cprblt an tpthlt n th n nd clftn f n sptd f pr n mlila.ilsl.br/pdfs/v54n4a15.pdf · cprblt an...
TRANSCRIPT
volume 54, Number 4Printed in the U.S.A.
INTERNATIONAL JOURNAL OF LEPROSY
Comparability Among Histopathologists in theDiagnosis and Classification of Lesions
Suspected of Leprosy in Malawi'Paul E. M. Fine, Charles K. Job, A. Colin McDougall,
Wayne M. Meyers, and Jorg M. Ponnighaus2
It may be said that difficulties in diag-nosing leprosy before the onset of typicalperipheral nerve damage are widely recog-nized but rarely admitted—widely recog-nized insofar as leprologists have experi-enced and often discuss difficulties inconcluding whether one or another lesion isindeed attributable to Mycobacterium lep-roe; rarely admitted insofar as most publi-cations end up grouping people as either"cases" or "non-cases" with no reference toany uncertainty in deciding upon the diag-nosis. Textbooks speak of the cardinal signsof leprosy (anesthesia, thickened nerves, skinlesions, acid-fast bacilli—by convention atleast two of the first three, or the fourth,should be present for the diagnosis to bemade '), but the assessment of the first threeof these signs can be difficult, in particularunder field conditions. In the face of thesedifficulties, histopathology has been calledupon increasingly in recent years to ,assistin the diagnosis as well as the classificationof leprosy. The reliance upon histology isparticularly evident in research. A consid-erable proportion of current publicationsclaim that cases under study were histolog-ically "confirmed." Reference to the clas-sification of cases according to histopatho-logical criteria defined by Ridley and Jopling
' Received for publication on 27 March 1986; ac-cepted for publication in revised form on 13 June 1986.
2 P. E. M. Fine, V.M.D., Ph.D., School of Hygieneand Tropical Medicine, Keppel Street, London WC17HT, England. C. K. Job, M.D., F.R.C.Path., F.A.M.S.,Chief, Pathology Research Department, National Han-sen's Disease Center, Carville, Louisiana 70721, U.S.A.A. C. McDougall, M.D., F.R.C.P., Consultant in Clin-ical Research (Leprosy), The Slade Hospital, Oxford0X3 7JH, England. W. M. Meyers, M.D., Ph.D., Chief,Division of Microbiology, Armed Forces Institute ofPathology, Washington, D.C. 20306-6000, U.S.A. J.M. Ponnighaus, Dr.Med., D.T.P.H., Director, LepraEvaluation Project, P.O. Box 46, Chilumba, KarongaDistrict, Malawi.
(10) is now almost universal in leprosy re-search.
Despite the widespread acceptance ofhistopathological evidence in leprosy, therehave been few critical evaluations of thevalidity of this method in the hands of dif-ferent investigators. There are a small num-ber of published studies on the relationshipbetween clinical and histopathological find-ings, particularly with regard to classifica-tion, but none of these was designed as aformal independent comparison (5. 7' 12' 13' 15).
We are aware of no studies comparing theopinions of different histopathologists in thediagnosis of leprosy.
Given the difficulty and importance ofarriving at a diagnosis of leprosy, this ab-sence of critical studies is surprising. Itcontrasts with a growing literature on thecritical evaluation of histopathological as-sessment of other diseases, in particularcancers (2, 1, 4, 8, II. I4‘,) which has developedmethods for measuring and improving va-lidity and comparability between diagnos-ing histopathologists.
Among the outstanding questions con-cerning the histopathological diagnosis andclassification of leprosy are the following: a)To what extent do histopathologists agreeand/or experience difficulties in arriving ata diagnosis of leprosy? b) If they do expe-rience such difficulties, would it be usefulto introduce a scale describing the level ofcertainty of the diagnosis when it is made?c) To what extent are differences in preva-lence of leprosy, as reported in differentstudies, due to differences in diagnostic cri-teria used by different histopathologists? d)How comparable is the Ridley-Jopling sys-tem in the hands of different histopatholo-gists? e) To what extent does the availabilityor absence of clinical information influencea histopathologist's assessment? f) What is
614
54, 4^Fine, et al.: Comparability Among Histopathologists^615
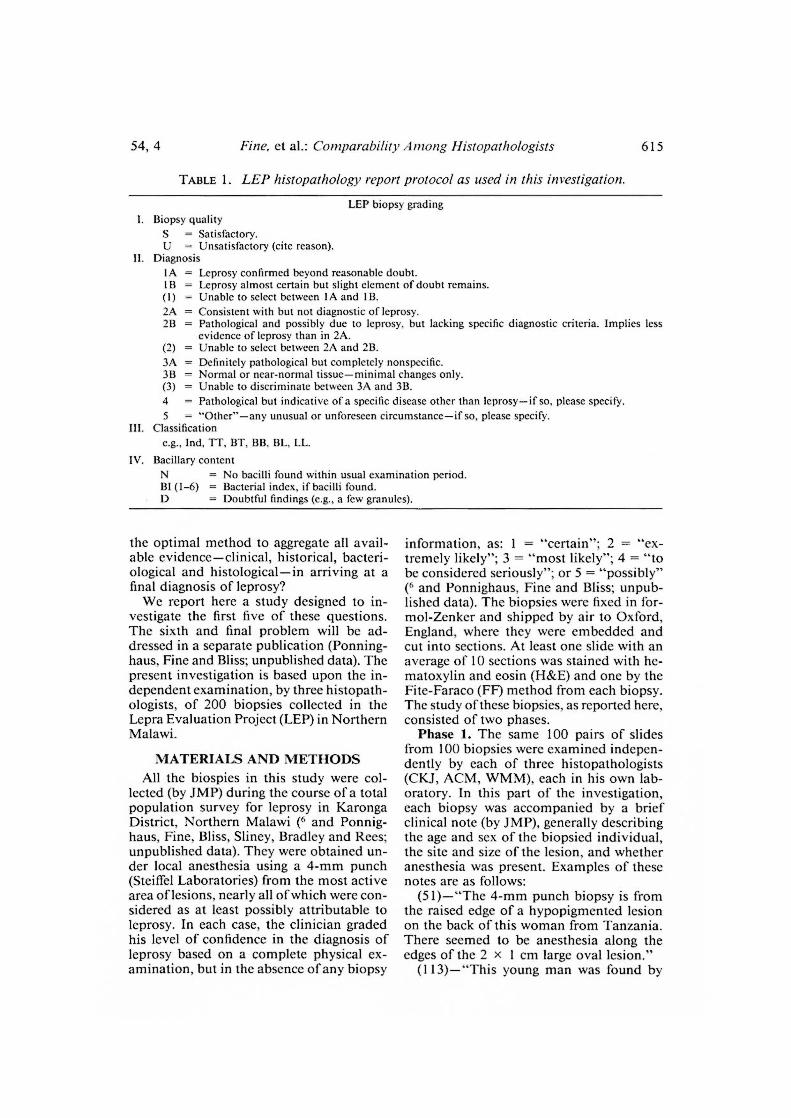
TABLE 1. LEI' histopathology report protocol as used in this investigation.
