creating a sustainable program - american college of ...€¢ work environment • program delivery...
TRANSCRIPT

4/3/2013
1
Improving the Health of Health Care Workers: A Comprehensive, Integrated Health Protection and Health
Promotion Program for the DH Family
1
Robert K. McLellan, MD, MPH, FACOEMMedical Director
Chief, Section of Occupational and Environmental MedicineAssociate Professor of Medicine, Community and Family Medicine, and The Dartmouth InstituteGeisel School of Medicine at Dartmouth
• Building the business case
• Aligning with corporate strategy
Creating a Sustainable Program
• Program planning
• Implementing
• Evaluating
McLellan.SafeWell Practice Guidelines at http://centerforworkhealth.sph.harvard.edu/images/stories/SafeWellPracticeGuidelines&ExecSumm_Sept2012.pdf
• Academic Medical Center
– 8000 employees
– 10,000 family members
Dartmouth‐Hitchcock
– 1000 physicians
– Multiple sites
4/3/2013
2
• Problem– Unsustainable, double digit
annual increases in health care costs
– Workforce sicker than benchmark organizations
Baseline Status
benchmark organizations– Patient complaints about
unhealthy appearing HCWs– Meager, siloed employee
health resources– We are a leading health care
organization. This is embarrassing. Can’t we do better!
• Investing in employee health makes good business sense
• Robust evidence base that
Show the Evidence to Leadership
• Robust evidence base that employer health and wellness initiatives can improve employee health
• Patient safety depends on healthy employees
Pilot a Rigorous Program
Work Environment Interventions to Optimize Health and Productivity of Workers with Cardiovascular Risk Factors
Supported by the CDC Health Protection Research Initiative: 5 R01 DP000105‐03
with Cardiovascular Risk Factors

4/3/2013
3
• Create a sustainable“culture of health” that would support population health
My Job
improvement over the long haul
• Not
• Comprehensive
– (a suite of resources)
• Integrated
– (leverage synergy)
• Health promotion
– (reduce lifestyle risks, manage chronic disease)
• A supportive work
Benchmarked Requirements for Success
( g y gy)
• Health protection
– Engaging employees founded on superior occupational health and safety
environment
• Measure and report
• Embedded in corporate business plan
http://www.cdc.gov/niosh/TWH/essentials.html
• Live well/work well must become integral to Dartmouth‐Hitchcock’s corporate
Our Strategy
culture …
4/3/2013
4
Achieve the healthiest population possible, leading the transformation of health care in our region and
Dartmouth-Hitchcock Vision
Dartmouth-Hitchcock Mission
We advance health through research, education, clinical practice and community
D‐H Vision and Mission
10
gsetting the standard for our nation.
Adopted by the D-H Board of Trustees on April 27th, 2007
p ypartnerships, providing each person the best care, in the right place, at the right time, every time
Strategic Initiatives to Achieve D-H Mission and Vision
Strategic Initiatives
Leaders in Quality
Education and Research Strength
Mission, Vision, Goals
11
5 Concurrent Strategic Planning Task Forces
Southern NH Growth
Tertiary Quaternary Care
Leadership
Strength
Operational Imperatives
Population Health
Management
Information Technology FinanceService & Access
People
2. Promote Healthiest Population Possible
MEASURED ADVANCEMENT IN POPULATION HEALTH
A Strategic Priority
Improve the Health Status of the Workforce
Launch Initiatives Focused on Employee Education, Promotion, and Early
Intervention
Extend Employee Health Status Improvement Model to Regional Employers &
Communities
If we can’t do it for ourselves, how can we do it for others ….f

4/3/2013
5
Live Well/ Work Well …A Strategic Priority
Vision: Achieve the Healthiest D‐H Workforce
Possible
Mission: Create a Culture of Health, Safety, and Well‐being
Scope: Employees and their families throughout the D‐H system
• Not a program
• …at the core of our institutional vision and mission
• …the way we do things at Dartmouth‐Hitchcock
• Aligned with institutional goals and embedded as a Key Tactic in the DH Operational plan
• Foundation for building an employer service line
• Tied to academic mission of investigating the science of health care delivery
• Both occupational andpersonal health are profoundly influenced by the work
Rationale for Integration of Health Protection with Health Promotion
environment and employer resources
• Personal and occupational risk factors interact

4/3/2013
6
• 85% of WC costs attributed to workers with medium or high health risk status reported on HRA
• Participation in an HRA reduced WC costs by
WC Claim Costs and Health Risk
p y$1238 per person
Musich JOEM 2001
• High risk participants 3 times more likely to file a WC claim than low risk
Kuhnen JOEM 2009
• Obesity
• Sleep deprivation
• Smoking
D d l h l b
Health Risks Associated with Increased Incidence and Severity of WR Injuries
• Drug and alcohol abuse
• Impairment from certain prescribed medicines
• Poorly controlled diabetes
• Depression
• Workplace conflict with supervisors or coworkers
Ostbye 2007; Bedno 2003; Trogdon 2008; Swaen 2006; Kim 2009; Beseler 2010
• Good physical fitness
• Absence of chronic illness
• Good mental health
Factors Associated With Low WR Injury Rates
Good mental health
Ostbye 2007, Maniscalco 1999, Musich 2001.

4/3/2013
7
Interaction of Personal and Occupational Risk Factors
Schulte et al. AJPH 2012
Schulte et al. AJPH 2012
Occupational Hazards Are Associated with Lifestyle

4/3/2013
8
Punnett 2010
Punnett 2010
Punnett 2010

4/3/2013
9
Workplace Stressors Shown to Affect Health Behaviors and Health Conditions
• High job demands– Rapid work pace
– Few rest break opportunities
L d i i l i d
• Lifestyle– Tobacco use– Lack of exercise– Alcohol use– Diet
d• Low decision latitude– Over work schedule
• Monotonous work
• Perceived job stress – Low job satisfaction
– Job insecurity
• Shift Work
– Lipids– Insufficient sleep
• Cardiovascular disease• Mental health disorders
• Cancer
Punett 2007
• Can be a source of – Occupational hazards
– Constraints on disease self‐management
– Barriers to healthy
The Work Environment
lifestyles
• Or … – Occupational health
protection
– Social support and motivation
– Health promotion
• A healthier workforce will be a safer workforce
• A safer workforce will
Foundational Premise
be a healthier workforce

4/3/2013
10
• Improving individual and population health of workers and their dependents will be facilitated by
– Integration of occupational health protection with
Foundational Premise
– Integration of occupational health protection with health promotion
– Synergy of community based with employer based services
Special Populations/Needs
DH Healthy
Workforce & Families
A Healthy Place to Work
IH & Safety
Occ Medicine
Community Based Employer Based
Retirees
Employees
Occupational Health and Work Ability
Dependents
Behavioral
Physical
Wellness
Information Technology
Benefits and Human Resource Policies
Measurement
Primary Care
Specialty Care
CommunityResources
Health coaching
Care Coordination
EAP/Behavioral Health
Workability
EE Medical Home
Health Plan & 3rd Party Vendors
Work Environment & Community Environment
• Physical environment
• Nutritional environment
• HR policies benefit design
Building A Healthy Work and Community Environment
HR policies, benefit design, work organization
• Social environment
• Information Environment
• Community Environment

4/3/2013
11
• Participation highly correlated with attributes of workgroup culture
Work Culture Affects Participation in Employer Sponsored Health Promotion
– Job satisfaction
– Perception of job safety
– Local leadership cares about me
– Able to express grievance
McLellan JOEM 2009
ChronicDisease
AcuteSelf‐limited Conditions
ModerateRisk
LowRisk
CatastrophicIllness
HighRisk
LowRisk
Design Program to Address a Spectrum of Needs
32
Maintain Health Manage DiseaseImprove LifestylePrevention/Early
Detection/ Self‐Care
Risk Reduction/ Self‐Care
Acute and Chronic Condition Management
– Occupational medicine
• Safety and Industrial hygiene
• Health coaching
• Behavioral health team
– Employee assistance
– Psychologist & psychiatrist
An Integrated Suite of Health Promotion and Protection Services
• Work ability program
• Primary care
– Care registries built with HWA and claims data
– Care coordination for lifestyle and disease management
• Over 30 FTEs (40 employees)

4/3/2013
12
Introducing a new primary care optionfor Dartmouth Hitchcock Employeesfor Dartmouth‐Hitchcock Employeesand their adult dependents enrolled in our health plan.
Integration?
• Reconfiguration of safety committee to integrate health promotion, work
Partners in Health, Environment, Wellness, and Safety
environment, occupational medicine, and safety activities

4/3/2013
13
Employee Engagement is Number One Challenge Of Health Management Programs
37
Source: Towers Watson NBGH 2010 Survey
Since occupational health risks cluster with personal health risks and impaired work performance …
Let’s use reports of injury to identify and engage those departments and employees that would most benefit from integrated health protection and promotion
The EROI (Electronic Report of Injury)• Web‐based, intranet
• Available throughout system and offsite through VPN
• Completed by eeCompleted by eeor supervisor
• Instant, auto e‐mail alert to all employer stakeholders (occ med, safety, HR, Workability, etc)
4/3/2013
14
– Rapid and more complete reporting
– Immediate notification of key parties
– Assures
• Timely medical care for the individual
The EROI
Timely medical care for the individual
• Safety interventions to prevent further injury in the population,
• Through aggregation, identification of highest risk work departments.
40
• Used for “just in time” integration of occupational and personal health care
• Prompts not only safety intervention, but also– Referral to individual and population health
Novel Approach: EROI as a Sentinel Event to Protect and Promote Health
promotion
– Integrated comprehensive investigation of work environment and organizational factors influencing workgroup health (personal as well as occupational)
• Management of work‐related exposure, injury or illness
• Identification of behavioral risk factors and/or co‐
Individual Response
/morbidities
• Referral to employer resources (EAP, Health coaching, workability programs) and as relevant to primary care/community resources

4/3/2013
15
Population Response:DH Occupational Injury and Illness Clusters
• 90% of the DHMC incidents are occurring in 10% (20) of reporting departments.
• 20 Departments had an incident rate > 20%
To the rescue …
Safety Wellness Action Team (SWAT)
• Work Safety Outliers
– High ROIor
– Cluster of eventsor
• Wellness and Performance Indicators
– < 25%ile HRA participationor
– Low culture of health index
SWAT Triggers
PLUSor
– Critical event– Low culture of health index
or
– Low percentile nursing qualityor
– Low percentile patient satisfaction
PLUS

4/3/2013
16
M
Review
qualitative
response to
surveys
C &D
Gate Keeper: Safety and Environmental Programs Reviews EROI data (At Risk; cluster or sentinel event)
(Workability) SWAT Assessment Form
(A)
No
Yes
Meets intervention criteria?
SWAT Unit/Work
Continue to monitor
SWAT Convenes
No
Yes
Distribution of surveys
C&D to larger unit group
‐Collection box on unit
‐Scored by LWWW Admin
SWAT Convenes
Meeting #2
Local
PHEWS/Safety
Indentify target issues
Identify resources
Plan interventions ( J )
Safety Wellness Action Team Process Flow
Meeting #1: Local
PHEWS/Safety Group ‐Discuss results
‐Unit engaged?
‐Integrated approach appropriate?
Prevention Committee Meeting Discussion: SWAT appropriate? ‐Concerns related by employee
health care provider
No
Yes
Key to resources
A. Action Triggers
B. Unit Dashboard
C. The Whole Worker Assessment
D. Dimensions Survey
J. Interventions Menu
‐‐‐‐‐‐‐‐‐ Workability Care Manager
Meetin
g series
90days
SWAT Unit/Work Group Dashboard
Review Dashboard with Unit Leadership
Interest?
Yes
No
Unit or Workgroup has PHEWS (safety) committee?
Work with PHEWS/Leadership to form local PHEWS (safety) committee
No
Yes
Send out Initial surveys (C and D)
Collection box on unit
Data analysis/scoring
LWWW Admin Intervention
SWAT Unit/Work
Group Dashboard
Data analysis
Improvement?
Local PHEWS/ Safety Group
‐ Continued monitoring ‐Provision of support
Resources
Yes
No
Unit Dashboard
• Initial open ended safety and socio‐environmental health assessments
• Self‐Scored psychosocial and personal health Assessments
Next Steps: Work Environment Assessment
– Whole worker questionnaire
– Culture of health
– Burn‐out
– Depression and Anxiety
– Perceived stress
– Physical well‐being

4/3/2013
17
• Stand‐up local PHEWS committee
• Integrated team intervention (SWAT) may include:– Ergonomic
– Supervisor training
Interventions
– Behavioral health
– Team/resiliency building
– Chaplaincy
– Lifestyle coaching
– Environmental changes to better support personal health, such as healthier food options, staffing, scheduling
Measuring the Impact:Value Chain Approach
• Work Environment• Program delivery
– Program components– Participation in assessments– Engagement in programsg g p g– Program satisfaction
• Health and well‐being– Job engagement– Health culture index– Readiness to change– Lifestyle risk
Measuring the Impact:Value Chain Approach
• Occupational health– eROI– OSHA rates– WC claim rates
• Personal clinical outcomesi i– Biometrics
– Quality of care– Disease burden
• Business outcomes– PMPM health claims cost– Lost productivity– Return on investment

4/3/2013
18
Selected Outcomes
NBGH Cafeteria Audit
8593
99
80
100
120
31
0
20
40
60
80
2006 2010 2011 2012
2006
2010
2011
2012
50.0%
60.0%
70.0%
2009‐10
HWA Participation Rates
10.8%
60.5% 62.0%
0.0%
10.0%
20.0%
30.0%
40.0%
HRA
Year of Program
2010‐11
2012
Behavioral EconomicIntervention

4/3/2013
19
78.78
81.72
79
80
81
82
83
Health and Wellness Assessment:
Average Lifestyle Score
55
76.83
74
75
76
77
78
Year 1 Year 2 Year 3
Average Lifestyle Score
Participation: 10.8% 60.5% 62%
T1 – T2 Behavioral Risk Improvements 3281 matched participants
4/3/2013
20
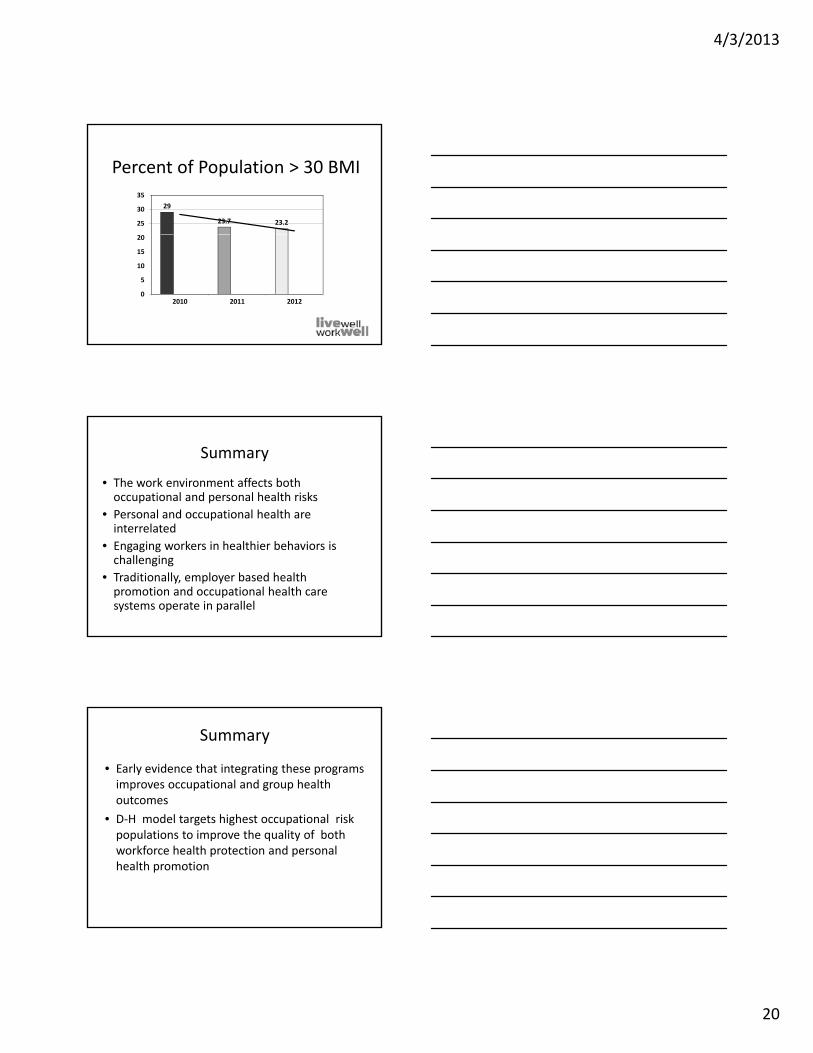
Percent of Population > 30 BMI
29
23.7 23.225
30
35
0
5
10
15
20
2010 2011 2012
• The work environment affects both occupational and personal health risks
• Personal and occupational health are i t l t d
Summary
interrelated
• Engaging workers in healthier behaviors is challenging
• Traditionally, employer based health promotion and occupational health care systems operate in parallel
• Early evidence that integrating these programs improves occupational and group health outcomes
• D H model targets highest occupational risk
Summary
• D‐H model targets highest occupational risk populations to improve the quality of both workforce health protection and personal health promotion

