critical care operational policy - east cheshire nhs trust care... · critical care delivery group...
TRANSCRIPT

1 Critical Care Operational Policy Dr Hunter v2 October 2016
Critical Care Operational Policy

2 Critical Care Operational Policy Dr Hunter v2 October 2016
Policy Title:
Critical Care Operational Policy
Executive Summary:
This combined Intensive Care and High Dependency Unit
policy provides guidance to all Trust healthcare professionals
regarding the admission of the Acutely ill Patient into Critical
Care.
Supercedes:
Operational Policy ICU only
Description of
Amendment(s):
Main additions include the medical management of
admissions and discharges
This policy will impact on:
All Clinical Staff
Financial Implications:
None identified
Policy Area:
Trust Wide
Document
Reference:
ECT002774
Version Number:
2
Effective Date:
04.10.2016
Issued By:
Dr Hunter
Review Date:
May 2019
Author:
(Full Job title )
Consultant Intensivist
Consultant Nurse
Impact
Assessment Date:
June 2017
APPROVAL RECORD
Committees / Group Date
Consultation / Approval:
Critical Care Delivery Group
04.10.2016

3 Critical Care Operational Policy Dr Hunter v2 October 2016
Contents
Definition of Critical Care
1 Introduction
2 Philosophy of the Service
3 General Management of the Critical Care Unit
5 Admission Criteria
6 Admission Process
7 Bed Management
7 Clinical Management
8 Discharge Procedure
9 Admission Algorithm
Appendix I: Adult Critical Care Delivery Group terms of reference
Appendix II: Admission of transfers to Critical Care (CCU) from other Hospitals
Appendix III: Standards for Critical Care transfer
Appendix IV: Critical Care transfers from East Cheshire NHS Trust to outside of the agreed
clinical network
Appendix V: Guidelines for return of staff after long distance escort duties and Air transfers.
Appendix VI: Guidance on Critical Care Transfers

4 Critical Care Operational Policy Dr Hunter v2 October 2016
Definition of Critical Care
Critical care areas have, traditionally, been divided into Intensive Care Units (ICUs), where
the highest level of care is given to the sickest patients, and High Dependency Units (HDUs),
where an intermediate level of care is provided for those who are not well enough to go back
on general wards. However, the Department of Health has recommended that the existing
division into high dependency and intensive care beds be replaced by a classification (Table
1) that focuses on the level of care that individual patients need.
Table 1. Levels of Care
Level 0 Patients whose needs can be met
through normal ward care in an acute
hospital.
Level 1 Patients at risk of their condition
deteriorating, or those recently relocated
from higher levels of care, whose needs
can be met on an acute ward with
additional advice and support from the
critical care team.
Level 2 Patients requiring more detailed
observation or intervention including
support for a single failing organ system
or post-operative care and those
‘stepping down’ from higher levels of
care.
Level 3 Patients requiring advanced respiratory
support alone or basic respiratory support
together with support of at least two
organ systems. This level includes all
complex patients requiring support for
multi-organ failure.
Critical Care can be broadly defined as a service for patients who have potentially
recoverable conditions who can benefit from more detailed observation and invasive
treatment than can be provided safely in an ordinary ward or high dependency area. It is
usually reserved for patients with threatened or established organ failure (Level 2 & 3
patients). Because critical care is an expensive and limited resource, the critical care
unit should be reserved for those patients who have a reasonable prospect of
substantial recovery. To avoid inappropriate utilisation of this scarce resource, the decision
to admit a patient to the critical care unit must be made at a senior level.

5 Critical Care Operational Policy Dr Hunter v2 October 2016
Level
1 INTRODUCTION
The Critical Care Unit (CCU) is currently commissioned to: four Level 3 (ICU) and two level 2
(HDU) beds. Each funded bed area is equipped and monitored according to Intensive Care
Society (ICS) Standards (May 1997).
2 PHILOSOPHY OF SERVICE
Critical Care represents the highest level of continuing patient care and treatment, which
involves continuing management and supervision by the multi-disciplinary team.
The philosophy of Macclesfield CCU considers that:
2.1 Critical Care provides a commitment to the needs and requirements of the critically ill
patient, using a holistic approach, to achieve recovery where possible, with the relief of
pain, discomfort and anxiety.
2.2 Each person is an individual with particular needs, and will be treated with respect,
empathy and preservation of dignity. Religious beliefs and cultural traditions will be
respected.
2.3 Communication with the patient and their carers is essential in the provision of intensive
care, and we will inform both patient and carers throughout their stay.