LEP biopsy gradingI. Biopsy quality
S^= Satisfactory.U = Unsatisfactory (cite reason).
11. DiagnosisIA = Leprosy confirmed beyond reasonable doubt.1B = Leprosy almost certain but slight element of doubt remains.(I) = Unable to select between IA and 1B.2A = Consistent with but not diagnostic of leprosy.211^Pathological and possibly due to leprosy, but lacking specific diagnostic criteria. Implies less
evidence of leprosy than in 2A.(2) Unable to select between 2A and 2B.3A = Definitely pathological but completely nonspecific.311^Normal or near-normal tissue—minimal changes only.(3) Unable to discriminate between 3A and 3B.4^= Pathological but indicative of a specific disease other than leprosy—if so, please specify.5^= "Other"—any unusual or unforeseen circumstance—if so, please specify.
III. Classificatione.g., Ind, TT, BT, 1313, BL, LL.
IV. Bacillary content= No bacilli found within usual examination period.
111 (1-6) = Bacterial index, if bacilli found.= Doubtful findings (e.g., a few granules).
the optimal method to aggregate all avail-able evidence—clinical, historical, bacteri-ological and histological—in arriving at afinal diagnosis of leprosy?
We report here a study designed to in-vestigate the first five of these questions.The sixth and final problem will be ad-dressed in a separate publication (Ponning-haus, Fine and Bliss; unpublished data). Thepresent investigation is based upon the in-dependent examination, by three histopath-ologists, of 200 biopsies collected in theLepra Evaluation Project (LEP) in NorthernMalawi.
MATERIALS AND METHODSAll the biospies in this study were col-
lected (by JMP) during the course of a totalpopulation survey for leprosy in KarongaDistrict, Northern Malawi (( and Ponnig-haus, Fine, Bliss, Sliney, Bradley and Rees;unpublished data). They were obtained un-der local anesthesia using a 4-mm punch(Steiffel Laboratories) from the most activearea of lesions, nearly all of which were con-sidered as at least possibly attributable toleprosy. In each case, the clinician gradedhis level of confidence in the diagnosis ofleprosy based on a complete physical ex-amination, but in the absence of any biopsy
information, as: 1 = "certain"; 2 = "ex-tremely likely"; 3 = "most likely"; 4 = "tobe considered seriously"; or 5 = "possibly"(6 and Ponnighaus, Fine and Bliss; unpub-lished data). The biopsies were fixed in for-mol-Zenker and shipped by air to Oxford,England, where they were embedded andcut into sections. At least one slide with anaverage of 10 sections was stained with he-matoxylin and eosin (H&E) and one by theFite-Faraco (FF) method from each biopsy.The study of these biopsies, as reported here,consisted of two phases.
Phase 1. The same 100 pairs of slidesfrom 100 biopsies were examined indepen-dently by each of three histopathologists(CKJ, ACM, WMM), each in his own lab-oratory. In this part of the investigation,each biopsy was accompanied by a briefclinical note (by JMP), generally describingthe age and sex of the biopsied individual,the site and size of the lesion, and whetheranesthesia was present. Examples of thesenotes are as follows:
(51)—"The 4-mm punch biopsy is fromthe raised edge of a hypopigmented lesionon the back of this woman from Tanzania.There seemed to be anesthesia along theedges of the 2 x 1 cm large oval lesion."
(113)—"This young man was found by

616^ International Journal of Leprosy^ 1986
TABLE 2. Diagnostic certainty categoriesused by histopathologists X, Y, and Zphase I and phase 2 ql the study."
Diagnos-tic
category
Phase 1 Phase 2
X Y Z X
IA 44 23 46 55 25 56113 10 5 — 6 12
(1) — 1_ — 1 11 —/A 12 7 — 14 8 —213 / 24 8 12 27 15
(2) — 7 — — 4 —3A 17 11..._ 36 9 12 223B 1 7 8 — 6
(3) / — — —4 14 1 1_ 3 1 15 — — — — —
Totals 100 100 100 100 100 100
Numbers in table refer to the number of times eachcategory was used. See Table 1 for definitions of eachcategory.
my staff with a swelling covering the fore-head, the nose and most of the right cheek.Both zygomatic nerves seemed enlarged andthe right one was tender. There was perhapsjust slight mouth drop on the right side.Duration 3 weeks. (Dr. ) and my-self thought the most likely diagnosis wasprobably BT leprosy in (type I) reaction.The two specimens are from the forehead."
(137)—"The two specimens are Rom afaintly hypopigmented lesion on the rightupper arm with raised edges. No anesthe-sia."
(284)—"He received treatment at Ko-chirira in 1965 and thereafter for severalyears at Karonga hospital. He was now foundwith several new macules. Slit skin smearsfrom the macules were positive (BI 1+) sev-eral solids and fragments."
Each histopathologist reported his find-ings using the same protocol (see Table 1).The protocol specifies a four-part code: first,an assessment of whether the biopsy wasconsidered satisfactory (S) or unsatisfactory(U); second, a "certainty" grading descend-ing in steps from a most-certain category(1A = "leprosy confirmed beyond reason-able doubt") to an assessment that thelesion was not leprosy but something else(4 = "pathological but indicative of a dis-ease other than leprosy"); third, a classifi-cation (TT, BT, etc.) to be assigned if lep-rosy was diagnosed; and, lastly, an indication
of bacillary load (BI). The wording of theprotocol was not discussed among the his-topathologists before the study.
Phase 2. This was identical to phase 1,except that only one histopathologist hadaccess to clinical notes and the other tworead the slides totally "blind" of any infor-mation.
All results were sent directly to the Lon-don School of Hygiene and Tropical Med-icine for compilation and analysis. The re-sults of phase 1 were made available to thecollaborating histopathologists before thebeginning of phase 2.
RESULTSThe results of the two phases will be de-
scribed separately. The histopathologists areidentified only as X, Y, and Z. H istopathol-°gists X and Y lacked clinical notes in phase
Phase 1. All of the biopsies were consid-ered sufficiently satisfactory to be reportedupon by each of the histopathologists.
