correlation of cpg island methylator phenotype with poor prognosis in hepatocellular carcinoma
TRANSCRIPT

Experimental and Molecular Pathology 88 (2010) 112–117
Contents lists available at ScienceDirect
Experimental and Molecular Pathology
j ourna l homepage: www.e lsev ie r.com/ locate /yexmp
Correlation of CpG island methylator phenotype with poor prognosis inhepatocellular carcinoma
Yue Cheng a,b,1, Changsong Zhang a,c,1, Jun Zhao a,1, Chenyang Wang a, Yun Xu a, Zhipeng Han a,Guocheng Jiang a, Xianling Guo a, Rong Li a, Xinxin Bu a, Mengchao Wu a, Lixin Wei a,⁎a Tumor Immunology and Gene Therapy Center, Eastern Hepatobiliary Hospital, Second Military Medical University, 225 Changhai Road, Shanghai 200438, Chinab Department of Clinical Oncology, the Hospital of Heyuan City, Guangdong, Chinac Clinical Oncology Laboratory, Changzhou Tumor Hospital, Medical College of Soochow University, Jiangsu, China
⁎ Corresponding author. Fax: +86 21 65566349.E-mail address: [email protected] (L. Wei).
1 Contributed equally to this work.
0014-4800/$ – see front matter © 2009 Elsevier Inc. Adoi:10.1016/j.yexmp.2009.10.008
a b s t r a c t
a r t i c l e i n f oArticle history:Received 17 May 2009and in revised form 16 October 2009Available online 29 October 2009
Keywords:CIMPMethylationHepatocellular carcinomaPrognosis
CpG island methylator phenotype (CIMP), in which multiple genes are concurrently methylated, is animportant mechanism in hepatocellular carcinoma development. We determined a hypermethylation profilein hepatocellular carcinoma (HCC).We examined the promoter methylation status of 10 genes in 60 cases of hepatocellular carcinoma (HCC), 60cases of paired non-tumor tissues, and 6 cases of normal tissues by methylation-specific PCR.The average methylated gene numbers were significantly different between HCC and nontumor tissues(pb0.001). We found metastasis, γ-glutamyl transpeptidase (GGT) and tumor node metastasis (TNM) stagewere significantly different among patients with different CIMP status. Patients with high frequency CIMPtumors had significantly worse survival than patients with intermediate frequency or no CIMP tumors(pb0.01 and pb0.05, respectively).Our results suggested that CIMP could serve as a molecular marker of late stage and poorly prognostic HCCdevelopment.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Hepatocellular carcinoma (HCC) is one of the most commonmalignancies in the world (El-Serag, 2002). HCC patient prognosis isgenerally poor, even after surgery or chemotherapy. The 5-yearoverall survival rate is between 35% and 41% after resection of primarytumors (Lai et al., 1995; Vauthey et al., 1995) and between 47% and61% after liver transplantation (Yoo et al., 2003). Systemic chemo-therapy gives a low response rate of only 10–20% and has shown nosignificant benefit regarding overall survival (Yeo and Mok, 2005).Given this poor therapeutic efficiency, development of biomarkers foraccurate HCC diagnosis is crucial for prescribing the most timely andeffective treatment.
Cytosine methylation of CpG islands is an epigenetic genesilencing mechanism involving chromatin structure modifications(Jones and Wolffe, 1999). Aberrant hypermethylation of CpG islandshas been implicated in transcriptional silencing of various genes indifferent tumor types (Melki et al., 1999; Baylin et al., 1998; Kwong etal., 2002), including HCC (Jones and Baylin, 2002; Herman and Baylin,
ll rights reserved.
2003; Herman et al., 1996). The methylation pattern of multiplegenes can provide useful information and an overall picture ofepigenetic alterations (Costello et al., 2000). However, there are onlylimited studies on such analysis in HCC (Shen et al., 2002; Yu et al.,2003; Lee et al., 2003). The hypermethylated subtype in tumors, alsocalled the CpG island methylator phenotype (CIMP), where multiplegenes are concurrently methylated, is a novel marker for tumorprogression (Toyota et al., 1999a,b). The methylator phenotypeindicates an underlying defect in the cellular machinery leading tohypermethylation (Laird, 2003; Tanemura et al., 2009; Segditsas etal., 2008). A new unbiased study strongly suggests that a CpG islandmethylator phenotype exists, thereby offering new cancer markers(Weisenberger et al., 2006).
Differential gene expression can be associated with the metastaticpotential of cancer cells. For example, E-cadherin in gastric cancer(Graziano et al., 2004), TIMP-3 (tissue inhibitor of metalloproteinase-3)in esophageal cancer (Darnton et al., 2005), SYK(spleen tyrosinekinase) in HCC (Yuan et al., 2006), breast cancer (Yuan et al., 2001)and T-lineage acute lymphoblastic leukemia (Goodman et al., 2003),RASSF1A (Ras association domain family 1) in neuroendocrine tumors(Liu et al., 2005) and P15 (p15INK4b) in HCC (Wong et al., 2000) mayall be involved in suppressing metastis and influencing prognosis. Inaddition, tumor-associated genes such as p14 (p14ARF), p16(p16INK4a), p53, RB1 (Retinoblastoma 1) and WTI (Wilms tumor 1)

113Y. Cheng et al. / Experimental and Molecular Pathology 88 (2010) 112–117
are frequently methylated in HCC (Shen et al., 2002; Zhang et al.,2007). We used these as maker genes to examine promotermethylation in HCC.
