cure of chronic viral infection by neutralizing antibody treatment
TRANSCRIPT
(2007) 267–271www.elsevier.com/locate/autrev
Autoimmunity Reviews 6
Cure of chronic viral infection by neutralizing antibody treatment
Mette Ejrnaes ⁎, Matthias G. von Herrath
La Jolla Institute for Allergy and Immunology, San Diego, CA, USA
Available online 12 October 2006
Abstract
Persistent infections can pose severe health risks. In many cases individuals fail to clear the virus and consequently chronicinfection, often associated with severe immunopathology, occurs. For some chronic infections it is known that systemic IL-10production can be increased. However, it is unclear, whether IL-10 affects the outcome of infection, amount ofimmunopathology and could be the actual cause for persistence. Conventional interferons (IFN) or anti-viral immunotherapiesattempting to augment anti-viral immunity directly in persistent infected individuals have failed to affect the outcome so far, butlowering the viral antigenic load has clear beneficial effects. Therefore, approaching the problem from a different angle isimportant. The use of neutralizing antibodies is one of the most successful methods to interfere with receptor-ligand interactionsin vivo. Optimal designs of therapeutic antibody treatment regimen are important in order to achieve maximal effects withminimal duration of immunosuppression or hyperactivation. In this review we reflect on the effects of a short time administrationof a neutralizing cytokine receptor antibody treatment of a chronic infection resulting in the establishment of anti-viral immuneresponses and viral clearance and speculate on the potential mechanisms involved in this successful therapeutic treatment.© 2006 Elsevier B.V. All rights reserved.
Keywords: Chronic infection; LCMV; Autoimmunity; Immune-regulation
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2671.1. Modulatory functions of IL-10 and effects in viral infections . . . . . . . . . . . . . . . . . . . . . . . . . 2671.2. The lymphocytic choriomeningitis virus model as a model of chronic viral infection . . . . . . . . . . . . . 2681.3. Potential clinical applications of neutralizing antibodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 268
2. Possible mechanisms involved in resolution of chronic viral infection upon blocking of IL-10 signaling . . . . . . . 269Take-home messages. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 270References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 270
⁎ Corresponding author. Department of Developmental ImmunologyLa Jolla Institute for Allergy and Immunology 10355 Science CenterDr San Diego, CA 92121 USA. Tel.: +1 858 558 3581; fax: +1 858558 3579.
E-mail address: [email protected] (M. Ejrnaes).
1568-9972/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.autrev.2006.09.002
1. Introduction
1.1. Modulatory functions of IL-10 and effects in viralinfections
Interleukin-10 (IL-10) is an immunosuppressivecytokine with implications for various immune and

268 M. Ejrnaes, M.G. von Herrath / Autoimmunity Reviews 6 (2007) 267–271
inflammatory diseases. IL-10 is produced by monocytes,macrophages, B cells, murine Th2 cells and someCD8+ Tcells [1,2]. In different cell types, the duration ofstimulation affects IL-10 expression differentially. Forexample upon lipopolysaccharide (LPS) or IFN-γactivation pro-inflammatory cytokines are rapidly pro-duced by macrophages, whereas IL-10 secretion isdelayed. Once IL-10 is produced it inhibits a broadspectrum of cellular immune responses, acting onantigen-presenting cells (APC) by i.e. preventing den-dritic cell (DC) maturation and thereby keeping the cellsin an immature state, and on B and T cells by inhibitingpro-inflammatory cytokine production [1]. Investigationshave revealed that more specifically IL-10 play importantroles in regulating expression of cell surface moleculesinvolved in activation and costimulation, hereunderMHCclass II, CD80, and CD86 [3,4] as well as chemokinesecretion [5,6] and modification of chemokine receptorexpression [7,8] (reviewed in [9]). Apart from thereported potent immune-modulatory effects on APCs,IL-10 also affects the balance of Th1- and Th2-typeimmune responses, as evidenced by findings in asthma,transplantation, tumor and autoimmunity models in vivo,as well as the outcome/duration of a viral infection.
