critical thinking and perianesthesia nursing in action
TRANSCRIPT
CLINICAL CLIPS
ACtbtadABoSM“wh
TqwttaltCtwAd
B
Ce
1
Critical Thinking and Perianesthesia Nursingin Action
Ellen E. Sullivan, BSN, RN, CPAN
S A MEMBER of the ASPAN Clinical Practiceommittee, I have the opportunity to respond
o questions from the membership on a regularasis. Most often the questions relate to currentrends in perianesthesia nursing or interpretingparticular standard or resource from the Stan-ards of Perianesthesia Nursing Practice.1
bout a year ago, I received a question fromeverly Caswell, BS, RN, Resource Nurse, Peri-perative Services at St Luke’s Hospital, part ofouthcoast Hospital Group in New Bedford,assachusetts. The question read as follows:
Should PACU RNs assist the anesthesiologistith blocks? They are asked to inject whilee/she holds the catheter.”
his was the second time that I had seen auestion similar to this. It was from someoneorking in a smaller community hospital where
here is no anesthesia residency program andherefore limited physicians that would be avail-ble to assist. I reviewed the Resource pub-ished in our Standards, “The Role of the Regis-ered Nurse in the Management of Analgesia byatheter Techniques (Epidural, Intrathecal, In-
rapleural, or Peripheral Nerve Catheters),”hich was developed by the American Nursesssociation in 1991.1 ASPAN participated in theevelopment of this statement along with other
Ellen E. Sullivan, BSN, RN, CPAN, is a Nurse-in-Charge atrigham and Women’s Hospital, Boston, MA.Address correspondence to Ellen E. Sullivan, BSN, RN,
PAN, 137 Tiffany Rd, Norwell, MA 02061; e-mail address:[email protected].
© 2007 by American Society of PeriAnesthesia Nurses.1089-9472/07/2202-0009$35.00/0
doi:10.1016/j.jopan.2007.01.00428
specialty nursing organizations. Within this doc-ument, it states, “Placement of a catheter orinfusion device, administration of the test doseof medication to determine correct catheter orinfusion device placement, and establishmentof analgesic dosage parameters by written orderfor patients who need acute or chronic painrelief or for the woman during labor should bedone by licensed professionals who are edu-cated in the specialty of anesthesia and physi-cians in other specialties who have beengranted clinical privileges by the institution.”Clearly the statement says that this is the physi-cian’s responsibility and for good reasons. Aphysician should be observing the patient’s re-sponse to the administration of the anestheticand it is critical that the catheter is positionedproperly to verify that it is not in a blood vessel.
At that time, I consulted with some ASPANcolleagues before responding and each re-sponse I received indicated that in their homestates, the RNs were not permitted to adminis-ter the initial dose through a catheter.
When Beverly submitted her inquiry to thecommittee she also provided a phone numberso I was able to contact her directly to discuss.These peripheral neuroaxial blocks were beingplaced by the anesthesiologist to provide re-gional anesthesia. Examples that Beverly de-scribed were interscalene blocks for shouldersurgery or femoral nerve blocks for total kneereplacement surgery. The members of the teamfelt that the patients would benefit from thistype of anesthesia for both the procedure and
postoperative pain relief. However, in the situ-Journal of PeriAnesthesia Nursing, Vol 22, No 2 (April), 2007: pp 128-131

ausi
ABmnvwscoawtoga
IwAitohdts
IooidtMtrb
CLINICAL CLIPS 129
tion as Beverly described it, the staff werensure if they were functioning outside of theircope of practice by actually injecting the med-cine through the catheter.
fter discussion of the actual scenario, botheverly and I felt that a strong case could beade that this was appropriate practice. The
urse was assisting under the guidance, obser-ation, and direction of the anesthesiologistho is holding the catheter in place. In this
cenario, the anesthesiologist is determiningorrect placement and subsequent stabilizationf the catheter, as well as the agent to bedministered and the amount to inject. The RNas facilitating this through the actual aspira-
ion and injecting the medicine under the directbservation and instruction of the anesthesiolo-ist. The patient was continuously monitorednd observed throughout the process.
