core temperature monitoring: essential for an optimized ... · core temperature monitoring:...
TRANSCRIPT

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Core temperature monitoring: essential for an optimized
perioperative care
Egil Lingaas
Department of Infection Prevention
Oslo University Hospital
Oslo, Norway
SEORNA, Stockholm, November 26th 2015

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Background
Surgical patients are at risk of developing
hypothermia at any stage of the
perioperative pathway.
Inadvertent perioperative hypothermia is a
common but preventable complication,
which is associated with poor outcomes for
patients.

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
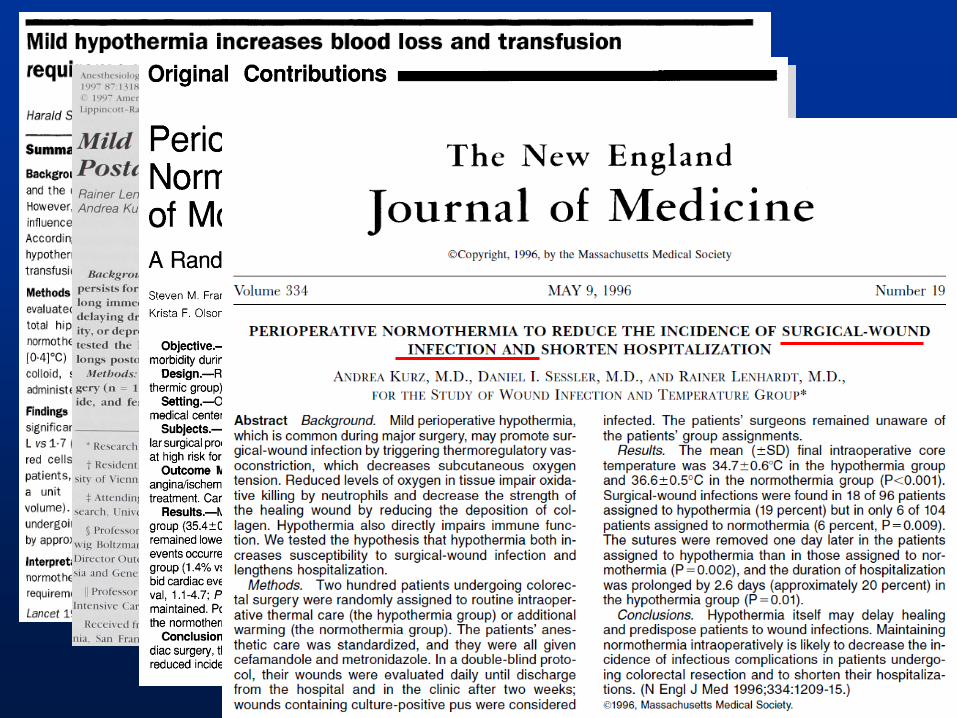
Adverse outcomes of perioperative hypothermia
Morbid myocardial outcomes
Surgical site infection
Coagulopathy
Increased allgogeneic transfusions
Negative nitrogen balance
Delayed wound healing
Delayed postanesthetic recovery
Prolonged hospitalisation
Shivering
Patient discomfort

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Inadvertent perioperative
hypothermia Implementing NICE guidance
2008
NICE clinical guideline 65
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Patients at higher risk of perioperative
hypothermia
Any two of the following:
ASA grade II to V
preoperative temperature below 36.0°C
undergoing combined general and regional
anaesthesia
undergoing major or intermediate surgery
at risk of cardiovascular complications.
