copyright © 2014 delhi academy of medical sciences, all rights reserved...
TRANSCRIPT

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 1/85
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 2/85
Test Information Test Name SWTS-OPHTHALMOLOGY-2017(MDMS) Total Questions 200
Test Type Examination Difficulty Level Difficult
Total Marks 800 Duration 120minutes
Test Question Language:- ENGLISH
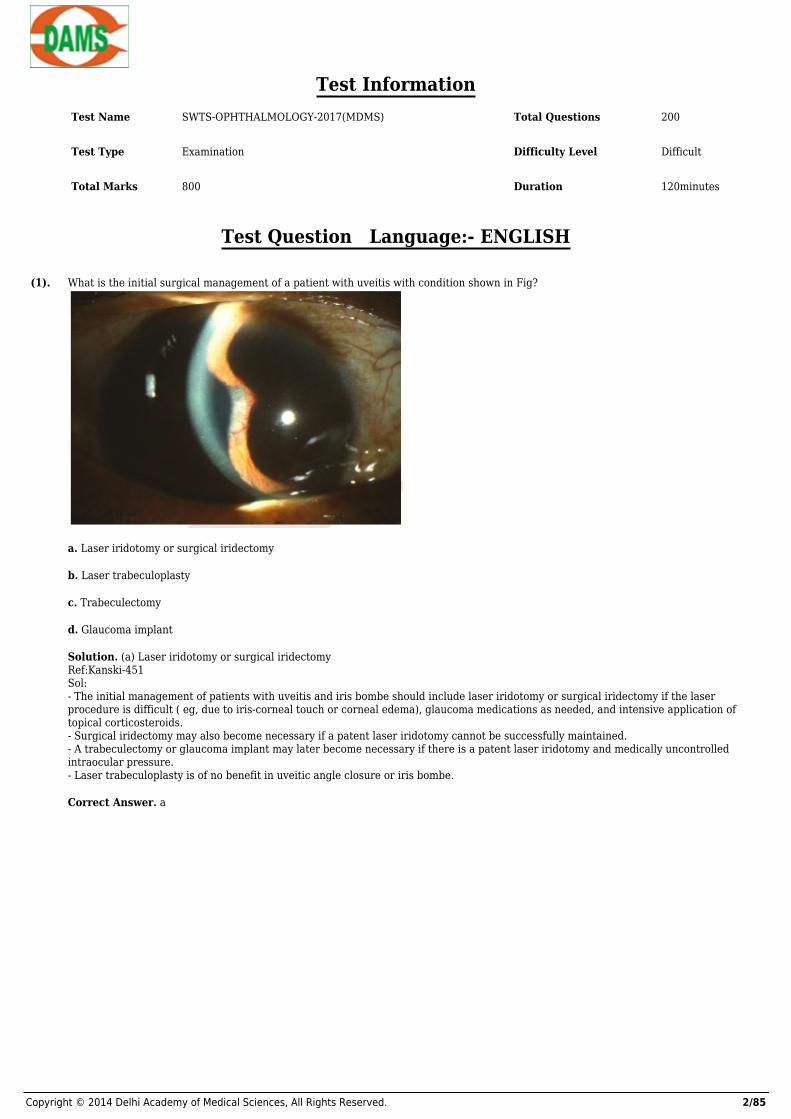
(1). What is the initial surgical management of a patient with uveitis with condition shown in Fig?
a. Laser iridotomy or surgical iridectomy
b. Laser trabeculoplasty
c. Trabeculectomy
d. Glaucoma implant
Solution. (a) Laser iridotomy or surgical iridectomyRef:Kanski-451Sol:- The initial management of patients with uveitis and iris bombe should include laser iridotomy or surgical iridectomy if the laserprocedure is difficult ( eg, due to iris-corneal touch or corneal edema), glaucoma medications as needed, and intensive application oftopical corticosteroids.- Surgical iridectomy may also become necessary if a patent laser iridotomy cannot be successfully maintained.- A trabeculectomy or glaucoma implant may later become necessary if there is a patent laser iridotomy and medically uncontrolledintraocular pressure.- Laser trabeculoplasty is of no benefit in uveitic angle closure or iris bombe.
Correct Answer. a

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 3/85
(2). A 56 year old woman complains of increasing difficulty reading the newspaper in the morning especially in bright sunlight. If her onlyocular abnormality is cataract, which type of lens opacity is she most likely to have
a. Posterior subcapsular
b. Nuclear
c. Cortical
d. Oil droplets
Solution. (a) Posterior subcapsularRef:Read the text belowSol:- Posterior subcapsular cataracts create more difficulty with glare and near vision. Progressive loss of vision from oil droplet is not oftenseen in this age.
Correct Answer. a
(3). A young baby with hypotonia and development delay is referred to ophthalmology where microphakia, posterior lenticonus and cataractare diagnosed. The intra-ocular pressure is 29mmHg bilaterally with Perkins tonometry. What abnormality would be MOST likely onurinalysis?
a. Red blood cells
b. Aminoaciduria
c. Leucocytes
d. Reducing substances
Solution. (b) AminoaciduriaRef:Glaucoma Medical Diagnosis and Therapy, 2nd edi, pg 398Sol:- This patient has features of Lowe's (oculocerebrorenal) syndrome, an inborn error of amino acid metabolism, which is X-linkedrecessive.- Fanconi's syndrome of the proximal renal tubules occurs in Lowe's syndrome, with aminoaciduria and low molecular weight proteinsfound in the urine
Correct Answer. b
(4). Which of the following corneal dystrophies is autosomal recessive?
a. Macular dystrophy
b. Lattice dystrophy type 1
c. Granular dystrophy
d. Fuchs endothelial corneal dystrophy
Solution. (a) Macular dystrophyRef:Kanski 6th edi. Pg 290Sol:- Macular corneal dystrophy is autosomal recessive, whereas lattice dystrophy type 1 andgranular dystrophy are autosomal dominant. Fuchs endothelial corneal dystrophy can show an autosomal dominant inheritance in somefamilies, but in the majority of cases the pattern of inheritance is yet to be elucidated
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 4/85
(5). Which is false regarding capillary haemangioma
a. First presents in adult life
b. When involving the skin , blanches on pressure
c. Usually requires no treatment
d. Is best treated initially with intralesional corticosteroid injection
Solution. (a) First presents in adult lifeRef:Kanski- 189Sol:- It manifests primarily in the first year, often in the neonatal period.- It blanches with pressure unlike a port wine stain.- It resolves spontaneously in the majority of cases
Correct Answer. a
(6). What is a typical finding in the early stages of Acanthamoeba keratitis?
a. Hypopyon
b. Ring infiltrate
c. Radial perineuritis
d. Corneal neovascularization
Solution. (c) Radial perineuritisRef:Alberts Principles and Practice of Ophthalmology– pg 723Sol:- Most studies of large outbreaks of Acanthamoeba keratitis note bilateral disease in 7%- 1 1 % of patients, unlike for other infectiouspathogens.- Ring infiltrates are a later manifestation of disease.- The pathognomonic finding of radial perineuritis does not appear to have prognostic significance for visual outcome.- Although overnight wear of rigid gas-permeable contact lenses may increase the risk of Acanthamoeba keratitis, overnight wear of softcontact lenses does not do so.
Correct Answer. c
(7). Which of the following is the most significant risk factor for pterygium development?
a. Peripheral Ulcerative Keratitis
b. Connective tissue disease
c. UV light exposure
d. Dry eye
Solution. (c) UV light exposureRef:Alberts Principles and Practice of Ophthalmology– pg 506Sol:- Pterygia are more common in sunny climates and in people who have spent significant time outdoors, reflecting exposure to UV light asa significant risk factor; there is a higher prevalence in men than in women.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 5/85
(8). Cataract occurs in:
a. Long-term chloroquine treatment
b. Long-term busulphan treatment
c. Hyperparathyroidism
d. Duchenne muscular dystrophy
Solution. (b) Long-term busulphan treatmentRef:Kansk- 337Sol:- Chloroquine causes cornea verticillata and maculopathy.- Busalfan is used in chronic myeloidleukaemia and can cause cataract. It is caused by hypoparathyroidism and conditions giving rise tohypocalcaemia.- Dystrophia myotonica givesrise to cataract.
Correct Answer. b
(9). Clinical features of ophthalmic herpes zoster include all except:
a. Scleritis
b. Ring-shaped corneal infiltrate
c. Entropion
d. Mucopurulent conjunctivitis
Solution. (b) Ring-shaped corneal infiltrateRef:Wills eye Manual-81Sol:- Herpes zoster is the most frequent local cause of scleritis.- Ring-shaped corneal infiltrateis seen in stromal infection by herpes simplex, Acanthamoeba and fungi.- Entropion may occur due to lid scarring; ectropion ,trichiasis and ptosis may also occur.
Correct Answer. b
(10). All of the following aremethods of estimating visual acuity in the preverbal child except:
a. Preferential looking testing
b. Visual evoked potentials
c. Electroretinography
d. Optokinetic nystagmus testing
Solution. (c) ElectroretinographyRef:Read the text belowSol:- ERG is not a method to estimate visual acuity.- Acuity estimates are best with visual evoked potentials.- OKN tests and preferential looking tests are fairly close behind.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 6/85
(11). A 30-year-old immunocompetent patient presents with a 1 - day history of vesicular lesionson his upper lip and the third recurrencewithin the past year of a dendritic epitheliallesion of his right cornea. Which of the following options would be the mostappropriatetreatment at this time?
a. Topical ophthalmic ganciclovir ointment 0 . 1 5 % 5 times a day for 1 week
b. Topical trifluridineeyedrops 1 % 9 times a day for 3 weeks
c. Systemic famciclovir 500 mg 3 times daily for 1 0 days
d. Systemic valacyclovir 500 mg 3 times daily for 1 0 days followed by maintenance dosing
Solution. (d) Systemic valacyclovir 500 mg 3 times daily for 1 0 days followed by maintenance dosingRef:Alberts Principles and Practice of Ophthalmology-- 637Sol:- None of the topical treatments has been shown to reduce recurrence of epithelial disease or stromal keratitis, and the topicaltrifluridine dosing schedule described is for too long.- Patients with repeated recurrences have been shown to benefit from long-term maintenance dosing of valacyclovir-short-term dosinghas not been shown to reduce recurrence.- This patient also has dermatologic lesions that would benefit from systemic therapy.
Correct Answer. d
(12). What is the most appropriate initial treatment of unilateral stem cell deficiency with irregularityextending into the visual axis that issecondary to contact lens use?
a. Boston type I keratoprosthesis
b. Corneal debridement
c. Discontinuation of contact lens use
d. Limbal stem cell allograft transplantation
Solution. (c) Discontinuation of contact lens useRef:Kanski -864Sol:- Unilateral stem cell deficiency secondary to contact lens wear is usually mild and responds well to discontinuation of contact lens usealong with a short course of topical corticosteroids.- If these measures are not effective, then localized corneal debridement of the superior portion of the irregular epithelium will allow thehealthy inferior corneal epithelium to replace the abnormal epithelium produced by the stem cell dysfunction.- Limbal stem cell allograft transplantation is reserved for more severe cases of stem celldysfunction such as that typically associatedwith Stevens- Johnson syndrome or bilateral chemical injuries.
Correct Answer. c
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 7/85
(13). A 60-year-old Afro-Caribbean patient complains of a whitish area on her left eye for several weeks. Her eye has been slightlyuncomfortable but with no discharge. On examination, there is peripheral corneal stromal thinning temporally with fluorescein poolingand corneal neovascularisation. Which blood test is least helpful in investigating the underlyingdiagnosis?
a. HIV antibodies
b. Rheumatoid factor
c. Anti-neutrophil cytoplasmic antibody
d. Purified protein derivative skin test
Solution. (a) HIV antibodiesRef:Kanski -277Sol:- This patient has signs suggestive of peripheral ulcerative keratitis.Underlying systemic causes of PUK include:- Rheumatoid arthritis- Wegener's granulomatosis- polyarteritisnodosa- relapsing polychondritis- infection: TB, syphilis- HIV or AIDS are not recognised causes of PUK
Correct Answer. a
(14). From what source does the cornea receive most of its glucose for nutrition?
a. Tear film
b. Aqueous humor
c. Limbal blood vessels
d. Corneal epithelium
Solution. (b) Aqueous humorRef:Alberts Principles and Practice of Ophthalmology- 423Sol:- Most of the glucose is transferred into the aqueous humor, from which it then diffuses through the permeable corneal endothelium andequilibrates in the stroma for nutritional use.- The corneal epithelium has tight junctions that do not allow the passage of fluid.- The limbal blood vessels supply oxygen to the cornea; they are the source of inflammatory cells in tight lens syndrome but not ofnutrition to the cornea.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 8/85
(15). Which of the following findings is most likely to be seen in a patient with systemic lupus erythematosus?
a. Chronic anterior uveitis
b. Intraretinal hemorrhages and cotton-wool spots
c. Intermediate uveitis
d. Acute anterior uveitis
Solution. (b) Intraretinal hemorrhages and cotton-wool spotsRef:Wills eye Manual, 6th edi. Pg 369Sol:- Lupus retinopathy is considered an important marker of systemic disease activity, and consists of cotton-wool spots with or withoutintraretinal hemorrhages occurring independently of hypertension; it is thought to be due to the underlying microangiopathy of thedisease.- Severe retinal vascular occlusive disease (both arterial and venous thromboses) may result in retinal nonperfusion ischemia, secondaryretinal neovascularization, and vitreous hemorrhage and appears to be associated with central nervous system lupus disease and thepresence of antiphospholipid antibodies.- Lupus choroidopathy, characterized by serous elevation of the neurosensory retina, pigment epithelium, or both; choroidal infarction;and choroidal neovascularization may be observed in patients with severe systemic vascular disease due to either hypertension fromlupus nephritis or systemic vasculitis.- Uveitis per se is distinctly uncommon in patients with lupus erythematosus.
Correct Answer. b
(16). The sclera:
a. Is thickest behind the insertions of the aponeurotic tendons of the extraocular muscles
b. Is composed mainly of collagen Type 1
c. Has more proteoglycans and glycosaminoglycans in its matrix than the cornea
d. Consists of regularly arranged collagen
Solution. (B)Ref:Alberts Principles and Practice of Ophthalmolog- 423Sol:- The sclera consists of dense irregular connective tissue, unlike the cornea which is regular in arrangement.- The sclera also has less proteoglycans and glycosaminoglycans in its matrix than the cornea.- The sclera is thinnest behind the insertions of the aponeurotic tendons and is composed mainly of Type 1 collagen.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 9/85
(17). 25-year-old Brazilian man presents with a history of decreased vision in his left eye for 1 week. Visual acuity is 20/70 and moderatevitritis is present. On dilated examination, a pigmented scar in the posterior pole with adjacent focal white chorioretinitis is present.Study the Fig, What is the most appropriate treatment?
a. Oral corticosteroids
b. Pyrimethamine, sulfadiazine, and prednisone
c. Intravenous acyclovir
d. Amphotericin B
Solution. (b) Pyrimethamine, sulfadiazine, and prednisoneRef:Kanski -468sSol:- This patient presents with the characteristic lesion of ocular toxoplasmosis (headlight in fog appearance): focal retinochoroiditis withoverlying vitreous inflammation adjacent to a pigmented chorioretinal scar.- Moreover, the patient is from Brazil, an area where toxoplasmosis is endemic.- The presence of significantly reduced visual acuity and vitritis are indications for treatment.- While numerous agents have been used to treat toxoplasmosis, there is no single drug or combination that should be appliedcategorically to every patient, nor is there consensus as to the most effective regimen.- The classic regimen for the treatment of ocular toxoplasmosis consists of "triple therapy" with pyrimethamine, sulfadiazine, andprednisone; because sulfonamides and pyrimethamine inhibit folic acid metabolism, folinic acid is added to try to prevent the decreasesin white blood cells and platelets that may result from treatment.- Some clinicians advocate adding clindamycin to this regimen as "quadruple" therapy. Alternative regimens include the use oftrimethoprim -sulfamethoxazole, azithromycin alone or in combination with pyrimethamine, and atovaquone. Intravitreal clindamycin hasbeen used successfully in patients in whom systemic therapy is either undesirable or not tolerated.- Oral corticosteroids are frequently added after 24-48 hours of antimicrobial therapy to treat the inflammatory component of thedisease, but are never used as monotherapy. Similarly, periocular injections of steroids are contraindicated in patients with oculartoxoplasmosis.- Intravenous acyclovir is the gold standard for the treatment of herpetic necrotizing retinitis, and amphotericin B is used in thetreatment of fungalendophthalmitis, particularly that caused by Aspergillus organisms.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 10/85
(18). The optic disc is a vertical oval, with average dimensions of :
a. 1.76mm horizontally by 1.92mm vertically
b. 1.92mm horizontally by 1.76mm vertically
c. 2.76mm horizontally by 1.92mm vertically
d. 1.92mm horizontally by 2.76mm vertically
Solution. (a) 1.76mm horizontally by 1.92mm verticallyRef:Read the text belowSol:- Optic cup is that central portion of disc where the axons are absent.- The optic disc is placed 3 to 4 mm to the nasal side of the fovea. It is a vertical oval, with average dimensions of 1.76mm horizontally by1.92mm vertically.- There is a central depression, of variable size, called the optic cup.
Correct Answer. a
(19). In Fundus color coding system, detached retina is shown in which of the following color -
a. Green
b. Red
c. Brown
d. Blue
Solution. (d) BlueRef:Read the text below
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 11/85
(20). Which of the following is not a feature of basal cell carcinoma of lid -
a. Occur on lower lid
b. Rodent Ulcer
c. Liver metastases common
d. Surgical excision treatment
Solution. (c) Liver metastases commonRef:Read the text belowSol:Basal cell carcinoma is a locally invasive tumor, and metastasis to distant sites is very rare. Most common sites in decreasing frequenciesare -- Lower Lid (50%), Inner canthus (25%), Upperlid (10%-15%), Lat. canthus (<5%)- Basal cell carcinoma is most comman lid malignancy (85% of all lid malignancies), which is most common in middle aged or elderlypatients.- Most common sub types - nodular, morpheaform. Rodent ulcer is an advanced appearance of the noduloulcerative type.- Ocular adnexal basalcarcinoma have a 3% mortality rate.- Tumor near/at medial canthus are most dangerous and may invade the orbit via lacrimal drainage system or extend to brain.- Surgical excision is best treatment modality, followed by lid reconstruction. Moh’s microsurgery is best technique to preserve the lidanatomy.
Correct Answer. c
(21). Roth Spot’s are most commonly seen in -
a. SABE
b. Anemia
c. CO poisoning
d. Leukemia
Solution. (a) SABERef:Read the text belowSol:- Roth spot is term used for white centered hemorrhages, particularly for SABE.- Such haemarrheges are also seen in numbers of conditions, called Pseudo - Roth spots, as they differ pathologically.White centered hemorrhages are seen in -A. Elevated venous pressure1. Neonatal birth trauma2. Complicated delivery in mothers3. Battered babies/Children4. Prolonged or difficult intubation5. Intracranial haemorrhages from AVMB. Ischemia (often with elevated venous pressure)1. Anemia2. Anoxia3. CO poisoningC. Capillary fragility .1. Hypertensive retinopathy2. Diabetic retinopathy3. Oral contraceptives4. Idiopathic
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 12/85
(22). Mittendorf’s dot is a congenital cataract. It is a remnant of
a. Hyaloid artery
b. Optic disc
c. Vitreous artery
d. Fetal nucleus
Solution. (a) Hyaloid arteryRef:Read the text belowSol:- This is a remnant of the hyaloid artery that has failed to dissolve and usually remains partly attached to the back surface of the lens ormay be free floating just behind the lens.- There may be a part of the hyaloid artery that trails off into the vitreous in a corkscrew-shape.