ACOEM POSITION STATEMENT
Optimizing Health Care Delivery by Integrating Workplaces,Homes, and Communities
How Occupational and Environmental Medicine Can Serve as a Vital Connecting Link BetweenAccountable Care Organizations and the Patient-Centered Medical Home
Robert K. McLellan, MD, Bruce Sherman, MD, Ronald R. Loeppke, MD, Judith McKenzie, MD,Kathryn L. Mueller, MD, Charles M. Yarborough, MD, Paul Grundy, MD, Harris Allen, PhD,
and Paul W. Larson, MS
EXECUTIVE SUMMARYIn recent years, the health care re-
form discussion in the United States hasfocused increasingly on the dual goals ofcost-effective delivery and better patient out-comes. A number of new conceptual modelsfor health care have been advanced to achievethese goals, including two that are wellalong in terms of practical development andimplementation—the patient-centered medi-cal home (PCMH) and accountable care or-ganizations (ACOs).
At the core of these two emergingconcepts is a new emphasis on encouragingphysicians, hospitals, and other health carestakeholders to work more closely togetherto better coordinate patient care through in-tegrated goals and data sharing and to createteam-based approaches that give a greaterrole to patients in health care decision-making. This approach aims to achieve betterhealth outcomes at lower cost.
The PCMH model emphasizes the-central role of primary care and facilita-tion of partnerships between patient, physi-cian, family, and other caregivers, andintegrates this care along a spectrum thatincludes hospitals, specialty care, and nurs-
This article was prepared by the Committee of theACOEM Council on Public Affairs of ACOEM:Robert K. McLellan, MD; Bruce Sherman, MD;Ronald R. Loeppke, MD; Judith McKenzie, MD;Kathryn L. Mueller, MD; Charles M. Yarborough,MD; Paul Grundy, MD; Harris Allen, PhD; andPaul W. Larson, MS. This was reviewed by theCommittee on Policy, Procedures, and Public Po-sitions and approved by the ACOEM Board ofDirectors on February 4, 2012.
ACOEM requires all substantive contributors to itsdocuments to disclose any potential competing in-terests, which are carefully considered. ACOEMemphasizes that the judgments expressed hereinrepresents the best available evidence at the timeof publication and shall be considered the posi-tion of ACOEM and not the individual opinionsof contributing authors.
Address correspondence to: Marianne Dreger, MA,ACOEM, Elk Grove Village, IL ([email protected]).
Copyright C© 2012 by American College of Occupa-tional and Environmental Medicine
DOI: 10.1097/JOM.0b013e31824fe0aa
ing homes. Accountable care organizationsmake physicians and hospitals more account-able in the care system, emphasizing organi-zational integration and efficiencies coupledwith outcome-oriented, performance-basedmedical strategies to improve the health ofpopulations. The ACO model is meant toimprove the value of health care services,controlling costs while improving qualityas defined by outcomes, safety, and patientexperience.
This document urges adoption of thePCMH model and ACOs, but argues that inorder for these new paradigms to succeedin the long term, all sectors with a stakein health care will need to become betteraligned with them—including the employercommunity, which remains heavily investedin the health outcomes of millions of Amer-icans. At present, ACOs are largely beingdeveloped as a part of the Medicare andMedicaid systems, and the PCMH modelis still gathering momentum and evolvingamong physicians. But, the potential existsfor implementation of both of these con-cepts across a much broader community ofpatients.
By extending the well-conceived in-tegrative concepts of the PCMH model andACOs into the workforce via occupationaland environmental medicine (OEM) physi-cians, the power of these concepts wouldbe significantly enhanced. Occupational andenvironmental medicine provides a well-established infrastructure and parallel strate-gies that could serve as a force multiplierin achieving the fundamental goals of thePCMH model and ACOs. In this paradigm,the workplace—where millions of Ameri-cans spend a major portion of their dailylives—becomes an essential element, nextto communities and homes, in an integratedsystem of health anchored by the PCMH andACO concepts. To be successful, OEM physi-cians will need to think and work innovativelyabout how they can provide today’s employerhealth services—ranging from primary careand preventive care to workers’ compensa-tion and disability management—within to-morrow’s PCMH and ACO models.
INTRODUCTION ANDBACKGROUND
Today, the American health care sys-tem faces enormous and growing challenges.Health care costs in the United States, alreadyhighest in the world, continue to spiral up-ward. An estimated 50 million Americans areuninsured and Medicare and Medicaid facehuge financial issues that threaten their long-term stability. Chronic health conditions areon the rise across all age groups, with morethan 50% of Americans having at least onechronic health condition.1 Millions of babyboomers are retiring, placing new strains onthe nation’s health care infrastructure at atime when the shortage of physicians in theUnited States is projected to reach 62,000 by2015 and 130,000 by 2025.2 Those workerswho remain in the system, increasingly besetby chronic disease, have a greater likelihoodof needing to access social security disabilityand Medicare before retirement age, poten-tially weakening the nation’s work capacityeven more.
In response to the dual problems of in-creased costs and the growth of the nation’suninsured population, Congress passed andthe President signed into law in 2010 the Af-fordable Care Act (ACA), a massive federalbill with wide-ranging mandates.3 Althoughmuch of the law has the practical intent ofsimply extending insurance coverage to thosewho are currently uninsured, it also has anumber of provisions intended to fundamen-tally transform the way care is delivered. In-centives are included, for example, to encour-age the adoption of electronic health records(EHRs) and to promote disease preventioninitiatives more widely.
Among these transformational strate-gies is a new emphasis on encouragingphysicians, hospitals, and other health sys-tem stakeholders to work together in newways to better coordinate care, creating amore team-based approach to health care.This approach aims to achieve better healthoutcomes at lower cost. Two models ofcare, in specific, are incentivized withinthe ACA:
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
504 JOEM Volume 54, Number 4, April 2012

JOEM Volume 54, Number 4, April 2012 Optimizing Health Care Delivery
• The Patient Centered Medical Home, aconcept that emphasizes the central roleof primary care and facilitation of partner-ships between patient, physician, family,and other caregivers, is built on a “whole-person” orientation that envisions care in-tegrated across all elements of the healthcare system and links hospitals, subspe-cialty care and nursing homes with a pa-tient’s community environment. Patientsreceive care in a setting that is famil-iar and in which their health care needsand choices are well known. A number ofleading physician organizations have beenproponents of the concept, including theAmerican Academy of Family Physicians(AAFP), American Academy of Pediatrics(AAP), American College of Physicians(ACP), and American Osteopathic Asso-ciation (AOA).4
• Accountable Care Organizations, acare model that makes physicians andhospitals more accountable in the caresystem, emphasizing organizationalintegration and efficiencies coupled withoutcome-oriented, performance-basedmedical strategies to improve the health ofpopulations, is meant to improve the valueof health care services, controlling costswhile improving quality as defined byoutcomes, safety, and patient experience.It envisions the medical home as a centrallocus in a spectrum of health care servicesapplying evidence-based approaches injoint ventures among organizations thatdecrease the fragmentation of the currentsystem. Guidelines for the developmentof ACOs within the Medicare system havebeen proposed by the federal governmentto encourage their growth.
The connecting thread betweenPCMH and ACOs is a shared vision thatintegration and coordination of health careservices, combined with a new emphasis onwhole-person team-oriented care delivery,drives value and represents a vital pathforward in true health reform. Interest inthe two concepts is growing, especially withincentives built into the ACA. A new Centerfor Medicare and Medicaid Innovationhas been established and is charged withimplementing PCMH and ACO demon-stration projects. State governments areinvestigating PCMH/ACO models, andmost of the major health plans have startedPCMH demonstrations. The Departmentsof Defense and Veterans Affairs haveboth adopted a PCMH-based approach tocare.5
As interest in PCMH and ACOs con-tinues to grow and demonstration projectsincrease, a new discussion is emerging abouthow a PCMH/ACO model for care could bemore widely implemented and systematized.In order for the PCMH/ACO model to suc-
ceed in the long term, all sectors with a stakein health care will need to become betteraligned with it—ranging from the medicaleducation community to government policy-making agencies and insurers. Of these sec-tors, one of the most impactful—and, it can beargued, most essential—to the future of thePCMH/ACO concept is the employer com-munity.
According to the US Census Bureau,55% of the US population is covered byemployer-based health plans—a total of 169million people.6 The health care decisions ofthese citizens are closely connected with theirworkplace, and in recent decades employ-ers have become increasingly proactive asproviders of programs and initiatives aimed atkeeping their workforces healthier. A grow-ing body of research shows an inextrica-ble link between the health of the work-force and the productivity of the workforce,and enlightened employers are taking stepsin response.7 From disease prevention pro-grams to on-site and near-site health clinicsstaffed by a spectrum of health care person-nel, they are becoming a more and more in-fluential part of the health care equation.
Moreover, if the PCMH/ACO conceptis built on the idea of a whole-person ap-proach to health, the workplace must logi-cally play an integral role. The workplace isorganically connected to the home and to thephysical communities in which workplacesexist. Individuals do not leave the impactsof their personal health risks on the doorstepwhen they leave for work just as they cannotleave the impacts of their workplace expo-sures when they return home. Health behav-iors extend across multiple environments andcannot be artificially separated.
Because health in the workplace,health at home, and health in communitiesare interconnected, workplace health initia-tives are uniquely positioned to leverage thecoordinated health and productivity enhance-ment strategies that are a fundamental goalof PCMH and ACOs. By better aligning thenation’s growing workplace health initiativeswith the long-term goals of the PCMH/ACOmovement, the potential impact of PCMHand ACOs could be dramatically increased.Efforts aimed at integrating health initia-tives in the workplace could ultimately beconnected with both the medical home andACOs, with the employer’s workplace healthpersonnel occupying roles as members ofan individual’s “health team” and medicalcommunity.
At the core of this envisioned effortwould be the nation’s OEM physicians, whoare trained in the development and deliveryof workplace health initiatives and are posi-tioned to serve as the critical connecting linkbetween PCMH/ACO concepts and the morethan 130 million Americans who make up theUS workforce. Thousands of US OEM physi-
cians currently serve as the central point ofconnection between these employed popula-tions and the overall US health care system.
Why is OEM Essential?Occupational and environmental
medicine physicians enhance the health ofworkers through preventive medicine, clin-ical care, disability management, research,and education. In the early days of occu-pational medicine, physicians specializingin the health of employees were primarilyreactive to the injuries and exposures thatoccurred in the workplace. Workers whobecame sick or were injured came to theworksite clinic; the physician’s focus wason treating the injured employee or on“work-related conditions.”
Now the role of the OEM physicianhas changed significantly. As disease preven-tion and wellness have become a greater partof the health care equation, OEM has ex-panded its scope and presence accordingly,contributing to scientific research, new clin-ical guidelines for medical care, and publichealth programming aimed at the workforceand the health of the environment. Asidefrom employers’ economic interest in thehealth of the workforce, the expanded fo-cus of occupational medicine is based onthe evidence that the employer resources inthe work environment can profoundly im-pact not just health and safety on the job butalso the personal health of employees. More-over, investigators have documented the syn-ergistic effect of integrating health protec-tion with health promotion. The additionalopportunity that an expanded focus on OEMbrings is integration of employer-based re-sources with community-based health careresources.8 Occupational and environmentalmedicine physicians currently focus their ex-pertise on improving the overall health of theworker, including areas such as preventionof infectious disease and decreasing obesity.These chronic conditions affect employeehealth and productivity in the workplace.
Occupational and environmentalmedicine physicians have developed exper-tise in assessing the ability of employees toperform work; the arrangements of work; thephysical, chemical, biological, and social en-vironments of the workplace; and the healthoutcomes of environmental exposures. Theyare skilled at using the tools of preventivemedicine (primary, secondary, and tertiary)to improve the health of a defined populationof workers and their families. They arealso trained in the complex return-to-work(RTW) process, an advanced system ofhealth monitoring that optimizes the time inwhich ill or injured workers can safely returnto work. Occupational and environmentalmedicine physicians—especially those inlarge corporations—often play a key role inbenefit design, bringing valuable medical
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 American College of Occupational and Environmental Medicine 505