Elevated levels of IL-10 mRNA have been observedin immune-responsive versus non-responsive metastaticmelanoma lesions [10]. Moreover, treatment with acombination of anti-IL-10 receptor (IL-10R) monoclo-nal antibody (mAb) and toll-like receptor 9 (TLR9)ligands has been shown to have potent therapeutic anti-tumor effects [11,12], pointing to the role of IL-10 in thedevelopment of cancer. Furthermore, IL-10 has alsobeen shown to play a role in the establishment of certainchronic viral infections such as human immunodefi-ciency virus (HIV-1) [13], hepatitis C (HCV) and humancytomegalovirus (HCMV) infections [14]. Interestingly,an increase in systemic IL-10 production has beendemonstrated upon HCV infection [15], and in somecases of infection with HIV [13,16–19].
1.2. The lymphocytic choriomeningitis virus model as amodel of chronic viral infection
Lymphocytic choriomeningitis virus (LCMV) belongsto the arena virus family and is a natural pathogen for bothhumans and mice [20]. LCMV infection of mice hasproven to be one of the most informative experimentalsystems for investigating various aspects of virology andimmunology. The various LCMV models offer forexample induction of acute infection upon LCMVArmstrong inoculation, associated with a rapid clearanceof the infection and immune-competent recipient with the
establishment of a stable memory T cell pool [21,22]. Incontrast inoculation with the LCMV variant Cl13, whichdiffers from its parent (LCMV Arm) virus at only oneamino acid positions in the virus glycoprotein isassociated with both functional impairment and deletionof virus-specific CD8 T cells and general immunosup-pression [23,24] leading to the establishment of a chronicinfection. Both systems are highly informative and arewell suited to reflect immune kinetics as they might occurin a variety of human chronic infections.
Alpha-dystroglycan (α-DG), a peripheral membraneprotein was identified as the receptor for LCMV [25]. Astronger binding of Cl13 to α-DG as compared to theArmstrong strain [26] was reported, indicating that theaffinity of the viral binding to its receptor might be acrucial element in determining the outcome of infectionwith LCMVArmstrong (lower affinity to α-DG) versusCl13 (high affinity to α-DG). Additionally, it has beenshown that differences in binding affinities of LCMVstrains to α-DG correlated with viral tropism and diseasekinetics [26], as LCMV Cl13 appears to cause a higherlevel of infection of APCs in the white pulp, includingperiarterial interdigitating DCs. Following, anti-viralCD8+ CTLs target these infected cells more effectivelyand consequently this CD8-dependent destruction of DCsin Cl13-infected mice leads to the ensuing immunosup-pression [27]. In vitro studies showing a decline of DCsafter infection with Cl13 but not LCMVArm support therelationship between loss of infected DCs and type ofviral infection [28]. Interestingly, this publication anddata fromour lab also shows a loss ofDCs, predominantlyrestricted to the CD11c+CD8α+ population and to a muchlesser extend the CD11c+CD8α− DC population.
1.3. Potential clinical applications of neutralizingantibodies
In contrast to acute infections, chronic viral infectionsare often amenable to IFN therapy. Among these,hepatitis C virus (HCV) and hepatitis B virus (HBV)infections are themost important and IFN-α is currently astandard treatment in HCV and HBV infections.Additionally, specific immunization strategies havebeen combined with direct anti-viral drug treatments,for example protease inhibitors and highly activeantiretroviral therapy (HAART) in HIV [29] andinterferon administration, and ribavirin in hepatitisinfections [30,31]. In all of the situations, where anti-viral drugs were employed, viral loads were significantlyreduced. However, complete elimination of the pathogenhas remained elusive, despite the fact that anti-viralimmunity was significantly increased in many instances.
