critical illness polyneuropathie - dgem.de · pathophysiologie recent studies have indicated a...
TRANSCRIPT
Critical illness Neuropathie –spezifischer Nährstoffmangel?
Michael JöbgesNeurologie
Brandenburg Klinik

Critical illness Polyneuropathie
• Geschichte:
Mertens HG: Die disseminierte Neuropathie nach Koma. Nervenarzt 1961;32:71-79
Olsen CW: Lesions of peripheral nerves developingduring coma. JAMA 1956
Critical illness Polyneuropathie
• Namensgebung:– Roelofs RI, Cerra F, Bielka N, Rosenberg L,
Delaney J. Prolonged respiratory insufficiency due to acute motor neuropathy: a new syndrome? Neurology 33:240, 1983
– Bolton CF, Gilbert JJ, Hahn AF, Sibbald WJ. Polyneuropathy in critically ill patients. J Neurol Neurosurg Psychiatry 47:1223-1231, 1984

Critical illness Polyneuropathie• Zuweisungen in die Brandenburg Klinik:
05
101520253035
2006 2007 2008 2009 2010
Neurologie Phase D
0
20
40
60
80
100
120
2006 2007 2008 2009 2010
Neurologie Phase C
0
20
40
60
80
100
120
2006 2007 2008 2009 2010
Neurologie Phase B
0
50
100
150
200
250
2006 2007 2008 2009 2010
Neurologie Gesamt

Critical illness Polyneuropathie

Critical illness Polyneuropathie
23 of the 48 patients had an ICU length of stay of atleast 7 days and therefore underwent two or more sets ofelectrophysiologic tests.
After 14 days

Symptome
• Schlaffe Parese (meist Bein betont, Gesicht oft ausgespart)
• Muskeleigenreflexe ↓• Distal betonte Hypalgesie, Thermhypästhesie• Nervus phrenicus kann mit betroffen sein
Weaning Zeiten dadurch häufig verlängert• Nervenleitgeschwindigkeiten normal, aber
Amplituden reduziert axonale Polyneuropathie

Critical illness PolyneuropathiePolyneuropathieAkut + nosokomial
Systemische Erkrankung(Vaskulitis, akute Porphyrie)
Abdominaler SchmerzGliederschmerzAteminsuffizienzTachykardie ??????
ArzneimittelInduziertCisplatinVinka-AlkaloideAmiodaronMetronidazolEtc.
spezifischeneurologische ErkrankungGuillain-Barré SyndromAIDS + CMV-Polyradikulo-neuropathie
Akute axonale Polyneuropathie des kritisch Kranken