The aim of the present study was to evaluate the diagnosticsignificance of CIMP status and its relation to HCC prognosis. Promotermethylation was analyzed for five tumor suppressor genes and fiveother tumor-associated genes. We defined cases as CIMP-negative(CIMP-N), CIMP-intermediate (CIMP-I, 1-3 methylated genes), andCIMP-high (CIMP-H; 4-5 methylated genes).
Methods
Patients and specimens
Tumor and corresponding non-cancer liver tissue specimenswere obtained from 60 patients with HCC. The frozen tissue sampleswere flash-frozen in liquid nitrogen immediately after surgicalresection and stored in -196 °C liquid nitrogen until analysis.Patients consisted of 49 men and 11 women, ranging in age from 33to 74 (54.36±9.12) years. HCC diagnosis was made by histologicalanalysis in all cases based mainly on H&E staining. TNM stage wasclassified according to the Edmondson–Steiner classification system(Edmondson and Steiner, 1954), and among them 48 had cirrhosis.Serologic examination indicated that 56 were hepatitis B surfaceantigen-positive or hepatitis C virus antibody (anti-HCV)-positive.Written informed consent was obtained from each patient, and thestudy protocol was approved by the local ethics committee.
Table 1Primer sequences for MSP analysis.
Gene Primer sequence (5′–3′)
SYK U# F⁎ ATTTTGTGGGTTTTGTTTR ACTTCCTTAACACACCCA
M F CGATTTCGCGGGTTTCGR AAAACGAACGCAACGC
P15 U F TGTGATGTGTTTGTATTR CCATACAATAACCAAAC
M F GCGTTCGTATTTTGCGGR CGTACAATAACCGAACG
E-cadherin U F TGGTTGTAGTTATGTATR ACACCAAATACAATCAA
M F TGTAGTTACGTATTTATR CGAATACGATCGAATCG
TIMP-3 U F TTTTGTTTTGTTATTTTTR CCCCCAAAAACCCCACC
M F CGTTTCGTTATTTTTTGTR CCGAAAACCCCGCCTCG
RASSF1A U F TTTGGTTGGAGTGTGTTR CAAACCCCACAAACTAA
M F GTGTTAACGCGTTGCGTR AACCCCGCGAACTAAAA
P16 U F TTATTAGAGGGTGGGGR CAACCCCAAACCACAAC
M F TTATTAGAGGGTGGGGR GACCCCGAACCGCGACC
P53 U F TTGGTAGGTGGATTATTR CCAATCCAAAAAAACAT
M F TTCGGTAGGCGGATTATR AAATATCCCCGAAACCC
WT1 U F TGGGATTTGGGTGGTATR CACCAACACCCACTACA
M F GTTAGGCGTCGTCGAGGR AAAACGCAAAATCCAAC
P14 U F TTTTTGGTGTTAAAGGGR CACAAAAACCCTCACTC
M F GTGTTAAAGGGCGGCGR AAAACCCTCACTCGCGA
RB1 U F GGGAGTTTTGTGGATGTR ACATCAAAACACACCCC
M F GGGAGTTTCGCGGACGR ACGTCGAAACACGCCCC
#M, methylated sequence; U, unmethylated sequence. ⁎F, forward sequence; R, reverse seq
Sodium bisulfite treatment
Non-tumor and tumor samples were digested overnight at 50 °Cwith proteinase K buffered in 1% SDS (pH=8). Genomic DNA oftumor or normal tissues was isolated by phenol–chloroform extrac-tion and ethanol precipitation. DNA was treated with sodium bisulfiteas described previously (Herman et al., 1996; Latham, 1996). Briefly,2 μg of genomic DNA was resuspended in 50 μl water and thendenatured in 2 M NaOH for 10 min at 37 °C. The denatured DNAwas diluted in 550 μl of freshly prepared solution containing 10 mMhydroquinone (Sigma-Aldrich, St. Louis, USA) and 3 M sodiumbisulfite (Sigma-Aldrich). The resultant solution was covered withmineral oil and incubated for 16 h at 50 °C. After incubation, thesamples were desalted using a Wizard DNA Clean-Up System(Promega, Madison, USA) and treated with 3 M NaOH for 5 min atroom temperature. Then 66 μl of NH4Ac and two volumes of 100%ethanol were added, and the DNA was precipitated for at least 1–2 h at −80 °C. After precipitation, the pellets were washed with70% ethanol, dried, resuspended in 20 μl of water, and stored at−20 °C.