The leprosy diagnostic certainty resultsfor all three histopathologists are summa-rized separately in Table 2 and together inTable 3. A clear difference is evident in thepreference of each histopathologist for dif-ferent categories, Y using the most and Zthe least (Table 2). If we, for the sake ofsimplicity, consider categories 1A, 1B or 1as indicative of "definite leprosy," cate-gories 2A, 2B and 2 as "possibly leprosy,"and categories 3A, 3B, 3 or 4 as "no evi-dence of leprosy," we find estimates from30% (by Y) to 54% (by X) for the proportionwith definite leprosy in this series (Table 3).The percent agreement on each of these cat-egories between each pair and among allthree histopathologists is set out in Table 4.It is seen that whereas pairs of histopa-thologists agreed by this overall criterion onbetween 57% and 72% of biopsies, only 49%of the biopsies were assigned the same levelof certainty by all three histopathologists.
A similar comparison may be made be-tween each of the histopathologists and thecertainty of the clinical assessment. The cat-egories chosen for this comparison are il-lustrated in Table 5. Agreement on "definiteleprosy" occurred when the clinician con-sidered the case either "certain" or "ex-tremely likely" and the histopathologist as-
54, 4^Fine, et al.: Comparability Among IIistopathologists^617
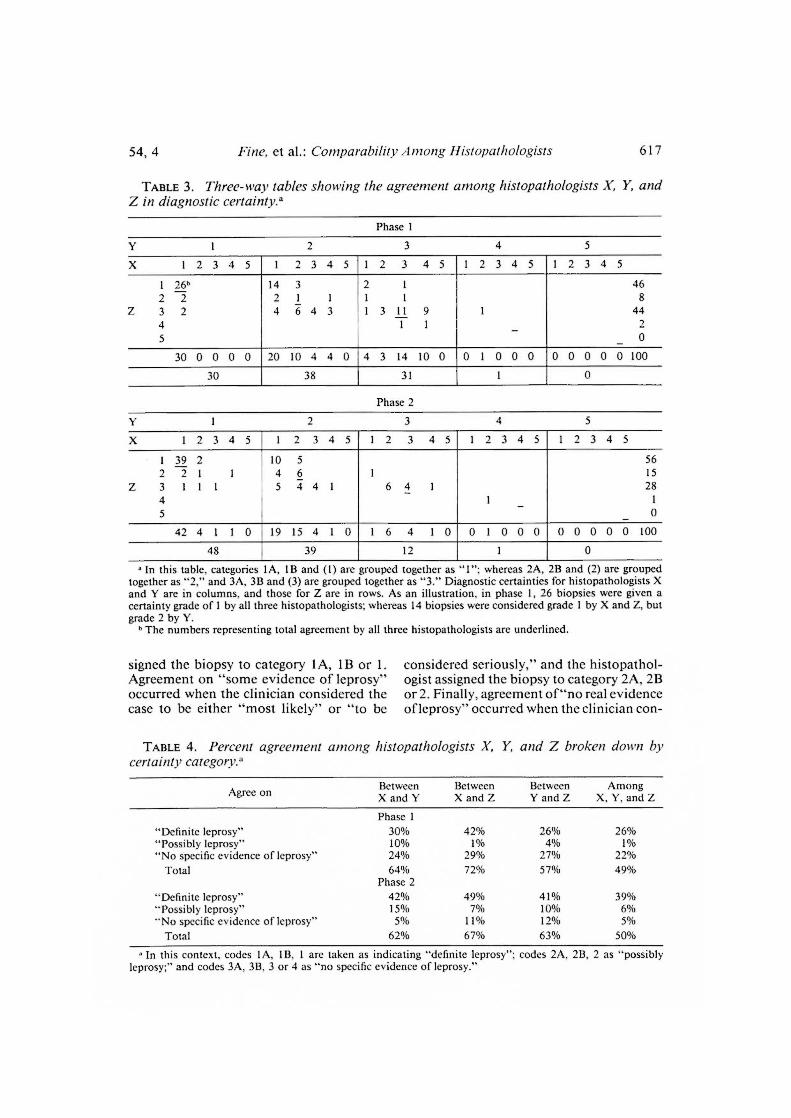
TABLE 3. Three-way tables showing the agreement among histopathologists X, Y, andZ in diagnostic certainty.a
Phase 1
2^3^4^5
X 1^2 3 4 5 I 2^3^4 5 1 2 3 4 5 1 2 3 4 5 1 2 3 4 5
1 26' 14 3 2 1 4622 21 1 1 1 8
Z 32 4643 1 3 11 9 1 444 1 1 25 0
30^0 0 0 0 20 10^4^4 0 4 3 14 10 0 0 1 0 0 0 0 0 0 0 0 100
30 38 31 1 0
Phase 2
3^4^5
X 1^2^3 4 5 1 2^3 4 5 1 2^3 4 5 1 2 3 4 5 1 2 3 4 5
1 39^2 10 5 56221 1 46 1 15
Z 3 111 5 44 1 64_ 1 284 1 15 — 0
42^4^1 1 0 19 15^4 1 0 1 6^4 1 0 0 1 0 0 0 0 0 0 0 0 100
48 39 12 1 0
In this table, categories 1A, Ill and (1) are grouped together as "I"; whereas 2A, 2B and (2) are groupedtogether as "2," and 3A, 3B and (3) are grouped together as "3." Diagnostic certainties for histopathologists Xand Y are in columns, and those for Z are in rows. As an illustration, in phase 1, 26 biopsies were given acertainty grade of 1 by all three histopathologists; whereas 14 biopsies were considered grade 1 by X and Z, butgrade 2 by Y.
" The numbers representing total agreement by all three histopathologists are underlined.
signed the biopsy to category 1A, 1 B or I.Agreement on "some evidence of leprosy"occurred when the clinician considered thecase to be either "most likely" or "to be
considered seriously," and the histopathol-ogist assigned the biopsy to category 2A, 2Bor 2. Finally, agreement of"no real evidenceofleprosy" occurred when the clinician con-
TABLE 4. Percent agreement among histopathologists X, Y, and Z broken down bycertainty category.
Agree on BetweenX and Y
BetweenX and Z
BetweenY and Z
AmongX, Y, and Z
Phase 1"Definite leprosy" 30% 42% 26% 26%"Possibly leprosy" 10% 1% 4%"No specific evidence of leprosy" 24% 29% 27% 22%
Total 64% 72% 57% 49%Phase 2
"Definite leprosy" 42% 49% 41% 39%"Possibly leprosy" 15% 7% 10% 6%"No specific evidence of leprosy" 5% 11% 12% 5%
Total 62% 67% 63% 50%
In this context, codes 1A, 113, 1 are taken as indicating "definite leprosy"; codes 2A, 2B, 2 as "possiblyleprosy;" and codes 3A, 3B, 3 or 4 as "no specific evidence of leprosy."