NICE

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Definition of hypothermia
• Hypothermia: a patient core temperature
of below 36,0°C
• Preoperative: 1 hour before induction of
anaesthesia
• Intraoperative: the total anaesthesia time
• Postoperative: 24 hours after entry into
the recovery area in the theatre suite
NICE
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Each patient should be assessed for their risk of inadvertent perioperative hypothermia and potential adverse consequences before transfer to the theatre suite. = measurement of temperature
Preoperative phase
NICE

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Preoperative warming
forced air warming should be started
preoperatively on the ward or in the emergency
department (unless there is a need to expedite
surgery because of clinical urgency)
Forced air warming should be maintained
throughout the intraoperative phase
If the patient’s temperature is below 36.0°C
in the hour before they leave the ward
or emergency department
NICE
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
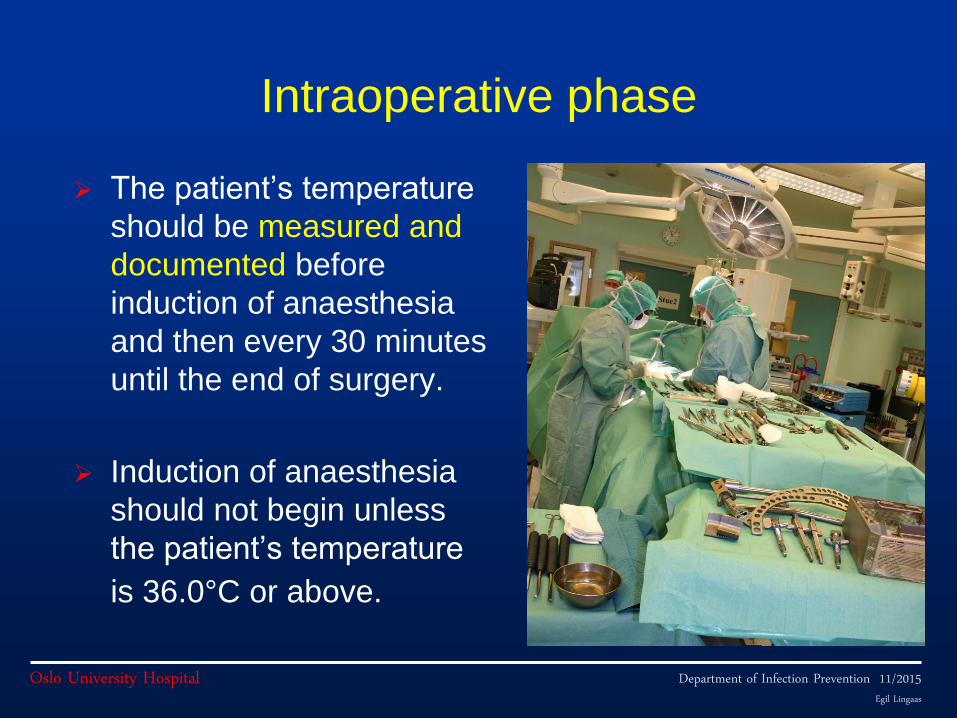
Intraoperative phase
The patient’s temperature
should be measured and
documented before
induction of anaesthesia
and then every 30 minutes
until the end of surgery.
Induction of anaesthesia
should not begin unless
the patient’s temperature
is 36.0°C or above.
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Postoperative phase
The patient’s temperature should be measured
and documented on admission to the recovery
room and then every 15 minutes
Ward transfer should not be arranged unless the
patient’s temperature is 36.0°C or above
If the patient’s temperature is below 36.0°C, they
should be actively warmed using forced air warming
until they are discharged from the recovery room or
until they are comfortably warm. NICE
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Arkilic CF et al. Anesth Analg 2009;91:662
Why don’t just ask the anesthesiologist?
In fact, someone did ….

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Arkilic CF et al. Anesth Analg 2009;91:662
Are anaesthesiologists able to estimate patient thermal status?
