cpd development - rcni · cpd development assessment and management of ... read this cpd article...
TRANSCRIPT
52 august 13 :: vol 28 no 50 :: 2014 © NURSING STANDARD / RCN PUBLISHING
CONTINUING PROFESSIONAL DEVELOPMENTCPD
Assessment and management of patients with ankle injuriesNS756 Walker J (2014) Assessment and management of patients with ankle injuries. Nursing Standard. 28, 50, 52-59. Date of submission: May 15 2014; date of acceptance: June 3 2014.
AbstractFoot and ankle injuries are common and can have a significant effect on an individual’s daily activities. Nurses have an important role in the assessment, management, ongoing care and support of patients with ankle injuries. An understanding of the anatomy and physiology of the ankle enables nurses to identify significant injuries, which may result in serious complications, and communicate effectively with the multidisciplinary team to improve patient care and outcomes.
AuthorJennie WalkerClinical educator for musculoskeletal and neurosciences, Queen’s Medical Centre, Nottingham.Correspondence to: [email protected]
KeywordsAnkle and foot injuries, ankle fractures, fracture, physical examination, orthopaedic nursing
ReviewAll articles are subject to external double-blind peer review and checked for plagiarism using automated software.
OnlineFor related articles visit the archive and search using the keywords above.
To write a CPD article: please email [email protected] on writing for publication are available at:rcnpublishing.com/r/author-guidelines
4 Page 60 Ankle injuries multiple choice questionnaire
4 Page 61 Abby Morrow-Barnes’s reflective account on acute confusion
4 Page 62 Guidelines on how to write a reflective account
Prepare for revalidation:read this CPD article and write a reflective accounthttp://revalidation.zone
Aims and intended learning outcomesThe aim of this article is to provide the reader with an understanding of foot and ankle injuries, including the mechanism, assessment and management of these injuries. After reading this article and completing the time out activities you should be able to:�4Explain the anatomy of the foot and ankle.�4Describe the assessment of foot and ankle injuries.�4Describe fracture classification systems for ankle fractures.�4Discuss the management of soft tissue injuries.�4List potential complications associated with surgical and conservative treatments of ankle fracture.
IntroductionThe foot and ankle are major weight-bearing structures that have a vital role in activities of daily living. Nurses are instrumental in the assessment and management of patients with ankle injuries in the emergency department and in the community. Therefore, nurses require an understanding of the incidence of ankle injuries, common types of injury and treatment strategies to assist them in providing appropriate assessment and treatment (Mai and Cooper 2009).
Ankle injuries account for approximately 10% of visits to the emergency department (DiGiovanni et al 2004). The most common injury is an acute sprain (Mai and Cooper 2009). It is estimated that more than 300,000 people present to the emergency department with acute ankle sprains each year (Roche et al 2009). These injuries most frequently affect young people who are physically and professionally
© NURSING STANDARD / RCN PUBLISHING august 13 :: vol 28 no 50 :: 2014 53
active (Prado et al 2013). The term sprain is often used to describe soft tissue trauma of the ankle (Yammine and Fathi 2011). Timely diagnosis and treatment can prevent long-term complications such as mechanical instability, stiffness and degenerative changes including osteoarthritis (Ekinci et al 2013). Mismanagement of acute strains can lead to persistent symptoms following the initial injury, including mechanical instability, recurrent swelling, and stiffness and long-term degenerative changes (Mai and Cooper 2009).
Ankle fractures are one of the most common bony injuries to the lower extremity and are a signifi cant source of morbidity for young and older people (Anderson et al 2008). Fractures often involve considerable damage to soft tissues, blood vessels, muscles and ligaments.