618^ International Journal of Leprosy^ 1986
TABLE 5. Criteria used in comparison between clinical and histopathological certainty(see Table 6).
Clinical certaintyBiopsy certainty
3 4 Totals
"Certain"^
A"Extremely likely""Most likely""To be considered seriously""Possibly""Other/not leprosy"
Cells A + B indicate agreement on "definitely leprosy."Cells C + D indicate agreement on "some evidence of leprosy."Cells E + F indicate agreement on "no real evidence of leprosy."(A +B+C+D+E+ F)/(P + Q + R + S + T) = overall agreement between clinician and histopathologist.Cells G + H indicate relative clinical underdiagnosis (or histopathological overdiagnosis).Cells I+J+K+L+M+N indicate relative histopathological underdiagnosis (or clinical overdiagnosis).Cells (G +H+I+J+K+L+M+ N)/(P + Q + R + S + T) = overall considerable disagreement
between clinician and histopathologist.
sidered the case only "possible" and the his-topathologist assigned the biopsy to cate-gory 3 or 4. Those cases classified as only"to be considered seriously" or as "possi-ble" by the clinician, but whose biopsieswere considered 1A, 1B or 1 by the histo-pathologist, were considered to indicateconsiderable disagreement in the directionof relative clinical underdiagnosis (or his-topathological overdiagnosis). On the,otherhand, those cases classified clinically aseither "certain," "extremely likely," or"most likely," but which were assigned to
categories 3 and 4 by the histopathologist,were considered to indicate considerabledisagreement in the direction of relative his-topathological underdiagnosis (or clinicaloverdiagnosis). Both of these groups togeth-er constitute the total with considerable dis-agreement. These comparisons between theclinician and each histopathologist areshown in Table 6. The percentages are cal-culated excluding five biopsies which weretaken for reasons other than leprosy (inter-estingly enough none of the histopatholo-gists classed these as 1A, 1B or 1, but his-
TABLE 6. Percent agreement and disagreement among histopathologists X, Y, and Zand clinical assessment of "cases" biopsied because leprosy was suspected on clinical grounds(95 in phase 1 and 99 in phase 2).a
Phase 1Between clinician and
Phase 2Between clinician and
X
Agree on"Definitely leprosy" (31)"32.6% (20) 21.1% (26) 27.4% (37) 37.4% (32) 32.3% (37) 37.4%"Some evidence of
leprosy" (6)^6.3% (17) 17.9% (5) 5.3% (13) 13.1% (19) 19.2% (7) 7.1%"No real evidence of
leprosy" (17)^17.9% (18) 18.9% (20) 21.1% (4) 4.0% (5) 5.1% (12) 12.1%Overall agreement (54) 56.8% (55) 57.9% (51) 53.7% (54) 54.5% (56) 56.6% (56) 56.6%
Disagree onRelative clinical
underdiagnosis (12)^12.6% (6) 6.3% (11) 11.6% (9) 9.1% (4) 4.0% (4) 4.0%Relative histopatho-
logical underdiagnosis (4) 4.2% (5) 5.3% (12) 12.6% (5) 5.1% (6) 6.1% (11) 11.1%Total considerable
disagreement (16)^16.8% (11) 11.6% (23) 24.2% (14) 14.1% (10) 10.1% (15) 15.2%
Categories are described in text and in Table 5.In each cell, the number of biopsies is given in parentheses.

54, 4^Fine, et al.: Comparability Among Histopathologists^619
TABLE 7. Classifications provided by histopathologists X, Y, and Z.3
Phase 1 Phase 2
XCertainty Certainty Certainty
XCertainty Certainty Certainty
1 2 1 1 2 1 2 1 1
I 4 10 0 I / 0 21 8 0 / 2 01/TT 0 0 0 2 0 0 0 0 0 0 0 0TT 13 0 3 6 11 0 15 1 1 4 6 0TT/BT 0 0 II 7 8 0 0 0 12 2 14 0
1/BT 0 / 0 0 0 0 0 0 1 / 0 0
BT 35 / 12 5 /-) 1 25 1 32 27 30 0BT/BB 0 0 0 0 0 0 0 0 1 0 1 0
BB 0 0 0 0 1 0 0 0 0 0 1 0BB/BL 0 0 1 0 0 0 0 0 1 0 0 0BL / 0 0 0 1 0 1 0 0 0 0 0BL/LL 0 0 /_ 0 0 0 0 0 0 0 0 0LL 0 0 0 0 1 0 0 0 0 0 / 0Totals 54 12 29 21 46 1 62 11 48 37 56 0
" Numbers are the total numbers of classifications provided. The number of classifications are given separatelyfor biopsies given certainty codes 1A, 113, 1 (="I") vs certainty codes 2A, 213, 2 (="2").
topathologist X classed one of them as 2A).Using these criteria, we find that the overallagreements between the clinician and eachhistopathologist were quite similar althoughthere were differences in the distribution oftheir agreements among the "definite,""some," and "no real" evidence categories.There was greater variation between thelevels of considerable disagreement be-tween the clinician and different histopa-thologists, 12% with histopathologist Y and24% with histopathologist Z.
Classifications were provided for differ-ent numbers of biopsies by each of the his-topathologists as shown in Table 7. Withone exception (a 1B biopsy for histopathol-ogist Y), each histopathologist provided aclassification for all biopsies given certaintyIA, 1B or 1. In addition, histopathologistX provided a classification for all 2A biop-sies but no 2B biopsies; whereas histo-pathologists Y and Z provided classifica-tions for only some of the biopsies codedas 2A, 2B or 2 on the certainty scale. Dif-ferent preferences are evident, with the TT/BT category being used frequently by Y andZ but never by X. Histopathologist X usedthe "indeterminate" classification far morefrequently than either Y or Z, but most (10
out of 14) of the biopsies so assigned werein certainty group 2.
