cosmetic - mansosp.mans.edu.eg/tmahdy/surgeons/ebooks/books/a review of bariatri… · cosmetic a...
TRANSCRIPT

COSMETIC
A Review of Bariatric Surgery Procedures
Morbid obesity is a chronic condition thatis extremely difficult to treat. In additionto unhealthy food choices and lifestyles,
effective treatment for morbid obesity is compli-cated by such factors as genetics and complexbehavioral issues, which are not fully under-stood. Although diet and exercise remain thefirst choices in obesity therapy, they are rarelysuccessful in achieving long-term weight loss. Ad-equate pharmacologic intervention remains elu-sive, and even among patients who do achieveweight loss through diet and exercise and/orpharmacologic intervention, only a low percent-age actually maintain this loss for any significantperiod of time.1,2
Bariatric surgery is currently the only therapyeffective at achieving weight loss with significantimprovement or resolution of comorbidities.3 Itis important that plastic surgeons planning bodycontouring surgery on massive weight loss pa-tients understand the varying physiological ef-fects these different procedures have on thebody. Despite losing massive amounts of weightwith significant overall improvements in health,these patients differ physiologically as comparedwith normal-weight individuals.
Bariatric procedures are typically classified asrestrictive, malabsorptive, or a combination ofboth. Purely malabsorptive procedures, the ear-liest bariatric surgeries performed, interrupt thedigestive process, whereas restrictive procedures,as the name implies, restrict food intake by al-tering the size of the stomach. The more com-mon techniques used today involve a combina-tion of both restriction and malabsorption.While these procedures are highly effective inhelping patients achieve and maintain weightloss, the patients are at risk for lifelong prob-lems, such as anemia and other nutritional defi-ciencies, that can ultimately affect the outcomeof body contouring surgery.
HISTORYBariatric surgery first began in the 1950s and
evolved from the experiences of general surgeonswho had to remove segments of patients’ small
intestines because of disease and/or necrosis. Itwas noted that patients who experienced “short-gut syndrome,” defined as removal of a significantportion of the small intestine, lost weight aftertheir operation. This was attributed to a decreasein the total absorptive surface area of the remain-ing intestine, which caused malabsorption of food.Different segments of the small intestine are re-sponsible for the absorption of vitamins, minerals,fats, proteins, and other nutrients, thus patientswith short-gut syndrome often experience sometype of vitamin and mineral deficiencies or diar-rhea due to food not being absorbed and/or di-gested properly. Early bariatric surgical proce-dures experimented with variations of the short-gut syndrome, and although patients lost weight,severe side effects began to emerge that motivatedsurgeons to enhance and improve their tech-nique.
Much of the early research done on the roleof the small intestine in digestion and absorption,as well as on bariatric surgery, took place at theUniversity of Minnesota. It was there, in the early1950s, that Dr. Richard L. Varco performed one ofthe first jejunoileal bypass procedures. In this pro-cedure, the proximal small intestine is joined tothe distal large intestine, bypassing a large sectionof the lower bowel. In 1954, Kremen et al.4 pub-lished the first article on bariatric surgery to ap-pear in a peer-reviewed journal, presenting theresults of a jejunoileal bypass procedure they hadperformed. Concurrently, surgeons in Sweden re-ported using a similar procedure, although theyexcised, rather than bypassed, portions of thesmall intestine.
The “14 � 4,” or end-to-side, jejunoileal bypasswas described by Payne and DeWind5 and was avery popular technique for 15 to 20 years. In thisprocedure, the first 35.6 cm of the jejunum wasconnected to the last 10.2 cm of the ileum, thusreducing the absorptive stream from 345 to 546cm to 45.7 cm. Although the jejunoileal bypasscaused nutritional deficiencies, mineral and elec-trolyte imbalances, and frequent diarrhea, pa-tients succeeded in losing weight. As these patientswere followed (for 10 to 20 years after surgery),more serious problems began to emerge, includ-ing acute hepatic failure, cirrhosis, and evendeath. It was determined that these more life-threatening issues were due to the overgrowth ofbacteria in the bypassed small intestine, where
Received for publication July 6, 2005; revised October 22,2005.Copyright ©2005 by the American Society of Plastic Surgeons
DOI: 10.1097/01.prs.0000196293.35455.4d
www.plasreconsurg.org8S

migration into the portal venous system and be-yond caused serious problems. Approximately 5percent of patients died during the first postop-erative year after these early, “short-gut” proce-dures, and it is estimated that as many as 30 to 50percent of patients developed cirrhosis within 25years of surgery. Because of the serious nature ofthese adverse events, the jejunoileal bypass is nolonger a recommended bariatric surgery proce-dure.
