cranial nerves i-vi “on old olympus towering tops a…” andrea gianniny eden treadway
TRANSCRIPT
CRANIAL NERVES I-VI
“On Old Olympus Towering Tops A…”
Andrea GianninyEden Treadway
Brief ReviewCNs : from brain pass through
foramina magnum of skullI-XII from ascending – descending CNs 1 & II attach to forebrain
◦I- telencephalon◦II- diencephalon◦Other 10 to brainstem
Primarily serve head/neck structures◦Vagus (X) extends to abdomen

Number Name Sensory/Motor/Both
I Olfactory On Some
II Optic Old Say
III Oculomotor Olympus Money
IV Trochlear Towering Matters
V Trigeminal Tops But
VI Abducens A My
VII Facial Finn Brother
VIII Auditory And Says
IX Glossopharyngeal
German Big
X Vagus Viewed Brains
XI Spinal Accessory
Some Matter
XII Hypoglossal Hops Most


I - OlfactorySensory nerve of smellFunction: transduce odor molecules
◦Cortical olfactory regions: responsible for olfactory awareness and
◦Limbic olfactory connections: responsible for integrating smell with emotions
◦Connections with hypothalamus play role in feeding behavior.
Formed by unmyelinated axons, terminates into two olfactory bulbs located in the inferior surface of the frontal lobe
Clinical Conditions - IDamage: deviations in ability to
smell◦Anosmia/hyposmia- Reduction or loss
of ability to smell◦Hyperosmia- Abnormally acute
sensation of smell
II - OpticSensory nerve of visionOptic nerve endings
receive light energy in theform of nerve potentials produced by photoreceptor cells in the retina.
Path: axons of the Optic Nerve travel until the optic chiasm and then as the optic tract. The optic tract then terminates in the Lateral Geniculate Body of the thalamus. There, the optic radiations travel to primary visual cortex.
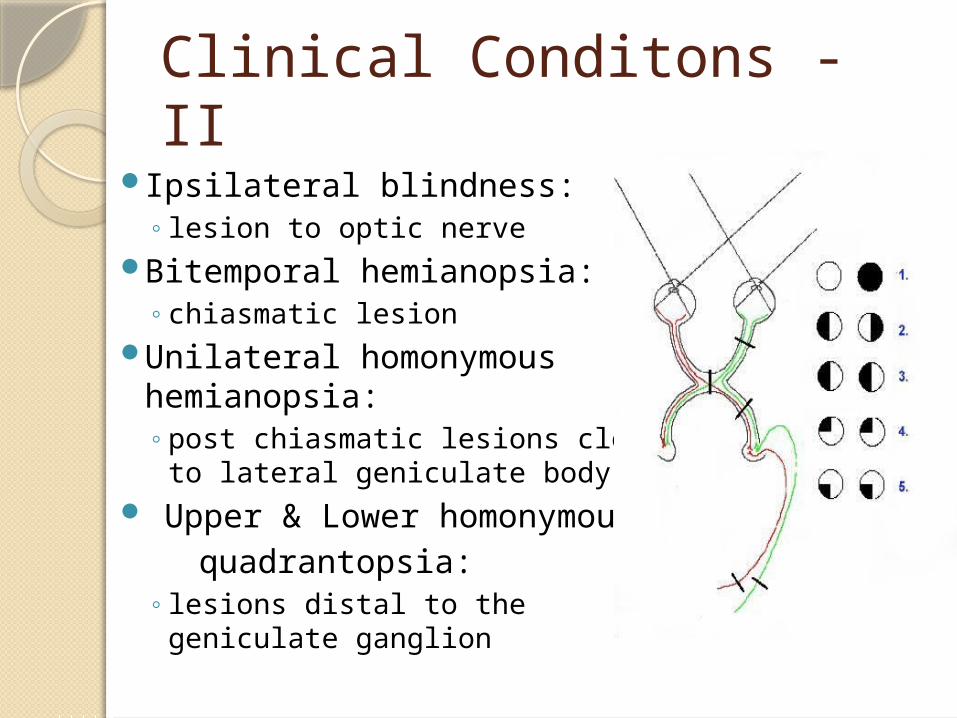
Clinical Conditons - IIIpsilateral blindness:
◦ lesion to optic nerveBitemporal hemianopsia:
◦ chiasmatic lesionUnilateral homonymous
hemianopsia: ◦ post chiasmatic lesions close
to lateral geniculate body Upper & Lower homonymous quadrantopsia:
◦ lesions distal to thegeniculate ganglion

