cover note - scripps institution of oceanography · cover note project synopsis ... from wood...
TRANSCRIPT

Cover Note
Project SynopsisThis report describes a health impact assessment (HIA) conducted to quantify the potential health benefitsas they relate to particulate matter (PM) pollution from wood burning, focusing on a case study withinAthens, Greece. The study includes a comprehensive and systematic literature review identifying relevantintervention studies that focused on wood burning strategies effects on ambient PM pollution. The datafrom the resulting studies were statistically pooled into a single range of effectiveness, and combined withAthens air quality data and peer-reviewed studies within Athens to assess the potential health benefits ofsuch wood-burning mitigation. The deliverable, in form of this report, is intended to facilitate the transferof information from scientists to local policy and decision-makers, humanitarian bodies, and citizens and aidin informed decision making, with a specific emphasis on inequity. In the context of Athens, this report fillsa knowledge gap in terms of conducting a literature review related to effectiveness of wood burning inter-ventions to reduce ambient PM, and will be background research for a specific strand of an European Unionproject, title "Smart Urban Solutions for air quality, disasters, & city growth, described herein. Furthermore,this report combines evidence from a multitude of perspectives, such as environmental, social, economic andhealth, which is necessary to argue for a policy in Greece’s current social and economic situation.
Risks & BarriersThroughout the course of this project, the central barrier was in the form of data limitations. The finerparticles emitted from wood burning, such as PM2.5, are considered to be of great concern due to adversehealth effects (i.e. further penetration into the lungs). Unfortunately, measurements of PM2.5 are sparseand relatively unreliable in Athens, and therefore, the following study utilized PM10 measurements instead.This focus on PM10 is justifiable since it is inclusive of finer particulate matter and due to the similarities inreduction resulting from the compared intervention studies selected from the systematic literature review,regardless of if they focused on measuring ambient PM10 or PM2.5. Furthermore, the PM data representscontribution from all sources, such as transportation, mobile, dust, etc., and is not solely representative ofPM emissions from wood burning. Nevertheless, the relative change in PM due to an intervention strategyreducing the pollutant from wood-burning would be directly attributable to this specific source, controllingfor the other sources contribution. If effective, reducing PM from wood burning will decrease the totalPM levels. Another risk to synthesizing data from intervention studies from around the world is that theregions may be dissimilar to Athens, but this was managed through performing a meta-analysis to reach astatistically powerful pooled estimate of PM reduction due to the interventions, comparing and contrast-ing the different regions, and conducting a sensitivity analysis to ensure that the variances were accounted for.
Dissemination & Project SustainabilityThe project has a long-term sustainability plan, along with a specific opportunity for dissemination. Aspreviously mentioned, it serves as phase zero background research for the larger EU project and will beuseful in identifying knowledge and data gaps, outlining a road map of needs for a more complete study tobe pursued in the long-term project. I will present on my Capstone research at the 3rd Annual InternationalPublic Health Conference in Athens, Greece hosted by the Athens Institute for Education and Researchfrom June 19-22, 2017. This gives me the unique opportunity to present my findings as well as personallydisseminate my report to my target audience.

Potential health co-benefits related tomitigation of air pollution from woodburning: A systematic review & healthimpact assessment case study in Athens,
Greece
Jennifer Bailey
June 2017
Declaration of Authorship
Jennifer BaileyMaster’s of Advanced Studies in Climate Science & PolicyScripps Institution of OceanographyUniversity of California, San DiegoContact: [email protected] linkedin.com/in/jennifer-bailey
Acknowledgments
I would like to thank all of the members of my Capstone Advisory Committee for all of the guidance andinput regarding the project’s design, development and production. I am also very grateful for the feedbackand companionship provided by the MAS CSP Cohort over the course of this year. I would like to expressparticular gratitude to Dr. Tarik Benmarhnia for his immense help and insight in every step of producingthis project, and to Dr. Evangelos Gerasopoulos and his colleagues for their willingness to provide me withdata, comments, and a local perspective. Lastly, I want to thank Amy Butros for being so helpful andlending her database and keyword expertise.
Capstone Advisory Committee (CAC) Approval
The following report has been completed under the supervision of the following CAC members, with approvalfor submittal indicated by the signatures of the Committee Chair and Expert Advisor.
Tarik Benmarhnia, PhD | Committee Chair & Expert AdvisorProfessor, Climate, Atmospheric Science, and Physical Oceanography & Family Medicine and Public Health,Scripps Institution of Oceanography, University of California, San Diego
Evangelos Gerasopoulos, PhD | Expert AdvisorResearch Director, Institute for Environmental Research & Sustainable Development, National Observatoryof Athens
Laurel Hunt | Committee MemberDirector of Strategic Partnerships & Secretary, Mediterranean Cities Climate Change Consortium (MC-4),Center for Urban Resilience, Loyola Marymount University
Ellie Farahani, PhD | Committee MemberExecutive Director, MAS CSPScripps Institution of Oceanography, University of California, San Diego
Lynn Russell, PhD | Committee MemberProgram Director, MAS CSPScripps Institution of Oceanography, University of California, San Diego

ContentsList of Figures i
List of Tables i
List of Acronyms & Abbreviations ii
List of Units ii
Executive Summary 1
1 Introduction 2
2 Health Impact Assessment Approach 4
3 Results 63.1 Study Selection & Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63.2 HIA Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63.3 Sensitivity Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
4 Discussion 84.1 Athens, Greece: A Case Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
4.1.1 Air Quality: Particulate Matter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94.1.2 Wood Burning for Residential Heating . . . . . . . . . . . . . . . . . . . . . . . . . . . 114.1.3 Health Impacts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134.1.4 Economic Viability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
5 Conclusion 16
References 17
Appendices 22

List of Figures
Figure 1: Co-benefits of energy efficiency programs related to wood burning 4
Figure 2: Map displaying locations of wood burning interventions 7
Figure 3: Meta-analysis results 8
Figure 4: HIA calculation methodology and main analysis results 9
Figure 5: Sensitivity analysis results 10
Figure 6: Wintertime daily average PM10 concentrations in Athens, Greece 11
Figure 7: Regional dust loads during maximum wintertime PM concentrations in Athens, Greece 12
Figure 8: Simulation results of intervention policies on total population and low and high SES groups 15
Figure 9: Systematic review study selection flow chart 23
Figure 10: HIA methodology and results from the secondary analysis 26
Figure 11: Graph displaying daily average PM10 levels in Athens, Greece 28
Figure 12: Map displaying locations of PM10 monitoring stations in Athens, Greece 29
List of Tables
Table 1: Literature Review Table 24
Table 2: Information regarding PM10 monitoring stations in Athens, Greece 27
i

List of Acronyms & Abbreviations
AP . . . . . . . . . . . . . . Air pollution
BAU . . . . . . . . . . . . Business as usual
BC . . . . . . . . . . . . . . Black carbon
CAC . . . . . . . . . . . . Capstone Advisory Committee
CI . . . . . . . . . . . . . . . Confidence interval
CO . . . . . . . . . . . . . . Carbon monoxide
CO2 . . . . . . . . . . . . . Carbon dioxide
CSP . . . . . . . . . . . . . Climate Science & Policy
ERF . . . . . . . . . . . . . Exposure response function
EU . . . . . . . . . . . . . . European Union
GBD . . . . . . . . . . . . Global Burden of Disease
GDP . . . . . . . . . . . . Gross domestic product
GHG . . . . . . . . . . . . Greenhouse gas
HIA . . . . . . . . . . . . . Health Impact Assessment
IPCC . . . . . . . . . . . . Intergovernmental Panel on Climate Change
MAS . . . . . . . . . . . . Master of Advanced Studies
PAF . . . . . . . . . . . . . Population attributable fraction
PAH . . . . . . . . . . . . . Polycyclic aromatic hydrocarbons
PM . . . . . . . . . . . . . . Particulate matter
PM2.5 . . . . . . . . . . . Particulate matter with a diameter of 2.5 micrometers or less
PM10 . . . . . . . . . . . . Particulate matter with a diameter of 10 micrometers or less
ROI . . . . . . . . . . . . . Return on investment
RR . . . . . . . . . . . . . . Relative risk or risk ratio
SES . . . . . . . . . . . . . . Socioeconomic status
SMURBS . . . . . . . Smart Urban Solutions for air quality, disasters, & city growth
WHO . . . . . . . . . . . World Health Organization
List of Units
µm . . . . . . . . . . . . . . Micrometer
µg/m3 . . . . . . . . . . Micrograms per cubic meter
ii

Executive Summary
Moving into the future as the climate changes and urban populations grow, it is increasingly importantto evaluate mitigation policies to diminish the impact of greenhouse gases (GHG), other trace gases andpollutants on a warming planet and to do so in a way that protects vulnerable populations. According tothe Intergovernmental Panel on Climate Change (IPCC), 47% of the increase in annual anthropogenic GHGemissions is directly due to energy supply, and without extensive efforts to mitigate and reduce, emissionswill continue to inflate as a result of global population growth and economic activities (IPCC, 2014b). Inorder to develop sustainably and preserve human health, source specific mitigation strategies are needed.
Athens, Greece is in the midst of an enduring economic crisis, which has led to an increase in wood burningas a less expensive method of residential heating in the winter, and at the same time is experiencing urbanpopulation pressure enhanced by refugees. Wood and biomass combustion results in particulate matter (PM)pollution that degrades air quality and has negative impacts to human health, with specific hazards to themost vulnerable. Reducing emissions from wood burning is a source-specific method to addressing air qualitydegradation, and indirectly climate change, through instituting policies aimed at human health co-benefits.
This study includes the results of a health impact assessment (HIA), which quantified the benefits to humanhealth as a result of intervention strategies to reduce PM pollution from wood burning activities, incorpo-rating Athens, Greece as an individual case study. A systematic review of approximately 7,000 documentsfrom the related peer-reviewed literature led to the inclusion of six applicable intervention studies. Extracteddata were utilized in a random effects meta-analysis to estimate a pooled reduction of 23% of PM due tothe intervention policies put in place in regards to wood burning. Using data from within Athens, Greece,an average of 0.44 (95% confidence interval (CI): 0.05-1.47) daily deaths could be prevented in Athens dueto a strategy reducing PM emissions from wood burning.
The impacts of such interventions were assessed through conducting a sensitivity analysis identifying thepotential for alleviation of premature deaths on members of lower socioeconomic status. While such apolicy would significantly prevent deaths from within the total population, the lower socioeconomic groupsexperienced on average 0.75 prevented daily average deaths compared to the 0.05 prevented deaths seen inthe high socioeconomic status groups. The results showed that a wood stove intervention policy has immensepotential to reduce average daily mortality, but to do so within the most disadvantaged groups, alleviatingenvironmental inequity.
Through incorporating Athens specific data, climate change co-benefits, social justice, and economic efficiencyin the assessment, the results support the far-reaching potential for an effective wood burning interventionpolicy in Athens. It is increasingly important to consider the myriad of co-benefits present in source-specificmitigation policies, especially in the context of Athens. The region is facing tough austerity measuresthreatening the quality of health care and social well-being and the increased presence of vulnerable groups,such as the high number of unemployed individuals (many of them youth) and refugees, whose status ofexclusion bring about disproportionate exposure to air pollution among other determinants of health andequity.
This risk assessment incorporates evidence from many fields to fully and quantitatively assess wood burninginterventions, and lay the basis for policies to be put in place that not only protect human health andmitigate emissions, but alleviate inequity and maximize benefits across sectors. The analysis within thisreport will help inform policy-makers with the initial evidence necessary to put progressive health policies inplace that will simultaneously and indirectly aid in environmental quality, emissions mitigation, and provecost-effective in a region under financial duress.
1