The next major development in malabsorptivebariatric procedures began to emerge in the1970s. Dr. Nicola Scopinaro of Italy developed aprocedure known as the biliopancreatic diversion.This procedure differed from the jejunoileal by-pass in that much less of the small intestine wasrendered nonfunctional, resulting in fewer liverproblems. Over time, significant modifications tothe procedure have taken place. Today, this sur-gery involves two steps. In the first step, a limitedgastrectomy is performed to reduce the stomachcapacity by a third, to 118 to 148 cc. In the secondpart of the procedure, a long biliopancreatic ormalabsorptive limb is created, with a 50-cm com-mon channel for absorption (Fig. 1).
One serious nutritional complication with bil-iopancreatic diversion is that of protein-caloriemalnutrition, which, on occasion, may require to-tal parenteral nutrition. Other complications in-clude anemia and bone demineralization. Of thecurrent bariatric procedures in use, the biliopan-
creatic diversion is the most complex and inducesthe greatest degree of malabsorption, which ac-counts for its success in maintaining weight loss.Some patients tend to favor this operation becauserequirements are minimal in terms of dietarymodification. Recent data from Dr. Scopinaro in-dicate that 72 percent excess body weight loss ismaintained for 18 years. In terms of the amountand duration of weight loss, these results are thebest that have been published to date.6
A modification of the original biliopancreaticdiversion, the biliopancreatic diversion with duo-denal switch, evolved under the guidance of Ca-nadian surgeon Dr. Picard Marceau and his col-leagues in Canada. This technique incorporates asleeve gastrectomy, leaving the pylorus of thestomach intact (Fig. 2). The reported advantage ofthe duodenal switch in this procedure is the elim-ination of stomal ulcer formation and dumpingsyndrome. (Dumping syndrome is a physiologicreaction in which certain foods that are typicallyhigh in sugar content cause “dumping,” charac-terized by symptoms of nausea, flushing and sweat-ing, light-headedness, and watery diarrhea.)
Although these largely malabsorptive proce-dures help bring about significant weight loss, theyplace patients at highest risk for long-term nutri-tional deficiencies and require careful long-termfollow-up. In addition, most patients will experi-ence an undesirable side effect of frequent, foul-smelling stools. The biliopancreatic diversion,therefore, has not gained widespread use.
Fig. 2. Biliopancreatic bypass with duodenal switch (BP:DS).Fig. 1. Scopinaro biliopancreatic bypass (BPB), with the limbsidentified. BPD, biliopancreatic diversion.
Volume 117, Number 1S • Bariatric Surgery Procedures
9S

Dr. Edward Mason of the University of Iowa tooka different approach in 1966 and developed whathas now become known as the gastric bypass,Roux-en-Y gastric bypass, or RYGB. In this proce-dure, both the size of the stomach and the outletfrom the reduced stomach are restricted. This sig-nificantly reduces the amount of food a patient isable to consume. The gastric bypass utilizes a lesserdegree of malabsorption, in which the new stomachpouch is connected to a section of the jejunum,bypassing the distal stomach, all of the duodenum,and some of the proximal jejunum. The earliestforms of gastric bypass were referred to as loop gas-tric bypass. This was later modified because the loopaspect of the procedure allowed for severe reflux ofbile and other digestive juices into the esophagus,with subsequent irritation and ulcer formation. Re-cently, this procedure has resurfaced at a small num-ber of centers, where it is performed laparoscopicallyand referred to as the “mini gastric bypass.” Thesepatients, however, continue to be at risk for alkalinegastritis and possibly a higher incidence of esopha-geal dysphagic changes.