3 GENERAL MANAGEMENT OF THE CRITICAL CARE UNIT
3.1 Strategic management of the CCU will be the overall responsibility of the Head of
Service and Clinical Director of the Urgent Care Business Unit, in co-operation with the
Clinical Lead for Intensive Care who has overall operational/administrative
responsibility for the running of the unit.
3.2 The Intensive Care team will be managed by the Head of Service for urgent care with
the Support of the Unit Manger.
3.3 The Critical Care Nursing team will have an agreed quota of staff and the unit manager
will be responsible for 24-hour rostering.
3.4 Operational policy will be decided by the Critical Care Delivery Group (CCDG) which is
chaired by the Lead Intensivist. The group meets every 3 months.
(see appendix I).
6 Critical Care Operational Policy Dr Hunter v2 October 2016
4 ADMISSION CRITERIA
ALL EMPTY STAFFED/UNSTAFFED BEDS MUST BE ENTERED ONTO
TO THE NHS Directory of Services (DOS) – WHICH MUST BE UPDATED
CONTEMPORANEOUSLY BUT AT LEAST 6 HOURLY
4.1 Criteria for admission;
Patients requiring more detailed observation or intervention than can be provided
on the general ward
Patients with reversible medical conditions who have a reasonable prospect of
substantial recovery
Patients that require or are likely to require advanced support
o Level 3 requiring support of two or more organ systems
o Level 2 requiring single system support and have significant co-morbidity
4.2 Admission of patients under 16 is permitted for stabilisation; however, these patients
would normally be admitted to a specialist paediatric Intensive Care Unit.
4.3 Patients requiring specialist treatment will be transferred to appropriate units.
5 ADMISSION PROCESS See Flowchart for admissions on page 9.
5.1 The source of referrals are expected to be:
Internally - all areas excluding SCBU and paediatrics (see 4.2 above)
Externally: referring hospitals nation-wide, or world-wide. (See: Appendix II)
5.2 Admission is arranged following discussion between the referring team (medical /
surgical etc), the anaesthetic team and the senior nurse in charge of ICU. Discussion
at consultant level is essential for all patients admitted to the critical care unit.
5.3 Access will be achieved via the 2nd On-Call Anaesthetist, who will discuss the case with
the on-call consultant for the CCU.
In the event of there being insufficient capacity to admit the patient, an attempt would
be made by the Nurse in charge to bring in appropriately skilled bank or agency staff,
or rearrange permanent staff’s shifts to accommodate this patient. If, however, the
patient cannot safely be accommodated, then the patient should be transferred to
another hospital with sufficient resources and capacity to manage that patient’s
condition.

7 Critical Care Operational Policy Dr Hunter v2 October 2016
5.4 If a patient requiring admission to CCU necessitates the discharge of another patient
and that patient’s referring team is not available or there is a dispute, the final decision
shall rest with the duty consultant for Critical Care.
5.5 It is the joint responsibility of both teams to undertake transfers in a safe and informed
manner.
5.6 Should it be necessary to transfer the patient then it is a joint responsibility of
anaesthetic and referring team to make alternative arrangements for a critical
care bed for the patient. Each case is unique and roles will vary. They should be
agreed at the outset.
5.6.1 The bed manager should get the latest information about bed availability from
DOS data base and validate the availability of the nearest beds. This
information will be given to both teams.
5.6.2 The anaesthetic and referring team will decide where the most appropriate
bed is and agree who will make the initial approach to the potential recipient
critical care unit.
5.6.3 Both teams must liaise with their respective teams at the receiving trust.
5.6.4 Both teams are responsible to ensure the patient is transferred in a safe
optimal clinical condition.
5.7 The Intensive Care Team will provide clinical support for facilitating a safe transfer.
Transfers will be undertaken according to North West Critical Care Network Transfer
Policy version1.1 August 2012 (available on CMCCN website and local ICU shared
drive). If a transfer is for a non-clinical reason then the transfer must be undertaken in
accordance with the guidelines in Appendix IV.
5.8 In the case of long distance transfers, See Appendix V Guidelines for return of staff
after long distance escort duties and Air transfers.
6 BED MANAGEMENT
6.1 The Bed Manager will be informed of any patient admission, and will co-operate with all
actions to make available an ICU bed.
6.2 Ideally one ICU bed should be available at all times. Priority must be given to the
discharge of patients in the Critical Care Unit who are suitable for ward care.
6.3 The bed manager will contact the Critical Care Unit between 0730 and 0800 to identify,
with the nurse-in-charge, any potential discharges and facilitate achievement of 6.2
above
Ideally no Level 3 patient should be refused admission to the critical care unit if Level
2 patients are occupying beds. However, individual circumstances may dictate that the
Level 2 patient(s) cannot safely be discharged back to the general ward environment.