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Torossian A. Eur J Anaestesiol 2007;24:668
October 13th 2004:
8081 patients in 316 hospitals in 16 European
countries
Temperature was monitored in 19.4 % of patients
Active warming was used for 38.5 % of patients
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
So, where to measure ….?
And with what technology….?
Methods for temperature measurement
Expansion
–Mercury, alcohol etc.
Liquid crystal
Infrared sensor
Electronic
–Thermistor
–Thermocouple
Heat flux (without active thermoelement)
Zero heat flux (with active thermoelement
Non-invasive methods (skin) Axilla
Usually 1-2 oC lower than actual core
temperature
Measurement errors frequent
Slow
Forehead
1. Liquid crystal - thermochrome substance
changing colour according to the temperature
Not accurate enough
2. Thermistors and thermocouples
About 2 o C must be added, but still a rather
inaccurate estimate of core temperature

Non-invasive methods (skin, contd)
Temporal artery
Inaccuracy caused by environmental
temperature and sweating
Generally not recommended for clinical
needs
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
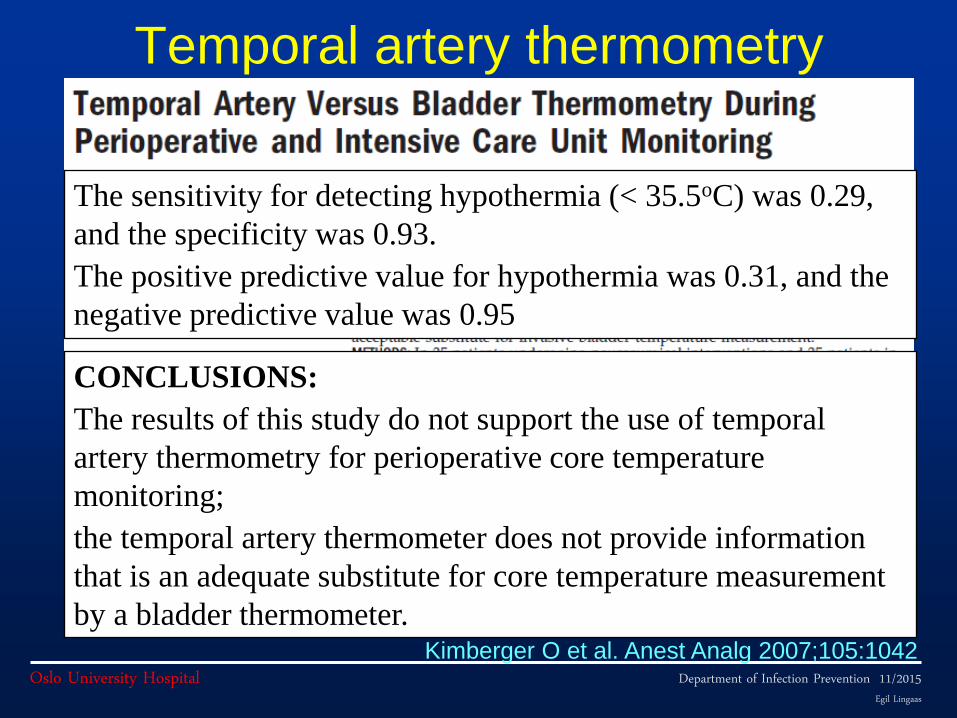
Temporal artery thermometry
Kimberger O et al. Anest Analg 2007;105:1042
The sensitivity for detecting hypothermia (< 35.5oC) was 0.29,
and the specificity was 0.93.
The positive predictive value for hypothermia was 0.31, and the
negative predictive value was 0.95
CONCLUSIONS:
The results of this study do not support the use of temporal
artery thermometry for perioperative core temperature
monitoring;
the temporal artery thermometer does not provide information
that is an adequate substitute for core temperature measurement
by a bladder thermometer.
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
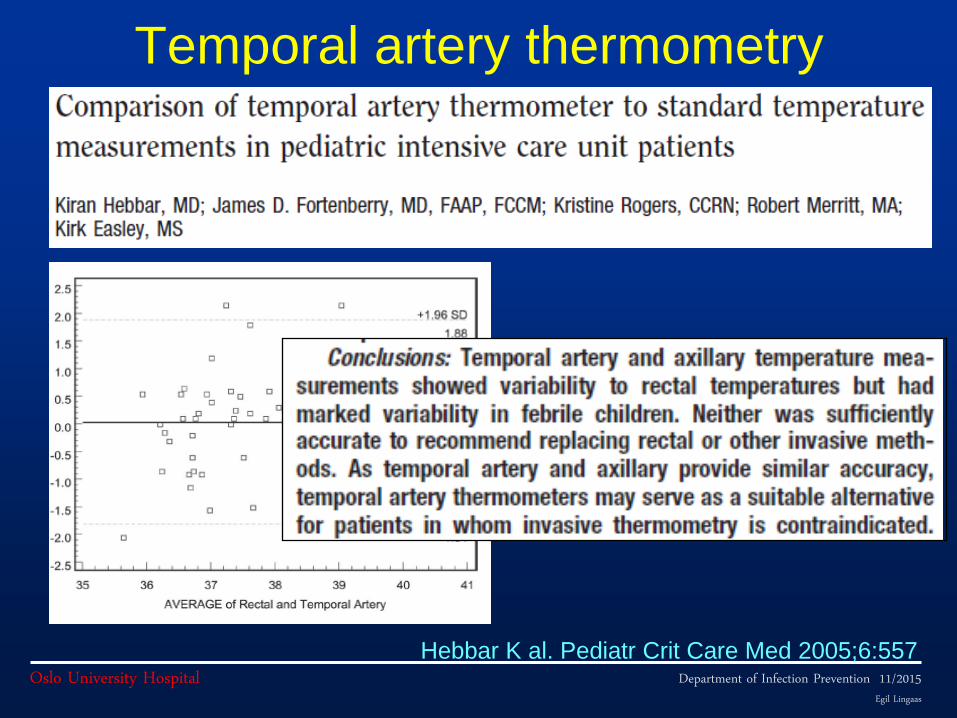
Temporal artery thermometry
Hebbar K al. Pediatr Crit Care Med 2005;6:557
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Minimally invasive methods Oral
Dependent on patient compliance
Not very reliable
influenced by previous food intake, mucosal inflammation, air circulation in mouth
Continuous measurement not feasible
Tympanic 1. Infrared/indirect
Very inaccurate and artifact-prone (position cerumen etc.
