cosmetic side effects and complications of variable- pulsed erbium
TRANSCRIPT
Cosmetic
Side Effects and Complications of Variable-Pulsed Erbium:Yttrium-Aluminum-GarnetLaser Skin Resurfacing: Extended Experiencewith 50 PatientsElizabeth L. Tanzi, M.D., and Tina S. Alster, M.D.Washington, D. C.
Recent advances in technology have provided laser sur-geons with new options for cutaneous laser resurfacing.Despite its popularity, there is limited information on theshort-term and long-term side effects and complicationsof variable-pulsed erbium:yttrium-aluminum-garnet (er-bium:YAG) laser skin resurfacing. The purpose of thisstudy was' to prospectively evaluate postoperative woundhealing, side effects, and complications of multiple-pass,variable-pulsed erbium:YAG laser skin resurfacing for fa-cial photodamage, rhytides, and atrophic scarring. Fiftyconsecutive patients with facial photodamage, rhytides, oratrophic scarring were treated with a variable-pulsed er-bium:YAG laser. Side effects and complications relating topostoperative healing, erythema, and pigmentary changeswere tabulated. Patients were evaluated at postoperativedays 3 through 7 and at 1, 3, 6, and 12 months after laserskin resurfacing. The average time for reepithelializationwas 5.1 days. Prolonged erythema (>1 month) was ob-served in three patients (6 percent). Transient hyperpig-mentation occurred in 20 patients (40 percent), with anaverage duration of 10.4 weeks. No cases of hypopigmen-tation or scarring were seen. In summary, a variable-pulsed erbium:YAG laser can safely be used for the treat-ment of facial photodamage, rhytides, and atrophicscarring. Although more postoperative erythema is seenafter variable-pulsed erbium:YAG laser treatment than isusually produced with a short-pulsed erbium:YAG sys-tem, the side-effect profile and recovery period aftervariable-pulsed erbium:YAG laser skin resurfacing stillare more favorable than after multiple-pass carbon di-oxide laser skin resurfacing. (Plast. Reconstr. Surg. Ill:1524, 2003.)
Cutaneous laser resurfacing has revolution-ized the treatment of facial photodamage, rhyt-ides, and atrophic scarring. Based on the prin-ciples of selective photothermolysis, cutaneousresurfacing lasers target water-containing tis-
sue, resulting in controlled vaporization.' Asso-ciated residual thermal injury in the dermisinitiates collagen shrinkage and remodeling.v "Although other methods of cutaneous resur-facing such as dermabrasion and chemicalpeels are still in use, the clinical results theytypically produce do not equal those of con-trolled laser vaporization.?:"!
Laser systems currently available for cutane-ous resurfacing include high-energy pulsedand scanned carbon dioxide, short-pulsed er-bium:YAG, and "modulated" (variable-pulsederbium:YAG or combined erbium:YAG/carbon dioxide) systems. Although carbondioxide laser skin resurfacing has beenshown to effect excellent clinical improve-ment of facial photodamage, rhytides, andatrophic scars,6-8,l2-16it is associated with anextended reepithelialization period and, insome cases, prolonged erythema that maypersist for several months.Fr'" More impor-tant, the potential for delayed-onset, perma-nent hypopigmentation may be seen in asmany as 20 percent of patients following mul-tiple-pass carbon dioxide laser treatment."In response to these disadvantages, other la-ser systems were developed in an attempt tolimit the prolonged recovery period and po-tentially high morbidity of these procedures.
The short-pulsed erbium:YAG laser was ap-proved for cutaneous laser resurfacing by theFood and Drug Administration in 1996. The2940-nm wavelength emitted by the erbium:
From the Washington Institute of Dermatologic Laser Surgery. Received for publication February 5, 2002.