8 Critical Care Operational Policy Dr Hunter v2 October 2016
7 CLINICAL MANAGEMENT OF PATIENTS WITHIN THE CRITICAL CARE UNIT
7.1 The clinical care of the patient will remain the shared responsibility of the Intensivist
and the Primary consultant of the Patient. Accountability for the critical care element
will remain with the Intensive Care consultant
7.2 Routine management will be prescribed and supervised by the doctor designated to
CCU (who is the 2nd on-call anaesthetist) under the supervision of the duty
consultant Intensivist. When indicated, discussion will be made with the referring
team.
7.3 Daily review from the referring team should take place early in the day (Before
09.30hrs). Any change in the treatment plan should be documented in the medical
notes and the duty anaesthetist informed. Where possible, treatment will be guided by
evidence based protocols.
7.4 Requests for investigations and any new prescriptions must be included in the early
review. All drug prescriptions must be reviewed on a daily basis. The prescribing of
drugs should comply with the hospital guidelines endorsed by the Medical
Management Group.
7.5 Decisions of a specific nature will be taken in consultation with the referring clinician if
able.
7.6 The anaesthetist or referring consultant (or the patient’s carers) may make requests
for an opinion from another discipline.
7.7 The registered nurse on duty will be responsible for the care and management of the
patient assuming the role of the primary or associate nurse.
7.8 The registered senior nurse on duty will be responsible for coordinating a multi-
disciplinary approach to patient care, liaising with other disciplines as necessary.
8 DISCHARGE PROCEDURE
8.1 A patient should be discharged from the CCU when the condition that led to referral
for intensive care has been adequately treated and reversed, or when the multi-
disciplinary team considers that the patient can no longer benefit from the treatment
available.
9 Critical Care Operational Policy Dr Hunter v2 October 2016
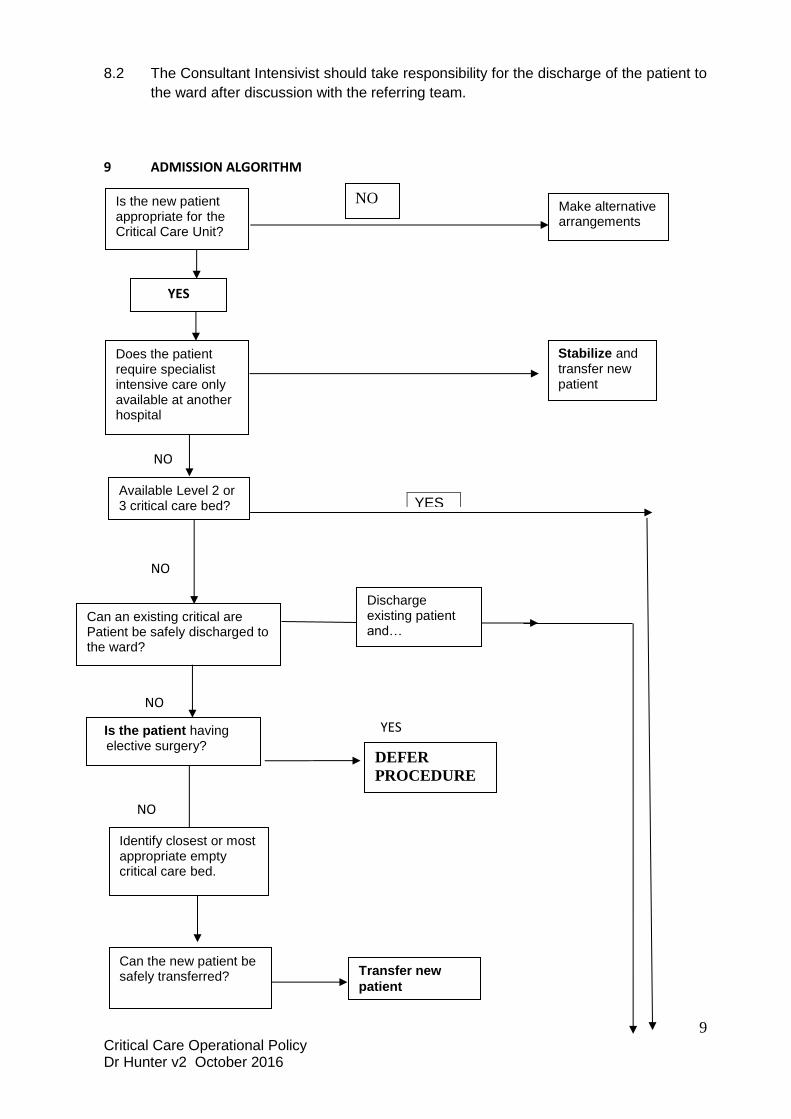
8.2 The Consultant Intensivist should take responsibility for the discharge of the patient to
the ward after discussion with the referring team.