Correct Answer. a
(23). Under the National Programme for Control of Blindness, who is supposed to conduct the vision screening of school students?
a. Ophthalmologists
b. School teachers.
c. Medical officers of health centres
d. Health assistants
Solution. (b) School teachers.Ref:Read the text belowSol:- Under the National Programme for Control of Blindness, School teachers are supposed to conduct the vision screening of schoolstudents
Correct Answer. b
(24). In Marcus Gunn pupil
a. Affected eye is less constricted than unaffected eye
b. Affected eye is more constricted than unaffected eye
c. Affected eye does not constrict
d. Affected eye shows paradoxical dilatation
Solution. (a) Affected eye is less constricted than unaffected eyeRef:Read the text belowSol:- Marcus Gunn pupil (relative afferent pupillary defect) is a medical sign observed during the swinging-flashlight test whereupon thepatient's pupils constrict less (therefore appearing to dilate) when a bright light is swung from the unaffected eye to the affected eye.- The affected eye still senses the light and produces pupillary sphincter constriction to some degree, albeit reduced.- The most common cause of Marcus Gunn pupil is a lesion of the optic nerve (distal to the optic chiasm) or severe retinal disease.
Correct Answer. a

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 13/85
(25). Cherry red spot is seen in all except
a. Niemann Pick disease
b. GM1 gangliosidosis
c. Tay Sach disease
d. Gaucher’s disease
Solution. (d) Gaucher’s diseaseRef:Read the text belowSol:Cherry red spots on retina seen in:- CRAO- Tay Sachs disease- GM1 gangliosidosis- Quinine amblyopia- Metachromatic leukodystrophy- Multiple sulfatase deficiency- Berlins disease- Sanhoffs disease- Niemann Pick disease
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 14/85
(26). All are important causes of childhood blindness in India except?

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 15/85
a. Glaucoma
b. Congenital dacryocystitis

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 16/85
c. Malnutrition

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 17/85
d. Ophthalmia neonatorum
Solution. (b) Congenital dacryocystitisRef: Vaughan & Asbury's General Ophthalmology17th EditionSol:- The relative importance of various causes of blindness differs according to the level of social development in the geographic area beingstudied.- In developing countries, cataract is the leading cause, with trachoma, glaucoma, leprosy, onchocerciasis, and xerophthalmia also beingimportant.- Corneal ulceration is also a significant cause of monocular blindness in the developing world. In more developed countries, blindness isto a great extent related to the aging process.- Cataract is still important despite the availability of facilities for its treatment, along with age-related macular degeneration andglaucoma.- Other causes are diabetic retinopathy, herpes simplex keratitis, retinal detachment, and inherited retinal degenerative disorders.- In terms of the worldwide prevalence of blindness, the vastly greater number of people in the developing world and the greaterlikelihood of their being affected mean that the causes of blindness in those areas are numerically more important.- Cataract is responsible for more than 22 million cases of blindness and glaucoma 6 million, while leprosy and onchocerciasis each blindapproximately 1 million individuals worldwide.- Interestingly, the number of individuals blind from trachoma has dropped dramatically in the past 10 years from 6 million to 1.3 million,putting it in seventh place on the list of causes of blindness worldwide.- Xerophthalmia is estimated to affect 5 million children each year; 500,000 develop active corneal involvement, and half of these goblind.- Central corneal ulceration is also a significant cause of monocular blindness worldwide, accounting for an estimated 850,000 cases ofcorneal blindness every year in the Indian subcontinent alone.- As a result, corneal scarring from all causes now is the fourth greatest cause of global blindness. Dacryocystitis- Infection of the lacrimal sac is a common disease that usually occurs in infants or postmenopausal women.- It is most often unilateral and always secondary to obstruction of the nasolacrimal duct.- In many adult cases, the cause of obstruction remains unknown.- Dacryocystitis is uncommon in the intermediate age groups unless it follows trauma or is caused by a dacryolith.- Spontaneous improvement follows passage of a dacryolith, but recurrence is the rule.- In infants, chronic infection accompanies nasolacrimal duct obstruction, but acute dacryocystitis is uncommon.- Acute dacryocystitis in children is often a result of Haemophilus influenzae infection. Prompt and aggressive treatment should beinstituted because of the risk of orbital cellulitis.- Acute dacryocystitis in adults is usually caused by Staphylococcus aureus or occasionally beta -hemolytic streptococci. In chronicdacryocystitis, Streptococcus pneumoniae or, rarely,- Candida albicans is the predominant organism—mixed infections do not occur. The infectious agent can be identified microscopically bystaining a conjunctival smear taken after expression of the tear sac.Clinical Findings- The chief symptoms of dacryocystitis are tearing and discharge.- In the acute form, inflammation, pain, swelling, and tenderness are present in the tear sac area.- Purulent material can be expressed from the sac. In the chronic form, tearing is usually the only sign.- Mucoid material usually can be expressed from the sac. It is curious that dacryocystitis is seldom complicated by conjunctivitis eventhough the conjunctival sac is constantly being bathed with pus exuding through the lacrimal puncta.- Corneal ulcer occasionally occurs following minor corneal trauma in the presence of pneumococcal dacryocystitis.- Chronic dacryocystitis increases the risk of endophthalmitis after cataract surgery.Treatment- Acute dacryocystitis usually responds to appropriate systemic antibiotics, and the chronic form can often be kept latent with antibioticdrops. However, relief of obstruction is the only cure.- In adults, the presence of a mucocele is evidence that the site of obstruction is in the nasolacrimal duct and that dacryocystorhinostomyis indicated. The patency of the canalicular system is ensured if mucus or pus is regurgitated through the puncta on compression of thesac.- Examination of the nose is important to ensure adequate drainage space between the septum and the lateral nasal wall.- Dacryocystorhinostomy consists of forming a permanent anastomosis between the lacrimal sac and the nose. With the externalapproach, exposure is gained by an incision over the anterior lacrimal crest.- A bony opening is made in the lateral wall of the nose, and the nasal mucosa is sutured to the mucosa of the lacrimal sac. An endoscopicapproach through the nose using lasers can be used for formation of the anastomosis between the lacrimal sac and the nose or tocompletely avoid an external incision.- Transluminal balloon dilation of the distal nasolacrimal system may also be useful for patients not suitable for surgery.- Excessive tearing (epiphora) is occasionally due to canalicular stenosis or obstruction at the junction of the common canaliculus andlacrimal sac.- In either case, compression of the sac does not cause regurgitation of fluid, mucus, or pus through the puncta, and no mucocele ispresent.- Intubation and irrigation of the canalicular system with a lacrimal cannula and x-ray studies with contrast media (dacryocystography)will identify the site of obstruction. Common canalicular obstruction may be treated by intubation of the passages with silicone stent for3–6 months.- A thick obstructing scar, however, will necessitate dacryocystorhinostomy and canaliculoplasty with silicone intubation of thecanalicular system.- In infantile dacryocystitis, the site of stenosis is usually at the valve of Hasner. Failure of canalization is a common occurrence (4–7% ofnewborns), but normally the duct opens spontaneously within the first month. Forceful compression of the lacrimal sac will sometimesrupture the membrane and establish patency.- If stenosis persists more than 6 months or if dacryocystitis develops, probing of the duct is indicated.- One probing is effective in 75% of cases. In the remainder, cure can almost always be achieved by repeated probing, by inward fractureof the inferior turbinate, or by a temporary silicone lacrimal splint. Probing should not be attempted in the presence of acute infection
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 18/85
(27). The AP diameter of a normal human eye ball
a. 18 mm
b. 24 mm
c. 30 mm
d. 36 mm
Solution. (b) 24 mmRef.:Read the text belowSol :- Normal Adult Eyeball :- Ap diameter - 24mm- Vertical diameter - 23mm- Volume - 6.5ml- Weight -7gm- 1 mm change in axial length of eyeball – 3D change in power.- 1 mm change in corneal curvature – 6D change in power
Correct Answer. b
(28). A semicircular fold of skin covering the medial canthus of eye is called
a. Coloboma
b. Microblepharon
c. Epicanthus
d. Distichiasis
Solution. (c) EpicanthusRef.:Read the text belowSol :Epicanthus :- Semicircular fold of skin covering the medial canthus- Disappear with the development of nose- Normal facial feature in Mongolian races- Most common congenital anomaly of eyelids
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 19/85
(29). Ectopia lentis is seen in all the following conditions except
a. Marfan syndrome
b. Lawrence Moon Biedl syndrome
c. Ehler – Danlos syndrome
d. Wil Marchesani syndrome
Solution. (b) Lawrence Moon Biedl syndromeRef.:Read the text belowSol :Ectopia lentis is a displacement or malposition of the eye's crystalline lens from its normal location. A partial dislocation of a lens istermed lens subluxation or subluxated lens; a complete dislocation of a lens is termed lens luxation or luxated lens. In humans, there area number of systemic conditions that are associated with ectopia lentis More common:- Marfan syndrome (upward and outward)- Homocystinuria (downward and inwards)- Weill-Marchesani syndrome- Sulfite oxidase deficiency- HyperlysinemiaLess common:- Ehlers-Danlos syndrome- Crouzon disease- Refsum syndrome- Kniest syndrome- Mandibulofacial dysostosis- Sturge-Weber syndrome- Conradi syndrome- Pfaundler syndrome- Pierre Robin syndrome- Wildervanck syndrome- Sprengel deformity
Correct Answer. b
(30). Colored halos are not seen in
a. Pterygium
b. Angle closure glaucoma
c. Mucopurulent conjunctivitis
d. Cataract
Solution. (a) PterygiumRef.:Read the text belowSol :CAUSES OF COLORED HALOS :- Acute angle closure glaucoma- Acute mucopurulent conjunctivitis (halos disappear on removing the discharge)- Corneal scar- Corneal edema (bullous keratopathy)- Early stages of cataract- Contact lens over wear- Haze in ocular media- Emsley – Fincham’s test – a stenopaeic slit is passed across the pupil- Glaucoma : halos remain intact- Immature cataract : halos break into segments
Correct Answer. a

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 20/85
(31). Acetazolamide
a. Inhibits distal Na+ uptake
b. Is a high efficacy diuretic
c. Causes metabolic alkalosis
d. Has persistent effect on aqueous humor production during chronic use.
Solution. (d) Has persistent effect on aqueous humor production during chronic use.Ref:Read the text belowSol:- Acetazolamide inhibits carbonic anhydrase – ↓ Na+ reabsorption in exchange of H+ at proximat tubule – systemic acidosis but alkalineurine. It is a low efficacy diuretic.- Long term use in glaucoma is effective.- It acts by lowering I.O.T. by decreasing aqueous humour production
Correct Answer. d
(32). Dangerous area of the eye is:
a. Ciliary body
b. Sclera
c. Optic nerve
d. Retina
Solution. (a) Ciliary bodyRef:Read the text belowSol:- The dangerous area of the eye is the region in the neighborhood of the ciliary- Body, and wounds or injuries in this situation are peculiarly dangerous.- Collecting ducts are lined by columnar epithelium
Correct Answer. a
(33). Terrien’s disease typically
a. Is unilateral
b. Leads to loss of epithelium
c. Causes visual impairment due to astigmatism
d. Affects females
Solution. (c) Causes visual impairment due to astigmatismRef:Wills eye Manual- 98Sol:- It is usually bilateral although sometimes asymmetrical, mostly seen in males over 60 years.- The corneal epithelium is usually intact.
Correct Answer. c
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 21/85
(34). Chronic postoperative endophthalmitis is most commonly caused by which organism?
a. Candida glabrata
b. Nocardia species
c. Klebsiellapneumoniae
d. Propionibacterium acnes
Solution. (d) Propionibacterium acnesRef:Kanski-345Sol:- Chronic postoperative bacterial endophthalmitis is most commonly due to Propionibacterium acnes.- Many other bacteria and fungi, such as Staphylococcus epidermidis and Corynebacterium species, also cause similar chronicendophthalmitis.- P acnes, a commensal, anaerobic, gram-positive, pleomorphic rod, is found on the eyelid skin and conjunctiva of healthy patients.
Correct Answer. d
(35). All of the following pass through the common tendinous ring except:
a. Inferior division of oculomotor nerve
b. Nasociliary nerve
c. Frontal nerve
d. Superior division of oculomotor nerve
Solution. (c) Frontal nerveRef:Read the text belowSol:- The frontal nerve passes superior to the common tendinous ring.- Structures passing within the ring include: the oculomotor nerve (superior and inferior divisions), abducent nerve, nasociliary nerve,sympathetic root of the ciliary ganglion and on occasion the inferior ophthalmic vein.
Correct Answer. c
(36). Which feature on radiographic imaging is most in keeping with an optic nerve meningioma:
a. Osteoblastic changes
b. Pleboliths
c. Fusiform enlargement of the optic nerve
d. Osteolytic changes
Solution. (a) Osteoblastic changesRef:Kanski-189Sol:- Radiographically, meningiomas produce hyperplastic bony changes, although bone destruction can be seen. An optic nerve meningiomaappears as a kinked nerve with rail-road track sign- Note: a fusiform enlargement of the nerve on imaging is typical of ON glioma.- Note: pleboliths are suggestive of orbital varices or other slow-flow venous abnormalities such as cavernous haemangioma.
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 22/85
(37). A 40-year-old patient with mitral regurgitation presents to clinic. You notice bilateral lens subluxations and a high-arched palate. Whichis true?
a. Inheritance is AR
b. There may be associated mental retardation
c. Accommodation is usually intact
d. Lens subluxation is typically downwards
Solution. (c) Accommodation is usually intactRef:Wills eye Manual- 406Sol:- This patient has Marfan’s syndrome, which is autosomal dominant.- Intellect is normal.- Associated systemic features include arachnodactyly, increased arm span:height ratio, high arched palate and cardiac valvularanomalies.- Lens subluxation is upwards in Marfan’s and zonules are present with intact accommodation, unlike homocystinuria where subluxationis downwards and zonules are absent with accommodation lost.
Correct Answer. c
(38). A young male presents with h/o unilateral progressive proptosis for many years. Swelling is increased on bending forward andcompressible,USG shows retrobulbar echogenicity. What is the diagnosis?
a. Neurofibromatosis
b. Orbital varix
c. Orbital A-V fistula
d. Orbital encephalocele
Solution. (b) Orbital varixRef: Grainger & Allison's Diagnostic Radiology, 5th edSol:Carotid-cavernous fistulae• Carotid-cavernous fistulae (CCFs) are fistulae between the carotid siphon and the cavernous sinus.• They may occur spontaneously, for example after rupture of a carotid siphon aneurysm or after trauma.• Clinically they present with engorgement of the orbit and globe (sclera and conjunctiva), pulsating exophthalmos, a bruit and eventually glaucoma and visual loss inlarger CCFs.• Cross-sectional imaging shows signs of orbital venous hypertension with an enlarged engorged superior ophthalmic vein and extra-ocular muscles• MRI shows signal void in the cavernous sinus and superior ophthalmic vein due to the presence of fast-flowing arterial blood.• The enlarged cavernous sinus may be bowed convex to the middle cranial fossa.• MR angiography shows filling of the cavernous sinus and superior ophthalmic vein in conjunction with the arterial anterior intracranial circulation.• Conventional angiography with injections of internal and external carotid arteries can usually distinguish between ‘direct’ fistulae and ‘indirect’ ones (a dural arteriovenousmalformation in the region of the cavernous sinus).• - Angiography may show filling of the ipsilateral or contralateral cavernous sinus via the intercavernous sinuses, and drainage into ipsilateral or bilateral superiorophthalmic veins, inferior petrosal sinuses, or even the cortical veins or spheno-parietal sinuses when severe.Venous varix• A venous varix is an enormously dilated vein representing a congenital or acquired (e.g. post-traumatic) venous malformation.• It may occur on its own or be associated with an intra-orbital or intracranial arteriovenous malformation.• Multiple varicosities may be present. Clinically they present with intermittent proptosis upon straining or coughing and retrobulbar pain.• On CT a venous varix is seen as an intraconal hyperdense lobulated mass with strong enhancement.• Phleboliths and clot may be present.• When small, a varix may not be seen unless it is made to enlarge with a Valsalva manoeuvre or during imaging in the prone position.• Orbital phlebography is no longer required for making the diagnosis.• MRI may reveal slow flowphenomena.• Clot due to spontaneous thrombosis is common, which can result in variable signal intensity on MRI.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 23/85
(39). True about Mooren’s ulcer are all except:
a. It is a superficial ulcer starting at the corneal margin
b. Pain is absent
c. It has advancing border
d. The presenting symptom is blurred vision due to irregular astigmatism
Solution. (b) Pain is absentReference – Read the text belowSol:- Mooren’s ulcer or chronic serpiginous ulcer or rodent ulcer is a very rare superficial ulcer.- It is accompanied by severe and persistent neuralagic pain and lacrimation.- It rarely perforates and is treated in initial stages with topical steroids
Correct Answer. b
(40). Commonest cause of Intra orbital tumor in childhood is
a. Rhabdomyosarcoma
b. Retinoblastoma
c. Chroidal melanoma
d. Iris naveus
Solution. (A) RetinoblastomaReference – Read the text belowSol:- Rhabdomyosarcoma arises more often in the orbit than in any other site of the body.- It is known to be the most common primary malignant orbital neoplasm of childhood.- But retinoblastoma is the most common intraocular malignancy of childhood as the eyeball is a part of the orbit; and the frequency ofretinoblastoma is more common than rhabdomyosarcoma.- So, retinoblastoma is the most common intraorbital malignancy of childhood
Correct Answer. a
(41). Essential atrophy of the choroid is a consequence of disordered metabolism of
a. Phenylalanine
b. Ornithine
c. Cysteine
d. Arginine
Solution. (b) OrnithineReference – Read the text belowSol:- Gynate atrophy is inherited as an autosomal recessive disease.- It occurs due to an inborn error of ornithine ketoacid aminotransferase enzyme; activity.- It is associated with an increase in the level of ornithine in the plasma, urine CSF and aqueous humor.- It presents with symptoms of nightblindness during the first decade of life.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 24/85
(42). Wound leak can be identified by:
a. Syringing and probing
b. Seidel’s test
c. Naffziger’s test
d. Rose Bengal dye
Solution. (b) Seidel’s testReference – Read the text belowSol:- Seidel’s test is done by instilling fluorescein dye in the conjunctival sac.
Correct Answer. b
(43). A 5-yrs-old child with a posterior fossa tumor complains of diplopia. On examination,the child have strabismus. Which extraocular palsy ismost likely to be there?
a. Superior oblique palsy
b. Lateral rectus palsy
c. Inferior oblique palsy
d. Medial rectus palsy
Solution. (b) Lateral rectus palsyRef:Read the text belowSol:- In the pediatric population, lateral rectus palsy, not superior oblique palsy, inferior oblique palsy medial rectus palsy, or superior rectuspalsy, is most commonly associated with brain tumors.- Therefore, it is the extraocular palsy most likely responsible for this patient’s symptoms.- Children rarely complain of diplopia (double vision) because they suppress the image of the affected eye.- With brain tumors, diplopia is a sign of increased intracranial pressure.- Eye examination may reveal strabismus from palsy of the lateral rectus secondary to involvement of the abducens.- Many children tilt their heads in an effort to compensate for the diplopia.- Other affected nerves are the oculomotor and, rarely, the trochlear.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 25/85
(44). Which of the following ocular conditions is autosomal dominant in inheritance?
a. Best disease
b. Gyrate atrophy
c. Lawrence-Moon-Biedel syndrome
d. Bassen Kornzweig disease
Solution. (a) Best diseaseRef: Vaughan & Asbury's General Ophthalmology17th EditionSol:Anatomic Classification of Macular Dystrophies Inner retina- X-linked juvenile retinoschisisPhotoreceptors- Cone-rod dystrophyRetinal pigment epithelium- Stargardt disease- Best diseaseBest Disease (Juvenile-Onset Vitelliform Dystrophy)- Best disease is an autosomal dominant disorder with variable penetrance and expressivity.- Onset is usually in childhood.- The fundoscopic appearance is variable and ranges from a mild pigmentary disturbance within the fovea to the typical vitelliform or"egg yoke" lesion located in the central macula- This characteristic cyst-like lesion is generally quite round and well demarcated and contains homogeneous opaque yellow materiallying at the apparent level of the retinal pigment epithelium.- The "egg yoke" may degenerate and be associated with subretinal neovascularization, subretinal hemorrhage, and extensive macularscarring. Visual acuity often remains good, and the ERG is normal.- An abnormal electro-oculogram (EOG) is the hallmark of the disease.- The genetic abnormality is a mutation in the VMD2 gene, which encodes a transmembrane calcium-sensitive chloride channel(bestrophin) expressed in retinal pigment epithelium.