269M. Ejrnaes, M.G. von Herrath / Autoimmunity Reviews 6 (2007) 267–271
Much attention has been paid to the role if IL-10 inviral infections as a potent anti-inflammatory immuno-suppressive cytokine with important potential clinicalapplications and the dual roles IL-10 plays in variousdiseases and therapeutic approaches to manipulating theeffect of IL-10 was recently described in detail byAsadullah and colleagues [32]. One major concern inclinically manipulating the levels of IL-10 is its criticalrole in the immune homeostasis. Long term applicationof IL-10 could cause immunodeficiency, whereascontinuous use of anti-IL-10 may lead to hyper-immunereactivation. However, blocking the cytokine receptoritself for a short period of time is a relative novelapproach to control the signaling effects of the cytokine.
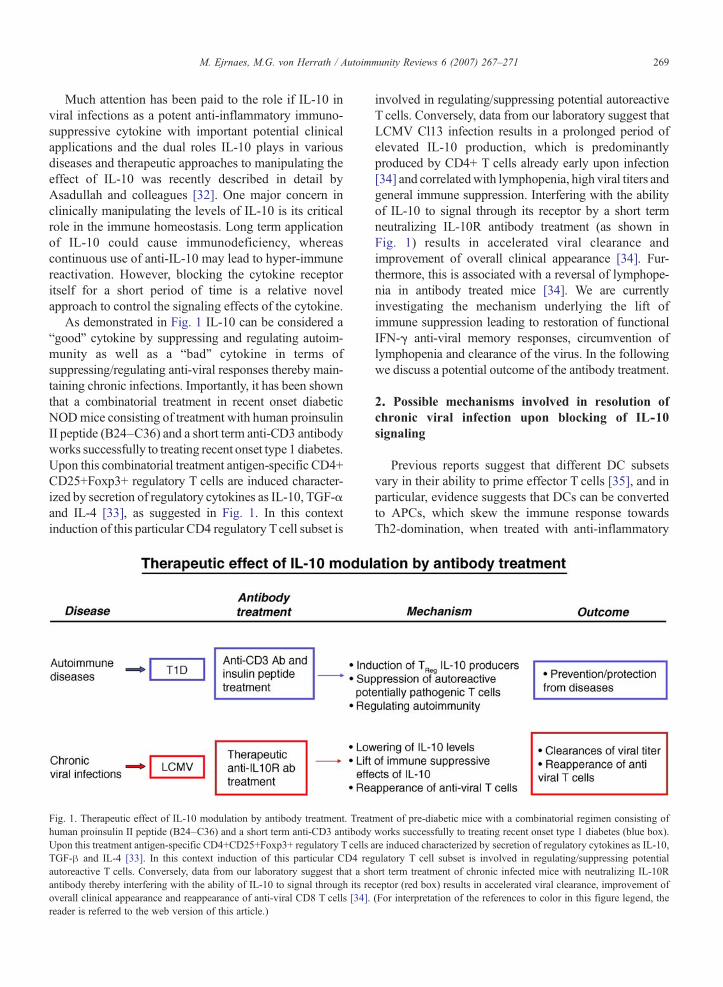
As demonstrated in Fig. 1 IL-10 can be considered a“good” cytokine by suppressing and regulating autoim-munity as well as a “bad” cytokine in terms ofsuppressing/regulating anti-viral responses thereby main-taining chronic infections. Importantly, it has been shownthat a combinatorial treatment in recent onset diabeticNODmice consisting of treatment with human proinsulinII peptide (B24–C36) and a short term anti-CD3 antibodyworks successfully to treating recent onset type 1 diabetes.Upon this combinatorial treatment antigen-specific CD4+CD25+Foxp3+ regulatory T cells are induced character-ized by secretion of regulatory cytokines as IL-10, TGF-αand IL-4 [33], as suggested in Fig. 1. In this contextinduction of this particular CD4 regulatory Tcell subset is
Fig. 1. Therapeutic effect of IL-10 modulation by antibody treatment. Treathuman proinsulin II peptide (B24–C36) and a short term anti-CD3 antibodyUpon this treatment antigen-specific CD4+CD25+Foxp3+ regulatory T cells aTGF-β and IL-4 [33]. In this context induction of this particular CD4 regautoreactive T cells. Conversely, data from our laboratory suggest that a shantibody thereby interfering with the ability of IL-10 to signal through its reoverall clinical appearance and reappearance of anti-viral CD8 T cells [34].reader is referred to the web version of this article.)