1 Introduction
The present and forthcoming impacts of climate change, primarily due to anthropogenic, or human-caused,emissions of greenhouse gases, pose significant hazards to the stability of natural and human systems. Scien-tists have been observing changes in the Earth’s climate, and have arrived at a consensus that the atmosphericGHG concentrations have skyrocketed, leading to increasingly warmer temperatures and rising sea levels,among other widespread impacts (IPCC, 2015). Carbon Dioxide (CO2), an abundant GHG, has surpassed400 parts per million, almost doubling since the pre-industrial era and for the first time since humans haveexisted (The Keeling Curve, 2017). A major contribution to GHGs and other pollutants, such as particulatematter, is through the burning of fossil fuels and the ways in which people produce and use energy. Theseemissions not only have complex interactions and implications for the changing climate system, but effecthuman and environmental health.
The basic requirements for maintaining health, such as clean air, safe drinking water, and availability offood, are drastically affected by a changing climate. The Global Burden of Diseases (GBD) study in 2015found that ambient PM2.5, particulate matter with a diameter sized 2.5 micrometers (µm) or less, ranked5th as a mortality factor, with exposure causing 4.2 million deaths in 2015 alone, corresponding to 7.6% ofthe total global deaths (Cohen et al., 2017). Sustainable development provides a framework for protectingthe improvements gained in health from economic development in the face of climate change, and cansimultaneously reduce inequity experienced by particular population groups that are more vulnerable.
The world’s population is projected to reach 9.7 billion people by the year 2050, growing from the currentglobal population of 7.3 billion (United Nations, Department of Economic and Social Affairs, PopulationDivision, 2015). Furthermore, people are concentrating in urbanized regions, causing the populations incities to surge. Significant negative impacts of climate change threaten urban regions directly throughincreasing heat, drought, and extreme weather events, and indirectly through scarcity of critical suppliesand resources, as well as poor air quality. Changing weather patterns resulting from climate change willhave regionally varying impacts on air quality. For example, reduced rainfall would increase the PM levelsin the atmosphere due to less efficient washout and higher resuspension (IPCC, 2014a). A common themeunderlying the burdens imposed by climate change is the profound effect on human health. As the changingclimate results in many complex relationships and unknowns in terms of environmental and human healthhazards, it must be a priority for communities to combat climate change through mitigation, adaptation,and resilience building.
The public health perspective of climate change has the opportunity to resonate deeply and bring a largergroup of actors together, such as climate scientists, human health experts, policy makers, and humanitarianbodies. Protecting the health and well-being of families and communities is a world-wide priority, and theeffects are more immediate and transparent in people’s daily lives compared to other climate mitigationapproaches. A multi-disciplinary approach to climate change, emphasizing human health, strengthens theargument for a need to act and harmonize goals to maximize health and environmental equity. Many articleshave explored the dual-opportunity that exists between reducing GHG emissions and pollutants and therelated improvements to human health (Watts et al., 2015; Cheng & Berry, 2013; Quam et al., 2017).Climate change mitigation policies that provide health co-benefits enhance the effectiveness and benefits ofthose strategies, even when quantified economically, resulting in a low or no-regret policy.
An approach to addressing climate change mitigation is to identify and reduce emissions from specific sources,such as transportation, combustion of fossil fuels, and energy systems. Air pollution (AP) as a result of theseprocesses contributes further to climate change, and considering health co-benefits of policies addressing airquality offsets the cost of climate change mitigation strategies and can occur in the short-term allowing forimproved local air quality (Bell et al., 2008). AP due to a variety of sources has become an increasinglyworrying problem, especially in populous regions where a wide variety of populations are exposed. In light ofthe growing understanding of causes of climate change, many countries and regions are turning to renewableor alternative energy sources.
Biomass (or wood) burning is an emerging and less understood source of pollution, in terms of processesinvolved and its contribution to global background levels. Wood is burned as a source of energy for heating
2

and cooking in both rural and urban settings, not being limited to solely developing or developed countriesand has more recently been considered a "carbon-neutral" energy source to be utilized as opposed to fossilfuels. The push for renewable energy has led to support of wood burning as a fuel source, or to produceelectricity, due to the offset between carbon emitted when the trees are cut down and subsequently burnedand the uptake of CO2 when replacement trees are planted. While the concept seems simple, scientistshave been divided due to the complex and potentially far-reaching effects of increased wood burning as amain energy source, such as increased logging degrading the biodiversity of forests, lag in time betweencarbon emissions and sequestration, and increased pollutants (Cornwall, 2017). Biomass energy has becomeprogressively popular throughout Europe, partially due to the European Union’s (EU) renewable energydirective, requiring 20% of energy consumption to be from renewable sources by 2020, with a major emphasison biomass energy (European Commission, 2009). Therefore, a trade-off exists between considering woodas a "carbon-neutral" energy source to be used in place of much more GHG intensive fossil fuels, its role inemitting other harmful pollutants, and the resulting impacts to environmental and human health.
As a result of burning organic matter, such as wood, smoke forms that is made up of gases (i.e. carbonmonoxide (CO), in addition to CO2), and fine particles, or particulate matter, with increased content oftoxic substances like polycyclic aromatic hydrocarbons (PAHs) and other organics. Additionally, blackcarbon (BC) is emitted largely from wood burning, as well as from the incomplete combustion of liquidfuels in vehicles, and is considered to be a major driver of climate forcing as BC is an efficient absorber ofsolar radiation, augmenting the current warming trend globally (IPCC, 2014a; Bond et al., 2013). ReducingBC can, therefore, have a cooling effect and contribute to near and long term mitigation of climate change.While all of these wood burning emissions have been linked to health impacts, particulate matter as a majorinhalable component of wood smoke is associated with short term and chronic mortality, as well as chronicexposure leading to a higher risk of respiratory and cardiovascular morbidity, and even lung cancer (Pope &Dockery, 2006; WHO, 2016).
Many policies that relate air pollution, specifically PM pollution, and mitigation have focused on trans-portation or industrial strategies, but it is clear that wood burning is a significant contributor to poor airquality in certain regions. AP from wood burning is well documented for indoor exposure, but wood andbiomass combustion also results in outdoor AP, which can have important implications for population healthsince outdoor AP impacts everyone whether or not they burn wood (Smith et al., 2014). Integrating humanhealth into policies that address certain pollutants from wood burning is an obvious strategy to alleviateclimate change contribution, while addressing local issues of air quality and degradation of human health.Furthermore, an opportunity exists to address inequity in exposure experienced by subsets of the population,particularly groups of lower socioeconomic class, certain ages, genders and health status. It is establishedwithin the literature that health is progressively better the high socioeconomic position of the person, andthat socially created vulnerabilities, such as race, gender or socioeconomic status (SES), are often ignoredbecause they are hard to quantify due to a lack of data and complexity surrounding the subgroups ofpopulations that vary regionally (Marmot et al., 2012; Cutter et al., 2003).
The co-benefits of mitigating wood burning emissions come in many forms (Figure 1) and provide evidencetowards instituting policies to address anthropogenic perturbations to the atmosphere that simultaneouslyquantify immediate and impactful health and social benefits. Due to wood being a quintessential fuel formany households across the world and an emphasis on the renewable aspect of the energy source in the faceof climate change, it is necessary to reduce emissions, and maximize efficiency and education to lessen theimpact on air quality and health. Energy efficiency measures aimed at reducing specific pollutants, suchas PM, from wood burning can result in environmental, health and social benefits. Extremely accessibleand economical strategies to reduce harmful emissions from wood burning include regular wood stove andfireplace maintenance and information regarding use and fuel requirements.
As population grows and urban regions experience expanding pressure, it is imperative for certain regions toimplement multi-dimensional policies utilizing co-benefits to maximize efficacy. One such region is Athens,the capital of Greece, which is undergoing a myriad of economic, social and environmental burdens puttingpressure on the city’s capability to be resilient and develop sustainably, upon which migration has added tosince 2015. The economic recession in Greece, emerging in the years following the 2008 global financial crisis,initially led to a reduction of emissions due to significant industrial activity and vehicle use cutbacks, but since
3

Figure 1: Co-benefits of energy efficiency programs related to wood burning interventions. Strategiesreducing emissions& pollutants from wood burning lead to environmental, health and social benefits (adaptedfrom Watts et al.).
2011-2012 has also led to increased biomass and wood burning, a less expensive method of residential heatingthan oil or modern heating technologies and has resulted in degraded wintertime air quality throughout theregion (Vrekoussis et al., 2013; Saffari et al., 2013; Fourtziou et al., 2017). Current policies have been putforth limiting emissions and setting targets within Europe, but the issue related to PM pollution from woodburning persists (Paraskevopoulou et al., 2015; Fourtziou et al., 2017). There remains a need to quantifyhealth impacts and provide this knowledge as a tool to local decision makers to address the problem withadequate policies. In response, an EU funded project, ERA-PLANET "the European network for observingour changing planet" has devoted one of its four strands to address urban pressures, namely air pollution,disasters and city growth, their reciprocal relations with climate change as well as their impacts on citizens,with an additional focus on migrants (Strand 1 - Smart cities and resilient societies, 2016). This strandproject, titled "Smart Urban Solutions for air quality, disasters, and city growth," shortened to SMURBS, hasemerged to explore, among other focuses, the disproportionate exposure on certain subsets of the populationand enhance informed decision making to aid in sustainable growth of European cities, fully exploitingsynergies from diverse observational platforms. This report contains the results of a systematic review ofexisting literature to identify wood burning interventions or mitigation strategies and applies the findings,according to health impact assessment methodology, to an Athens, Greece case study. Quantifying the healthand economic impacts of intervention strategies, such as improved wood stove technology or maintenance,in Athens will serve as background research to the EU project, and provide evidence of the potential healthco-benefits of reducing wood burning emissions to facilitate the use of comprehensive information by localdecision-makers. Additionally, this work is the first HIA effort to identify possible wood burning interventionsand quantify the burden associated with such environmental exposure, and has potential implications forother regions.
2 Health Impact Assessment Approach
A HIA, or risk assessment, is a tool that supports cross-sectoral action for health by providing politicaldecision-makers with quantitative and qualitative information about the human health effects of a policy
4