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 26/85
(45). The vitreous body in adult eye develops from:
a. Primary vitreous
b. Secondary vitreous
c. Tertiary vitreous
d. None
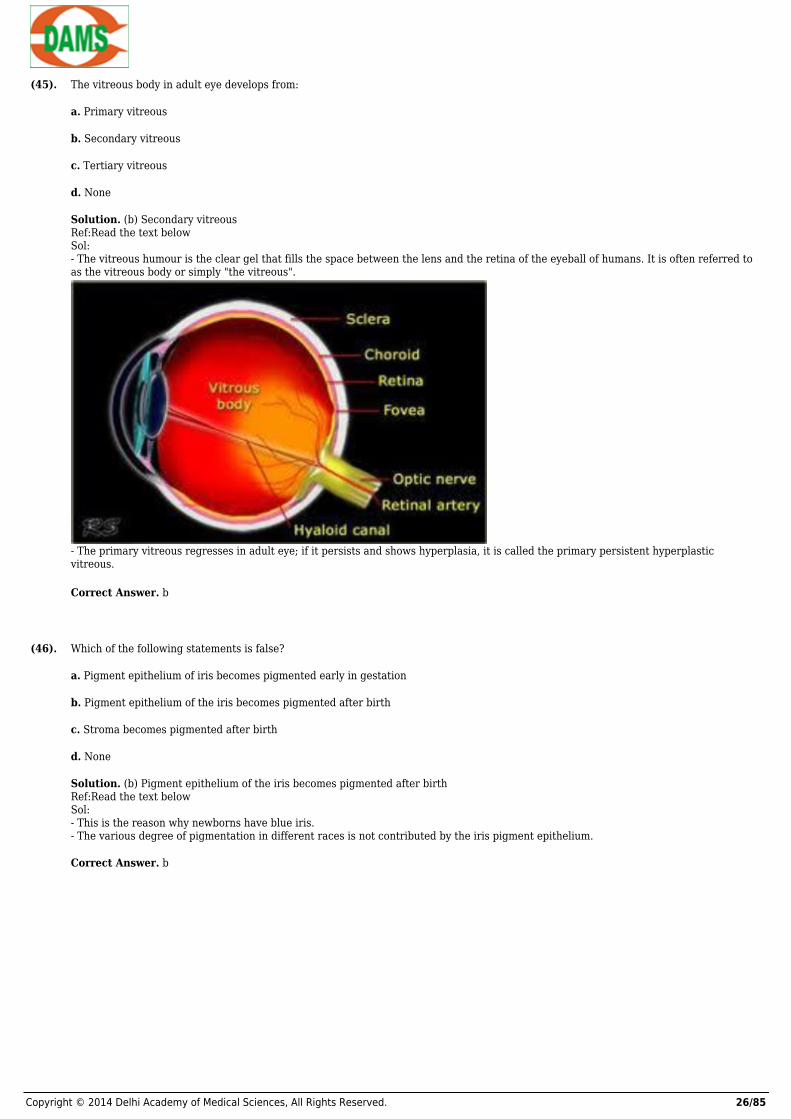
Solution. (b) Secondary vitreousRef:Read the text belowSol:- The vitreous humour is the clear gel that fills the space between the lens and the retina of the eyeball of humans. It is often referred toas the vitreous body or simply "the vitreous".
- The primary vitreous regresses in adult eye; if it persists and shows hyperplasia, it is called the primary persistent hyperplasticvitreous.
Correct Answer. b
(46). Which of the following statements is false?
a. Pigment epithelium of iris becomes pigmented early in gestation
b. Pigment epithelium of the iris becomes pigmented after birth
c. Stroma becomes pigmented after birth
d. None
Solution. (b) Pigment epithelium of the iris becomes pigmented after birthRef:Read the text belowSol:- This is the reason why newborns have blue iris.- The various degree of pigmentation in different races is not contributed by the iris pigment epithelium.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 27/85
(47). Which nerve carries the parasympathetic fibers?
a. Nerve to the medial rectus
b. Nerve to the superior rectus
c. Nerve to the inferior oblique
d. Nerve to the superior oblique
Solution. (c) Nerve to the inferior obliqueRef:Read the text belowSol:- The parasympathetic fibres start from the Edinger-Westphal nucleus and run in the main trunk of the third nerve, as far in the orbit.- Then the fibres passes into the branch which supplies the inferior oblique muscle; leaving it by the short root of the ciliary ganglion
Correct Answer. c
(48). Nerve supply to the lacrimal sac is:
a. Supratrochlear nerve
b. Nasociliary nerve
c. Infraorbital nerve
d. Supraorbital nerve
Solution. (b) Nasociliary nerveRef:Read the text belowSol:- The lacrimal sac is the upper dilated end of the nasolacrimal duct, and is lodged in a deep groove formed by the lacrimal bone andfrontal process of the maxilla. It connects the lacrimal canaliculi, which drain tears from the eye's surface, and the nasolacrimal duct,which conveys this fluid into the nasal cavity.- Infratroclear nerve is the terminal branch of the nasociliary nerve.- It supplies the lacrimal sac; medial conjunctiva and canaliculi.
Correct Answer. b
(49). Equatorial diameter of the crystalline lens is:
a. 7mm
b. 8mm
c. 9mm
d. 10mm
Solution. (c) 9mmRef:Read the text belowSol:- The lens is a transparent, biconvex structure in the eye that, along with the cornea, helps torefract light to be focused on the retina.- The lens, by changing shape, functions to change thefocal distance of the eye so that it can focus on objects at various distances, thusallowing a sharp real image of the object of interest to be formed on the retina.- The diameter of the crystalline lens is 9 mm. average power of adult lens is +20 D.- It has two surfaces, i.e. anterior and posterior.- The anterior surface is less convex than the posterior surface
Correct Answer. c
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 28/85
(50). Themost common side effect associated with carbonic anhydrase inhibitor is:
a. Renal colic
b. Nervousness
c. Numbness and tingling of fingers and toes
d. Nausea
Solution. (c) Numbness and tingling of fingers and toesRef– Read the text belowSol:- Carbonic anhydrase inhibitor, e.g. acetazolamide is a very potent antiglaucoma drug. It can reduce IOP by 40-60 percent.- It has multiple side effects, the most common being paresthesiae. Other side effects include hypokalemia.
Correct Answer. c
(51). Investigation of optic nerve damage is:
a. Pachometry
b. Fluorescein angiography
c. Perimetery
d. Siedel’s test
Solution. (c) PerimeteryRef– Read the text belowSol:- Perimetery is a useful tool to detect visual field changes and it is also useful in the management of glaucoma.
Correct Answer. c
(52). A patient presents with bilateral sixth nerve palsy. Where is the most likely location of nerve compression?
a. The pons at the level of the abducens nuclei
b. The cerebello-pontine angle
c. The cavernous sinus
d. The clivus
Solution. (d) The clivusRef:Kanski - 822Sol:The most common cause of a bilateralsixth nerve palsy is raised intracranial pressure.- The sixth nerve travels through the subarachnoid space where it ascends the clivus and enters the cavernous sinus.- Within the subarachnoid space, the sixth nerve can be stretched against the clivus as the brain stem herniates through the foramenmagnum due to increased intracranial pressure, which can cause a bilateral sixth nerve palsy
Correct Answer. d
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 29/85
(53). Which genus of organism is most commonly isolated in bleb-associated endophthalmitis:
a. Neisseria
b. Propionibacterium
c. Staphylococcus
d. Streptococcus
Solution. (d) StreptococcusRef:Read the text belowSol:- Acute bleb-associated endophthalmitis can occur at any time following successful filtration surgery.- Pneumococcus (Streptococcus pneumoniae) and Haemophilus influenzae are the most frequent pathogens
Correct Answer. d
(54). A 22-year-old adult with mental handicap, short stature and brachydactyly is referred by his optician with deteriorating visual acuity. Younote bilateral ant dislocated lenses. What other lens anomaly might you anticipate?
a. Anterior lenticonus
b. Posterior lenticonus
c. Microspherophakia
d. Posterior polar cataract
Solution. (c) MicrospherophakiaRef:Kanski - 367Sol:The clinical features are in keeping with Weill-Marchesani, which is a rare AD (or AR) inherited disorder.Features of Weill-Marchesani include:Systemicshort staturebrachydactylystiff jointsmental handicapOcularEctopia lentisspherophakia or microspherophakiaangle anomalypre-senile vitreous liquefaction
Correct Answer. c
(55). Acquired causes of canalicular obstruction include all except
a. Weakness of the lacrimal pump
b. Herpes simplex infection
c. Stevens-Johnson syndrome
d. topical idoxuridine
Solution. (a) Weakness of the lacrimal pumpRef:Read the text belowSol:- The canaliculi remain patent in lacrimal pump failure.
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 30/85
(56). 30 minutes following instillation of a drop into the normal eye of an emmetropic 20-year-old , there is mydriasis, and the near point ofaccommodation is 10 cm.The drop could be:
a. Phenylephrine
b. Guanethidine
c. Physostigmine
d. Cyclopentolate
Solution. (a) PhenylephrineRef:Read the text belowSol:- Mydriasis results from either sympathetic stimulation or parasympathic blockade.- The near point of accommodation given is normal for a 20-year –old and indicates that the parasympathetic stimulation toaccommodation has not been blocked.
Correct Answer. a
(57). Cavernous haemangioma
a. Is the most common primary orbital tumour
b. Presents as acute proptosis
c. Presents in childhood
d. Is usually situated outside the muscle cone
Solution. (a) Is the most commonprimary orbital tumourRef:Alberts Principles and Practice of Ophthalmology-3029Sol:- It causes slowly progressive axial proptosis seen in young adult and middle –aged patients.- It is seen within the cone, usually inferior or lateral to the optic nerve.
Correct Answer. a
(58). What vitamin is most critical for the photoreceptor response to light?
a. A
b. B
c. C
d. E
Solution. a) ARef:Read the text belowSol:- 1 1 -cis-retinal is a vitamin A derivative.- Vitamins C and E play antioxidant roles in the retina but do not participate in the light response of the retina
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 31/85
(59). The following is typical of occipital cortex lesions;
a. Incongruous field defects
b. Macular sparing
c. Relative afferent pupil defect
d. Abnormal saccadic eye movements
Solution. (b) Macular sparingRef:Kanski-812Sol:- Incongruous field defects suggests an optic tract or lateral geniculate lesion.- Pupil response is normal in occipital lesions.- Abnormal saccadic eye movements occur in frontal cortex lesions. Parieto-occipital lesions cause abnormal pursuit movements.
Correct Answer. b
(60). In benign intracranial hypertension all are two except;
a. No visual symptoms occur.
b. Optic disc swelling occurs
c. Diplopia occurs.
d. CT brain scan is normal.
Solution. -NA-
Correct Answer. a
(61). The following are features of dorsal midbrain syndrome;
a. Adie pupil
b. Disturbance of vertical gaze
c. Third cranial nerve palsy
d. Optic nerve pallor
Solution. (b) Disturbance of vertical gazeRef:Wills eye Manual, - 246Sol:- There is near-light dissociation of pupil reactions.- Saccadic vertical gaze is typically involved earlier in disease than pursuit gaze.- The third cranial nerve nucleus is in the ventral midbrain and is uninvolved.- Optic nerve is normal.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 32/85
(62). What are the main contributors to the innervation of the cornea?
a. Short anterior ciliary nerves
b. Long anterior ciliary nerves
c. Short posterior ciliary nerves
d. Long posterior ciliary nerves
Solution. (d) Long posterior ciliary nervesRef: Alberts Principles and Practice of Ophthalmology- 430Sol:- Innervation to the cornea is via the first branch of the trigeminal nerve.- Approximately 70 to 80 branches of the long posterior ciliary nerves enter the cornea peripherally after losing their myelin sheath 1 to 2mm before the limbus.
Correct Answer. d
(63). Which is the difference in light sensitivity of the rods compared with the cones?
a. Equal in sensitivity
b. 10 times more sensitive
c. 1000 times more sensitive
d. 10,000 times more sensitive
Solution. (c) 1000 times more sensitiveRef:Read the text belowSol:- The rods are 100 to 1000 times more sensitive to light than the cones, allowing better vision in dim light.- At this luminance level, the cones are not triggered; therefore, the world appears as shades of grey.- Fine resolution of detailed is hampered in this lighting condition because the rods are not concentrated in the fovea like the cones.- The highest concentration of the rods is actually 20 deg. from the fovea
Correct Answer. c
(64). Within which bony structures is the nasolacrimal sac located?
a. Lacrimal, ethmoid
b. Maxillary, ethmoid
c. Nasal, lacrimal
d. Lacrimal, maxillary
Solution. (d) Lacrimal, maxillaryRef: Kanski- 151Sol:- The lacrimal sac fossa is bordered by the anterior lacrimal crest of the maxillary bone and the posterior lacrimal crest of the lacrimalbone.- In a DCR , the stony is created at the Maxillolacrimal suture line located in the lacrimal sac fossa.
Correct Answer. d
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 33/85
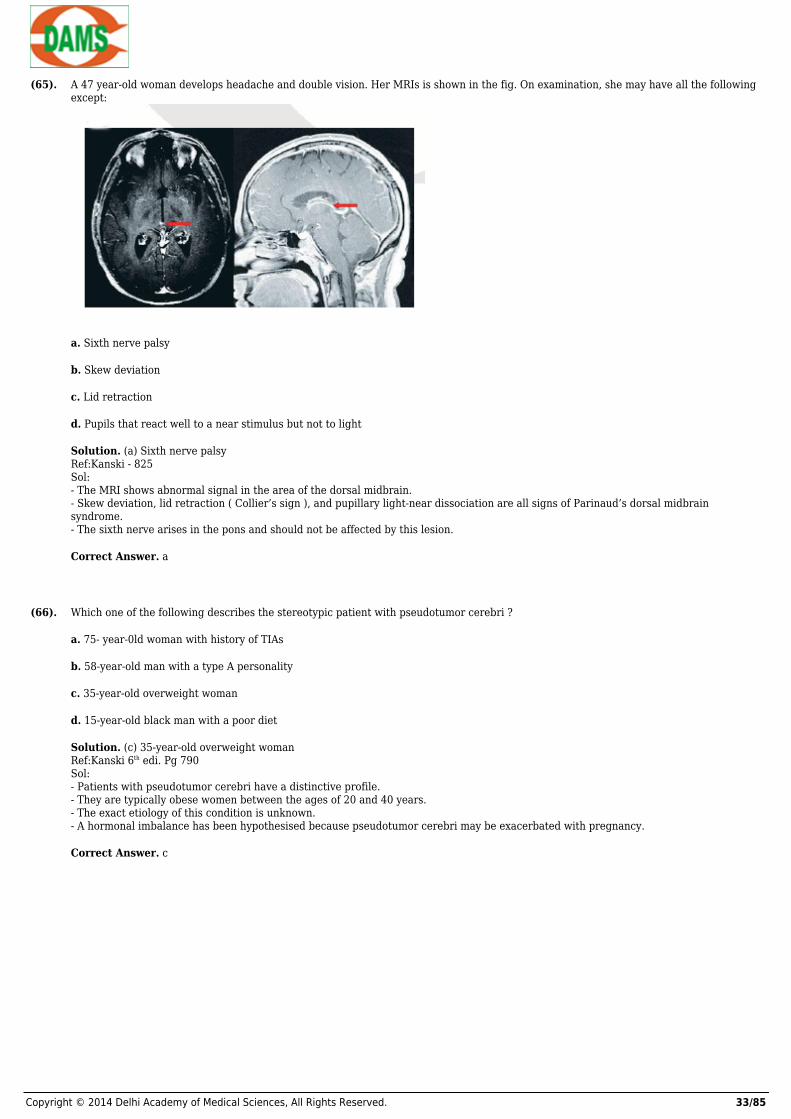
(65). A 47 year-old woman develops headache and double vision. Her MRIs is shown in the fig. On examination, she may have all the followingexcept:
a. Sixth nerve palsy
b. Skew deviation
c. Lid retraction
d. Pupils that react well to a near stimulus but not to light
Solution. (a) Sixth nerve palsyRef:Kanski - 825Sol:- The MRI shows abnormal signal in the area of the dorsal midbrain.- Skew deviation, lid retraction ( Collier’s sign ), and pupillary light-near dissociation are all signs of Parinaud’s dorsal midbrainsyndrome.- The sixth nerve arises in the pons and should not be affected by this lesion.
Correct Answer. a
(66). Which one of the following describes the stereotypic patient with pseudotumor cerebri ?
a. 75- year-0ld woman with history of TIAs
b. 58-year-old man with a type A personality
c. 35-year-old overweight woman
d. 15-year-old black man with a poor diet
Solution. (c) 35-year-old overweight womanRef:Kanski 6th edi. Pg 790Sol:- Patients with pseudotumor cerebri have a distinctive profile.- They are typically obese women between the ages of 20 and 40 years.- The exact etiology of this condition is unknown.- A hormonal imbalance has been hypothesised because pseudotumor cerebri may be exacerbated with pregnancy.
Correct Answer. c
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 34/85
(67). Which of the following signs would not be expected with a classic migraine?
a. Premonitory aura
b. Scintillating lights
c. Headache
d. Persistent leg tingling and weakness
Solution. (d) Persistent leg tingling and weaknessRef:Kanski- 833Sol:- The classic migraine has several components; a preceding aura, expanding scintillating scotoma, and throbbing headache.- Neurologic deficits are not usually found, which may suggest alternate causes, such as a complex migraine, TIA, or stroke.
Correct Answer. d
(68). Which one of the following is not involved with vertical eye movements?
a. Frontal eye fields
b. Paramediian pontine reticular formation
c. Interstitial nucleus of Cajal
d. Trochlear nucleus
Solution. (b) Paramediian pontine reticular formationRef:Wills eye Manual- 267Sol:- The supra nuclear control of vertical saccades originates in the frontal eye fields or in the superior colliculus. They project to neutronsin the rostral interstitial nucleus of.- The medical longitudinal fascicles ( riMLF ) and on to the nuclei of cranial nerve III and IV .- The interstitial nucleus of Cajal is involved with vertical pursuit control.- The Paramedian pontine reticular formation (PPRF ) controls horizontal eye movements
Correct Answer. b
(69). Neuroblastoma is characterized by all of the following except;
a. Metastasis from the adrenal gland
b. Possible spontaneous regression
c. Poor prognosis if diagnosed before 1 year of age
d. Periorbital ecchymosis
Solution. (c) Poor prognosis if diagnosed before 1 year of ageRef:Kanski -921Sol:- Neuroblastoma is the most frequent source of orbital metastasis in children.- Metastases occur from adrenals, mediastinum, and neck. Approximately 20% of all neuroblastoma patients exhibit ocular involvement,which can be the initial manifestation of the tumour.- The mean age of presentation in orbital neuroblastoma metastasis is about 2 years.- Their prognosis is very poor in general, but prognosis is considerably better in infants under 1 year of age.- Spontaneous regression of this tumour may be seen in rare instances.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 35/85
(70). Patient with clinically significant diabetic macular edema with non progressive diabetic retinopathy was treated with macular gridphotocoagulation. The pt still has the following condition given in Fig. What is the preferred treatment?
a. Intravitreal bevacizumab
b. Pars plana vitrectomy
c. Repeat macular grid photocog
d. Augmented macula photocog
Solution. (b) Pars plana vitrectomyRef:Alberts Principles and Practice of Ophthalmology- 1807Sol:- The treatment of vitreo macular traction and thick taut posterior hyaloids is ppv
Correct Answer. b
(71). Aqueous humour is produced at the rate of:
a. 0.45uI/minute
b. 1.0 u1/minute
c. 1.5 u1/minute
d. 2.0 u1/minute
Solution. (d) 2.0 u1/minuteRef– Read the text belowSol:- Aqueous humour is produced from the plasma within the capillary network of the ciliary process of the pars plana at the rate of 2.0u1/minute.