MSP (methylation-specific PCR)
DNA methylation was determined by MSP (Herman et al., 1996;Chang et al., 2006). MSP distinguishes unmethylated alleles of agiven gene based on DNA sequence alterations after bisulfitetreatment of DNA, which converts unmethylated but not methylated
Product size (bp) References
GGTG 140 (20)AACTTC 243GAAACTTGTGGTT 154 (20)AACCAATT 148ACCGATTATTTTTAGTGGTGTT 120 (20)ATCAAACCAAATTTTAGTGGCGTC 112AACCGTGTTTTTGGTTTT 122 (21)TCATTTCGGTTTC 116
AATGTG 105 (24)AAACAAATC 93ACGATGGATTGT 151 (20)CATAACGGATCGC 150GTAATGTTT 247 (21)ATCACTTG 193AACTTG 124 (23)CCATTA 110ACCTGGTGTAGT 132 (20)ACAACAATAGC 122CGAGAT 172 (22)ATGAC 172G
uence.
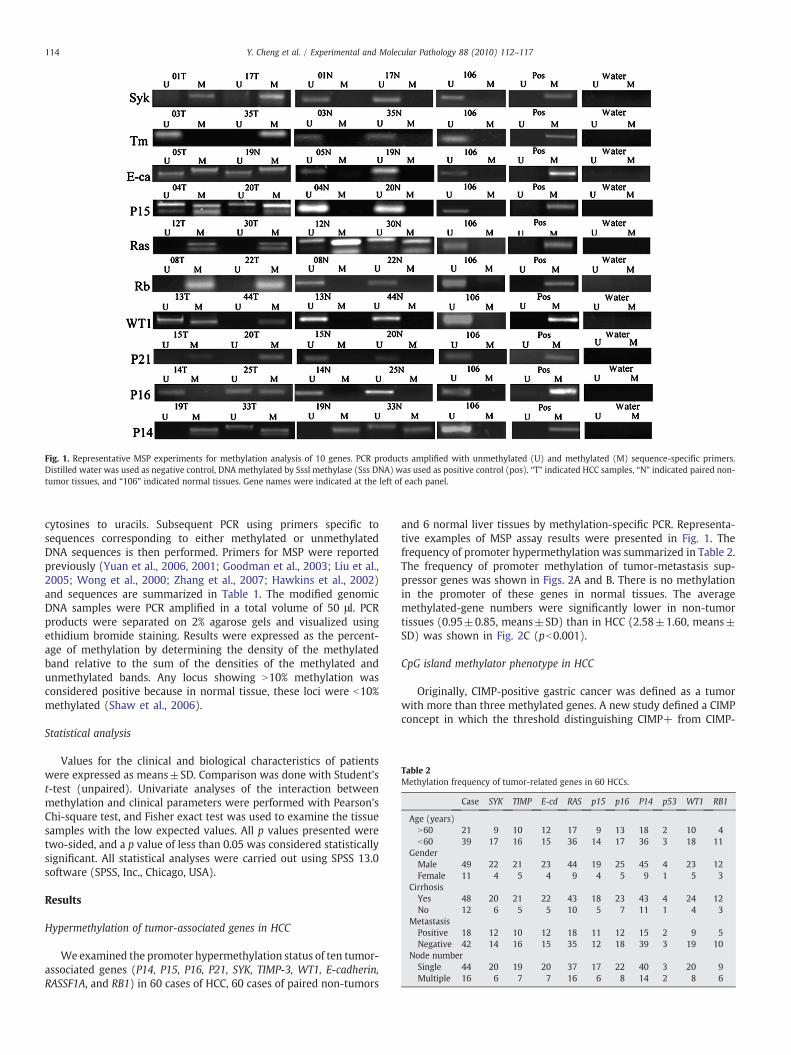
Fig. 1. Representative MSP experiments for methylation analysis of 10 genes. PCR products amplified with unmethylated (U) and methylated (M) sequence-specific primers.Distilled water was used as negative control, DNA methylated by SssI methylase (Sss DNA) was used as positive control (pos). “T” indicated HCC samples, “N” indicated paired non-tumor tissues, and “106” indicated normal tissues. Gene names were indicated at the left of each panel.
Table 2Methylation frequency of tumor-related genes in 60 HCCs.
Case SYK TIMP E-cd RAS p15 p16 P14 p53 WT1 RB1
Age (years)N60 21 9 10 12 17 9 13 18 2 10 4b60 39 17 16 15 36 14 17 36 3 18 11
GenderMale 49 22 21 23 44 19 25 45 4 23 12Female 11 4 5 4 9 4 5 9 1 5 3
CirrhosisYes 48 20 21 22 43 18 23 43 4 24 12No 12 6 5 5 10 5 7 11 1 4 3
MetastasisPositive 18 12 10 12 18 11 12 15 2 9 5Negative 42 14 16 15 35 12 18 39 3 19 10
Node numberSingle 44 20 19 20 37 17 22 40 3 20 9Multiple 16 6 7 7 16 6 8 14 2 8 6
114 Y. Cheng et al. / Experimental and Molecular Pathology 88 (2010) 112–117
cytosines to uracils. Subsequent PCR using primers specific tosequences corresponding to either methylated or unmethylatedDNA sequences is then performed. Primers for MSP were reportedpreviously (Yuan et al., 2006, 2001; Goodman et al., 2003; Liu et al.,2005; Wong et al., 2000; Zhang et al., 2007; Hawkins et al., 2002)and sequences are summarized in Table 1. The modified genomicDNA samples were PCR amplified in a total volume of 50 μl. PCRproducts were separated on 2% agarose gels and visualized usingethidium bromide staining. Results were expressed as the percent-age of methylation by determining the density of the methylatedband relative to the sum of the densities of the methylated andunmethylated bands. Any locus showing N10% methylation wasconsidered positive because in normal tissue, these loci were b10%methylated (Shaw et al., 2006).
