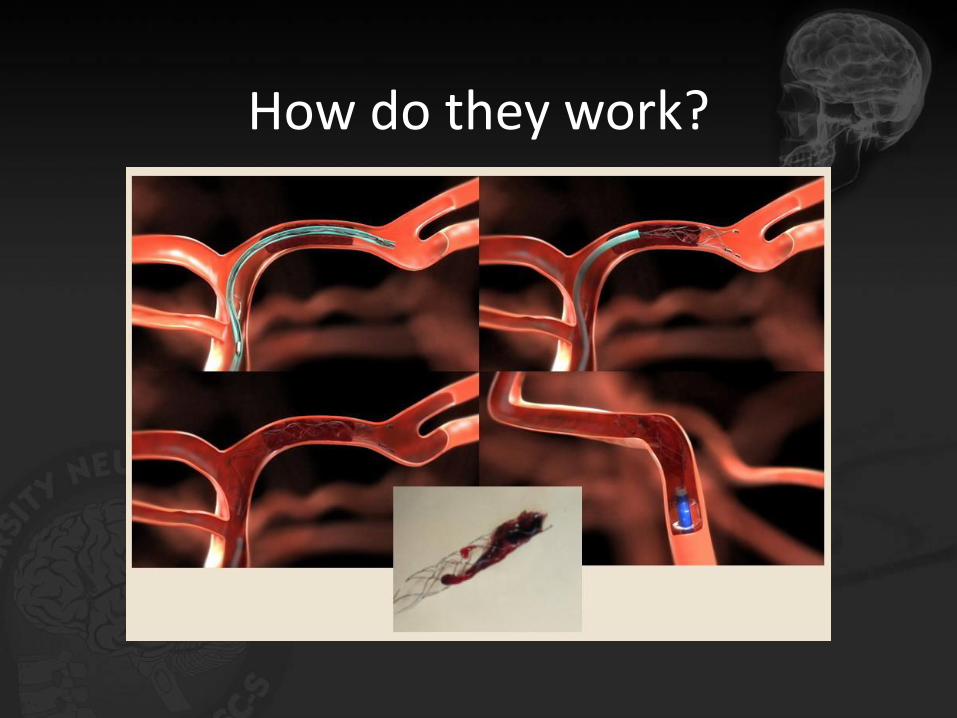
How do they work?

55 yo male with left side hemiparesis. 5 hrs onset.

Stentriever

Stentriever

Ischemic stroke
• What to do?
Stroke symptoms
CT AND CTAHemorrhage/changes?
Stop
Major branch occlusion?
yesno
no Stop
yes
Neurointerventional suite
If 0-4.5 hrs give IVtPA AND
ICA-M2, VBAASPECTS 6-10
2015 AHA/ASA Focused Update
Guidelines for the Early Management of Patients with Acute Ischemic Stroke

Guideline Classifications
CLASS 1 (STRONG) Benefit >>> Risk
Suggested phrases for writing recommendations
• Is recommended
• Is indicated/useful/effective/beneficial
• Should be performed/administered/other
CLASS (STRENGTH) OF RECOMMENDATION
CLASS 2a (MODERATE) Benefit >> Risk
Suggested phrases for writing recommendations
• Is recommended
• Is indicated/useful/effective/beneficial
• Should be performed/administered/other
CLASS 2b (WEAK) Benefit ≥ Risk
Suggested phrases for writing recommendations
• May/might be reasonable
• May/might be considered• Usefulness/effectiveness is unknown/unclear, uncertain or not well
established
CLASS 3: No Benefit (MODERATE) Benefit = Risk
Suggested phrases for writing recommendations
• Is not recommended• Is not indicated/useful/effective/beneficial• Should not be performed/administered/other
CLASS 3: Harm (STRONG) Benefit < Risk
Suggested phrases for writing recommendations
• Is not recommended• Is not indicated/useful/effective/beneficial• Should not be preformed/administered/other
LEVEL A
• High-quality evidence from more than 1 randomized controlled trial
• Is indicated/useful/effective/beneficial
• Should be performed/administered/other
LEVEL B-R (Randomized)
• Moderate-quality evidence from 1 or more randomized controlled trial
• Meta-analysis of moderate-quality randomized controlled trial
LEVEL B-NR (Nonrandomized)
• Moderate-quality evidence from 1 or more well-designed, well-executed nonrandomized studies, observational studies, or registry studies
• Meta-analyses of such studies
LEVEL C
• Randomized or nonrandomized observational or registry studies with limitations of design or execution
• Meta-analyses of such studies
LEVEL E
• Consensus of expert opinion based on clinical experience with evidence is insufficient, vague, or conflicting
LEVEL (QUALITY) OF EVIDENCE
Focused Update Sections
Endovascular Interventions
Imaging Systems of Stroke Care
Section 1 Section 2 Section 3

