copd presentation atlantic canada - moncton (english) of niv in copd.pdf · gold pocket guide to...
TRANSCRIPT

November01,2013_SectorConfidential1
COPD:HomeNIV…..Istherebenefits?
October13thMoncton,NB

ConflictofInterestDisclosures
Type of Potential Conflict Employee ofPhilipsRespironics Inc.
Grant/Research SupportConsultant
Speakers’ BureausFinancial support
Other
2.Iwishtodisclosethefollowingpotentialconflictsofinterest,OR
3.Thematerialpresentedinthislecturehasnorelationshipwithanyofthesepotentialconflicts,OR
4.Thistalkpresentsmaterialthatisrelatedtooneormoreofthesepotentialconflicts,andthefollowingobjectivereferencesareprovidedassupportforthislecture:1.2.3.
1.Idonothaveanypotentialconflictsofinteresttodisclose,OR
X

3
COPD – fast facts
• leading cause of death
• Million afflicted
• Million diagnosed
• 3rd
• 3
• 1.5
3

4
ManagingCOPDpatientsisamajorissue
SOURCE:CanadianThoracicSociety
GrowingCOPDpopulation Increasingeconomicburden
COPDreadmissionsareplacingincreaseddemandsonhealthsystems,governmentsand
payersthroughouttheworld.
3millionMorethan
afflictedinCanada
50%afflictedUpto
Remainundiagnosed

WhyfocusonCOPD?Onlychronicdiseasewheremortalitystillrising

6
Change in COPD Mortality compared with
other major causes from 1970-2002
COPD Heart disease Cancer Stroke Accidents DiabetesDeath rate (% change) 102.8% -52.1% -2.7% -63.1% -41.0% 3.2%
-80.0%
-60.0%
-40.0%
-20.0%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0% Death rate (% change)
U.S.LeadingCausesofDeath;JAMA,September14,2005– Vol.294,No.106

Canada:COPDPrevalence,Aged65+,2010

1:4 Canadians >35 years will develop COPD Hospitalizationratesare60%higherinruralareas
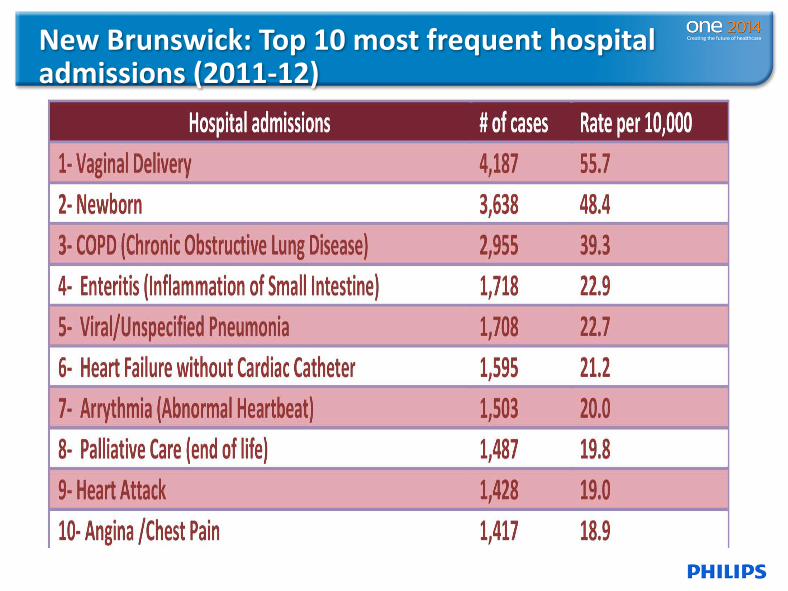
NewBrunswick:Top10mostfrequenthospitaladmissions(2011-12)

• NewBrunswick:HospitalreadmissionsforCOPDpatients
•within30days6%•within90days13%•within180days23%• Source:CIHIPortal- NBfacilities(AcuteCare)for2009/10.

1

EconomicCOPDimpactinAlberta.KeyPoints
1

13
CurrentCOPDpatientreadmittance scenario
23% of patients readmitted within 30-180 days² @ $7,400 per patient average readmission¹
¹Toyetal.TheeconomicimpactofexacerbationsofCOPDandexacerbationdefinition.Areview.COPD 2010:7:214-228²NationalQualityForum#1891,October26,2012

MarketDynamics
Changingpayer
modelsandlandscape
• Keepingpatientsoutofthehospitalisnowafinancialpriority
Hospitalswillbepenalized3%
• UnplannedadmissionsforCOPDwithin30daysofdischarge
Planningforpost-discharge
• Involvesstrongpartnershipwithallpost-acutecareproviders
15
COPDisnotglamour!
DrJohnHaggie,ministerofhealth,NL