2. Direct
Uncomfortable for patient
Risk of tympanic perforation

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Infrared aural canal thermometers
Imamura M et al. Acta Anaesthesiol Scand 1998;42:1222
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Infrared aural canal thermometers
Imamura M et al. Acta Anaesthesiol Scand 1998;42:1222

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Infrared aural canal thermometers
Imamura M et al. Acta Anaesthesiol Scand 1998;42:1222
Conclusion: We conclude that none of the tested aural canal
infrared thermometers was sufficiently accurate and precise for
perioperative use

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Minimally invasive methods (contd)
Rectal Better than other minimally invasive methods
High temporal latency depending on the filling of
the ampulla recti, with delays up to 1 h.
Still less accurate than aesophageal and bladder
temperature measurement

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Most non-invasive methods are
unpresise
Temperature Measurement
Core Sites
–Pulmonary artery
–Distal esophagus
–Nasopharynx
–Tympanic membrane by thermocouple
Other generally-reliable sites
–Bladder
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
All “core sites” are more or less
invasive
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Invasive methods for core temperature
measurement
Nasopharyngeal Option primarily for the anaesthezised ventilated
patient
Offers adequate accuracy (1)
Uncomfortable in non-anaesthezied patients
Not suitable for pre-operative measurement
(1) Maxton FL et al. J Adv Nurs 2004;45:214
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Invasive methods for core temperature