or program (WHO, 2006). The HIA approach is particularly useful in the context of Athens, Greece byproviding aid to policy-makers and stakeholders in making choices that are cost-effective, inclusive of linkagesbetween health and the environment, and scientifically sound. The goal of such an assessment is to provideinformation and quantitative evidence to citizens, policy-makers, and humanitarian bodies that will resultin the implementation of a policy suiting local needs, protecting vulnerable populations, and allowing forsustainable development in the context of urban growth and a changing climate.
The following assessment adhered to the World Health Organization’s (WHO) methodology for quantitativeassessment of environmental health impacts at population level (WHO, 2017). The pollutant of concernfor this specific study is PM10, or particulate matter with a diameter of ten micrometers (µm) or less,which has a thorough articulation of its effects on health and is a typical and widely monitored pollutantemitted by many sources, including wood burning for activities such as household heating. For the purposeof this study, strategies reducing PM10 emissions from wood burning activities as a source were the focus.Although PM10 is inclusive of this pollutant emanating from all sources, mitigating these emissions fromwood burning through intervention strategies will reduce overall PM, and by definition reduce PM10 fromthe specific source of wood burning.
The initial step in the process was to conduct a systematic literature review to identify intervention stud-ies that assessed the change in PM levels prior and subsequent to implementation of a strategy to reduceemissions from wood burning activities (Appendix A). From the final selected studies that met the inclu-sion criteria and measured an effective reduction in ambient PM10 as a result of an intervention policy, arandom effects meta-analysis was conducted to obtain pooled estimates of PM reductions associated withthe strategies utilized within the studies (Cooper, 2017). The pooled estimate of PM10 reductions due tointerventions was then compared with the current exposure of the pollutant in Athens, Greece (the locationof the case study). The data corresponding to the current exposure, which can be defined as the observedvalues of PM10 or the business as usual (BAU) scenario, was provided through the publicly available mea-surements published by the Ministry of Environment and Energy and literature within Athens (Ministry ofEnvironment & Energy, 2015; Stafoggia et al., 2017). Utilizing current exposure and the potential reductionin exposure of PM10, the exposure difference that could result in Athens with the implementation of suchwood burning interventions was computed.
An exposure response function (ERF), the relationship between the amount of exposure and the resultingchanges in a specific health outcome, which in this case is mortality, was selected from the same study withinAthens, Greece. An additional analysis was completed employing an ERF corresponding to differences inexposure and health impacts to different socioeconomic classes. The relative risk (RR) exposure difference,which represents increased response in relation to increased PM pollution, was calculated combining the valuerepresenting the reduction of PM10 due to the intervention in terms of Athens with the ERFs from literature.The final, and most important step involved calculating the population attributable fraction (PAF), whichis a measure of the proportion of mortality associated with PM10 exposure, and health outcome data fromliterature to estimate the number of preventable premature deaths attributable to the intervention inducedreduction in PM10 (Refer to Appendix B for the detailed methodology). Moreover, the following HIAincludes an economic perspective to policies mitigating emissions from wood burning. The more establishedand expansive wood burning intervention programs have put forth either an estimation in cost, or a cost-benefit analysis of the program to gauge effectiveness. This information on the particular studies in theHIA is incorporated with systematically estimated return on investment (ROI) values relating to healthinterventions to provide economic evidence towards potential intervention benefits. To further account fordifferences between studies, a sensitivity, or uncertainty, analysis was conducted applying the calculationsof each individual study to quantitatively explore the variance of the studies. This is an essential stepto bolstering a risk assessment’s conclusions and findings by showing the variability as it relates to eachindividual study identified in the literature review as opposed to the pooled estimate resulting from themeta-analysis.
Applying the health impact assessment approach results in an estimation of the magnitude of health improve-ments, in terms of prevented mortality that are attributable to wood burning mitigation strategies employedand monitored elsewhere. Additionally, the risk assessment allows for an exploration into the different effectson exposure and preventable deaths that might persist within different groups of the population, such as
5

groups of lower socioeconomic status. Looking at health from a broad perspective and incorporating vari-ous types of evidence through acknowledging social, economic, and environmental effects, lays the basis forinformed decision making in Athens, Greece that maximize health gains while lessening adverse impacts ofwood burning.
3 Results
3.1 Study Selection & Characteristics
As a result of the systematic literature review utilizing the Web of Science database, nine out of the originallyidentified 7,000 studies satisfied the criteria for inclusion within this risk assessment. Although there wereonly a small number of applicable intervention studies, depicted in Figure 2, spatially they were set inlocations ranging from Tasmania, an island off of Australia’s south coast, to Libby, a rural mountain city innorthwest Montana. Three of the nine studies showed no positive effect of the intervention on PM levels intheir respective regions, further limiting the number of studies to be utilized in the health impact assessmentto a total of six. Of the ultimately included studies, the main intervention strategies consisted mainly of awood heater or stove replacement or change-out program, with one exception in the San Joaquin Valley AirBasin, where mandatory curtailment was required when air quality was forecast to be poor. Additionally,two studies assessed main interventions, which were combined with other methods to reduce PM exposure,such as educational campaigns, incentives, banning open fires, and enhanced enforcement of standards andregulations related to wood stoves. The largest impact on ambient PM due to an intervention took placein Christchurch, New Zealand where a large-scale wood stove change-out program, combined with previousinterventions and financial incentives, resulted in a 36% reduction in winter mean PM10 concentrations (Scott& Scarrott, 2011). The other notable article, and arguably the most regularly cited intervention study in theliterature, took place in Libby, Montana where an expansive wood stove replacement program was correlatedto a 27.6% reduction in ambient winter time PM2.5 (Noonan et al., 2012). This look at the interventionprogram in Libby, was long term and more expansive than the other two studies, which were short term looksat ambient PM levels. For this reason, the least effective measure is seen to be the mandatory curtailmentthat took place in the San Joaquin Valley Air Basin, which reduced outdoor PM levels by 20% (Yap &Garcia, 2015).
3.2 HIA Analysis
In order to aggregate the reduced PM levels from the intervention studies identified in the literature review,a random effects meta-analysis was conducted to combine the results of the similar studies (Figure 3). Thepooled estimate, a more robust and statistically powerful result for use in the HIA, is a synthesis of theweighted average of the results, taking the differences of the studies into account (Lunet, 2012).
The pooled estimate of a 23% (95% CI: 19-27%) reduction in ambient PM due to wood burning interventionswas primarily used throughout this HIA, as in the main analysis and calculations following the research de-sign depicted in Figure 4. Utilizing data from a current study associating particulate matter and mortalityin Athens, which found the current exposure of PM10 in Athens to be 36 µg/m3 (95% CI: 15-57 µg/m3),the exposure response function to be a 0.66% (95% CI: 0.28-1.04%) increase in mortality risk per 10 µg/m3
increase in PM10, and the daily average mortality to be 80 deaths (95% CI: 68-92 deaths). The concludingcalculation, quantifying the health outcome of such wood burning interventions, was estimated to be 0.44(95% CI: 0.05-1.47) prevented average daily non-accidental deaths, which include cardiovascular and respi-ratory causes. In order to calculate the confidence intervals for all values, the lower and upper bounds ofthe 95% CI, which are shown in parenthesis within each box of Figure 4, were calculated consistently in thesame method for each step of the HIA calculation.
6

Figure 2: Map displaying the study locations deduced from the systematic literature review and Athens,Greece indicated for spatial understanding. Green icons represent a study that assessed an intervention thatsuccessfully reduced ambient PM levels, and red icons mark studies that did not effectively lower outdoor PMexposure (and, therefore, were not included in the main analysis). Each icon shows a wood stove interventionstrategy. Three studies focused on the intervention in Libby, Montana and two took place within respectivecities in Tasmania, Australia.
3.3 Sensitivity Analysis
To further account for inter-study differences in the applicable results to Athens, a sensitivity analysis wasconducted (Figure 5). This step incorporated exploring the differences in health outcome by applying theestimated reduction in PM due to interventions, current PM10 exposure data and mortality averages fromAthens, and utilizing literature defined ERFs to represent high and low socioeconomic class. Again, this cal-culation systematically calculated the confidence intervals of such estimates. This allowed for the sensitivityanalysis to explore the uneven impact such an intervention policy, and the resulting reduction in PM couldhave on a more vulnerable subset of the population. In all cases, the effect of a wood stove intervention onprevented deaths was larger for groups of lower socioeconomic status, indicating a disproportionate effect ofcurrent PM induced mortality on populations characterized as a lower socioeconomic class. The impact ofan intervention on the groups of higher socioeconomic class is profoundly lower than to the low SES group.This pattern of augmented preventable deaths in low SES groups due to an intervention, total populationfollowing behind, with high SES groups very close to zero persisted using three PM level scenarios: PM10
measurements as an average of the five most representative monitoring stations in Athens, just the averageof the station experiencing the minimum PM exposure, and the maximum averaged station. Furthermore, itwas as expected that the highest potential for reduced mortality for all groups is with the maximum station,followed closely by the averaged, more representative PM10 exposure.
7

Figure 3: Forest plot showing the pooled estimate, indicated by the blue diamond, of the reduction inambient PM due to wood burning related interventions. The relative risk is located within the ES column,and the percentage in PM reduction is the ES - 1, i.e. the pooled estimate is a 23% (95% CI: 19-27%)reduction in ambient PM10 as a result of the combined intervention studies.
4 Discussion
4.1 Athens, Greece: A Case Study
Athens, the capital city of Greece, is experiencing numerous economic, social, environmental and latelymigratory burdens putting pressure on the city’s capability to be resilient and develop sustainably. AlthoughGreece’s population has experienced a slightly negative growth rate (-0.4) as a whole, 78% of the populationresides in urban areas (UNdata | country profile | Greece, 2016). The population of the Athens metropolitanarea is 4.1 million people, accounting for 39% of the total population of Greece (Hellenic Statistical Authority,2016b). Further adding to the urban pressure, as of April 2017, over 5,000 refugees arrived to Greece by sea,joining the estimated 47,426 refugees already staying on just the mainland (UNHCR, 2017b, 2017a). Theeconomic situation in Greece has been complicated following the Great Recession that took hold subsequentto the world financial crisis, including issues surrounding bankruptcy, austerity measures, and unemployment(23.1%), comprising of almost 50% of the younger age group (Hellenic Statistical Authority, 2016a). Whilethe annual gross domestic product, or GDP growth in 2015 was still slightly negative, it is projected thatit will break even to 0% growth in 2016 (World Bank, 2016). The majority of GDP in Greece can beattributed to the 80.9% contribution of the service industry, which includes tourism (Hellenic StatisticalAuthority, 2016a).
The financial crisis and tough austerity measures have revealed an alarming situation within Greece in termsof well-being and health care. The austerity and regressive taxes have seemed to increase the poverty and
8

Figure 4: HIA calculation methodology including the results from the main analysis, the pooled estimate forbox (1) considering only the effective intervention studies in relation to ambient PM. The current exposure,ERF, and health outcome data were taken from Stafoggia et al.. This figure is adapted from Mueller et al..
inequality gaps between income levels in Greece and resulted in severe cuts in funding towards health care.There has been an increase in suicides and mental illnesses with the alarming unemployment rates sincethe financial crisis. Long term unemployment has been shown to lead to increased social isolation, poverty,morbidity, and mortality specifically in migrants (Ifanti et al., 2013). Groups of the population that aredisadvantaged and excluded, such as unaccompanied minors, unemployed, migrants, those with pre-existinghealth conditions, have fewer social opportunities (Ifanti et al., 2013; Marmot et al., 2012). The need toaddress the inequity in exposure to health hazards, becomes a human rights issue and policies are neededthat prioritize excluded groups.
In the midst of an already tumultuous situation, climate change is expected to impede economic activity,specifically in the Mediterranean sub-region, including tourism and agriculture, threatening the stabilityof the region further. There is high confidence that population health will be affected negatively and dis-proportionately due to climate change impacts, such as heat, drought, flooding, and pressure on criticalinfrastructure (IPCC, 2014b). Climate change merged with current vulnerabilities present in Greece, couldmean compromised public health for a growing urban population and specifically for underrepresented andvulnerable groups, such as people in lower social classes or refugees.
4.1.1 Air Quality: Particulate Matter
Densely populated and urban regions have been shown to lead to deterioration of air quality and, therebyimpact environmental and human health, contributing greatly to the global burden of disease (Chen & Kan,2008). Climatically, Athens is susceptible to high particle levels as it is located within the MediterraneanBasin and impacted by both natural and human caused particulate concentrations, influencing the regionsair quality (e.g., Paraskevopoulou et al., 2015). The region is classified as a hot-summer Mediterraneanclimate, generally mild and temperate with warm and dry summers and wetter winters that average near10◦ Celsius. Particulate matter emissions from multiple sources, both local and transboundary, have been
9