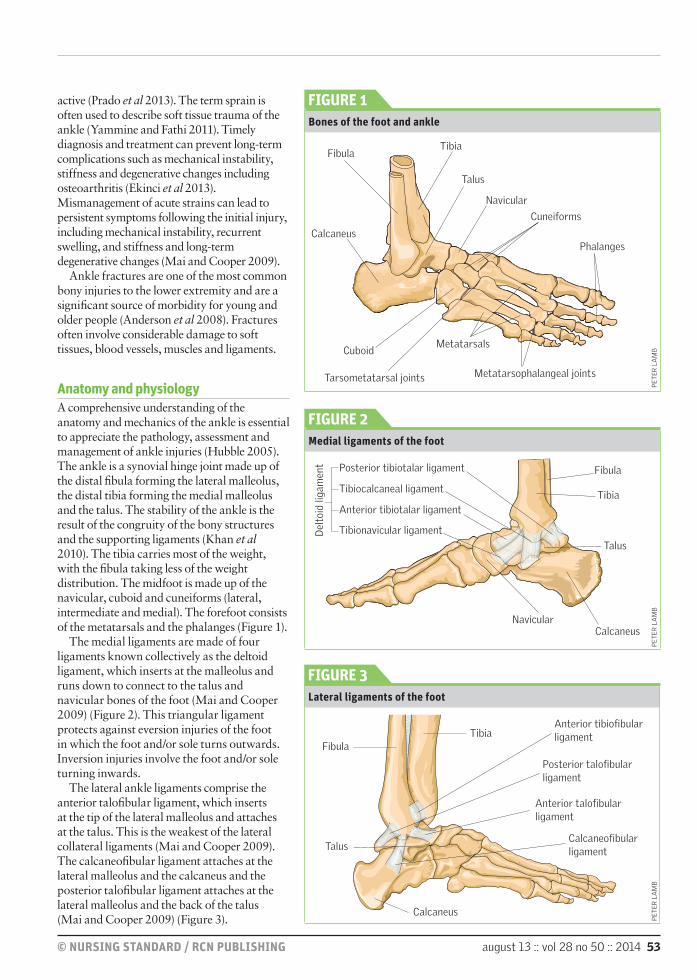
Anatomy and physiologyA comprehensive understanding of the anatomy and mechanics of the ankle is essential to appreciate the pathology, assessment and management of ankle injuries (Hubble 2005). The ankle is a synovial hinge joint made up of the distal fi bula forming the lateral malleolus, the distal tibia forming the medial malleolus and the talus. The stability of the ankle is the result of the congruity of the bony structures and the supporting ligaments (Khan et al 2010). The tibia carries most of the weight, with the fi bula taking less of the weight distribution. The midfoot is made up of the navicular, cuboid and cuneiforms (lateral, intermediate and medial). The forefoot consists of the metatarsals and the phalanges (Figure 1).
The medial ligaments are made of four ligaments known collectively as the deltoid ligament, which inserts at the malleolus and runs down to connect to the talus and navicular bones of the foot (Mai and Cooper 2009) (Figure 2). This triangular ligament protects against eversion injuries of the foot in which the foot and/or sole turns outwards. Inversion injuries involve the foot and/or sole turning inwards.
The lateral ankle ligaments comprise the anterior talofi bular ligament, which inserts at the tip of the lateral malleolus and attaches at the talus. This is the weakest of the lateral collateral ligaments (Mai and Cooper 2009). The calcaneofi bular ligament attaches at the lateral malleolus and the calcaneus and the posterior talofi bular ligament attaches at the lateral malleolus and the back of the talus (Mai and Cooper 2009) (Figure 3).
FIGURE 1 Bones of the foot and ankle
TibiaFibula
Fibula
Talus
Talus
Navicular
Cuneiforms
Metatarsals
Metatarsophalangeal joints
PhalangesCalcaneus
Cuboid
Tarsometatarsal joints
Fibula
TibiaAnterior tibiofi bular ligament
Posterior talofi bular ligament
Anterior talofi bular ligament
Calcaneofi bular ligament
Talus
Calcaneus
Calcaneus
Tibia
Navicular
Tibionavicular ligament
Anterior tibiotalar ligament
Tibiocalcaneal ligament
Posterior tibiotalar ligament
Del
toid
liga
men
t
FIGURE 2Medial ligaments of the foot
FIGURE 3 Lateral ligaments of the foot
PE
TE
R L
AM
B
PE
TE
R L
AM
B
PE
TE
R L
AM
B

54 august 13 :: vol 28 no 50 :: 2014 © NURSING STANDARD / RCN PUBLISHING
CPD orthopaedic nursing
A syndesmosis is an articulation where two bones are joined tightly by ligaments. The ankle syndesmosis consists of the intraosseous membrane, anterior and posterior tibiofibular ligaments (ATFL and PTFL) and the transverse ligament situated near the PTFL(McMullen 2004, Khan et al 2010). If the syndesmosis fails, the lateral malleolus displaces, resulting in an unstable ankle joint (Hubble 2005). The syndesmosis is a major ligament in Weber injury classification, a system of classifying ankle fractures (Weber 1972) (Figure 4).