III - OculomotorMotor nerveInnervates four of six extrinsic eye musclesForm & Function: composed of two components
◦ Somatic: Innervates the four extrinsic eye muscles & levator superioris, which is responsible for movement of eye lids.
◦ Visceral: innervates the intrinsic ocular eye muscles and controls parasympathetic functions including light reflex (constriction of pupils) and accommodation-convergence (modification of lens for near vision)
CN III is one of only four CNs that are involved in parasympathetic functions (along with VII, IX, and X)

Clinical Conditions - IIIExternal Opthalamoplegia:
Paralysis of extrinsic eye muscles and levator superiorsis.◦Lateral Striabismus: deviation of ipsi
eye to the lateral side May result in diplopia (double vision)
◦Ptosis: eye lid drooping Internal Opthalamoplegia:
Paralysis of intrinsic muscles ◦Mydriasis: permanent dilation of pupil
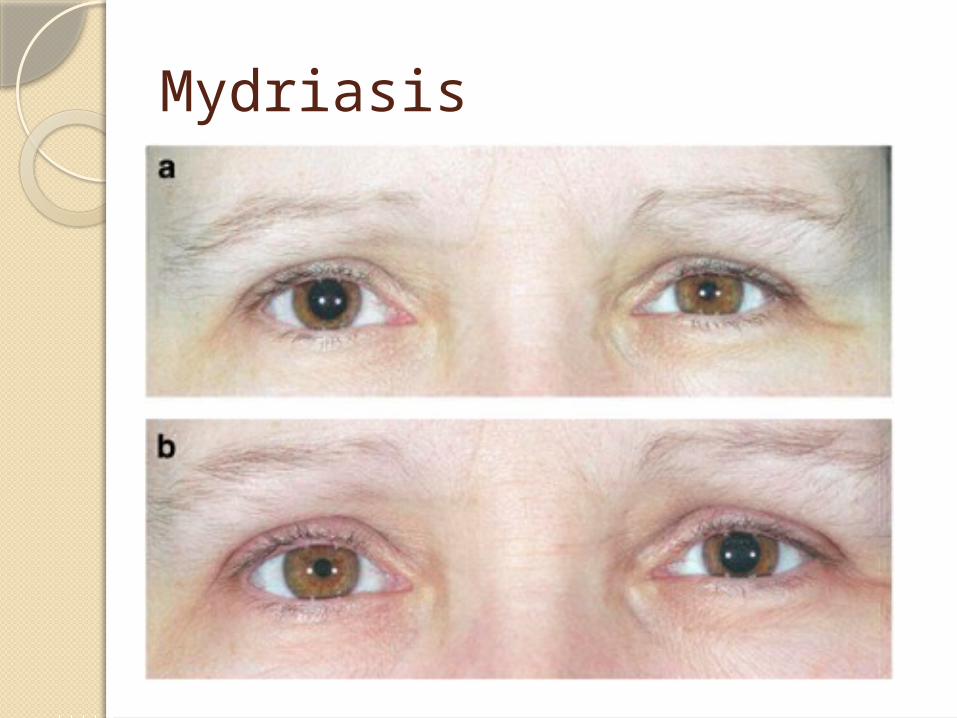
Mydriasis

IV - TrochlearMotorEye muscle movement (III, IV, & VI)Innervation: extrinsic muscle
◦Superior oblique Action: abducts and depresses
eyeball◦Moves eye outward and down
Only CN that exits posterior side of brainstem

Clinical Conditions - IVDamage: difficulty looking down
and outAlso, eye fixed in upward, medial
gaze

VI - AbducensMotorInnervation: extrinsic eye muscle
◦Lateral rectusAction: abducts eyeball horizontallyRuns long intracranial course therefore
more susceptible to damage