Correct Answer. d
(72). Reticular retinoschisis is splitting of retina between:
a. Outer plexiform and inner nuclear layer
b. Nerve fiber layer and ganglion cell layer
c. Ganglion cell layer and inner plexiform layer
d. Inner plexiform layer and outer nuclear layer
Solution. (b) Nerve fiber layer and ganglion cell layerRef– Read the text belowSol:- Reticular relinoschisis is the splitting of retina at the level of nerve fiber layer.- This is a bilateral condition, generally involving the inferotemporal periphery of both fundii.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 36/85
(73). Flame-shaped haemorrhages occurs at the level of
a. Outer nuclear layer
b. Outer plexiform layer
c. Inner plexiform layer
d. Nerve fiber layer
Solution. (d) Nerve fiber layerRef– Read the text belowSol:- Flame-shaped haemorrhages are superficial; while the dot and blot haemorrhages are present in the deeper layers of retina.
Correct Answer. d
(74). Most common cause of visual loss in background diabetic retinopathy is:
a. Retinal haemorrhage.
b. Preretinal haemorrhage
c. Maculopathy..
d. Vascular dilatation.
Solution. (c) Maculopathy.Ref– Read the text belowSol:- Unless the macula is involved, there is no visual loss in a patient of background diabetic retinopathy.
Correct Answer. c
(75). The eye has reached about two-thirds of what will be its adult size by the age of:
a. 1 years
b. 2 year
c. 6 months
d. 4 months
Solution. (c) 6 monthsRef– Read the text belowSol:- During the first three to six months, the retina is fairly well-developed, and babies can visualize small objects. Depth perception alsodevelops. By six months of age, the eye has reached about two-thirds of what will be its adult size. At this stage, the two eyes are mostlikely working together.- The result is good binocular, or two-eyed, vision. It is during the first year of life that the eyes' greatest physical development occurs.- A child's clarity of vision (visual acuity) has usually developed to 20/20 by the time the child reaches six months of age. At this time,babies achieve fairly precise eye movement control. At ages eight to 12 months, babies are judging distances well.
Correct Answer. c
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 37/85
(76). Degenerative myopia, also known as malignant, pathological, or progressive myopia, is characterized by:
a. Anterior staphyloma
b. Low refractive error
c. Subnormal visual acuity after correction
d. None.
Solution. (c) Subnormal visual acuity after correctionRef– Read the text belowSol:- Degenerative myopia, also known as malignant, pathological, or progressive myopia, is characterized by marked fundus changes, suchas posterior staphyloma, and associated with a high refractive error and subnormal visual acuity after correction.- This form of myopia gets progressively worse over time. Degenerative myopia has been reported as one of the main causes of visualimpairment
Correct Answer. c
(77). Earliest visual rehabilitation occurs in which of the following surgery?
a. Intracapsular cataract extraction
b. Extracapsular cataract extraction
c. Phacoemulsification
d. Argon laser photocoagulation
Solution. (c) PhacoemulsificationRef– Read the text belowSol:- The main advantage of phacoemulsification procedure is shorter convalescence period due to a rapid wound healing and earlystabilization of the refractive error.
Correct Answer. c
(78). To do gonioscopy perioperatively which of the following goniolens should be used?
a. Goldmann
b. Zeiss
c. Koepp’s
d. None
Solution. (c) Koepp’sRef– Read the text belowSol:- Koeppe’s and Barkan’s goniolens are the direct goniolens which do not require a slit lamp.- Goldmann and Zeiss are indirect goniolens which require a slit lamp.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 38/85
(79). When viewing the gonioscopic angle; the usual order in which structures are seen, starting from the cornea are:
a. Iris process, scleral spur, schwalbe’s line, trabecular meshwork
b. Scleral spur, iris process, trabecular meshwork, Schwalbe’s line
c. Schwalbe’s line, trabecular meshwork, scleral spur, iris process
d. Schwalbe’s line, trabecular meshwork, iris process, scleral spur
Solution. (c) Schwalbe’s line, trabecular meshwork, scleral spur, iris processRef– Read the text belowSol:
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 39/85
(80). Thenormal degree of anterior chamber angle is:
a. 15-25°
b. 25-35°
c. 35-45°
d. 45-55°
Solution. (c) 35-450°Ref– Read the text belowSol
Correct Answer. c
(81). Theapplanation tonometer is based on:
a. Lincoff’s law
b. Stoke’s law
c. Imbert-Fick’s law
d. Boyle’s law
Solution. (c) Imbert-Fick’s lawRef– Read the text belowSol:- Applanation tonometer is based on imbert-Fick’s law, which states that for an ideal, dry, thin-walled sphere, the pressure inside thesphere(P) equals the force necessary to flatten its surface (F) divided by the area of flattening (A) i.e. P=F/A.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 40/85
(82). Three weeks following IOL implantation,a patient complains of diminished vision,on fundus fluorescent angiography flower petalhyperfluorescence of macula is noted. Most likely diagnosis is-
a. CME
b. Central serous retinopathy
c. Macular dystrophy
d. ARMD
Solution. (a) CMERef:Read the text belowSol :- Flower petal pattern in the FFA is diagnostic of cystoid macular edema and is a known complication after cataract surgery.- FFA finding in CSR: Smoke-stack pattern and Enlarging Ink-blot pattern
Correct Answer. a
(83). White uveitis is seen in-
a. Sarcoidosis
b. VKH
c. JRA
d. Pars planitis
Solution. (c) JRARef:Read the text belowSol :- Sarcoid has Koeppe and Busaca nodule- VKH has sunset glow fundus with Dalen Fuchs nodules- Pars planitis has snowballs and snowflakes
Correct Answer. c
(84). In Trachoma intense inflammation stage, % of vessels which should be blanched are :
a. 10%
b. 20%
c. 40%
d. 50%
Solution. (d) 50%Ref:Read the text belowSol :FISTO – WHO classification for Trachoma- 1% tetracycline is used for the treatment .- The drug of choice for treatment and also for blanket therapy is now azithromycin .dose: 1gm for adults and in children it is 20mg/kg .- It is a single dose therapy given weekly for 3 weeks.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 41/85
(85). Ciliary staphyloma can occur in :
a. Corneal ulcer
b. Myopia
c. Scleritis
d. Trauma at limbus
Solution. (c) ScleritisRef:Read the text belowSol :- Staphyloma is an ectatic condition of the eyeball with herniation of the uveal tissue.- Posterior staphyloma is a feature of : Pathological myopia.- Corneal ulcer – Anterior staphyloma- Trauma at limbus – Intercalary Staphyloma
Correct Answer. c
(86). Treatment of choice for ptosis with Marcus Gunn jaw winking phenomenon is:
a. Farsanella-Servat operation
b. LPS resection
c. Unilateral frontalis sling operation
d. Bilateral frontalis sling operation
Solution. (d) Bilateral frontalis sling operationRef: Read the text belowSol :- If we do a LPS resection, the jaw-winking phenomena will increase. If we do a unilateral sling surgery there will be an asymmetrical lidlag.- The best operation would be bilateral LPS disinsertion (thereby ablating the LPS action) and a bilateral sling surgery.
Correct Answer. d
(87). Conjunctival ulcer is seen in :
a. Embedded foreign body
b. Tuberculous lesion
c. Syphilitic lesion
d. Sarcoidosis
Solution. (d) SarcoidosisRef: Read the text belowSol :- Sarcoidosis may infrequently involve the conjunctiva causing an ulcer.- It presents as a nodular, translucent lesion, orange in colour, usually located in the folds of the lower fornix.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 42/85
(88). Uhthoff’s sign is seen in:
a. Diabetic retinopathy
b. Demyelinating optic neuritis
c. Craniopharyngioma
d. Diabetes insipidus
Solution. (b) Demyelinating optic neuritisRef.:Read the text belowSol :- Uhthoff’s phenomenon is seen in demyelinating disease in which there is an impairment of vision with increased body temperature.
Correct Answer. b
(89). Anomaloscope is used to detect :
a. Squint
b. Retinopathy
c. Congenital glaucoma
d. Color blindness
Solution. (d) Color blindnessRef.:Read the text belowSol :- An anomaloscope is based on a color match. Two different light sources have to be matched to the same color. On one side you have ayellow color which can be adjusted in brightness. The other side consists of a red and a green light whereas the proportion of mixture isvariable.- As every color on a computer display is made up from the three base colors red, green, and blue, an anomaloscope can’t really bereproduced online. So this red-green color blindness test is just a simple reproduction with room for improvement
Correct Answer. d
(90). Leber’s optic neuropathy has the following features except:
a. It commonly affects healthy males
b. It causes uniocular, sudden painless, progressive and permanent visual loss
c. Pupillary reflexes are affected early in the disease
d. Typical visual field defects are centrocaecal which eventually become absolute
Solution. (c) Pupillary reflexes are affected early in the diseaseRef.:Read the text belowSol :- In Leber’s optic neuropathy the papillary light reactions frequently remain fairly brisk despite severe visual loss.- It commonly affects healthy males- It causes uniocular, sudden painless, progressive and permanent visual loss- Typical visual field defects are centrocaecal which eventually become absolute
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 43/85
(91). Papilloedema has all the following characteristic except :
a. Marked loss of vision
b. Blurring of disc margins
c. Hyperemia of disc
d. Field defect
Solution. (a) Marked loss of visionRef.:Read the text belowSol :- Visual acuity in papilloedema is usually normal unless the fovea is involved with haemorrhage, exudates or edema.
Correct Answer. a
(92). Causes of drug induced optic neuropathy are all except :
a. Ethambutol
b. INH
c. Cloramphenicol
d. Rifampicin
Solution. (d) RifampicinRef.: Read the text belowSol :DRUG INDUCED OPTIC NEUROPATHY- Ethambutol- INH- Cloramphenicol- Rifampicin- Streptomycin.
Correct Answer. d
(93). “Pie in the floor” field defects are seen in:
a. Optic tract lesions
b. Lateral geniculate lesions
c. Temporal lobe lesions
d. Parietal lobe lesions
Solution. (d) Parietal lobe lesionsRef.:Read the text belowSol :- If the superior fibers of the optic radiations are involved, an inferior quadrantic hemianopia is produced called “Pie in the Floor”.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 44/85
(94). Mayer’s loop representsthe :
a. Optic tract lesions
b. Lateral geniculate lesions
c. Temporal lobe lesions
d. Parietal lobe lesions
Solution. (c) Temporal lobe lesionsRef.:Read the text belowSol :
Correct Answer. c
(95). Proptosis can also be defined a reading than how many mm from the lateral orbital rim to the corneal apex?
a. 18 mm
b. 19 mm
c. 20 mm
d. 21 mm
Solution. (d) 21Ref.:Read the text belowSol :Proptosis is graded as- Mild (21-23 mm)- Moderate (24-27 mm)- Severe 28 mm or more
Correct Answer. d
(96). Most common cause of carotid – cavernous fistula is:
a. Trauma
b. Idiopathic
c. Congenital
d. Endocrine cause
Solution. (a) TraumaRef.:Read the text belowSol :- Trauma accounts for 75 percent of cases, while idiopathic cause is seen in 25 percent of cases.
Correct Answer. a

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 45/85
(97). Most common primary orbital tumor in adults producing proptosis is:
a. Neurofibroma
b. Osteoma
c. meningioma
d. Cavernous hemangioma
Solution. (d) Cavernous hemangiomaRef.:Read the text belowSol :- Cavernous hemangioma is a type of blood vessel malformation (hemangioma) that has relatively large blood-filled spaces (cavities).- Cavernous hemangiomas do not contain tissue of the organ in which they are situated.- They can arise virtually anywhere in the body and are considered to be benign neoplasms. Unlike the capillary hemangiomas, they canbe disfiguring and do not tend to regress. They may also lead to spontaneous or traumatic bleeding and ulcerations.
Correct Answer. d
(98). All are true about brawny scleritis except :
a. Shows pitting on pressure
b. Encircles the cornea
c. Requently passes beyond the equator
d. Shows a diffuse inflammation
e. Appears gelatinous
Solution. (c) Requently passes beyond the equatorRef.:Read the text belowSol :BRAWNY SCLERITIS- This inflammation involves the entire anterior sclera.- There is a distortion of pattern of vascular plexuses, i.e. loss of the normal radial pattern.- Shows pitting on pressure- Encircles the cornea- Shows a diffuse inflammation- Appears gelatinous
Correct Answer. c
(99). The treatment of anterior non-necrotizing scleritis is:
a. Local nonsteroidal anti-inflammatory drugs
b. Systemic tablet indomethacin
c. Local steroid drops
d. Systemic steroids
Solution. (b) Systemic tablet indomethacinRef.:Read the text belowSol :ANTERIOR NON-NECROTIZING SCLERITIS TREATMENT- NSAIDS Oral non-steroidal anti-inflammatory drugs (NSAIDs) are the first-line agent for mild-to-moderate scleritis. These consist ofnon-selective or selective cyclo-oxygenase inhibitors (COX inhibitors). Non-selective COX-inhibitors such as flurbiprofen, indomethacinand ibuprofen may be used. Indomethacin 50mg three times a day or 600mg of ibuprofen three times a day may be used.- Corticosteroids Topical corticosteroids may reduce ocular inflammation but treatment is generally systemic. Corticosteroids may beused in patients unresponsive to COX-inhibitors or those with posterior or necrotizing disease.- Immunomodulatory agentsIf the disease is inadequately controlled on corticosteroids, immunomodulatory therapy may be necessary.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 46/85
(100). Pharmacological testing of Horner’s syndrome includes :
a. Testing by cocaine
b. Hydroxyamphetamine test
c. Neostigmine test
d. All of the above
Solution. (d) All of the above.Ref.:Read the text belowSol :- Tests (A) and (B) are used to test the miotic pupil.- Both coaine 4 percent and hydroxyl-amphetamine 1 percent (Paredrine) are indirect sympathominetic drugs.- Cocaine 4 percent eyedrops when instilled in normal eye will dilate the normal pupil but not the Homer’s pupil.- While paredrine will dilate the pupil in preganglionic lesions but not in postganglionic lesions, (as this drugs acts by entering thevesicular space and causing the noradrenalin e to be released in the synaptic cleft.
Correct Answer. d
(101). Which form of uveitis is most common in ocular sarcoidosis?
a. Panuveitis
b. Intermediate uveitis
c. Anterior uveitis
d. Choroiditis
Solution. (A) PanuveitisRef:Wills eye Manual- 372Sol:- Two-thirds of patients with sarcoid uveitis have anterior uveitis.- Two forms of anterior uveitis exist.- One is chronic, recurrent anterior uveitis that is difficult to treat and control with corticosteroids.- The other is an acute granulomatous iridocyclitis that responds well to corticosteroid therapy.
Correct Answer. a
(102). Schwart’z syndrome is caused by;
a. Retinal pigment epithelial cells blocking the trabecular meshwork
b. Forward rotation of the lens-iris diaphragm
c. Ciliary body and choroidal adema
d. Photoreceptor outer segments blocking the trabecular meshwork
Solution. (d) Photoreceptor outer segments blocking the trabecular meshworkRef:Kanski - 701Sol:- Schwartz syndrome is high IOP associated with a rhegmatogenous retnal detachment.- Photoreceptor outer segments migrate transvitreally into the aqueous, block the trabecular outflow pathways, and result in IOPelevation.
Correct Answer. d
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 47/85
(103). What cell type is found in an aqueous specimen in ocular toxocariasis?
a. Eosinophils
b. T lymphocytes
c. Macrophages.
d. Polymorphonuclear neutrophils
Solution. (a) EosinophilsRef:Read the text belowSol:- An eosinophilic granuloma occurs with Toxocara intraocular infection.- On histopathology, the reaction may be so vigrous that the Toxocara organism may not be visible.
Correct Answer. a
(104). What is the predominant cause for damage to ocular structures from infection by onchocerca
a. Infiltration of retinal tissue
b. Obstruction of the trabecular meshwork
c. Toxins produced by the larvae
d. Inflammatory reaction to dead microfilaria
Solution. (d) Inflammatory reaction to dead microfilariaRef: Wills eye Manual- 365Sol:- Onchocerca volvulus infection results in widespread dissemination of the microfilarial larvae.- These microfilarial can be seen swimming in the anterior chamber.- The live organisms may cause a mild uveitis and obstruct the trabecular meshwork; however, dead organisms incite a vigorousinflammatory reaction, which causes much more ocular damage.
Correct Answer. d
(105). Compared with plasma, aqueous humour has an increased concentration of which one of these components?
a. Protein
b. Ascorbate
c. Glucose
d. Carbon dioxide
Solution. (b) AscorbateRef:Glaucoma Medical Diagnosis and Therapy- 40Sol:- Compared with plasma, aqueous is slightly hypertonic and acidic.- Aqueous has a marked excess of ascorbate ( 15 times greater than that of arterial plasma ) and a marked deficit of protein (0.2% inaqueous as compared to 7% in plasma ).
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 48/85
(106). Which one of the following statements is false for pseudoexfoliation glaucoma
a. It has a worse prognosis than primary open angle glaucoma ( POAG )
b. It may be monocular or binocular
c. Lens extraction alleviates the condition
d. The IOP is often higher than POAG
Solution. (c) Lens extraction alleviates the condition.Ref:Kanski - 397Sol:- PXF is an age related disease involving an accumulation of abnormal fibrillar extracellular material within ocular and systemic tissues.- Glaucoma occurs more commonly in eyes with PXF than in those without it.- In fact PXF has been recognized as the most common identifiable cause of glaucoma.- The glaucoma is a secondary open angle glaucoma and can be unilateral or bilateral. IOPs can be quite elevated and are often higherthan in POAG. Glaucoma associated with PXF tends to respond less well to medical therapy than does POAG, to be more difficult to treat,to require surgical intervention more often, and to have a worse overall prognosis.- Unfortunately, lens extraction is not curative, although the pressure may be lowered by few mm of Hg following simple cataractextraction.
Correct Answer. c
(107). Which lesion might lead to development of a macular pucker ( epiretinal membrane ) ?
a. Cobblestone degeneration
b. Retinal hole
c. Choroidal nevus
d. Bone spicule pigmentation
Solution. (b) Retinal holeRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 2315Sol:- In all patients who develop a macular pucker, the peripheral retina needs to be examined carefully to ensure that no retinal tears orholes exist.- The lesions may allow migration of RPE cells, which are thought to be able to transform into fibroblast-like cells, leading to epiretinalmembrane formation.
Correct Answer. b
(108). What percentage of the population will have a cilioretinal artery ?
a. 85%
b. 65%
c. 45%
d. 25%
Solution. (d) 25%Ref:Kanski, 6th edi, pg 566Sol:- In 15% to 25% of patients, a cilioretinal artery may be present to perfuse the macula. Pulsatile flow of blood with each heartbeat may beseen in these arteries.- In the case of a CRAO, the cilioretinal artery may allow preservation of central acuity.- Fluorescein angiography shows the extensive retinal arterial nonperfusion, except in the distribution of the cilioretinal artery in apatient with a CRAO.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 49/85
(109). What ocular complication may result after a central retinal artery occlusion ( CRAO )
a. Corneal edema
b. Staphyloma
c. Rubeosis iris
d. CNVM
Solution. (c) Rubeosis irisRef:Kanski 6th edi. Pg 591Sol:- The incidence of rubeosis may be as high as 15% to 20% after CRAO.- These patients may also develop neonvascularization of the disc and retina.
Correct Answer. c
(110). The CME in which one of the following conditions would have leakage on fluorescein angiography ?
a. Goldmann- Favre
b. Juvenile X-linked retinoschisis
c. Nicotinic acid maculopathy
d. Epiretinal membrane
Solution. (d) Epiretinal membraneRef:Wills eye Manual, 6th edi. Pg 318Sol:- Conditions that may have CME without leakage of fluorescein include Goldmann- Favre, retinitis pigmentosa, and nicotinic acidmaculopathy.- Epiretinal membranes may cause a CME that leaks from traction and distortion of paramacular capillaries.