McLellan et al JOEM Volume 54, Number 4, April 2012
perspective to this process. In addition tothe skill sets they apply to the health ofindividuals, OEM physicians bring expertisein the health of populations—in essence,serving as public health officers for thenation’s employed populations.
In one area in particular—workers’compensation—the standard of practice byOEM physicians encompasses many of thebedrock principles of the PCMH model andACOs. Studies show that physicians who ad-here to established best practices in workers’compensation cases improve patient healthresults and reduce costs.9,10 Occupationaland environmental medicine physicians inworkers’ compensation are trained to beoutcome-oriented, placing a premium on re-turning functionality to injured or ill employ-ees and returning them to the workplace in atimely manner. They also focus on measur-able outcomes, controlling costs, and inte-grating care across a team, which can includeprimary care physicians, specialists, physi-cal therapists, industrial hygienists, employ-ers, and many others—mirroring the goalsof PCMH and ACOs. In sum, OEM physi-cians represent an integrating health profes-sion, serving as a connecting link betweenthe community-based health care system andemployer-based health services.
About This DocumentThis document explores the poten-
tially powerful connection between the OEMcommunity in the United States, ACOs, andthe PCMH, and outlines the key pointsof intersection between the three (Fig. 1).Features of employer-sponsored health ser-vices that are essential to and complemen-tary with those available in PCMH andACOs are highlighted, along with opportu-nities to integrate OEM services more fullyinto the PCMH/ACO model to make it moreeffective.
FIGURE 1. Connections between theworkplace, the community, and thehome.
A wide range of current infrastruc-ture resources in the workplace are alsohighlighted—resources that could be lever-aged to dramatically extend the impact ofPCMH and ACOs. These range from adeep and wide infrastructure for supportinghealth behavior change (employee benefit de-sign, workplace incentive programs, and so-cial reinforcement mechanisms) to employer-sponsored health innovations such as exercisefacilities, workplace nutrition programs, andworksite clinics delivering urgent, and some-times primary, care in addition to occupa-tional health services.
This article examines OEM’s al-ready well-established alignment with thewhole-person concept that runs through thePCMH/ACO model, highlighting medicalsurveillance in the workplace, the use ofhealth risk assessments, and case manage-ment in programs such as workers’ compen-sation. In addition, this article offers uniquestructural components that could be actuallyadded to the PCMH/ACO model to make itmore effective: For example, OEM’s exper-tise in maintenance and restoration of func-tion as a health outcome, which could beuseful in PCMH, use of business-relevanthealth and productivity outcomes measuresand metrics or its use of evidence-basedguidelines and its growing ability to demon-strate return on investment gained from work-place health programs, both of which couldbenefit ACO strategies. The document con-cludes with a set of basic recommenda-tions for bringing the employer community,PCMH and ACOs into closer alignment forthe overall benefit of the nation’s patients, cre-ating a new health care paradigm comprisingthese three elements.
THE EMERGING ROLE OF ACOSAND PCMH IN US
HEALTH CAREThe rise of the PCMH and ACO con-
cepts within the US health care system hasbeen rapid—coalescing and gathering mo-mentum recently.
The PCMH ConceptAlthough the ideas behind the PCMH
concept have been discussed for years, theidea gained significant traction in 2007 whenthe AAP, AAFP, ACP, and AOA adopted aset of joint principles describing the charac-teristics of the PCMH.4 Following are amongthe key principles in the PCMH concept, asenvisioned by these groups:
• Personal physician: In a PCMH system,each patient has an ongoing relationshipwith a personal physician.
• Physician-directed medical practice: Thepersonal physician leads a team of indi-viduals at the practice level who work col-lectively to provide care. Patient-centered
medical home teams may include a widerange of participants—from physicians,physician assistants, nurse practitioners,nurses, and pharmacists to social workersand educators.
• Whole-person orientation: The personalphysician is responsible for providing caredirectly or arranging for care by coordi-nating with other qualified professionals.The care settings range from acute care tochronic care, prevention, and end-of-lifecare. An emphasis is placed on prevention.
• Coordinated care: Care is coordinatedacross all levels of the health caresystem—ranging from physician offices tohospitals to home health care and nurs-ing homes. Patients receive care when andwhere they need and want it, in a way thatresponds to their unique needs.
• Quality and safety: Quality and safety isensured through the use of evidence-basedmedicine (EBM), clinical decision sup-port tools, patient engagement in decision-making, information technology, per-formance measurement, and continuousquality improvement strategies.
• Wider access to physician services: En-hanced access is made possible throughopen-scheduling systems, electronic com-munication, and other methods.
• Payment reforms: Payment becomes akey tool in advancing the PCMH con-cept; physicians are incentivized to makethe system succeed, sharing in the sav-ings from reduced hospitalizations andfor achieving measurable and continuousquality improvements or adopting infor-mation technology, for example.
PCMH: “Neighbors”In 2010, the ACP published The
Patient-Centered Medical Home Neigh-bor: The Interface of the Patient-CenteredMedical Home with Specialty/SubspecialtyPractices.10 This monograph outlined anapproach to integrating specialty and sub-specialty practices with the PCMH to as-sure effective coordination of care and meetthe goals of the PCMH. The occupationalmedicine clinic, whether located at an em-ployer’s worksite or in the community, is animportant PCMH neighbor, which brings notonly a valuable clinical specialty but also akey linkage with employers.
Accountable Care OrganizationsAlthough PCMH provides the center-
piece for a new, more efficient, and effectivehealth system, it relies on another compo-nent to achieve its potential—the ACO. Someview ACOs as representing a greater “med-ical neighborhood”: the extensive commu-nity of specialists and other providers that,together, comprise an accountable systemthat delivers value-based care and ensurescost savings, largely through assumption of
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
506 C© 2012 American College of Occupational and Environmental Medicine

JOEM Volume 54, Number 4, April 2012 Optimizing Health Care Delivery
financial risk due to projected health carecost trends. If health care cost trend is mit-igated, then ACOs will share in a portionof the savings. According to the US Depart-ment of Health and Human Services, ACOsare intended to provide better care for in-dividuals, better health for populations, andslower growth in costs through improvementsin care and a more satisfying care experiencefor both patients and providers.11
The establishment of ACOs is for-mally outlined in the recently passed ACA,and a new Center for Medicare and MedicaidInnovation has been established and chargedwith implementing demonstration projects ofboth ACOs and the PCMH. In the fall of2011, the National Committee for QualityAssurance released the standards and guide-lines that compose its new Accountable CareOrganization Accreditation Program, and thefirst ACO contracts with Medicare were es-tablished in January 2012.
Although the structure and implemen-tation of the ACO and PCMH concepts arestill being discussed and debated, there iswidespread agreement that they representreasonable approaches to improve health carequality and lower the current cost trend. TheObama Administration has estimated thatACOs could deliver nearly $1 billion in sav-ings in the first 3 years of their rollout underMedicare.12 Savings gleaned from the imple-mentation of ACOs would be distributed asbonuses to participating hospitals, other orga-nizations, and physicians, who meet qualitystandards and keep costs below benchmarksset by the government. Without the supportand participation of the employer communitythese goals will be difficult to achieve.
Participants in Medicare ACOs mayinclude physicians in group practices, net-works of individual practices, hospitals thatemploy physicians, and partnerships in-volving these groups and other health-provider organizations, such as long-termcare facilities.13 Elements of ACOs includethe following:
• Care teams, composed of primary carephysicians, physician assistants, nursepractitioners, specialists, and others whocoordinate patient care across the spectrumof an illness episode and health status.
• Added focus on use of EBM, quality out-comes, and safety engineering.
• Increased use of information technologyin all aspects of care.
• Reduction of high-volume and high-profitmargin services, new emphasis on valueand outcomes.
An evidence- and outcome-based sys-tem of best practices, as envisioned in theACO model, has the potential to return signif-icant savings to Medicare, which, accordingto former Centers for Medicare and Med-icaid Services Director Don Berwick, MD,
spent $26 billion in 2009 on care for patientswho returned to hospitals within a month oftheir release.14 In the private sector, varioushealth care entities are also establishing ACOdemonstration projects. In a large-scale pilotproject in New York, for example, in 2011,six health plans paid incentives of $1.5 mil-lion to 236 primary care physicians in 11practices for demonstrating PCMHs in NewYork’s Hudson Valley. In combination, thepractices impact nearly a half million patientsin the Hudson Valley area.15
WHY EMPLOYERS CAREABOUT ACOS AND PCMH
Health care costs in the US con-tinue to rise sharply—an issue that affectsboth individuals and employers. Average em-ployer medical costs increased rapidly in thedecade between 2000 and 2010, and showno signs of slowing down.16 Between 2001and 2011, employer premiums for health in-surance more than doubled according to theKaiser Family Foundation.17 Employers areincreasingly impacted by a number of signif-icant national health and demographic trends,for example:
• The incidence of chronic health conditionsis increasing across all age groups in theUnited States. It is expected that in the nearfuture, conditions such as diabetes, heartdisease, and cancer will add an enormousburden to already high costs of health carespending. One study found that more than80% of medical spending goes toward carefor chronic conditions.1
• Health risks leading to chronic conditionsare also on the rise. According to the USCenters for Disease Control and Preven-tion, in 2007, only one state (Colorado)had a prevalence of obesity less than 20%.Thirty states had a rate of 25% or more.18
• The American workforce is aging. It is es-timated that between 2006 and 2016 thenumber of workers aged 55 to 64 yearswill increase by 36.5% whereas workersaged between 65 and 74 years and morethan 75 years will increase by 80%.19 By2015, one in every 5 workers will be 55years or older.20
• Older workers face more health chal-lenges. Older workers typically suffer fromchronic health conditions and have mul-tiple health risks. Moreover, the chronicconditions most common among olderworkers often require more care, are moredisabling, and are more difficult and costlyto treat than the chronic conditions that aremore common in younger age groups.21
Employers face these trends with greatconcern. Increasingly, they understand thatas the health risks of the US population in-crease, the disease burden on the workforceincreases—and they recognize that this does
not bode well for their companies. Researchshows that as common chronic conditions,such as cancer, heart disease, and diabetes,increase in the workplace, they drive up to-tal health-related costs for employers.7 Otherhealth conditions among workers—rangingfrom musculoskeletal/pain disorders to de-pression and obesity—add additional costs.7
But employers’ medical and pharma-ceutical cost burden related to these condi-tions is just the tip of a potentially huge ice-berg of overall costs. Employers are also nowseeing evidence of significant productivity-cost impacts related to poor health. Re-search shows a much greater connection be-tween employee health and productivity inthe workplace than was ever realized in thepast.
Studies have shown, for example, thaton average, for every one dollar they spend onworker medical/pharmacy costs, employersabsorb two to three dollars of health-relatedproductivity costs.7 These indirect costs aremanifested largely in the form of presen-teeism (a condition in which employees areon the job but not fully productive), absence,and disability.
Employers bear the cost of poor healthin the workplace directly through employer-provided health care plans and indirectlythrough lowered productivity. As studiesincreasingly show the connection betweenhealthy employees, lowered costs, and in-creased productivity, employers have becomeattentive to initiatives that can help them raisethe level of health and wellness among theirworkers. The PCMH and ACO models, withtheir emphasis on prevention, better patientoutcomes, greater efficiency, and loweredhealth costs, align well with employers’ long-term interests related to workplace health.
Thus, employer involvement in a na-tional movement toward PCMH and ACOs iscritical. Employers are uniquely positionedto recognize, measure, and respond to the in-direct costs related to poor health, as well asthe direct costs, and can help raise awarenessof how important both of these factors are toour overall health system.
Because OEM physicians, workingclosely with the employer community, are ex-perienced at identifying these indirect costsand measuring them, they represent a strongresource for the successful implementationof the PCMH/ACO models. To achieve theirgoals of better outcomes at lower cost,PCMH/ACO operational systems will needto include measurements of both the directand indirect costs of poor health.
Extending measures of indirect costsalongside measures of direct costs could helpaccelerate the adoption of PCMH/ACO ini-tiatives beyond Medicare. The drivers of indi-rect costs—presenteeism, absenteeism, anddisability—speak to the reasons why employ-ers and purchasers “buy” health care; that is,
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 American College of Occupational and Environmental Medicine 507

McLellan et al JOEM Volume 54, Number 4, April 2012
the return they hope to gain from their invest-ment. The inclusion of indirect—as well asdirect—cost measurements in the operationalunderpinnings of PCMH/ACO initiativeswould yield new opportunities for promot-ing purchaser “buy-in” into these initiatives.
WORKPLACE HEALTH:CURRENT ENVIRONMENT
AND TRENDSEmployers’ interest in workplace
health and wellness programming as a busi-ness strategy is clear and well documented.A growing number of companies aim to keeptheir workers more fit by offering resourcessuch as health screenings for high blood pres-sure or cholesterol, newsletters and otherhealth-education materials, fitness counsel-ing and exercise rooms, and more healthyfood choices in vending machines and cafe-terias. They are also instituting more com-prehensive wellness initiatives that involvesophisticated use of health risk assessments,behavior modification programs, and the pro-vision of primary care clinical medical ser-vices in the workplace.
These expanding initiatives in the em-ployer community share many of the goalsand methodologies that are central to thePCMH and ACO models. Elements in PCMHand ACO programming that show up in manyemployer programs range from team-basedapproaches and coordination of care to theuse of electronic information technology todrive results.
Studies show for example, a new inter-est among employers in EBM—a key compo-nent of both PCMH and ACOs—as a tool forachieving cost savings. Employers are usingEBM as the basis for “evidence-based benefitdesign,” a concept that allows them to assessworkforce health and productivity at the indi-vidual disease level and to generate and refinestrategies aimed at health improvements.22
In this model, routine data about health andmedical costs, health promotion and preven-tion efforts, employee health outcomes, andoverall productivity are carefully analyzedand integrated to identify cost drivers anddevelop interventions, including case man-agement for workers with specific diseases.Worker’s compensation data, in particular,offer employers the opportunity to use abest practice measuring-and-monitoring ap-proach to health care, with an emphasis onoptimal results.
Employers are also focusing theirhealth and wellness efforts on populationhealth—another key component of PCMHand ACOs. In workplace settings, OEMphysicians act essentially as populationhealth officers, working with employers in atype of parallel public health system. The Na-tional Aeronautics and Space Administration(NASA), for example, has implemented a
widely studied paradigm of workforce healththat “requires a service construct oriented to-ward human performance; a health modelfocused on population, rather than on indi-vidual goals and objectives; and a measure-ment system oriented toward health statusand outcomes.”23 The NASA program, fo-cused on outcomes for more than 20,000 em-ployees in its system, shares the ACO phi-losophy of continuous quality improvementprocesses and use of best practices, leadingto improved health outcomes for populations.Medical surveillance is a core competencyof the OEM physicians who often administerthese large-scale population-health programsin the workplace.
A strong orientation toward preventivehealth is also on the rise in the workplace, an-other key element of PCMH and ACO plan-ning. Organizations with comprehensive pre-vention programs have proven that they canlower total health care costs, with shortersick leaves, reductions in long- and short-term disability, and improved general work-force health.24 Common prevention strate-gies being introduced into the workplace in-clude health promotion, health education,lifestyle management, job ergonomics, nu-trition counseling, prenatal care, immuniza-tions, and wellness/fitness programs. Healthintervention programs aimed at addressingtobacco use or screening for high cholesterolor hypertension are becoming common in theworkplace and have been shown by studies tobe effective.25,26
Some employers are also implement-ing on-site clinical services that offer manyof the features embedded in the PCMH/ACOconstruct—including EHRs and evidence-based treatment. Although the number ofemployers offering on-site or near-site pri-mary care clinics is still small in the US,their potential to lower costs while improv-ing outcomes has been well documented. Oneof the best examples is Quad/Graphics, alarge Wisconsin-based printing firm, whichinstituted its Quad/Med system of employer-owned medical clinics in the 1990s. Today theclinics employ 42 full-time providers. Actu-arial studies have shown that the clinics saveQuad/Graphics 17% to 31% in health carecosts, compared with other similar employ-ers, while improving the health status andhealth-risk profile of its employees.27
WHY WORKPLACE HEALTHSHOULD BE ALIGNED WITHTHE PCMH/ACO MODELS
The workplace is organically con-nected to the home and to the physical com-munities in which workplaces exist. Healthbehaviors and health risks extend across allthree environments and cannot be artificiallyseparated.8 Just as factors in the workplacecan affect health and well-being at home and
in the community, activities and behaviorsoutside the workplace can affect health andproductivity on the job. In fact, health im-pacts work, and work impacts health.
Research shows that it is becomingincreasingly difficult to distinguish individ-ual behavior at and away from work.28 Thismakes it more difficult to draw the distinc-tion that individuals can only directly affecttheir own health through their actions awayfrom work, whereas employers only directlyaffect worker health through the workplaceenvironment. The concept of health must beconsidered in a broader, more holistic con-text.
Moreover, the integration of healthstrategies between home, workplace, andcommunity can have a kind of ripple ef-fect. Studies show that employer wellnessprograms can be used to influence the well-being of families as well as individuals. In anIBM study, for example, more than 11,000employees participated in a health programthat included goals such as limiting fast food,walking children to school, and limiting timespent with video games. As a result, familyphysical activity increased by 17.1%, healthyeating increased by 11.8%, and use of video-games decreased.29
US Surgeon General Regina Ben-jamin, MD, summed it up by saying “We can’tlook at health in isolation. It’s not just in thedoctor’s office. It’s got to be where we live, wework, we play, we pray. If you have a healthycommunity, you have a healthy individual.”30
Thus, the workplace environment can-not be ignored or approached separately inthe context of a national PCMH/ACO strat-egy aimed at improving health outcomes andlowering costs. According to the US Depart-ment of Labor, the community of workersin the United States is vast, with 143 mil-lion full- and part-time workers. Employeesspend more than 8 hours of their day in theworkplace, and workforce policies influence65% of all adults.31
This community works within a giantinfrastructure that in many ways is perfectlypositioned to act as a conduit for a nationalhealth improvement effort. The natural ad-vantages the workplace brings as a settingfor health improvement strategies include:
• Workplace programs can reach segmentsof the population who may not have accessto health information in other settings.
• Workplace programs are readily accessibleto employees, who spend much more timein the workplace than in their clinician’soffice.
• Workplaces concentrate groups of peopletogether who share common purpose andculture.
• The work environment can be utilized toadvocate for and provide access to healthylifestyles.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
508 C© 2012 American College of Occupational and Environmental Medicine