n thinking this through, it seemed as thoughe certainly understood the intent of both theSPAN Resource and the State Boards of Nurs-
ng; however, we thought that if we presentedhe circumstances to the Massachusetts Boardf Registration in Nursing they would agree thataving the RN deliver the medicine under theirect supervision and observation of the anes-hesia provider would meet the intent of thetandard of practice.
asked Beverly if she was up for the challengef working together to see if approval could bebtained from the Massachusetts Board of Reg-
stration in Nursing to participate in this manneruring the procedure. I made the initial call tohe Board and was directed to Mr Gino Chiasi,SN, RN, for questions regarding nursing prac-
ice. He was very helpful and receptive to ourequest. Mr Chiasi recommended that a letter
e written to the Massachusetts Board of Regis-tration in Nursing describing in detail all aspectsof the procedure. The Board would then reviewthe request and formally respond. Mr Chiasi saidthat the Massachusetts Board of Registration inNursing has legal jurisdiction over nursing prac-tice and nursing education in Massachusetts,whereas other state boards of nursing maintainthe same right to govern what is and what is notnursing practice in their states.
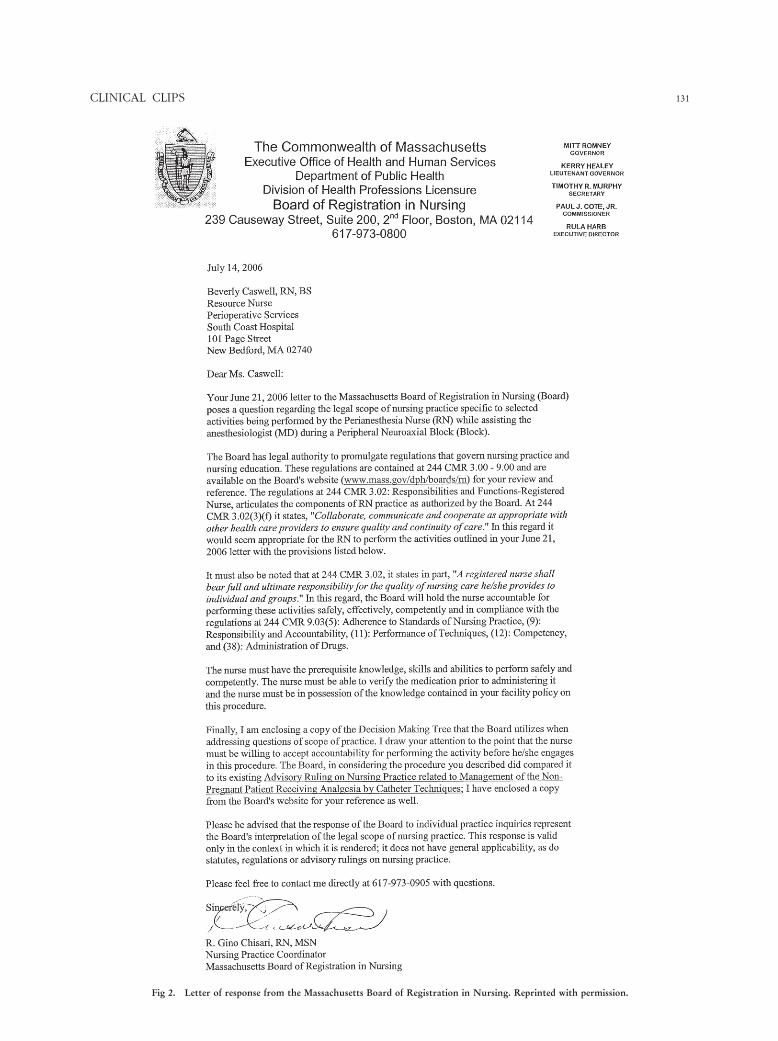
Beverly took it upon herself to compose theletter to the Massachusetts Board of Registrationin Nursing. She also enclosed a copy of theASPAN Resource. The following is a text of theletter that was sent to the Massachusetts Boardof Registration in Nursing followed by the ac-tual response from the Board (Figs 1 and 2).
