culturally competent care chia-ling mao, ph.d., rn. associate professor school of nursing san jose...
TRANSCRIPT
Culturally Competent Care
Chia-Ling Mao, Ph.D., RN.Associate ProfessorSchool of Nursing
San Jose State University
Objectives
• Define ethnocentrism
• Discuss how the cultural background of the nurse influences the way in which care is delivered.
• Understand the variety of influences that culture and ethnicity have on theinterpretations of the concepts of health and illness.
Culture
• A set of standard for behavior which a group of people attribute to those around them and which they used to orient their behavior
• Meanings, values, and behavioral norms that are learned and transmitted in the dominant society and within its social groups.
• Culture powerfully influences cognitions, feelings, and the “self” concept, as well as the diagnostic process and treatment decision (DSM-IV)

Jewish
• Inter culture difference – Ashkenazi – from Russian, Eastern Europe– Sephardic – Spain, Portugal, the Mediterranean area– Sabra – Born in Israel black Jews from Ethiopia
• value the nuclear family and community• Health seeking beliefs and behaviors are seen as a responsibility to maintain good
health. • Kosher diet – no pork and shellfish; dietary practices• genetic disorders (especially Ashkenazi Jews) – Tay-Sachs disease, Gaucher
Disease and Canavan Disease • Religion
– Torah –Hebrew bible, tree of life,– Sabbath – no work– Rabbi -
• The dying person should not be left alone, after the person dies the body should be wrapped and is put on the floor with the feet facing the door for a short period, a candle may be placed at the head; no creamation
Vienamese
• Nodding is done out of respect and does not necessarily mean agreement or understanding. Direct eye contact is viewed as disrespectful as is a man touching a woman in public or anyone touching another’s head which is considered sacred
• It is inappropriate for women to discuss childbearing, sex, or contraception in the presence of men
• Causes of illness is viewed from Yin & yang; supernatural or spiritual influences, biomedical reasons
• Mental illness is stigmatized – PTSD, depression, anxiety. • SUNDS sudden unexpected nocturnal death syndrome
Race
• A number of broad division of the human species, based on a common geographic origin, certain shared physical characteristics and distinguished from other by a characteristic distribution of gene frequencies.
Ethnicity
• Collectively of people within a larger society defined on the basis of both common origins, shared symbols and standards for behavior
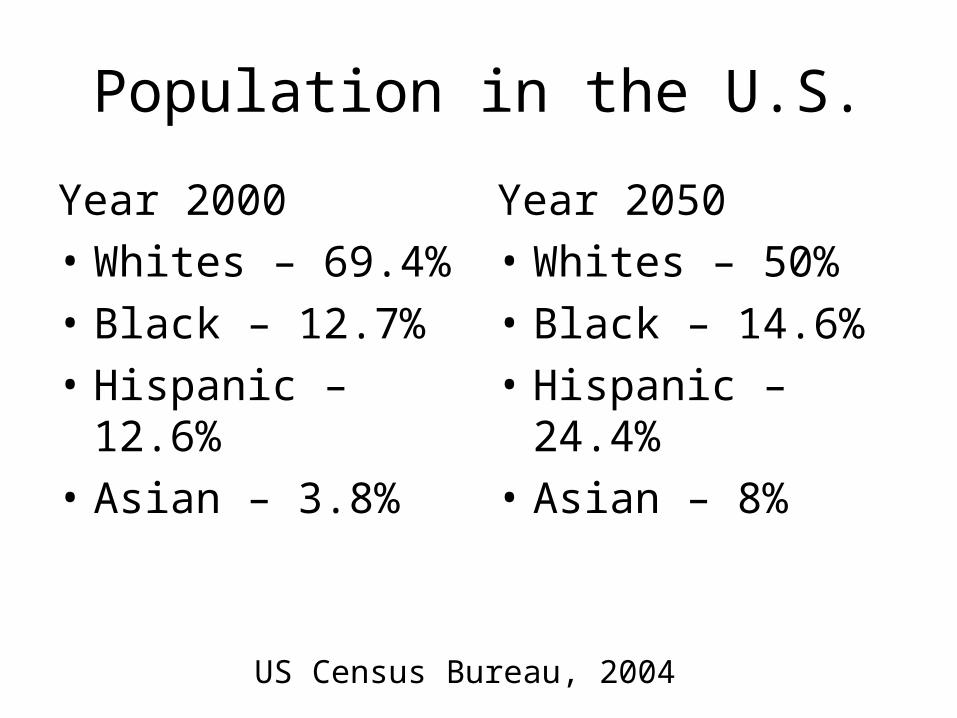
Population in the U.S.
Year 2000
• Whites – 69.4%
• Black – 12.7%
• Hispanic – 12.6%
• Asian – 3.8%
Year 2050
• Whites – 50%
• Black – 14.6%
• Hispanic – 24.4%
• Asian – 8%
US Census Bureau, 2004