involved in regulating/suppressing potential autoreactiveT cells. Conversely, data from our laboratory suggest thatLCMV Cl13 infection results in a prolonged period ofelevated IL-10 production, which is predominantlyproduced by CD4+ T cells already early upon infection[34] and correlatedwith lymphopenia, high viral titers andgeneral immune suppression. Interfering with the abilityof IL-10 to signal through its receptor by a short termneutralizing IL-10R antibody treatment (as shown inFig. 1) results in accelerated viral clearance andimprovement of overall clinical appearance [34]. Fur-thermore, this is associated with a reversal of lymphope-nia in antibody treated mice [34]. We are currentlyinvestigating the mechanism underlying the lift ofimmune suppression leading to restoration of functionalIFN-γ anti-viral memory responses, circumvention oflymphopenia and clearance of the virus. In the followingwe discuss a potential outcome of the antibody treatment.
2. Possible mechanisms involved in resolution ofchronic viral infection upon blocking of IL-10signaling
Previous reports suggest that different DC subsetsvary in their ability to prime effector T cells [35], and inparticular, evidence suggests that DCs can be convertedto APCs, which skew the immune response towardsTh2-domination, when treated with anti-inflammatory
ment of pre-diabetic mice with a combinatorial regimen consisting ofworks successfully to treating recent onset type 1 diabetes (blue box).re induced characterized by secretion of regulatory cytokines as IL-10,ulatory T cell subset is involved in regulating/suppressing potentialort term treatment of chronic infected mice with neutralizing IL-10Rceptor (red box) results in accelerated viral clearance, improvement of(For interpretation of the references to color in this figure legend, the

270 M. Ejrnaes, M.G. von Herrath / Autoimmunity Reviews 6 (2007) 267–271
cytokines such as IL-10 [35,36]. Subclasses of DCs havebeen shown to have the potential to differentially skewcytokine production towards Th1- or Th2-profiles [37].Notably, it has been suggested that CD8α− DCs induceTh2-profiles whereas CD8α+ DCs preferentially stimu-late IFN-γ production and therefore induce Th1 profiles[38]. In this context we find that activation of IL-10-producing virus-specific CD4+ T cells LCMV-specific Tcells in chronically infected mice is linked to interactionwith CD8α− DCs. Considering that the generalized stateof lymphopenia induced by Cl13 infection might bemediated by APC subsets inducing IL-10 production,this might lead to 1) either down-regulation of pro-inflammatory responses in a general manner or, 2) morespecifically, inhibit the induction or expansion of anti-viral CTLs, 3) IL-10 may directly decrease the viabilityof CD8α+ DCs as has been previously suggested[39,40]. In the state of chronic Cl13 infection, prominentCD8α− DCs with reduced ability to prime Th1/Tc1effectors “by default” become the modulators of the Tcell response and thus derail anti-LCMV immunitythrough the production of IL-10. While the precise modeof action of IL-10 is unknown, LCMV-specific immunecells activated in this context may in turn acquire theability to produce IL-10 and provide inappropriate orinsufficient anti-viral help to other cell types, in par-ticular CD8+ T cells, thus leading to persistent infection.The remaining CD8α− DCs, which appear ill-equippedto propagate anti-viral effectors, are potential supportersof further IL-10 production. Following, elevated con-centrations of IL-10 in the milieu may thus lead to furthermodulation of DC function and thereby a vicious circle isestablished. As a consequence, only disruption of IL-10signaling will have the ability to break this circle andenable the recovery of appropriate anti-viral immunityby the infected host. Since blockade of IL-10 signalinglikely directly acts on DCs, a central switch in immunitycould be implanted in this way directly at the core, wheremost immune responses are orchestrated.