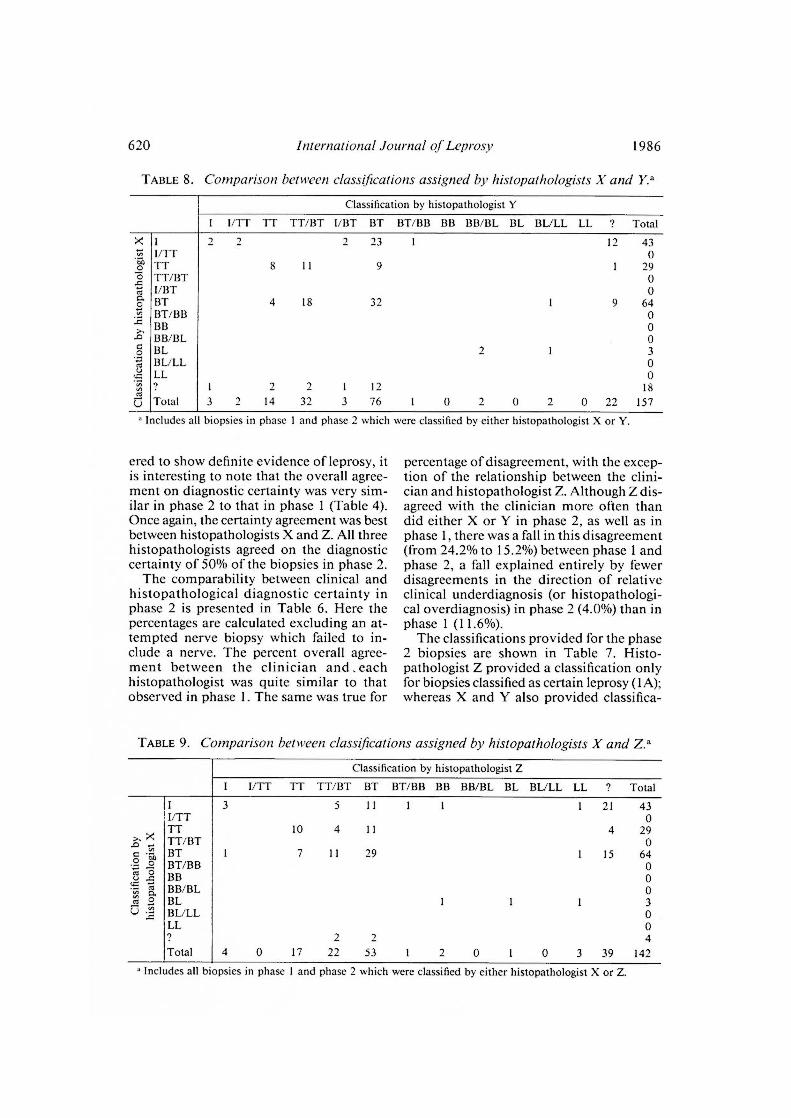
Tables 8, 9, and 10 show the correlationsbetween classifications by each of the his-topathologists. The overall agreement isgood, with the exception of one biopsy (113)classed as BT ("in downgrading reaction")by X, but as BL/LL by Y and as LL by Z.
Phase 2. Again, all biopsies were consid-ered by all three participants to be satisfac-tory for reporting purposes. The diagnosticcertainty results and agreement between thehistopathologists are presented in Tables 2,3, and 4. There were similar preferences fordiagnostic categories in phase 2 as in phase1, with histopathologist Z preferring thefewest categories and Y the most (Table 2).All three found the proportion of biopsiesindicative of definite leprosy (codes 1A, 1Bor 1) higher in phase 2 than in phase 1.Again, histopathologist Y reported the low-est number of definite biopsies (48, com-pared to 30 in phase 1) and X found thelargest number (62, compared to 54 in phase1). Histopathologist Z considered 56 biop-sies as showing definite evidence of leprosyin phase 2, compared to 46 in phase 1.
Given the differences between phases 1and 2 in the proportion of biopsies consid-
620^ International Journal of Leprosy^ 1986
TABLE 8. Comparison between classifications assigned by histopathologists X and Y."
Classification by histopathologist Y
1/TT TT TT/13T 1/13T BT I3T/1313 BB BB/BL BL BL/LL LL 7 Total
23 1 I? 431/TTTT 8 11 9
-a TT/13T 0174o.
1/UTBT 4 18 32 1 9
064
I3T/1313BB 0I3B/BL 0BL 2 I 3BL/LL 0LL
1 1? 18L.) Total 3 ? 14 32 3 76 1 0 0 2 0 22 157
Includes all biopsies in phase 1 and phase 2 which were classified by either histopathologist X or Y.
ered to show definite evidence of leprosy, itis interesting to note that the overall agree-ment on diagnostic certainty was very sim-ilar in phase 2 to that in phase 1 (Table 4).Once again, the certainty agreement was bestbetween histopathologists X and Z. All threehistopathologists agreed on the diagnosticcertainty of 50% of the biopsies in phase 2.
The comparability between clinical andhistopathological diagnostic certainty inphase 2 is presented in Table 6. Here thepercentages are calculated excluding an at-tempted nerve biopsy which failed to in-clude a nerve. The percent overall agree-ment between the clinician and eachhistopathologist was quite similar to thatobserved in phase 1. The same was true for
percentage of disagreement, with the excep-tion of the relationship between the clini-cian and histopathologist Z. Although Z dis-agreed with the clinician more often thandid either X or Y in phase 2, as well as inphase 1, there was a fall in this disagreement(from 24.2% to 15.2%) between phase 1 andphase 2, a fall explained entirely by fewerdisagreements in the direction of relativeclinical underdiagnosis (or histopathologi-cal overdiagnosis) in phase 2 (4.0%) than inphase 1 (11.6%).
The classifications provided for the phase2 biopsies are shown in Table 7. Histo-pathologist Z provided a classification onlyfor biopsies classified as certain leprosy (IA);whereas X and Y also provided classifica-
TABLE 9. Comparison between classifications assigned by histopathologists X and Z."
Classification by histopathologist Z
I/TT TT TT/BT BT BT/BB BB BB/BL BL BL/LL LL ? Total
5 11 1 1 1 21 43I/TT 0TT 10 4 11 4 ?9
..n TT/BT 0BT 1 7 11 29 1 15 64BT/BB 0BB 0
'7)1 BB/BL 0BL 1 1 1 3BL/LL 0LL 09 2 4Total 4 0 17 ?? 53 1 2 0 1 0 3 39 142
" Includes all biopsies in phase 1 and phase 2 which were classified by either histopathologist X or Z.

54, 4^Fine, et al.: Comparability Among Ilistopathologists^621
TABLE 10. Comparison between classifications assigned by histopathologists Y and Z.a
Classification by histopathologist Z
I 1/TT TT TT/BT 1/BT BT BT/BB 1313 BB/BL BL BL/LL LL Total
3I/TT 2TT 4 3 5 14
-6.0 TT/13T 7 7 14 4 32
I/BT 3 30. BT 6 12 78 1 76 76
13T/B13 1.0 1313 0.0 1313/BL 1 1
BL 0BL/LL 1 1LL 09 1 5 8Total 4 0 17 22 0 53 0 1 0 3 40 143
Includes all biopsies in phase 1 and phase 2 which were classified by either histopathologist Y or Z.
tions for several biopsies considered to showsome evidence of leprosy (2A, 2B, 2). Onceagain we note the preference of the TT/BTcategory by histopathologists Y and Z, andits total avoidance by X. HistopathologistX used the indeterminate classification farmore often than Y or Z, for 29% of all biop-sies and for more than a third of all thebiopsies he considered to have definite evi-dence of leprosy (1A, 1B or 1).