DOl: 10.1097/01.PRS.0000049647.65948.50
1524

Vol. 111, No. 4 / ERBIUM:YAG LASER RESURFACING
YAG laser corresponds to the peak absorptioncoefficient of water and is absorbed 12 to 18times more effectively by superficial, water-containing cutaneous tissue than the 10,600-nmwavelength of the carbon dioxide laser.s! Short-pulsed (250 /-Lsec)erbium:YAGlasers reliably ab-late 5 to 15 /-Lmof tissue per pass at a fluence of5 J/cm2, producing a residual zone of thermaldamage not exceeding 15 /-Lm.22,23These findingsare in contrast to the changes observed aftercarbon dioxide cutaneous laser resurfacing,which produces 20 to 60 /-Lmof tissue ablationand up to 150 ius: of residual thermal damageper pass.As a result of precise tissue ablation anda limited zone of thermal damage, short-pulsederbium:YAG laser treatment results in fasterreepithelialization and an improved side-effectprofile compared with carbon dioxide cutaneouslaser skin resurfacing.24-27 Because of these ad-vantages, it was initially postulated that theshort-pulsed erbium:YAG laser system wouldcompletely replace the carbon dioxide laser asa resurfacing tool; however, this initial enthu-siasm was tempered by poor intraoperative he-mostasis and the system's limited ability toeffect significant collagen shrinkage. 8,22
To address these limitations, modulated er-bium:YAG laser systems were developed to im-prove hemostasis and increase the amount ofcollagen shrinkage. With extended pulse dura-tions up to 500 /-Lsec,variable-pulsed erbium:YAGlaser systems combine tissue ablation withinduction of dermal collagenization by meansof controlled thermal injury." Despite the in-creasing popularity of variable-pulsed erbium:YAG laser skin resurfacing treatments, there islimited information documenting the short-term and long-term side effects and complica-tions of this procedure. The objective of thisstudy was to prospectively evaluate postopera-tive wound healing, side effects, and complica-tions of multiple-pass, variable-pulsed erbium:YAGlaser skin resurfacing for the treatment offacial photodamage, rhytides, and atrophicscarnng.
MATERIALS AND METHODS
Fifty consecutive patients (47 female andthree male, aged 21 to 71 years, skin photo-types I through V) with moderate-to-severe fa-cial photodamage, rhytides, or atrophic scarswere included in the study. Five patients (10percent) reported dermabrasion to the in-volved areas more than 3 years before studyinitiation. Eleven patients (22 percent) had
1525
received collagen injections in the remote past.Three patients (6 percent) had undergone afull face lift more than 5 years before the study.Two patients (4 percent) had undergone full-face carbon dioxide laser skin resurfacing 6years previously, and one patient (2 percent)had received a phenol peel more than 5 yearsbefore the study.
Each patient received laser treatment in anoutpatient surgical facility by a single surgeon(T.S.A.) with a dual-mode sequential ablation/coagulation pulsed erbium:YAG laser (Con-tour; Sciton, Palo Alto, Calif.). Cutaneous an-esthesia was obtained with regional nerveblocks using 1% lidocaine with 1:200,000 epi-nephrine. For full-face procedures, intrave-nous anesthesia was administered by a certifiednurse anesthetist using a combination ofpropofol, midazolam, fentanyl, and ketamine.The laser was calibrated to 90-/-Lmablation(22.5 J/cm2) and 50-/-Lmcoagulation using asquare scanning handpiece with 50 percentoverlap to vaporize the epidermis in a singlepass over the entire face. An additional one totwo regional passes were delivered using iden-tical laser settings to treat residual rhytides orscars. Laser scans were placed adjacent to oneanother without overlapping, thereby prevent-ing char formation. Partially desiccated skinwas thoroughly removed with saline-soakedgauze between each laser pass, producing skinwith a clean, pale-pink hue with minimal to nobleeding. The partially desiccated tissue re-maining from the final laser pass was left intactto serve as a biological wound dressing.
Immediately after treatment, Aquaphor oint-ment (Beirsdorf, Inc., Wilton, Conn.) was ap-plied to the irradiated skin. Each patient wasinstructed to perform gentle facial rinses withdilute acetic acid soaks several times daily, fol-lowed by application of Aquaphor and a cool-ing mask (SkinVestment, Inc., Washington,D.C.). A 10-day course of prophylactic antiviraltreatment (valacyclovir 500 mg two times perday) was prescribed beginning on the day ofsurgery. Patients were observed closely duringthe first postoperative week, during which timeany residual coagulated debris was gently loos-ened and/or removed with cool compresses.All patients were able to apply camouflagemakeup within 7 to 10 days postoperatively.