The Achilles tendon attaches the gastrocnemius and soleus muscles in the calf to the calcaneus bone (Khan et al 2010), enabling people to walk, run and jump (Gibbons 2011).Complete time out activity 1
PathophysiologySoft tissue injurySoft tissue injuries can involve ligaments, tendons, synovial bursae and fascia. A sprained ankle occurs when one or more of the ligaments in the ankle is torn or partially torn. Many factors can predispose an individual to ankle injuries such as poor joint proprioception, slow muscular response to off-balance positions, running on uneven surfaces and lax ligaments. Ankle sprains can occur through excessive stress on the ligaments as a result of rotation (movement of the foot towards or away from the midline), inversion or eversion of the foot. When the foot is moved outside its normal range of motion, the excess force puts strain on the ligaments, which can damage or sprain the ligament. In some instances, an avulsion fracture may occur as a result of overstretching the ligaments and causing small fragments of bone to be pulled off (Larsen 2002).
Fractures of the foot and ankle can occur through various mechanisms of injury, such as direct forces causing fracture, crush injury as a result of direct trauma, stress or fatigue fractures caused by repetitive forces such as in long distance running or pathological fractures caused by disease processes such as cancer (Larsen 2002). Common mechanisms for ankle fractures include eversion, inversion, external rotation and vertical loading – for example jumping from a height (McMullen 2004). The use of corticosteroids may predispose patients to osteoporosis, which can increase the risk of fracture (Ralston and McInnes 2014).
Inversion injuries are the most common type of ankle sprain and account for the majority of ankle injuries (Mai and Cooper 2009).
Inversion of the ankle results in stretching of the ligaments on the lateral side of the foot, commonly the anterior talofibular ligament and the calcaneofibular ligament (Figure 3). Since inversion of the ankle often includes combination of movements such as dorsiflexion and rotation (Larsen 2002), it is important to establish what the patient was doing at the time to identify which structures may have been injured in the process. Eversion injuries are much less common and characteristically result in medial ankle sprain (Clare 2004).
Ligament injuries are often categorised in accordance with their severity as follows (Prado et al 2013):�4Grade 1 – spraining of the ligament, slight stretching of the ligament with some damage.�4Grade 2 – partial injuries without joint instability, partial tearing of the ligament.�4Grade 3 – complete injury with compromised joint stability, complete tear of the ligament.
A mild sprain would be classed as grade 1 and a severe strain would be grade 3.
FracturesA fracture is the loss of continuity of bone. There are several common types of fracture in the foot. One of the most common injuries to the metatarsals is an avulsion injury to the base of the fifth metatarsal, which is misdiagnosed commonly as an ankle sprain (Larsen 2002). Most ankle fractures are malleolar, with 60-70% being unimalleolar, and the most common injured part being the distal fibula (Ekinci et al 2013).
Ankle fractures can also be classified to describe the extent of the injury and the stability of the joint. Different methods have been used to classify ankle injuries; the two most common systems include the Lauge-Hansen (Lauge-Hansen 1950) and Danis-Weber (Weber 1972) systems.
The Lauge-Hansen (1950) classification system focuses on the trauma mechanism using two words: the first word describes the position of the foot at the time of the injury and the second word describes the direction of the deforming force (Khan et al 2010). Each classification has progressive stages of injury. Injuries are classified as supination-adduction (stages 1-2), supination-eversion (stages 1-4), pronation-abduction (stages 1-3), and pronation-eversion (stages 1-4) (Nielsen et al 1990). This classification system is not used frequently.
The Danis-Weber classification system (Weber 1972) categorises ankle fractures
1 Consider the different ankle injuries that you have seen or experienced. Think about how the injury occurred (mechanism of injury) and what structures were involved in the injury. 2 Investigate the
different classification systems for ankle injuries – which do you find the easiest to use? The following website may be helpful in visualising the different stages of injuries: http://tinyurl.com/ankleinjuries Find out what system is used in your local area.