9 ADMISSION ALGORITHM
NO
NO
Y
NO
YES
NO
YES
Is the new patient appropriate for the Critical Care Unit?
Is the patient having elective surgery?
Make alternative arrangements
Stabilize and transfer new patient
DEFER
PROCEDURE
Available Level 2 or 3 critical care bed?
Can an existing critical are Patient be safely discharged to the ward?
Identify closest or most appropriate empty critical care bed.
Can the new patient be safely transferred? Transfer new
patient
Does the patient require specialist intensive care only available at another hospital
Discharge existing patient and…
NO
YES

10 Critical Care Operational Policy Dr Hunter v2 October 2016
NO
Appendix II Critical Care Delivery Group
Title:
Critical Care Delivery Group
Authors Name: Heather Cooper
Scope: Critical Care Only Classification:
Replaces: Terms of Reference 2015
To be read in conjunction with the following documents: Critical Care Operational Policy
Unique Identifier:
Review Date: May 2019 This document is no longer authorised for use after this date
Issue Status: 0.1 Issue No: 1 Issue Date:
Authorised by: Authorisation Date:
Document for Public Display: Yes
After this document is withdrawn from use it must be kept in an archive for 6 years.
Archive: Date added to Archive:
Officer responsible for archive:
Manage the new patient in temporary facility until bed available on critical care
When bed available on critical care
ADMIT NEW PATIENT
11 Critical Care Operational Policy Dr Hunter v2 October 2016
1.0 Definition
1.1 The Trust is required to have a Critical Care Delivery Group following the guidance of the
NHS Comprehensive Critical Care Review 2000.
2.0 Purpose of Meeting 2.1 The purpose of the Committee is to regularly review all aspects of the performance of the
Trust Critical Care Service, and to ensure the effective delivery of a safe, acceptable,
integrated and flexible critical care service which is driven by the needs of patients
2.2 Within its overall purpose and responsibilities and the requirements of Standing Orders
and Standing Financial Instructions, the Committee will have authority to:
2.21 Develop strategies relating to the provision of critical care
2.22 Develop policies relating to the provision of critical care
2.23 Develop plans to ensure the sustainability of the service facilities for the
delivery of critical care services
2.24 Develop and agree organisational arrangements for the delivery of critical care
services
2.25 Agree the clinical governance arrangements for critical care
3.0 Responsibilities
3.1 To ensure that strategies and policies for critical care are reviewed and amended
appropriately
3.2 To review overall performance of the service against best practice and other
standards
3.3 To provide capacity that meets the need of commissioned services
3.4 Provide services consistent with expected national standards
3.3 To identify major issues and risks relating to critical care and to establish processes
to resolve those issues
3.4 To represent the trust and actively participate in the activities of the Mersey and
Cheshire critical care network
12 Critical Care Operational Policy Dr Hunter v2 October 2016
3.5 To present progress, performance and proposals of the Trust Critical Care Service to
the Clinical Management Board
3.6 To identify significant risks to patients and to the Trust arising from the service, and to
report these regularly to the Safety, Quality and Standards Urgent Care Group.
4.0 Reporting Arrangements 4.1 The Group may establish working groups, standing or ad hoc, to resolve issues relating
to critical care and for the effective conduct of its business.
4.2 Will report into the Acute and Integrated Community Care Services Directorate Board 5.0 Frequency of Meetings 5.1 The Committee will meet quarterly in accordance with a schedule agreed by the
Committee. Exceptionally, individual meetings may be cancelled or rearranged either as
agreed by the Committee or the Chair.
5.2 As a minimum, the Committee must meet twice per year 5.3 Additional meetings may be called with the agreement of the Chair to deal with issues of
major importance and/or urgency which would require more time than would be available within a scheduled meeting.