We are currently expanding our investigations of theunderlying mechanisms and particularly working atnarrowing down the optimal timing of anti-IL-10R abtreatment with potential translation to human chronicviral infections.
Take-home messages
• Chronic viral infections are often associated withelevated levels of IL-10.
• IL-10 treatment has varying therapeutic effects.• Neutralizing IL-10 receptor antibody treatment clearschronic viral infection.
• Restoration of anti-viral T cell responses followingtherapeutic IL-10R treatment in chronic infectedmice points to a immunosuppressive role of IL-10 inmaintaining disease.
• Optimal timing of anti-IL10R ab treatment is essentialin as much as early treatment is more efficacious ascompared to late treatments post-infection.
References
[1] Fiorentino DF, Zlotnik A, Vieira P, Mosmann TR, Howard M,MooreKW, et al. IL-10 acts on the antigen-presenting cell to inhibitcytokine production by Th1 cells. J Immunol 1991;146:3444.
[2] O'GarraA, StapletonG,DharV, PearceM, Schumacher J, RugoH,et al. Production of cytokines by mouse B cells: B lymphomas andnormal B cells produce interleukin 10. Int Immunol 1990;2:821.
[3] Ding L, Linsley PS, Huang LY, Germain RN, Shevach EM. IL-10inhibits macrophage costimulatory activity by selectively inhibit-ing the up-regulation of B7 expression. J Immunol 1993;151:1224.
[4] Willems F, Marchant A, Delville JP, Gerard C, Delvaux A, VeluT, et al. Interleukin-10 inhibits B7 and intercellular adhesionmolecule-1 expression on human monocytes. Eur J Immunol1994;24:1007.
[5] Jinquan T, Larsen CG, Gesser B, Matsushima K, Thestrup-Pedersen K. Human IL-10 is a chemoattractant for CD8+ Tlymphocytes and an inhibitor of IL-8-induced CD4+ T lympho-cyte migration. J Immunol 1993;151:4545.
[6] Kasama T, Strieter RM, Lukacs NW, Burdick MD, Kunkel SL.Regulation of neutrophil-derived chemokine expression by IL-10. J Immunol 1994;152:3559.
[7] Sozzani S, Ghezzi S, Iannolo G, Luini W, Borsatti A, PolentaruttiN, et al. Interleukin 10 increases CCR5 expression and HIVinfection in human monocytes. J Exp Med 1998;187:439.
[8] Takayama T, Morelli AE, Onai N, Hirao M, Matsushima K,Tahara H, et al. Mammalian and viral IL-10 enhance C-Cchemokine receptor 5 but down-regulate C-C chemokine receptor7 expression by myeloid dendritic cells: impact on chemotacticresponses and in vivo homing ability. J Immunol 2001;166:7136.
[9] Pestka S, Krause CD, Sarkar D, Walter MR, Shi Y, Fisher PB.Interleukin-10 and related cytokines and receptors. Annu RevImmunol 2004;22:929.
[10] Mocellin S, Ohnmacht GA, Wang E, Marincola FM. Kinetics ofcytokine expression in melanoma metastases classifies immuneresponsiveness. Int J Cancer 2001;93:236.
[11] Vicari AP, Trinchieri G. Interleukin-10 in viral diseases andcancer: exiting the labyrinth? Immunol Rev 2004;202:223.
[12] Vicari AP, Chiodoni C, Vaure C, Ait-Yahia S, Dercamp C,Matsos F, et al. Reversal of tumor-induced dendritic cell paralysisby CpG immunostimulatory oligonucleotide and anti-interleukin10 receptor antibody. J Exp Med 2002;196:541.
