cryptic pericentric inversion of chromosome 17 detected by fluorescence in situ hybridization study...
TRANSCRIPT
Letter to the Editor
Cryptic Pericentric Inversion of Chromosome 17Detected by Fluorescence In Situ HybridizationStudy in Familial Miller-Dieker Syndrome
To the Editor:
We read with great interest the article, in this jour-nal, by Masuno et al. [1995] titled ‘‘Miller-Dieker Syn-drome Due To Maternal Cryptic Translocation.’’ Miller-Dieker syndrome (MDS) is characterized by Type I lis-sencephaly due to the arrest of neural migration at10–14 weeks of gestation and specific facial abnormali-ties. A high-resolution banding study led to the eluci-dation of a microdeletion of 17p13.3 band in about halfof the MDS patients [Dobyns, 1991]. Recently, fluores-cence in situ hybridization (FISH) study using the cos-mid probe D17S379 from the MDS critical region of the17p13.3 band was shown to be very useful for detectingsubtle microdeletions or cryptic translocations [Ku-wano et al., 1991; Ledbetter et al., 1992]. We would liketo report another family in which the microdeletionresulted from a paternal cryptic pericentric inversion ofchromosome 17.
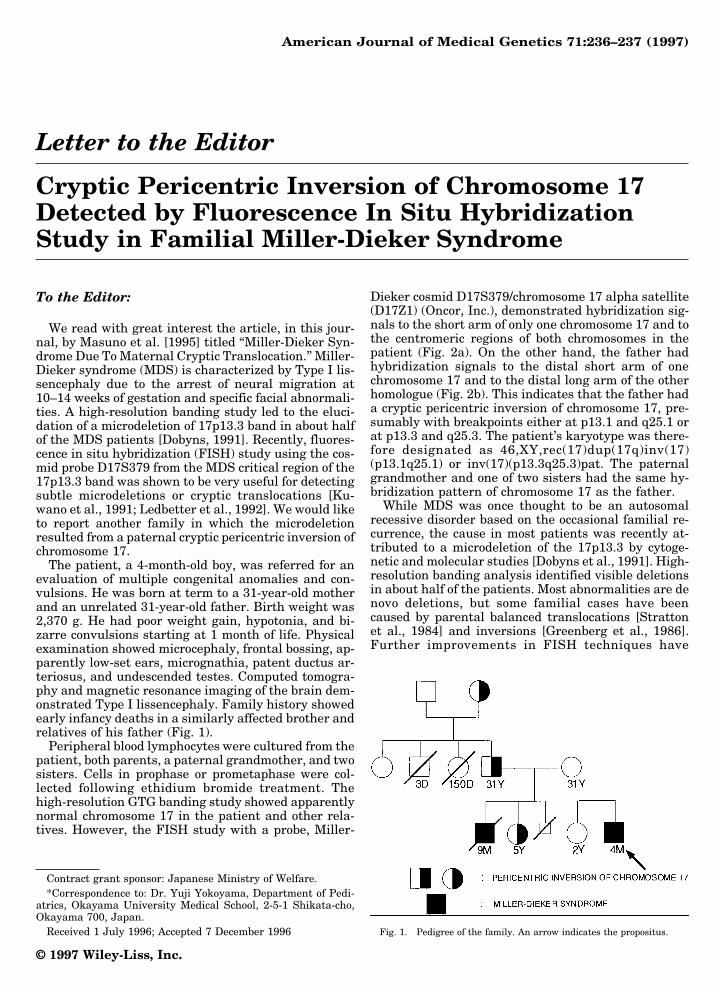
The patient, a 4-month-old boy, was referred for anevaluation of multiple congenital anomalies and con-vulsions. He was born at term to a 31-year-old motherand an unrelated 31-year-old father. Birth weight was2,370 g. He had poor weight gain, hypotonia, and bi-zarre convulsions starting at 1 month of life. Physicalexamination showed microcephaly, frontal bossing, ap-parently low-set ears, micrognathia, patent ductus ar-teriosus, and undescended testes. Computed tomogra-phy and magnetic resonance imaging of the brain dem-onstrated Type I lissencephaly. Family history showedearly infancy deaths in a similarly affected brother andrelatives of his father (Fig. 1).
Peripheral blood lymphocytes were cultured from thepatient, both parents, a paternal grandmother, and twosisters. Cells in prophase or prometaphase were col-lected following ethidium bromide treatment. Thehigh-resolution GTG banding study showed apparentlynormal chromosome 17 in the patient and other rela-tives. However, the FISH study with a probe, Miller-
Dieker cosmid D17S379/chromosome 17 alpha satellite(D17Z1) (Oncor, Inc.), demonstrated hybridization sig-nals to the short arm of only one chromosome 17 and tothe centromeric regions of both chromosomes in thepatient (Fig. 2a). On the other hand, the father hadhybridization signals to the distal short arm of onechromosome 17 and to the distal long arm of the otherhomologue (Fig. 2b). This indicates that the father hada cryptic pericentric inversion of chromosome 17, pre-sumably with breakpoints either at p13.1 and q25.1 orat p13.3 and q25.3. The patient’s karyotype was there-fore designated as 46,XY,rec(17)dup(17q)inv(17)(p13.1q25.1) or inv(17)(p13.3q25.3)pat. The paternalgrandmother and one of two sisters had the same hy-bridization pattern of chromosome 17 as the father.