The patients were evaluated daily duringpostoperative days 3 through 7, and at 1, 3, 6,and 12 months after laser skin resurfacing. Thepresence and duration of side effects and com-
1526plications were recorded at each postoperativepatient visit (Fig. 1). If prolonged erythema orhyperpigmentation was noted, the patient wasevaluated every 2 weeks until its complete res-olution. Daily use of topical 5% glycolic acid(M.D. Forte; Herald Pharmacal, Inc., ColonialHeights, Va.), and/or 0.1% Nfurfuryladenine(Kinerase; ICN Pharmaceuticals, Aurora,Ohio), and/or kojic acid/lactic acid mix(KojiLac-C; Young Pharmaceuticals, Wethers-field, Conn.) was prescribed for patients withhyperpigmentation, as were biweekly tomonthly 30% glycolic acid peels that were per-formed in-office until the dyspigmentation wascorrected (Fig. 2).
RESULTS
The average time to reepithelialization (de-fined by the absence of serous discharge andthe presence of new skin) was 5.1 days. Post-
PLASTIC AND RECO STRUCTIVE SURGERY, Aprill, 2003
treatment erythema was seen in all patientsstudied; however, it persisted longer than 1month in three patients (6 percent). Postinflam-matory hyperpigmentation was observed at theJ-month follow-up visit in 20 patients (40 per-cent), predominantly in those patients withdarker skin tones. Total resolution of dyspigmen-tation was noted within an average of 10.4 weeks.Mild acne occurred in eight patients (16 per-cent) during the first postoperative week, pre-sumably because of the use of occlusive oint-ment. All cases of acne were easily controlledwith oral minocycline (75 mg two times per dayfor 1 week). Five patients experienced milia (10percent) and dermatitis was noted in three pa-tients (6 percent), the latter condition resolvingwith the use of a mild topical corticosteroidcream. No cases of herpetic or fungal infectionswere encountered; however, nine patients (18percent) experienced limited superficial bacte-
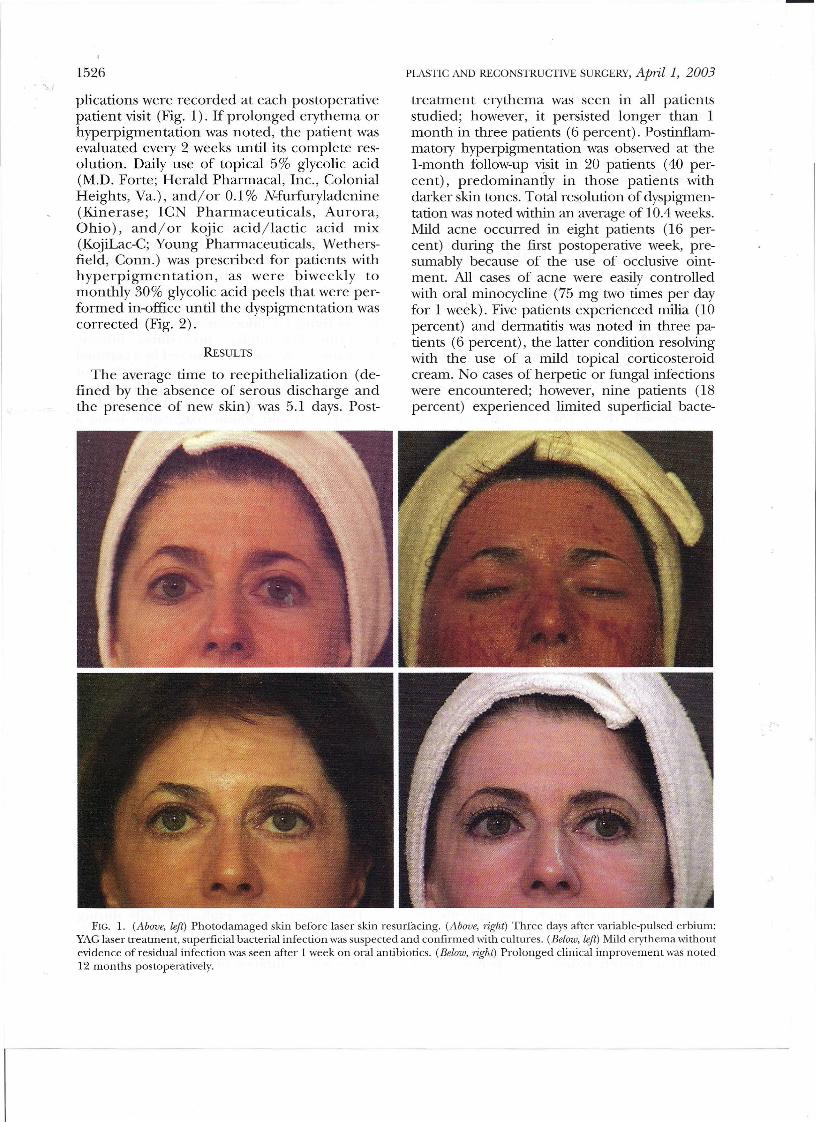
FIG. 1. (Above, left) Photodamaged skin before laser skin resurfacing. (Above, right) Three days after variable-pulsed erbium:YAG laser treatment, superficial bacterial infection was suspected and confirmed with cultures. (Below, left) Mild erythema withoutevidence of residual infection was seen after 1 week on oral antibiotics. (Below, right) Prolonged clinical improvement was noted12 months postoperatively.