JOEM Volume 54, Number 4, April 2012 Optimizing Health Care Delivery
• Communicating with workers is straight-forward, due to well-established and orga-nized communications channels.
• Social and organizational supports areavailable in the workplace.
• Organizational hierarchies make possiblethe efficient introduction of new proce-dures, practices, and norms.
• The physical environment of the work-place can be used to affect health behaviors(cafeteria/food selection, ergonomic officedesign, use of stairways, landscaping, etc).
• Financial and other incentives can be uti-lized in the workplace to gain participationin programs.32
It makes abundant sense to better inte-grate the growing effort among employersto improve the health of the workforce—using the nations’ built-in employer infras-tructure and resources—with the aims andpurposes of the new PCMH and ACO mod-els. By aligning and increasing these efforts,the spirit and intent of PMCHs and ACOscould be leveraged dramatically for greaterimpact on overall health care reform.
OEM’S UNIQUE RESOURCES:UNLEASHING THE POWER OF
WORKPLACE HEALTHSTRATEGIES AS A PART OF A
NEW NATIONAL HEALTHVISION
What role can the nation’s OEM physi-cians play in this effort? As noted, a widerange of current PCMH/ACO-friendly re-sources already exist in the workplace. Theserange from a substantial and well-establishedinfrastructure for supporting health behaviorchange (employee benefit design, workplaceincentive programs, and social reinforcementmechanisms) to employer-sponsored healthinnovations such as exercise facilities andworkplace nutrition programs.
Physicians trained in the core compe-tencies of OEM have played a major rolein the conceptualization, development, andadministration of many workplace healthresources—which have expanded signifi-cantly in recent decades. The OEM commu-nity is an important driver behind the neweffort by employers to bring a true culture ofhealth to the workplace.
Occupational and environmentalmedicine physicians have become thenation’s leading experts in the complexinterplay of factors that affect health in theworkplace, developing expertise in assessingthe ability of employees to perform work,the physical, chemical, biological, and socialenvironments of the workplace, employerhealth plans, and the health outcomes ofenvironmental exposures. They have uniqueclinical training in managing the health of
individuals as well as the health of popula-tions, and they are skilled at using the toolsof preventive medicine to improve the healthof a defined population of workers and theirfamilies. Perhaps most importantly, OEMphysicians occupy a critical position at thecenter of virtually all health-related trans-actional activities in the workplace. Theyrepresent the single part of the workplacehealth infrastructure that is often connectedwith virtually all of the other parts—seniormanagement; benefits and human resources;legal; worker’s compensation; governmentregulatory agencies; labor and unions,hospitals, and public health organizations.Occupational and environmental medicinephysicians are a fulcrum of workplacehealth, serving as an important point ofliaison between employer, employee, gov-ernment, and all components of the healthcare system—understanding the needs andchallenges of each of these diverse groups.They provide a unique bridge between theclinical/scientific medical community andthe business-based employer community.
With training in a diverse set of com-petencies, OEM physicians display practiceattributes that mirror many aspects of PCMHand ACOs. Their focus on population healthmanagement, for example, enables OEMphysicians to design and implement strate-gies crucial to improving the health of de-fined populations as envisioned by ACOs.Their familiarity with workers’ compensa-tion and disability management systems pro-vides grounding in the sort of team-oriented,integrated care envisioned by the PCMHmodel. As “preventionists,” OEM physiciansare particularly skilled at risk-factor analysis,an element of the PCMH model that is in-creasingly used by employers as a means ofpreventing health issues with their workersand lowering costs. All of these services andothers provided by OEM physicians extendthe reach of the PCMH/ACO model by serv-ing as a part of the “medical neighborhood”of care that complements the PCMH.
As noted earlier, OEM physicians alsohave the advantage of understanding and de-veloping care strategies that recognize andseek to manage indirect costs and theirsources, alongside direct costs. Of all theclinical specialties, they are best positionedto lead an effort to incorporate indirect costmeasures into the PCMH/ACO models.
Opportunities to Integrate OEMServices into the PCMH/ACOModel
With diverse training and unique skillsets, OEM physicians are at the helm of aninfrastructure that is well positioned to be in-tegrated as a functioning piece of the newPCMH/ACO paradigm. Population healthcare has evolved significantly in recent years
at many large employers, incorporating cre-ative new approaches and sophisticated pro-grams that impact delivery of care far beyondresponding to individual injuries or illnesses.Examples of workplace resources that are al-ready positioned to become a more formalpart of a larger national PCMH/ACO offer-ing include the following:
On-site OEM clinics• Worksite clinics can be included as phys-
ical extensions of community-based med-ical homes, and provide urgent care,chronic condition monitoring, and preven-tive care screening. In particular, improvedaccess to point-of-care services can be uti-lized to promote effective chronic con-dition management. For small clinicianpractices, access to supplemental clinicalstaff may help to off-load low-intensityhealth care services, freeing the physi-cian for more high-acuity/high-intensitypatient care needs. It may also be appropri-ate to consider worksite clinics function-ing in this role as eligible for a portion ofoutcome-based performance incentives. Inthis scenario, worksite clinics can providesupport for PCMH by serving as a bridgebetween patients and their primary carephysicians. Clinic personnel can offer sup-port for chronic disease management, forexample, or provide health education andlifestyle management. Rather than com-peting with PCMH, OEM worksite clinicsin this way can bring additional resourcesto PCMH.33
Employer-sponsored programs for work-ers
• Health coaches, employee assistance pro-grams/behavioral health services, exercisefacilities, health messaging, healthy nu-tritional environment, social support, andhealth screenings have all become morecommon in the workplace.
• As described earlier, worksite-providedhealth-related services can complementexisting community primary care services.Improved access to these services foremployees can facilitate engagement andpromotion of healthy lifestyle behaviors,which may be adopted by family mem-bers, and help to reduce the disparities ofhealth care access.34,35
Financial and social opportunities to sup-port behavior change
• Occupational and environmental medicineclinicians can collaborate with employersto incorporate financial or other incentivesinto the workplace to promote healthy be-haviors. In addition to representative ex-amples of benefit design, activity-basedincentives, and a healthy-food-choice sub-sidy, these strategies can be broad rang-ing and include elimination of co-pays foraccess to primary care services, as someemployers have done.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 American College of Occupational and Environmental Medicine 509

McLellan et al JOEM Volume 54, Number 4, April 2012
• In collaboration with workgroups in anorganization, OEM resources can triggerthe power of social networks to promotehealthy lifestyles.
Near-site full service primary care clinics• Under the guidance of OEM physicians,
some employers have implemented near-site primary care for employees and familymembers, with a comprehensive deliverymodel that has incorporated the elementsof the PCMH model. Use of employer-provided primary care clinics are oftenincentivized through lower out-of-pocketemployee and family member costs. In ru-ral communities and underserved areas ofthe country, these clinics have an addedadvantage in that they can help reducehealth access disparities that these areasfrequently face.
Whole-person services• Medical providers, in general, have not
adopted a practice of acquiring informa-tion about a person’s job that may becritical to understanding that person’shealth or ability to work safely.36 Al-though a cornerstone of PCMH care iswhole-person orientation, the OEM clin-ician augments the whole-person perspec-tive by including a deep understanding ofthe relationship between a worker’s healthand his or her job hazards and demands.Work-focused services include workers’compensation management, preplacementphysical capability examinations, medi-cal surveillance, and ergonomic consul-tation. The findings of these evaluationscan complement existing primary carepractices.
Assessment of work fitness and disabilityprevention and management
• One of the important attributes of OEMphysicians is that they can provide sup-port for stay-at-work and RTW practices.In this role, injured or ill workers can re-turn to work in a more timely and medi-cally safe manner. Collaboration betweencommunity PCMH and OEM physicianscan generate employer value by optimizingworkforce health and productivity. Ulti-mately, employer-based disability preven-tion and management programs benefit thegreater society by reducing the number ofpeople requiring social security disabilityinsurance.
Public health, surveillance, and diseaseprevention in conjunction with community-based public health
• Occupational and environmental medicinephysicians, like those in other special-ties, are increasingly adopting electronicmedical records. Their growing presencein the OEM community will eventuallybe an essential component in the effortto more tightly connect health across theboundaries of home and the workplace—especially facilitating the connection be-
tween OEM specialists and primary carephysicians.
• In the workplace setting, OEM physiciansmay be among the earliest to identifyand monitor for outbreaks of infectiousconditions among employees. They arealso in a position to promote public healthinterventions in the workplace, includinginfection prevention behaviors, such ashand washing and social distancing, aswell as provide a convenient source ofimmunization programs for employees. Inrecent years, workplace health programshave become much more proactive; med-ical professionals bring health strategiesand messages directly to employees,rather than passively waiting for them toattend clinics or report health issues.
• Other resources include:• Mass immunization and screening, such
as flu shots, biometric testing/diabetesscreening.
• Environmental interventions.• Safety improvements in work environ-
ments.• Proactive employer interactions, includ-
ing offering healthier food options, op-portunities for physical activity throughenvironmental design, creating recre-ational opportunities.
Practice guidelines• Occupational and environmental medicine
evidence-based guidelines emphasizefunctional outcomes as a part of healthmeasurement and return to activity andwork as part of a treatment plan. Screeningfor psychosocial factors, such as depres-sion, which can increase the severityof many conditions, and the judicioususe of opioids/pain management, can beprovided by OEM clinicians in a worksiteclinic setting. These clinical care activitiescan either complement—or in regionsof limited clinical community resources,supplement—the available offerings as apart of the guidelines process.
Putting the Concepts intoPractice: IBM and Quad/Graphics
Employers are increasingly creatingworkplace health initiatives that put touse many of these OEM capabilities andstrengths for the benefit of their employeepopulations. Two leading examples are IBMand Quad/Graphics, which have created so-phisticated health infrastructures that haveled to documented improvements in healthoutcomes as well as cost savings.
IBMIBM has become a leading proponent
of a modernized, digitally connected modelof health care delivery, with a focus on bet-ter integration between all members of thehealth care team. It has launched the Patient-Centered Primary Care Collaborative in an
effort to create an environment of coordi-nated, integrated, accessible, and compres-sive care for employees. A number of pilotprojects structured with coordinated care inmind have delivered measurable results forIBM: In one pilot study, the new coordi-nated care model resulted in a 36.3% dropin hospital days, 32.2% drop in emergencydepartment visits and significant savings incosts. IBM’s collaborative program empha-sizes population health management, patient-centered prevention, and integration of ef-forts among primary care, hospitals, and spe-cialists who are accountable for the quality,outcomes, and cost of health care receivedby that population. As a part of its move to-ward coordinated and integrated care, IBMnow asks health care plans to offer patientself-management support, performance out-come measures, open scheduling, the use ofEHRs, and other elements commonly foundin both ACOs and the PCMH concept.37–39
Quad/GraphicsBy creating worksite health clinics
that focus on comprehensive primary careand wellness programs, the Wisconsin-basedprinting company Quad/Graphics trans-formed itself from a purchaser of health in-surance to an investor in employee healthand productivity. The worksite clinics, man-aged through its subsidiary, Quad/Med, placea high priority on patient health and conve-nience by organizing care so that it is ori-ented toward prevention and outcomes ratherthan production. Patient visits, which last 30minutes or longer, enable physicians to ad-dress health prevention needs and promotethe company’s wellness programs, which pro-mote physical activity, weight loss, smokingcessation, and early identification and con-trol of diabetes, as well as risk factors forcardiovascular disease. The company’s healthcare model has helped to lower costs, improvehealth outcomes for employees, and enhancetheir experience of care.27
WHERE DO WE GO FROMHERE?
Strategies for Integrating OEMWith the PCMH/ACO Model
Infrastructure strategies• The workplace should be better leveraged
as an ideal place to support improvementin health behaviors. A new, stronger em-phasis should be placed on the inclusionof the workplace as one of the key settingsfor addressing individual and populationhealth.
• PCMH and ACOs should take advan-tage of the population health manage-ment experience and skills of occupationalphysicians, many of whom effectivelymanage populations. Occupational and
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
510 C© 2012 American College of Occupational and Environmental Medicine

JOEM Volume 54, Number 4, April 2012 Optimizing Health Care Delivery
environmental medicine physicians willplay a central role as integrators of em-ployer and community-based health re-sources.
• An effort should be made to build aware-ness that the social benefit of enhancedproductivity from improved health re-quires engagement of employers to supportdisability prevention programs. To pro-mote this awareness, the development andintegration of measures of indirect costsand the factors that drive them should beintegrated in PCMH/ACO operations.
• Employers should work with the govern-ment sector and medical community toestablish a roadmap for integrating thePCMH and ACO models with currentworkplace health-oriented infrastructureto accelerate adoption of a true workplaceculture of health.
• Initiatives should be launched to integrateefforts at creating a workplace culture ofhealth with similar efforts in the commu-nities in which workplaces are located.Employers should engage with local insti-tutions, ranging from city governments toschools and not-for-profit organizations.
• A more standardized system of met-rics should be developed in conjunc-tion with employers and OEM providersto better measure the impact of work-place health initiatives on both healthoutcomes and total benefit costs, includ-ing productivity costs. Accountable careorganizations must be able to addressand measure concepts such as “work ca-pacity,” disability prevention, and RTWprescriptions.40
• Financial incentives being considered asa part of the PCMH/ACO models shouldbe translated and extended into the work-place to extend the focus on full costsavings (absenteeism/presenteeism costsavings as well as medical/pharmacy costsavings), quality outcomes, and value-based decision-making.
• Similar incentives should be implementedthat would encourage employers to part-ner with insurers who are aligned with thePCMH/ACO models. The ACA, for ex-ample, includes the promotion of PCMHsin its minimum requirements for partici-pation by qualified health plans in healthinsurance exchanges.
• The system of EBM should always includefunctional status measures in addition torisk and disease status. Maintenance andrestoration of function must be a part ofevidence-based treatment.
• Occupational medicine residencies shouldbe funded to ensure the supply of an on-going and critically needed resource: theinclusion of an OEM physician as a mem-ber of the health team positioned to facil-itate synergy between PCMH, ACOs, andemployers.
• Alignment of major stakeholder groupswhose interests are not necessarily consis-tent is needed to ensure PCMH/ACO ini-tiatives gain traction. The employer/OEMcommunity can play a major role in en-couraging this effort. Tactics can be shapedand implemented to foster and advancethe collaboration and cooperation neededfrom diverse groups. These tactics may in-clude steps such as government appoint-ments, targeted tax incentives, the estab-lishment of best practices, and the creationof educational programs for providers andconsumers.41
OEM clinician strategies• Organizations in the occupational health
community, including the ACOEM(American College of Occupational andEnvironmental Medicine), should educatetheir members about the PCMH/ACOmodels and provide them with the tools toengage more proactively in the creationand management of PCMH and ACOs intheir regions and localities.
• Occupational and environmental medicineclinicians working with employers, andparticularly corporate medical personnel,should be provided with education regard-ing health benefit strategies to enhancetheir ability to more broadly apply theirpublic health knowledge and skills to theemployer setting.
• By virtue of their public health training,OEM clinicians can take a more active rolein community health improvement efforts,by applying their employer-focused pop-ulation health management expertise to acommunity level.
• Occupational and environmental medicineclinics can work with local PCMHs to berecognized as “PCMH Neighbors” impor-tant to realizing the goals of both PCMHand ACOs. In particular, OEM clinicianscan use their expertise in disability pre-vention and management to add value forACOs and employers in the health man-agement of employed populations. Occu-pational and environmental medicine clin-icians can work to integrate these princi-ples into community health care practices,as well as ACO performance metrics.
• With their population health managementexperience and skills, OEM cliniciansshould be incorporated into the adminis-trative framework of ACOs.
• Occupational and environmental medicinephysicians should work more proactivelyto encourage an increase in the numberof workplaces offering on-site clinical ser-vices for workers.
CONCLUSIONAccountable care organizations and
the PCMH concept offer great promise inhelping the United States achieve mean-
ingful health reform. Encouraging a moreteam-based approach to care delivery andbetter coordination and information sharingbetween all stakeholders providing healthcare services can ultimately improve patientoutcomes and lower costs.
Both concepts have much develop-ment work ahead before they are widely in-tegrated in the health system; for now, muchof the focus of the ACO model, for exam-ple, has been aimed at Medicare/Medicaidpatients. But there are indications that theACO/PCMH paradigm will be adopted morebroadly. Hospitals and some of the largesthealth insurers in the country, including Hu-mana, United Healthcare, and Cigna, alreadyhave announced their intention to form theirown ACOs to serve the private market.42 And,the PCMH continues to gain visibility, thanksto the strong backing organizations such asAAFP, AAP, ACP, and AOA.4
For these new paradigms to continueto evolve and to succeed in the long term,all sectors with a stake in health care willneed to become better aligned with them—especially the employer community, whichis structurally connected through benefit de-sign and workplace wellness programs withthe health outcomes of millions of Amer-icans. The nation’s community of OEMspecialists—which is at the frontline of work-place health—is the logical catalyst and con-necting link between ACOs, the PCMH con-cept and the nation’s employers.
With its focus on disease prevention,wellness, and public health programming, theOEM community can help complete the in-tegration of health between the home, com-munity, and workplace, which is essential tothe successful implementation of ACOs andthe PCMH model. As the government contin-ues to develop formal standards for ACOs,and leading health organizations adopt thePCMH model, the role of the workplacehealth community should be integrated intothese efforts.
REFERENCES1. Partnership for Solutions. Chronic Condi-
tions: Making the Case for Ongoing Care.Johns Hopkins University, Baltimore, MD:Partnership for Solutions; 2004 Update. Avail-able at: www.partnershipforsolutions.org/DMS/files/chronicbook2004.pdf . AccessedNovember 29, 2011.
2. Association of American Medical Colleges.The Complexities of Physician Supply and De-mand: Projections Through 2025. Washing-ton, DC: Association of American MedicalColleges; 2008.
3. Public Law 111-148–111th Congress. ThePatient Protection and Affordable Care Act.(2010). Available at: http://www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf. Accessed March 19, 2012.
4. American Osteopathic Association, AmericanAcademy of Family Physicians, American
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 American College of Occupational and Environmental Medicine 511