Endovascular Interventions
Imaging Systems of Stroke Care
Section 1 Section 2 Section 3

Endovascular Interventions
1) Patients eligible for IV rtPA should receive IV rtPA even if endovascular treatments are being considered (Class I; Level of Evidence A).
new revised unchanged
Strong

2) Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria:
• pre-stroke modified Rankin score (mRS) 0-1
• acute ischemic stroke receiving IV rtPA within 4.5 hours of onset according to guidelines from professional medical societies,
• causative occlusion of the internal carotid artery or proximal middle cerebral artery (M1),
• age 18 years and over,
• National Institutes of Health Stroke Scale (NIHSS) score of 6 or greater,
• Alberta Stroke Program Early Computed Tomography Score (ASPECTS) of 6 or greater, and
• treatment can be initiated (groin puncture) within 6 hours of symptom onset
(Class I; Level of Evidence A).
Endovascular Interventionsnew revised unchanged
Strong

Endovascular Intervention
3) As with IV rtPA, reduced time from symptom onset to reperfusion with endovascular therapies is highly associated with better clinical outcomes. To ensure benefit, reperfusion to TICI grade 2b/3 should be achieved as early as possible and within 6 hours of stroke onset (Class I; Level of Evidence B-R).
new revised unchanged
Strong
Endovascular Intervention
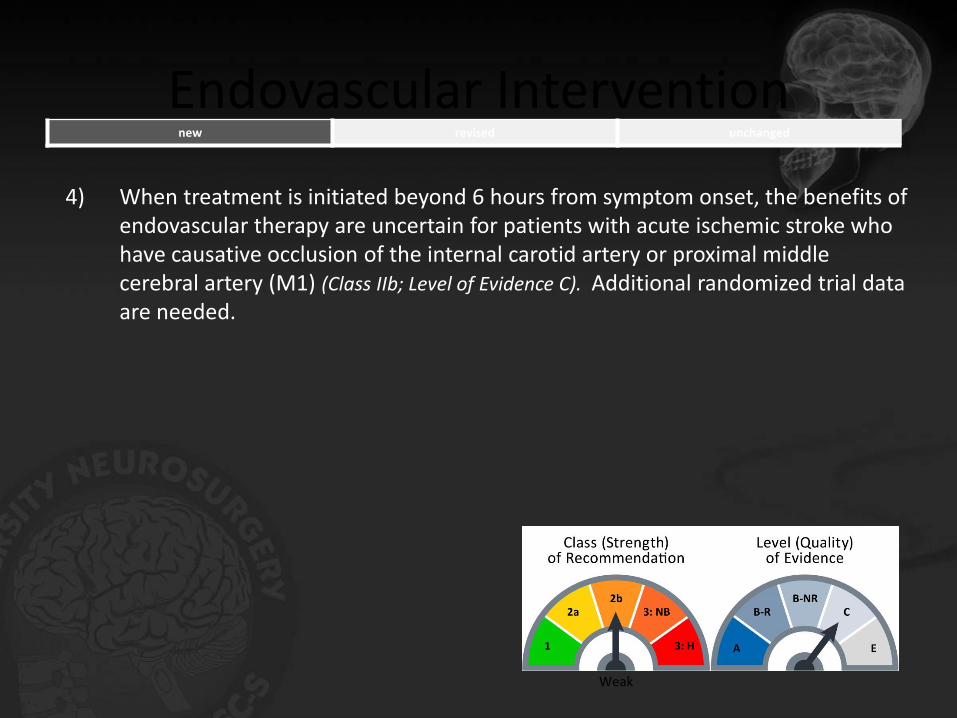
4) When treatment is initiated beyond 6 hours from symptom onset, the benefits of endovascular therapy are uncertain for patients with acute ischemic stroke who have causative occlusion of the internal carotid artery or proximal middle cerebral artery (M1) (Class IIb; Level of Evidence C). Additional randomized trial data are needed.
new revised unchanged
Weak

Endovascular Intervention
5) In carefully selected patients with anterior circulation occlusion who have contraindications to IV rtPA, endovascular therapy with stent retrievers completed within 6 hours of stroke onset is reasonable (Class IIa; Level of Evidence
C). There are inadequate data available at this time to determine the clinical efficacy of endovascular therapy with stent retrievers for those patients whose contraindications are time-based or non-time based (such as prior stroke, serious head trauma, hemorrhagic coagulopathy or receiving anticoagulant medications).
new revised unchanged
Moderate

Summary
• Mechanical thrombectomy with stentrievers has finally proven better outcomes than IV-tPA alone and has achieved level 1A evidence.
• Use of MRI was discouraged in all studies.
• If faced with a stroke patient:– Order CT and CTA at same time.
– Give IV tpa if indicated and transfer to center with endovascular capabilities.
– Look for major branch occlusion and calculate ASPECTS score
– Rule of 6: NIHSS>6, < 6hrs onset, ASPECTS >6