Statistical analysis
Values for the clinical and biological characteristics of patientswere expressed as means±SD. Comparison was done with Student'st-test (unpaired). Univariate analyses of the interaction betweenmethylation and clinical parameters were performed with Pearson'sChi-square test, and Fisher exact test was used to examine the tissuesamples with the low expected values. All p values presented weretwo-sided, and a p value of less than 0.05 was considered statisticallysignificant. All statistical analyses were carried out using SPSS 13.0software (SPSS, Inc., Chicago, USA).
Results
Hypermethylation of tumor-associated genes in HCC
We examined the promoter hypermethylation status of ten tumor-associated genes (P14, P15, P16, P21, SYK, TIMP-3, WT1, E-cadherin,RASSF1A, and RB1) in 60 cases of HCC, 60 cases of paired non-tumors
and 6 normal liver tissues by methylation-specific PCR. Representa-tive examples of MSP assay results were presented in Fig. 1. Thefrequency of promoter hypermethylation was summarized in Table 2.The frequency of promoter methylation of tumor-metastasis sup-pressor genes was shown in Figs. 2A and B. There is no methylationin the promoter of these genes in normal tissues. The averagemethylated-gene numbers were significantly lower in non-tumortissues (0.95±0.85, means±SD) than in HCC (2.58±1.60, means±SD) was shown in Fig. 2C (pb0.001).
CpG island methylator phenotype in HCC
Originally, CIMP-positive gastric cancer was defined as a tumorwith more than three methylated genes. A new study defined a CIMPconcept in which the threshold distinguishing CIMP+ from CIMP-

Fig. 2. Histogram of methylated promoter genes distribution. Number of methylatedpromoter genes per sample in 60 HCC (A), 60 paired non-tumor tissues (B). Andaverage methylated gene numbers is significantly different between HCC (2.58±1.60,means±SD) and paired non-tumor tissues (0.95±0.85, means±SD, pb0.001, C).
Table 3Clinicopathologic features of CIMP-H, CIMP-I, CIMP-N in HCC.
Case (n) CIMP-H CIMP-I CIMP-N p value⁎
Age (years)N60 21 6 12 3 0.866b60 39 13 22 4
GenderMale 49 14 29 6 0.553Female 11 5 5 1
MetastasisPositive 18 10 8 0 0.030Negative 42 9 26 7
CirrhosisYes 48 14 28 6 0.693No 12 5 6 1
Node numberSingle 44 12 26 6 0.422Multiple 16 7 8 1
GGT (IU/L)b50 15 2 9 4 0.02050–100 19 4 12 3N100 26 13 13 0
AFP (ug/L)b20 15 2 10 3 0.33420–400 24 8 13 3N400 21 9 11 1
TNM stageI 4 0 2 2 0.001II 31 4 23 4III 17 11 5 1IV 8 4 4 0
HepatosisHBV 41 13 23 5 0.839HCV+HBV 15 5 9 1
⁎ Statistical significance determined using the Pearson's Chi-square test and Fisherexact test.
115Y. Cheng et al. / Experimental and Molecular Pathology 88 (2010) 112–117
samples was determined by minimizing the sum of squared errorswithin the group (Weisenberger et al., 2006).
In this study, CIMP statuswas classified as CIMP-H samples (four tofive methylated genes), CIMP-I samples (one to three methylatedgenes) and CIMP-N samples (no methylated genes). We found thesetumor suppressor genes were frequently methylated in metastaticHCC. There was no methylation in normal tissues. Thus we classifiedtumors as CIMP-H (31.7%, n=19), CIMP-I (56.7%, n=34), and CIMP-N (11.6%, n=7) as shown in Fig. 3. We next investigated the numberof other tumor-associated methylated genes compared with that of
Fig. 3. Summary of methylation of SYK, TIMP-3, E-cadherin, P15, RASSAF1A in 60 HCC. Filleunmethylation; CIMP is defined by the number of CpG islandsmethylated in each sample as foCIMP-N (zero methylated genes).
five marker genes. We found that CIMP-H HCC showed a significantlyhigher number of methylated genes (4.0±0.9) than CIMP-I (1.7±1.1,pb0.05) and CIMP-N (0.7±0.8; pb0.01). In addition, the number ofmethylated genes in CIMP-I HCC was significantly higher than that inCIMP-N HCC.
Clinicopathologic features of CIMP
The clinicopathologic features were compared among CIMP-H,CIMP-I and CIMP-N (Table 3). We found that clinicopathologicfeatures of CIMP-H, CIMP-I and CIMP-N were significantly differentin HCC with metastasis (p=0.030), GGT (p=0.020) and TNM stage(p=0.001). There was no difference among CIMP status in age,gender, cirrhosis, node-number, AFP and hepatosis.