measurement (contd.)
Esophageal High accuracy
Easy to attach to patient
Not very prone to artifacts
Rather uncomfortable for the anaesthezised
ventilated patient
Not suitable for pre-operative measurement
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Invasive methods for core temperature
measurement (contd.)
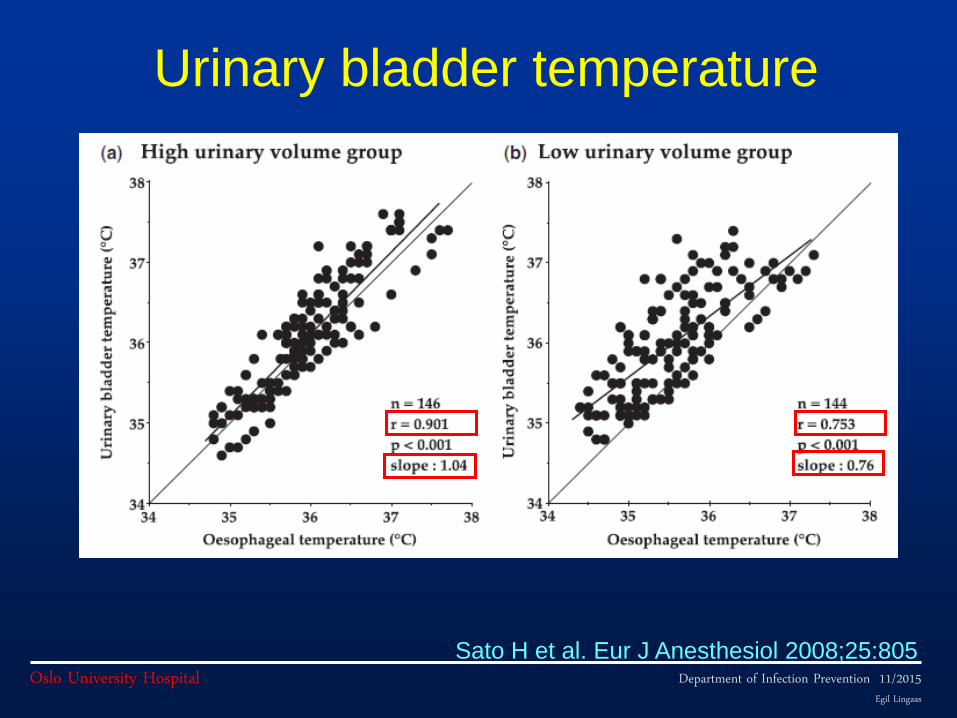
Bladder temperature High accuracy, but may produce false values with
low urine output
Low risk of dislocation
Not suitable for pre-operative measurement
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Sato H et al. Eur J Anesthesiol 2008;25:805
Urinary bladder temperature
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Sato H et al. Eur J Anesthesiol 2008;25:805
Urinary bladder temperature
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
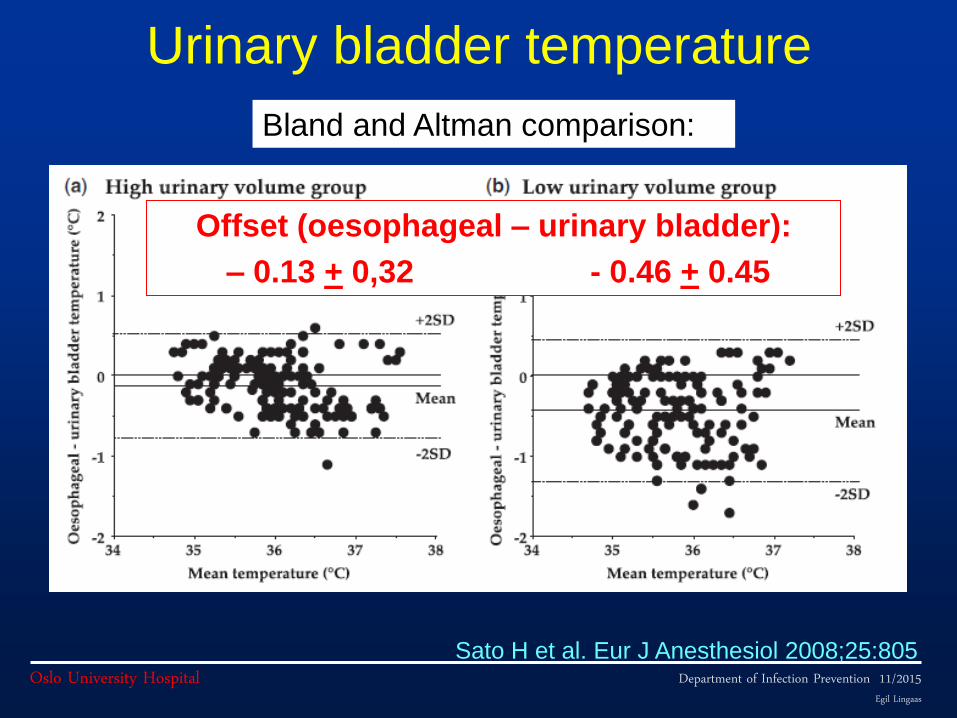
Urinary bladder temperature
Sato H et al. Eur J Anesthesiol 2008;25:805
Offset (oesophageal – urinary bladder):
– 0.13 + 0,32 - 0.46 + 0.45
Bland and Altman comparison:
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
The gold standard core temperature
The temperature measured next to the
heart (e.g. pulmonary artery)
Brain temperature
Both methods are extremely invasive

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
Non-invasive measurement of
core temperature
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
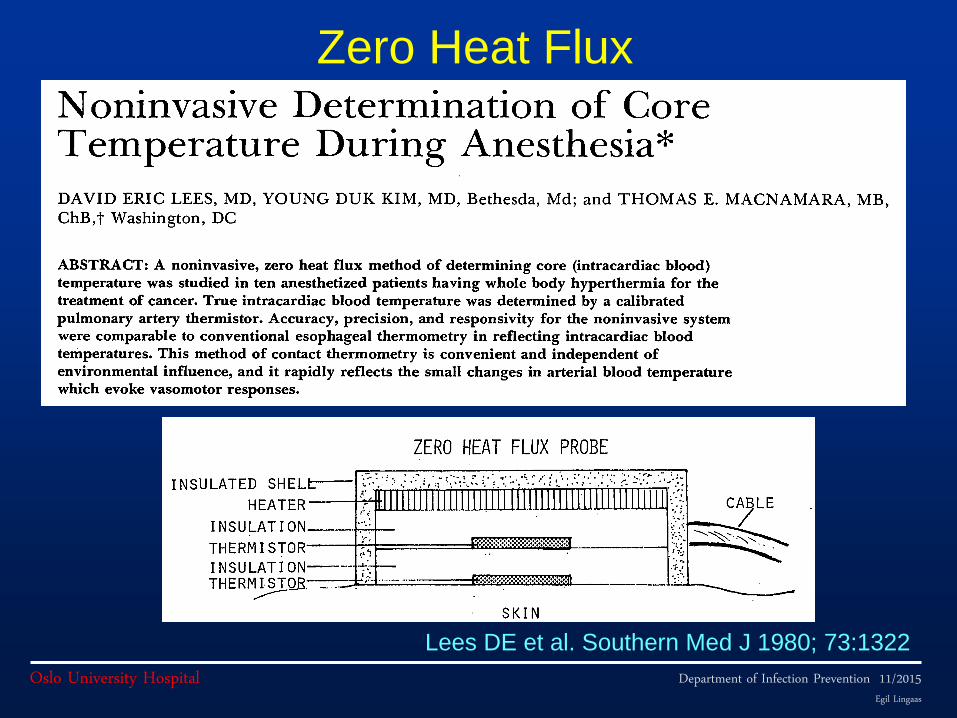
Zero Heat Flux
Based on thermic isolation of an area of the skin
and an actively warming thermoelement
that is heated until there is no more heat transfer
between the patient and the environment.