US POPULATION• 1998• WHITE 72%• BLACK 12%• HISPANIC 11%• ASIAN 4%• NATIVE AMERICAN
1%
• PROJECTED 2030• WHITE 60%• BLACK 13%• HISPANIC 19%• ASIAN 7%• NATIVE AMERICAN
1%

Sources: US Census Bureau
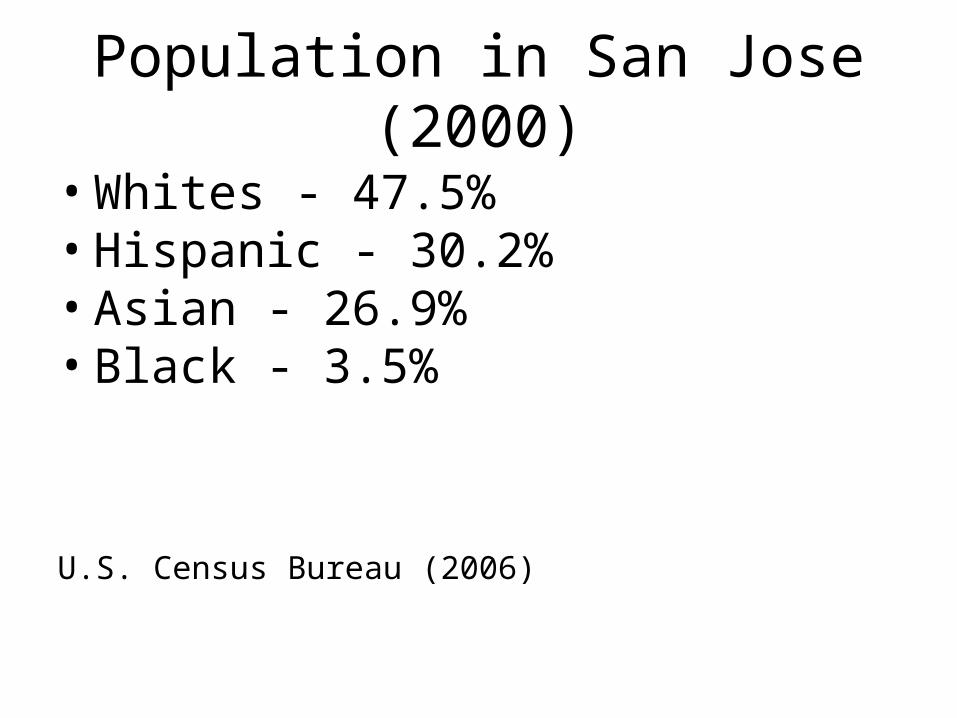
Population in San Jose (2000)
• Whites - 47.5% • Hispanic - 30.2%• Asian - 26.9% • Black - 3.5%
U.S. Census Bureau (2006)

Minorities Receive Lower Quality Health Care Than Whites
• Institute of Medicine, 100 studies reviewed over past 10 yrs.
• Full report www.nap.edu/books/030908265X/html• Minorities less likely to receive sophisticated Txs for
AIDS• More likely to have leg amputations for diabetes• Poorer relationships with MDs