Vol. 111, No. 4 / ERBIUM:YAG LASER RESURFACING 1527
FIG. 2. (Above, left) Moderate atrophic scarring on the cheeks of a man with skin phototype N. (Above, right) Completereepithelialization and mild erythema wa~noted 1 week after variable-pulsed erbium:YAGlaser treatment. (Below, left) Hyper-pigmentation evident at 1 month postoperatively resolved with the use of topical bleaching creams and light glycolic acid peelsby the third postoperative month (below, right).
DISCUSSION
Laser skin resurfacing has become one ofthe most popular techniques for the treatment
of cutaneous photodamage, rhytides, and atro-phic scars." Although previous reports havedocumented the efficacy of modulated erbium:YAG laser skin resurfacing for these indica-tions,30-37limited data exist concerning the fre-quency, severity, and duration of side effectsand complications associated with its use.
The immediate postoperative recovery pe-riod and incidence of prolonged erythema are
rial infections that responded fully to oral cipro-floxacin (500 mg two times per day for 5 days).No hypopigmentation or hypertrophic scarringwas observed in any study patient throughout the12-month study period (Table I).
TABLE ISide Effects of Variable-Pulsed Er:YAGLaser Treatment"
ProlongedSkin Type n Erythema Hyperpigmcntation Infection Acne Milia Dermatitis Hypopigmentation Scarring
I 20 2 2 4 3 2 1 0 0II 16 1 4 3 4 2 1 0 0III 7 0 7 1 1 1 1 0 0IV 5 0 5 1 0 0 0 0 0V 2 0 2 0 0 0 0 0 0Total 50 3 (6%) 20 (40%) 9 (18%) 8 (16%) 5 (10%) 3 (6%) 0 0
* Er:YAG, erbium-yttrium-argon-garnet.
1528more favorable with variable-pulsed erbium:YAG laser treatment than with cutaneous car-bon dioxide laser resurfacing. Prolonged ery-thema occurs in a significantly large number ofpatients following multiple-pass carbon diox-ide laser skin resurfacing.6,17-20 In the presentstudy of 50 patients treated with a variable-pulsed erbium:YAG laser, reepithelializationwas complete in an average of 5 days, and onlythree (6 percent) cases of prolonged erythemawere seen. In a split-face comparison of 16patients following pulsed carbon dioxide andvariable-pulsed erbium:YAG laser skin resurfac-ing, Rostan et aP6 reported decreased ery-thema, less edema, and faster healing on theside treated with the erbium:YAG laser.
Postinflammatory hyperpigmentation is notuncommon following cutaneous laser resurfac-ing.8,17-20 Jeong and Kye34 documented hyper-pigmentation in eight of 35 patients (23 per-cent, skin photo types III through V) treatedwith a variable-pulsed erbium:YAG laser for pit-ted acne scars. Similarly, 40 percent of ourpatient -predominantly those with darkerskin tones-developed hyperpigmentation. Allcases of hyperpigmentation responded com-pletely to a combination oflight chemical peelsand topical bleaching creams. Although hyper-pigmentation following variable-pulsed erbi-um:YAG laser skin resurfacing can last longerthan that seen after treatment with a short-pulsed erbium:YAG laser, it is not as persistentas that observed after multiple-pass carbon di-oxide laser resurfacing (average: variable-pulsed erbium:YAG laser, 10.4 weeks; carbondioxide laser, 16 weeks) .17,22,37
Delayed-onset, permanent hypopigmenta-tion is a serious complication of any type oflaser skin resurfacing procedure and oftentakes several months to develop. To date, therehave been only three published cases of hypo-pigmentation as a consequence of variable-pulsed erbium:YAG laser treatment.Y'" Al-though hypopigmentation was not observed inour study population at the I-year follow-upevaluation, additional confirming studies arewarranted to assess its true incidence.