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Lees DE et al. Southern Med J 1980; 73:1322
Zero Heat Flux
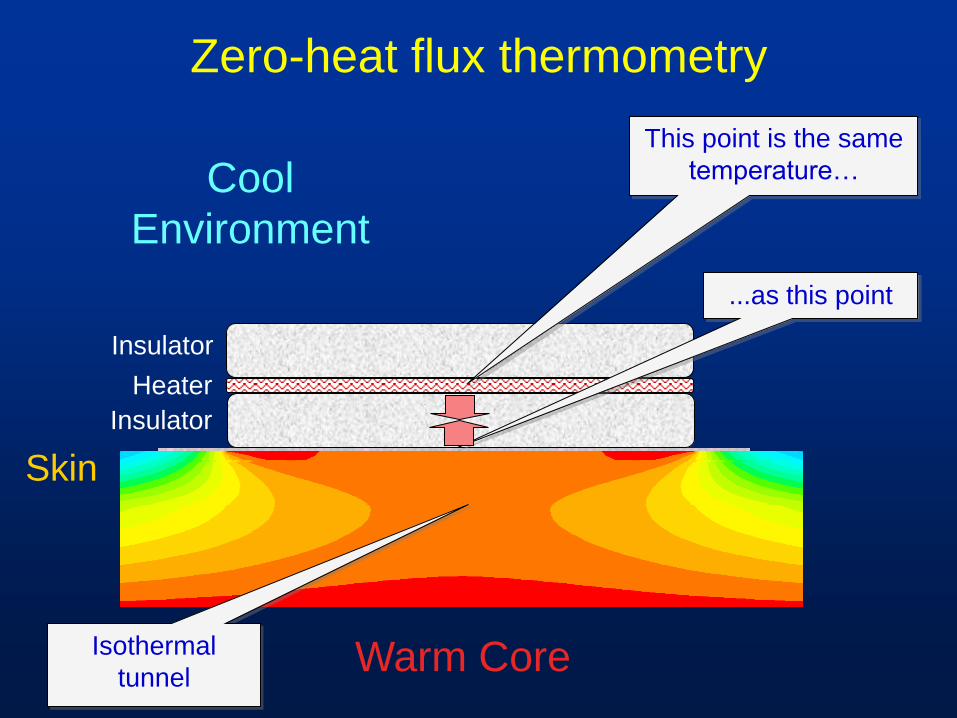
Zero-heat flux thermometry
Warm Core
Cool
Environment
Heater
This point is the same
temperature…
...as this point
Skin
Insulator
Insulator
Isothermal
tunnel
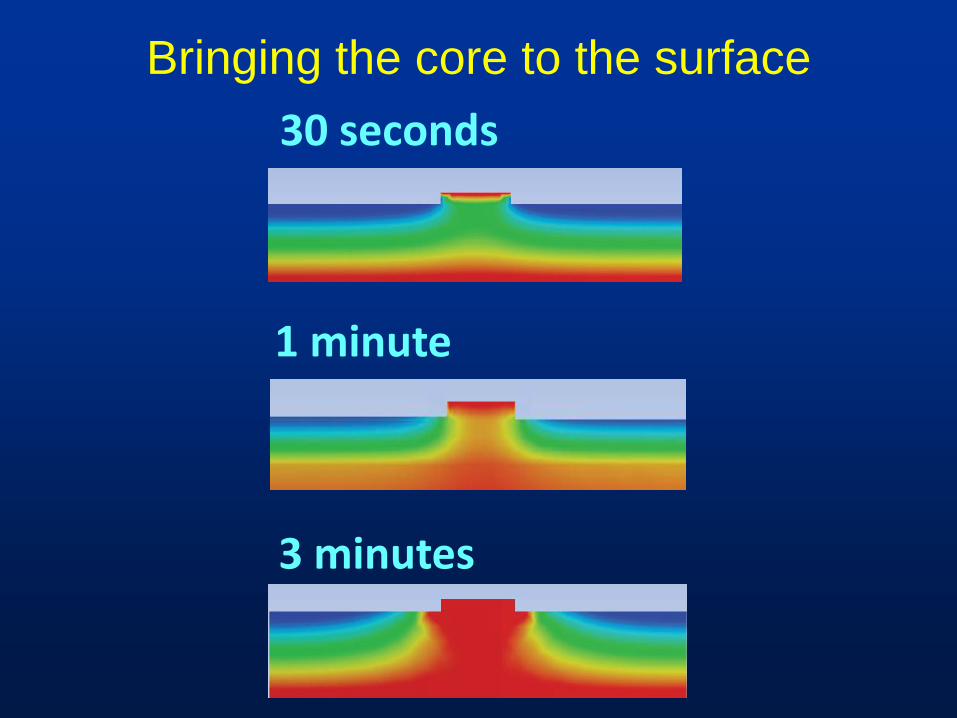
Bringing the core to the surface
30 seconds
3 minutes
1 minute