[13] Granelli-Piperno A, Golebiowska A, Trumpfheller C, Siegal FP,Steinman RM. HIV-1-infected monocyte-derived dendritic cellsdo not undergo maturation but can elicit IL-10 production and Tcell regulation. Proc Natl Acad Sci U S A 2004;101:7669.
[14] Rigopoulou EI, Abbott WG, Haigh P, Naoumov NV. Blocking ofinterleukin-10 receptor-a novel approach to stimulate T-helpercell type 1 responses to hepatitis C virus. Clin Immunol 2005;117:57.
[15] Accapezzato D, Francavilla V, Paroli M, Casciaro M, Chircu LV,Cividini A, et al. Hepatic expansion of a virus-specific regulatory

271M. Ejrnaes, M.G. von Herrath / Autoimmunity Reviews 6 (2007) 267–271
CD8(+) T cell population in chronic hepatitis C virus infection.J Clin Invest 2004;113:963.
[16] Ameglio F, Cordiali Fei P, Solmone M, Bonifati C, Prignano G,Giglio A, et al. Serum IL-10 levels in HIV-positive subjects:correlation with CDC stages. J Biol Regul Homeost Agents1994;8:48.
[17] Ji J, Sahu GK, Braciale VL, Cloyd MW. HIV-1 induces IL-10production in human monocytes via a CD4-independent pathway.Int Immunol 2005;17:729.
[18] Autran B, Legac E, Blanc C, Debre P. ATh0/Th2-like function ofCD4+CD7-T helper cells from normal donors and HIV-infectedpatients. J Immunol 1995;154:1408.
[19] Akridge RE, Oyafuso LK, Reed SG. IL-10 is induced duringHIV-1 infection and is capable of decreasing viral replication inhuman macrophages. J Immunol 1994;153:5782.
[20] Zinkernagel RM, Doherty PC. Restriction of in vitro T cell-mediated cytotoxicity in lymphocytic choriomeningitis within asyngeneic or semiallogeneic system. Nature 1974;248:701.
[21] Marker O, Volkert M. Studies on cell-mediated immunity tolymphocytic choriomeningitis virus in mice. J Exp Med 1973;137:1511.
[22] Moskophidis D, Assmann-Wischer U, Simon MM, Lehmann-Grube F. The immune response of the mouse to lymphocyticchoriomeningitis virus. V. High numbers of cytolytic Tlymphocytes are generated in the spleen during acute infection.Eur J Immunol 1987;17:937.
[23] Moskophidis D, Lechner F, Pircher H, Zinkernagel RM. Viruspersistence in acutely infected immunocompetent mice by ex-haustion of antiviral cytotoxic effector T cells. Nature 1993;362:758.
[24] Lin MY, Welsh RM. Stability and diversity of T cell receptorrepertoire usage during lymphocytic choriomeningitis virusinfection of mice. J Exp Med 1998;188:1993.
[25] Cao W, Henry MD, Borrow P, Yamada H, Elder JH, Ravkov EV,et al. Identification of alpha-dystroglycan as a receptor forlymphocytic choriomeningitis virus and Lassa fever virus.Science 1998;282:2079.
[26] Smelt SC, Borrow P, Kunz S, Cao W, Tishon A, Lewicki H, et al.Differences in affinity of binding of lymphocytic choriomenin-gitis virus strains to the cellular receptor alphadystroglycancorrelate with viral tropism and disease kinetics. J Virol 2001;75:448.
[27] Borrow P, Evans CF, Oldstone MB. Virus-induced immunosup-pression: immune system-mediated destruction of virus-infecteddendritic cells results in generalized immune suppression. J Virol1995;69:1059.