Clinical Conditions - VIDamage: medial strisbismus (because
medial rectus [CN III] is unopposed) which in turn may cause diplopia◦Medial strasbismus: affected eye turns
medially◦Diplopia: double vision
Medial Longitudinal Fasciculus – brainstem tract that helps communication between CNs III, IV, & VI and vestibular system and neck muscles◦Coordinates eye muscles for gaze control
and head position with eye movements doll’s eye reflex
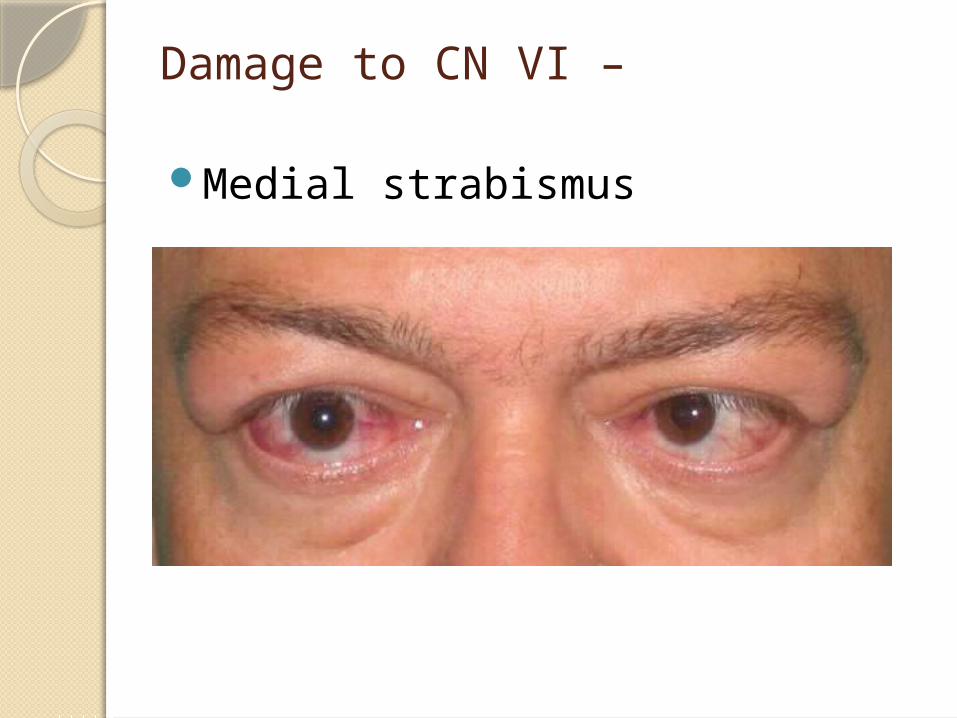
Damage to CN VI –
Medial strabismus
V - TrigeminalLargest CNMixedSensory innervation: from faceMotor innervation: to chewing
muscles◦Sensory & motor components for Jaw Jerk
Reflex - lesion causes exaggerated reflex3 branches (tri)
◦V1. Opthalamic nerve (sensory)◦V2. Maxillary nerve (sensory)◦V3. Mandibular nerve (sensory and motor)


V – Trigeminal (cont.)Action:
◦Sensory: cutaneous (touch, pain, temperature) and… proprioceptive (awareness of relative muscle
movement) sensations from the: face, head, oral and nasal cavities Sinuses and teeth Anterior 1/3 of tongue Anterior half of pinna, external auditory meatus, and
external surface of TM
◦Motor: controls muscles of mastication (chewing) and speech production, tensor veli palatini (soft palate) and tensor tympani (middle ear muscle) CN V: controls muscles involved in chewing but NOT
facial expressions

V – Trigeminal (cont.)Mandibular nerve: only carries
general sensory sensations from mouth, NOT taste ◦(e.g. touch/position,
pain/temperature)◦Taste fibers from anterior 2/3 of
tongue carried by lingual nerve then chorda tympani (branch of CN VII)
◦Taste fibers from posterior 1/3 and pharynx carried by branches of CNs VII, IX, and X
Clinical Testing - VSensory: lightly touch parts of pt’s
face with cotton or blunt object◦Check for sneezing reflex and corneal
reflex (blink in response to touching cornea)
◦Jaw Jerk ReflexMotor: check masseter muscle by
asking pt to bite down hard◦Ask pt to open mouth against
resistance at base of chin

Clinical Conditions - VDamage to Sensory portion:
◦Ipsilateral loss of sensation ◦Loss of sneezing and blinking
reflexes◦Trigeminal Neuralgia
Sudden intense pain in eyes, lips, nose, scalp, forehead, and jaw
Nerve severing in rare cases to treat

Clinical Conditions - VDamage to Motor portion:
◦Ipsilateral muscles of mastication paralyzed
◦Absent Jaw Jerk reflex, muscle tics/twitching
◦Dysarthria – paralyzed mandible and soft palate cause misarticulations

Clinical Conditions - VWallenberg Syndrome:
◦Believed to be stroke involving Posterior Inferior Cerebellar Artery [PICA]
◦Loss of pain/temperature sensation from Ipsilateral (same) side of face Contralateral (opposite) side of body
◦Reason: the ascending spinothalamic tract in the medulla carries pain/temp info from contralateral side of body is adjacent to descending tract of CN V which carries pain/temp info from ipsilateral side of face A stroke cutting off blood supply in this area
(e.g. clot in PICA) destroys both tracts