Institute of Medicine:
• Among 13,000 heart patients for every 100 whites who had a procedure to clear the heart arteries, only 74 blacks did
• Of 15,578 urban ER patients blacks were 1.5 times more likely to be denied authorization by managed care providers
• Differences exist even when insurance, income, age, and the severity of the disease are the same for both groups
Health Issues: Cardiovascular
• Cardiovascular- death rate from heart attack 30% higher in African Americans
• Heart attacks declined by 29% in whites vs 21 % for African Americans
• Death rates from stroke were 40% higher in African American adults
HHS Disparities Initiative, 9/24/2002

Health Issues: Diabetes
• Diabetes is 2 times higher in African Americans and 1.9 times higher in Hispanics
• Native Americans have 2.6 times the rate of Diabetes and Pima Natives of Arizona have the highest known prevalence in the world
National Center for Health Statistics, 2002
Disparities: Syphilis/Hepatitis
• Cases of primary and secondary syphilis in 1999 with 30 times greater rate in African Americans
• Asian Americans represent 50% of those infected with Hepatitis B
• Minority teens with higher incidence of Hepatitis B and C
AAP, Committee on Infectious Disease, 2000National Center for HIV, STD, and TB Prevention
Disparities : Tuberculosis
• Of all tuberculosis cases reported in 1991-2001, 80% were in racial and ethnic minorities
• Tuberculosis increased by 51% for Asian Americans and 30% for Hispanics
• Asian Americans and Pacific Islanders, 4% of the US population had 22% of the cases
NCHSTP Division of TB Elimination

Immunizations
• 48% African American and 56% Hispanic receive influenza vaccine compared to 67% Whites
• 31% of African American and 30% of Hispanics receive pneumococcal vaccine compared to 57% Whites
• In 2001 African Americans and Hispanic aged 65 and older were less likely to report having received vaccination
Morbidity and Mortality Weekly, 2002
Disparities: Mental Health
• Native Americans disproportionate rate of depression and substance abuse
• Minorities have less access to mental health services and receive poorer quality services
• Under-represented in mental health research
National Center for Health Statistics, 2002

Other Cultural Domains
• Folk beliefs/religion - can be confused with “religiosity”
• Stereotyping labels - avoid generalizations• Ethnopharmacology - genetic influence, effect,
metabolism• Herbal therapies - interactions with meds• Folk healers & treatment approaches, e.g.., hysteria,
psychosis
Cultural competence &impact on clinical outcomes
• Patients fear of being misunderstood or disrespected; • Providers are not familiar with the prevalence of
conditions among certain minority groups • Providers may fail to take into account differing
responses to medication • Providers may lack knowledge about traditional
remedies, leading to harmful drug interactions • Patients may not adhere to medical advice because they
do not understand or do not trust the provider; • Providers may order more or fewer diagnostic tests for
patients of different cultural backgrounds
Ethnic Disparities in Health Care
• African American women are more likely than European American women to die from breast cancer, despite having a lower incidence of the disease.
• Infant mortality rates are 2.5 times greater for African Americans and 1.5times greater for Native Americans than for European Americans.
• Influenza death rates are higher for African Americans and American Indian/Alaska Natives/Native Alaskans than they are for European Americans.
• Mortality for colorectal cancer is highest for African Americans, followed by Native Alaskans, and then Hawaiians.

Needs for cultural competence
• American nurses experienced a lack of cultural confidence in caring for culturally diverse populations - Coffman, Shellman, & Bernal (2004) and Hagman (2006)
• There were gaps in healthcare providers’ knowledge of other cultures and how to care for them in culturally sensitive ways - Jones, Cason, and Bond (2004)
Other evidences
• Negative racial stereotypes - rate black patients as more likely to abuse drugs and alcohol, less likely to comply with medical advice, and less likely to participate in cardiac rehab than white patients - Van Ryn and Burke (2000)
• Less Dx test - physicians were less likely to recommend catheterization procedures for black female patients than white or black male patients if they experienced the same kind of symptoms. Schulman et al. (1999)
Cultural Competence is a Process
• American Nurses Association published its first guidelines on cultural diversity in nursing curricula in 1986 - understanding the concept of human diversity including cultural and racial variations
• The Board of Registered Nursing of California (2006) has required all nursing schools in California to include cultural diversity and competence into their curricula
Language barriers and disparity
• Utilization of health care services– Fewer doctor visit and less preventive services– More diagnostic test to compensate communication
problems• Satisfaction
– Less satisfied unless with interpreter• Adherence
– Miss the appointment or drop out• Outcomes• Patient education
Health Disparities
• President Clinton (1998) set the goal – reduce health disparities by the year 2010.
• Target areas: (NIH, 2003)– Infant mortality, – Cancer screening and management, – Cardiovascular disease, – Diabetes,– HIV/AIDS, – Immunization