McLellan et al JOEM Volume 54, Number 4, April 2012
Academy of Pediatrics, American College ofPhysicians. Joint principles of the patient-centered medical home. 2007. Available at:www.medicalhomeinfo.org/downloads/pdfs/JointStatement.pdf. Accessed March 14,2012.
5. Kugler JP, Padden M, Miller P, et al. Patient-centered medical home: baseline view acrossthe services and HA/TMA. Presented at:2010 Military Health System Conference;January 15, 2010; National Harbor, Mary-land. Available at: www.health.mil/Libraries/2010 MHS Conference Presentations/Patient-Centered Medical Home - BaselineView Across the Services and HA-TMA.pdf . Accessed November 29, 2011.
6. DeNavas-Walt C, Proctor BD, Smith JC.U.S. Census Bureau, Current Population Re-ports, P60–239. Income, Poverty, and HealthInsurance Coverage in the United States:2010. Washington, DC: US GovernmentPrinting Office; 2011. Available at: www.census.gov/prod/2011pubs/p60–239.pdf. Ac-cessed November 29, 2011.
7. Loeppke R, Taitel M, Richling D, et al. Healthand productivity as a business strategy. J Oc-cup Environ Med. 2007;49:712–721.
8. Hymel P, Loeppke R, Baase C, et al. Work-place health protection and promotion: a newpathway for a healthier–and safer–workforce.J Occup Environ Med. 2011;53:695–702.
9. Green-McKenzie J, Rainer S, Behrman A,Emmett E. The effect of a health caremanagement initiative on reducing workers’compensation costs. J Occup Environ Med.2002;44:1100–1105.
10. American College of Physicians. The patient-centered medical home neighbor: the in-terface of the patient-centered medicalhome with specialty/subspecialty practices.Philadelphia, PA: American College ofPhysicians; 2010: Policy Paper. Availableat: www.acponline.org/advocacy/where westand/policy/pcmh neighbors.pdf . AccessedNovember 29, 2011.
11. Berwick DM. Launching accountable careorganizations—the proposed rule for theMedicare Shared Savings Program. N EnglJ Med. 2011;364:e32. Available at: www.nejm.org/doi/full/10.1056/NEJMp1103602.Accessed November 29, 2011.
12. Johnson A. Rules aim to reshape medical prac-tices. Wall Street Journal. April 1, 2011.
13. Affordable Care Act to improve quality ofcare for people with Medicare [press release].Washington, DC: US Department of Healthand Human Services. March 31, 2011. Avail-able at: www.hhs.gov/news/press/2011pres/03/20110331a.html. Accessed November 30,2011.
14. Evans M. Of interest: it’s quality time.Modern Healthcare. May 3, 2011. Avail-able at: www.modernhealthcare.com/article/20110503/BLOGS01/305039984. AccessedNovember 29, 2011.
15. Mosquera M. Insurers pay New York physi-cians $1.5 million to become ‘medical homes.’Government Health IT. March 9, 2011.Available at: http://govhealthit.com/news/insurers-pay-new-york-physicians-15-million-become-medical-homes. Accessed Novem-ber 29, 2011.
16. Employer health costs to rise in 2011.Reuters. Sept. 27, 2010. Available at: www.reuters.com/article/2010/09/27/us-usa-healthcare-costs-idUSTRE68Q3N520100927.Accessed November 29, 2011.
17. Kaiser Family Foundation and Health Re-search & Educational Trust. Employer HealthBenefits: 2011 annual survey. Menlo Park,CA: Kaiser Family Foundation and Health Re-search & Educational Trust; 2011. Availableat: http://ehbs.kff.org/pdf/2011/8225.pdf . Ac-cessed November 29, 2011.
18. US Centers for Disease Control and Pre-vention. Vital signs: state-specific obesityprevalence among adults — United States,2009. MMWR Morb Mortal Wkly Rep. August6, 2010;59:951–955. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/mm5930a4.htm?s_cid=mm5930a4_w. Accessed Novem-ber 30, 2011.
19. US Bureau of Labor Statistics. Older workers.July 2008. Available at: www.bls.gov/spotlight/2008/older workers/pdf/older workersbls spotlight.pdf . Accessed November 30,2011.
20. Selden B. The aging workforce: a disappearingasset? Management Issues. March 21, 2008.Available at: www.management-issues.com/2008/3/21/opinion/the-aging-workforce-%E2%80%93-a-disappearing-asset.asp. Ac-cessed November 29, 2011.
21. Summer L, O’Neill G, Shirey L. Chronic Con-ditions: A Challenge for the 21st Century.Washington, DC: National Academy on anAging Society; 1999. Challenges for the 21stCentury: Chronic and Disabling Conditions,No. 1:1–6. Available at: www.agingsociety.org/agingsociety/pdf/chronic.pdf . AccessedNovember 30, 2011.
22. Bunn WB L III, Allen H, Stave GM, Naim AB.How to align evidence-based benefit designwith the employer bottom-line: a case study. JOccup Environ Med. 2010;52:956–963.
23. Institute of Medicine of The NationalAcademies. Integrating Employee Health: AModel Program for NASA. Washington, DC:National Academies Press; 2005. Availableat: www.nap.edu/openbook.php?record id=11290&page=R1. Accessed November 30,2011.
24. Baicker K, Cutler D, Song Z. Workplace well-ness programs can generate savings. HealthAff (Millwood). 2010;29:304–311.
25. Sutherland LA, Kaley LA, Fischer L. Guidingstars: the effect of a nutrition navigation pro-gram on consumer purchases at the supermar-ket. Am J Clin Nutr. 2010;91:1090S–1094S.Available at: www.ajcn.org/content/91/4/1090S.long. Accessed November 8, 2011.
26. Gottlieb NH. Workplace smoking policies andprograms. In:Breslow L, ed. Encyclopedia ofPublic Health. Vol 4. Farmington Hills, Mich:Gale Group; 2002:1316–1317. Available at:www.scribd.com/doc/62881478/Encyclopedia-of-Public-Health-Vol-4–2001. AccessedNovember 29, 2011.
27. Zastrow R, Van Gilder T, Quadracci LJ. Prac-tice profile. An employer-directed health planthat seeks to reenergize primary care. HealthAff (Millwood). 2010;29:976–978.
28. Seabury SA, Lakdawalla D, Reville RT. TheEconomics of Integrating Injury and Illness
Prevention and Health Promotion Programs.Santa Monica, CA: RAND Institute for CivilJustice; 2005.
29. Sepulveda MJ, Lu C, Sill S, YoungJM, Edington DW. An observational studyof an employer intervention for chil-dren’s healthy weight behaviors. Pediatrics.2010;126:e1153–e1160.
30. Brown E. Surgeon general discusses healthand community. Los Angeles Times. March 13,2011.
31. Schroeder SA. We can do better – im-proving the health of the American peo-ple. N Engl J Med. 2007;357:1221–1228.Available at: www.nejm.org/doi/full/10.1056/NEJMsa073350. Accessed November 29,2011.
32. Goetzel RZ, Roemer EC, Liss-Levinson RC,Samoly DK. Workplace Health Promotion:Policy Recommendations that EncourageEmployers to Support Health ImprovementPrograms for Their Workers. Washington,DC: Partnership for Prevention; 2008: Pre-vention Policy Paper. Available at: www.prevent.org/data/files/initiatives/workplacehealtpromotion-policyrecommendations.pdf . Accessed November 29, 2011.
33. Sherman B. Worksite clinics and the patient-centered medical home: competition or col-laboration? Am J Manag Care. 2010;16:323–325.
34. Izlar AC. Verizon works to eliminate dis-parities in health care for its diverse work-force. Health Aff (Millwood). 2005;24:421–423.
35. Izlar AC. The corporate role in reducingdisparities: initiatives under way at Verizon.Health Aff (Millwood). 2011;30:1992–1996.
36. Institute of Medicine. Incorporating oc-cupational information in electronichealth records. Washington, DC: NationalAcademies Press; 2011. Available at: www.nap.edu/openbook.php?record_id=13207&page=R1. Accessed November 30, 2011.
37. Bindman AB, Grumbach K, Osmond D,Vranizan K, Steward AL. Primary care andreceipt of preventive services. J Gen InternMed. 1996;11:269–276.
38. Safran DG, Taira DA, Rogers WH, KosinskiM, Ware JE, Tarlove AR. Linking primary careperformance to outcomes of care. J Fam Pract.1998;47:213–220.
39. Stewart Al, Grumbach K, Osmond DH,Vranizan K, Komaromy M, Bindman AB. Pri-mary care and patient perceptions of access tocare. J Fam Pract. 1997;44:177–185.
40. Sherman B, Parry T, Hanson J. Patient-centered Medical Home Performance Met-rics for Employers. Washington, DC: Patient-Centered Primary Care Collaborative Cen-ter for Employer Engagement; 2010: WhitePaper. Available at: www.pcpcc.net/files/metrics guide 2011.pdf . Accessed November29, 2011.
41. Allen H. Sustainable healthcare reform: to-ward a national strategy built on recent em-ployer “health and productivity” successes. JHealth Productivity. 2011;5:10–12.
42. Gold J. FAQ on ACOs: accountable care orga-nizations: ACO is the hottest three-letter wordin health care. Kaiser Health News. October21, 2011.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
512 C© 2012 American College of Occupational and Environmental Medicine
ACOEM GUIDANCE STATEMENT
Workplace Health Protection and PromotionA New Pathway for a Healthier—and Safer—Workforce
Pamela A. Hymel, MD, Ronald R. Loeppke, MD, Catherine M. Baase, MD, Wayne N. Burton, MD, Natalie P.Hartenbaum, MD, T. Warner Hudson, MD, Robert K. McLellan, MD, Kathryn L. Mueller, MD, Mark A. Roberts,
MD, Charles M. Yarborough, MD, Doris L. Konicki, MHS, and Paul W. Larson, MS
T raditionally, health protection and health promotion activitieshave operated independently of each other in the workplace.
Health protection has usually been viewed as encompassing the activ-ities that protect workers from occupational injury and illness rangingfrom basic safety training to the use of protective gear, work orga-nization, and safety-enhancing modifications. Health promotion, bycontrast, has usually been viewed as encompassing the activities thatmaintain or improve the personal health of a workforce—rangingfrom health risk assessments to wellness initiatives and immuniza-tions.
By placing boundaries around these activities (creating work-place “silos”), their overall effectiveness has been limited. A newconcept, “Workplace Health Protection and Promotion,” seeks toaddress this limitation by systematically integrating these two previ-ously independent functions. Today’s best evidence indicates that theaims of both health protection and health promotion interventionsare best achieved when they are working in concert.
Workplace health protection and promotion enhances theoverall well-being of a workforce by more closely integrating healthpromotion and health protection activities along a continuum. Inthis model, health promotion interventions contribute dynamicallyto improved personal safety in addition to enhancing personalhealth, while occupational safety interventions contribute dynam-ically to improved personal health in addition to enhancing personalsafety.
The two factors, personal health and personal safety—eachessential to a productive worker and to a productive workplace–are effectively combined in a symbiotic manner that increases theirimpact on overall health and productivity. The whole becomes greaterthan the sum of its parts. Once health protection and promotionprograms are intertwined and deployed strategically to enhance eachother, a healthier workforce thus becomes a safer workforce and viceversa.
Organizations, whether large or small, can engage in this newstrategy by systematically integrating their health promotion safetyand environmental programs, policies, and processes. Activities in-corporated in workplace health protection and promotion are diverseand reflect a wide range of functions and goals. Examples includeassessing worker health status, addressing personal health risks, theearly recognition and treatment of injury or illness, job safety ini-tiatives and efforts to create cultures of health and safety, disabilityprevention and return-to-work programs, emergency preparednessplanning, and behavioral health and environmental safety initiatives.While these may appear to be diverse approaches, they are all aimedat the same thing: promoting overall health and preventing workplaceinjuries and illnesses.
Stated simply, workplace health protection and promotion isthe strategic and systematic integration of distinct environmental,health, and safety policies and programs into a continuum of activi-
Copyright C© 2011 by American College of Occupational and EnvironmentalMedicine
DOI: 10.1097/JOM.0b013e31822005d0
ties that enhances the overall health and well-being of the workforceand prevents work-related injuries and illnesses.
ABOUT THIS DISCUSSION ARTICLEThis discussion article makes the case for a new way of ap-
proaching health protection and health promotion, advancing thepremise that a healthier workforce will be a safer workforce and asafer workforce is a healthier workforce. This article discusses thecurrent state of workplace health, safety, and environmental pro-grams; reviews the literature on the impact of these programs; anddiscusses how the integration of health protection and promotionactivities can improve safety and decrease workplace injuries andillness.
PROBLEMCurrently, most workplace health protection programs (ie,
safety and work environment) are separated from workplace healthpromotion (WHP) programs (ie, wellness and disease management).The two are often housed in completely distinct organizational di-visions with health protection often residing in non-health orientedunits and health promotion initiatives a function of human resourcesor benefits. These programs are usually run as distinct, separateactivities, with minimal attempts at integration. This lack of inte-gration prevents optimal resource utilization and impedes efforts tomaximize the overall health and productivity of the workforce.
HYPOTHESISIntegrating traditionally independent health protection and
health promotion activities will create synergy and enhance the over-all health and well-being of the workforce while decreasing the like-lihood of workplace injuries and illnesses.
WHAT IS DRIVING THE NEED TO INTEGRATEHEALTH PROTECTION AND HEALTH PROMOTION?
The American health care system faces enormous challengesand is on a collision course with several trends that have dire conse-quences for the nation:
• Chronic health conditions are on the rise across all age groupsin the United States, and it is expected that in the near future,conditions such as diabetes, heart disease, and cancer will add anenormous burden to already high costs of health care. Employerswill be particularly impacted as they provide medical benefits foremployees and absorb the costs of absenteeism and of long- andshort-term disability claims.1
• Nearly 50% of Americans have one chronic health condition, andof this group, nearly half have multiple chronic conditions.2 Onestudy found that more than 80% of medical spending goes towardcare for chronic conditions.2
• Health risks leading to chronic conditions are also on the rise. Ac-cording to the Centers for Disease Control and Prevention (CDC),in 2007, only one state (Colorado) had a prevalence of obesity lessthan 20%. Thirty states had a prevalence equal to or greater than25%.3
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
JOEM Volume 53, Number 6, June 2011 695