Department of Infection Prevention 11/2015 Egil Lingaas
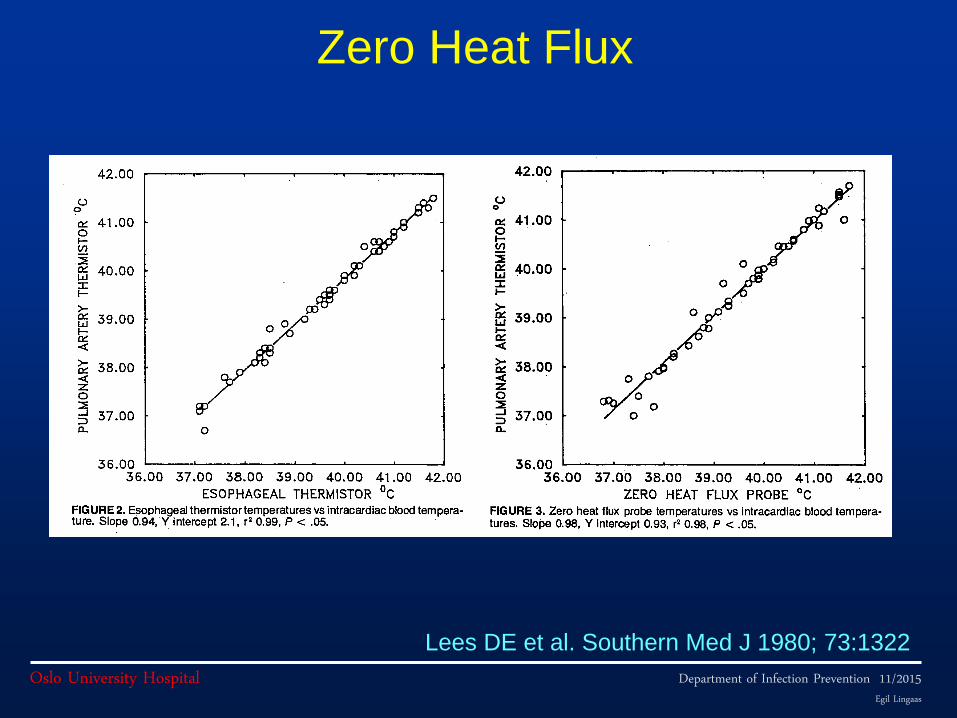
Oslo University Hospital Lees DE et al. Southern Med J 1980; 73:1322
Zero Heat Flux
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Kimberger O et al. J Anaesth 2009;103:226
Results:
98 % of all values were within + 0.5 oC of oesophageal temperature.
Sensitivity and specificity for detection of hypothermia were 0.77 and
0.93 respectively.