Problems with Health Disparities- with cultural factors
Flaskerud, J. et al (2002) – a review of 79 articles in the past 5 decades:
– Ignorance of certain groups (indigenous peoples)
– Inappropriate lump together • Hispanic members of disparate groups with
their own cultural identity eg., Puerto Ricans, Mexicans, Cubans, Dominicans
• Asian & Pacific islanders
Impact of Cultural Competency
• More successful patient education• Increases in pt’s health care seeking behavior• More appropriate testing and screening• Fewer diagnostic errors.• Avoidance of drug complications• Greater adherence to medical advice• Expanded choices and access to high-quality
clinicians.
Negotiation Process
• Listen: to the client’s perspective• Teach: from your knowledge in language appropriate
for client & family• Compare: similarities & differences, disagree but do
not devalue client’s view• Compromise:
– if client treatment not harmful, promote
– If harmful, explain harm and suggest alternatives
Ethnopharmacology
Ethnopharmacology
• Assumptions– Ethnic culture affects beliefs about health, illness,
medications, interactions with healthcare providers, & comply with prescribed medications as well as response physiologically to medications.

Ethnicity affects drug responses
• Genetic and/or cultural factors make influence on – Drug’s absorption, metabolism, distribution, and
excretion– Drugs’ mechanism of action & effects at the target
site– Patient adherence & education
•

Beliefs about health, illness, medications
• White• Intolerance to pain• High expectation to be
cured or well managed through technology, powerful drugs
• Management of microbes > bolster resistance to them
• Asians • Drug’s safety profile >
its effectiveness• Use lower doses and
fewer reported side effects
• Quick remove of S/S does not equal to a permanent cure

Interaction with healthcare providers
• Language barrier
– Nonverbal communication
• Trusting relationships
– Attire, attitude
• Family involvement
– Decision maker
Adherence with prescribed medications
• Beliefs on the medication
– Discontinue the med when symptoms ease
– Thwart the acceptance of drugs with a delayed onset of action
– Stop taking the med if the diseases is not common in their original country
Culture preferences, rituals, or fears
• Ways of taking the med. ie. Oral, injection,
• Rituals ie. Fasting
• Concerns about addictive effects
Physiologic response to medications
• Genetic polymorphisms
• 3-5% of whites compare to 15-20% of Asians are poor metabolizers of drugs affected by mephenytoin polymorphism ie. Diazepam, imipromine
• Asians and Eskimos need lower doses of anxiolytics than white

Physiologic response to medications (II)
• Jewish & Clozapine – risk for agranulocytosis. 20% as compared with the non-Jewish population of 1%.
• Asians, Indians, and Pakistanis require lower doses of lithium and antipsychotic drugs.
• Asians showed more EPS given same dose of Haldol.
Ethnicity and antihypertensive drugs
• Captopril found less effective in blacks than in whites
• Losartan is less effective in lowering BP in blacks.
• Thiazide diuretics is more effective in blacks.

Nursing implications
• Be knowledgeable about drugs’ varied responses in patients from different ethnic groups.
• Careful monitoring
• “No two people are alike”

Ethical dilemmas
Basic Theories
• Utilitarianism – goal-basedthe greatest happiness for the greatest number
• Deontology – duty based, love-based– Autonomy – human right; self-determination– Beneficence – do good – Justice - fairness– Non-maleficence – do no harm– Veracity – telling the truth– Fidelity - keeping promise

Comparison of 2 major theories
Utilitarian• Consequences
• Who is the majority
• What is happiness
Deontology• Action & motives
• Value
• knowledge

Ethical theory & scientific theory
• Justify human action
• Acceptance of theory
• Action
• Explain phenomenon
• True or false
• Predict, control