In conclusion, variable-pulsed erbium:YAGlaser skin resurfacing is relatively safe for facialphotodamage, rhytides, and atrophic scarring.The variable-pulsed erbium:YAG laser offersseveral advantages over short-pulsed erbium:YAG laser systems, including improved intraop-erative hemostasis and visibility and enhancedclinical outcomes. Although the reepithelial-
PLASTIC AND RECONSTRUCTIVE SURGERY, April 1, 2003
ization process and the persistence of postop-erative erythema after variable-pulsed erbium:YAG laser resurfacing are more prolongedthan those seen following short-pulsed erbium:YAG treatment, the overall side-effect profileand recovery period' are more favorable thanafter multiple-pass carbon dioxide laser resur-facing. In addition, and of particular impor-tance in the treatment of patients with darkerskin tones, the postinflammatory hyperpig-mentation seen with variable-pulsed erbium:YAG laser skin resurfacing is less persistentthan that observed after treatment with thecarbon dioxide laser.Tina S. Alster, M.D.Washington Institute of Dermatologic Laser Surgery2311 M Street, N.W, Suite 200Washington, D. C. [email protected]
REFERENCES
1. Anderson, R. R, and Parrish,]. A. Selective photother-molysis: Precise microsurgery by selective absorptionof pulsed radiation. Science 220: 524, 1983.
2. Ross, E. V., McKinlay, J. R, and Anderson, R R. Whydoes carbon dioxide resurfacing work? A review. Arch.Dermatol. 135: 444, 1999.
3. Smith, K. S., Skelton, H. G., Graham,]. S., et al. Depthof morphologic skin damage and viability after one,two and three passes of a high-energy, short-pulse CO2
laser (TruPulse) in pig skin. Dermatol. Surg. 37: 204,1997.
4. Ross, E. V., aseef, G. S., McKinlay,]. R., et al. Com-parison of carbon dioxide laser, erbium:YAG laser,dermabrasion, and dermatome: A study of thermaldamage, wound contraction, and wound healing in alive pig model. Implications for skin resurfacing. JAm.Acad. Dermatol. 42: 92, 2000.
5. Alster, T. S., Kauvar, A. N. B., and Geronemus, R G.Histology of high-energy pulsed CO2 laser resurfacing.Semin. Cutan. JvIed. Surg. 15: 189, 1996.
6. Alster, T. S., Nanni, C. A., and Williams, C. M. Com-parison of four carbon dioxide resurfacing lasers: Aclinical and histopathologic evaluation. Dermatol. Surg.25: 153, 1999.
7. Alster, T. S., and Garg, S. Treatment of facial rhytideswith a high-energy pulsed CO2 laser. Plast. Reconstr.SUlK. 98: 791, 1996.
8. Alster, T. S. Cutaneous resurfacing with CO2 and erbi-um:YAGlaser: Preoperative, intraoperative, and post-operative considerations. Plast. Reconstr. Surg. 103:619, 1999.
9. Fitzpatrick, R. E. Resurfacing procedures: How do youchoose? Arch. Dermatol. 136: 783, 2000.
10. Kitzmiller, W.]., Visscher, M., Page, D. A., et al. A con-trolled evaluation of dermabrasion versus CO2 laserresurfacing for the treatment of perioral wrinkles.Plast. Reconstr. SUlK. 106: 1366, 2000.
11. Fitzpatrick, R. E., Tope, W. D., Goldman, M. P., et al.Pulsed carbon dioxide laser, trichloroacetic acid,Baker-Gordon phenol, and dermabrasion: A com-parative clinical and histologic study of cutaneous
Vol. 111, No.4 / ERBIUM:YAG IASER RESURFACING
"I resurfacing in a porcine model. Arch. Dermatol. 132:469, 1996.
12. Walia, S., and Alster, T S. Prolonged clinical and his-tologic effects from CO2 laser resurfacing of atrophicacne scars. Dermatol. Surg. 25: 926, 1999.
13. Apfelberg, D. B. Ultrapulse carbon dioxide laser withCPG scanner for full-face resurfacing of rhytides, pho-toaging, and acne scars. Plast. Reconstr. Surg. 99: 1817,1997.