Correct Answer. d
(111). Exudative detachments occur in all of the following conditions except:
a. Vogt-Koyanagi-Harada Syndrome ( VKH )
b. Myopia
c. Toxemia of pregnancy
d. CMV retinitis
Solution. (b) MyopiaRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 2305Sol:- Although exudative retinal detachments may occur in CMV retinitis, it is very uncommon .- Myopia is not associated with exudative retinal detachments.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 50/85
(112). A copper intraocular foreign body can cause all of the following except ?
a. Sunflower cataract
b. Kayser-Fleischer rings
c. Suppurative endophthalmitis
d. Irreversibly flat ERG
Solution. (d) Irreversibly flat ERGRef:Wills eye Manual, 6th edi. Pg 48Sol:- Intraocular copper foreign bodies may result in two distinct disease processes.- One is a mild form called chalcosis.- The other is a more severe suppurative form of endophthalmitis. The severity of intraocular inflammation is directly proportional to theconcentration of copper within foreign body.- Chalcosis occurs in copper amalgams that contain significant amounts of nickel or other metals.- Chalcosis is characterized by mild intraocular inflammation, development of a sunflower cataract, and Kayser- Fleischer rings.- Characteristically, early removal of the intraocular foreign body in chalcosis can improve the amplitudes of the ERG, which have beensuppressed from the presence of intraocular copper ions.
Correct Answer. d
(113). Which of the following diagnostic studies is indicated in the evaluation of age-related maculardegeneration (AMD) to detect the presenceof choroidal neovascularization (CNV)?
a. Fluorescein angiography
b. Magnetic resonance imaging
c. Corneal topography
d. Computerized axial tomography
Solution. (a) Fluorescein angiographyRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 1677Sol:- Fluorescein angiography is indicated in the evaluation of age-related macular degeneration (AMD) to detect the presence of choroidalneovascularization (CNV).
Correct Answer. a
(114). A patient has synthesis scintillans. Which historical feature is most probable?
a. Previous blunt trauma with hyphema
b. Dense arcues senilis
c. Carotid atherosclerosis with a history of amaurosis
d. Cushingoid appearance from long-term steroid use
Solution. (a) Previous blunt trauma with hyphemaRef:Read the text belowSol:- Synchysis scintillans can be seen in patients after resolution of vitreous haemorrhage.- Refractile, yellow, cholesterol crystals usually float freely in the liquefied vitreous and will settle inferiorly with time.- A systemic hyperilipidemic state is not necessary.
Correct Answer. a
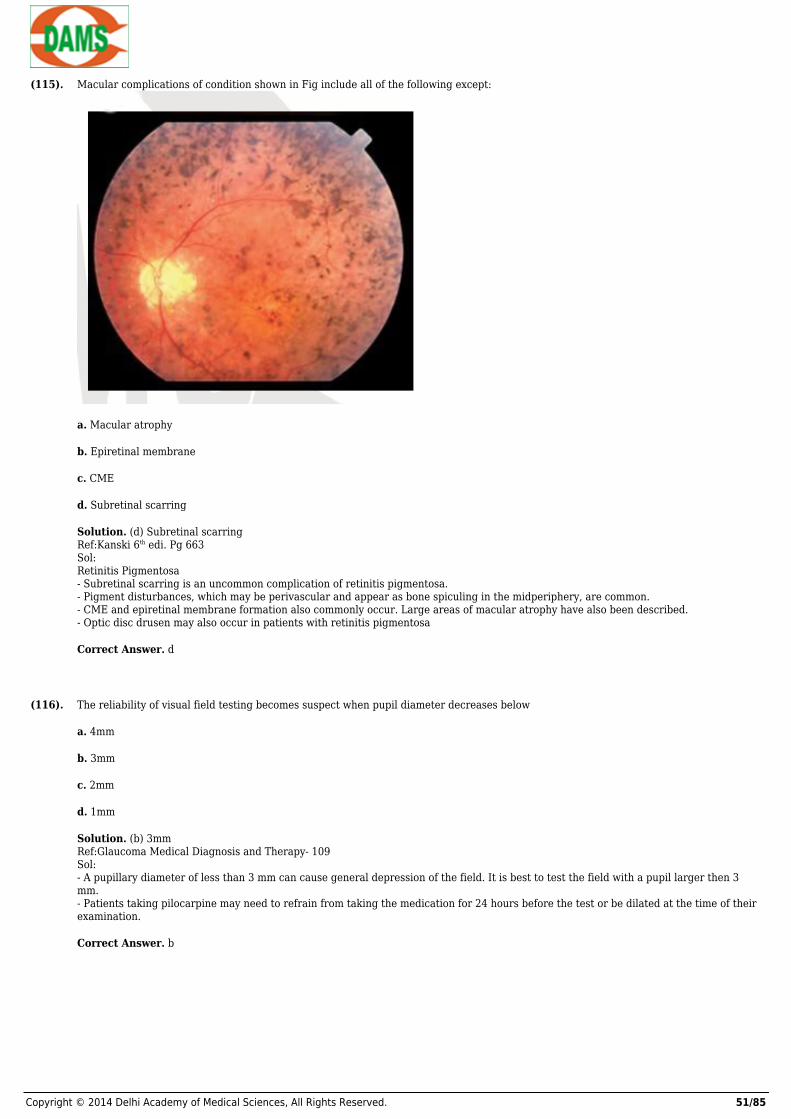
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 51/85
(115). Macular complications of condition shown in Fig include all of the following except:
a. Macular atrophy
b. Epiretinal membrane
c. CME
d. Subretinal scarring
Solution. (d) Subretinal scarringRef:Kanski 6th edi. Pg 663Sol:Retinitis Pigmentosa- Subretinal scarring is an uncommon complication of retinitis pigmentosa.- Pigment disturbances, which may be perivascular and appear as bone spiculing in the midperiphery, are common.- CME and epiretinal membrane formation also commonly occur. Large areas of macular atrophy have also been described.- Optic disc drusen may also occur in patients with retinitis pigmentosa
Correct Answer. d
(116). The reliability of visual field testing becomes suspect when pupil diameter decreases below
a. 4mm
b. 3mm
c. 2mm
d. 1mm
Solution. (b) 3mmRef:Glaucoma Medical Diagnosis and Therapy- 109Sol:- A pupillary diameter of less than 3 mm can cause general depression of the field. It is best to test the field with a pupil larger then 3mm.- Patients taking pilocarpine may need to refrain from taking the medication for 24 hours before the test or be dilated at the time of theirexamination.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 52/85
(117). All of the following conditions areassociated with increased pigmentation of the trabecular meshwork on gonioscopy except:
a. Pseudoexfoliation syndrome (PXF )
b. Pigment dispersion syndrome
c. Prior trauma
d. All of the above
Solution. (d) All of the aboveRef:Kanski -400Sol:- In a young normal eye, it is unusual to see ant trabecular pigment band.- This is because insufficient pigment has filtered through the trabecular meshwork to form a visible pigmented line.- If pigmentation is apparent, it is usually most prominent in the inferior angle.- The two most common conditions in which the pigment band is very prominent are pigment dispersion syndrome / pigmentaryglaucoma and PXF / pseudoexfoliation glaucoma.- Lesser amounts of trabecular pigmentation can be seen in iritis, diabetes, or following intraocular surgery, trauma, or laser.
Correct Answer. d
(118). The following Fig can be present in all of the following conditions except:
a. Oculocutaneous albinism
b. PXF
c. Plateau iris syndrome
d. Pigment dispersion syndrome
Solution. (c) Plateau iris syndromeRef:Wills eye Manual- 222Sol:- These are transillumination defects of iris.- In oculocutaneous albinism there is diffuse transillumination of the iris.- Patients with exfoliation syndrome have peripupilliary transillumination defects.- Peripheral discrete or confluent iris transillimination defects may be seen in pigment dispersion syndrome.- Plateau iris syndrome does not customarily produce transillumination defects
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 53/85
(119). What is the best initial therapy for malignant glaucoma?
a. Pilocarpine 2%
b. Laser iridotomy
c. Mydriatic-cycloplegic therapy
d. Lens removal
Solution. (c) Mydriatic-cycloplegic therapyRef:Glaucoma Medical Diagnosis and Therapy- 406Sol:- Malignant glaucoma, or aqueous misdirection, occurs when aqueous is secreted into and sequestered in the vitreous cavity, pushing thelens, hyaloid face, and iris forward, thus collapsing the anterior chamber and blocking the trabecular meshwork.- The IOP often rises to 20 to 60 mm Hg, and the anterior chamber is shallow both centrally and peripherally.- The common clinical feature include 1) shallow or flat anterior chamber, 2) increased or normal IOP, 3) poor response to miotics, 4)favourable response to cycloplegics-mydriatics.- Mydriatic-cyloplegics help by pulling the lens-iris diaphragm posteriorly.
Correct Answer. c
(120). A10-year-old girl has bulging and blepharoptosis of both upper eyelids and repeated episodes of eyelid inflammation and swelling shownin Fig. What is the most likely diagnosis?
a. Blepharochalasis
b. Dermatochalasis
c. Steatoblepharon
d. Blepharospasm
Solution. (a) BlepharochalasisRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 3267Sol:- Blepharochalasis is a rare inherited condition that occurs more commonly in young females than males and consists of repeated boutsof eyelid inflammation and edema.- Recurrent idiopathic eyelid swelling eventually leads to blepharoptosis secondary to dehiscence or attenuation of the levatoraponeurosis. Anterior bulging of the lacrimal gland or orbital fat may also occur.
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 54/85
(121). Treatment of choice for angular conjunctivitisis
a. Potassium sulphate
b. Salicylic acid
c. Sodium thiosulphate
d. Zinc oxide
Solution. (d) Zinc oxideRef: Readthe text belowSol :- Zinc oxide is rapidly effective in treating angular conjunctivitis by inhibiting the proteolytic fermentation of the bacteria.
Correct Answer. d
(122). Deep leucoma is best treated by :
a. Tattooing
b. Lamellar keratoplasty
c. Keratectomy
d. Penetrating keratoplasty
Solution. (d) Penetrating keratoplastyRef: Read the text belowSol :- Lamellar keratoplasty is done for superficial corneal opacities.
Correct Answer. d
(123). The color of fluorescein staining in corneal ulcer is :
a. Yellow
b. Blue
c. Green
d. Royal blue
Solution. (c) GreenRef: Read the text belowSol :- Fluorescein positive lesions in cornea and conjunctiva appear as green; best seen with cobalt blue filter of the slit-lamp.- Fluorescein dye is an extracellular dye, which stains the tear films and epithelial defects
Correct Answer. c
(124). The syndrome consisting of symmetrical enlargement of lacrimal and salivary glands is :
a. Sjogren’s syndrome
b. Mikulicz’s syndrome
c. Sturge-Weber syndrome
d. Vogt koyonagi Harada syndrome
Solution. (b) Mikulicz’s syndromeRef: Read the text belowSol :- Mikulicz’s syndrome consists of enlargement of lacrimal, parotid, sublingual, buccal, platal and submaxillary gland.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 55/85
(125). Blow-out fracture includes all the following except :
a. Enophthalmos
b. Cheek anesthesia
c. Diplopia
d. Anisokonia
Solution. (d) AnisokoniaRef: Read the text belowSol :- There can be anisokoria due to involvement of pupillomotor postganglionic cholinergic fibres present in the inferior oblique muscle.
Correct Answer. d
(126). In orbital cellulitis, which of the following is false :
a. It is a common cause of proptosis in childhood
b. Commonly seen due to infection spreading from surrounding sinusitis
c. It is commonly bilateral
d. Cavernous sinus thrombosis
Solution. (c) It is commonly bilateralRef: Read the text belowSol :- Orbital cellulitis commonly occurs in children, secondary to sinusitis. It is generally unilateral.- Its four cardinal signs are proptosis, lid swelling, chemosis, impaired extraocular movements.
Correct Answer. c
(127). Most common type of glaucoma in India is:
a. Acute congestive glaucoma
b. Chronic simple glaucoma
c. Lens induced glaucoma
d. Steroid induced glaucoma
Solution. (b) Chronic simple glaucomaRef– Read the text belowSol:- Primary OAG is the commonest form of Glaucoma in Caucasians and Africans
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 56/85
(128). Early signs of infantile glaucoma include all the following except:
a. Epiphora
b. Photophobia
c. Blepharospasm
d. Corneal enlargement
Solution. (d) Corneal enlargementRef– Read the text belowSol:- Congenital glaucoma is caused by a defect in the channel through which aqueous humor normally exits the eye. Because of the constantobstruction of the outflow of aqueous humor, a chronic increase in intraocular pressure develops.- Most cases of congenital glaucoma are inherited in an autosomal recessive pattern.- Infants with this disorder have received two copies of the same defective gene — one from the mother and one from the father.- Those who inherit only one copy of the gene from either parent are carriers of the disease, but they do not develop it themselves.- Corneal enlargement is usually not an early sign of buphthalmos.
Correct Answer. d
(129). In myopia which one of the following is most common?
a. Equatorial staphyloma
b. Posterior staphyloma
c. Ciliary staphyloma
d. Intercalary staphyloma
Solution. (b) Posterior staphylomaRef– Read the text belowSol:DegreeMyopia, which is measured in diopters by the strength or optical power of a corrective lens that focuses distant images on the retina, hasalso been classified by degree or severity:Low myopia usually describes myopia of −3.00 diopters or less (i.e. closer to 0.00).Medium myopia usually describes myopia between −3.00 and −6.00 diopters. Those with moderate amounts of myopia are more likely tohave pigment dispersion syndrome or pigmentary glaucoma.High myopia usually describes myopia of −6.00 or more. People with high myopia are more likely to have retinal detachmentsandprimary open angle glaucoma.- In high myopia, the whole of the posterior pole of the eye may herniated backwards as a posterior staphyloma.- They are also more likely to experience floaters, shadow-like shapes which appear singly or in clusters in the field of vision. Roughly30% of myopes have high myopia
Correct Answer. b
(130). The eye in a newborn child is
a. Hyperope with regular astigmatism
b. Hypermetropic
c. Hypermetropic with irregular astigmatism
d. Myopia
Solution. (b) HypermetropicRef– Read the text belowSol:- At birth a child is born with +2 to +3D hypermetropia without astigmatism, which increases upto the age of 6 years to +4D between 6to 8 years it levels off, then begins to decreases until the early teens.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 57/85
(131). The most sensitive part of the Retina is called:
a. Fusca centralis
b. Fovea centrails
c. Choroidal plexus
d. Optic disc
Solution. (b) Fovea entrailsRef:Read the text belowSol:- Fovea centralis, a depression or pit has only cones in the neuroepithelial layer.- Rods are absent in this region.
Correct Answer. b
(132). Which vascular artery is present in the embryonic ocular fissure?
a. Ophthalmic artery
b. Retinal artery
c. Short posterior ciliary artery
d. Hyaloid artery
Solution. (d) Hyaloid arteryRef– Read the text belowSol:- The hyaloid artery is a branch of the ophthalmic artery, which is itself a branch of the internal carotid artery.It is contained within theoptic stalk of the eye and extends from the optic disc through the vitreous humor to the lens.- Usually fully regressed before birth, its purpose is to supply nutrient to the developing lens in the growing fetus.- During the tenth week of development in humans (time varies depending on species), the lens grows independent of a blood supply andthe hyaloid artery usually regresses. Its proximal portion remains as the central artery of the retina.- Regression of the hyaloid artery leaves a clear central zone through the vitreous called the hyaloid canal or Cloquet's canal.- This embryonic fissure is essential in the development of the eye; as it allows the out growth of axons from ganglion cells forming theoptic nerve and the ingrowths of hyaloids artery which is necessary for the growth and development of the eye.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 58/85
(133). All the following structures develop from the neuroectoderm except.
a. Neurosensory retina
b. Retinal pigment epithelium
c. Episclera
d. Ciliary Body
Solution. (c) EpiscleraRef– Read the text belowSol:Neuroectoderm (or neural ectoderm) is the term for ectoderm which receives BMP-inhibiting signals from proteins such as noggin, whichleads to the development of the nervous system from this tissue.The types of neuroectoderm include:- Neural cresto pigment cells in the skino ganglia of the autonomic nervous systemo dorsal root ganglia.o facial cartilageo spiral septum of developing hearto ciliary body of the eyeo adrenal medulla- Neural tubeo brain (rhombencephalon, mesencephalon and prosencephalon)o spinal cord and motor neuronso retinao posterior pituitary
Correct Answer. c
(134). A patient with good LPS action, ptosis disappears upon instillation of neostigmine. The best operative modality for such kind of patientwill be
a. Farsanella-Servat operation
b. LPS resection
c. Unilateral frontalis sling operation
d. Bilateral frontalis sling operation
Solution. (a) Farsanella-Servat operationRef– Read the text belowSol:- Ptosis due to Horner’s syndrome is treated best with farsanella-Servat operation; in which part of Muller’s muscle, upper part of tarsalplate and palpebral conjunctiva is resected.- The Fasanella-Servat operation is effective for mild to moderate ptosis from a variety of causes and for contour abnormality correctionin patients with little or no ptosis. Despite the long-held belief that excision of the accessory lacrimal glands of Wolfring leads to dry eyesymptoms, our study found this to be the exception.- This procedure has the advantage of high reliability when reasonable preoperative criteria are applied and is minimally invasive
Correct Answer. a
(135). How many long posterior ciliary are present in the eye?
a. 2
b. 3
c. 4
d. 5
Solution. (a) 2Ref– Read the text belowSol:- There are two long posterior ciliary artery which are present at 3 o’clock and 9’ o’clock position.
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 59/85
(136). The sclera is thinnest at
a. Limbus
b. Posterior to the insertion of the Rectii muscle
c. Equator
d. Posterior pole.
Solution. (b) Posterior to the insertion of the Rectii muscleRef– Read the text belowSol:- Posterior to the insertion of the Rectii muscle the sclera is approximately 0.3mm thick; at the limbus it is 0.7mm thick and at theposterior pole it is approximately 1mm thick.
Correct Answer. b
(137). Cystoid macular edema occurs due to a break in:
a. Outer blood-retinal barrier
b. Inner blood-retinal barrier
c. Both of the above
d. None of the above
Solution. (b) Inner blood-retinal barrierRef– Read the text belowSol:- Due to a break in inner blood-retinal barrier, there is increase in vascular permeability of retinal blood in vessels causing cystoidmacular edema.
Correct Answer. b
(138). Chronic use of the following medications has been reported to cause canalicular stenosis except;
a. Echothiophate
b. Idoxuridine
c. Epinephrine
d. Atropine
Solution. (d) AtropineRef:Read the text belowSol:Canalicular stenosis may follow infections (herpetic, trachoma, infectious mononucleosis ) inflammations ( Stevens-Johnson syndrome,ocular pempphogoid ), trauma ( lacerations, chemical or thermal injuries, repeated probings ), allergy, irradiation, tumors( rarely ),canaliculitis, and use of eye drops.- Eye drops, including antivirals, strong miotics, and epinephrine-containing compounds, have been implicated most frequently.Alberts Principles and Practice of Ophthalmology-3210
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 60/85
(139). What is the most common reason for failure of a DCR?
a. Obstruction at the level of common canaliculus or bony stony site
b. Unsuspected lacrimal sac tumor
c. Recurrent infection of the lacrimal sac
d. Dacryoliths ( lacrimal stones)
Solution. (a) Obstruction at the level of common canaliculus or bony stony siteRef:Kanski 6th edi. Pg 160Sol:- The two most common causes of DCR failure are obstruction at the common canaliculus and obstruction at the bony ostomy site.- Recurrent obstruction can result in recurrent infection and dacryolith formation.- Unsuspected tumors may also cause recurrent obstruction but are not the major cause of DCR failure.
Correct Answer. a
(140). A 12-year-old boy involved in a motor vehicle accident 3 months ago presents with a complaint of left-sided epiphora since the accident,along with a 1-week history of fever and progressive swelling, redness, and pain in the left medial canthal region with mucopurulentdischarge from the medial canthus.Appropriate initial work-up of this patient includes all of the following except;
a. A complete ophthalmic exam
b. CT scan of the orbits and sinuses
c. Probing and irrigation of the left nasolacrimal system
d. Culture and Gram stain of the medial cantonal discharge
Solution. (c) Probing and irrigation of the left nasolacrimal systemRef: Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 3503Sol:- In acute dacryocystitis, probing of the nasolacrimal system is not indicated.- Complete ophthalmic evaluation is necessary to determine whether a surrounding orbital cellulitis is present.- Culture and Gram stain may help direct antibiotic therapy. In situations of previous trauma, radiographic imaging will help evaluate anyanatomic changes.