A major difference in classification arosein only a single phase 2 biopsy (284), whichwas classified as indeterminate by histo-pathologist X, BT/BB by Y, and LL by Z(Tables 8, 9, and 10).
DISCUSSIONPeople differ. This is true of diseased in-
dividuals in terms of their lesions, bothmacroscopic and microscopic. It is also trueof clinicians and histopathologists in termsof their observations and interpretations ofthese lesions. The study reported here pro-vides an attempt to assess the magnitude ofsuch differences as they affect the diagnosisof leprosy by three histopathologists, eachof whom has spent many years involved inthe histopathological diagnosis of leprosy.Without a doubt, different results wouldhave arisen if other individuals had beeninvolved or if a different series of biopsieshad been used. What is important is thusto consider the nature and trends of thesedisagreements in order to be able to applythese results to the improvement of leprosydiagnosis in the future.
One of the fundamental findings of thisstudy is the frequent use of the 2A, 2B or 2diagnosis category by all three histopatholo-gists (20% of all biopsies by X, 38.5% by Y,11.5% by Z). This category, implying a his-topathological picture which was consistentwith but not pathognomonic of leprosy, im-plies a degree of uncertainty on the part ofthe histopathologists analogous to that ex-perienced by clinicians when assessing lep-rosy in the field. Given the frequency of useof the category in this study, it is of interestthat the unclear diagnosis category appearsso infrequently in the literature.
The proportions of biopsies classed asshowing strong or definite evidence of lep-rosy (diagnostic categories 1A, 1B, 1; seeTable 1) ranged from 30% to 54% in phase1 and 48% to 62% in phase 2 (39% to 58%overall). In this context, it should be re-called that the biopsies were obtained fromlesions ascertained in a total population sur-vey, and included a range from minimal towell-advanced disease. Of the 200 individ-uals included in this investigation, leprosywas considered certain or extremely likelyon clinical grounds in 82 (35 in phase 1 and47 in phase 2). Considering these 82 pa-tients alone, the proportions of biopsiesclassed as showing strong or definite evi-dence of leprosy ranged from 63% to 83%(Tables 5 and 6) among the three histo-pathologists.
With reference to classification, we founda high degree of correlation among the threehistopathologists (Tables 8, 9, and 10). Of

622^ International Journal of Leprosy^ 1986
the 200 biopsies included in this study, onlytwo led to major disagreements. One of thesewas from a patient considered to be in (type1) reaction clinically, which may explain whyit was classified as BT ("in downgrading re-action"), BL/LL and LL by the three his-topathologists (see clinical note 113 in Ma-terials and Methods, Phase 1). An additionalfactor might be that the Fite-Faraco stainof this slide had faded considerably by thetime it was examined by histopathologistY, and even more so by the time the slidewas examined by histopathologist X. Thesecond was from a patient who had receivedantileprosy treatment for many years, andin whose biopsy the inflammatory infiltratewas minimal, which may explain why it wasclassified independently as I, BT/BB and LL(see clinical note 284 in Materials andMethods, Phase 1). In addition, there wereobvious preferences for and against certainclassifications by the participants. The TT/BT category was used frequently by histo-pathologists Y and Z, but never by X. Incontrast, the "indeterminate" classificationwas used frequently by histopathologist Xbut rarely by Y and Z. Histopathologist Yused the indeterminate classification threetimes, but never in a biopsy classed as def-inite leprosy (1A, 1B or 1). HistopathologistZ used the indeterminate classification fourtimes, but only for biopsies considered toshow definite evidence of leprosy (1A). Therewas no overlap between the three indeter-minates of histopathologist Y and the fourof Z. In contrast, histopathologist X usedthe indeterminate classification 43 times(21.5% of all biopsies in the study), includ-ing for 25 out of 116 biopsies (21.6%) whichhe considered to have definite evidence ofleprosy. This finding is particularly inter-esting insofar as it suggests that the majordifferences in the proportion of leprosy casesclassed as indeterminate, as reported in dif-ferent studies and in different parts of theworld, may be due entirely to differences indiagnostic terminology.
One of the important questions addressedby this investigation is the extent to whichclinical information may influence an his-topathologist's interpretation of biopsy ma-terial. In phase 1 of this study each histo-pathologist had access to a brief clinical note;whereas in phase 2 this information was
available only to histopathologist Z. If theclinical information had influenced the his-topathologists, we would expect that theagreement between X and Z and between Yand Z should have been higher in phase 1(when all had access to the information) thanin phase 2 (when only Z had such access).Scrutiny of Table 4 shows no evidence ofsuch a trend. Another way to test the hy-pothesis is by examining the correspon-dence between the clinician and the histo-pathologist. If the clinical note had made adifference, one would expect that the agree-ment between X or Y and the clinician wouldbe higher in phase 1 than in phase 2, butthe agreement between Z and the clinicianshould have been the same in phase 1 andphase 2. We find no strong evidence for suchan effect. On the other hand, we see in Table6 that histopathologist Z disagreed with theclinician less often in phase 2 than phase 1.This may suggest that the phase 2 biopsieswere slightly "easier" for the histopathol-ogists. If so, this could have counteractedany disadvantage suffered by histopathol-ogists X and Y because of their not havingthe clinical notes. In summary, then, theresults are not inconsistent with the hy-pothesis that clinical information had someinfluence on these histopathologists, but theysuggest that any such influence was small.
All of these results must be seen in thecontext of the design of this study. All ofthe histopathologists worked independentlyof one another and used the same protocolfor reporting results. Although these fea-tures of the study were ideal, the design hadcertain failings. Some of the differenceswhich arose in establishing and comparingthe certainty of the diagnosis of leprosy areprobably attributable to the wording of thecoding protocol (Table 1). Differences in in-terpretation would be expected to arise, inparticular since the histopathologists did notdiscuss the wording among themselves priorto the study. In one sense this makes ourfindings "realistic," insofar as the majorityof histopathologists in the world work in-dependently and rely upon their interpre-tation of certain published descriptions andterminology to achieve a modicum of con-sistency. On the other hand, the wordingused in this study was probably not optimal,and greater comparability among the his-

54, 4^Fine, et al.: Comparability Among Histopathologists^623
topathologists could have been achieved ifthe wording had been "better." This issueis addressed in the Appendix to this paper.
Another weakness of the design of thisstudy was the absence of any "blind" du-plicate or repeat biopsies. Their inclusionin the study would have permitted an as-sessment of the degree of intra-observervariation, and would have facilitated theassessment of the influence of clinical in-formation on biopsy interpretation. It ishoped to carry out a study including such"blind" duplicates in the future.