Hymel et al JOEM Volume 53, Number 6, June 2011
• A 2001 study found that annual medical claims’ costs for peoplewith five or more health risks were double the costs of individualswho were healthier, that is, had two or fewer health risks.4
• The American workforce is aging, and it is projected that between2006 and 2016, the number of workers 55 to 64 years of age willincrease by 36.5%, while workers between 65 and 74 years of ageand older than 75 years will increase by 80%.5 By 2015, one inevery five workers will be 55 years of age or older.6
• Older workers typically suffer from chronic health conditions andhave multiple health risks. The chronic conditions most commonamong older age groups often require more care, are more dis-abling, and are more difficult and costly to treat than the chronicconditions that are more common in younger age groups.7
In addition to these trends, the percentage of women in theworkforce is increasing, and today, women comprise 46.8% of theworkforce.8 The distribution of nonfatal occupational injuries bysex varies by occupational sector. “In 2007, females accounted for68.4 percent of injuries occurring in management, professional, andrelated occupations, while making up 51.2 percent of the workforcein that sector. Similarly, females represented 56.4 percent of theservice workforce, but accounted for 61.1 percent of injuries in thatsector.”9
As the nation grapples with these trends, employers more andmore have begun to understand that as the health risks of the USpopulation increase, the disease burden on the workforce moves inparallel, and they recognize that this formula does not bode well forthe economic health of their companies.
Research has shown that common chronic conditions, suchas cancer, heart disease, and diabetes, are driving up total health-related costs in the workplace.10–12 Other health conditions amongworkers—ranging from musculoskeletal/pain and depression toobesity—are adding to those costs.13,14
In addition to a steadily rising medical and pharmaceuticalcost burden, employers are now also seeing evidence of significantproductivity–cost impacts related to poor health. Research is begin-ning to show a much greater connection between employee healthand productivity in the workplace than was ever realized in the past.
For example, studies have shown that on average for every onedollar spent on worker medical/pharmacy costs, employers absorbtwo to three dollars of health-related productivity costs.15 These costsare manifested largely in the form of presenteeism (a condition inwhich employees are on the job but not fully productive), absence,and disability. Compounding these issues for employers is the impactof safety issues and health-related environmental-hazard costs.
Statistics show that work-related accidents and injuries exertan enormous toll on employers. Accidents, overexertion, or injuriescaused by excessive lifting, carrying, or pushing, adds significantly toemployer costs–with an annual impact in the billions of dollars. TheNational Safety Council (NSC) has estimated that on-the-job injuriescost the United States more than $130 billion annually.16 Included inthis figure are wage and productivity losses of $68 billion, medicalcosts of $24 billion, and administrative costs of $22 billion.
In addition to these safety- and hazard-related injury costs,the effort of administering to the needs of injured workers is alsoextremely costly.17 The NSC estimates that employers spend wellmore than $10 billion in time lost for employees who were notinjured but involved in the reporting and investigation of injuries.16
The cost of protecting employees from environmental hazardsin the workplace is also substantial. While the overall cost of envi-ronmental regulation in the United States has been estimated to beroughly 2% of the gross domestic product, for some industries, itis particularly high.18 The costs associated with benzene protectionin coal factories or for arsenic protection in glass-manufacturingplants—both of which run in the millions of dollars per life-year–
are common examples of potential economic burdens as employersaddress environmental safety issues.
When all of these factors are added together, they spell outa difficult reality for the United States: the national pipeline ofhealthy, productive workers faces significant health-related chal-lenges. Moreover, the cost of responding to these workplace healthand safety issues has the potential to undermine America’s competi-tiveness in the global marketplace. More than ever before, the nationneeds to take steps to ensure the optimal health of its workforce.
DEFINING THE NEW “WORKPLACE”Amidst all of these megatrends, the very nature and definition
of the workplace are changing. The stationary-manufacturing andproduct-oriented workplaces of the past centuries have morphed intomuch-wider, all-encompassing virtual work environments that spanworkplace, home, and community, as technology enables workers tostay connected 24/7/365. This new environment makes it possibleto work anyplace, anytime. As employers fulfill the need to supplycustomers in a more efficient and timely manner, around-the-clockwork activity has increased, making not only where employees areworking but also when they work important elements in the new-ageworkforce.
As companies have downsized and right sized to meet the neweconomy, increasing numbers of contingent workers are used as staffin workplaces. These individuals may have numerous employers whomake up their annual income and, in many cases, may not have accessto health benefits. Twenty percent of wage-and-salary employees nowwork a shift other than a regular daytime shift, and many are workingextended hours or more than one job.19
DEFINING THE NEW “WORKFORCE”As noted, the workforce is aging. In addition, women are
entering the workforce in greater numbers.8
• In 1950, only one in every three women or 33.9% of all women(16 years of age or older) were in the labor force.
• By 2010, 59.2% of the 122 million women aged 16 years andolder participated in the labor force, either working or looking forwork.
• In 2010, women comprised 46.8% of the total workforce, up from45% in 1998.
• Unemployment among women is lower than for men. In 2009,only 8.1% of women were unemployed compared with 10.3% ofmen.8
The growing presence of women in the workforce is signifi-cant in that women traditionally make the health care decisions forthe family. Now that they are actively involved in the workplacein increasing numbers, this presents an opportunity for the imple-mentation of safety and health programs with the potential for abroad-ranging impact on the family.
Likewise people are working longer, resulting in an olderworkforce. According to the Bureau of Labor Statistics (BLS), be-tween 1970 and 2007, there was a 101% increase in workers age,that is, 65 years of age and older.20 During the same time span, totalemployment increased only 59%. For men older than 65 years, theincrease was 75%, but for women, the increase was 147%. The BLSprojects that between 2006 and 2016, the number of workers aged55 to 64 years will increase by 36.5%, while the number of workersbetween 65 and 74 years and older than 75 years will increase by80%.20
As previously mentioned, older workers suffer from morehealth risks and/or chronic medical conditions that are usually morecostly to treat. A 2003 Towers Perrin report indicated that the annualaggregate medical claims’ costs for employees and their dependentsbetween the ages of 25 and 29 years was $2148.21 This figure roseto $4130 for those between the ages of 40 and 44 years and to $7622
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
696 C© 2011 American College of Occupational and Environmental Medicine

JOEM Volume 53, Number 6, June 2011 Workplace Health Protection and Promotion
for employees between the ages of 60 and 64 years. As the workforceages, the medical and pharmacy costs of employers are projected torise.
THE PROFOUND IMPACT OF HEALTHIN THE WORKPLACE
In this new environment, where the pressure on both workersand employers is intense and where health costs are skyrocketingand chronic disease and safety and environmental hazards pose newthreats, health promotion and health protection measures aimed atthe nation’s workforce could have significant long-term impact, po-tentially saving billions in costs.
A growing body of research demonstrates the connection be-tween improved health and functional status, worker productivity,and lowered total costs.
• A 2007 study on health and productivity management programs,funded by the Association of State and Territorial Chronic DiseaseProgram Directors, National Association of Chronic Disease, con-cluded that well-designed health programs in the workplace couldachieve long-term health and productivity improvements in work-site populations.22
• A 2005 study demonstrated that individuals who reduced theirhealth risks generally saw an improvement in productivity,whereas those who increased their health risks or remained thesame showed decreased productivity.23
• A Harvard analysis of the literature on costs and savings associ-ated with prevention programs in the workplace found that medicalcosts were reduced by $3.27 and absenteeism costs were reducedby $2.73 for every $1.00 spent on comprehensive workplace well-ness and prevention programs.24
• Another study found that lowering obesity rates alone could lead toproductivity gains of $254 billion and avoidance of $60 billion intreatment expenditures.25 A recent study determined that employ-ers could achieve significant savings by reducing the prevalence ofobesity, particularly among those with a body mass index greaterthan 35.26
• A variety of return-on-investment studies have shown that forevery dollar invested in health promotion over a 3-year period,return-on-investment for employers ranges from $1.40 to $4.70.27
WHY WORKPLACE HEALTH IS ESSENTIAL TOHEALTH REFORM
These trends and statistics suggest that health is not onlyof great value to individuals and populations but also to businessand industry. Enlightened employers—whether small, medium, orlarge—are beginning to look beyond health care benefits as a costto be managed and instead are considering the benefits of goodhealth as an investment to be leveraged. This creates a scenario inwhich a proactive extension of a “culture of health and safety” intothe American workplace can provide a critical piece in the overallhealth-system reform puzzle.
The workplace offers unique resources and infrastructure foraddressing the health problems of the overall US population. Withmany adult Americans spending much of their active, waking hoursconnected in some way to the workplace, the sheer volume of individ-uals who can be reached through workplace health programs is vast.The CDC estimates that 65% of the adult population of the UnitedStates can be reached through worksites. Research indicates thatworksite health programs represent an ideal opportunity to have animpact on the health behaviors of working adults and their families.28
There are many other reasons why a new focus on health inthe workplace makes sense, including the following:
• Workplace programs can reach segments of the population whomay not have access to health information in other settings.
• Workplaces concentrate groups of people together who share com-mon purpose and culture.
• The work environment can be utilized to advocate for and provideaccess to healthy lifestyles.
• Communicating with workers is straightforward, due to preestab-lished and well-organized communication channels.
• Social and organizational supports are available in the workplace.• Organizational hierarchies make possible the introduction of pro-
cedures, practices, and norms.• The physical environment of the workplace can be used to af-
fect health behaviors (cafeteria/food selection, ergonomic officedesign, use of stairways and landscaping, etc).
• Financial and other incentives can be utilized in the workplace togain participation in programs.29
Studies show that health promotion activities in the workplacehave the capacity to influence both individuals and populations. Pub-lic health promotion—which has used social policy and engineeringinterventions along with health education to decrease dental caries,improve highway safety, and decrease smoking prevalence in theUnited States—can be very effectively applied in the workplace.
As one part of multicomponent initiatives to improve dietarybehavior, for example, several interventions have been found to beeffective in increasing healthy food choices. These include point-of-sale education and labeling30 and enriching and subsidizing healthfood choices available through cafeterias and vending machines.31,32
Worksite policies banning tobacco use at the workplace havealso gathered momentum in recent years and have added to over-all efforts to decrease smoking and limit exposure to second-handsmoke.33
Employee assistance programs aimed at reducing chemicaldependence among employees have been shown to result in signifi-cant long-term impacts.34,35
In short, the workplace can be considered a microcosm oflarger society and as such can provide an effective setting for address-ing both individual health and the health of populations. Programsin the workplace can reach and engage segments of the populationthat may not otherwise be exposed to health-improvement efforts.
TRADITIONAL SAFETY AND WELLNESS SILOS NOTOPTIMAL FOR WORKPLACE HEALTH
The evidence clearly shows that the health of the workforce isinextricably linked to the productivity of the workforce and the healthof the nation’s economy. It also shows that employers increasinglyrecognize this link and are interested in improving worker health byexpanding workforce health protection and health promotion pro-grams. Employers in recent decades have devoted more resourcesand attention to the subject. In one study, a majority reported thatthey have established some form of health promotion effort in theworkplace.36
But are these efforts sufficient to significantly impact work-force health nationally and to introduce a true culture of health andsafety in the workplace?
While the national recognition and embrace of programs forworkplace health protection and health promotion are clearly on therise, the 2004 National Worksite Health Promotion Survey found thatonly 6.9% of surveyed organizations met the criteria for comprehen-sive health programming for employees.37 This falls far short of the75% target that has been outlined in the federal government’s HealthyPeople Program.38 “Safety” and “wellness” are still in distinctsilos.
Few employers have created truly integrated programs, whichcomprehensively address both health promotion and health protec-tion in a systematic fashion. In the majority of workplaces, the “well-ness community” and the “safety community” are simply not con-necting; they operate far too independently.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2011 American College of Occupational and Environmental Medicine 697

Hymel et al JOEM Volume 53, Number 6, June 2011
The “safety” side of the equation—encompassing the ac-tivities that protect workers from occupational injury and illnessand promote a better work environment—is often housed in anorganizational sector that is completely separated from health andwellness. The “safety committee” in a mid-sized manufacturing com-pany may have no formal connection with the coordinator of thecompany’s wellness incentive program, housed in human resources,for example.
The “wellness” side of the equation—encompassing the ac-tivities that maintain or improve the personal health of a workforce—may be focused and engaged in the same company, with the benefitsplanning and implementation team, but be out of touch with core op-erations involving Occupational Safety and Health Administration(OSHA) regulations and safety impacts.
Why the disconnect? Some may view the occupational healthcommunity’s efforts at health promotion and disease prevention as adrain on resources that are needed for occupational health protectionactivities. Conversely, others may view health protection, safety, andenvironmental hazard efforts as overly isolated in achieving broadpopulation health goals.
As National Institute for Occupational Safety and Health(NIOSH) has noted, “The occupational health community has seenefforts at generic health promotion and disease prevention in theworkplace at best as drawing needed resources from occupationalhealth protection strategies, and at worst involving victim blamingand distracting attention from the occupational health needs of work-ers. There has been concern that a narrow focus on health promotionwill deflect employers from their legal responsibilities to provideworkplaces free of recognizable hazards.”39
Lessons can be learned from the health protection/safety focusof employers. Since the establishment of the OSHA on April 28,1971, the number of workplace fatalities, injuries, and illnesses hasdecreased. In 1970, approximately 14,000 workers were killed onthe job. By 2009, that number had fallen to approximately 4340 evenwhen the workforce doubled in size to more than 130 million workersat more than 7.2 million worksites. Since the establishment of OSHA,the rate of reported serious workplace injuries and illnesses declinedfrom 11 per 100 workers in 1972 to 3.6 per 100 workers in 2009.Clearly, companies have adopted a “Culture of Safety” and havemade vast improvements to the workplace to ensure a safe workforce.Today, if someone experiences a serious job-related injury, the siteusually shuts down and a root-cause analysis is completed before thecontinuation of work. However, if an overweight employee were tohave a heart attack on the job, work would continue uninterrupted.That same focus and “Culture of Safety” that companies adoptedover the last 40 years in response to workplace injury and illnessneed to be translated to a “Culture of Wellness,” focusing on theoverall health of employees.
MAKING THE CASE FOR INTEGRATINGWORKPLACE HEALTH PROTECTION AND HEALTH
PROMOTIONThe time has come to move these often-independent employer
health promotion and health protection activities to a new, more-effective level through integration. Increasingly, thought leaders inthe traditional sectors of wellness and safety are advancing the ques-tion: Could health improvements translate to safety improvements,safety improvements translate to health improvements, and the syn-ergies gained by integrating the two create significantly healthierworkplaces?
By better coordinating distinct environmental, health, andsafety policies and programs in the workplace into a continuumof activities, it is theorized that employers can substantially enhancethe overall health and well-being of the workforce while better pre-venting the work-related injuries and illnesses. In short, a healthier
workforce can be a safer workforce; a safer workforce can be ahealthier workforce.
This is an intuitive conclusion, which on its face seems logical.We know, for example, that employees can improve their muscularand cardiovascular response capabilities through exercise and nutri-tion programs; does it, therefore, follow that their ability to avoidinjury is enhanced via heightened fitness levels? Conversely, weknow that ergonomically oriented safety programs reduce injuries,for example, but do they also contribute to overall health gains forindividuals?
Evidence is beginning to point in these directions. Good phys-ical condition, absence of chronic illness, and good mental healthare the factors that have been scientifically observed to be associatedwith low occupational injury rates.40–42 It has been clearly shown,for example, that workers with certain adverse health risk factors aremore likely to sustain injuries than those without such risks. Amongthese factors are obesity, sleep deprivation, having poorly controlleddiabetes, being a smoker, abusing drugs and/or alcohol, or beingimpaired by certain prescription medications.40,43,44
This evidence is one of the driving factors behind the adoptionof more aggressive screening for the presence of numerous medicalconditions and illnesses in a variety of US Department of Transporta-tion examinations (eg, Federal Motor Carrier Safety Administration(FMCSA) medical examinations for commercial drivers and FederalAviation Administration (FAA) examinations for pilots.) Identifyingmedical conditions that impact safety has been proven effective inlowering accidents among commercial drivers and pilots.45,46
Researchers have found a statistically increased risk for acci-dental death in obese employees47 and have determined that hearingloss and poor eyesight are also associated with injuries at work.Crawford et al found that those who self-reported their hearing as“not good” were at increased the risk for an accident at work,48 whileChoi et al49 reported that workers with self-reported fair/poor hear-ing had a twofold risk for an injury at work. Girard et al50 foundsimilar relative risks in a retrospective study.
Zwerling et al51 reported that self-reported poor and fair visionincreases the risk of occupational injury by about 50%. Browninget al52 reported a similar association between self-reported problemsof vision and injuries at work.52
Many studies have found an increased risk for an occupationalinjury connected to fatigue, as well as a clear correlation betweenpoor sleep and the risk for an injury at work.53,54 One study reported atwofold risk for an injury at work in employees with sleep disorders.55
Several studies observed increased injury rates in employeesreporting conflicts at work, either with coworkers or with supervisors,and a much higher incidence of self-reported injuries in those whohad depressive symptoms.56–58
Costs associated with these various workplace health/safetyrisks have also been well documented. A University of Michi-gan study showed that 85% of workers’ compensation costs wereattributed to worker health status tied to risk assessment.59 In a2009 study conducted by Kuhnen et al,60 a comparison of low-riskhealth risk assessment (HRA) participants with high-risk participantsshowed that those with high risk were nearly 3 times more likely tofile a worker’s compensation (WC) claim, whereas medium-risk par-ticipants were 1.5 times more likely to file a short-term disabilityclaim.60
While there is ample evidence to indicate that wellness pro-motion affects safety, evidence proving that safety affects wellness isless readily available. We need to know much more about how safetyimpacts on wellness. That said, some current research does suggestan inherent connection.
A recent study of worker health programs at Navistar, for ex-ample, shows a strong cross-silo linkage between safety and healthresults in an integrated environment.61 After the creation of a com-prehensive, integrated health initiative that spanned both sides of
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
698 C© 2011 American College of Occupational and Environmental Medicine