TIM
CO
UG
HLI
N
© NURSING STANDARD / RCN PUBLISHING august 13 :: vol 28 no 50 :: 2014 55
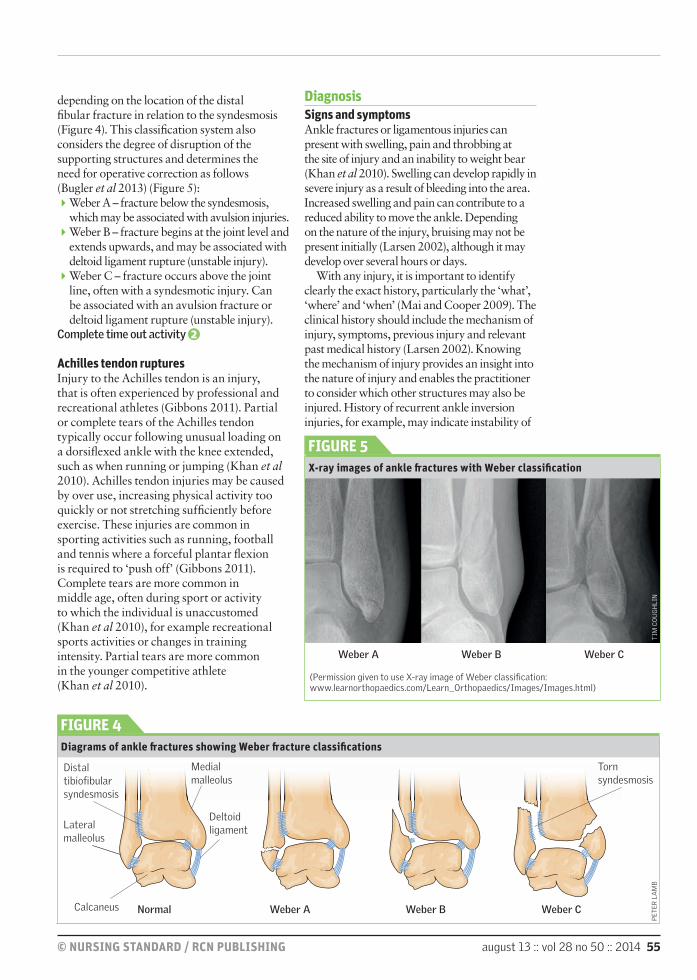
depending on the location of the distal fi bular fracture in relation to the syndesmosis (Figure 4). This classifi cation system also considers the degree of disruption of the supporting structures and determines the need for operative correction as follows (Bugler et al 2013) (Figure 5):�4Weber A – fracture below the syndesmosis, which may be associated with avulsion injuries.�4Weber B – fracture begins at the joint level and extends upwards, and may be associated with deltoid ligament rupture (unstable injury).�4Weber C – fracture occurs above the joint line, often with a syndesmotic injury. Can be associated with an avulsion fracture or deltoid ligament rupture (unstable injury).
Complete time out activity 2
Achilles tendon rupturesInjury to the Achilles tendon is an injury, that is often experienced by professional and recreational athletes (Gibbons 2011). Partial or complete tears of the Achilles tendon typically occur following unusual loading on a dorsifl exed ankle with the knee extended, such as when running or jumping (Khan et al 2010). Achilles tendon injuries may be caused by over use, increasing physical activity too quickly or not stretching suffi ciently before exercise. These injuries are common in sporting activities such as running, football and tennis where a forceful plantar fl exion is required to ‘push off’ (Gibbons 2011). Complete tears are more common in middle age, often during sport or activity to which the individual is unaccustomed (Khan et al 2010), for example recreational sports activities or changes in training intensity. Partial tears are more common in the younger competitive athlete (Khan et al 2010).
DiagnosisSigns and symptoms Ankle fractures or ligamentous injuries can present with swelling, pain and throbbing at the site of injury and an inability to weight bear (Khan et al 2010). Swelling can develop rapidly in severe injury as a result of bleeding into the area. Increased swelling and pain can contribute to a reduced ability to move the ankle. Depending on the nature of the injury, bruising may not be present initially (Larsen 2002), although it may develop over several hours or days.
With any injury, it is important to identify clearly the exact history, particularly the ‘what’, ‘where’ and ‘when’ (Mai and Cooper 2009). The clinical history should include the mechanism of injury, symptoms, previous injury and relevant past medical history (Larsen 2002). Knowing the mechanism of injury provides an insight into the nature of injury and enables the practitioner to consider which other structures may also be injured. History of recurrent ankle inversion injuries, for example, may indicate instability of
FIGURE 4 Diagrams of ankle fr actures showing Weber fr acture classifi cations
Normal Weber A Weber B Weber C
Weber A Weber B Weber C
FIGURE 5 X-ray images of ankle fr actures with Weber classifi cation
(Permission given to use X-ray image of Weber classifi cation: www.learnorthopaedics.com/Learn_Orthopaedics/Images/Images.html)
Distal tibiofi bular syndesmosis
Medial malleolus
Deltoid ligamentLateral
malleolus
Calcaneus
Torn syndesmosis
PE
TE
R L
AM
B

56 august 13 :: vol 28 no 50 :: 2014 © NURSING STANDARD / RCN PUBLISHING
CPD orthopaedic nursing
the lateral ligaments of the foot (Larsen 2002).During the initial assessment of an ankle injury, it is important to differentiate between fractures and strains. Assessing the severity of the pain and the ability to walk at any time since the injury are useful indicators of the extent of the injury. It is important to enquire about the force of the injury, because fractures sustained from low impact or weak forces may be an indication of osteoporosis (Ralston and McInnes 2014). This information, coupled with that of the mechanism of injury, can be particularly useful. For example, a patient who injured an ankle the previous day by falling over in high heels, and who continued to weight bear, but presents with swelling and inability to weight bear is less likely to have the same degree of injury as someone who injured his or her ankle playing rugby and has been unable to weight bear on it since. In Achilles tendon injuries, the patient often describes hearing a sudden ‘pop’ and experiences pain and swelling across the tendon; the pain is commonly likened to being hit across the back of the ankle with a stick (Gibbons 2011).