While MDS was once thought to be an autosomalrecessive disorder based on the occasional familial re-currence, the cause in most patients was recently at-tributed to a microdeletion of the 17p13.3 by cytoge-netic and molecular studies [Dobyns et al., 1991]. High-resolution banding analysis identified visible deletionsin about half of the patients. Most abnormalities are denovo deletions, but some familial cases have beencaused by parental balanced translocations [Strattonet al., 1984] and inversions [Greenberg et al., 1986].Further improvements in FISH techniques have
Contract grant sponsor: Japanese Ministry of Welfare.*Correspondence to: Dr. Yuji Yokoyama, Department of Pedi-
atrics, Okayama University Medical School, 2-5-1 Shikata-cho,Okayama 700, Japan.
Received 1 July 1996; Accepted 7 December 1996 Fig. 1. Pedigree of the family. An arrow indicates the propositus.
American Journal of Medical Genetics 71:236–237 (1997)
© 1997 Wiley-Liss, Inc.

greatly enhanced the speed and accuracy for the iden-tification of submicroscopic chromosome rearrange-ments involving the 17p13.3 band. Cryptic transloca-tions, which were first detected by FISH studies, werereported in several families with multiple MDS af-fected children [Kuwano et al., 1991; Alvarado et al.,1993; Kohler et al., 1994; Masuno et al., 1995]. Kings-ton et al. [1996] reported the first case of cryptic peri-centric inversion, inv(17)(p13.3q25.1), detectable onlyby FISH. The present family seems to be the secondcase of cryptic pericentric inversion of chromosome 17.The inversion was cytogenetically unidentifiable in ourfamily due to the similarity in size and banding patternof the inverted portions of the distal short and long armof chromosome 17.
The father and one sister are at a relatively high riskof having MDS offspring. Prenatal diagnosis using theFISH method is indicated in subsequent pregnancies ofthis family. This report emphasizes the necessity ofFISH study in genetic counseling of every MDS familyeven with a cytogenetically normal 17p13.3 band.
ACKNOWLEDGMENTS
This study was supported in part by a grant from theJapanese Ministry of Welfare to Koji Narahara.
REFERENCES
Alvarado M, Bass HN, Caldwell S, Jamehdor M, Miller AA, Jacob P (1993):Miller-Dieker syndrome: Detection of a cryptic chromosome transloca-tion using in situ hybridization in a family with multiple affected off-spring. Am J Dis Child 147:1291–1294.
Dobyns WB, Curry CJR, Hoyme HE, Turlington L, Ledbetter DH (1991):Clinical and molecular diagnosis of Miller Dieker syndrome. Am J HumGenet 48:584–594.
Greenberg F, Stratton RF, Lockhart LH, Elder FFB, Dobyns WB, Ledbet-ter DH (1986): Familial Miller-Dieker syndrome associated with peri-centric inversion of chromosome 17. Am J Med Genet 23:853–859.
Kingston HM, Ledbetter DH, Tomlin PI, Gaunt KL (1996): Miller-Diekersyndrome resulting from rearrangement of a familial chromosome 17inversion detected by fluorescence in situ hybridisation. J Med Genet33:69–72.
Kohler A, Hain J, Müller U (1994): Familial half cryptic translocationt(9;17). J Med Genet 31:712–714.
Kuwano A, Ledbetter SA, Dobyns WB, Emanuel BS,Ledbetter DH(1991):Detection of deletions and cryptic translocations in Miller-Dieker syn-drome by in situ hybridization. Am J Hum Genet 49:707–714.
Ledbetter SA, Kuwano A, Dobyns WB, Ledbetter DH(1992): Microdeletionsof chromosome 17p13 as a cause of isolated lissencephaly. Am J HumGenet 50:182–189.
Masuno M, Imaizumi K, Nakamura M, Matsui K, Goto A, KurokiY(1995):Miller-Dieker syndrome due to maternal cryptic translocationt(10;17)(q26.3;p13.3). Am J Med Genet 59:441–443.
Stratton RF, Dobyns WB, Airhart SD, Ledbetter DH (1984): New chromo-somal syndrome: Miller-Dieker syndrome and monosomy 17p13. HumGenet 67:193–200.
Yuji Yokoyama*Koji NaraharaMichio TeraokaKiyoko KoyamaYoshiki SeinoDepartment of PediatricsOkayama University Medical SchoolOkayama, Japan
Shinichi YagiTohru KonishiToshio MiyawakiDepartment of PediatricsToyama Medical and Pharmaceutical UniversityToyama, Japan
Fig. 2. a: Submicroscopic deletion at 17p13.3 of the propositus. b: Cryptic pericentric inversion on chromosome 17 of the father.
Letter to the Editor 237