JOEM Volume 53, Number 6, June 2011 Workplace Health Protection and Promotion
the health protection/health promotion spectrum, Navistar reportedsubstantial gains in both overall health and safety results. Injury in-cidence frequency rate dropped to 455 injuries in 2009 comparedwith 2446 injuries in 1998.62 Navistar’s both workers’ compensationcosts and hospital admission rate per employee dropped, and the com-pany achieved a 48% decrease in “controllable absences” (workplaceinjuries/illness).
Navistar’s experience bolsters the notion that implementationof comprehensive health protection and promotion activities can leadto a culture of health in the workplace. Other research is increasinglypointing to this broader connection. Emerging studies of the impactof the work environment on the health of workers are suggesting thatthe impact lies far beyond what has been traditionally categorized asoccupational health and illness. For example, shiftworkers are morelikely to eat poorly and suffer from obesity and diabetes.63 Femaleshiftworkers may be at a higher risk of breast cancer.64
Pioneering research by Laura Punnett of the University ofMassachusetts has suggested that a host of factors is related to mus-culoskeletal injuries in the workplace—ranging far beyond safety-oriented measures such as the mechanics of lifting, posture, etc, andencompassing such factors as socioeconomic status and lifestyle be-haviors. When these multivariate factors are addressed together, thepotential for overall health gains in employees is increased.65
Numerous studies of the impact of shiftwork have shownthat changes aimed at sleep deprivation as a safety issue have alsodemonstrated improvements on health conditions ranging from di-abetes and obesity to cardiovascular disease.66 But, perhaps, mostcompelling in establishing the link between safety and wellness are“sequencing” studies, indicating that participation by employees inwellness programs is less likely when such programs are introducedin workplaces with unaddressed safety issues.67 The research sug-gests that a firm foundation of solid safety efforts is necessary beforean organizational wellness effort can yield optimal results—a pow-erful argument for the integration of the safety and wellness silos. Acombination of safety and wellness appears to be necessary to movean organization forward in adopting a true culture of health.
Reflecting this evidence base, an increasing number of or-ganizations have, in recent years, developed initiatives and pro-duced guidance documents supporting the fundamental importanceof improving and maintaining health status as a bridge to improvingsafety results and integrating safety programs as a key foundationfor achieving overall health. In the United States, the American Col-lege of Occupational and Environmental Medicine (ACOEM), NSC,NIOSH, and others have begun to elevate this concept of integra-tion, as have international organizations, including the World HealthOrganization/International Labour Organization, the United King-dom’s National Health Service, and the European Union’s Safetyand Health at Work Strategy.
Common elements in the new integrative models include thefollowing:
• Building a “whole life” approach to health and safety, which com-bines both on-the-job and off-the-job dimensions in a unified vi-sion that leads to a true culture of health;
• Stressing the importance and connection of overall health andwellness to safety outcomes; and
• Recognizing the evolution in the nature of workplace hazards andincluding this awareness in the development of health strategies.
The NIOSH introduced its WorkLife Initiative in 2007 to bet-ter integrate employee health strategies,68 and the State of Californiathis year introduced a similar initiative with a guideline for employerstitled “The Whole Worker: Guidelines for Integrating OccupationalHealth and Safety with Workplace Wellness Programs.”69
The NIOSH and other organizations stress that continued im-provements in injury reductions are not just a reflection of excellence
in traditional safety areas, such as machine guarding, but also aredependent on improvements in personal health.
The National Aeronautics and Space Administration has alsoimplemented a widely studied paradigm of workforce health—onethat embraces a more holistic, cross-silo view of a “healthy work-force: Employers that have traditionally been responsible for safety,environmental, and occupational health concerns will, of necessity,become more involved with work life issues, health behaviors, andsocial interactions.”70
The National Aeronautics and Space Administration’s de-scription of its wellness and safety paradigm provides a strong modelfor integration, calling for an approach that “requires a service con-struct oriented toward human performance; a health model focusedon population, rather than on individual goals and objectives; and ameasurement system oriented toward health status and outcomes. Asystems approach rather than a programs approach better supportsthis paradigm because systems are constructed of linkages and seeksynergy. Systems operations require thinking, work processes, andresource utilization, which emphasize integration, collaboration, andoptimizing overall performance rather than stand-alone componentsor programs.”70
It is important to note that there may be a certain amount ofproductivity loss that cannot be recovered through health and safetyprograms. Recent research has identified the “normal impairmentfactor” (NIF)—an amount of productivity loss that is not attributableto health risks and therefore not available for “recapture,” usinghealth and productivity management programs.
StayWell Health Management and Riedel & Associates Con-sultants, Inc, established the NIF in 2009, and research demonstratedthat the NIF comprised 3.4% of all productivity loss or 1.8 weeks perperson per year. This finding was based on a sample of 772,750 em-ployees, representing 106 employers within five industry sectors.71
In a new study, the authors tested the original NIF against a groupof 577,186 employees completing the HealthMedia, Inc, health riskappraisal. Their NIF comprised 3.5% of all productivity loss.72
These studies demonstrate that two unique and very large em-ployee health risk appraisal databases identified normal impairmentfactors of 3.4% and 3.5%, respectively. This amount of nonhealthrisk-related productivity loss needs to be taken into consideration toaccurately quantify the amount of loss that is avoidable and there-fore can be impacted by integrated health protection and promotionprograms.
COMPLETING THE CONTINUUM: TAKING HEALTHPROTECTION AND PROMOTION HOME
The workplace is organically connected to the home and tothe physical communities in which workplaces exist. Health behav-iors extend across all three environments and cannot be artificiallyseparated. Just as factors in the workplace can affect health and well-being at home and in the community, exposures, activities, and otherelements outside the workplace can affect health and productivity onthe job.
In an important study, Seabury et al73 point out that it isbecoming increasingly difficult to distinguish individual behavior atand away from work. This makes it more difficult to draw the distinc-tion that individuals can only directly affect their own health throughtheir actions away from work, while employers only directly affectworker health through the workplace environment. As Cherniacket al74 put it: “Prevention of chronic disease factors, as well as ef-forts to maintain high function and effectiveness cannot be confinedto a 40-hour work week.”
The workplace environment can be utilized to stimulatehealthy lifestyle habits that can be carried over to the home envi-ronment. For example, encouraging employees to take the stairs (uptwo, down three), creating walking trails in and around the work-site, offering healthy snack options in vending machines and at
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2011 American College of Occupational and Environmental Medicine 699

Hymel et al JOEM Volume 53, Number 6, June 2011
meetings, providing access to on-site exercise facilities, and encour-aging stretch breaks, all these activities assist in establishing healthylifestyle behaviors.
Research of Punnett et al75 on multivariate factors inworkplace safety and injuries provides epidemiologic evidence,suggesting that there is not a clear dividing line between “work-related” and “non–work-related” injuries. The concepts of injuryand illness must be considered in a broader context.
Thus, it makes sense for an organized national effort promot-ing workforce health and protection to be coordinated with effortssuch as the emerging “medical home” concept, championed by theall primary care specialties, which envision a strong emphasis onpartnerships between patients and a medical team to achieve optimalhealth.
By logical extension, efforts aimed at integrating health pro-motion and health protection in the workplace can ultimately beconnected with the medical home, with the employer occupying arole as a member of an individual’s “health team” and medical com-munity.
The same argument can be made for connecting the workplacehealth protection and promotion concept with a variety of otherhealth system initiatives—ranging from the adoption of electronichealth records to national antismoking and nutritional awarenesscampaigns.
As a vital component in a three-legged stool composed ofworkplace, home, and community, workplace health protection andpromotion programs can then have an even greater impact on overallhealth care reform.
NIOSH is refocusing workplace health efforts on integra-tion across silos and sectors, notably connecting workplaces, homes,and communities through the funding of several academic Work-Life Centers of Excellence.74 Three WorkLife Centers of Excellencehave been created to support and expand multidisciplinary research,training, and education to stimulate the integration of workplacehealth protection and workplace health promotion. The Centers areas follows:
University of Iowa, Health Workforce, Center of Excellence,whose goals are as follows:• To implement, evaluate, and compare health protection/health
promotion models, including an intervention based around anintegrated worker safety/health promotion committee and anintervention using health counseling to integrate the delivery ofhealth protection and health promotion services in the publicsector.
• To establish a learning network of interactive partnerships withemployers; employee groups, including unions; and health or-ganizations.
• To serve as a state and national information, education, andpolicy resource on employee health programs.76
Center for the Promotion of Health in the New EnglandWorkplace—a consortium of the University of Massachusettsand the University of Connecticut. The Center’s research objec-tives are as follows:• To assess the value of the integration or coordination of health
protection and health promotion in the workplace.• To integrate two core public health areas (Occupational Health
and Safety and Health Promotion), linking primary preventionto the workplace and the workplace to primary prevention.
• To evaluate whether this strategy provides enhanced health ben-efits and/or greater cost-effectiveness.
• To evaluate opportunities and obstacles in the traditional publichealth infrastructure.77
Harvard School of Public Health Center for Work, Health,and Well-being—the goals of the center are as follows:
• To establish, facilitate, and maintain a collaborative networkof researchers interested and engaged in worker health acrossdiverse disciplines, including occupational health and safety,social/behavioral sciences, social epidemiology, industrial hy-giene, social policy, organizational change, medicine, nursing,economic analysis, and labor relations.
• To foster and expand collaborations with employers, laborunions, and intermediary organizations to help to shape the cen-ter’s directions and to influence the dialogue among these con-stituencies regarding the application of integrated approachesto worker health.
• To synthesize and apply lessons learned from prior research onthe integration of occupational safety and health and WHP.
• To initiate research in two high-priority employment sectors,health care, and construction, across several studies.
• To cultivate future transdisciplinary research initiatives throughstrategically planned pilot projects.
• To train future and practicing professionals with a stake in thehealth of working people on needed skills and methods forintegrating occupational safety and health and WHP.
• To disseminate best practices and programs for integrated effortsto key stakeholders.
• To contribute to national priorities and future research direc-tions aimed at furthering integrated approaches to worker healththrough collaborations with NIOSH as part of this cooperativeagreement.78
These Centers will be publishing the results of their research andadditional information may be found on their respective websites.
CONCLUSIONTraditionally, health protection and health promotion activi-
ties have operated independently in the workplace. Health protectionhas usually been viewed as encompassing the activities that protectworkers from occupational injury and illness—ranging from basicsafety training to the use of protective gear and safety-enhancingmodifications to equipment. Health promotion, by contrast, has usu-ally been viewed as encompassing the activities that maintain orimprove the personal health of a workforce—ranging from healthrisk assessments to wellness initiatives and immunizations.
The creation of workplace “silos” that place boundariesaround these activities has been a limiting factor in organizations’ability to develop truly integrated health initiatives, reducing theiroverall effectiveness. While we have made great strides in creating aculture of safety and health protection in the United States since theestablishment of OSHA 40 years ago and have made encouragingprogress in establishing a culture of wellness and health promotionin more recent decades, the two have yet to meet and merge into atrue “culture of health.”
A new way of approaching these two vital activity centers isneeded—one that will integrate them into a concept called “work-place health protection and promotion.” This is the path to creatinga sustainable culture of health.
Simply defined, workplace health protection and promotionis the strategic and systematic integration of distinct environmental,health, and safety policies and programs into a continuum of activi-ties that enhances the overall health and well-being of the workforceand prevents work-related injuries and illnesses.
Organizations, whether large or small, can engage in this newstrategy by systematically integrating their health promotion andsafety programs, policies, and processes. This includes implement-ing programs that recognize the interactions of safety, environment,and health; creating a climate in which employees believe that anorganization cares about their health and safety; building a culture inwhich a health and safety mindset becomes a “24/7” way of thinking;and promoting an off-the-job health and safety focus that becomes
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
700 C© 2011 American College of Occupational and Environmental Medicine