Identifying the time of injury and any first aid measures implemented, such as ice to reduce swelling, is part of thorough history taking. Enquiring about the place where the injury occurred can also identify other important factors such as risk of contamination of wounds. For example, a person with open wounds sustained in a field will require tetanus immunisations if he or she has not previously completed the recommended immunisation programme. If the patient has fallen, causative factors for the fall may need to be considered. Social factors should also be assessed to identify how the patient will cope with the injury, such as climbing stairs and doing the shopping. Referral to the multidisciplinary team may be required for further assessment.
Clinical examinationInspection should begin with assessing whether the patient is able to walk. If the patient is able to mobilise, there is likely to be an antalgic gait. Being able to walk on an injured ankle decreases the likelihood of serious injury but does not completely rule out the risk of fracture (Mai and Cooper 2009). Both legs should be exposed to allow for comparison of one ankle with the other, which should involve inspection of all aspects of the ankle and the knee (Larsen 2002). The clinician should inspect for signs of swelling, bruising, deformity, cyanosis,
pallor or breaks in the skin (Hubble 2005). The Achilles tendon should be examined for signs of misalignment, swelling or a visible gap in the tendon. Deformity or misalignment of the foot may indicate fracture or dislocation. Different patterns of colouration or discolouration between the feet may indicate vascular compromise, either as a result of compression of the blood vessels, or bleeding. Swelling is common directly over the site of injury, although extensive swelling should alert the clinician as it can put the limb at risk of compartment syndrome. Significant swelling should be monitored carefully because undetected and unmanaged compartment syndrome can result in severe consequences for the patient such as amputation of the limb (Lintz et al 2011).Complete time out activity 3
The aim of palpation is to determine the maximum point of tenderness and to distinguish between soft tissue and bony tenderness to decide if an X-ray is required. It is useful to start with areas that are not swollen or bruised, because the patient may be unwilling to continue with the examination once pain is elicited (Mai and Cooper 2009). The main areas to palpate include medial and lateral malleoli, the base of the fifth metatarsal, metatarsophalangeal joints, phalanges and the heel. In Achilles tendon injuries, there may be a palpable deficit in the tendon with weak plantar flexion and a positive Thompson test, also known as a Simmonds’ test. During this test, the patient lies prone with the feet hanging free off the end of the examination couch. On squeezing the calf of the unaffected ankle, there should normally be dorsiflexion of the ankle. Squeezing the calf of the affected side will not result in movement of the foot. This lack of movement is considered a positive test and likely to signify a rupture of the Achilles tendon. Poor anatomical knowledge and technique can lead to inaccurate examination of the foot and ankle, which can lead to inaccurate diagnosis and inappropriate treatment of the injury (Roche et al 2009).
Neurovascular assessment includes testing pulses, sensation and movement. Increased temperature may be the result of swelling and erythema or infection, whereas coolness may indicate ischaemia and should be checked with pedal pulses and capillary refill time tests (the skin is pressed with a finger until it blanches, and when the pressure is released the time taken for

© NURSING STANDARD / RCN PUBLISHING august 13 :: vol 28 no 50 :: 2014 57
the skin to reperfuse and return to its normal colour is documented – this should be less than two seconds) (Mai and Cooper 2009). Normal ankle movements consist of plantar flexion, dorsiflexion, eversion and inversion. Range of movement should be assessed actively and passively, unless a fracture is suspected (Hubble 2005). Active movements should be performed initially by the patient, and then movements can be performed passively by the examiner. Affected ankle movements should be compared with the unaffected ankle to determine any difference, along with movements above or below the injured site (Larsen 2002). In acute injury, the range of movement may be reduced as a result of pain and swelling. It is important to remember there is a difference between not being able to move the joint and produce movement and not moving as a result of pain (Mai and Cooper 2009).