Prognostic significance of CIMP in HCC
The prognostic roles of CIMP status has been evaluated in othertumor types. For example, CIMP was associated with poor prognosisin esophageal adenocarcinoma (Eads et al., 2001). We determinedwhether CIMP status had prognostic value in HCC (Fig. 4). Survivalrates were significantly different between CIMP-H, CIMP-I and CIMP-N (p=0.0146). Prognosis was worse in CIMP-H tumors were than
d boxes indicated the presence of methylation; open boxes indicated the presence ofllows: CIMP-H (four to fivemethylated genes); CIMP-I (one to threemethylated genes),

Fig. 4. Overall survival of 60 HCC patients grouped according to CIMP-N (top), CIMP-I(middle), and CIMP-H (bottom). Actuarial probabilities were calculated by the Kaplan–Meier method and compared with the log-rank test. After resection of primary tumors,patients with different CIMP status in primary tumors was different in survival rate(p=0.0146). Patients with CIMP-H in primary tumors had a worse overall survival ratethan those with CIMP-N (pb0.01) and CIMP-I (pb0.05).
116 Y. Cheng et al. / Experimental and Molecular Pathology 88 (2010) 112–117
CIMP-N (pb0.05) and CIMP-I tumors (pb0.01), but there was nosignificant difference between CIMP-I and CIMP-N. Therefore, CIMP-positive tumor indicates a poor prognosis in HCC.
Discussion
HCC ranks as the fifth most common cancer in the world. Thedevelopment and progression of HCC is a multiple step process andthe understanding of the molecular pathways underlying hepatocar-cinogenesis is limited. Genetic changes can be used as cancer markers.Several reports have suggested that epigenetics may play animportant role in cancer development, especially aberrant methyla-tion of CpG islands in HCC (Oue et al., 2006; Shen et al., 2007; Kondohet al., 2001). We examined the promoter methylation status of tentumor-associated genes selected on the basis of biological significancein HCC. The frequency of promoter methylation varied from 20% forP21 and 90% for P14. We also examined the CD44, P27, NM23, PTENand GSTP1 promoter methylation in HCC and non-parried tumors, butthere was no significant difference in clinicopathologic features ormethylation in HCC (data not shows). Our currentwork demonstratedthat methylation changes could be used to clarify the exposures thatcontributed to the development of HCC and prognosis. Metastasis-epigenetic interaction studies may be necessary for understandingcarcinogenesis mechanisms and could be used to identify novelopportunities for cancer prevention and treatment.
The recently described hypermethylator phenotype in colorectalcancer, termed CIMP, affects about half of all cases (Toyota et al.,1999). The term CIMP has been used for a subset of tumors withpromoter methylation in multiple genes including colorectal, pancre-as, esophagus and stomach, among others (Toyota et al., 1999a,b; Eadset al., 2001; Kondoh et al., 2001; Yamashita et al., 2003; Nosho et al.,2008). In colorectal cancer, CIMP-positive phenotype is associatedwith distinct clinicopathologic features like tumor location, femalesex, and age (Yamashita et al., 2003). The prognostic roles of CIMPstatus have been evaluated in several types of cancers, such asesophageal adenocarcinoma, where CIMP is associated with poorprognosis (Eads et al., 2001). Meanwhile, the concept of CIMP recentlyhas been challenged (Kondoh et al., 2001), but the evaluation of alarge, population-based sample strongly supports the biologicrelevance of CIMP in colon cancer (Samowitz et al., 2005). CpG islandmethylator phenotype associated with environment and elevatedserum Alpha fetoprotein level in HCC has been discovered (Shen et al.,2002; Zhang et al., 2007).
However the prognostic role of CIMP status in HCC is unclear andthere is little information about the prognostic significance ofconcordant gene methylation. In this study we showed CIMPassociations with HCC metastasis, suggesting a major role for CIMPin the pathogenesis of metastatic HCC. Possibly, hypermethylatedtumor suppressor-metastasis genes become silenced, which maysubsequently enhance HCC invasiveness and worsen prognosis. Wealso discovered differential methylation in HCC, paired non-tumorsand six normal tissues, suggesting the importance of methylation incancer development.
The main focus of this study was to identify accurate prognosticbiomarkers for HCC patients after hepatectomy. Several clinicopath-ological features andmolecularmarkers, with varied predictive powerhave been linked to HCC prognosis. These include clinical features(tumor size, tumor number and vascular invasion, underlying livercirrhosis, Child-Pugh classification, and tumor microvessel density)(Yamamoto et al., 2004; Bilimoria et al., 2001; Vauthey et al., 2002;Poon et al., 2002) and molecular markers (P27 expression andP53mutation) (Fiorentino et al., 2000; Honda et al., 1998). It has beenreported that P16 promoter methylation frequencies in HCC may varysignificantly among different geographic locations (e.g., 34.4% inChinese populations, 12.2% in Egyptians) (Shen et al., 2002).