Dr. Ward Griffen developed a modificationof the gastric bypass procedure by replacing theloop aspect with a Roux-en-Y gastrojejunostomy(Fig. 3). The general term “gastric bypass” nowrefers to the Roux-en-Y technique, in which thesmall intestine is reconfigured into a Y with twolimbs (Roux and biliopancreatic) and a com-mon channel. A thumb-sized stomach pouch iscreated by stapling just below the esophagus.The jejunum is divided approximately 30 cmbelow the stomach, and the new pouch is con-nected to the Roux limb, also known as thealimentary tract. The gastric remnant, duode-num, and first portion of the jejunum drain viathe biliopancreatic limb, with the digestivejuices (gastric secretions, bile, and digestive en-zymes) entering the common channel distally.This modification reduces or eliminates theproblem of bile-induced gastritis seen in theloop gastric bypass. One variant of the gastricbypass, the long-limb gastric bypass, utilizes agreater degree of malabsorption, with a bilio-pancreatic limb of at least 150 cm and withconsequences more like those of the biliopan-creatic diversion. The difference is that thelong-limb gastric bypass uses the jejunum as analimentary tract, whereas the ileum serves thisfunction in the biliopancreatic diversion.
Due in large part to fewer postoperative com-plications and durable long-term weight loss, gas-tric bypass has quickly become the most com-monly performed bariatric procedure.
PURELY RESTRICTIVE PROCEDURESIn an attempt to eliminate the long-term
effects of malabsorption, Dr. Mason and othersworked on developing purely restrictive bariat-ric procedures. This led to a procedure knownas the vertical banded gastroplasty (Fig. 4). Inthis procedure, a circular “window” is madethrough the stomach a few inches below theesophagus. A surgical stapler is used to create asmall vertical pouch by putting a row of staplesfrom the window toward the esophagus. Thepouch is carefully measured to hold approxi-mately 15 ml of solid food. A polypropylene
Fig. 3. Roux-en-Y gastric bypass with a retrocolic, retrogastricRoux limb via a laparoscopic procedure.
Fig. 4. Vertical banded gastroplasty.
Plastic and Reconstructive Surgery • January Supplement 2006
10S
band is placed through the window, around theoutlet of the pouch, and secured to itself. Theband controls the size of the outlet and keeps itfrom stretching.
The greatest advantage of the vertical bandedgastroplasty is the elimination of malabsorption toachieve weight loss. Complications include esoph-ageal reflux and stomal narrowing or widening,which may require reoperation. Although long-term weight loss is respectable with verticalbanded gastroplasty, results are not as successful asthose seen with the gastric bypass.