Figure 5: Results of the sensitivity analysis conducted using data from each of the six studies, with confidenceintervals and medians indicated. Each box depicts the associated preventable daily deaths to an interventionpolicy in the context of current exposure in Athens, Greece. The calculations used data from Ministry ofEnvironment & Energy, Stafoggia et al. & Forastiere et al..
noted as a major pollutant of concern, and primarily due to more well-established adverse health impacts,there is a focus on PM of smaller diameter (i.e. PM2.5). Due to data limitations and lack of consistentmeasurements of fine particles in Athens, concentrations of PM10 were used to assess and quantify relatedhealth impacts within this study. The correlations made using PM10 are justifiable for multiple reasons.Not only does a change in PM10 represent an overall reduction of particulate matter, inclusive of all smallerparticles, but the relative change is very similar between the intervention studies regardless of whether theyevaluated PM10 or PM2.5 (shown in Figure 3). The European Commission sets forth Air Quality Standards,for which the maximum concentration regarding PM10 is limited to 50 µg/m3 for 35 permitted exceedenceseach year (European Commission, 2016). For just one station, Aristotle, which is an urban-traffic classifiedmonitoring station, there were 69 exceedences of this limit in 2015. The equivalent standards regardingPM2.5 are even more stringent, highlighting a need to focus on monitoring and limiting emissions of finerparticles, even including PM with a diameter of one µm or less (Gerasopoulos et al., 2007).
Additionally, it is important to examine the multiple sources and contributors to PM levels in Athens. WhileFigure 11 displays the 2015 daily average PM levels, Figure 6 shows the 2015 average wintertime PM10
concentrations from the five selected and representative monitoring stations within the Athens metropolitanarea. Figure 6 allows for a view into variability in PM concentrations and potential sources during thewinter months (January, February, November & December) of 2015, when wood burning is used in theAthens, contributing to some extent to degraded wintertime air quality. The black circles on the Figure 6indicate the maximum daily averaged PM concentration for each winter month. In order to determine theunderlying factor for the peak in PM levels, each maximum day was evaluated for dust events in the regionusing the Barcelona Supercomputer NMMB/BSC-Dust Model (Figure 7). The days with maximum PMlevels in January, November, and December seem to not be associated with dust events, and in this period of
10

the year there is well documented quantification of the influence of PM from wood burning affecting the largeconcentrations for those days (e.g., Fourtziou et al., 2017). This follows intuition especially for December25th, as it is common to burn wood in open fireplaces and stoves during holidays, and generally duringweekends in combination with heating demand when people stay at home (Athanasopoulou et al., 2017).
Additional sources of PM besides biomass burning and dust events, include sea salt, combustion processes,traffic sources, and industrial emissions. It is noteworthy that the annual PM10 averages in Athens havedecreased from 2001 to 2013 by 32%, along with the institution of policies related to traffic emissions andpollutant reduction targets, and also decreased fossil fuel burning as a result of the financial crisis and highfuel prices (PM10 Trends in AIRUSE Cities, 2016; Gratsea et al., 2017). Regardless of the overall decreasingPM trend, CO values in the winter evening have increased as a result of the new smog phenomenon in Athenswhile in the summer morning and evening, as well as winter morning values have decreased (Gratsea et al.,2017).
Figure 6: Daily averaged PM10 concentrations (µg/m3) in the winter months of 2015. The black circlesindicate the monthly maximum PM10 level. The concentrations are averaged from five representative stationsin Athens, Greece, described in Appendix C, Table 2. Data is adapted from the Ministry of Environment &Energy.
4.1.2 Wood Burning for Residential Heating
While biomass burning in Athens is a wintertime problem and not a major source of annual pollution, it is arelatively new contributor to PM. The financial crisis has fostered a phenomenon in the winter months, whereextreme smog events occur, particularly at night, that lead to significant and acute exposure. Furthermore,wood burning will remain an affordable fuel source while oil and alternative fuels have high prices. Much ofthe problem specifically to Athens, is the burning of wood in open fireplaces, which prior to the crisis wereutilized for "recreational" burning as a part of culture, but are now used for heating out of necessity. For thisreason, it is not as straightforward to solve the entire problem with a wood stove replacement intervention,but rather fuel switch, maintenance, cleaning and education in usage could aid in reducing the emissions ofpollutants.
The contribution of wood burning has been estimated within Athens to range between 1.4-7% to total PM10
and 11% of total PM2.5 in urban background and suburban monitoring areas, respectively (PM Speciation
11

Figure 7: Dust load in the region corresponding to each monthly wintertime maximum PM concen-tration. Images from the NMMB/BSC-Dust model, operated by the Barcelona Supercomputing Center(http://www.bsc.es/ESS/bsc-dust-daily-forecast/).
and Source Apportionment , 2016). On a smog period basis, this contribution to total PM10 may rangetypically within 30% during the day to 70% during the night (Athanasopoulou et al., 2017). Althoughwood as a fuel source has been highlighted as a "carbon-neutral" alternative energy option and is publiclyperceived as a "green" fuel, that classification neglects other harmful pollutants that have negative impactsto the environment and health. Many studies have examined the concentrations of other pollutants emittedfrom biomass burning, such as CO and black carbon, as well as characterizing toxic tracers of wood burningin order to assess the impact that increased biomass burning has had in the region (Gratsea et al., 2017;Fourtziou et al., 2017). There has been an emergence of such studies in the years following the financialdownturn, analyzing the composition of pollutants and aerosols in the years since and especially examiningthe poor winter-time air quality, which is mostly of episodic nature. A limitation lies within the lack ofbiomass specific PM studies and data from before the crisis to adequately compare the impact on PMconcentration of wood burning.
In December of 2013, Article four of a common ministerial decision for Athens, Greece addressed and targetedPM10 emission from combustion hearths when measured hourly concentrations greater than 101 µg/m3, i.e.conditions that favor smog (Hellenic Republic, 2013). Although not mandatory, the ministry recommendsfor people to stop usage of fireplaces, stoves, biomass solid fuels and boilers during those conditions. Thepush is towards utilizing natural gas to improve efficiency and reduce the emissions that have critical impacts
12

to health of individuals and contribute toward nighttime smog event in the city. The most applicable studyin terms of Athens is the San Joaquin Valley Air Basin’s mandatory curtailment method, which was theleast effective intervention strategy analyzed. Even as the least effective strategy, the health benefits werewell above the BAU scenario, or no intervention program, with a credible number of prevented deaths forthe total population (0.43 (95% CI: 0.23-0.72)) and even high prevented mortality within the low SES group(0.55 (95% CI: 0.36-0.76)).
In Athens, a mandatory requirement could help the situation, but other, more effective interventions thathave greater implications for health gains should be explored. Interventions are needed in order to tacklethis concern, especially due to the fact that pollution from such sources is greatly affected by the appliancetype, age, the operator’s behavior, and fuel properties, and in many cases treated wood or combustible wasteare used. Beyond PM, wood burning is of concern for other emissions reasons as mentioned previously, andto further fortify a need to address such a specific source is through mitigating other dangerous pollutantsthat can accelerate climate change.
4.1.3 Health Impacts
Particulate matter is a commonly emphasized air pollutant due to the adverse health impacts associatedwith exposure, such as respiratory health effects, heart diseases, and premature mortality, among othercorrelations, such as aggravated asthma (Cohen et al., 2017). Within Greece, studies have focused onPM10 exposure in relationship to increased hospital admissions for respiratory diseases and also reductionsin disability-adjusted life years, setting a case for the need to address such a pollutant, even if the finerparticles (i.e. PM2.5) have been closely correlated with deeper inhalation and penetration into the lungs(Kassomenos et al., 2013; Moustris et al., 2016; Bergauff et al., 2009).
This assessment clearly quantifies an immense health benefit to reducing particulate matter pollution inAthens via a wood stove intervention study, with exceptionally high potential to reduce the largest magnitudeof mortality from members of the lower socioeconomic class. With the pooled estimate of interventionattributable reduced PM exposure of 23% (95% CI: 19-27%) and Athens specific exposure of 36 µg/m3
(95% CI: 15-57), there was a resulting 0.44 (95% CI: 0.05-1.47) daily average deaths prevented (Figure 4).This current exposure value is very close to the average value of 32 µg/m3 from the five representativestations. Extrapolated beyond the daily estimate, this corresponds to over 150 avoided premature deathsannually in the mid-range. Merely investigating the mortality outcome in response to wood burning relatedPM underestimates the potential health gains due to not accounting for hospitalizations, diseases and othercostly and detrimental health outcomes.
The sensitivity analysis showed the immense opportunity that such a policy could have within Athens, andspecifically for groups of lower SES. In all cases, the lower SES group of individuals benefited the mostfrom a intervention induced reduction in PM levels, even within the minimum average PM levels in Athens(Figure 5). In terms of the individual study extremes, the extensive wood stove change-out intervention inChristchurch indicated the highest benefit in terms of mortality, while the specific mandatory curtailmentmethod during certain forecasts utilized in the San Joaquin Valley Air Basin was the least effective, althoughwell above the business as usual scenario with a credible number of prevented deaths for the total population(0.43 (95% CI:0.23-0.72)) and even high prevented mortality within the low SES (0.55 (95% CI:0.36-0.76)).Lower socioeconomic status groups benefit the most from these intervention policies, dwarfing the impacts tothe higher SES portion of the population, which are well below 0.5 prevented daily average deaths regardlessof the PM metric.
In an effort to further quantify benefits related to instituting a wood stove intervention policy within Athens,a simulation was conducted to examine the equity aspect of such a strategy (Figure 8). The calculations forthe simulation followed the same methodology as the main HIA analysis (Figure 4), but the main differencewas the use of two ERFs to explain the differential benefit for the same PM reduction between the lowerand higher socioeconomic groups. Once again, the results enforce the notion that the strong effects of PMon mortality effect a large portion of the population, but not in terms of population within the higher SESbracket. The results show that the dose response, or health impact with exposure, is not equal between the
13