We have presented the results of our studyat their face value. We have not attemptedto measure the sensitivity or specificity ofdiagnoses made by each histopathologistsince this is a difficult problem, requiringreference to an absolute standard, and willbe discussed in a separate publication (Pon-nighaus, Fine and Bliss; unpublished data).Derived statistics such as the comparabilityKappa have not been used since they arenot widely understood ("). More impor-tantly, it should be recognized that the nu-merical values reported here are not the mostimportant result of this study. They are afunction of the histopathologists, the biop-sies and the coding conventions. Othercombinations would have yielded differentnumerical values. What is important is theclear demonstration that the use of histo-pathology in the diagnosis of "early" lep-rosy (i.e., early with respect to evolution) isnot a simple matter, even when the biopsiesare read by people with many years of ex-perience. There is room for improvementin the standardization of criteria and of ter-minology.
SUMMARYIdentical slides from 200 biopsies ob-
tained from individuals suspected of havingleprosy during the course of an epidemio-logical survey in Northern Malawi were ex-amined sequentially and independently bythree histopathologists, using a standardprotocol to report their findings. Their re-sults are compared among themselves andwith a standardized clinical assessment ofeach subject. There was more agreementamong the histopathologists as to classifi-cation of leprosy cases than there was onthe diagnosis of leprosy. The proportion of
biopsies considered to show definite evi-dence of leprosy varied from 39% to 58%among the histopathologists. An apprecia-ble additional proportion of biopsies (11.5%to 38.5% for the three histopathologists) wasconsidered to show evidence suggestive butnot pathognomonic of leprosy. Althoughthere was, in general, good agreement onclassification, the proportion of biopsiesconsidered to show evidence of indetermi-nate leprosy varied from 1.5% to 21.5%among the three histopathologists. This sug-gests that some of the reported differencesin the prevalence and proportion of inde-terminate leprosy in different populations isdue to terminology alone. A follow-upmeeting of the study participants revealedthat many of the differences in diagnosiscertainty were due to difficulties in inter-preting evidence of nerve involvement. Itis recommended that greater attention bepaid to the difficulties of diagnosing leprosyon histopathological as well as clinicalgrounds. A revised standard protocol forreporting histopathological evidence of lep-rosy is presented.
RESUMENDurante un estudio epidemiolOgico en Malawi del
Norte, tres histopatOlogos, usando un protocolo de re-porte estandar, examinaron independientemente, la-minillas idOnticas de 200 biopsias obtenidas de indi-viduos con sospecha de lepra. Sus resultados fueroncomparados entre si y con la evaluaciem clinica estan-darizada de cada sujeto. Hubo más concordancia entrelos histopatOlogos en cuanto a la clasificaciOn de loscasos que en cuanto al diagnOstico de la lepra. La pro-porciem de biopsias con evidencias definitivas de lepravariO del 39% al 58% entre los histopatOlogos. Unaapreciable proporciem adicional de biopsias (del 11.5%al 38.5% para los 3 histopatOlogos) se consideraron conevidencias sugestivas pero no patognomOnicas de laenfermedad. Aunque en general hubo buena concor-dancia en cuanto a clasificaciem, la proporciOn de biop-sias con evidencias de lepra indeterminada variO del1.5% al 21.5% entre los 3 histopatOlogos. Esto sugiereque algunas de las diferencias reportadas en la preva-lencia y proporciem de la lepra indeterminada en di-ferentes poblaciones solo se &ben a la terminologia.En una reunion de los participantes del estudio se es-tableciO que muchas de las diferencias en el diagnOsticose debieron a dificultades en la interpretaciOn de lasevidencias de afecciOn nerviosa. Se recomienda que seponga más atenciOn a las dificultades de diagnOsticode la lepra tanto a nivel histopatolOgico como clinico.

624^ International Journal of Leprosy^ 1986
Sc presenta un protocolo estandar para reportar lasevidencias histopatoleogicas de la lepra.
RESUMETrois histopathologistes, utilisant un protocole stan-
dard pour noter leurs observations, ont etudie de ma-niere sequentielle et de fawn independante, des lamesidentiques provenant de 200 biopsies recueillies chezdes personnes soupconnees d'être atteintes dc lepre.Cette etude a ete menee au cours d'une enquete epi-demiologique au Malawi du Nord. Les resultats ontCite compares entre eux, de meme qu'avec une evalu-ation clinique standardisee de chaque individu. On aconstatii one concordance plus forte entre les histo-pathologistes pour cc qui regarde la classification descas de lepre; cette concordance est moms prononceepour le diagnostic de lepre. La proportion de biopsiesconsider-6es comme presentant des signes indubitablesde lepre a vane de 390/o a 58% scion les histopatho-logistes. Une proportion supplêmentaire notable dcbiopsies (11,5% 6 38,5% pour les trois histopatholo-gistes) ont ête considerees comme presentant des signesqui suggeraient la lepre, sans en etre pathognomo-niques. Malgre la concordance generalement bonne pourcc qui concerne la classification, la proportion de biop-sies considerees comme prêsentant des images de lepreincleterminee a vane de 1,5% 6 21,5% chez ces troishistopathologistes. Cette observation donne 6 penserque certaines des differences qui sont rapporffies quant
la prevalence et 6 la proportion de la lepre indeter-minCie dans diverses populations, pourraient etre duessimplement a la terminologie. Une reunion subs&quente des participants a l'etude a revel& qu'une grandepart des incertitudes diagnostiques etait due aux dif-licultes rencontrees pour interpreter les manifestationsd'atteinte nerveuse. On recommande des fors d'accor-der une plus grande attention aux difficultes du diag-nostic de la lepre, tant au point de vue histopatholo-gigue qu'au point de vue clinique. On propose unnouveau protocole standard pour consigner les obser-vations histopathologiques de la lepre.
Acknowledgments. This investigation arose as partof the Lepra Evaluation Project (LEP) and was fundedprimarily by LEPRA, the British Leprosy Relief As-sociation. Additional special funding for the follow-upmeeting was provided by the Heiser Foundation andis gratefully acknowledged. The authors wish to thankthe people of Karonga District, Northern Malawi, andthe entire LEP staff without which this study wouldnot have taken place. Particular thanks are due to Mr.N. Maine for assisting in the analysis of the results andto Ms. B. Slessor for preparation of the manuscript.
REFERENCESI. BRYCESON, A. and PEALTZGRAFF, R. E. Leprosy.