MODERN TRENDSModifications to the vertical banded gastro-
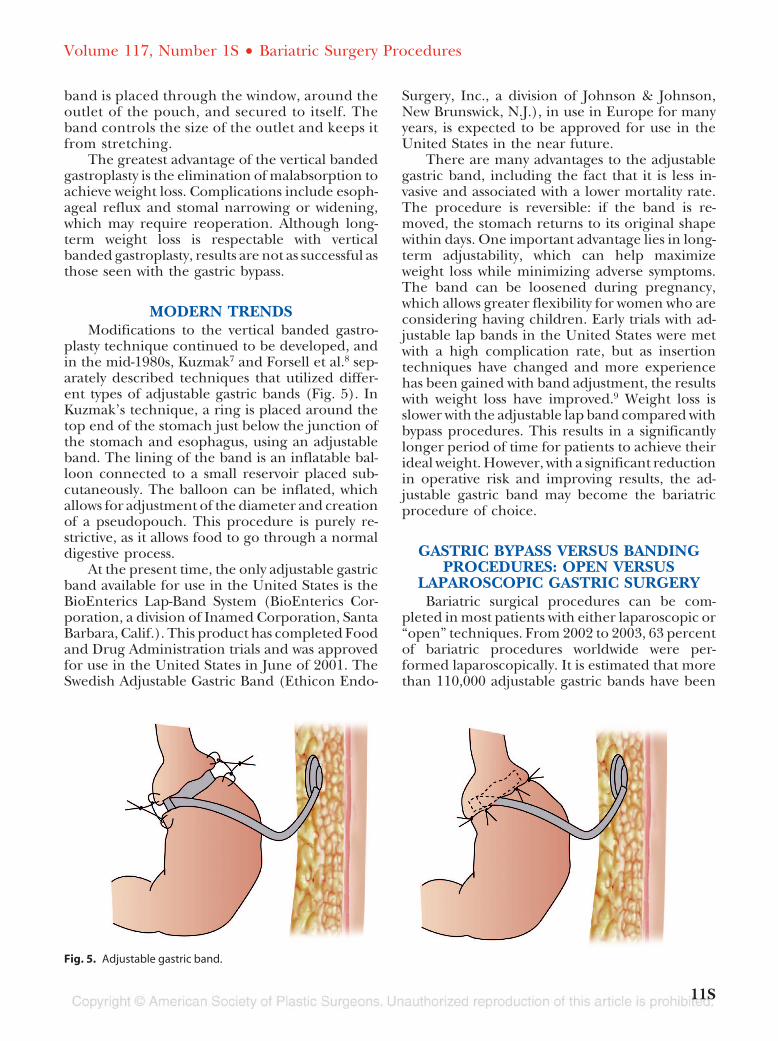
plasty technique continued to be developed, andin the mid-1980s, Kuzmak7 and Forsell et al.8 sep-arately described techniques that utilized differ-ent types of adjustable gastric bands (Fig. 5). InKuzmak’s technique, a ring is placed around thetop end of the stomach just below the junction ofthe stomach and esophagus, using an adjustableband. The lining of the band is an inflatable bal-loon connected to a small reservoir placed sub-cutaneously. The balloon can be inflated, whichallows for adjustment of the diameter and creationof a pseudopouch. This procedure is purely re-strictive, as it allows food to go through a normaldigestive process.
At the present time, the only adjustable gastricband available for use in the United States is theBioEnterics Lap-Band System (BioEnterics Cor-poration, a division of Inamed Corporation, SantaBarbara, Calif.). This product has completed Foodand Drug Administration trials and was approvedfor use in the United States in June of 2001. TheSwedish Adjustable Gastric Band (Ethicon Endo-
Surgery, Inc., a division of Johnson & Johnson,New Brunswick, N.J.), in use in Europe for manyyears, is expected to be approved for use in theUnited States in the near future.
There are many advantages to the adjustablegastric band, including the fact that it is less in-vasive and associated with a lower mortality rate.The procedure is reversible: if the band is re-moved, the stomach returns to its original shapewithin days. One important advantage lies in long-term adjustability, which can help maximizeweight loss while minimizing adverse symptoms.The band can be loosened during pregnancy,which allows greater flexibility for women who areconsidering having children. Early trials with ad-justable lap bands in the United States were metwith a high complication rate, but as insertiontechniques have changed and more experiencehas been gained with band adjustment, the resultswith weight loss have improved.9 Weight loss isslower with the adjustable lap band compared withbypass procedures. This results in a significantlylonger period of time for patients to achieve theirideal weight. However, with a significant reductionin operative risk and improving results, the ad-justable gastric band may become the bariatricprocedure of choice.
GASTRIC BYPASS VERSUS BANDINGPROCEDURES: OPEN VERSUS
LAPAROSCOPIC GASTRIC SURGERYBariatric surgical procedures can be com-
pleted in most patients with either laparoscopic or“open” techniques. From 2002 to 2003, 63 percentof bariatric procedures worldwide were per-formed laparoscopically. It is estimated that morethan 110,000 adjustable gastric bands have been
Fig. 5. Adjustable gastric band.