6.0 Membership 6.1 Full Members
Chair – Lead Consultant Anaesthetist/Intensivist
Consultant Anaesthetist/Intensivist
Consultant Surgeon
Consultant Physician
Consultant Nurse, Critical Care
Head of Service Urgent Care
Senior Nurse ICU/HDU
Audit Facilitator /SILS
Practice Development Facilitator
Matron for Urgent care
6.2 Members by invitation
Chief Pharmacist or Link pharmacist
Director of Operations CCG
Representative from C&M Critical Care Network
6.3 Where applicable, deputies will attend for principals who are unable to attend 7.0 Quorate

13 Critical Care Operational Policy Dr Hunter v2 October 2016
7.1 The quorum for meetings of the Committee will be two consultants and one manager of
the service, one of whom must have an intensive care background. Deputies will not
count towards the quorum except when covered by formal acting up arrangements as
defined in the Standing Orders of the Trust
8.0 Chairmanship 8.1 The Committee will be chaired by the Lead Consultant Anaesthetist/Intensivist. In their
absence another Consultant member of the Committee will chair the meeting.
9.0 Conduct of Meetings 9.1 Minutes and papers will be available as covered in the Freedom of Information Act 9.2 The Chair or member of the Committee will present minutes of the Committee to the
Clinical Management Board.
9.3 All meetings will have a documented record.
9.4 Agendas will be prepared and circulated in advance.
9.5 Minutes will be approved by the Chair before submission to the Clinical Management Board or wider circulation and approved by the Committee at the next meeting of the Committee
9.6 Any member may place an item on the agenda and may propose any other urgent
business at a meeting. Other business may be placed on the agenda at the request of
an attendee and with the agreement of the Chair.
9.7 Members will have the right to speak and if necessary vote at meetings of the
Committee. Attendees may speak with the agreement of the Chair and their opinions
sought but will not participate in any formal vote.
9.8 Any interest in the matter under discussion (as defined in Standing Orders) will be
declared. The person declaring an interest will withdraw while the issue is being
discussed.
9.9 In the event of a formal vote, a simple majority will prevail. In the event of a tied vote, the
Chair will have a deciding vote.
9.10 Approval, review and variation of Terms of Reference
The Committee will review the Terms of Reference annually for submission to the Clinical
Management Board who may formally change the Terms of Reference at any time, either at
its own initiation or following a request for variation submitted by the Committee.

14 Critical Care Operational Policy Dr Hunter v2 October 2016
15 Critical Care Operational Policy Dr Hunter v2 October 2016
Appendix II: Admission of transfers to Critical Care (ICU) from other Hospitals
There is currently considerable pressure on critical care beds in the Northwest Region. This
has led to a large number of patients being transferred between Trusts’ Critical care Units.
This policy is to clarify how such admissions to East Cheshire NHS Trust should be
conducted.
1. All enquiries from a hospital seeking admission of a patient to the Critical Care Unit at
East Cheshire should be directed to the anaesthetist registrar on-call.
2. Only the duty Intensivist or on-call consultant anaesthetist will state whether there is
potential to accept outside admissions. This will be after discussion with the senior
nurse for Critical Care regarding staffing levels/skill mix and consideration to any
other potential admissions within the hospital.
3. Once the Anaesthetic / ICU team has agreed that they could take the patient, it
will be made clear to the referring Trust that they must get agreement from the
admitting service to accept the patient. The consultant for the admitting service
must be involved in the decision to admit and accept responsibility for the
patient to Macclesfield DGH. If this role is delegated to a registrar, it is the
registrar alone who has responsibility to inform the admitting consultant.
4. If the admitting consultant is not happy to admit the patient, then the patient cannot
be admitted to the Trust.
5. Once the admitting consultant has agreed to take a patient, the consultant/registrar
should notify the on-call anaesthetic team and the ICU of their decision.

16 Critical Care Operational Policy Dr Hunter v2 October 2016
Appendix III
For Guidance on’ Inter’ and ‘Intra’ transfer of the Acutely Ill Patient, Please see North west
Critical Care Network Transfer Policy.
Appendix IV:
NON CLINICAL TRANSFERS FROM EAST CHESHIRE NHS TRUST TO A TRUST
OUTSIDE OF THE AGREED CLINICAL NETWORK
1. Extract from HSC 2000/17 Modernising Critical care Services:
Where, exceptionally, it is proposed to transfer a critical care patient outside the local clinical
network, transfers must be agreed by the responsible consultant in both NHS trusts and the
respective NHS Trust Chief Executives. The NHS Trust from which the patient is being
transferred will be expected to also inform the host Health Authority Chief Executive of the
transfer.
2. East Cheshire NHS Trust is part of The Mersey and Cheshire Local Critical care
Network
Within the network, Transfer Related Groups have been agreed and are based on
hospitals that are geographically close. If a transfer had to happen at all (the
exception being due to clinical reasons) the transfer should be to the closest
hospital where there is a bed. For East Cheshire NHS Trust these will include:
Mid Cheshire Warrington
Stockport South Manchester
Central Manchester North Staffordshire
Critical care transfers to a trust outside of the Transfer related group, for non-
clinical reasons must only be undertaken in accordance with the guidance below.