groups as most benefits are concentrated within the low SES group. While there are inter-city differences,the social class of individuals were determined to be an effect modifier of their exposure to PM, with a strongassociation to mortality. It remains to be determined whether the enhanced effect on lower socioeconomicgroups is due to increased exposure, heightened susceptibility to health impacts because of an alreadydeprived health status, or through a combination of both, making the group more affected by exposure(Forastiere et al., 2007). Regardless, the results show that a priority should be on enhancing environmentalequity through reducing the risk to disadvantaged portions of the population. This approach will maximizehealth benefits, and result in progressive policies that alleviate the burden of mortality on more susceptiblesubgroups, which in the case of Athens, a large portion of the population struggles from poverty, includingthe migrant population. In Athens, where the social inequality is growing as a result of the economic crisis,this finding is extremely relevant and provides additional evidence to policy makers to implement woodburning intervention policies that not only overall benefit health but also reduce the level of inequity andpromote social justice.
The migrant crisis within the Mediterranean region, although it has lessened in magnitude, is still significant.The migrant population on the mainland and islands in Athens is an underrepresented group and by nothaving the ability to incorporate such data into an assessment, means that the impact of an interventionpolicy would have an even larger effect on mortality expanded to include the refugee community, which isalready suffering from overcrowding and insufficient access to medical care.
The results of this study supports the application of health equity to public policies specifically relatedto exposure to air pollution. Such policies will contribute towards increasing the total population healthby decreasing overall exposure to pollutants, but has the potential to aim towards reducing inequity thatclearly exists within lower socioeconomic classes and other subgroups of the population, such as migrants.The results are also an underestimation due to only considering one health outcome (mortality) and not otheroutcomes, such as hospitalizations and diseases, and because only outdoor PM concentrations were included,not indoor or personal exposure to PM. As governments aim to enact effective policies, it is necessaryto incorporate facets focused on minimizing the proven injustice of exposure while maximizing long-termand comprehensive benefits. This is becoming increasingly more important as increased air pollution canexacerbate an already deep divide in health impacts, and the need for cross-sectoral transfer of knowledgeis necessary to fully integrate health equity into local policies (Cartier et al., 2015; Wang et al., 2016).
4.1.4 Economic Viability
Due to the tumultuous state the Greek economy has been in since the recession, it is extremely importantto assess the cost-effectiveness of policies put in-place, and in doing so quantify and incorporate evidencefrom multiple perspectives to ensure benefits are maximized. A systematic review of return on investmentin relation to health intervention studies found that the median ROI for interventions that protected healthspecifically to be 34.2 to one (Masters et al., 2017). Furthermore, the large-scale intervention programand effort put forth in Christchurch, New Zealand, which was also the most effective strategy in reducingambient PM levels included within this assessment, performed an extensive review on the cost-effectivenessof the programs over time. The large-scale project, which included additional strategies to incentivize betterhome insulation, cleaner fuels, and wood stove technological improvements, led to net benefits amountingto over 750 million Euros (Grimes et al., 2012). The calculations included health and energy benefits asa result of the long-term project. The intervention that took place in Launceston in Tasmania, Australia,titled the Wood Heater Replacement Program, a 1.66 million Euro project focused on smaller supplementaryinterventions such as education campaigns and enforcement (Johnston et al., 2013). Abiding by the findingsof the systematic review, a 34.2 to one ROI for the Launceston project would make the project extraordinarilycost effective.
The large return on investment that is found on average within health intervention studies, and the excep-tionally large quantification of benefits outweighing the costs in the New Zealand study, shows that such aprogram is likely to be extremely economically viable due to the potential for large returns. The previouslymentioned point that this assessment is underestimating the overall benefits that a wood burning interven-tion could have in Greece, is also tied to the additional amount of cost savings in terms of health costs
14

Figure 8: In an effort to gauge the potential in health impacts to specific groups of the population in Athens,a simulation was performed to show the health effects of hypothetical interventions that ranged from reducingPM exposure from 0% to 30%. The green line is associated with low socioeconomic status (SES) bound bythe upper and lower 95% confidence intervals, the purple line indicates the reduction associated with highSES bound by its upper and lower 95% confidence intervals. The dotted black line represents the mid valuefor the total population, including both low and high SES. Calculations made using data from Ministry ofEnvironment & Energy, Stafoggia et al., & Forastiere et al..
and budgetary gains, while the country’s budget is under intense scrutiny and constraint. Any economythat is struggling financially must institute policies that are particularly cost-effective, in order to maximizetotal benefits to the population. The potential gains for the lower SES group of the population, which isvery prevalent currently in Athens, creates viability for such a mitigation strategy. Furthermore, such anintervention could assuage the government’s apprehension to prohibit or ban wood burning, or implementa policy further distancing the lower socioeconomic groups from attaining heating in the winter. To fullyassess the costs and benefits, it would be necessary to incorporate the cost of wood burning on health, the airquality, and also on water scarce and wildfire prone forests that are pressured due to the use of wood fuel, andall of these costs get more expensive when considering long-term climate change impacts. In order to ensurethe safety of citizens, especially susceptible groups, such as migrants, it is necessary to put mitigation effortsin place to allow for energy security and efficiency. This study can be useful for future ROI calculations inproviding proof of health benefits to be considered, specifically in terms of the greater health gains to bemade for lower socioeconomic classes. The results of instituting such an intervention policy, would lead toa win-win or no-regret policy, bettering air quality for all citizens and work towards lessening the excessiveand asymmetric health burden that exists for the most vulnerable populations.
15

5 Conclusion
As a result of this health impact assessment, policies addressing the particulate matter pollution relatedto wood burning have been shown to alleviate negative health impacts, in particular health impacts tothe most vulnerable groups, and by association lessen environmental impacts, working towards mitigatingclimate change. The following findings of the assessment are outlined below:
• The HIA approach is extremely useful for analyzing the effectiveness and viability of policies, partic-ularly in the context of climate change mitigation and related health co-benefits. The most effectiveapproach would be to institute a combination of multiple intervention policies, such as in Christchurch,New Zealand.
• The systematic review performed within the report serves as useful evidence moving forward, andoutlines the need for additional studies assessing intervention impacts to PM levels and human health,and particularly highlights the need for comprehensive and reliable monitoring of PM2.5 and PM10.
• Pooling the varying results from intervention studies identified in the literature review, the resultsshowed a reduction in PM exposure of 23% (95% CI: 19-27%). Specifically in Athens, Greece, suchreduction in PM was calculated to prevent 0.44 (95% CI: 0.05-1.47) average daily deaths. This corre-sponds to 44 avoided premature deaths for 100 days of winter time in the region, which is a conservativeestimate due to inclusion of only one health outcome and the exclusion of indoor exposure to PM fromwood burning.
• The sensitivity analysis, accounting for inter-study variability of the intervention studies, and theincorporation of social and economical factors allow for a potential framework and extrapolation ofsuch policies to Athens, as well as other cities and urban areas facing issues related to wood burning.
• Inequity between health impacts to certain vulnerable groups persists, and there is an opportunity toimprove the well-being for these groups through implementation of wood-burning intervention policies,specifically in Athens, Greece. Additionally, the results of this report present an excellent opportunityfor reducing disproportionate health impacts from AP exposure, specifically proving the need for equityto be factored into public policies.
• The groups of the population qualifying as low SES can benefit more than 13.5 times as much as thehigher SES groups (1.08 compared to 0.08 prevented daily deaths, respectively) with such policies ifPM levels are reduced by 30%, providing confirmation that the burden of mortality due to ambient PMrests more on disadvantaged groups, but also identifying that relatively easy, cost-effective strategiescould be put forth allowing for increased environmental equity.
16

References
Athanasopoulou, E., Speyer, O., Brunner, D., Vogel, H., Vogel, B., Mihalopoulos, N., & Gerasopoulos, E.(2017, March). Changes in the domestic heating fuel in Greece: effects on atmospheric chemistry andradiation. Atmospheric Chemistry and Physics Discussions, 1–33. Retrieved from http://www.atmos-chem-phys-discuss.net/acp-2017-139/ doi: 10.5194/acp-2017-139
Aung, T. W., Jain, G., Sethuraman, K., Baumgartner, J., Reynolds, C., Grieshop, A. P., . . . Brauer,M. (2016, July). Health and Climate-Relevant Pollutant Concentrations from a Carbon-FinanceApproved Cookstove Intervention in Rural India. Environmental Science & Technology , 50 (13), 7228–7238. Retrieved from http://pubs.acs.org/doi/abs/10.1021/acs.est.5b06208 doi: 10.1021/acs.est.5b06208
Bell, M. L., Davis, D. L., Cifuentes, L. A., Krupnick, A. J., Morgenstern, R. D., & Thurston, G. D. (2008,December). Ancillary human health benefits of improved air quality resulting from climate changemitigation. Environmental Health, 7 (1). Retrieved from http://ehjournal.biomedcentral.com/articles/10.1186/1476-069X-7-41 doi: 10.1186/1476-069X-7-41
Bergauff, M. A., Ward, T. J., Noonan, C. W., & Palmer, C. P. (2009, June). The effect of a wood-stove changeout on ambient levels of PM2.5 and chemical tracers for woodsmoke in Libby, Montana.Atmospheric Environment , 43 (18), 2938–2943. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S135223100900185X doi: 10.1016/j.atmosenv.2009.02.055
Bond, T. C., Doherty, S. J., Fahey, D. W., Forster, P. M., Berntsen, T., DeAngelo, B. J., . . . Zender, C. S.(2013, June). Bounding the role of black carbon in the climate system: A scientific assessment: BLACKCARBON IN THE CLIMATE SYSTEM. Journal of Geophysical Research: Atmospheres, 118 (11),5380–5552. Retrieved from http://doi.wiley.com/10.1002/jgrd.50171 doi: 10.1002/jgrd.50171
Cartier, Y., Benmarhnia, T., & Brousselle, A. (2015, December). Tool for assessing health and equity impactsof interventions modifying air quality in urban environments. Evaluation and Program Planning , 53 ,1–9. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S0149718915000713 doi:10.1016/j.evalprogplan.2015.07.004
Chen, B., & Kan, H. (2008, March). Air pollution and population health: a global challenge. Environ-mental Health and Preventive Medicine, 13 (2), 94–101. Retrieved from http://link.springer.com/10.1007/s12199-007-0018-5 doi: 10.1007/s12199-007-0018-5
Cheng, J. J., & Berry, P. (2013, April). Health co-benefits and risks of public health adaptation strategiesto climate change: a review of current literature. International Journal of Public Health, 58 (2),305–311. Retrieved from http://link.springer.com/10.1007/s00038-012-0422-5 doi: 10.1007/s00038-012-0422-5
Cohen, A. J., Brauer, M., Burnett, R., Anderson, H. R., Frostad, J., Estep, K., . . . Forouzanfar, M. H.(2017, May). Estimates and 25-year trends of the global burden of disease attributable to ambient airpollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet , 389 (10082),1907–1918. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S0140673617305056doi: 10.1016/S0140-6736(17)30505-6
Cooper, H. M. (2017). Research synthesis and meta-analysis: a step-by-step approach (Fifth Edition ed.).Los Angeles: SAGE.
Cornwall, W. (2017, January). Is wood a green source of energy? Scientists are divided. Science. Re-trieved from http://www.sciencemag.org/news/2017/01/wood-green-source-energy-scientists-are-divided doi: 10.1126/science.aal0574
17