The functional significance of tumor-associated gene methylationcould be an initiating event leading to progressive inactivation in HCCcells. We hope that a better understanding of CIMP molecular eventsand prognosis will ultimately improve our ability to use demethyla-tion drugs to treat HCC. Further study is necessary to clarify the linkbetween prognosis and tumor-associated gene methylation inhepatocarcinogenesis. Additional studies are necessary to clarify thedetailed clinicopathological features of tumors with andwithout CIMPusing a large number of cases and more tumor suppressor genesmoving forward, global identification of novel hypermethylated genesin HCC will be critical.
Conflict of interest statementThe authors declare that there are no conflicts of interest.
Acknowledgments
This project was supported by the Special Funds for NationalNatural Science Foundation of China (30700981, 30801347,30870974, 30901722), the Commission of Science and Technologyof Shanghai Municipality (045407047, 08XD14003), National key Sci-Tech Sepcial Project of China (2008ZX10002-019, 2008ZX10002-025),Key Cancer project of CAS (KSCX1-YW-22), Key Basic Research Project(2010CB945600), and Science Fund for Creative Research Groups(30921006).
References
Baylin, S.B., Herman, J.G., Graff, J.R., Vertino, P.M., Issa, J.P., 1998. AlterationsIn DNAmethylation: a fundamental aspect of neoplasia. Adv. Cancer Res. 72, 141–196.
Bilimoria, M.M., Lauwers, G.Y., Doherty, D.A., Nagorney, D.M., Belghiti, J., Do, K.A.,Regimbeau, J.M., Ellis, L.M., Curley, S.A., Ikai, I., Yamaoka, Y., Vauthey, J.N.,International Cooperative Study Group on Hepatocellular Carcinoma, 2001.Underlying liver disease, not tumor factors, predicts long-term survival afterresection of hepatocellular carcinoma. Arch. Surg. 136, 528–535.
Chang, M.S., Uozaki, H., Chong, J.M., Ushiku, T., Sakuma, K., Ishikawa, S., Hino, R., Barua,R.R., Iwasaki, Y., Arai, K., Fujii, H., Nagai, H., Fukayama, M., 2006. CpG islandmethylation status in gastric carcinoma with and without infection of Epstein-Barrvirus. Clin. Cancer Res. 12 (10), 2995–3002.
Costello, J.F., Frühwald, M.C., Smiraglia, D.J., Rush, L.J., Robertson, G.P., Gao, X., Wright, F.A., Feramisco, J.D., Peltomäki, P., Lang, J.C., Schuller, D.E., Yu, L., Bloomfield, C.D.,Caligiuri, M.A., Yates, A., Nishikawa, R., Su Huang, H., Petrelli, N.J., Zhang, X.,O'Dorisio, M.S., Held, W.A., Cavenee, W.K., Plass, C., 2000. Aberrant CpG-islandmethylation has non-random and tumour-type-specific patterns. Nat. Genet. 24,132–138.
Darnton, S.J., Hardie, L.J., Muc, R.S., Wild, C.P., Casson, A.G., 2005. Tissue inhibitor ofmetalloproteinase-3 (TIMP-3) gene is methylated in the development ofesophageal adenocarcinoma: loss of expression correlates with poor prognosis.Int. J. Cancer 115, 351–358.
117Y. Cheng et al. / Experimental and Molecular Pathology 88 (2010) 112–117
Eads, C.A., Lord, R.V., Wickramasinghe, K., Long, T.I., Kurumboor, S.K., Bernstein, L.,Peters, J.H., DeMeester, S.R., DeMeester, T.R., Skinner, K.A., Laird, P.W., 2001.Epigenetic patterns in the progression of esophageal adenocarcinoma. Cancer Res.61, 3410–3418.
Edmondson, H.A., Steiner, P.E., 1954. Primary carcinoma of the liver: a study of 100cases among 48,900 necropsies. Cancer 7, 462–503.
El-Serag, H.B., 2002. Hepatocellular carcinoma: an epidemiologic view. J. Clin.Gastroenterol. 35, S72–S78.
Fiorentino, M., Altimari, A., D'Errico, A., Cukor, B., Barozzi, C., Loda, M., Grigioni, W.F.,2000. Acquired expression of p27 is a favorable prognostic indicator in patientswith hepatocellular carcinoma. Clin. Cancer Res. 6, 3966–3972.
Goodman, P.A., Burkhardt, N., Juran, B., Tibbles, H.E., Uckun, F.M., 2003. Hypermethyla-tion of the spleen tyrosine kinase promoter in T-lineage acute lymphoblasticleukemia. Oncogene 22, 2504–2514.
Graziano, F., Arduini, F., Ruzzo, A., Bearzi, I., Humar, B., More, H., Silva, R., Muretto, P.,Guilford, P., Testa, E., Mari, D., Magnani, M., Cascinu, S., 2004. Prognostic analysis ofE-cadherin gene promoter hypermethylation inpatients with surgically resected,node-positive, diffuse gastric cancer. Clin. Cancer Res. 10, 2784–2789.
Hawkins, N., Norrie, M., Cheong, K., Mokany, E., Ku, S.L., Meagher, A., O'Connor, T., Ward,R., 2002. CpG island methylation in sporadic colorectal cancers and its relationshipto microsatellite instability. Gastroenterology 122 (1), 376–387.