3. Transferring patients outside of the agreed Local Critical care Network
Prior to transfer outside of the Transfer related group, the responsible Consultants
(Referring and On-call anaesthetist), together with the Senior Nurse for critical care
and the Bed manager should ensure that:
3.1. all-reasonable steps have been taken to accommodate the patient within the ICU
and HDU at Macclesfield District General Hospital
3.2. And, failing that, all-reasonable steps have been taken to accommodate the patient
within the local Transfer related group.
3.3. The Intensive Care Bed information service CMS for up to date information about
critical care bed availability.
4. Notification of the receiving Trusts’ Chief Executive
4.1. If a patient needs to be transferred out of the Transfer related group, the referring
consultant (i.e. Surgeon/Physician) must agree the transfer with the receiving
consultant.
4.2. Following this agreement,

17 Critical Care Operational Policy Dr Hunter v2 October 2016
4.2.1. During office hours, the Bed Manager will notify the Trust Chief Executive or
designated deputy of the transfer who should agree the transfer with the with
Chief executive of the receiving Trust
4.2.2. Out of office hours, the Bed manager/Night Sister will notify the on-call
manager who will notify the Chief Executive or designated deputy
Effective Date: January 9th 2001 as indicated in the letter date January 9
th 2001 from Andrew Clough, Critical Care Co-ordinator,
NHSE.

18 Critical Care Operational Policy Dr Hunter v2 October 2016
Appendix V: Guidelines for return of staff after long distance escort duties and Air transfers.
1 This document sets out guidance for the rapid and reasonable return of staff, that
have been escorting critically ill patients over long distances, back to their base
hospital when either:
The returning ambulance is unable to complete the return journey
The transfer is by air, and return flight is not possible
2 Generally, the escorting staff will be returned by ambulance. In the case of long
distance transfers, this may not be possible due to restrictions placed on the
ambulance service relating to maximum driving times.
3 For air transfers, where the transferring vehicle returns staff to a landing site in the
Macclesfield area, then EAST CHESHIRE NHS Trust should arrange transport via the
normal routes (Order taxi via Switchboard).
4 No definition is placed on long distance. Each case should be considered separately.
The key factor is the ability of the transferring vehicle to return the escorting staff.
5 When transfer by air or long distance by land is arranged, the return of the escorting
staff must be planned. In many cases, air transfers happen during the limited daylight
hours of winter and return by air is not possible. The escorting staff will normally have
the following equipment with them:
Transfer bag (mobile phones are available from switchboard)
Portable monitor
Portable ventilator and D size oxygen cylinder
A number of infusion devices, pressure bags and monitoring cables.
A moderate quantity of drugs, syringes and needles including Controlled Drugs
6 If return travel is not possible using the transferring vehicle, then return by taxi is the
only practicable method. Public transport should not be used due the risk of personal
injury related to the volume of equipment and drugs being transported.
7 Return travel arrangements should be organised by the bed-manager at East
CHESHIRE NHS Trust while the transfer is being arranged. The switchboard at the
recipient hospital should be asked to arrange a return taxi through their contracted
company. This should ensure some security and reliability to the return journey. The
recipient trust will then invoice East CHESHIRE NHS Trust quoting the reference “ICU
TRANSFER TAXI”. The Trust organising the transfer should be asked to send the
invoice to:
Transport Manager
Operation Services Directorate
East CHESHIRE NHS TRUST
Victoria Road
Macclesfield, CHESHIRE, SK10 3BL TEL: 01625 421000
Claims for associated costs (food etc) should be submitted via the normal routes.
copies of this policy should be held in: On-call managers file, bed managers file, ICU + A+E
(copy in transfer bags), Anaesthetic Department.

19 Critical Care Operational Policy Dr Hunter v2 October 2016
REFERENCES
Standards for Intensive Care Units. Intensive Care Society. 1997, 2007.
Comprehensive Critical Care: A review of adult critical care services. DoH. 2000.
East Cheshire NHS Transfer of the Acutely ill Patient (see Intranet)
Department of Health (1996) Guidelines on admission to and discharge from
intensive care and high dependency units. DoH, London
Intensive Care Society (1997) Guidelines for transport of the critically ill adult. British
Medical Association London
20 Critical Care Operational Policy Dr Hunter v2 October 2016
Equality Analysis (Impact assessment) Please START this assessment BEFORE writing your policy, procedure, proposal, strategy or service
so that you can identify any adverse impacts and include action to mitigate these in your finished
policy, procedure, proposal, strategy or service. Use it to help you develop fair and equal services.