Roles of the nurse
• Nurse’s fundamental responsibility- value, concern, goals
• Ethics of caring – empathy, nurturing, commitment, being an advocate
• Participation of the family in decision making – social assessment
Ethical Issues in Nursing
• Quantity vs. quality of life
• Pro-choice vs. pro-life
• Freedom vs. control
• Truth-telling vs. deception
• Distribution of limited resources
• Empirical knowledge vs. personal belief
Methods of moral reasoning
• Deductive – code, creed, …– Inflexibility, value conflict, no motivation
• Inductive – custom, cases, …– Static & preventing progressive social change
• Intuition – combination of subjective, objective, & relativistic aspect
• Dialectical – philosophical aspect, art…
Cultural competence training
• Health care institutions– Interdisciplinary programs
• Nursing service – Orientation – demographic data of the pop, ethical-legal
consequences, appropriate resources– In-service – – Interdisciplinary team
• Nursing education – Undergraduate level – core course– Graduate level – specialty areas
Factors to consider
• Time – past vs. present, interpretation
• Circumstances – setting, knowledge
• Religion – beliefs, creation vs. revolution
• Science – hard data vs. philosophy
• Technology – change of nature
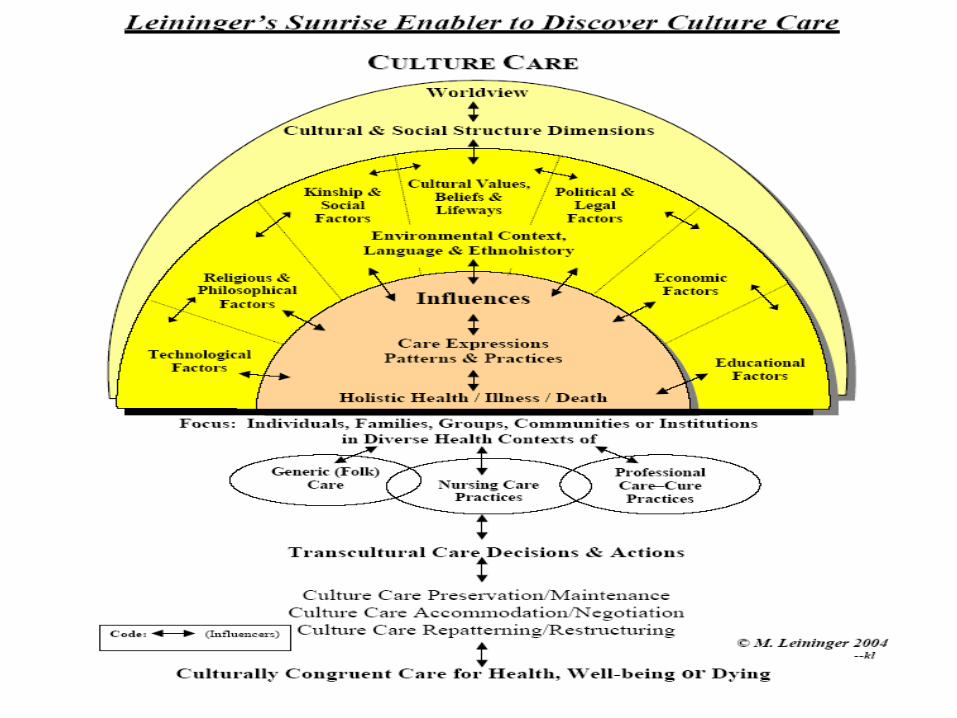
Leininger’s Transcultural Care Theory –
Sunrise Enabler• Developed in the mid-1950s and early 1960s.• To discover the meanings and ways to give
care to people who have different values and lifeways.
• To guide nurses to provide nursing care that fits with those that are being cared for.
• Not only focuses on nurse-client interaction but also includes care for families, groups, communities, cultures and institutions.
Application of Theory
• Care always occurs in a cultural context
• Culture is viewed as framework people use to solve human problems
• Culture is “the lifeways of an individual or a group with reference to values, beliefs, norms, patterns, and practices” (Leininger, 1997, p. 38)
Working with Interpreters
• Qualifications– Bilingual, bicultural, understands English medical
vocabulary
– Comfort in the medical setting, understands significance of the health problem
– Preserves confidentiality
• Multiple Roles:– Translator of Language
– Culture Broker
– Patient Advocate: Convey expectations, concerns