Herman, J.G., Baylin, S.B., 2003. Gene silencing in cancer in association with promoterhypermethylation. N. Engl. J. Med. 349, 2042–2054.
Herman, J.G., Graff, J.R., Myöhänen, S., Nelkin, B.D., Baylin, S.B., 1996. Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proc. Natl.Acad. Sci. U. S. A. 93, 9821–9826.
Honda, K., Sbisà, E., Tullo, A., Papeo, P.A., Saccone, C., Poole, S., Pignatelli, M., Mitry, R.R.,Ding, S., Isla, A., Davies, A., Habib, N.A., 1998. p53 mutation is a poor prognosticindicator for survival in patients with hepatocellular carcinoma undergoingsurgical tumour ablation. Br. J. Cancer 77, 776–782.
Jones, P.A., Baylin, S.B., 2002. The fundamental role of epigenetic events in cancer.Nat. Rev. Genet. 3, 415–428.
Jones, P.L., Wolffe, A.P., 1999. Relationships between chromatin organization and DNAmethylation in determining gene expression. Semin. Cancer Biol. 9, 339–347.
Kondoh, N., Wakatsuki, T., Hada, A., Shuda, M., Tanaka, K., Arai, M., Yamamoto, M., 2001.Genetic and epigenetic events in human hepatocarcinogenesis. Int. J. Oncol. 18,1271–1278.
Kwong, J., Lo, K.W., To, K.F., Teo, P.M., Johnson, P.J., Huang, D.P., 2002. Promoter hyper-methylationofmultiplegenes innasopharyngeal carcinoma.Clin. CancerRes. 8, 131–137.
Lai, E.C., Fan, S.T., Lo, C.M., Chu, K.M., Liu, C.L., Wong, J., 1995. Hepatic resection forhepatocellular carcinoma. An audit of 343 patients. Ann. Surg. 221, 291–298.
Laird, P.W., 2003. The power and the promise of DNA methylation markers. Nat. Rev.Cancer 3, 253–266.
Latham, K.E.X., 1996. Chromosome imprinting and inactivation in the early mammalianembryo. Trends Genet. 12, 134–138.
Lee, S., Lee, H.J., Kim, J.H., Lee, H.S., Jang, J.J., Kang, G.H., 2003. Aberrant CpG island hyper-methylation along multistep hepatocarcinogenesis. Am. J. Pathol. 163, 1371–1378.
Liu, L., Broaddus, R.R., Yao, J.C., Xie, S., White, J.A., Wu, T.T., Hamilton, S.R., Rashid, A.,2005. Epigenetic alterations in neuroendocrine tumors: methylation of RAS-association domain family 1, isoform A and p16 genes are associated withmetastasis. Mod. Pathol. 18 (12), 1632–1640.
Melki, J.R., Vincent, P.C., Clark, S.J., 1999. Concurrent DNA hypermethylation of multiplegenes in acute myeloid leukemia. Cancer Res. 59, 3730–3740.
Nosho, K., Yamamoto, H., Takahashi, T., Mikami, M., Hizaki, K., Maehata, T., Taniguchi,H., Yamaoka, S., Adachi, Y., Itoh, F., Imai, K., Shinomura, Y., 2008. Correlation oflaterally spreading type and JC virus with methylator phenotype status incolorectal adenoma. Hum. Pathol. 39 (5), 767–775.
Oue, N., Mitani, Y., Motoshita, J., Matsumura, S., Yoshida, K., Kuniyasu, H., Nakayama, H.,Yasui, W., 2006. Accumulation of DNA methylation is associated with tumor stagein gastric cancer. Cancer 106, 1250–1259.
Poon, R.T., Ng, I.O., Lau, C., Yu, W.C., Yang, Z.F., Fan, S.T., Wong, J., 2002. Tumormicrovessel density as a predictor of recurrence after resection of hepatocellularcarcinoma: a prospective study. J. Clin. Oncol. 20, 1775–1785.
Samowitz, W.S., Albertsen, H., Herrick, J., Levin, T.R., Sweeney, C., Murtaugh, M.A.,Wolff, R.K., Slattery, M.L., 2005. Evaluation of a large, population-based sample
supports a CpG island methylator phenotype in colon cancer. Gastroenterology129, 837–845.
Segditsas, S., Sieber, O.M., Rowan, A., Setien, F., Neale, K., Phillips, R.K., Ward, R., Esteller,M., Tomlinson, I.P., 2008. Promoter hypermethylation leads to decreased APCmRNA expression in familial polyposis and sporadic colorectal tumours, but doesnot substitute for truncating mutations. Exp. Mol. Pathol. 85 (3), 201–206.
Shaw, R.J., Akufo-Tetteh, E.K., Risk JM Field, J.K., Liloglou, T., 2006. Methylationenrichment pyrosequencing: combining the specificity of MSP with validation bypyrosequencing. Nucleic. Acids Res. 34 (11), 78 28.
Shen, L., Ahuja, N., Shen, Y., Habib, N.A., Toyota, M., Rashid, A., Issa, J.P., 2002. DNAmethylation and environmental exposures in human hepatocellular carcinoma.J. Natl. Cancer Inst. 94, 755–761.