Eg. If there is an impact on Deaf people, then include in the policy how Deaf people will have equal
access.
1. What is being assessed?
Critical Care Operational Policy
Details of person responsible for completing the assessment:
Justine Somerville
Unit Manager/Senior Sister
Intensive Care/High Dependency Unit
State main purpose or aim of the policy, procedure, proposal, strategy or service:
(usually the first paragraph of what you are writing. Also include details of legislation, guidance,
regulations etc which have shaped or informed the document)
This combined Intensive Care and High Dependency Unit policy provides guidance to all Trust healthcare
professionals regarding the admission of the Acutely ill Patient into Critical Care.
2. Consideration of Data and Research To carry out the equality analysis you will need to consider information about the people who use the
service and the staff that provide it. Think about the information below – how does this apply to your
policy, procedure, proposal, strategy or service
2.1 Give details of RELEVANT information available that gives you an understanding of who
will be affected by this document
Cheshire East (CE) covers East Cheshire CCG. Cheshire West & Chester (CWAC) covers Vale Royal.
In 2011, 370,100 people resided in CE and 329,608 people resided in CWAC.
Age: East Cheshire and South Cheshire CCG’s serve a predominantly older population than the national
average, with 19.3% aged over 65 (71,400 people) and 2.6% aged over 85 (9,700 people).
Vale Royal CCGs registered population in general has a younger age profile compared to the CWAC
average, with 14% aged over 65 (14,561 people) and 2% aged over 85 (2,111 people).
Since the 2001 census the number of over 65s has increased by 26% compared with 20% nationally.
The number of over 85s has increased by 35% compared with 24% nationally.
Race:
In 2011, 93.6% of CE residents, and 94.7% of CWAC residents were White British
5.1% of CE residents, and 4.9% of CWAC residents were born outside the UK – Poland and India
being the most common
3% of CE households have members for whom English is not the main language (11,103 people)
and 1.2% of CWAC households have no people for whom English is their main language.
Gypsies & travellers – estimated 18,600 in England in 2011.
Gender: In 2011, c. 49% of the population in both CE and CWAC were male and 51% female. For
CE, the assumption from national figures is that 20 per 100,000 are likely to be transgender and for
CWAC 1,500 transgender people will be living in the CWAC area.
21 Critical Care Operational Policy Dr Hunter v2 October 2016
Disability:
In 2011, 7.9% of the population in CE and 8.7% in CWAC had a long term health problem or
disability
In CE, there are c.4500 people aged 65+ with dementia, and c.1430 aged 65+ with dementia in
CWAC. 1 in 20 people over 65 has a form of dementia
Over 10 million (c. 1 in 6) people in the UK have a degree of hearing impairment or deafness.
C. 2 million people in the UK have visual impairment, of these around 365,000 are registered as
blind or partially sighted.
In CE, it is estimated that around 7000 people have learning disabilities and 6500 people in
CWAC.
Mental health – 1 in 4 will have mental health problems at some time in their lives.
Sexual Orientation:
CE - In 2011, the lesbian, gay, bisexual and transgender (LGBT) population in CE was
estimated at18,700, based on assumptions that 5-7% of the population are likely to be lesbian,
gay or bisexual and 20 per 100,000 are likely to be transgender (The Lesbian & Gay
Foundation).
CWAC - In 2011, the LGBT population in CWAC is unknown, but in 2010 there were c.
20,000 LGB people in the area and as many as 1,500 transgender people residing in CWAC.
Religion/Belief:
The proportion of CE people classing themselves as Christian has fallen from 80.3% in 2001 to 68.9%
In 2011 and in CWAC a similar picture from 80.7% to 70.1%, the proportion saying they had no
religion doubled in both areas from around 11%-22%.
Christian: 68.9% of Cheshire East and 70.1% of Cheshire West & Chester
Sikh: 0.07% of Cheshire East and 0.1% of Cheshire West & Chester
Buddhist: 0.24% of Cheshire East and 0.2% of Cheshire West & Chester
Hindu: 0.36% of Cheshire East and 0.2% of Cheshire West & Chester
Jewish: 0.16% of Cheshire East and 0.1% of Cheshire West & Chester
Muslim: 0.66% of Cheshire East and 0.5% of Cheshire West & Chester
Other: 0.29% of Cheshire East and 0.3% of Cheshire West & Chester
None: 22.69%of Cheshire East and 22.0% of Cheshire West & Chester
Not stated: 6.66% of Cheshire East and 6.5% of Cheshire West & Chester
Carers: In 2011, nearly 11% (40,000) of the population in CE are unpaid carers and just over 11%
(37,000) of the population in CWAC.