Translation factors
• Language: how are new words created?– Navajo: Penicillin = “the strong white medicine shot you
get for a cold”
• Minimize jargon, e.g., “machine to look at your heart” instead of “EKG”
• Nonverbal communication = 60% of all communication
• Nodding may indicate politeness, not comprehension• Bilingual interviewing takes at least twice as long as
monolingual interviews!
Caretakers’ Responsibilities in Using Translator
• Learn and use a few phrases of greeting and introduction in the patient’s native language. This conveys respect and demonstrates your willingness to learn about their culture.
• Tell the patient that the interpreter will translate everything that is said, so they must stop after every few sentences.
Caretakers’ Responsibilities (II)
• When speaking or listening, watch the patient, not the interpreter. Add your gestures, etc. while the interpreter is translating your message.
• Reinforce verbal interaction with visual aids and materials written in the client’s language.
• Repeat important information more than once.• Always give the reason or purpose for a treatment or
prescription.• Make sure the patient understands by having them explain it
themselves.• Ask the interpreter to repeat exactly what was said.• Personal information may be closely guarded and difficult to
obtain.• Patient often request or bring a specific interpreter to the clinic.
Caretakers’ Responsibilities
• In some cultures it may not be appropriate to suggest making a will for dying patients or patients with terminal illnesses; this is the cultural equivalent of wishing death on a patient.
• Avoid saying “you must... Instead teach patients their options and let them decide, e.g., “some people in this situation would...”
Cultural Diversity and Health Care
It is because we are different that each of us is special.
HEALTHY PEOPLE 2010• Plan to eliminate disparities in health care
provision and in health outcomes by 2010
• Addresses highly preventable conditions
• Requires participation by health care providers to be successful
• Includes issues of cultural and linguistic competence in access to care

Cultural Competency• Defined as a set of congruent practice skills,
behaviors, attitudes and policies that come together in a system, agency or among providers and professionals that enables that system, agency, or professionals to work effectively in cross-cultural situations.
Cross TL, Bazron BJ, et al. Towards a Culturally Competent System of Care. CASSP Technical Assistance Center,
Georgetown University Child Development Center, March 1989
Title VI-Civil Rights Act• “No person in the United States shall, on the
ground of race, color, or national origin, be excluded from participation in, be denied the benefits of, or be subjected to discrimination under any program or activity receiving Federal financial assistance.”

CULTURAL COMPETENCE
• Culturally appropriate, community-driven programs are critical
• Promote cultural awareness • Encourage cultural competence inclusion in medical
school and health careers curriculum• Advocate for the needs of the patients by providing
translators, culturally competent information and instructions in simple language

Impact of Cultural Competency
• More successful patient education• Increases in pt’s health care seeking behavior• More appropriate testing and screening• Fewer diagnostic errors.• Avoidance of drug complications• Greater adherence to medical advice• Expanded choices and access to high-quality
clinicians.
Transcultural Nursing- Leininger, 1997
• Definition- A formal area of study and practice focused on comparative holistic culture care, health and illness patters of people with respect to differences and similarities in their cultural values, beliefs, and lifeways with the goal to provide culturally congruent, competent and compassionate care
Cultural needs
• Equal access to treatment and care• Respect for cultural beliefs and practices
• Leininger, (1995) & Narayanasamy, (2003)– Religious beliefs, taboos, customs– Dietary, personal care needs, daily routines – Dying needs– Communication needs – Cultural safety needs,
Cultural needs (Cont’d)
– Pain – Health practice– Time orientation – Space – Family

Equal access to treatment and care
• Ethnicity
– racial discrimination,
– racial harassment and
– oppression
• Secondary problems
– stress
– psychological trauma

Communication needs
• Barrier – Impede early detection– delay prompt treatment and care
• Forms – Language– Non-verbal communication
• Translation services– Interpreters– Family interpreters
• Health condition – acute illness & crisis
Cultural safety needs
• Engage clients as partners
• Respect & rapport -> self-esteem
• Cultural negotiation & culture compromise