Shen, L., Toyota, M., Kondo, Y., Lin, E., Zhang, L., Guo, Y., Hernandez, N.S., Chen, X.,Ahmed, S., Konishi, K., Hamilton, S.R., Issa, J.P., 2007. Integrated genetic andepigenetic analysis identifies three different subclasses of colon cancer. Proc. Natl.Acad. Sci. U. S. A. 20;104(47), 18654–18659.
Tanemura, A., Terando, A.M., Sim, M.S., van Hoesel, A.Q., de Maat, M.F., Morton, D.L.,Hoon, D.S., 2009. CpG island methylator phenotype predicts progression ofmalignant melanoma. Clin Cancer Res. 15 (5), 1801–1807.
Toyota, M., Ahuja, N., Ohe-Toyota, M., Herman, J.G., Baylin, S.B., Issa, J.P., 1999a. CpGisland methylator phenotype in colorectal cancer. Proc. Natl. Acad. Sci. U. S. A. 96,8681–8686.
Toyota, M., Ahuja, N., Suzuki, H., Itoh, F., Ohe-Toyota, M., Imai, K., Baylin, S.B., Issa, J.P.,1999b. Aberrant methylation in gastric cancer associated with the CpG islandmethylator phenotype. Cancer Res. 59, 5438–5442.
Vauthey, J.N., Klimstra, D., Franceschi, D., Tao, Y., Fortner, J., Blumgart, L., Brennan, M.,1995. Factors affecting long-term outcome after hepatic resection for hepatocel-lular carcinoma. Am. J. Surg. 169, 28–34.
Vauthey, J.N., Lauwers, G.Y., Esnaola, N.F., Do, K.A., Belghiti, J., Mirza, N., Curley, S.A.,Ellis, L.M., Regimbeau, J.M., Rashid, A., Cleary, K.R., Nagorney, D.M., 2002. Simplifiedstaging for hepatocellular carcinoma. J. Clin. Oncol. 20, 1527–1536.
Weisenberger, D.J., Siegmund, K.D., Campan, M., Young, J., Long, T.I., Faasse, M.A., Kang,G.H., Widschwendter, M., Weener, D., Buchanan, D., Koh, H., Simms, L., Barker, M.,Leggett, B., Levine, J., Kim, M., French, A.J., Thibodeau, S.N., Jass, J., Haile, R., Laird,P.W., 2006. CpG island methylator phenotype underlies sporadic microsatelliteinstability and is tightly associated with BRAF mutation in colorectal cancer.Nat. Genet. 38, 787–793.
Wong, I.H., Lo, Y.M., Yeo, W., Lau, W.Y., Johnson, P.J., 2000. Frequent p15 promotermethylation in tumor and peripheral blood from hepatocellular carcinomapatients. Clin. Cancer Res. 6 (9), 3516–3521.
Yamamoto, M., Takasaki, K., Otsubo, T., Katsuragawa, H., Katagiri, S., Yoshitoshi, K.,Ariizumi, S., Saito, A., Nakano, M., 2004. Favorable surgical outcomes in patientswith early hepatocellular carcinoma. Ann. Surg. 239, 395–399.
Yamashita, K., Dai, T., Dai, Y., Yamamoto, F., Perucho, M., 2003. Genetics supersedesepigenetics in colon cancer phenotype. Cancer Cell 4, 121–131.
Yeo, W., Mok, T.S., 2005. A randomized phase III study of doxorubicin versus cisplatin/interferon alpha-2b/doxorubicin/fluorouracil (PIAF) combination chemotherapyfor unresectable hepatocellular carcinoma. J. Natl. Cancer Inst. 97, 1532–1538.
Yoo, H.Y., Patt, C.H., Geschwind, J.F., Thuluvath, P.J., 2003. The outcome of livertransplantation in patients with hepatocellular carcinoma in the United Statesbetween 1988 and 2001: 5-year survival has improved significantly with time.J. Clin. Oncol. 21, 4329–4335.
Yuan, Y., Mendez, R., Sahin, A., Dai, J.L., 2001. Hypermethylation leads to silencing of theSYK gene in human breast cancer. Cancer Res. 61, 5558–5561.
Yuan, Y., Wang, J., Li, J., Wang, L., Li, M., Yang, Z., Zhang, C., Dai, J.L., 2006. Frequentepigenetic inactivation of spleen tyrosine kinase gene in human hepatocellularcarcinoma. Clin. Cancer Res. 12 (22), 6687–6695.
Yu, J., Zhang, H.Y., Ma, Z.Z., Lu, W., Wang, Y.F., Zhu, J.D., 2003. Methylation profiling oftwenty four genes and the concordant methylation behaviors of nineteen genesthat may contribute to hepatocellular carcinogenesis. Methylation profiling oftwenty four genes and the concordant methylation behaviors of nineteen genesthat may contribute to hepatocellular carcinogenesis. Cell Res. 13, 319–333.
Zhang, C., Li, Z., Cheng, Y., Jia, F., Li, R., Wu, M., Li, K., Wei, L., 2007. CpG islandmethylatorphenotype association with elevated serum alpha-fetoprotein level in hepatocel-lular carcinoma. Clin. Cancer Res. 13 (3), 944–952.