JOEM Volume 53, Number 6, June 2011 Workplace Health Protection and Promotion
as important as, and overlaps with, the on-the-job health and safetyfocus.
By extending this concept in this way—taking it beyond thewalls of the workplace and connecting it with other health promotioninitiatives in the home and community—workplace health protectionand promotion can contribute tangibly to a stronger overall nationalhealth care system and improved health outcomes for the populationin general.
While logic, anecdotal evidence and a growing body of re-search suggest that integration of health promotion and health pro-tection initiatives in the workplace can help to pave the way forimprovements in workforce health and productivity; more researchis needed to strengthen this hypothesis, particularly in measuring theimpact of safety programs on workforce wellness.
RECOMMENDATIONSTo advance the concept of integrated health protection and
promotion, the nation’s employers and policymakers should worktogether on a basic agenda for research and change, incorporatingseveral key action steps. These include the following:
1. A set of best practices in the integration of health protection andhealth promotion in the workplace should be gleaned from theinitial pilot programs referenced in this document.
2. Results of these pilot studies should be translated into practicalguides for nationwide implementation by employers. Dissemina-tion should occur through a variety of vehicles, including confer-ences, Web sites, seminars, and publications. An emphasis shouldbe placed on providing guidance for small- to medium-sized em-ployers.
3. Public policy options supporting integrated health protection andpromotion strategies should be developed and communicated, en-gaging key stakeholders, including federal and state lawmakers,employers and insurers, labor unions and pension funds, healthcare providers, and health and safety professionals and other or-ganizations.
4. Incentives at the federal, state, and local level should be ad-justed and implemented, encouraging employers to adopt inte-grated health protection and promotion strategies.
5. Government and private sector organizations and agencies shouldexpand research on the synergy between health protection andhealth promotion in the workplace. While some evidence existsto suggest the benefits that can be gained by better integrationof health promotion and health protection, much more targetedresearch is necessary. Specifically, more studies are needed thatare aimed explicitly at demonstrating the tie between specificwellness activities and safety or injury and illness reduction andproductivity. This can be accomplished through pilot programs inkey industry sectors to gauge the impact of workplace health andwellness programs on workplace safety through demonstrating adecrease in on the job injuries and illnesses.
6. An effort should be made to coordinate a strategy of health pro-tection and promotion in the workplace with other national healthcare initiatives, including the growth of evidence-based medicine.Functional research and metrics from the workplace should beintegrated with clinical, evidence-based outcomes to create newstandards for determining the value and impact of workplace pro-grams.
7. Systems for measuring the effectiveness of combined health pro-tection and promotion programs should be standardized so thatthey can be readily utilized across industries/employers. A broadsweep of key metrics should be incorporated, including functionalstatus, cost impact, patient satisfaction, and clinical outcomes.
8. Funding for the NIOSH WorkLife Center of Excellence programshould be extended to every region of the United States; all cen-ters should be fully funded to allow continued development of a
comprehensive research, translation, and outreach program to allemployment sectors.
A Committee of the Health and ProductivitySection of ACOEM developed this document
REFERENCES1. Thorpe KE. Factors accounting for the rise in health care spending in the
United States: the role of rising disease prevalence and treatment intensity.Public Health. 2006;20:1002–1007.
2. Chronic Conditions: Making the Case for Ongoing Care. September 2004Update to Chronic Care in America: A 21st Century Challenge, a Study ofthe Robert Wood Johnson Foundation & Partnership for Solutions. Baltimore,MD: Johns Hopkins University; 2004.
3. Centers for Disease Control and Prevention. Vital Signs: State-SpecificObesity Prevalence Among Adults–United States, 2009 Weekly. MMWR.2010;59(30): 951–955.
4. Edington DW. Emerging research: a view from one research center. Am JHealth Promo. 2001;15:341–349.
5. Bureau of Labor Statistics. Older workers. July 2008. www.bls.gov/spotlight/2008/older-workers/. Accessed February 11, 2011.
6. Selden B. The Aging Workforce—A Disappearing Asset? Management is-sues. March 21, 2008. www.management-issues.com/2008/3/21/opinion/the-aging-workforce-a-disappearing-asset.asp. Accessed February 11, 2011.
7. Summer L, O’Neill G, Shirey L. Chronic conditions: a challenge for the 21stcentury. National Academy on an Aging Society. Monograph; 1999;1:1.
8. Bureau of Labor Statistics. Quick stats on women workers, 2009.www.dol.gov/wb/stats/main.htm. Accessed February 11, 2011.
9. US Department of Health and Human Services/Health Resources and Ser-vices Administration.Women’s Health USA, 2009. Rockville, Maryland: USDepartment of Health and Human Services; 2009:45.
10. Collins JJ, Baase C, Sharda C, et al. The assessment of chronic health condi-tions on work performance, absence, and total economic impact for employers.J Occup Environ Med. 2005;47:547–557.
11. Thorpe KE. The rise in health care spending and what to do about it. HealthAff. 2005;24:1436–1445.
12. Loeppke R, Taitel M, Richling D, et al. Health and productivity as a businessstrategy. J Occup Environ Med. 2007;49:712–721.
13. Henke RM, Carls GS, Short ME, et al. The relationship between health risksand health and productivity costs among employees at pepsi bottling group.J Occup Environ Med. 2010;52:519–527.
14. Curkendall S, Ruiz KM, Joish V, Mark TL. Productivity losses amongtreated depressed patients relative to health controls. J Occup Environ Med.2010;52:125–130.
15. Loeppke R, Taitel M, Haufle V, Parry T, Kessler R, Jinnett K. Health andproductivity as a business strategy: a multi-employer study. J Occup EnvironMed. 2009;51:411–428.
16. National Safety Council. Injury Facts, 2001 Edition. Itaska, IL: NationalSafety Council; 2001.
17. Wright DW, Beard MJ, Edington DW. Association of health risks with thecost of time away from work. J Occup Environ Med. 2002;44:1126–1134.
18. Pfizer WA, Kopp R. Calculating the Cost of Environmental Regulation.Washington, DC: Resources for the Future; 2003.
19. Cummings KJ, Kreiss K. Contingent workers and contingent health. JAMA.2008;299:448–450.
20. US Bureau of Labor. Statistics spotlight highlights trends toward more olderworkers. July 2008. www.agingworkforcenews.com/2008/07/us-bureau-of-labor-statistics-spotlight.html. Accessed February 11, 2011.
21. Feinsod RR, Davenport TO. The Aging Workforce: Challenge or Opportunity?Scottsdale, Arizona: WorldatWork; 2006: 1–23.
22. Goetzel RZ, Shecter D, Ozminkowski RJ, Marmett PF, Tabrizi MJ, Roe-mer EC. Promising practices in employer health and productivity manage-ment efforts: findings from a benchmarking study. J Occup Environ Med.2007;49:111–130.
23. Burton WN, Chen CY, Conti DJ, Schultz AB, Pransky G, Edington DW.The association of health risks with on-the-job productivity. J Occup EnvironMed. 2005;47:769–777.
24. Baicker K, Cutler D, Song Z. Workplace wellness programs can generatesavings. Health Aff. 2010;29:1–8.
25. Devol R, Bedroussian A, Charuworn A, et al. An Unhealthy America: TheEconomic Burden of Chronic Disease. Charting a New Course to Save Livesand Increase Productivity and Economic Growth. Santa Monica, California:Milken Institute; 2007.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2011 American College of Occupational and Environmental Medicine 701

Hymel et al JOEM Volume 53, Number 6, June 2011
26. Finkelstein EA, DiBonaventura M, Burgess SM, Hale BC. The Costs ofobesity in the workplace. J Occup Environ Med. 2010;52:971–976.
27. Goetzel RZ, Juday TR, Ozminkowski RJ. What’s the ROI? a systematic re-view of return-on-investment studies of corporate health and productivitymanagement initiatives. AWHP’s Worksite Health. 1999;6:12–21.
28. Schorder SA. We can do better: improving the health of the American people.N Engl J Med. 2007;357:1221–1228.
29. Goetzel RZ, Roemer EC, Liss-Levinson RC, Samoly DK. Workplace HealthPromotion: Policy Recommendations that Encourage Employers to SupportHealth Improvement Programs for Their Workers. Washington, DC: Partner-ship for Prevention; 2008.
30. Sutherland LA, Kaley LA, Fischer L. Guiding stars: the effect of a nutritionnavigation program on consumer purchases at the supermarket. Am J ClinNutr. 2010;91:1090S–1094S.
31. French SA, Hannan PJ, Harnack LJ, Mitchell NR, Toomey TL, Gerlach A.Pricing and availability intervention in vending machines at four bus garages.J Occup Environ Med. 2010;52:S29–S33.
32. Lemon SC, Pratt CA. Worksite environmental interventions for obesity con-trol: an overview. J Occup Environ Med. 2010;52:S1–S3.
33. Breslow L, Cengage G.Workplace Smoking Policies and Programs. En-cyclopedia of Public Health. 2002. eNotes.com. 2006. http//www.enotes.com/public-health-encyclopedia/workplace-smoking-policies-programs.Accessed February 24, 2011.
34. Hartwell TD, Steele P, French MT, Potter FJ, Rodman NF, Zarkin GA.Aiding troubled employees: the prevalence, cost, and characteristics of em-ployee assistance programs in the United States. Am J Public Health. 1996;86:804–808.
35. French MT, Zarkin GA, Bray JW, Hartwell TD. Costs of employee assistanceprograms: findings from a national survey. Am J Health Promot. 1997;11:219–222.
36. Testimony of Cathy Baase, MD, before the Senate Committee on Health,Education, Labor and Pensions; 2009:23.
37. Linnan L, Bowling M, Childress J, et al. Results of the 2004 National WorksiteHealth Promotion Survey. Am J Public Health. 2008;98:1–7.
38. US Department of Health and Human Services. Healthy People 2010. 2nded. With Understanding and Improving Health and Objectives for ImprovingHealth (2 vols). Washington, DC: US Government Printing Office; 2000.
39. National Institute for Occupational Safety and Health. www.cdc.gov/niosh/worklife. Accessed October 2010.
40. Ostbye T, Dement JM, Krause KM. Obesity and workers’ compensation. ArchIntern Med. 2007;167:766–773.
41. Maniscalco P, Lane R, Welke M, Mitchell JH, Husting L. Decreased rate ofback injuries through a wellness program for offshore petroleum employees.J Occup Environ Med. 1999;41:813–820.
42. Musich S, Napler D, Edington DW. The association of health risks withworkers’ compensation costs. J Occup Environ Med. 2001;43:534–541.
43. Bedno SA, Li Y, Cowan DN, Neibuhr DW. Increased Risk of Heat IllnessAmong Male U.S. Army Recruits Exceeding Body Fat Standards. Silver Spring,Maryland: Department of Epidemiology, Walter Reed Army Institute of Re-search. 2003.
44. Trogdon JG, Finkelstein EA, Hylands T, Dellea PS, Kamal-Bahl SJ. Indirectcosts of obesity: a review of the current literature. Obes Rev. 2008;9:489–500.
45. Parks PD, Durand G, Tsismenakis AJ, Vela-Bueno A, Kales SN. Screeningfor obstructive sleep apnea during commercial driver examinations. J OccupEnviron Med. 2009;51:275–282.
46. Howard ME, Desai AV, Grunstein RR, et al. Sleepiness, sleep-disorderedbreathing, and accident risk factors in commercial vehicle drivers. Am JRespir Crit Care Med. 2004;170:1014–1021.
47. Tsai SP, Donnelly RP, Wendt JK. Obesity and mortality in a prospective studyof a middle-aged industrial population. J Occup Environ Med. 2006;48:22–27.
48. Crawford JM, Wilkins JR III, Mitchell GL, Moeschberger ML, Bean TL,Jones LA. A cross-sectional case control study of work-related injuries amongohio farmers. Am J Ind Med. 1998;34:588–599.
49. Choi SW, Peek-Asa C, Sprince NL, et al. Hearing loss as a risk factor foragricultural injuries. Am J Ind Med. 2005;48:293–301.
50. Girard SA, Picard M, Davis AC, et al. Multiple work-related accidents:tracing the role of hearing status and noise exposure. Occup Environ Med.2009;66:319–324.
51. Zwerling C, Sprince NL, Wallace RB, Davis CS, Whitten PS, Heeringa SG.Risk factors for occupational injuries among older workers: an analysis of thehealth and retirement study. Am J Public Health. 1996;86:1306–1309.
52. Browning SR, Truszczynska H, Reed D, McKnight RH. Agricultural injuriesamong older Kentucky farmers: the farm family health and hazard surveillancestudy. Am J Ind Med. 1998;33:341–353.
53. Ott MG, Oberlinner C, Lang S, et al. Health and safety protection for chemicalindustry employees in a rotating shift system: program design and acute injuryand illness experience at work. J Occup Environ Med. 2009;51:221–231.
54. Burch JB, Yost MG, Johnson W, Allen E. Melatonin, sleep and shift workadaptation. J Occup Environ Med. 2005;47:893–901.
55. Chau N, Mur JM, Benamghar L, et al. Relationships between certain individ-ual characteristics and occupational injuries for various jobs in the construc-tion industry: a case-control study. Am J Ind Med. 2004;45:84–92.
56. Swaen GM, van Amelsvoort LP, Bultmann U, Slangen JJ, Kant IJ. Psychoso-cial work characteristics as risk factors for being injured in an occupationalaccident. J Occup Environ Med. 2004;46:521–527.
57. Kim HC, Park SG, Min KB, Yoon KJ. Depressive symptoms and self-reportedoccupational injury in small and medium-sized companies. Int Arch OccupEnviron Health. 2009;82:715–721.
58. Beseler CL, Stallones L. Safety knowledge, safety behaviors, depression, andinjuries in Colorado farm residents. Am J Ind Med. 2010;53:47–54.
59. Musich S, Napier D, Edington DW. The association of health risks withworkers’ compensation costs. J Occup Environ Med. 2001;43:534–541.
60. Kuhnen AE, Burch SP, Shenolikar RA, Joy KA. Employee health and fre-quency of workers’ compensation and disability claims. J Occup EnvironMed. 2009;51:1041–1048.
61. Bunn WB, Stave GM, Allen H, Naim AB. Evidence-based benefit design:toward a sustainable health care future for employers. J Occup Environ Med.2010;52:951–955.
62. Bunn WB, Stave GM, Allen GM, Naim AB. How to align evidence-basedbenefit design with the employer bottom-line: a case study. J Occup EnvironMed. 2010;52:956–963.
63. Suwazono Y, Sakata K, Okubo Y, et al. Long-term longitudinal stud on therelationship between alternating shift work and the onset of diabetes in maleJapanese workers. J Occup Environ Med. 2006;48:455–461.
64. Reed VA. Shift work, light at night and the risk of breast cancer. AAOHN J.2011;59:1–9.
65. Punnett L, Wegman DH. Work-related musculoskeletal disorders: theepidemiologic evidence and the debate. J Electromyography Kinesiol.2004;14:13–23.
66. DeMoss C, McGrail M, Haus E, Crain AL, Asche SE. Health and perfor-mance factors in health care shift workers. J Occup Environ Med. 2004;46:1278–1281.
67. Sorensen G, Barbeau E, Hunt MK, Emmons K. Reducing social disparitiesin tobacco use: a social contextual model for reducing tobacco use amongblue-collar workers. Am J Public Health. 2004;94:230–239.
68. National Institute for Occupational Safety and Health. Steps to ahealthier US Workforce initiative; history of the worklife initia-tive. www.cdc.gov/niosh/worklife/steps/default.html. Accessed October 15,2010.
69. The Whole Worker: Guidelines for Integrating Occupational Health and Safetywith Workplace Wellness Programs. Oakland, CA: Commission on Health andSafety and Workers’ Compensation; 2010.
70. Workforce Health, Performance, Readiness, Resilience. Integrating EmployeeHealth: A Model Program for NASA, Institute of Medicine. Washington, DC:National Academies Press; 2005.
71. Reidel JE, Grossmeier J, Haglund-Howieson L, Buraglio C, Anderson DR,Terry PE. Use of a normal impairment factor in quantifying avoidableproductivity loss because of poor health. J Occup Environ Med. 2009;51:283–295.
72. Lenneman J, Schwartz S, Giuseffi DL, Wang C. Productivity and health: anapplication of three perspectives to measuring productivity. J Occup EnvironMed. 2011;53:55–61.
73. Seabury SA, Lakdawalla D, Reville RT. The Economics of Integrating In-jury and Illness Prevention and Health Promotion Programs. Santa Monica,California: RAND Institute for Civil Justice; 2005.
74. Cherniack M, Henning R, Merchant JA, Punnett L, Sorenson G, WagnerG. Statement on national worklife priorities. Am J Indus Med. 2011;54:10–20.
75. Punnett L, Cherniack M, Henning R, Morse T, Faghri P. A conceptualframework for integrating workplace health promotion and occupational er-gonomics programs. Public Health Reports. 2009;124:16–25.
76. University of Iowa Center of Excellence. www.public-health.uiowa.edu/hwce/. Accessed February 11, 2011.
77. Center for the Promotion of Health in the New England Workplace.www.uml.edu/centers/cph-new/. Accessed February 11, 2011.
78. Harvard School of Public Health Center for Work, Health and Well-being. http://centerforworkhealth.sph.harvard.edu. Accessed February 11,2011.
Copyright © 2011 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
702 C© 2011 American College of Occupational and Environmental Medicine