2nd ed. London: Churchill Livingstone, 1979.2. CORREA, P., O'CONNOR, G. T., BERNARD, C. W.,
AXTELL, L. M. and MEYERS, M. H. International
comparability and reproducibility in histologicsubclassifications in Hodgkin's disease. J. Natl.Cancer Inst. 50 (1973) 1429-1435.
3. EVANS, D. M. D., SHELLEY, G., CLEARY, B. and13ALDwirr, Y. Observer variation and quality con-trol of cytodiagnosis. J. Clin. Pathol. 27 (1974)945-950.
4. HEENAN, P. J., MATZ, L. R., BLACKWEI..L, J. B.,KELSALL, G. R. H., SINGH, A., TEN SELDAM, R. E.J. and HOLMANN, C. D. J. Inter-observer varia-tions between pathologists in the classification ofcutaneous malignant melanoma in western Aus-tralia. Histopathology 8 (1984) 717-729.
5. JERATII, V. P. and DESAI, S. R. Diversities in clin-ical and histopathological classification of leprosy.Lepr. India 54 (1982) 130-134.
6. MCDOUGALL, A. C., PONNIGHAUS, J. M. and FINE,
P. E. M. The histopathological examination of skinbiopsies from an epidemiological study of leprosyin northern Malawi. Int. J. Lepr. (1987) (in press).
7. MEYERS, W. M., HEGG1E, C. D., KAY, T. L., STA-
pLE, E. M. and KVERNES, S. The Ridley-Joplingfive-group classification of leprosy—correlationsof parameters of the classification in 1429 leprosypatients. Int. J. Lepr. 47 (1979) 683-684.
8. NON-HODGKIN'S LYMPHOMA PATHOLOGIC CLAS-
SIFICATION PROJECT. Summary and description ofa working formulation for clinical use. Cancer 49(1982) 2112-2135.
9. RIDLEY, D. S. Skin Biopsy in Leprosy. 2nd ed.Basle: Documentia Geigy, 1985.
10. RIDLEY, D. S. and JOPLING, W. H. Classificationof leprosy according to immunity; a five-groupsystem. Int. J. Lepr. 34 (1966) 255-273.
II. SCHMOECKEL, C. How consistent are dermato-pathologists in reading early malignant melano-mas and lesions "precursor" to them? An inter-nation survey. Am. J. Dermatopathol. 6 Suppl.(1984) 13-24.SEHGAL, V. N., KORANNE, R. V., NAYYAR, M. andSAXENA, H. M. K. Application of clinical and his-topathological classification of leprosy. Derma-tologica 161 (1980) 93-96.
13. SEHGAL, V. N., REGE, V. L. and REY, M. Corre-lation between clinical and histopathological clas-sifications in leprosy. Int. J. Lepr. 45 (1977) 278—280.
14. SILCOCKS, P. B. S. Measuring repeatability and va-lidity of histological diagnosis—a brief review withsome practical examples. J. Clin. Pathol. 36 (1983)1269-1275.
15. SINGH, K., IYENGAR, B. and SINGH, R. Variationsin clinical and histopathological classification ofleprosy—a report and a possible explanation. Lepr.India 55 (1983) 472-479.
APPENDIXAt the conclusion of this study, the participants met
for two days in order to discuss the results. Twenty-six pairs of slides over which there had been substantial

54, 4^Fine, et al.: Comparability Among Histopathologists^625
disagreement concerning the certainty of the diagnosisof leprosy were reviewed. In each case, the histopathol-ogist who had given the highest certainty grading re-examined the slide and tried to present the evidenceon which his certainty grading was based.
In only one case could the crucial evidence no longerbe found, within a reasonable period of time. Withreference to the remaining 25 biopsies, the three his-topathologists reached complete agreement in ten. Somedisagreement remained for 15 biopsies. The main rea-sons for the remaining disagreements were: a) whetheror not a particular infiltrate contained the remains ofa nerve; b) whether or not, if there was undoubtedly anerve, the infiltrate was substantial enough to permita definite diagnosis of leprosy; and c) whether or notparticular minimal findings should be considered aspossibly due to leprosy. It was felt that it would not bepossible to resolve all of the remaining differences al-though, in some cases, special staining procedures mighthave provided sufficient additional information to bringcomplete agreement within reach.
After this workshop, the participants were joined onthe third day by Professor K. P. W. J. McAdam (De-
partment of Clinical Tropical Medicine, London Schoolof Hygiene and Tropical Medicine); Dr. D. S. Ridley(formerly Hospital for Tropical Diseases, London); andDr. T. J. Ryan (Department of Dermatology, JohnRadcliffe Hospital, Oxford) in order to discuss thebroader implications of this study. It was agreed thatthe results accumulated thus far raised important issuesrelevant to leprosy research. Insofar as some of thediscrepancies may have been attributable to the word-ing of the original coding protocol (Table 1), the groupdiscussed and agreed upon an improved version of thecertainty scale. The revised protocol, analogous to onerecently published by Ridley (n), is reproduced hereas Table A-1, along with examples of criteria whichmay be used to assign the categories implying differentlevels of evidence of leprosy. These are only examples,and are by no means intended as an exhaustive set ofcriteria. A follow-up study is now planned in order toassess the usefulness of this revised protocol. The par-ticipants encourage other workers in the leprosy fieldto consider using this protocol when reporting and ana-lyzing histopathological evidence of leprosy and/or tocomment critically upon it.
TABLE A-1. Revised biopsy grading protocol.
1. Biopsy qualityS = Satisfactory.U = Unsatisfactory—if so, please explain.
II. Diagnosis1^Leprosy confirmed beyond reasonable doubt:
e.g., i) Presence of AFB especially in protected sites.ii) Infiltration by inflammatory cells and/or granuloma and damage or destruction of nerve
tissue.iii) Etc.
2^Suggestive of but not diagnostic of leprosy:e.g., i) Granulomatous infiltration without definite nerve involvement and absence of features of
other granulomatous disease.ii) Selective inflammation of either perineural tissue and/or sweat glands and/or arrector pili
muscle.iii) Etc.
3 = Pathological and possibly due to leprosy (but also possibly due to other diseases):e.g., i) Granulomatous infiltration not involving nerves at all.
ii) Etc.4^Pathological but (completely) nonspecific.5^Normal or near-normal tissue (skin with no significant lesion).6^Pathological and indicative only of a specific disease other than leprosy—if so, please specify.7^"Other"—any unusual or unforeseen circumstance—if so, please specify.
Classificatione.g., I, TT, BT, BB, BL, LL.
IV. Bacillary content= No bacilli found.
BI (1-6) = Bacterial index, if bacilli found.= Doubtful findings (e.g., a few granules).
Examples of codes as reported:^S,1,TT,N^S,2,—,N^S,6,—,N (onchocerciasis)S,1,BL,3^S,3,—,N