Conclusions:
The new double-sensor thermometer is sufficiently accurate to be
consideres an alternative to distal oesophageal core temperature
measurement, and may be particularly useful in patients undergoing
regional manaesthesia
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Teunissen LPJ et al. Physiol Measurement 2011;32:559
Zero Heat Flux
Department of Infection Prevention 11/2015 Egil Lingaas
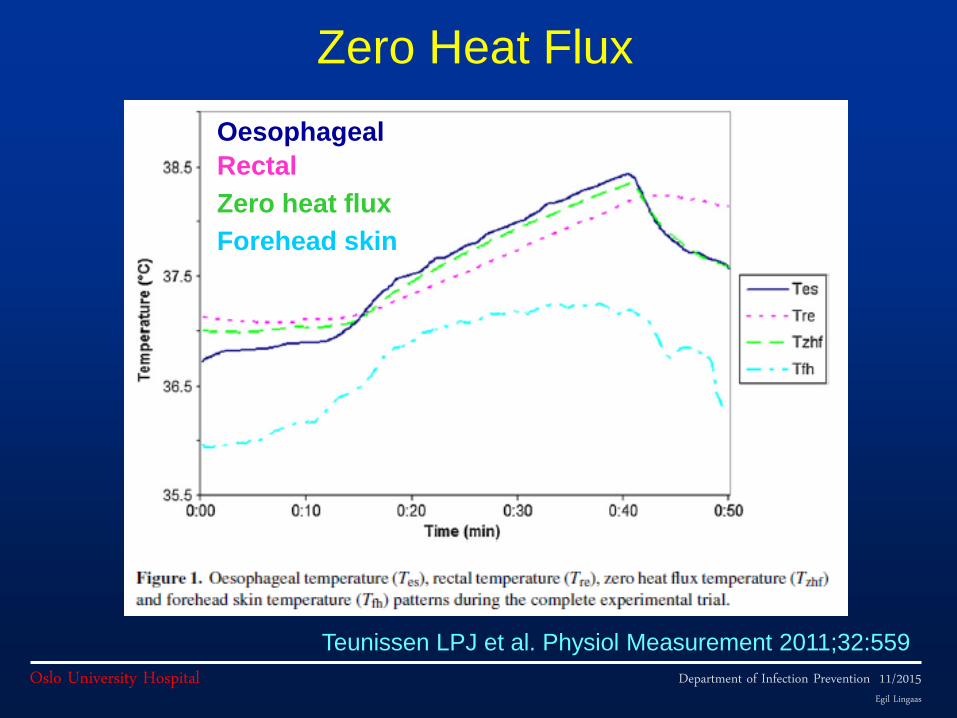
Oslo University Hospital Teunissen LPJ et al. Physiol Measurement 2011;32:559
Zero Heat Flux
Oesophageal
Rectal
Zero heat flux
Forehead skin

Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital Teunissen LPJ et al. Physiol Measurement 2011;32:559
Zero Heat Flux
Department of Infection Prevention 11/2015 Egil Lingaas
Oslo University Hospital
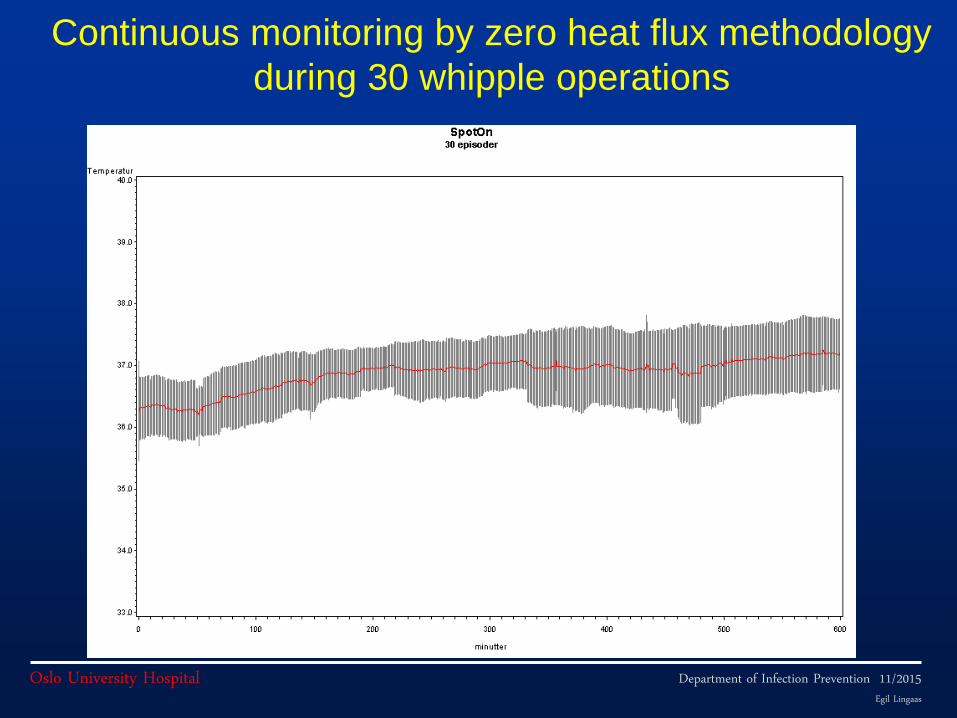
Continuous monitoring by zero heat flux methodology
during 30 whipple operations
Conclusions
The use of temperature monitoring for control of
core temperature is important for patient safety
during surgery.
Monitoring should start before surgery (at the
ward), and continue throughout the perioperative
phase.
Zero heat flux technology eliminates the need for
invasive monitoring, is monitoring core temperature
and facilitates continuous monitoring througout the
perioperative period