Mimicry and antibody-mediated cell signaling in autoimmu
The mechanisms by which autoantibodies against cardiac mHere, Li Y. et. al. (J Immunol 2006; 177: 8234-40) showderived from experimental autoimmune myocarditis targecAMP-dependent protein kinase A activity. Ab-mediated canti-IgG, or by specific inhibitors of the beta-adrenergic rebetween CM and the beta-AR. Passive transfer of purifieddeposition and apoptosis in the heart, leading to a cardiomnovel findings link anti-CM Ab with the beta-AR and sub
[28] Sevilla N, McGavern DB, Teng C, Kunz S, Oldstone MB. Viraltargeting of hematopoietic progenitors and inhibition of DCmaturation as a dual strategy for immune subversion. J ClinInvest 2004;113:737.
[29] Palella Jr FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J,Satten GA, et al. Decliningmorbidity and mortality among patientswith advanced human immunodeficiency virus infection. HIVOutpatient Study Investigators. N Engl J Med 1998;338:853.
[30] Torriani FJ, Rodriguez-Torres M, Rockstroh JK, Lissen E,Gonzalez-Garcia J, Lazzarin A, et al. Peginterferon Alfa-2a plusribavirin for chronic hepatitis C virus infection in HIV-infectedpatients. N Engl J Med 2004;351:438.
[31] Kamar N, Boulestin A, Selves J, Esposito L, Sandres-Saune K,Stebenet M, et al. Factors accelerating liver fibrosis progressionin renal transplant patients receiving ribavirin monotherapy forchronic hepatitis C. J Med Virol 2005;76:61.
[32] Asadullah K, Sterry W, Volk HD. Interleukin-10 therapy—review of a new approach. Pharmacol Rev 2003;55:241.
[33] Bresson D, Togher L, Rodrigo E, Chen Y, Bluestone JA, HeroldKC, et al. Anti-CD3 and nasal proinsulin combination therapyenhances remission from recent-onset autoimmune diabetes byinducing Tregs. J Clin Invest 2006;116:1371.
[34] Ejrnaes M, von Herrath MG, Christen U. Cure of chronic viralinfection and virus-induced type 1 diabetes by neutralizingantibodies. Clin Dev Immunol 2006;13:67.
[35] Liu YJ. Dendritic cell subsets and lineages, and their functions ininnate and adaptive immunity. Cell 2001;106:259.
[36] Buelens C, Willems F, Delvaux A, Pierard G, Delville JP, Velu T,et al. Interleukin-10 differentially regulates B7-1 (CD80) and B7-2 (CD86) expression on human peripheral blood dendritic cells.Eur J Immunol 1995;25:2668.
[37] Mosmann TR, Coffman RL. TH1 and TH2 cells: differentpatterns of lymphokine secretion lead to different functionalproperties. Annu Rev Immunol 1989;7:145.
[38] Maldonado-Lopez R, De Smedt T, Michel P, Godfroid J, Pajak B,Heirman C, et al. CD8alpha+ and CD8alpha-subclasses ofdendritic cells direct the development of distinct T helper cells invivo. J Exp Med 1999;189:587.
[39] Maldonado-Lopez R, Maliszewski C, Urbain J, Moser M.Cytokines regulate the capacity of CD8alpha(+) and CD8alpha(−) dendritic cells to prime Th1/Th2 cells in vivo. J Immunol2001;167:4345.
[40] Re F, Strominger JL. IL-10 released by concomitant TLR2stimulation blocks the induction of a subset of Th1 cytokines thatare specifically induced by TLR4 or TLR3 in human dendriticcells. J Immunol 2004;12:7548.
ne myocarditis.
yosin (CM) may lead to heart dysfunction is unknown.that autoantibodies to CM in anti-CM sera and mAbsted the heart cell surface and induced Ab-mediatedell signaling of protein kinase A was blocked by CM,ceptor (beta-AR) pathway. mAbs confirmed mimicryAb (IgG) from CM-immunized rats resulted in IgGyopathic heart disease phenotype in recipients. Thesesequent Ab-mediated cell signaling in the heart.