Ottawa foot and ankle rulesThe Ottawa foot and ankle rules (Stiell et al 1992) were developed to rationalise the use of radiography in the assessment of ankle injuries in patients over 18 years. Exclusion factors other than age used in the initial study included pregnancy, isolated injuries of the skin (lacerations, abrasions or burns) or if the injury had occurred more than ten days previously (Stiell et al 1992). The Ottawa foot and ankle rules are used by practitioners to determine the need for X-ray in patients with an ankle injury by helping to differentiate between fractures of the ankle and mid-foot from other ankle injuries that do not require X-ray (Hubble 2005). Caution is required in patients who are intoxicated, who have other distracting painful injuries or who have decreased sensation in their legs. Ankle X-ray series are required only if there is pain in the malleolar zone and any one of the following (Stiell et al 1995):�4Bone tenderness along the distal 6cm of the posterior edge of the fibula or tip of the lateral malleolus.�4Bone tenderness along the distal 6cm of the posterior edge of the tibia or tip of the medial malleolus.�4Inability to bear weight both immediately and in the emergency department.
Some injuries, however, may not be visible using X-rays and may require further imaging, such as magnetic resonance imaging, to rule out ligament injury (Yammine and Fathi 2011). Ultrasound has been used for many years to examine musculoskeletal tissues because it allows detection of small changes that may
occur (Ekinci et al 2013). Ultrasound imaging is particularly useful when assessing tendonitis or ruptures of the Achilles tendon.
ManagementThe initial goal of managing ankle injuries is to minimise pain, decrease swelling and keep the injury from extending (Mai and Cooper 2009). Initial management may use the mnemonic RICE (Rest, Ice, Compression, Elevation). In some areas, this mnemonic may also include ‘Protection’ to make PRICE. The aim of compression is to reduce haemorrhage and oedema in the surrounding area. This works on the principle that reducing swelling will reduce pain in the ankle and allow a greater range of movement, encouraging a quicker return of normal ankle movement (Pollard and Cronin 2005). The use of compression in managing injuries remains controversial and is not universally applied. Watts and Armstrong (2001) conducted a randomised controlled trial to determine the effectiveness of compression in mild to moderate ankle sprains. The study did not demonstrate a difference in functional recovery time, although there was an increase in analgesia use in patients receiving compression. Elevating the injured ankle also aims to reduce swelling since this prevents pooling of the blood in the lower extremity (Mai and Cooper 2009). Cryotherapy is best obtained by applying ice packs to the ankle with a thin layer of clothing or material protecting the skin. Length of time and frequency vary, but cryotherapy is often used for 15–30 minutes at a time, several times a day for the first 36–48 hours after the injury (Mai and Cooper 2009).
The stability of the ankle is the main determinant of prognosis and definitive management (Khan et al 2010). Stable injuries can be managed conservatively and non-operatively, whereas unstable injuries may require surgical intervention. Stable injuries may be immobilised with a below-knee back slab or partial cast, which may be made into a full cast when the swelling has subsided (Khan et al 2010). Splints and orthotic devices may be used as an alternative to traditional casting techniques.Complete time out activity 4
Both casts and splints immobilise injuries to promote healing and maintain alignment. Splints can be quicker to apply than traditional
3 Find out what tools are available in your area to assess the neurovascular status of the patient’s limb following a fracture or injury. An example of an assessment tool can be found using the following weblink: http://tinyurl.com/NeuroVasAssessment Think about what actions you should take if you are concerned about ischaemia or compartment syndrome. 4 Find out which
techniques are used in your local area to immobilise ankle injuries. List the advantages and disadvantages of each method?

58 august 13 :: vol 28 no 50 :: 2014 © NURSING STANDARD / RCN PUBLISHING
CPD orthopaedic nursing
casts and have the advantage that they can be removed easily for inspection of the skin or wounds and for examination or X-ray. Splints may be static or dynamic (allowing controlled movement), which provides more treatment flexibility. Disadvantages of splints can include excessive movement at the injury site if the splint is not applied correctly or the patient is not compliant with the splint instructions. There are also limitations in splint application as a result of the ready made state and lack of ability to cater for every injury. Casting, however, provides individualised treatment for each patient and injury and, therefore, offers effective immobilisation. Complications of casting include compartment syndrome and pressure ulcers, so it is important that casts are applied by practitioners with appropriate skills and knowledge and, ideally, who have attended specialist training (Larsen 2002, British Orthopaedic Association 2014).