Cutter, S. L., Boruff, B. J., & Shirley, W. L. (2003, June). Social Vulnerability to Environmental Haz-ards*. Social Science Quarterly , 84 (2), 242–261. Retrieved from http://doi.wiley.com/10.1111/1540-6237.8402002 doi: 10.1111/1540-6237.8402002
European Commission. (2009). Renewable energy: Moving towards a low carbon economy. Retrieved fromhttps://ec.europa.eu/energy/en/topics/renewable-energy
European Commission. (2016, August). Air Quality Standards. Retrieved from http://ec.europa.eu/environment/air/quality/standards.htm
Forastiere, F., Stafoggia, M., Tasco, C., Picciotto, S., Agabiti, N., Cesaroni, G., & Perucci, C. A. (2007,March). Socioeconomic status, particulate air pollution, and daily mortality: Differential exposure ordifferential susceptibility. American Journal of Industrial Medicine, 50 (3), 208–216. Retrieved fromhttp://doi.wiley.com/10.1002/ajim.20368 doi: 10.1002/ajim.20368
Fourtziou, L., Liakakou, E., Stavroulas, I., Theodosi, C., Zarmpas, P., Psiloglou, B., . . . Mihalopoulos, N.(2017, January). Multi-tracer approach to characterize domestic wood burning in Athens (Greece)during wintertime. Atmospheric Environment , 148 , 89–101. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S1352231016308081 doi: 10.1016/j.atmosenv.2016.10.011
Gerasopoulos, E., Koulouri, E., Kalivitis, N., Kouvarakis, G., Saarikoski, S., Mäkelä, T., . . . Mihalopoulos,N. (2007, May). Size-segregated mass distributions of aerosols over Eastern Mediterranean: seasonalvariability and comparison with AERONET columnar size-distributions. Atmospheric Chemistry andPhysics, 7 (10), 2551–2561. Retrieved from http://www.atmos-chem-phys.net/7/2551/2007/ doi:10.5194/acp-7-2551-2007
Gratsea, M., Liakakou, E., Mihalopoulos, N., Adamopoulos, A., Tsilibari, E., & Gerasopoulos, E. (2017,August). The combined effect of reduced fossil fuel consumption and increasing biomass combus-tion on Athens’ air quality, as inferred from long term CO measurements. Science of The To-tal Environment , 592 , 115–123. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S0048969717305491 doi: 10.1016/j.scitotenv.2017.03.045
Grimes, A., Denne, T., Howden-Chapman, P., Arnold, R., Telfar-Barnard, L., Preval, N., & Young,C. (2012, June). Cost Benefit Analysis of the Warm Up New Zealand Programme (Final Re-port). Retrieved from http://www.healthyhousing.org.nz/wp-content/uploads/2012/05/NZIF_CBA_report-Final-Revised-0612.pdf
Hellenic Republic. (2013, December). Short-term action plan to address atmospheric pollution by particulatematter (Common Ministerial Decision No. 3272).
Hellenic Statistical Authority. (2016a, December). Labour Force (Monthly Data). Retrieved from https://www.statistics.gr/en/statistics/-/publication/SJO02/-
Hellenic Statistical Authority. (2016b). Population and Social Conditions. Retrieved from http://www.statistics.gr/en/statistics/pop
Ifanti, A. A., Argyriou, A. A., Kalofonou, F. H., & Kalofonos, H. P. (2013, November). Financial crisisand austerity measures in Greece: Their impact on health promotion policies and public health care.Health Policy , 113 (1-2), 8–12. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S0168851013001541 doi: 10.1016/j.healthpol.2013.05.017
IPCC. (2014a). 2013: Anthropogenic and Natural Radiative Forcing. In Climate Change 2013: ThePhysical Science Basis: Contribution of Working Group I to the Fifth Assessment Report of the In-tergovernmental Panel on Climate Change. New York: Cambridge University Press. Retrieved from
18

https://www.ipcc.ch/pdf/assessment-report/ar5/wg1/WG1AR5_Chapter08_FINAL.pdf
IPCC. (2014b). 2014: Europe. In: Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part B:Regional Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovern-mental Panel on Climate Change (Tech. Rep.). Intergovernmental Panel on Climate Change. Retrievedfrom http://www.ipcc.ch/pdf/assessment-report/ar5/wg2/WGIIAR5-Chap23_FINAL.pdf
IPCC. (2015). Climate change 2014: synthesis report (R. K. Pachauri & L. Mayer, Eds.). Geneva, Switzer-land: Intergovernmental Panel on Climate Change. (OCLC: 914851124)
Johnston, Hanigan, I., Henderson, S., & Morgan, G. (2013, January). Evaluation of interventions to reduceair pollution from biomass smoke on mortality in Launceston, Australia: retrospective analysis of dailymortality, 1994-2007. BMJ , 346 (jan08 12). Retrieved from http://www.bmj.com/cgi/doi/10.1136/bmj.e8446 doi: 10.1136/bmj.e8446
Johnston, O., Johnston, F., Todd, J., & Williamson, G. (2016, November). Community-Wide Distributionof a Catalytic Device to Reduce Winter Ambient Fine Particulate Matter from Residential WoodCombustion: A Field Study. PLOS ONE , 11 (11). Retrieved from http://dx.plos.org/10.1371/journal.pone.0166677 doi: 10.1371/journal.pone.0166677
Kassomenos, P. A., Dimitriou, K., & Paschalidou, A. K. (2013, August). Human health damage caused byparticulate matter PM10 and ozone in urban environments: the case of Athens, Greece. EnvironmentalMonitoring and Assessment , 185 (8). Retrieved from http://link.springer.com/10.1007/s10661-013-3076-8 doi: 10.1007/s10661-013-3076-8
The Keeling Curve. (2017, May). Retrieved from https://scripps.ucsd.edu/programs/keelingcurve/
Lunet, N. (Ed.). (2012). Epidemiology - Current Perspectives on Research and Practice. In-Tech. Retrieved from http://www.intechopen.com/books/epidemiology-current-perspectives-on-research-and-practice (DOI: 10.5772/2241)
Marmot, M., Allen, J., Bell, R., Bloomer, E., & Goldblatt, P. (2012, September). WHO European reviewof social determinants of health and the health divide. The Lancet , 380 (9846), 1011–1029. Retrievedfrom http://linkinghub.elsevier.com/retrieve/pii/S0140673612612288 doi: 10.1016/S0140-6736(12)61228-8
Masters, R., Anwar, E., Collins, B., Cookson, R., & Capewell, S. (2017, March). Return on investmentof public health interventions: a systematic review. Journal of Epidemiology and Community Health,jech–2016–208141. Retrieved from http://jech.bmj.com/lookup/doi/10.1136/jech-2016-208141doi: 10.1136/jech-2016-208141
Ministry of Environment & Energy. (2015). Data Measurements. Retrieved from http://www.ypeka.gr/Default.aspx?tabid=495&locale=el-GR&language=en-US
Ministry of Environment & Energy. (2016, September). Annual Report on Atmospheric Pollution 2015(Annual Report). Ministry of Environment & Energy. Retrieved from http://www.ypeka.gr/Default.aspx?tabid=490&language=el-GR
Moustris, K. P., Proias, G. T., Larissi, I. K., Nastos, P. T., Koukouletsos, K. V., & Paliatsos, A. G.(2016, January). Health impacts due to particulate air pollution in Volos City, Greece. Journal ofEnvironmental Science and Health, Part A, 51 (1), 15–20. Retrieved from http://www.tandfonline.com/doi/full/10.1080/10934529.2015.1079099 doi: 10.1080/10934529.2015.1079099
Mueller, N., Rojas-Rueda, D., Basagaña, X., Cirach, M., Cole-Hunter, T., Dadvand, P., . . . Nieuwenhuijsen,
19

M. (2016, June). Urban and Transport Planning Related Exposures and Mortality: A Health ImpactAssessment for Cities. Environmental Health Perspectives, 125 (1). Retrieved from http://ehp.niehs.nih.gov/EHP220 doi: 10.1289/EHP220
Noonan, C. W., Ward, T. J., Navidi, W., & Sheppard, L. (2012, May). A rural community interventiontargeting biomass combustion sources: effects on air quality and reporting of children’s respiratoryoutcomes. Occupational and Environmental Medicine, 69 (5), 354–360. Retrieved from http://oem.bmj.com/lookup/doi/10.1136/oemed-2011-100394 doi: 10.1136/oemed-2011-100394
Paraskevopoulou, D., Liakakou, E., Gerasopoulos, E., & Mihalopoulos, N. (2015, September). Sources ofatmospheric aerosol from long-term measurements (5years) of chemical composition in Athens, Greece.Science of The Total Environment , 527-528 , 165–178. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S0048969715004581 doi: 10.1016/j.scitotenv.2015.04.022
PM10 Trends in AIRUSE Cities (LIFE11/ENV/ES/584 No. 3). (2016, December). Retrieved from http://airuse.eu/wp-content/uploads/2013/11/R03_AIRUSE-PM10-trends-in-AIRUSE-cities.pdf
PM Speciation and Source Apportionment (LIFE11/ENV/ES/584 No. 4). (2016, December). Re-trieved from http://airuse.eu/wp-content/uploads/2013/11/R04_AIRUSE-PM-Speciation-and-source-apportionment.pdf
Pope, C. A., & Dockery, D. W. (2006, June). Health Effects of Fine Particulate Air Pollution: Lines thatConnect. Journal of the Air & Waste Management Association, 56 , 709–742.
Quam, V., Rocklöv, J., Quam, M., & Lucas, R. (2017, April). Assessing Greenhouse Gas Emissions andHealth Co-Benefits: A Structured Review of Lifestyle-Related Climate Change Mitigation Strate-gies. International Journal of Environmental Research and Public Health, 14 (5), 468. Retrieved fromhttp://www.mdpi.com/1660-4601/14/5/468 doi: 10.3390/ijerph14050468
Saffari, A., Daher, N., Samara, C., Voutsa, D., Kouras, A., Manoli, E., . . . Sioutas, C. (2013, December).Increased Biomass Burning Due to the Economic Crisis in Greece and Its Adverse Impact onWintertimeAir Quality in Thessaloniki. Environmental Science & Technology , 47 (23), 13313–13320. Retrievedfrom http://pubs.acs.org/doi/abs/10.1021/es403847h doi: 10.1021/es403847h
Scott, A. J., & Scarrott, C. (2011, June). Impacts of residential heating intervention measures on airquality and progress towards targets in Christchurch and Timaru, New Zealand. Atmospheric En-vironment , 45 (17), 2972–2980. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S1352231010007624 doi: 10.1016/j.atmosenv.2010.09.008
Smith, K. R., Bruce, N., Balakrishnan, K., Adair-Rohani, H., Balmes, J., Chafe, Z., . . . Rehfuess, E.(2014, March). Millions Dead: How Do We Know and What Does It Mean? Methods Used in theComparative Risk Assessment of Household Air Pollution. Annual Review of Public Health, 35 (1), 185–206. Retrieved from http://www.annualreviews.org/doi/10.1146/annurev-publhealth-032013-182356 doi: 10.1146/annurev-publhealth-032013-182356
Stafoggia, M., Schneider, A., Cyrys, J., Samoli, E., Andersen, Z. J., Bedada, G. B., . . . Forastiere, F.(2017, March). Association Between Short-term Exposure to Ultrafine Particles and Mortality in EightEuropean Urban Areas:. Epidemiology , 28 (2), 172–180. Retrieved from http://Insights.ovid.com/crossref?an=00001648-201703000-00004 doi: 10.1097/EDE.0000000000000599
Strand 1 - Smart cities and resilient societies. (2016). Retrieved from http://www.era-planet.eu/index.php/the-program/strands/strand-1/
UNdata | country profile | Greece. (2016). Retrieved from http://data.un.org/CountryProfile.aspx
20