16
ClinicalEvidence
16PhilipsConfidentialInformation

COPD stagesSeverity classified by spirometry
Stage 1
Stage 2
Stage 3
Stage 4
17
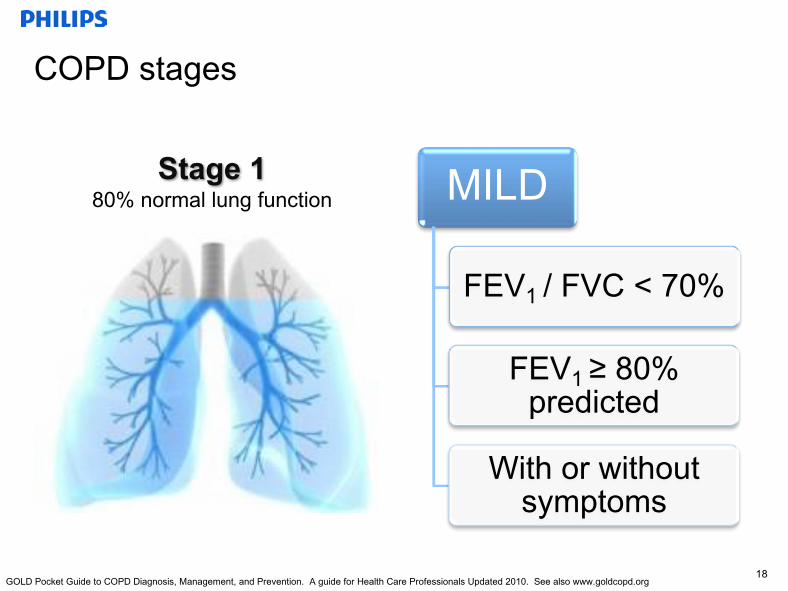
COPD stages
MILD
FEV1 / FVC < 70%
FEV1 ≥ 80% predicted
With or without symptoms
Stage 180% normal lung function
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org18

COPD stages
MODERATE
FEV1 / FVC < 70%
50% ≤ FEV1 < 80%
predicted
Stage 250 – 80% normal lung function
GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org19

COPD stages
SEVERE
FEV1 / FVC < 70%
30% ≤ FEV1 < 50%
predicted
Stage 330 – 50% normal lung function
Modified from GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org20

COPD stagesSeverity classified by spirometry
VERY SEVERE
FEV1 / FVC <70%
FEV1 <30% predicted
Stage 4Less than 30% normal lung function
Modified from GOLD Pocket Guide to COPD Diagnosis, Management, and Prevention. A guide for Health Care Professionals Updated 2010. See also www.goldcopd.org21
22PhilipsConfidentialInformation
COPDSimplyput;itsanAIROUTproblem.CO2hastobeclearedtomanagept.ventilation.

PathologicallinksfromDiseasetoSigns
Emphysema
ChronicBronchitis
Infection
Deteriorationofthe
Parenchyma
InflammationoftheBronchioli
Mucous
EFL
DynamicHyperinflation
↑WOB
↑PaCO2
↓PaO2
Va/Qmismatc
hAlveolarDeadspac
e
AlveolarDestruction

ReadmissionRiskfactors
• Previoushospitaladmission(ICU/ventilation)• HigherlevelsofPaCO2
• Dyspnea• Long-termoxygentherapy• Noroutinephysicalactivity• Poormedicationcompliance• Nosupport/caregiver
EconomicCOPDimpactinAlberta.KeyPoints
25
26
CarbonDioxideisariskfactorforreadmission
1.KesslerR,FallerM,Fourgaut G,Mennecier B,Weitzenblum E.1999.Predictivefactorsofhospitalizationforacuteexacerbationinaseriesof64patientswithchronicobstructivepulmonarydisease.AmericanJournalofRespiratory&CriticalCareMedicine,159:158–642. Bahadori,K,Fitzgerald,M.RiskfactorsofhospitalizationandreadmissionofpatientswithCOPDexacerbation– systematicreview,InternationalJournalofCOPD
2007:2(3)241–2513. Ligtowler JVetal.Non-invasivepositivepressureventilationtotreatrespiratoryfailureresultingfromexacerbationsofCOPD;CochraneSystematicReview.BMJ.
2003.Jan25:326(7382):185.4. Duiverman ML,Wempe JB,etal.Two-yearhome-basednocturnalnoninvasiveventilationaddedtorehabilitationinchronicobstructivepulmonarydiseasepatients:
arandomizedcontrolledtrial.Respir Res.2011Aug23;12:112.5. DeBackerL,Vos W,etal.Theeffectsoflong-termnoninvasiveventilationinhypercapnic COPDpatients:arandomized
controlledpilotstudy.Int JChron ObstructPulmon Dis.2011;6:615-24.
• ElevatedPCO2 isariskfactorforhospitaladmissionforaCOPDpatient.1• 52%ofthestudiesreportedPaCO2asariskfactorforreadmission.2
• NIVhasbeenshowntobethemosteffectivetreatmentoptionforreducingPaCO2 inhypercapnic COPDpatients.3
• ClinicalstudiesonNIVinhypercapnic COPDshowimprovedbloodgasesandlowerhospitalizationratescomparedtopatientsnottreatedwithNIVathome.4,5