Displaced or extensive fractures and injuries with syndesmotic widening are indictors for surgical fixation (Khan et al 2010). Non-surgical management of complex injuries may result in malunion, non-union, reduced range of motion at the ankle joint and reduced ankle function scores (Anderson et al 2008). Open reduction and internal fixation can restore articular congruity, for example, although such practices are associated with other intra-operative risks, infection and damage to nerves and surrounding structures (Howard et al 2003). There are additional challenges for older patients with trauma, in particular decreased bone quality as a result of pathologies such as osteoporosis or osteomalacia, which make fracture fixation and fracture healing more complex (Anderson et al 2008). Older patients are also more likely to have poorer pre-operative health, with an increased number of comorbidities, which can correlate with higher peri-operative complications (Anderson et al 2008). It is important to identify potential complications during initial and pre-operative assessments to ensure adequate preparation for surgery and that appropriate post-discharge support is in place.
Complete immobilisation of the ankle will result in decreased ankle strength and flexibility as a result of lack of use. It is important that, following removal of immobilisation devices or surgical fixation, patients are assessed by physiotherapists to help regain ankle strength and flexibility and aided in order to optimise function. In the early stages after injury, the
initial focus of rehabilitation may be as simple as increasing the range of movement as the pain decreases. Introducing exercises after ankle sprains will help to strengthen the ankle, increase ankle stability and speed up the recovery process. Effective rehabilitation and strengthening of the ankle will also help to reduce the risk of future injury. Rehabilitation following ankle injury can be a lengthy process and should ideally be overseen by a physiotherapist or sports therapist.Complete time out activity 5
In many areas of work, nurses assess patients with ankle injuries, request X-rays and diagnose the injury. Derksen et al (2007) demonstrated that nurses are capable of assessing and treating patients with foot and ankle trauma at least as accurately as junior doctors. The use of nurse practitioners in the emergency department has been shown to be an effective strategy in reducing patient waiting times (Derksen et al 2007).
Nurses are ideally placed to assess patient needs and offer holistic care and support. Assessment of patients’ social circumstances, employment, living circumstances and activities of daily living are an important part of managing ankle injuries, since assessment of needs and delivery of appropriate care may have a significant effect on patient outcome and experience (Hubble 2005). The effects of ankle injuries on the ability to carry out activities of daily living should not be underestimated, especially in the older person who may not have extensive social support.
It is important to assess the patient’s pain and ensure adequate pain relief is available because poor pain control can hinder recovery (Lin et al 2008). The nurse should also assess the risk of pressure ulcers, particularly in the older person who may be at increased risk of developing complications as a result of reduced mobility. The risk of venous thromboembolism (VTE) is increased as a result of immobility, although it may be further increased with the use of plaster casts and splinting devices, as with orthopaedic surgery (National Institute for Health and Care Excellence 2010). The use of mechanical and pharmacological preventive strategies should be considered carefully in any patients with an increased VTE risk to ensure that appropriate preventive methods are implemented.
Providing written information, in addition to verbal information, can be particularly useful because it will give the patient time to
5 Find written information on exercises that can be used following an ankle sprain or ankle injury. How useful do you think these exercises are? The following website may be helpful: http://tinyurl.com/ankleexercises

© NURSING STANDARD / RCN PUBLISHING august 13 :: vol 28 no 50 :: 2014 59
process the type and management of the injury, physiotherapy exercises, care of the cast or splint, medication and any follow-up details.
ConclusionFoot and ankle injuries are common. Nurses have a multifaceted role in the assessment, diagnosis and management of such injuries, supporting patients through
the rehabilitation process. Understanding the pathophysiology and mechanisms of injury will help practitioners assess and manage foot and ankle injuries in an appropriate manner and communicate effectively with the multidisciplinary team. An awareness of the risks and complications associated with injury and of appropriate treatment strategies will help to optimise patient care NSComplete time out activity 6
ReferencesAnderson SA, Li X, Franklin P, Wixted JJ (2008) Ankle fractures in the elderly: initial and long-term outcomes. Foot & Ankle International. 29, 12, 1184-1188.
British Orthopaedic Association (2014) The Role of the Orthopaedic Technician/Casting Room Nurse. www.boa.ac.uk/events/ciancasting-room-nurse (Last accessed: July 16 2014.)
Bugler KE, White TO, Thordarson DB (2013) Ankle Fractures. tinyurl.com/pj8qv3q (Last accessed: July 16 2014.)
Clare M (2004) Ankle sprains and instability. In Brown DE, Neumann RD (Eds) Orthopedic Secrets. Third edition. Hanley & Belfus, Philadelphia PA, 389-394.
Derksen RJ, Coupé VM, van Tulder MW, Veenings B, Bakker FC (2007) Cost-effectiveness of the SEN-concept: Specialized Emergency Nurses (SEN) treating ankle/foot injuries. BMC Musculoskeletal Disorders. 8, 99.