2.2 Evidence of complaints on grounds of discrimination: (Are there any complaints or concerns
raised either from patients or staff (grievance) relating to the policy, procedure, proposal, strategy
or service or its effects on different groups?)
There are no complaints relating to this policy
2.3 Does the information gathered from 2.1 – 2.3 indicate any negative impact as a result of this
document?
No
3. Assessment of Impact
Now that you have looked at the purpose, etc. of the policy, procedure, proposal, strategy or service
(part 1) and looked at the data and research you have (part 2), this section asks you to assess the
impact of the policy, procedure, proposal, strategy or service on each of the strands listed below.

22 Critical Care Operational Policy Dr Hunter v2 October 2016
RACE:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect, racial groups differently? Yes No √
Explain your response: If relatives/carers/partner’s first language is not English, than staff will follow the trust interpretation
policy.
__________________________________________________________________________________
__
GENDER (INCLUDING TRANSGENDER):
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect, different gender groups differently? Yes √ No
Explain your response: In 2.2 the policy states that people will be treated with respect and empathy and dignity will be
preserved. As the unit is a specialized area, there may be both men and women treated in the unit.
Staff will try and locate separate sexes apart from each other where possible and use curtains to
promote dignity. For a transgender patient, there may be a number of issues to consider in order to
preserve a person’s dignity when in ICU – please refer to trust Transgender Policy for support.
DISABILITY
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect, disabled people differently? Yes No √
Explain your response:
If relatives/carers/partner has a sensory disability then information can be communicated in the most
appropriate format and staff will follow the trust interpretation policy where appropriate.
__________________________________________________________________________________
___
AGE:
From the evidence available does the policy, procedure, proposal, strategy or service, affect, or
have the potential to affect, age groups differently? Yes No √
Explain your response:
This policy relates to adult Critical Care. Young children and babies are discouraged from visiting due
to risk of infection and the fact that equipment in the unit can appear overwhelming and frightening.
__________________________________________________________________________________
LESBIAN, GAY, BISEXUAL:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect, lesbian, gay or bisexual groups differently? Yes No √
Explain your response: There should be no adverse impacts. Staff have access to equality and
diversity training.
-
__________________________________________________________________________________
_
RELIGION/BELIEF:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect, religious belief groups differently? Yes No √
Explain your response:
This policy will respect religious and cultural beliefs, promoting privacy and facilitating access to
prayer and spiritual support.
__________________________________________________________________________________
___
23 Critical Care Operational Policy Dr Hunter v2 October 2016
CARERS:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect, carers differently? Yes No √
Explain your response: Carers will be supported to be involved in the patient’s care where
appropriate and this will be reviewed regularly. At critical times such as end of life carers can stay
overnight. For patients with learning disabilities, carers are allowed to stay and support the patient, but
are advised to take breaks and staff work to ensure that both patient and carers get some rest. There is
a carer involvement care plan which should be implemented.
__________________________________________________________________________________
___
OTHER: EG Pregnant women, people in civil partnerships, human rights issues.
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have
the potential to affect any other groups differently? Yes No √
Explain your response: No other impacts identified.
-
__________________________________________________________________________________
___
4. Safeguarding Assessment - CHILDREN a. Is there a direct or indirect impact upon children? Yes No √
b. If yes please describe the nature and level of the impact (consideration to be given to all children;
children in a specific group or area, or individual children. As well as consideration of impact now or
in the future; competing / conflicting impact between different groups of children and young people:
c. If no please describe why there is considered to be no impact / significant impact on children All staff
receive safeguarding training. Young children and babies are discouraged from visiting due to risk of
infection and the fact that equipment in the unit can appear overwhelming and frightening.
5. Relevant consultation Having identified key groups, how have you consulted with them to find out their views and that the
made sure that the policy, procedure, proposal, strategy or service will affect them in the way that
you intend? Have you spoken to staff groups, charities, national organisations etc?
N/A
6. Date completed: 4th
April 2017 Review Date: October 2018
7. Any actions identified: Have you identified any work which you will need to do in the
future to ensure that the document has no adverse impact? no
Action Lead Date to be Achieved
Check that all staff are aware of the interpretation
policy and how to access an interpreter
JS July 2017
Check all staff are aware of carer involvement care
plan and are implementing same.
JS July 2017
8. Approval – At this point, you should forward the template to the Trust Equality and
Diversity Lead [email protected]
Approved by Trust Equality and Diversity Lead: Date: 20.6.17