?crName=GREECE
UNHCR. (2017a, January). Greece Factsheet January 2017 (Tech. Rep.). United Nations High Commissionerfor Refugees. Retrieved from https://data2.unhcr.org/en/documents/download/54221
UNHCR. (2017b, March). Weekly Report (Tech. Rep.). United Nations High Commissioner for Refugees.Retrieved from https://data2.unhcr.org/en/documents/download/55032
United Nations, Department of Economic and Social Affairs, Population Division. (2015). WorldPopulation Prospects: The 2015 Revision, Key Findings and Advance Tables (Working PaperNo. ESA/P/WP.241). Retrieved from https://esa.un.org/unpd/wpp/publications/files/key_findings_wpp_2015.pdf
Vrekoussis, M., Richter, A., Hilboll, A., Burrows, J. P., Gerasopoulos, E., Lelieveld, J., . . . Mihalopoulos, N.(2013, January). Economic crisis detected from space: Air quality observations over Athens, Greece.Geophysical Research Letters, 40 (2), 458–463. Retrieved from http://doi.wiley.com/10.1002/grl.50118 doi: 10.1002/grl.50118
Wang, L., Zhong, B., Vardoulakis, S., Zhang, F., Pilot, E., Li, Y., . . . Krafft, T. (2016, December). AirQuality Strategies on Public Health and Health Equity in Europe—A Systematic Review. InternationalJournal of Environmental Research and Public Health, 13 (12), 1196. Retrieved from http://www.mdpi.com/1660-4601/13/12/1196 doi: 10.3390/ijerph13121196
Ward, T. J., Palmer, C. P., Houck, J. E., Navidi, W. C., Geinitz, S., & Noonan, C. W. (2009, July).Community Woodstove Changeout and Impact on Ambient Concentrations of Polycyclic AromaticHydrocarbons and Phenolics. Environmental Science & Technology , 43 (14), 5345–5350. Retrievedfrom http://pubs.acs.org/doi/abs/10.1021/es8035253 doi: 10.1021/es8035253
Watts, N., Adger, W. N., Agnolucci, P., Blackstock, J., Byass, P., Cai, W., . . . Costello, A. (2015, November).Health and climate change: policy responses to protect public health. The Lancet , 386 (10006), 1861–1914. Retrieved from http://linkinghub.elsevier.com/retrieve/pii/S0140673615608546 doi:10.1016/S0140-6736(15)60854-6
WHO (Ed.). (2006). Air quality guidelines: global update 2005: particulate matter, ozone, nitrogen dioxide,and sulfur dioxide. Copenhagen, Denmark: World Health Organization. (OCLC: ocn162119780)
WHO. (2016, September). Ambient (outdoor) air quality and health (Fact Sheet). World Health Organization.Retrieved from http://www.who.int/mediacentre/factsheets/fs313/en/
WHO. (2017). The Health and Environment Linkages Initiative (HELI) - Quantitative assessment of en-vironmental health impacts at population level. Retrieved from http://www.who.int/heli/tools/quantassess/en/
World Bank. (2016). Greece | Data. Retrieved from http://data.worldbank.org/country/greece
Yap, P.-S., & Garcia, C. (2015, April). Effectiveness of Residential Wood-Burning Regulation on DecreasingParticulate Matter Levels and Hospitalizations in the San Joaquin Valley Air Basin. American Jour-nal of Public Health, 105 (4), 772–778. Retrieved from http://ajph.aphapublications.org/doi/10.2105/AJPH.2014.302360 doi: 10.2105/AJPH.2014.302360
Zuk, M., Rojas, L., Blanco, S., Serrano, P., Cruz, J., Angeles, F., . . . Masera, O. (2007, May). Theimpact of improved wood-burning stoves on fine particulate matter concentrations in rural Mexicanhomes. Journal of Exposure Science and Environmental Epidemiology , 17 (3), 224–232. Retrieved fromhttp://www.nature.com/doifinder/10.1038/sj.jes.7500499 doi: 10.1038/sj.jes.7500499
21

Appendices
A Systematic Literature Review
A.1 Search Strategy
A systematic literature review was performed by searching the Web of Science Core Collection database toidentify articles investigating the effectiveness of strategies reducing particulate matter pollution from woodburning stoves and heaters. For the purpose of this study, the focus was limited to peer-reviewed articlespublished in English. The search was not restricted to a certain time period or geographical location, as thegoal was to perform a comprehensive literature review of all available studies assessing intervention policies.The keywords utilized within the database consisted of a combination of groups of search terms representing“air pollution,” “interventions,” and “evaluation” connected using the Boolean operator AND. By default, theWeb of Science database searched both the title and abstract for selection of results based off of the inputsearch terms. The full list of keywords, which were selected through comparison with keywords from studiesidentified in the initial literature search and discussion with my expert advisor, are separated by categoryand shown below.
Air Pollution: “particulate matter” OR PM OR PM2.5 OR PM10 OR “total suspended particles”OR TSP OR black carbon OR “greenhouse gases” OR particulate pollution OR “air quality” OR “airpollution” OR (biomass combustion) OR (biomass burning) OR (wood burning) OR “wood smoke”OR firewood OR “wood fuel” OR “residential heating”
Intervention: “wood burning stove*” OR “wood stove*” OR cookstoves OR “cook stoves” OR inter-vention OR (technology intervention) OR (“wood stove” improvement*) OR (“wood stove” efficiency)OR (changeout program* OR change-out program*) OR (“wood heater” replac*) OR enforcement ORregulations OR (targeted intervention) OR (emission* guidelines) OR (increase* wood prices) OR “airquality” OR policy OR strateg* OR “air pollution”
Impact/Evaluation: (human health) OR impact OR “risk assessment” OR improvement* OR re-duction OR “health benefit” OR “exposure level” OR “well-being” OR assessment OR (health risks)OR evaluation OR emissions OR “public health”
The asterisk represents the truncation symbol, which allows for the inclusion of all possible word endingswithin in the search. Quotation marks indicate exact phrase searching, meaning that a search of a phraseenclosed within quotation marks will retrieve records containing only the exact phrase. Parenthesis allowfor the grouping of compound Boolean operators.
The identified articles were first examined by title to narrow the results according to the inclusion criteria.Next, the abstracts were screened and upon approval, the final selection of articles were downloaded in full-text to assess for viability of data-extraction. To ensure completeness, the references of the final selectedliterature were screened and additional internet searches and examination of related reviews were performed.
Studies that met the following eligibility criteria were included within the literature review:
1. Focus on an intervention strategy aimed at a type of improvement or alteration to wood stoves.
2. Measured ambient particulate matter concentrations as a proxy for pollution from wood stoves.
3. Report the impact of the intervention scenario(s) in the form of a quantitative change in particulatematter levels.
22

A.2 Search Results
The literature search yielded a list of 6,962 articles for review (Figure 9). Screening of titles and abstractsresulted in 29 articles. Each piece of literature was read in full to gauge eligibility for data extraction, anda total of nine articles satisfied the criteria. Due to three studies not measuring a resulting improvement toambient PM levels, they were excluded from the main analysis in order to hypothesize an effective strategyfor Athens, Greece. A secondary analysis was conducted, to ensure that the effect of inclusion of the studiesthat had a worsening in PM conditions was extremely minimal (Figure 10). Lastly, the reference list of eachof nine studies was screened to ensure completeness in the review process, but no additional studies meetingthe inclusion criteria were identified.
Figure 9: Flow chart depicting the study selection process and the number of studies filtered at each stage.
A.3 Data Extraction
With the finalized selection of nine studies, data was extracted from each to fully populate the literaturereview table (Table 1). Individual study information is included regarding characteristics, specific detailsabout the intervention strategy, and particulate matter measurements. In the case of three previouslymentioned studies, there was no positive influence of the intervention on PM concentrations. In order tohypothesize a reasonable and effective intervention in Athens, it is justifiable to exclude these three studies.Additionally, all of the excluded studies measured PM2.5 in relation to wood burning strategies, and in thecase of the smaller studies set in developing countries, i.e. India and Mexico, outdoor air pollution was notthe main assessment goal, and was therefore not measured extensively or long-term pre and post-intervention.
23

Stu
dy
Loc
atio
nIn
terv
enti
onT
ype
Stu
dy
Per
iod
Pol
luta
ntM
ea-
sure
d
%C
han
gein
PM
Com
mun
ity-W
ideDistributionof
aCatalytic
Deviceto
ReduceW
inter
AmbientFineParticulate
Matterfrom
Residential
Woo
dCom
bustion:
AField
Stud
y(O
.Joh
nston,
John
ston
,Tod
d,&
Williamson,
2016)
Perth,
Tasman
ia,
Australia
Com
mun
ity
engagement&
distribu
tion
ofcatalytic
combu
stors
2013-2014
PM
2.5
-18%
Health,an
dClim
ate-Relevan
tPollutant
Con
centration
sfrom
aCarbo
n-Finan
ceApp
rovedCoo
kstove
Intervention
inRural
India(A
unget
al.,2016)
Kop
pa,
Karna
taka,
India
Woo
dcook
stove
replacem
ent
2011-2012
PM
2.5
-38%
Effe
ctivenessof
Residential
Woo
d-Burning
Regulationon
Decreasing
Particulate
MatterLe
vels
and
Hospitalizations
intheSa
nJo
aquin
ValleyAir
Basin
(Yap
&Garcia,
2015)
SanJo
aquin
ValleyAir
Basin,
Califo
rnia,
U.S.A
.
Man
datory
curtailm
entof
residentialw
ood
burningwhenair
qualityforecast
tobe
poor
2000-2006
PM
2.5
20%
Evaluationof
intervention
sto
redu
ceair
pollu
tion
from
biom
asssm
okeon
mortalityin
Laun
ceston
,Australia:
retrospe
ctivean
alysis
ofda
ilymortality
1994-2007(Joh
nstonet
al.,2013)
Laun
ceston
,Tasman
ia,
Australia
Woo
dhe
ater
replacem
ent
program,
education&
enforcem
ent
1997-2007
PM
10
22%
Aruralc
ommun
ityintervention
targeting
biom
asscombu
stionsources:
effects
onair
qualityan
drepo
rtingof
child
ren’s
respiratoryou
tcom
es(N
oona
net
al.,
2012)
Libb
y,Mon
tana
,U.S.A
.
Woo
dhe
ater
replacem
ent
program
2003-2009
PM
2.5
28%
Impa
ctsof
residentialh
eating
intervention
measureson
airqu
alityan
dprogress
towards
targetsin
Christchu
rchan
dTim
aru,
New
Zealan
d(Scott
&Scarrott,
2011)
Christchu
rch,
New
Zealan
d
Woo
dhe
ater
replacem
ent
program
1999-2009
PM
10
36%
Com
mun
ityWoo
dstove
Cha
ngeout
and
Impa
cton
AmbientCon
centration
sof
Polycyclic
Aromatic
Hyd
rocarbon
san
dPheno
lics(W
ardet
al.,2009)
Libb
y,Mon
tana
,U.S.A
.
Woo
dhe
ater
replacem
ent
program
2004-2008
PM
2.5
19%
The
effectof
awoo
dstove
chan
geou
ton
ambientlevels
ofPM2.5an
dchem
ical
tracersforwoo
dsmokein,Libby,M
ontana
(Bergauff
etal.,2009)
Libb
y,Mon
tana
,U.S.A
.
Woo
dhe
ater
replacem
ent
program
2004-2008
PM
2.5
19%
The
impa
ctof
improved
woo
d-bu
rning
stoves
onfin
epa
rticulatematter
concentrations
inruralM
exican
homes
(Zuk
etal.,2007)
Com
achu
én,
Micho
acán
,Mexico
Coo
kstove
replacem
ent
2004-2005
PM
2.5
-3%
Tab
le1:
Literature
Review
Tab
le
24