Correct Answer. c
(141). What is the most common cause of unilateral childhood proptosis?
a. Capillary hemangioma
b. Thyroid-related orbitopathy
c. Orbital haemorrhage
d. Orbital cellulitis
Solution. (d) Orbital cellulitisRef:Alberts Principles and Practice of Ophthalmology- 2961Sol:- The most common cause of unilateral childhood proptosis is most often orbital cellulitis, secondary to ethmoid sinusitis or respiratorytract infections.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 61/85
(142). All of the following clinical findings can be associated with Goldenhar’s syndrome except;
a. Eyelid colhbomas
b. Lipodermoids
c. Duane’s syndrome
d. Proptosis
Solution. (d) ProptosisRef:Kanski 6th edi. Pg 66Sol:- Goldenhar’s syndrome involves abnormalities of the first and second branchial arches.- Eyelid colobomas, lipodermoids, and Duane’s syndrome are all part of a large list of clinical findings associated with Goldenhar’s.- Additional findings include microphthalmia, anophthalmia, optic nerve hypoplasia, ocular colobomas, preauricular fistulas and skintags, and palatal and facial clefts.- Proptosis is seen more often with the synostosis, which includes both Crouzon’s and Apert’s syndromes.
Correct Answer. d
(143). Which one of the following regarding megalocornea is true ?
a. Most common inheritance is autosomal dominant.
b. Associated with progressive corneal enlargement.
c. Corneal diameter greater than 10mm.
d. Associated with Down syndrome.
Solution. (d) Associated with Down syndromeRef:Alberts Principles and Practice of Ophthalmology, - 438Sol:- Megalocornea is usually an X-linked, isolated, nonprogressive congenital corneal enalargement with a horizontal corneal diameter ofgreater than 13 mm.- It has been associated with systemic conditions such as Down, Marfan’s, and Alpor’s syndromes, craniosynostosis, and facialhemiatrophy.
Correct Answer. d
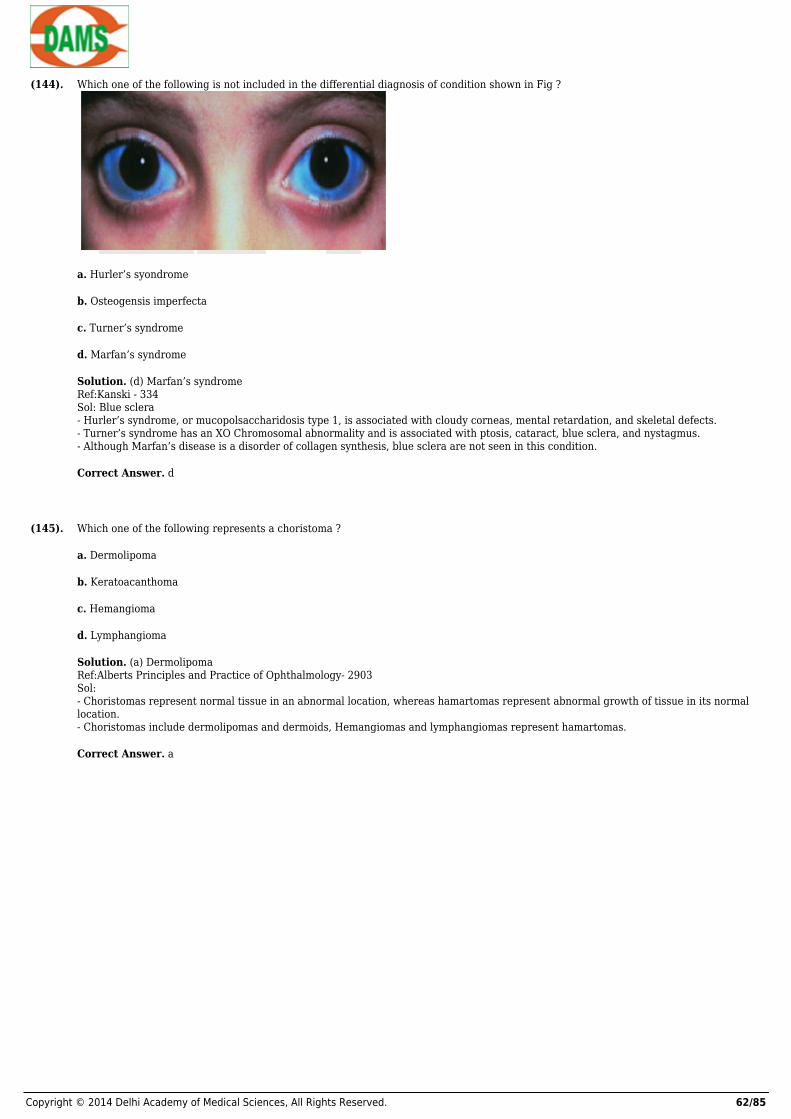
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 62/85
(144). Which one of the following is not included in the differential diagnosis of condition shown in Fig ?
a. Hurler’s syondrome
b. Osteogensis imperfecta
c. Turner’s syndrome
d. Marfan’s syndrome
Solution. (d) Marfan’s syndromeRef:Kanski - 334Sol: Blue sclera- Hurler’s syndrome, or mucopolsaccharidosis type 1, is associated with cloudy corneas, mental retardation, and skeletal defects.- Turner’s syndrome has an XO Chromosomal abnormality and is associated with ptosis, cataract, blue sclera, and nystagmus.- Although Marfan’s disease is a disorder of collagen synthesis, blue sclera are not seen in this condition.
Correct Answer. d
(145). Which one of the following represents a choristoma ?
a. Dermolipoma
b. Keratoacanthoma
c. Hemangioma
d. Lymphangioma
Solution. (a) DermolipomaRef:Alberts Principles and Practice of Ophthalmology- 2903Sol:- Choristomas represent normal tissue in an abnormal location, whereas hamartomas represent abnormal growth of tissue in its normallocation.- Choristomas include dermolipomas and dermoids, Hemangiomas and lymphangiomas represent hamartomas.
Correct Answer. a
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 63/85
(146). Which organism is not a usual commensal found on the lids and lashes ?
a. Moraxella catarrhalis
b. Haemophilus influenzae
c. Propionibacterium acnes
d. Staphylococcus epidermidi
Solution. (b) Haemophilus influenzaeRef:Read the text belowSol:- A number of bacteria are found commonly in the enviroment.- These can be recovered from the eyelashes, and most of the time they do not cause ocular disease. Corynebacterium spp,Staphylococcus epidermidis, Moraxella catarrhalis, and Streptococcus viridians are frequently found.- Gram-negative organisms are not usually found on the ocular surface.- Pathogenic bacteria include Haemophilus influenzae, Pseudomonas aeruginosa, Streptococcus pneumoniae, Staphylococcus aureus,Bacillus subtilise, and Neisseria gonorrhoeae.
Correct Answer. b
(147). all are correct excep regarding pterygium of the eye except
a. Histopathology shows fibrovascular ingrowth just beneath Bowman’s layer
b. A pigmented iron ( ferry’s line ) is found at the corneal edge of the lesion
c. Prolonged UV exposure is a risk factor
d. Recurrence after treatment is rare
Solution. (d) Recurrence after treatment is rareRef:Kanski-242Sol:- Pterygia are wings-shaped folds of conjunctiva and fibrovascular tissue that invade the superficial cornea.- The exact etiology is not known, but a strong casual relationship has been documented with ultraviolet light exposure.- Destruction of Bowman’s layer and changes in corneal astigmatism often occur.- If inflamed, they may become hypertrophic with localized changes of the adjacent cornea, which may include punctate keratopathy andeven dellen formation.- Iron diposition at the leading edge of the pterygium is known as a Stocker’s line.- They may be observed, but excision is often indicated if the visual axis is threatened or if extreme irritation exists. The recurrence rateis significant, with approximately 40% recurring by simple excision.- Conjunctival autograft and amniotic membrane graft may lower recurrence rate according to some studies. Application of mitomycin Cmay also prevent recurrence.- The lesions are rarely malignant, and metastasis would be extremely uncommon.
Correct Answer. d
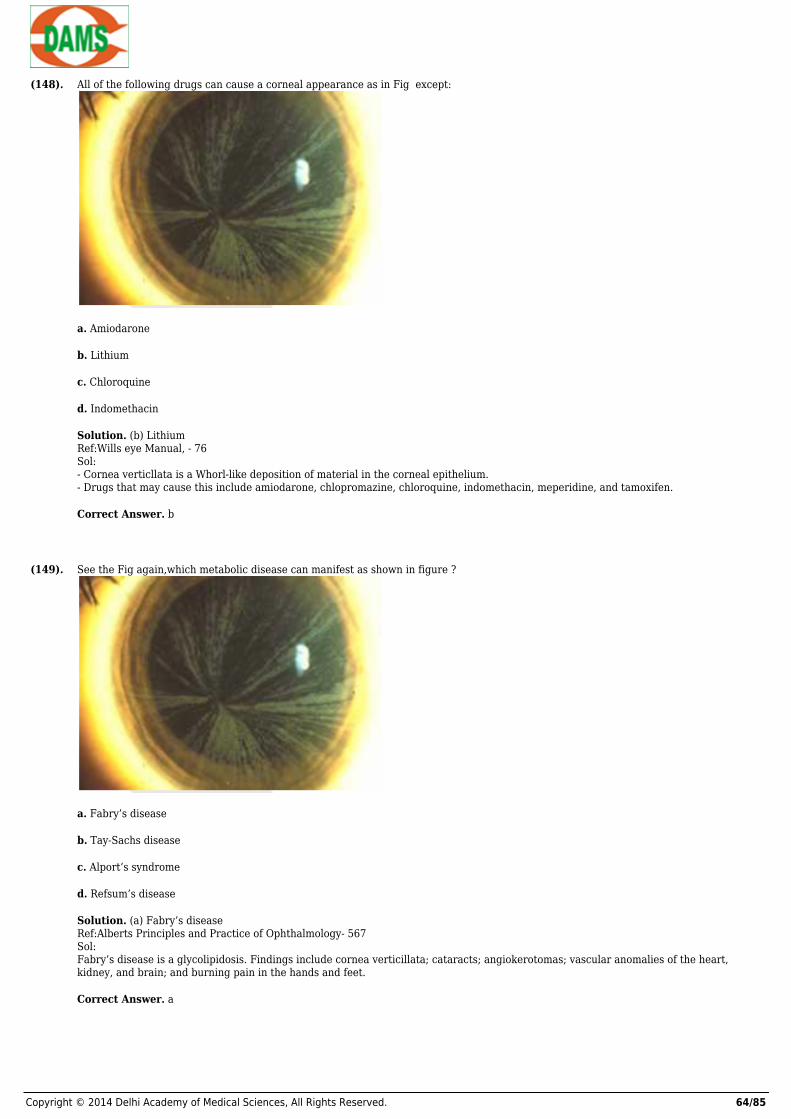
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 64/85
(148). All of the following drugs can cause a corneal appearance as in Fig except:
a. Amiodarone
b. Lithium
c. Chloroquine
d. Indomethacin
Solution. (b) LithiumRef:Wills eye Manual, - 76Sol:- Cornea verticllata is a Whorl-like deposition of material in the corneal epithelium.- Drugs that may cause this include amiodarone, chlopromazine, chloroquine, indomethacin, meperidine, and tamoxifen.
Correct Answer. b
(149). See the Fig again,which metabolic disease can manifest as shown in figure ?
a. Fabry’s disease
b. Tay-Sachs disease
c. Alport’s syndrome
d. Refsum’s disease
Solution. (a) Fabry’s diseaseRef:Alberts Principles and Practice of Ophthalmology- 567Sol:Fabry’s disease is a glycolipidosis. Findings include cornea verticillata; cataracts; angiokerotomas; vascular anomalies of the heart,kidney, and brain; and burning pain in the hands and feet.
Correct Answer. a
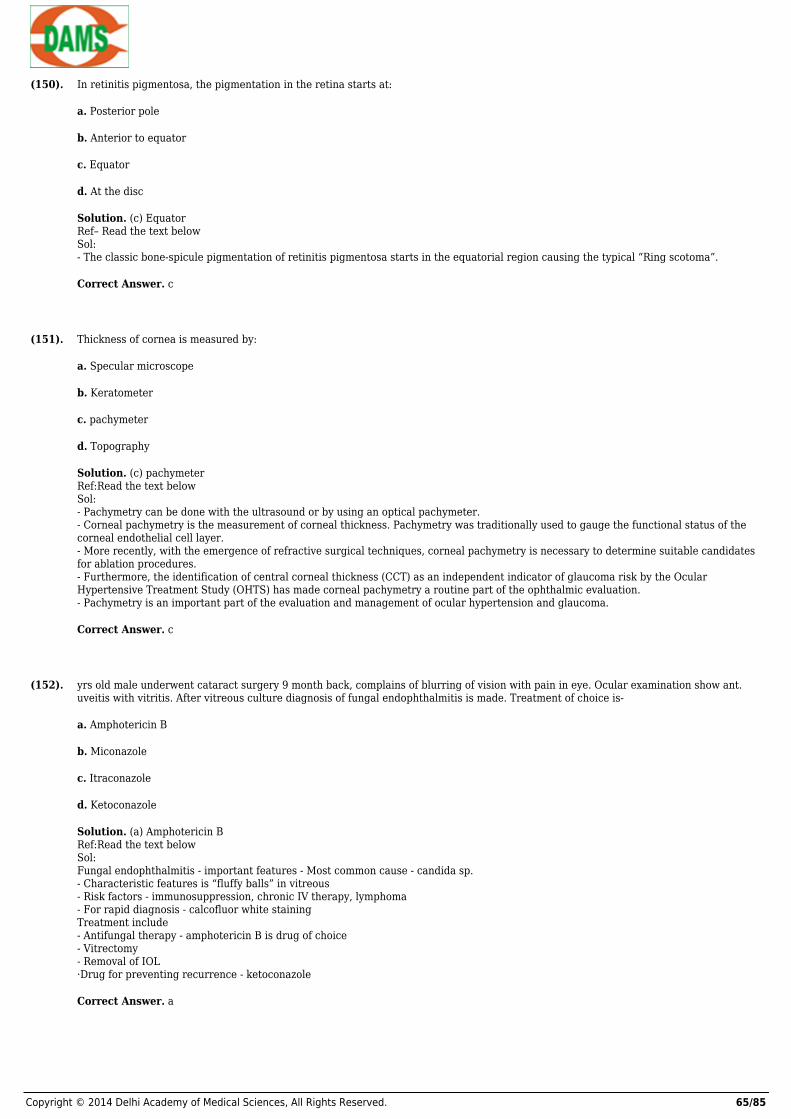
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 65/85
(150). In retinitis pigmentosa, the pigmentation in the retina starts at:
a. Posterior pole
b. Anterior to equator
c. Equator
d. At the disc
Solution. (c) EquatorRef– Read the text belowSol:- The classic bone-spicule pigmentation of retinitis pigmentosa starts in the equatorial region causing the typical “Ring scotoma”.
Correct Answer. c
(151). Thickness of cornea is measured by:
a. Specular microscope
b. Keratometer
c. pachymeter
d. Topography
Solution. (c) pachymeterRef:Read the text belowSol:- Pachymetry can be done with the ultrasound or by using an optical pachymeter.- Corneal pachymetry is the measurement of corneal thickness. Pachymetry was traditionally used to gauge the functional status of thecorneal endothelial cell layer.- More recently, with the emergence of refractive surgical techniques, corneal pachymetry is necessary to determine suitable candidatesfor ablation procedures.- Furthermore, the identification of central corneal thickness (CCT) as an independent indicator of glaucoma risk by the OcularHypertensive Treatment Study (OHTS) has made corneal pachymetry a routine part of the ophthalmic evaluation.- Pachymetry is an important part of the evaluation and management of ocular hypertension and glaucoma.
Correct Answer. c
(152). yrs old male underwent cataract surgery 9 month back, complains of blurring of vision with pain in eye. Ocular examination show ant.uveitis with vitritis. After vitreous culture diagnosis of fungal endophthalmitis is made. Treatment of choice is-
a. Amphotericin B
b. Miconazole
c. Itraconazole
d. Ketoconazole
Solution. (a) Amphotericin BRef:Read the text belowSol:Fungal endophthalmitis - important features - Most common cause - candida sp.- Characteristic features is “fluffy balls” in vitreous- Risk factors - immunosuppression, chronic IV therapy, lymphoma- For rapid diagnosis - calcofluor white stainingTreatment include- Antifungal therapy - amphotericin B is drug of choice- Vitrectomy- Removal of IOL·Drug for preventing recurrence - ketoconazole
Correct Answer. a

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 66/85
(153). Disinsertion of retina at the ora serrata is referred as :-
a. Retinal detachment
b. Retinoschisis
c. Retinal dialysis
d. Lattice degeneration
Solution. (b) RetinoschisisRef:Read the text belowSol:- Retinoschisis is splitting of retina at level of the outer plexiform layer at ora serrata, unlike retinal detachment, which is separationbetween sensory retina from pigment epithelium.- Lattice degen. is peripheral retinal degeneration, more common in myopes, and predisposes for RD.
Correct Answer. b
(154). All of the following are the factors related with recurrent hemorrhage in case of traumatic hyphema, except -
a. Large hyphema
b. Black race
c. Elderly aged
d. hypotony
Solution. (c) Elderly agedRef:Parson - 408Sol:Recurrent hemorrhage occurs is 4 - 35% of the case of traumatic hyphema , usually during 2nd - 5th day following the blunt oculartrauma. The reasons for the recurrent haemorrhage are clot fibrinolysis and retraction Risk factors that may be associated with anincreased risk of developing a recurrent hemorrhage- Antiplatelet or anticoagulant ingestion- Race - Black & Hispanic- Age - Younger- IOP - HypotonyInitial hyphemma - large (>1/2 of AC or eight ball hyphema)A recurrent hemorrhage carries a poor prognosis with risk of following complications -- Secondary glaucoma- Corneal blood staining- Poor visual outcome
Correct Answer. c
(155). Deterioration of the visual acuity is least in which type of astigmatism :-
a. Compound
b. Mixed
c. Hyperopic
d. Myopic
Solution. (b) MixedRef:Parson - 54Sol:- Higher degree of astigmatism cause a lowering of visual acuity.- This is usually least in mixed astigmatism,probably because the circle of least confusion falls upon or near the retina
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 67/85
(156). Lamina fusca is a part of :
a. Cornea
b. Iris
c. Sclera
d. Retina
Solution. (c) ScleraReference – Read the text belowSol:- It is the innermost layer of sclera, composed of thin collagen bundles and pigmented cells.
Correct Answer. c
(157). Posterior embryotoxon is
a. Arcus senilis
b. Arcus juvenilis
c. Prominent termination of Descemet’s membrane
d. Prominent termination of Bowman’s membrane.
Solution. (c) Prominent termination of Descemet’s membraneReference – Read the text belowSol:- Termination of Descemet’s membrane is also called Schwalbe’s line which form the anterior border of the trabecular meshwork.- Axenfield-Rieges anomaly is always associated with posterior embryotoxon.- Alagille syndrome is associated with posterior embryotoxon in 95% of cases.
Correct Answer. c
(158). Retinoscopy is also known as:
a. Windows test
b. Shadow test
c. Image test.
d. Tension test
Solution. (b) Shadow testReference – Read the text belowSol:- Retinoscopy on skiascopy as the shadow test is the most practical method of estimating the refraction objectively.- It is ideally done at a distance of 1 meter either with a Prestley smith or with a streak retinoscope.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 68/85
(159). The conjunctival fluid is significantly more alkaline in patients with all of the following except:
a. Lens wearers
b. Lacrimal stenosis
c. Keratitis
d. Mycotic keratitis
Solution. (a) Lens wearersRef– Read the text belowSol:- The pH of the conjunctival fluid was measured with a micro-glass-electrode in the inferior conjunctival fornix of 200 persons.- The conjunctival fluid was significantly more acid in contact lens wearers (6.66 +/- 0.28, N = 26), but became normalized after removalof the lens (6.49 +/- 0.32----7.09 +/- 0.19, N = 8, P less than 0.001.- The conjunctival fluid was significantly more alkaline in patients with lacrimal stenosis (7.13 +/- 0.28, N = 11), keratitis (7.14 +/- 0.28,N = 10), especially mycotic keratitis and postoperatively (7.15 +/- 0.22, N = 10, the first 24 h after corneal transplantation).- There was, perhaps, a tendency towards alkalisation in eyes with keratoconjunctivitis sicca, whereas the pH was normal in the otherpathological states, or the number of cases representing these may be too small.