14. Fitzpatrick, R. E., Goldman, M. P., Satur, N. M., et al.Pulsed carbon dioxide laser resurfacing of photo-agedfacial skin. Arch. Dermatol. 132: 395, 1996.
15. Alster, T S., and West, T B. Resurfacing atrophic facialscars with a high-energy, pulsed carbon dioxide laser.Dermatol. Surg. 22: 151, 1996.
16. Waldorf, H. A., Kauvar, A. N. B., and Geronemus, R. G.Skin resurfacing of fine to deep rhytides using a char-free carbon dioxide laser in 47 patients. Dermatol. Surg.21: 940, 1995.
17. Nanni, C. A., and Alster, T. S. Complications of carbondioxide laser resurfacing: An evaluation of 500 pa-tients. Dermatol. Surg. 24: 315, 1998.
18. Alster, T S., and Lupton,]. R. Treatment of complica-tions of laser skin resurfacing. Arch. Facial Plast. Surg.2: 279, 2000.
19. Alster, T S., and Lupton,]. R. Prevention and treat-ment of side effects and complications of cutaneouslaser resurfacing. Plast. Reconstr. Surg. 109: 308, 2002.
20. Bernstein, L.]., Kauvar, A. N. B., Grossman, M. c., et al.The short- and long-term side effects of carbon diox-ide laser resurfacing. Dermatol. Surg. 23: 519, 1997.
21. Walsh,]. T,Jr., Flotte, T]., and Deutsch, T F. Er:YAGlaser ablation of tissue: Effect of pulse duration andtissue type on thermal damage. Lasers Surg. M.ed. 9:314, 1989.
22. Alster, T S. Clinical and histologic evaluation of sixerbium:YAG lasers for cutaneous resurfacing. LasersSurg. Med. 24: 87, 1999.
23. Alster, T S., and Lupton,]. R. Erbi m:YAGcutaneouslaser resurfacing. Dermaiol. Clin. 19: 453, 2001.
1529
24. Bass, L. S. Erbium:YAG laser skin resurfacing: Prelim-inary clinical evaluation. Ann. Plast. Surg. 40: 328,1998.
25. Weinstein, C. Erbium laser resurfacing: Current con-cepts. Plast. Reconstr. Surg. 103: 602, 1999.
26. Weiss, R. A., Harrington, A. C., Pfau, R. C., et al. Peri-orbital skin resurfacing using high-energy erbium:YAGlaser: Results in 50 patients. Lasers Surg. Med. 24:81, 1999.
27. Khatri, K. A., Ross, V., Grevelink,]. M., et al. Compar-ison of erbium:YAG and carbon dioxide lasers in re-surfacing of facial rhytides. Arch. Dermatol. 135: 391,1999.
28. Zachary, C. B. Modulating the Er:YAGlaser. Lasers Surg.Med. 26: 223, 2000.
29. Alster, T S.,and Lupton,]. R. An overviewof cutaneouslaser resurfacing. Clin. PZast. Surg. 28: 37, 2001.
30. Weinstein, C. Modulated dual mode erbium/C02 la-sers for the treatment of acne scars. J Cutan. LaserTher. 1: 203, 1999.
31. Weinstein, C., and Scheflan, M. Simultaneously com-bined Er:YAGand carbon dioxide laser (Derma K) forskin resurfacing. Clin. PZast. Surg. 27: 273, 2000.
32. Goldman, M. P., Marchell, N., and Fitzpatrick, R. E. La-ser skin resurfacing of the face with a combined CO2/
Er:YAGlaser. Dermatol. Surg. 26: 102, 2000.33. Pozner, ]. N., and Roberts, T L., III. Variable-pulse
width Er:YAGlaser resurfacing. Clin. Plast. Surg. 27:263,2000.
34. Jeong,]. T, and Kye,Y. C. Resurfacing of pitted facialacne scars with a long-pulsed Er:YAGlaser. Dermatol.Surg. 27: 107, 2001.
35. Sapijaszko,M.]. A., and Zachary, C.B. Er:YAGlaser skinresurfacing. Dermatol. CZin. 20: 87,2002.
36. Rostan, E. F., Fitzpatrick, R. E., and Goldman, M. P.Laser resurfacing with a long pulse erbium:YAG lasercompared to the 950 ms pulsed CO2 laser. Lasers Surg.Med. 29: 136, 2001.
37. Alster, T S. Cutaneous resurfacing with Er:YAGlasers.Dermaiol. Surg. 26: 73, 2000.