Transcultural Care Practice
• Initiative• Enthusiasm• Commitment of individuals and groups• Strategic planning• Organization & coordination of services• Funding• Education• Recruitment & research

Giger-Davidhizar (2004) - Assessment Model
Culturally Unique
Individual
BiologicalVariations
EnvironmentalControls Time
Social Organization
Space
Communication
Transcultural Nursing : Assessment & Intervention. Mosby

ACCESS Model – Narayanasamy, 2002
• Assessment
• Communication
• Culture negotiation and compromise
• Establishing respect and rapport
• Sensitivity
• Safety
Campinha-Bacote’s Cultural Competence Model
• Cultural awareness
• Cultural skill
• Cultural knowledge
• Cultural encounters
• Cultural desire

Campinha-Bacote, J.(2003)
Cultural awareness
• Becoming appreciative, and sensitive to the values, beliefs, lifeways, practices, and problem solving strategies of clients' culture.
• Exam personal prejudices and bias, one's own cultural background

Cultural knowledge
• seeking and obtaining a sound educational foundation concerning the various world views of different cultures.
• obtaining knowledge regarding specific physical, biological, and physiological variations among ethnic groups
Cultural skill
• ability to collect relevant cultural data regarding the client's health histories and presenting problems as well as accurately performing a culturally specific physical assessment.
Cultural Encounter
• Engaging directly in cross-cultural interactions with clients from culturally diverse backgrounds.
• Being aware of the intra-ethnic variation, which refers to the fact that there is more variation within a cultural group than across cultural groups
Cultural desire
• the motivation of health care providers to "want to" engage in the process of cultural competence
Purnell’s Model
• Macro level – global society, community, family, individual, health
• Cultural domains – overview, communication, family roles, workforce issues, bioculturl ecology, high-risk behaviors, nutrition, pregnancy & childbearing practices, death rituals, spirituality, health care practice/practitioners
• Cultural consciousness• Unknown phenomenon
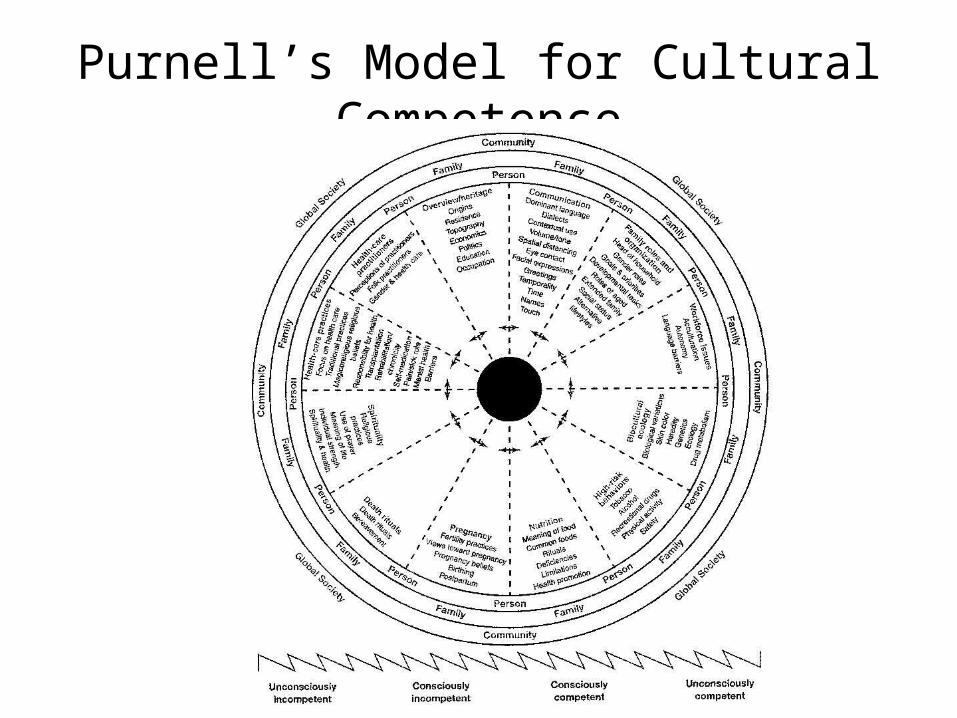
Purnell’s Model for Cultural Competence