Correct Answer. a
(160). Latent period of photo ophthalmia is how many hours?
a. 1 to 2 hours
b. 4 to 5 hours
c. 10 to 12 hours
d. 27 to 30 hours
Solution. (b) 4 to 5 hoursRef– Read the text belowSol:- There is usually a latent period of 4 to 5 hours between exposure and onset of symptoms.- It is generally caused by exposure to welding light.
Correct Answer. b
(161). A boy presents with diplopia and restriction of eye movement following blunt trauma to his eye. X-ray reveals blow out fracture of theorbit. Which orbital wall is most likely to be involved.
a. Superior wall
b. Inferior wall
c. Lateral wall
d. medial wall
Solution. (b) Inferior wallRef– Read the text belowSol:- Blow out fracture of the orbit generally involves the inferior wall.- These fractures occurs due to sudden increase in orbital pressure, when it is struck by an object of diameter . / = 5 cm.
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 69/85
(162). Mutton fat keratic precipitates, seen on slit lamp examination are present in:
a. Granulomatous iridocyclitis
b. Choroidits
c. Non-granulomatous iridocyclitis
d. viteous hemorrhage
Solution. (a) Granulomatous iridocyclitisRef– Read the text belowSol:- Mutton fat keratic precipitates are suggestive of a chronic granulomatous process. The differential diagnosis includes sarcoidosis,syphyllis, and tuberculosis. Other unusual chronic infections may also produce mutton fat keratic precipitates e.g. leprosy, brucellosis,coccidiomycosis.- Mutton fat KPS have a greasy or waxy appearance.- They are composed of epitheloid and mononuclear macrophages.
Correct Answer. a
(163). Regardinginterstitial keratitis which of the following is false?
a. It is commonly seen in syphilis, tuberculosis and leprosy
b. It is an inflammation involving the full thickness of the cornea
c. Salmon patch is a pathognomonic finding
d. Treatment involves topical steroids, cycloplegics and specific etiological treatment.
Solution. (b) It is an inflammation involving the full thickness of the corneaRef– Read the text belowSol:- Interstitial keratitis is an inflammation of corneal stroma without primary involvement of either the epithelium or the endothelium.- It is also seen in Cogan’s syndrome in which there is interstitial keratitis, deafness, vitiligo and tinnitus.- Wessley’s ring is seen in viral interstitial keratitis.
Correct Answer. b
(164). Lucid interval of Vogt is seen in
a. Diabetic retinopathy
b. Photo-ophthalmia
c. Sympathetic ophthalmia’s
d. Arcus senilis.
Solution. (d) Arcus senilis. Ref– Read the text belowSol:- Both arcus senilis and arcus juvenilis are separated from the limbus by a clear zone called the lucid interval.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 70/85
(165). The deposits shown in the Fig are localised to which layer of cornea ?
a. Epithelium
b. Bowman’s layer
c. Posterior stroma
d. Descemet’s membrane
Solution. (d) Descemet’s membraneRef:Read the text belowSol:- Figure shows a Kayser- Fletcher ring in the cornea, which represents deposition of copper in the posterior lamella of Descemet’smembrane.
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 71/85
(166). Study the Fig again,whichone of the following statements regarding this disease is true?
a. It is an isolated, nonhereditary disease
b. The corneal findings can be used to monitor therapy
c. It is caused by a defect in the kidney
d. The corneal findings are pathognomonic for this patient’s disease
Solution. (b) The corneal findings can be used to monitor therapy.Ref:Alberts Principles and Practice of Ophthalmology- 567Sol:- Figure shows a Kayser- Fletcher ring in the cornea, which represents deposition of copper in the posterior lamella of Descemet’smembrane.- Such a ring may be seen in Wilson’s disease, primary biliary cirrhosis, chronic hepatitis, or progressive intrahepatic cholestasis ofchildhood, but patient only patients with Wilson’s disease will show neurologic findings.- Treatment of Wilson’s disease is with penicillamine, and the Kayser-Fleischer ring will disappear with appropriate treatment, therebyproviding a means to monitor therapy. The defect in Wilson’s disease is a decreased production of ceruloplasmin by the liver.
Correct Answer. b
(167). All are grades of binocular single vision except
a. Simaltaneous macular perception
b. Fusion
c. Fixation
d. Stereopis
Solution. (c) FixationRef:Read the text belowSol :- Stereopsis is depth perception.- It is both binocular and uniocular.- True stereopsis refers to binocular stereopsis.- It mainly occurs due to horizontal disparity with one object usually located behind the fixation point. Binasal disparity indicateshorizontal disparity.- Grades of BSV:- Grade1 : simultaneous perception- Grade2: Fusion- Grade3: Stereopsis .- Time period when BSV is formed: 5-6 yrs
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 72/85
(168). Cystoid macular edema occurs due to a break in:
a. Outer blood-retinal barrier
b. Inner blood-retinal barrier
c. Both of the above
d. None of the above
Solution. (b) Inner blood-retinal barrierRef:Read the text belowSol :- Inner blood-retinal barrier is composed of the tight junction of retinal capillaries,endothelial cells and the outer blood-retinal barrierconsists of tight junctional complexes [ zonula occludens and zonula adherens] which are located between adjacent RPE cells.
Correct Answer. b
(169). Drug of choice for angle closure glaucoma is
a. Pilocarpine
b. Timolol
c. Acetazolomide
d. Latanoprost
Solution. (a) PilocarpineRef:Read the text belowSol :- DOC for angle closure with very high IOP is Acetazolamide- Treatment of choice is Peripheral Iridotomy
Correct Answer. a
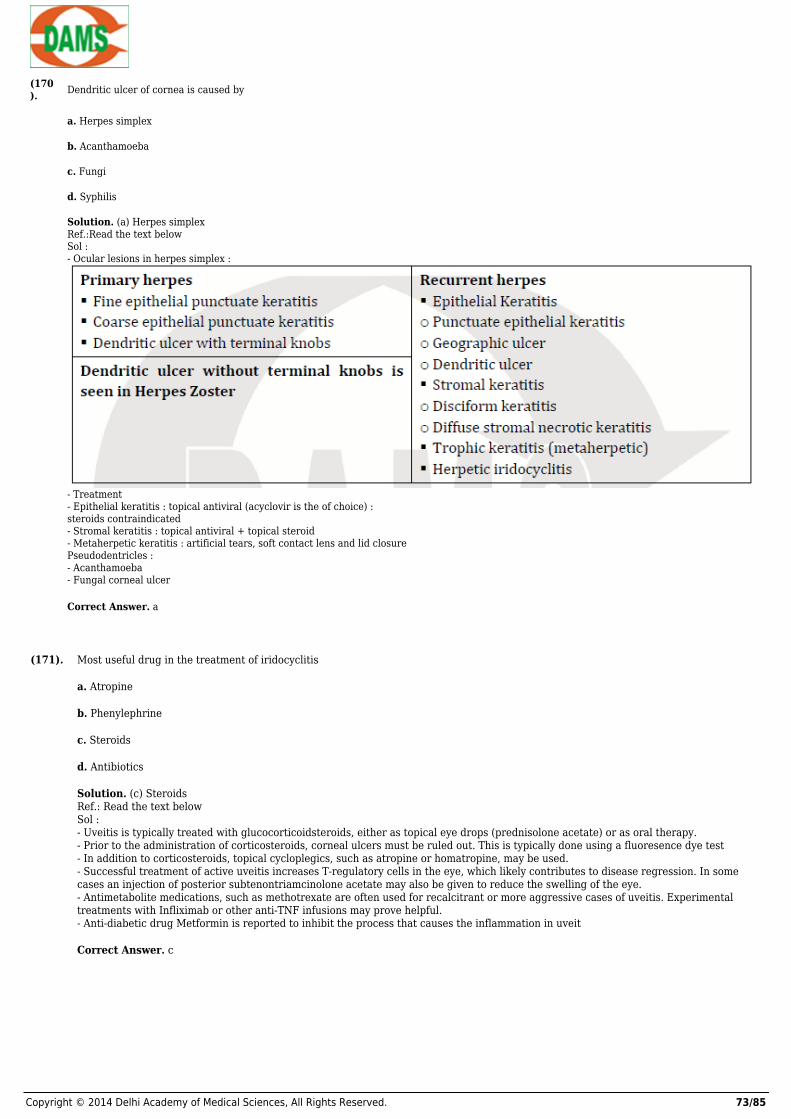
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 73/85
(170). Dendritic ulcer of cornea is caused by
a. Herpes simplex
b. Acanthamoeba
c. Fungi
d. Syphilis
Solution. (a) Herpes simplexRef.:Read the text belowSol :- Ocular lesions in herpes simplex :
- Treatment- Epithelial keratitis : topical antiviral (acyclovir is the of choice) :steroids contraindicated- Stromal keratitis : topical antiviral + topical steroid- Metaherpetic keratitis : artificial tears, soft contact lens and lid closurePseudodentricles :- Acanthamoeba- Fungal corneal ulcer
Correct Answer. a
(171). Most useful drug in the treatment of iridocyclitis
a. Atropine
b. Phenylephrine
c. Steroids
d. Antibiotics
Solution. (c) SteroidsRef.: Read the text belowSol :- Uveitis is typically treated with glucocorticoidsteroids, either as topical eye drops (prednisolone acetate) or as oral therapy.- Prior to the administration of corticosteroids, corneal ulcers must be ruled out. This is typically done using a fluoresence dye test- In addition to corticosteroids, topical cycloplegics, such as atropine or homatropine, may be used.- Successful treatment of active uveitis increases T-regulatory cells in the eye, which likely contributes to disease regression. In somecases an injection of posterior subtenontriamcinolone acetate may also be given to reduce the swelling of the eye.- Antimetabolite medications, such as methotrexate are often used for recalcitrant or more aggressive cases of uveitis. Experimentaltreatments with Infliximab or other anti-TNF infusions may prove helpful.- Anti-diabetic drug Metformin is reported to inhibit the process that causes the inflammation in uveit
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 74/85
(172). Smoke stack sign in Flourescein angiogram is seen in
a. Central serous retinopathy
b. Retinitis pigmentosa
c. Retinal detachment
d. Coat’s disease
Solution. (a) Central serous retinopathyRef.:Read the text belowSol :Central serous retinopathy- Spontaneous serous detachment of neurosensory retina in the macular region- Males, 20-40 yrs, type A personality- Imbalance between sympathetic and parasympathetic drive that maintains the autoregulation of choroidal circulation – hyperpermeability leading to leakage of fluid across the outer blood retinal barrier.- Sudden painless loss of vision- Relative positive scotoma, Micropsia, Metamorphopsia- Ophthalmoscopy – circular ring reflex present, foveal reflex absent- Usually self limiting but often recurrent- FFA – ink blot pattern or smoke stack pattern
Correct Answer. a
(173). Lacrimal secretion is mediated by all except:
a. Inferior salivatory ganglion
b. Geniculate ganglion.
c. Greater petrosal nerve.
d. Zygomaticotemporal nerve.
Solution. (a) Inferior salivatory ganglionRef:Read the text belowSol : Can be remembered by SG2 PZ – sup salivatory ganglion, geniculate ganglion, greater petrosal nerve, pterygopalatine ganglion,zygomaticotemporal nerve- Treatment of congenital dacryocystitis in a 4 month old child: antibiotic with massage- In DCR we make the opening in : middle meatus.- NLD opens in the inferior meatus of nose .
Correct Answer. a
(174). The common ocular pathology associated with trisomy 13 is –
a. Capillary hemangioma
b. B/L micro-ophthalmia
c. Dermoid cyst
d. Neurofibroma
Solution. (b) B/L micro-ophthalmiaRef:Read the text belowSol : Trisomy-13 is called Patau syndrome . Features are: OCULAR FEATURESa. Microphthalmosb. Corneal opacityc. Peter’s anomalyd. Cataracte. Retinal dysplasiaSYSTEMIC FEATURESa. Microcephalyb. Cleft lip and palatec. Low –set ears
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 75/85
(175). Popcorn simulating lesion between normal and avascular retina is which stage of ROP?
a. ROP 1
b. ROP 2
c. ROP 3
d. ROP 4
Solution. (b) ROP 2Ref:Read the text belowSol :- GRADE 1 IS DEMARCATION LINE- GRADE 2 IS RIDGE FORMATION- GRADE 3 NEOVASCULARISATION- GRADE 4 IS SUBRETINAL RD- GRADE 5 IS RETINAL DETACHMENT .1. Most important factor for occurrence of ROP is low birth weight or prematurity, --- it is prematurity.2. Ideal time to screen the child for ROP --- it is between 32wks to 36wks .3. Treatment of ROP is --- laser photocoagulation of the hypoxic retina .]
Correct Answer. b
(176). A 25 year old lady presents with sudden, severe bilateral loss of vision more so on right side with no perception of light.Rest of theexamination including Pupillary reflex,fundus & optokinetic nystagmus are normal.she was able to touch tips of her finger with right eyeclosed but not with left eye closed. Most likely diagnosis-
a. Optic neuritis
b. Anterior ischaemic optic neuropathy
c. Cmv retinitis
d. Funtional visual loss
Solution. (d) Funtional visual lossRef:Read the text belowSol :- Pupillary reactions will not be normal in optic neuritis and anterior ischemic optic neuropathy and fundus shows blurred disc margin.- In CMV retinitis ,fundus shows sauce and cheese retinopathy.- The above symptoms are more in favour of functional visual loss
Correct Answer. d
(177). Dilator pupillae is supplied by –
a. Post ganglionic parasympathetic fibers from Edinger Westphal nucleus
b. Post ganglionic sympathetic fibers from cervical sympathetic chain
c. III nerve
d. Sympathetic fibers from fronto orbital branch of V nerve
Solution. (b) Post ganglionic sympathetic fibers from cervical sympathetic chainRef:Read the text below .Sol :- Ophthalmic division of trigeminal ie ophthalmic nerve arises from the trigeminal ganglion, and in the cavernous sinus it divides intothree branches ie lacrimal,frontal and nasociliary.- Nasociliary contains the sympathetic fibres from the sympathetic chain , which through the long ciliary nerves , supply the dilatorpapillae.
Correct Answer. b
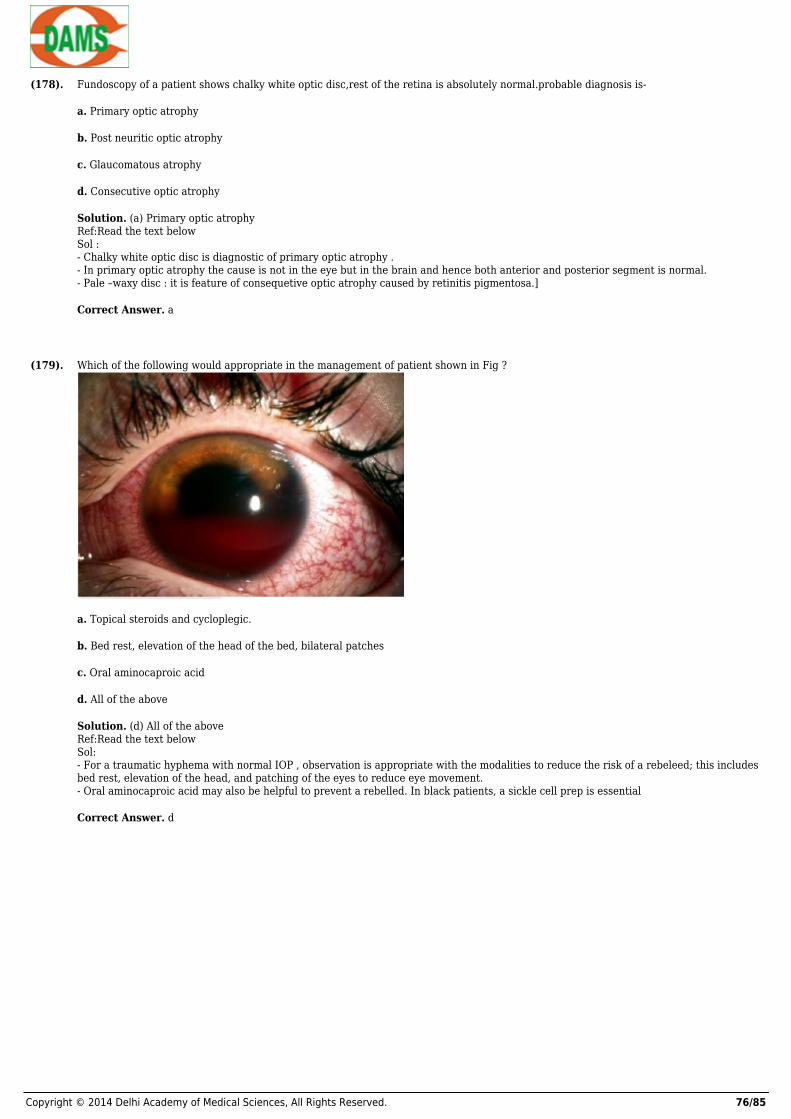
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 76/85
(178). Fundoscopy of a patient shows chalky white optic disc,rest of the retina is absolutely normal.probable diagnosis is-
a. Primary optic atrophy
b. Post neuritic optic atrophy
c. Glaucomatous atrophy
d. Consecutive optic atrophy
Solution. (a) Primary optic atrophyRef:Read the text belowSol :- Chalky white optic disc is diagnostic of primary optic atrophy .- In primary optic atrophy the cause is not in the eye but in the brain and hence both anterior and posterior segment is normal.- Pale –waxy disc : it is feature of consequetive optic atrophy caused by retinitis pigmentosa.]
Correct Answer. a
(179). Which of the following would appropriate in the management of patient shown in Fig ?
a. Topical steroids and cycloplegic.
b. Bed rest, elevation of the head of the bed, bilateral patches
c. Oral aminocaproic acid
d. All of the above
Solution. (d) All of the aboveRef:Read the text belowSol:- For a traumatic hyphema with normal IOP , observation is appropriate with the modalities to reduce the risk of a rebeleed; this includesbed rest, elevation of the head, and patching of the eyes to reduce eye movement.- Oral aminocaproic acid may also be helpful to prevent a rebelled. In black patients, a sickle cell prep is essential
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 77/85
(180). Study the fig again,If this patient’s intraocular pressure (IOP ) had been elevated and a small amount of corneal blood staining resulted,what would be the MOST appropriate next step ?
a. Anterior chamber washout
b. Topical carbonic anhydrase inhibitor
c. Continued observation
d. Injection of tissue plasminogen activator into the anterior chamber
Solution. (a) Anterior chamber washoutRef:Wills eye Manual, 6th edi. Pg 21Sol:- If IOP is elevated in hyphema and there are no signs of corneal blood staining, medical management of the IOP is appropriate.- A carbonic anhydrase inhibitor may not be the best agent to lower IOP with the possibility of sickle cell in a black patient.- If the IOP still remains elevated and / or signs of corneal blood staining appear, then surgical intervention is necessary with an anteriorchamber washout.- Intracameral t-PA may be able to lyse the clot; however, the blood breakdown products will still remain in the anterior chamber, and theIOP will be unaffected.
Correct Answer. a
(181). All of the following have been associated with scleritis except:
a. Gout
b. Tuberculosis
c. Leprosy
d. Behcet’s disease
Solution. (d) Behcet’s diseaseRef:Kanski 6th edi. Pg 325Sol- Scleritis has been associated with infectious disease (syphilis, tuberculosis, herpes zoster, and leprosy), autoimmune diseases (rheumatoid arthritis, Wegener’s granulomatosis, systemic lupus erythematosus, and polyarteritis nodosa ), and metabolic diseases (gout).
Correct Answer. d

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 78/85
(182). All of the following areacceptable therapies for scleritis except:
a. Posterior sub-Tenon’s steroid injection
b. oral nonstreoidal antiflammatory agents (NSAIDs )
c. topical cyclosporine
d. systemic steroids
Solution. (a) Posterior sub-Tenon’s steroid injectionRef:Kanski, 6th edi, pg 456Sol:- Injection of steroids into sub-Tenon’s space is contraindicated because it may increase the risk of scleral thinning and melting.- Initial management is usually with an oral NSAID agent followed by systemic steroids and topical cyclosporine.- Eventually, systemic immunosuppressives with azathioprine or methotrexate may be necessary.