There may be other perianesthesia RNs aroundthe country who have also faced this issue. Ineach case, you should make sure that you haveverified the practice with your own State Boardof Registration in Nursing as well as assuringthat you have the appropriate institutional pol-icy and procedure to guide your staff.
This is truly an example of one nurse acceptingthe challenge and taking the initiative to make adifference in patient outcomes through the useof critical thinking and a proactive approach.The journey began by researching the availableresources, networking with colleagues, examin-ing the intent of the resource, applying theprinciples of safe patient care, and obtainingadvice and approval from the State Board ofNursing: a true win-win solution for the perian-esthesia nurse, the anesthesia provider, and,ultimately, patient comfort and safety.
Reference
1. American Society of Perianesthesia Nurses. Standards ofPerianesthesia Nursing Practice 2006. Cherry Hill, NJ:
ASPAN; 2006.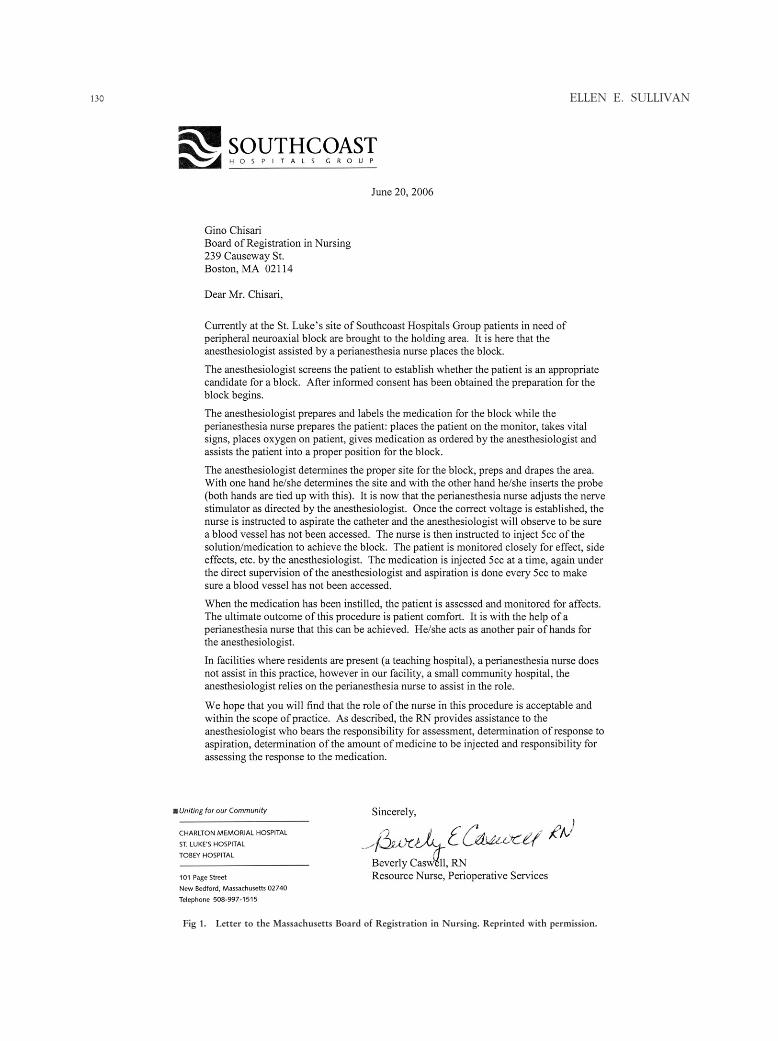
ELLEN E. SULLIVAN130
Fig 1. Letter to the Massachusetts Board of Registration in Nursing. Reprinted with permission.
CLINICAL CLIPS 131
Fig 2. Letter of response from the Massachusetts Board of Registration in Nursing. Reprinted with permission.