Culturally Competent Organization
• US Census Bureau, 2000 – total population = 281,421,906– Latio 35.5 million = 12.1%– African American = 12.9%– Asians = 4.2% (60% is foreign born)– Multiracial = 2.4%
• Ethnic minorities accounts for one fourth of the nation’s population
• In 2020, it will be near to 40%• 10% of RNs in the US are from racial/ethnic
minority background (2000)*
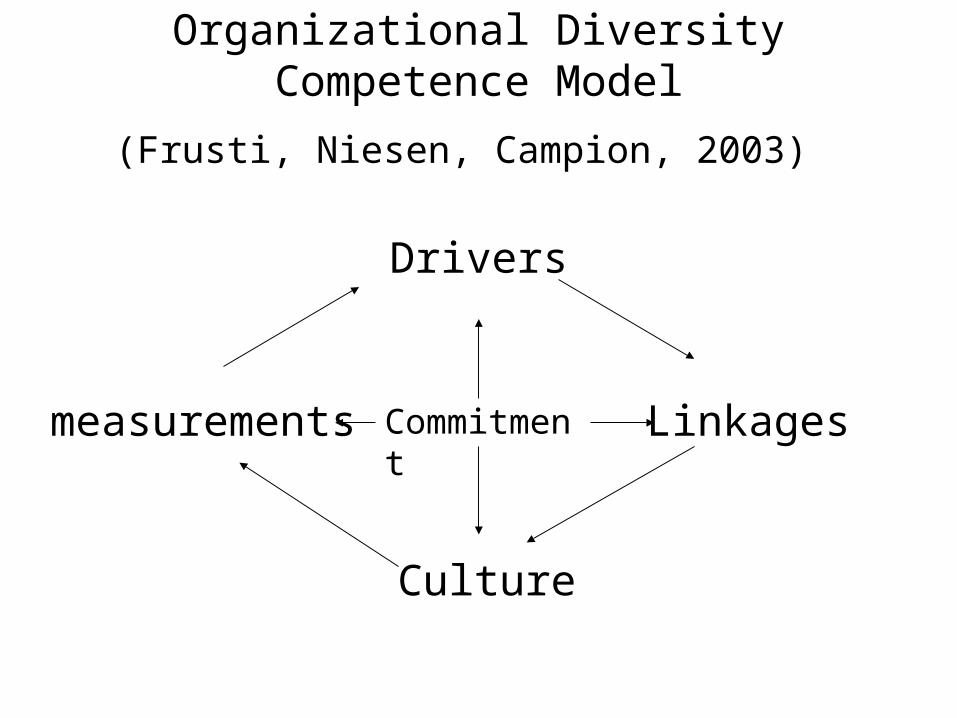
Organizational Diversity Competence Model
(Frusti, Niesen, Campion, 2003)
Commitment
Drivers
measurements Linkages
Culture
Ethic Conflicts
• Genetic counseling
• Family and community involvement in patient care
• Religious ritual ie Sabbath, fasting
• Delay in help seeking

Negotiation Process
• Listen: to the client’s perspective• Teach: from your knowledge in language appropriate
for client & family• Compare: similarities & differences, disagree but do
not devalue client’s view• Compromise:
– if client treatment not harmful, promote
– If harmful, explain harm and suggest alternatives
Conclusion
• Culture is learned & exists in a constant state of change
• Nursing is not “culturally free” but rather is “culturally determined” – avoid ethnocentric
• Much diversity within a cultural group as across cultural groups.
• Culturally competence is a dynamic, fluid, continuous process.
• Goal: discover culturally relevant facts about the client to provide culturally appropriate and competent care
Globalization :Q: How to define globalization?A: Princes Diana’s deathQ: How come?A: An English princess with an Egyptian boy-friend crashes in a French tunnel, in a German car with a Dutch engine, driven by a Belgian who was pissed on Scottish whiskey, followed closely by an Italian paparazzi, on Japanese motorcycles, treated by an American doctor, using Brazilian medicines.And this is sent to you by a Israeli, using Bill Gates’Technology which he stole from the Taiwanese.