Correct Answer. a
(183). Of the following, what is currently the most common indication for penetrating keratoplasty in adults ?
a. Fuchs’ dystrophy
b. Aphakic bullous keratopathy
c. Pseudophakic bullous keratopathy
d. Herpes simplex keratitis
Solution. (c) Pseudophakic bullous keratopathyRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 829Sol:- Pseudophakic bullous keratopathy is the most frequent indication for penetrating keratoplasty in adults.- This condition may decline in the future because of improvements in the design of anterior chamber and iris-fixated IOLs and inphacoemulsification techniques.- Regrafts and keratoconus are also frequent indications for keratoplasty
Correct Answer. c
(184). According to the Collaborative Corneal Transplant Study:
a. Human leukocyte antigens ( HLA ) tissue matching was clearly advantageous
b. HLA tissue matching was considered cost-effective
c. ABO blood type incompatibility was shown to be possible risk factor
d. Peripheral corneal vascularization was not a significant risk factor
Solution. (c) ABO blood type incompatibility was shown to be possible risk factorRef:Alberts Principles and Practice of Ophthalmology- 817Sol:- The most interesting conclusion of this study was that even for high-risk keratoplasties, HLA tissue matching was neither clearlyadvantageous nor cost effective.- The possibility also existed of a correlation of risk and ABO blood type incompatibility.- Further study is needed to decide whether this is a necessary screening test.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 79/85
(185). Most rigid gas permeable contact lens wearers should discontinue use of their lenses at least how many days before a refractiveevaluation?
a. 7 days
b. 21 days
c. 30 days
d. 60 days
Solution. (b) 21 daysRef:Wills eye Manual- 90Sol:- Most contact lens wearers are very reluctant to discontinue use of their lenses for any significant amount of time.- Stability of refraction and topography are important when deciding on a surgical plan.- Most surgeons require at least 2 to 3 weeks of a contact lens “ holiday “ to verify stability.- Some individuals require a longer period before they show stability.
Correct Answer. b
(186). In keratoconus, the cone is situated at the
a. Center of cornea
b. Just below the center of cornea
c. Just above the center of cornea
d. Either side of cornea.
Solution. (b) Just below the center of corneaRef– Read the text belowSol:Keratoconus (KC) is a progressive, noninflammatory, bilateral (but usually asymmetrical) ectatic corneal disease, characterized byparaxial stromal thinning and weakening that leads to corneal surface distortion. Visual loss occurs primarily from irregular astigmatismand myopia, and secondarily from corneal scarring. Protrusion usually but not exclusively affects the axial and inferonasal cornea.- Thinning of cornea seen in keratoconus, occurs at the apex of the cone.- This cone is often decentered inferiorly or inferonasally.
Correct Answer. b
(187). Redundancy of the upper lid skin is called
a. Blepharophimosis
b. Dermatochalasis
c. Belpharochalasis
d. Symblpheron.
Solution. (b) DermatochalasisRef– Read the text belowSol:- Dermatochalasis at times is so severe that it presents as a fold of skin overhanging a normally placed lid margin.- This form of pseudoptosis may require Blepheroplasty for relief.- Blepharochalasis occurs due to the recurrent attacks of severe edema of the eyelids which damages the contents of the eyelid, whichmight cause the eyelid to droop.
Correct Answer. b

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 80/85
(188). InCrede’s method what percentage of AgNo3 is used
a. 0.75 percent
b. 0.5 percent
c. 1 percent
d. 1.25 percent.
Solution. (c) 1 percentRef– Read the text belowSol:A method for preventing ophthalmia neonatorum by administering one drop of a 2 percent solution of silver nitrate into each eye of anewborn infant.- For prophylaxis of Ophthalmia neonatrum due to Gonnococcal infection, a drop of 1 percent Ag No3 may be installed in each eyes of theneonate.- {Ag No3 solution stronger than 1 percent should not be used, as it can cause corneal opacity.}
Correct Answer. c
(189). Generally hypermetropia is not seen beyond how many dioptres:
a. +3D
b. +4D
c. +5D
d. +6D
Solution. (d) +6DReference – Read the text belowSol:- Axial hypermetropia is its most common cause.- Generally shortening of not more 2 mm is present.- As each 1mm is equivalent to +3D, thus hypermetropia is rarely seen more than +6D.
Correct Answer. d
(190). 76 years female has come to ophthalmologist with complain of red painful eye with marked impairment of vision. Local examinationsshow she has hypermature cataract. Likely diagnosis is -
a. Primary angle closure glaucoma
b. Phacomorphic glaucoma
c. Phacoantigenic uveitis
d. Phacolytic glaucoma
Solution. (d) Phacolytic glaucomaRef:Read the text belowSol:- Patient is having phacolytic glaucoma, seen in hypermature cataract form release of lens protein through intact capsule.- In phacomorphic glaucoma AC depth is shallow and dilated pupil.- In PACG AC depth in shallow, phacoantigenic uveitis occurs following trauma.
Correct Answer. d
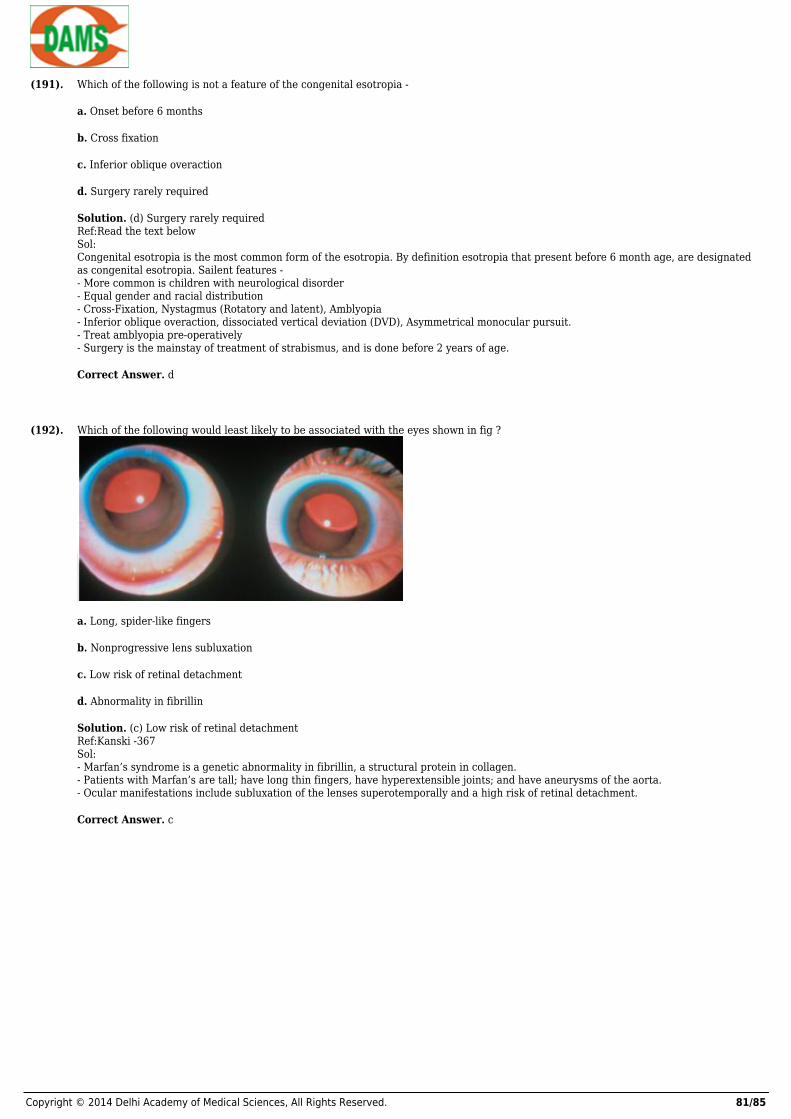
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 81/85
(191). Which of the following is not a feature of the congenital esotropia -
a. Onset before 6 months
b. Cross fixation
c. Inferior oblique overaction
d. Surgery rarely required
Solution. (d) Surgery rarely requiredRef:Read the text belowSol:Congenital esotropia is the most common form of the esotropia. By definition esotropia that present before 6 month age, are designatedas congenital esotropia. Sailent features -- More common is children with neurological disorder- Equal gender and racial distribution- Cross-Fixation, Nystagmus (Rotatory and latent), Amblyopia- Inferior oblique overaction, dissociated vertical deviation (DVD), Asymmetrical monocular pursuit.- Treat amblyopia pre-operatively- Surgery is the mainstay of treatment of strabismus, and is done before 2 years of age.
Correct Answer. d
(192). Which of the following would least likely to be associated with the eyes shown in fig ?
a. Long, spider-like fingers
b. Nonprogressive lens subluxation
c. Low risk of retinal detachment
d. Abnormality in fibrillin
Solution. (c) Low risk of retinal detachmentRef:Kanski -367Sol:- Marfan’s syndrome is a genetic abnormality in fibrillin, a structural protein in collagen.- Patients with Marfan’s are tall; have long thin fingers, have hyperextensible joints; and have aneurysms of the aorta.- Ocular manifestations include subluxation of the lenses superotemporally and a high risk of retinal detachment.
Correct Answer. c
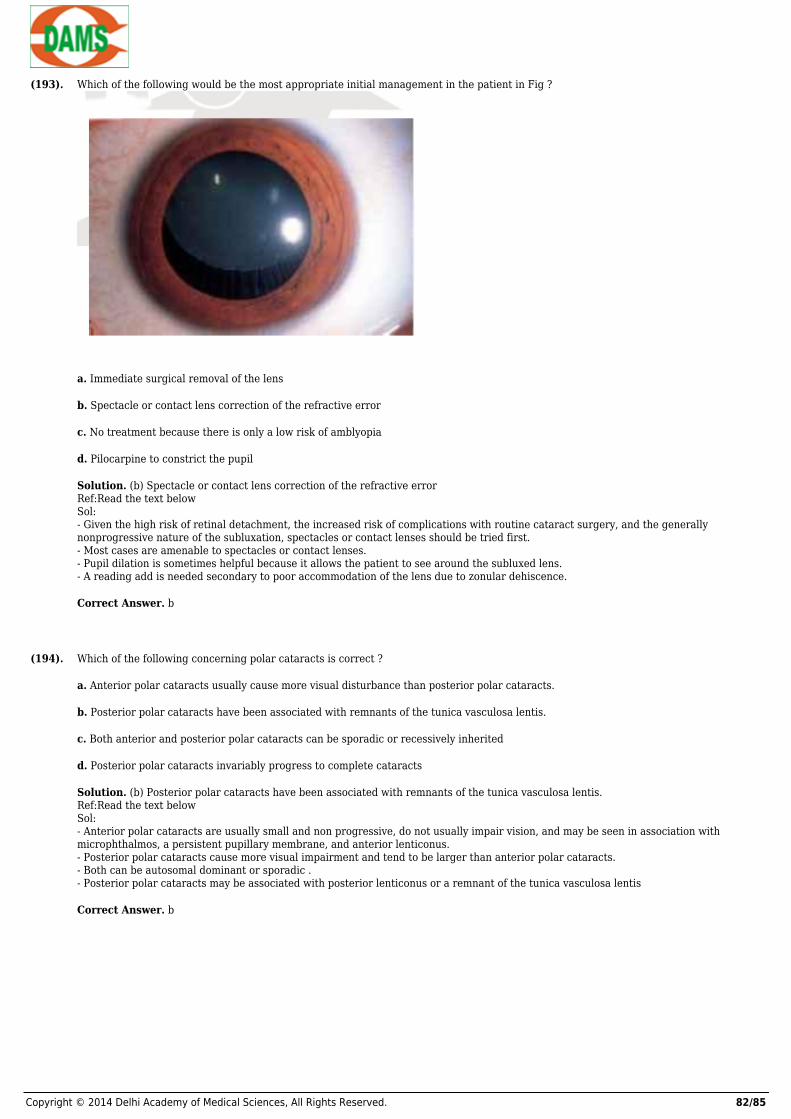
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 82/85
(193). Which of the following would be the most appropriate initial management in the patient in Fig ?
a. Immediate surgical removal of the lens
b. Spectacle or contact lens correction of the refractive error
c. No treatment because there is only a low risk of amblyopia
d. Pilocarpine to constrict the pupil
Solution. (b) Spectacle or contact lens correction of the refractive errorRef:Read the text belowSol:- Given the high risk of retinal detachment, the increased risk of complications with routine cataract surgery, and the generallynonprogressive nature of the subluxation, spectacles or contact lenses should be tried first.- Most cases are amenable to spectacles or contact lenses.- Pupil dilation is sometimes helpful because it allows the patient to see around the subluxed lens.- A reading add is needed secondary to poor accommodation of the lens due to zonular dehiscence.
Correct Answer. b
(194). Which of the following concerning polar cataracts is correct ?
a. Anterior polar cataracts usually cause more visual disturbance than posterior polar cataracts.
b. Posterior polar cataracts have been associated with remnants of the tunica vasculosa lentis.
c. Both anterior and posterior polar cataracts can be sporadic or recessively inherited
d. Posterior polar cataracts invariably progress to complete cataracts
Solution. (b) Posterior polar cataracts have been associated with remnants of the tunica vasculosa lentis.Ref:Read the text belowSol:- Anterior polar cataracts are usually small and non progressive, do not usually impair vision, and may be seen in association withmicrophthalmos, a persistent pupillary membrane, and anterior lenticonus.- Posterior polar cataracts cause more visual impairment and tend to be larger than anterior polar cataracts.- Both can be autosomal dominant or sporadic .- Posterior polar cataracts may be associated with posterior lenticonus or a remnant of the tunica vasculosa lentis
Correct Answer. b
Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 83/85
(195). Which of the following is not associated with microspherophakia ?
a. Small stature, stubby fingers, reduced joint mobility
b. Alport’s syndrome
c. Congenital rubella
d. Hyperlysinemia
Solution. (d) HyperlysinemiaRef:Kanski - 367Sol:- All of these conditions have been reported to be associated with microspherophakia, except hyperlysinemia, which has been related toectopic lentis.- Patients with Weill-Marchesani have small stature, stubby fingers with broad hands, and stiff joints.- Weill-Marchesani is also associated with anterior dislocation of the lens
Correct Answer. d
(196). Which of the following is not a reported complication following YAG capusulotomy ?
a. Iritis
b. Retinal detachment
c. Corneal edema
d. Subluxation of lens
Solution. (c) Corneal edemaRef:Read the text belowSol:- Complications of YAG capsulotomies result from the energy delivered to the eye.- The YAG creates micro explosions that disrupts the posterior capsule.- This may also put traction on the vitreous, causing a retinal break.- Elevated IOP, iritis, and macular edema are also resulting complications.- Corneal edema should not result if laser is properly focused at the posterior capsule.
Correct Answer. c
(197). A 68-year-old man underwent cataract extraction with phacomulisification and insertion of posterior chamber IOL. The first daypostoperatively, he comes back with moderate epithelial and stromal edema. One week later, the edema is still present. Which is NOT acause for his persistent corneal edema ?
a. Elevated IOP
b. Chemical toxicity
c. Epithelial down growth
d. Surgical trauma
Solution. (c) Epithelial down growthRef:Read the text belowSol:- Among the causes of corneal edema the day following cataract extraction are elevated IOP ( From inflammation, glaucoma, debrisclogging the trabecular meshwork ), corneal decompensation ( low endothelial counts as in Fuchs’ dystrophy, endothelial chemicaltoxicity ), or trauma to the endothelium.- Epithelial down growth would not present immediately after surgery but would take weeks to develop.- The corneal decompensation would overlie the area of the downgrowth, and a membrane may be seen on the endothelium and iris.
Correct Answer. c

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 84/85
(198). Which one of the following is not a risk factor for CRVO ?
a. Hypertension
b. Glaucoma
c. Diabetes
d. Prosthetic cardiac valves
Solution. (d) Prosthetic cardiac valvesRef:Kanski - 584Sol:- Histopathologically, CRVO occurs as a result thrombosis at the lamina cribrosa.- Risk factors for CRVO include hypertension, glaucoma, diabetes, hyperopia, hypercoagulable states, and older age.- Emboli are associated with arterial occlusion rather than venous obstruction.
Correct Answer. d
(199). Which retinal layer accounts for the petalloid cystic appearance of cystoid macular edema ( CME ) ?
a. Nerve fibre layer
b. Inner plexiform layer
c. Outer plexiform layer
d. Outer nuclear layer
Solution. (c) Outer plexiform layerRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 1793Sol:- The radiating fibres of Henle in the outer plexiform layer lead to the cystic spaces in CME.
Correct Answer. c
(200). All of the following may develop a similar complication leading to central visual loss except:
a. Presumed ocular histoplasmosis syndrome ( POHS )
b. Angioid streaks
c. Pathologic myopia
d. Nanophthalmos
Solution. (d) NanophthalmosRef:Alberts Principles and Practice of Ophthalmology, 3rd edi – pg 1901Sol:- POHS, angioid streaks, and pathologic myopia may lead to development of choroidal neovascular membranes.- Nanophthalmos is associated with uveal effusions and serous retinal detachments
Correct Answer. d
Test Answer 1.(a) 2.(a) 3.(b) 4.(a) 5.(a) 6.(c) 7.(c) 8.(b) 9.(b) 10.(c)
11.(d) 12.(c) 13.(a) 14.(b) 15.(b) 16.(b) 17.(b) 18.(a) 19.(d) 20.(c)
21.(a) 22.(a) 23.(b) 24.(a) 25.(d) 26.(b) 27.(b) 28.(c) 29.(b) 30.(a)
31.(d) 32.(a) 33.(c) 34.(d) 35.(c) 36.(a) 37.(c) 38.(b) 39.(b) 40.(a)
41.(b) 42.(b) 43.(b) 44.(a) 45.(b) 46.(b) 47.(c) 48.(b) 49.(c) 50.(c)
51.(c) 52.(d) 53.(d) 54.(c) 55.(a) 56.(a) 57.(a) 58.(a) 59.(b) 60.(a)
61.(b) 62.(d) 63.(c) 64.(d) 65.(a) 66.(c) 67.(d) 68.(b) 69.(c) 70.(b)
71.(d) 72.(b) 73.(d) 74.(c) 75.(c) 76.(c) 77.(c) 78.(c) 79.(c) 80.(c)
81.(c) 82.(a) 83.(c) 84.(d) 85.(c) 86.(d) 87.(d) 88.(b) 89.(d) 90.(c)

Copyright © 2014 Delhi Academy of Medical Sciences, All Rights Reserved. 85/85
91.(a) 92.(d) 93.(d) 94.(c) 95.(d) 96.(a) 97.(d) 98.(c) 99.(b) 100.(d)
101.(a) 102.(d) 103.(a) 104.(d) 105.(b) 106.(c) 107.(b) 108.(d) 109.(c) 110.(d)
111.(b) 112.(d) 113.(a) 114.(a) 115.(d) 116.(b) 117.(d) 118.(c) 119.(c) 120.(a)
121.(d) 122.(d) 123.(c) 124.(b) 125.(d) 126.(c) 127.(b) 128.(d) 129.(b) 130.(b)
131.(b) 132.(d) 133.(c) 134.(a) 135.(a) 136.(b) 137.(b) 138.(d) 139.(a) 140.(c)
141.(d) 142.(d) 143.(d) 144.(d) 145.(a) 146.(b) 147.(d) 148.(b) 149.(a) 150.(c)
151.(c) 152.(a) 153.(b) 154.(c) 155.(b) 156.(c) 157.(c) 158.(b) 159.(a) 160.(b)
161.(b) 162.(a) 163.(b) 164.(d) 165.(d) 166.(b) 167.(c) 168.(b) 169.(a) 170.(a)
171.(c) 172.(a) 173.(a) 174.(b) 175.(b) 176.(d) 177.(b) 178.(a) 179.(d) 180.(a)
181.(d) 182.(a) 183.(c) 184.(c) 185.(b) 186.(b) 187.(b) 188.(c) 189.(d) 190.(d)
191.(d) 192.(c) 193.(b) 194.(b) 195.(d) 196.(c) 197.(c) 198.(d) 199.(c) 200.(d)