Questions!
1. At what point do the CNs pass through the skull?
a. medullab. jugular foraminac. foramina magnumd. brainstem
10 of the 12 CNs originate where?
a. diencephalon b. brainstem c. cerebellum d. medulla

Of the first 6 cranial nerves, which is the only mixed nerve?
a. Trochlear b. Oculomotorc. Abducensd. Trigeminal

Which cranial nerve exits the brainstem posteriorly?
a. Vagus
b. Trochlear c. Trigeminal d. Spinal Accessory

This cranial nerve innervates an extrinsic eye muscle (superior oblique) and is responsible for abducting and depressing the eyeball.
a. CN II b.CN III c. CN IV d. CN VI

This cranial nerve innervates an extrinsic eye muscle (lateral rectus) and is responsible for abducting the eyeball horizontally.
a. CN II b. CN III c. CN IV d. CN VI

Damage to the Abducens nerve (VI) will result in what kind of damage?
a. medial strabismus b. lateral strabismus c. Wallenberg Syndrome d. hemianopsia (blindness in half of
visual field)

is an important tract in the brainstem that facilitates communication between CNs III, IV, and VI as well as the vestibular system and neck muscles. This tract also coordinates muscles for the doll’s eye reflex.
a. Medial Longitudinal Fasciculus b. Spinothalamic tract in medulla c. Pyramidal tract d. Lateral Corticospinal Tract

The largest cranial nerve is .
a. CN IV b. CN V c. CN X d. CN XII

CN controls muscles of mastication as well as the tensor veli palatini and tensor tympani muscles involved in speech production.
a. CN X
b. CN VII c. CN V d. CN VI

A rare condition with symptoms of intense pain in a patient’s face (eyes, lips, nose, jaw, etc.) is known as .
a. PICA b. Occipital Neuraligia c. Wallenberg Syndrome d. Trigeminal Neuralgia

What branch of the Trigeminal nerve accounts for its motor functions?
a. Opthalamic b. Mandibular c. Maxillary d. Facial

Wallenberg Syndrome is a condition characterized by loss of pain/temperature sensation from the
side of the body and the side of the face.
a. ipsiliateral; contralateral b. ipsiliateral; ipsilateral c. contralateral; contralateral d. contralateral; ipsilateral

The sensory portion of this cranial nerve carries cutaneous and proprioceptive sensations from the anterior 1/3 of the tongue and the anterior half of the pinna, external auditory meatus, and external surface of the TM.
a. CN V b. CN VII c. CN IX d. CN IV

A condition that causes a reduction or loss of the ability to smell is known as _____________.
a. Hyperosmia b. Neuralgia c. Anosmia d. Wallenberg Syndrome

CN ___ innervates four of the six extrinsic eye muscles.
a. CN VI b. CN II c. CN III d. CN IV

A lesion to CN ____ can cause ipsilateral blindness.
a. CN I b. CN II c. CN III d. CN IV

Sensory endings of CN ____ are responsible for responding to noxious sensations, such as those associated with mace spray, onions, and mustard oil.
a. CN V b. CN IV c. CN II d. CN I

Connections of Cranial Nerve ___ with the hypothalamus play an important role in feeding behavior.
a. CN III b. CN II c. CN IV d. CN I

The visceral portion of CN ____ controls parasympathetic functions such as light reflex and accommodation-convergence reflex.
a. CN IV b. CN III c. CN I d. CN II

Which of the following nerves do NOT serve parasympathetic functions of the autonomic system?
a. CN III b. CN IX c. CN II d. CN VII

Paralysis of the extrinsic eye muscles and levator superiorsis is known as ____________________.
a. External Opthalamoplegia b. Internal Opthalamoplegia c. External Neuralgia d. Internal Neuralgia

All of the following are Motor or Mixed nerves EXCEPT:
a. CN III b. CN IV c. CN II d. CN V

Lateral striabismus caused from a lesion to CN III can cause double vision, which is formally known as:
a. Mydriasis b. Bitemporal hemianopsia c. Ipsilateral blindness d. Diplopia

Where are the two olfactory bulbs, where CN I terminates, located?
a. Superior surface of Temporal lobe
b. Inferior surface of Frontal lobe
c. Inferior surface of Occipital lobe
d. Superior surface of Occipital lobe