B Health Impact Assessment Methodology & Calculations
An array of data sources and analytic methods outlined below were used to determine the potential effectsof intervention policies reducing PM pollution from wood burning on the health of the population in Athens,Greece and the distribution of those effects within the population in regards to socioeconomic status.
B.1 Main Analysis
The health impact was assessed based on the estimated pooled exposure levels resulting from the meta-analysis (Figure 3). This estimation was done using Stata Statistical Software, to arrive at a weightedaggregated range of values correlated to the intervention studies and reduced ambient PM levels. The analysiswas done after excluding data from the three aforementioned studies that measured worsened outdoor PMpollution in the context of the article. In addition, a second pooled estimate was calculated keeping twoof the excluded studies, besides India, to show the effect such a calculation had on the prevented healthoutcome (Figure 10). The primary pooled estimate was used for all other calculations due to the goal of thisstudy and attempting to assess realistic and applicable intervention strategies.
For the main analysis, depicted in Figure 3, the current exposure of PM10 was utilized from the study withinAthens and compared with the meta-analysis pooled result to deduce the exposure difference between thetwo (Stafoggia et al., 2017). Using the exposure response function from the same piece of literature toassess increased mortality risk due to PM10 exposure, the relative risk exposure difference was calculated.RR exposure difference takes the ERF and finds its equivalence for exposure difference in terms of thisspecific group of intervention studies reduction in particulate levels. The next step of calculations deducedthe preventable health outcome, which was identified through the same study (Stafoggia et al., 2017) wherethey assessed daily average non-accidental deaths. In order to identify the number of preventable deaths, thehealth outcome data was combined with the RR exposure difference calculated specifically for the interventionreduced exposure of PM. In order to incorporate the uncertainty, the lower 95% confidence interval of eachstep of the calculation was systematically used to produce the final lower bound of the prevented number ofaverage daily deaths due to the interventions. Similarly, the upper bound of the 95% CI was applied withineach step to account for the uncertainty.
B.2 Secondary Analysis
The secondary analysis, with calculation values in line within Figure 10, follows an identical pattern tothe assessment described above, with one exception. In order to account for two of the three studies thatshowed no benefit to PM levels post-intervention strategy, a separate meta-analysis was conducted to definea pooled estimate to compare with the main analysis results. This pooled estimate excluded India due tomany reasons keeping the intervention from being a viable option for Athens, including India’s status as adeveloping country, focus on cook-stoves within a small rural village, and the main goal of the study wasdetermining the change in indoor and personal exposure to PM2.5. Furthermore, the study in India onlybriefly measured ambient PM, and from just two monitoring locations. The results of the second meta-analysis displayed understandably lower reduction values, 14% compared to 23% exposure minimizationdue to the interventions. Additionally, the prevented average daily deaths as a result of the strategies waslower for the secondary analysis, but even with the incorporation of the ineffective interventions in terms ofambient PM levels, still resulted in a positive, and meaningful amount of prevented premature deaths.
B.3 Sensitivity Analysis
The sensitivity, or uncertainty, analysis was conducted to display the inter-study differences, but also in-corporating the consideration of disproportionate impacts on different SES groups. Figure 5 displays theresults of the sensitivity examination. The specific intervention reduced PM exposure from each study wasused in concert with the current (2015) PM10 exposure in Athens, Greece. Within this analysis there were
25
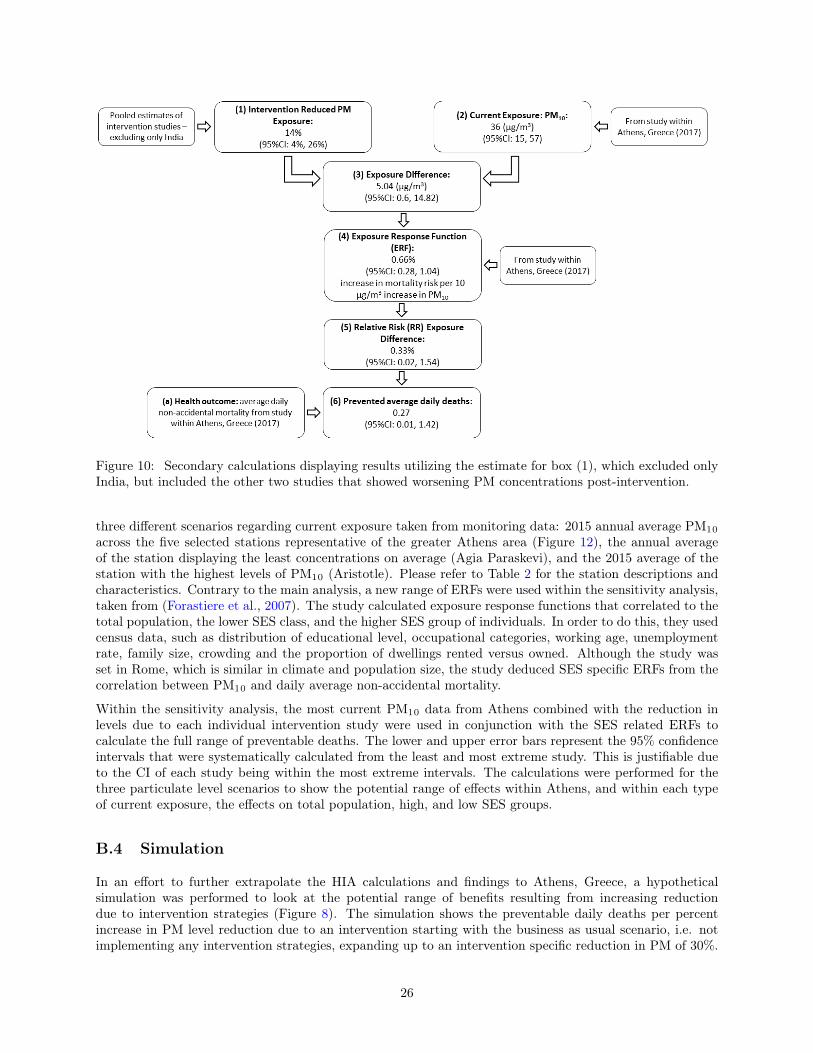
Figure 10: Secondary calculations displaying results utilizing the estimate for box (1), which excluded onlyIndia, but included the other two studies that showed worsening PM concentrations post-intervention.
three different scenarios regarding current exposure taken from monitoring data: 2015 annual average PM10
across the five selected stations representative of the greater Athens area (Figure 12), the annual averageof the station displaying the least concentrations on average (Agia Paraskevi), and the 2015 average of thestation with the highest levels of PM10 (Aristotle). Please refer to Table 2 for the station descriptions andcharacteristics. Contrary to the main analysis, a new range of ERFs were used within the sensitivity analysis,taken from (Forastiere et al., 2007). The study calculated exposure response functions that correlated to thetotal population, the lower SES class, and the higher SES group of individuals. In order to do this, they usedcensus data, such as distribution of educational level, occupational categories, working age, unemploymentrate, family size, crowding and the proportion of dwellings rented versus owned. Although the study wasset in Rome, which is similar in climate and population size, the study deduced SES specific ERFs from thecorrelation between PM10 and daily average non-accidental mortality.
Within the sensitivity analysis, the most current PM10 data from Athens combined with the reduction inlevels due to each individual intervention study were used in conjunction with the SES related ERFs tocalculate the full range of preventable deaths. The lower and upper error bars represent the 95% confidenceintervals that were systematically calculated from the least and most extreme study. This is justifiable dueto the CI of each study being within the most extreme intervals. The calculations were performed for thethree particulate level scenarios to show the potential range of effects within Athens, and within each typeof current exposure, the effects on total population, high, and low SES groups.
B.4 Simulation
In an effort to further extrapolate the HIA calculations and findings to Athens, Greece, a hypotheticalsimulation was performed to look at the potential range of benefits resulting from increasing reductiondue to intervention strategies (Figure 8). The simulation shows the preventable daily deaths per percentincrease in PM level reduction due to an intervention starting with the business as usual scenario, i.e. notimplementing any intervention strategies, expanding up to an intervention specific reduction in PM of 30%.
26

The preventable daily average non-accidental mortality corresponding to each percent increase in reductionwas calculated using the current average exposure levels of PM within Athens, the ERF’s for different SESsubgroups, and the average daily mortality from literature within Athens (Forastiere et al., 2007; Stafoggiaet al., 2017). Consistent with the other HIA calculations, the lower and upper bounds of the confidenceintervals were calculated systematically.
C Air Pollution Surveillance in Athens, Greece
Particulate matter is measured within Athens from a multitude of different stations. For the purposes of thisstudy, a set of stations measuring PM10 that were the most representative of Athens’ different environmentswere selected due to the advice of Dr. Evangelos Gerasopoulos, a local expert. These stations are described inTable 2 and they are spatially represented in Figure 12. The measurements were taken hourly, but averagedinto a daily value and were taken using beta radiation absorption methods. The Aristotle Station (1) hadthe highest average levels of PM10 (40.71 µg/m3), perhaps due to its proximity to the city center and beingwithin an urban location with traffic. The St. Paraskevi station represented the minimum average valuesof PM10 for the course of 2015 (20.95 µg/m3), which also follows intuition due to its suburban-backgroundcharacteristics and location on the outskirts of the city area. The average PM10 concentration for all fivestations was 32.16 µg/m3, which is very close to the value used by Stafoggia et al. (36 µg/m3) in the mainHIA analysis of this report. Air pollution has been monitored and made publicly available from 1984 through2015 at the time of this report, and annual reports produced starting in 2001, where the data, trends, and in-formation regarding air quality and related policies are discussed (Ministry of Environment & Energy, 2016).
Station No. &Name
MonitoringStation Type
Height (metersabove sea level)
Latitude Longitude
1. Aristotle(Αριστοτέλους)
Urban-Traffic 95 37◦59’16"N 24◦43’39"E
2. Lycovrisi(Λυκόβρυση)
Suburban 234 38◦04’04"N 23◦47’19"E
3. Maroussi(Μαρούσι)
Urban-Traffic 170 38◦01’51"N 23◦47’14"E
4. Nea Smyrni(Νέα Σμύρνη)
Suburban-Background
50 37◦55’55"N 23◦42’46"E
5. St. Paraskevi(Αγ. Παρασκευή)
Suburban-Background
290 37◦59’42"N 23◦49’09"E
Table 2: Information regarding the particulate matter monitoring stations in Athens, Greece as they corre-spond to Figure 12. This data was taken from the Ministry of Environment & Energy.
27

Figure 11: Graph displaying the 2015 average annual PM10 concentrations from five representative moni-toring stations show in Figure 12 within the Athens metropolitan area. The annual average is just over 32µg/m3 for all stations. Data from the Ministry of Environment & Energy.
28

Figure 12: Map of Athens displaying the locations of the five air pollution monitoring stations used withinthis HIA study. This map is adapted from geodata.gov.gr.
29