Volume 117, Number 1S • Bariatric Surgery Procedures
11S

placed laparoscopically (worldwide) since 1993.In the United States, however, gastric bypass stillaccounts for the vast majority of weight loss sur-gery procedures, with the most common beingsome form of the Roux-en-Y gastric bypass proce-dure. Adjustable lap bands, although gaining pop-ularity in the United States, are not covered by
most insurance companies, thus limiting their cur-rent usage. As more safety and efficacy data on lapband outcomes are gathered, and as surgeons gainmore experience with these new devices, there willmost likely be a continued increase in the numberof gastric banding procedures performed in theUnited States (Fig. 6 and Table 1).
Fig. 6. Spectrum of bariatric procedures. Courtesy of Jeffrey L. Sebastian, M.D. All rights reserved.
Table 1. Bariatric Surgery: Procedure Review
DateIntroduced Name M/R Description Comments
1954 Jejunoilealbypass
M Upper small intestine joined tolower part of intestine bypassinglarge section of lower bowel
Small intestine reduced from610 cm to 46 cm; patientsexperienced diarrhea, mineraland electrolyte imbalance, andliver cirrhosis; high mortalityrate–- discontinued
Mid-1970s Verticalbandedgastroplasty
R Create a pouch that holds 100-200cc; current technique, 59-118 cc
Cannot be adjusted withoutadditional surgery if problemsexist
1970s–1980s Gastric stapling R & M Volume of stomach reduced bystapling upper portion
Opening of band stretches,reducing initial weight loss
1977 Roux-en-Y R & M Thumb-size pouch created bystapling off upper portion ofstomach
Small size limits food intake
1979 Biliopancreaticdiversion
R & M Similar to Roux-en-Y, creates astomach pouch and bypasses partof small intestine
Larger pouch than Roux-en-Y
1988 Duodenalswitch
R & M Portion of the duodenum isbypassed from digestive continuity
May be covered by someinsurance plans
1990s Adjustablegastricbanding
R Ring placed above top end ofstomach using inflatable band
Continues to improve withavailability of new andimproved adjustable lap bands;weight loss not as dramatic aswith other bariatric procedures
M/R, malabsorptive/restrictive.
Plastic and Reconstructive Surgery • January Supplement 2006
12S

REFERENCES
1. North American Association for the Study of Obesity and theNational Heart, Lung, and Blood Institute. The Practical Guide:Identification, Evaluation, and Treatment of Overweight and Obesity inAdults (NIH Publication No. 00-4084). Bethesda, Md.: NationalInstitutes of Health, 2000.
2. North American Association for the Study of Obesity (NAASO)and the National Heart, Lung, and Blood Institute. ClinicalGuidelines on the Identification, Evaluation, and Treatment of Over-weight and Obesity in Adults: The Evidence Report (NIH PublicationNo. 98-4083). Bethesda, Md.: National Institutes of Health,1998.
3. Buchwald, H., Avidor, Y., Braunnald, E., et al. Bariatric surgery: Asystematic review and meta-analysis. J.A.M.A. 292: 1724, 2004.
4. Kremen, J. A., Linner, L. H., andNelson, C. H. An experimentalevaluation of the nutritional importance of proximal and distalsmall intestine. Ann. Surg. 140: 439, 1954.
5. Payne, J. H., andDeWind, L. T. Surgical treatment of obesity.Am. J. Surg. 118: 141, 1969.
6. Scopinaro, N., Adami, G. F., Marinari, G. M., et al. Biliopancreaticdiversion: Two decades of experience. In M. Deital and S. M.Cowan, Jr. (Eds.), Update: Surgery for the Morbidly Obese Patient.Toronto, Canada: FD Communications, 2000. Pp. 227-228.
7. Kuzmak, L. I. Silicone gastric banding: A simple and effectiveoperation for morbid obesity. Contemp. Surg. 28: 13, 1986.
8. Forsell, P., Hallberg, D., and Hellers, G. Gastric banding for mor-bid obesity: Initial experience with a new adjustable band. Obes.Surg. 3: 369, 1993.
9. Buchwald, H. Bariatric surgery worldwide. Obes. Surg. 14: 1157, 2004.
Volume 117, Number 1S • Bariatric Surgery Procedures
13S