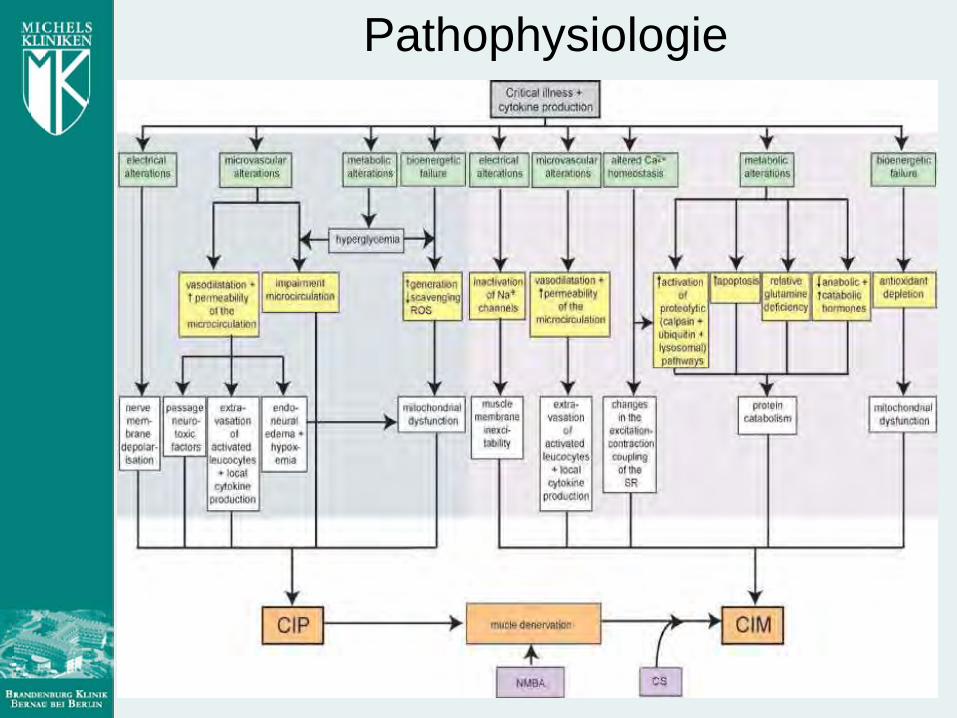
Pathophysiologie

Pathophysiologie

Pathophysiologie

Pathophysiologie
• In studies of the nerve microenvironment in experimental animals, it was shown that hyperglycemia increases endovascular resistance, with reduced nerve blood flow and resulting endoneurial hypoxia.
Low PA, Tuck RR, Takeuchi M. Nerve microenvironment in diabetic neuropathy. In: Dyck PJ, Thomas PK, Asbury AK, Winegrad Al, Porte DJr, eds. Diabetic neuropathy. Philadelphia: WB Saunders Company, 1987: 268-77
Pathophysiologie
Deteriorating peripheral nerve function was also associated with a progressive fall in serum albumin. This may reflect increased micro-vascular permeability and a shift of albumin out of the intravascular compartment. Such a shift could be occurring at the peripheral blood-nerve barrier which is particularly susceptible to the histamine-like substances that are secreted in sepsis. This process would theoretically further increase endoneurial edema, and hence, hypoxia.
Pathophysiologie
Recent studies have indicated a disturbance of the microcirculation of various organs in the sepsis and multiple organ failure syndrome. Shunting of blood from peripheral tissues to more central tissues such as the brain, heart, liver and kidneys may be one mechanism of this disturbance. Since blood vessels supplying peripheral nerve lack autoregulation, suchnerves would be particularly susceptible to peripheral microcirculation disturbances.Low PA, Tuck RR. Effects of changes of blood pressure respiratory acidosis and hypoxia on blood flow in the sciatic nerve of the rat. J Physiol 1984; 347:513-24

Therapie
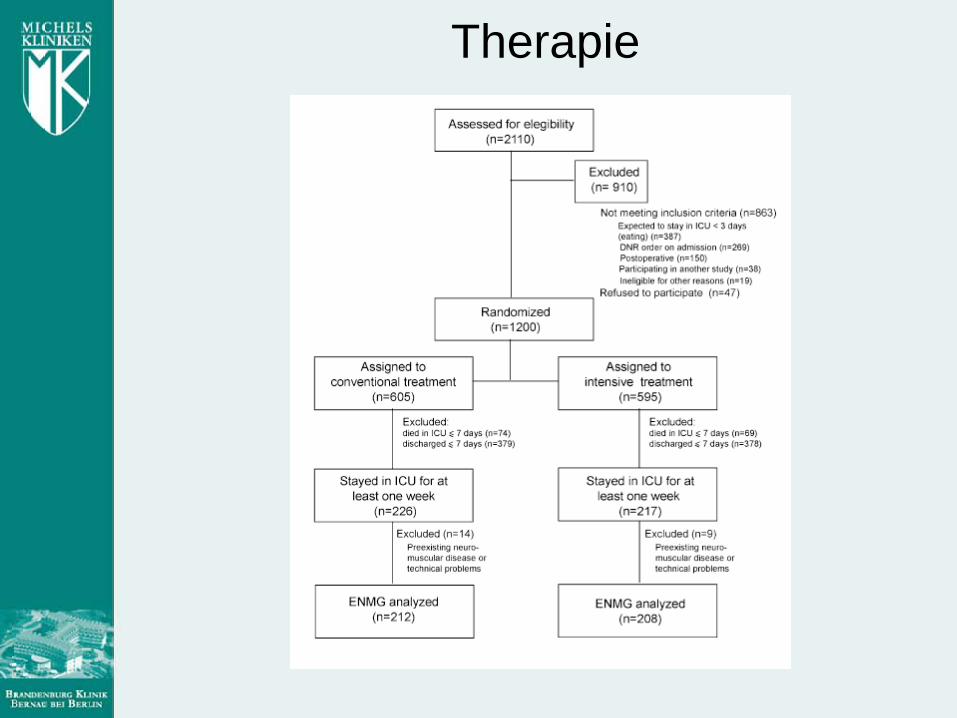
Therapie

TherapieIntensive insulin therapy (IIT) was aimed at blood glucose levels of between 80 and110 mg/dl. The conventional insulin therapy (CIT) approach required insulin only when blood glucose rose above 215 mg/dl and tapering or stopping insulin when blood glucose fell below 180 mg/dl. These levels were achieved with 22 (5–43) units insulin per day in the conventional group and 71 (52–101) units in the intensive group (p 0.0001).

Therapie
days
days
Therapie
Prolonged infusion of neuromuscular blocking agents was an independent riskfactor for the occurrence of at least one positiveENMG (p 0.02; OR, 2.01 [1.10–3.99]). Other independent protective factors were age(p 0.003; OR, 0.98 [0.96–0.99], peryear added) and number of days of treatment with glucocorticoids (p0.02; OR, 0.97 [0.94–0.99], per added day).