DiGiovanni BF, Partal G, Baumhauer JF (2004) Acute ankle injury and chronic lateral instability in the athlete. Clinics in Sports Medicine. 23, 1, 1-19.
Ekinci S, Polat O, Günalp M, Demirkan A, Koca A (2013) The accuracy of ultrasound evaluation in foot and ankle trauma. American Journal of Emergency Medicine. 31, 11, 1551-1555.
Gibbons L (2011) Diagnosing Achilles tendon injuries in the
emergency department. Emergency Nurse. 21, 5, 26-30.
Howard JL, Buckley R, McCormack R, Pate, G, Leighton R, Petrie D, Gaplin R (2003) Complications following management of displaced intra-articular calcaneal fractures: a prospective randomised trial comparing open reduction internal fixation with nonoperative management. Journal of Orthopaedic Trauma. 17, 4, 241-249.
Hubble C (2005) Ankle fractures. Emergency Nurse. 13, 4, 32-38.
Khan W, Oragui E, Akagha E (2010) Common fractures and injuries of the ankle and foot: functional anatomy, imaging, classification and management. Journal of Perioperative Practice. 20, 7, 249-258.
Larsen D (2002) Assessment and management of foot and ankle fractures. Nursing Standard. 17, 6, 37-46.
Lauge-Hansen N (1950) Fractures of the ankle II. Combined experimental-surgical and experimental-roentgenologic investigations. Archives of Surgery. 60, 5, 957-985.
Lin C, Moseley A Refshauge K (2008) Rehabilitation for ankle fractures in adults. Cochrane Database of Systematic Reviews. Issue 3, CD005595.
Lintz F, Colombier J-A, Letenneur J, Gouin F (2011) Management of foot and ankle sequelae of acute compartment
syndrome of the leg. British Journal of Bone and Joint Surgery. 93B, Supp IV, 496-497.
Mai N, Cooper L (2009) Assessment of ankle injuries. Journal of School Nursing. 25, 1, 34-39.
McMullen ST (2004) Foot and ankle trauma. In Brown DE, Neumann RD (Eds) Orthopedic Secrets. Third edition. Hanley & Belfus, Philadelphia PA, 394-397.
National Institute for Health and Care Excellence (2010) Venous Thromboembolism: Reducing the Risk. Reducing the Risk of Venous Thromboembolism (Deep Vein Thrombosis and Pulmonary Embolism) in Patients Admitted to Hospital. Clinical guideline No. 92. NICE, London.
Nielsen J, Dons-Jenson H, Sørensen H (1990) Lauge-Hansen Classification of Malleolar Fractures: An Assessment of the Reproducibility in 188 Cases. tinyurl.com/m597286 (Last accessed: July 16 2014.)
Pollard A, Cronin G (2005) Compression bandaging for soft tissue injury of the ankle: a literature review. Emergency Nurse. 13, 6, 20-25.
Prado MP, Fernandes TD, Camanho GL, Mendes AAM, Amodio DT (2013) Mechanical instability after acute ankle ligament injury: randomized prospective comparison of two forms of conservative treatment. Revista Brasileira de Orthopedia. 48, 4, 307-316.
Ralston S, McInnes I (2014) Rheumatology and bone disease. In Walker B, Colledge N, Ralston S, Penman I (Eds) Davidson’s Principles & Practice of Medicine. 22nd edition. Churchill Livingstone Elsevier, Edinburgh, 1057-1136.
Roche A, Hunter L, Pocock N, Brown D (2009) Physical examination of the foot and ankle by orthopaedic and accident and emergency clinicians. Injury. 40, 2, 136-138.
Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR (1992) A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Annals of Emergency Medicine. 21, 4, 384-390.
Stiell I, Wells G, Laupacis A et al (1995) Multicentre trial to introduce the Ottawa ankle rules for the use of radiography in acute ankle injuries. British Medical Journal. 311, 7005, 594-597.
Watts B, Armstrong B (2001) A randomised control trial to determine the effectiveness of double Tubigrip in grade 1 and 2 (mild to moderate) ankle sprains. Emergency Medicine Journal. 18, 1, 46-50.
Weber BG (1972) Die Verletzungen des Oberen sprunggelenkes. Second edition. Verlag Hans Huber, Bern.
Yammine K, Fathi Y (2011) Ankle “sprains” during sport activities with normal radiographs: incidence of associated bone and tendon injuries on MRI findings and its clinical impact. Foot. 21, 4, 176-178.
6 Now that you have completed the article, you might like to write a reflective account. Guidelines to help you are on page 62.