Pathophysiologie

Pathophysiologie

Pathophysiologie

Pathophysiologie
Intensive Care Med 1998: 24;87
The lipid component of parenteral and enteral feedings is a mixture of polyunsaturated fatty acids (PUFAs) derived from vegetable oils.…infusion of PUFAs in an oxidation-prone condition like sepsis andmultiple organ failure can have several deleterious consequences that would favor the development of CIP. The oxidative modification of circulating lipids is damaging to the vascular endothelium, and this effect could promote widespread microvascular injury and ischemic axonal injury.Oxidative modification of exogenous lipids can also promote peroxidative injury in lipid-rich structures such as cell membranes and axon sheaths. Finally, infusion of dietary lipids can stimulate the production of inflammatory cytokines, and this effect will magnify the risk of inflammatory-mediated cell injury.
Pathophysiologie
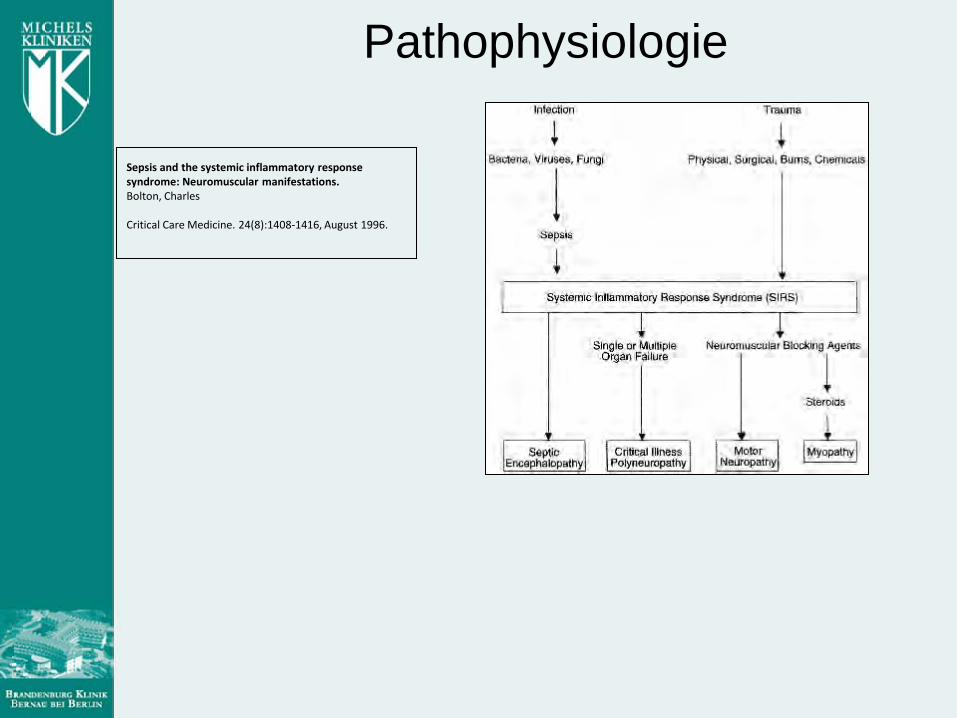
Sepsis and the systemic inflammatory response syndrome: Neuromuscular manifestations.Bolton, Charles
Critical Care Medicine. 24(8):1408-1416, August 1996.

PathophysiologieTheoretical mechanisms of neuromuscular complications of the systemic inflammatory response syndrome (SIRS). 1) Sepsis induces a release of cytokines that cause increased capillary permeability. This effect, and other microvascular mechanisms, induce a critical illness polyneuropathy, with distal axonal degeneration of nerve and denervation atrophy of muscle. 2) Neuromuscular (N-M) blocking agents in the presence of SIRS traverse the hyperpermeable capillary membrane and have a direct toxic effect on nerve, or cause ``functional denervation'' to increase denervation of muscle. 3) Steroids gain access to muscle by this mechanism, and, in the presence of denervation due to 1 and 2, induce a thick filament myopathy and varying degrees of necrosis. Combinations of 1, 2, and 3 may occur in the same patient. Adapted with permission from Bolton [10].
Pathophysiologie
Zusammenfassung I:
• Die critical illness Neuropathie ist eine häufige axonale Neuropathie.
• Periphere motorische und sensible Symptome bestimmen ihr Erscheinungsbild.
• Die Diagnose kann mit Hilfe der klinischen Neurophysiologie gestellt werden.
• Die Folgen für die Patienten sind erheblich

Zusammenfassung II:
• Die Schädigung des peripheren Nervensystems kann sehr rasch nach dem Eintreten einer Sepsis geschehen.
• In der Pathophysiologie sind wahrscheinlich entzündliche und metabolisch / nutritive Aspekte von Bedeutung.
• Insbesondere eine sorgfältige Behandlung des Blutzuckerspiegels kann der Entstehung vorbeugen.
• Zur Zeit ist noch unklar ob ein anderer Nahrungsbestandteil und ggf. welcher eine CIP mit auslöst .

Zusammenfassung III:
• Wichtigste Therapie sind übende Verfahren aus den Bereichen Physio- + Ergotherapie (Rehabilitation!).
Fragen?

Vielen Dankfür Ihre
Aufmerksamkeit