27
2
WhydoCOPDpatientsexacerbate?
ØTheyfailinadherenceofsteroidalsØTheyfailinmednebadherenceofbronchodilators
ØTheiractivitylevelsdecreaseorstopØTheyfailtomakefollowupphysicianappointments.

28
Ifweknowthecausesoftheseexacerbations,whyare
readmissionratesashighas23%?• WHATISMISSING?NIV?
• WhywouldwewanttotreatthesepatientsanydifferentlyinthehomethanwedowhentheyarriveintheER??

29
• NIVhasshowntobethemosteffectiveinreducingCO2 instablehypercapnicCOPDpatients.3
• Wheninitiatedearlythiscanhelpreducehospitaladmissionratesandthecostofhealthcare,whileimprovingthequalityoflife.3
TreatingCOPDinthehome
³(Ligtowler JV,Wedzicah JA,ElliottMW,RamFs.Non-invasiveventilationpositivepressureventilationtotreatrespiratoryfailureresultingfromexacerbationsofCOPD.CochraneSystematicReview.BMJ2003Jan25:326(7382):185
2
30

31

32
Hot-HMVERS2016abstract
• Multi-centre,RCTfundedbyPhilipsRespironicsandResMed– 116patients
§ SevereCOPD§ Recentlifethreateningexacerbation§ PaCO2>7kPA
– Interveneintherecoveryphase– Followupat6weeks,3monthsand1year
• Titrationstrategy– Highpressurestocorrectnocturnalhypoventilation
§ MeanIPAP=24§ Meanrate=14§ MeanEPAP=4
– O2startedatdaytimerate
• Results– Prolongedadmissionfreesurvivalform1.4to4.3months(p=0.007)

33
1.CoughlinS.,LiangWE,Parthasarathy S.RetrospectiveAssessmentofHomeVentilationtoReduceRehospitalization inChronicObstructivePulmonaryDisease.JClin SleepMed.2015Jun15;11(6):663-70.
MultifacetedCOPDprogramshowntoimprovecare
34
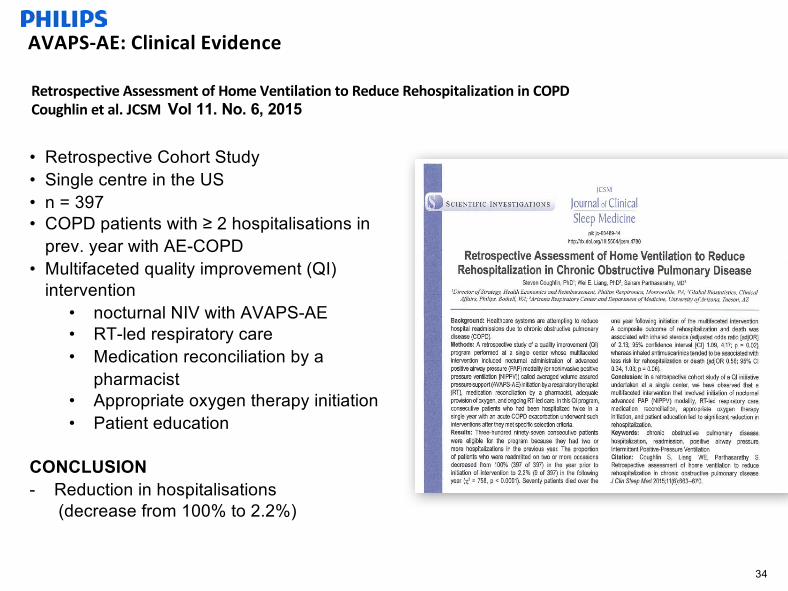
AVAPS-AE:ClinicalEvidence
• Retrospective Cohort Study• Single centre in the US• n = 397• COPD patients with ≥ 2 hospitalisations in
prev. year with AE-COPD• Multifaceted quality improvement (QI)
intervention • nocturnal NIV with AVAPS-AE• RT-led respiratory care• Medication reconciliation by a
pharmacist• Appropriate oxygen therapy initiation• Patient education
CONCLUSION- Reduction in hospitalisations
(decrease from 100% to 2.2%)
RetrospectiveAssessmentofHomeVentilationtoReduceRehospitalizationinCOPDCoughlinetal.JCSMVol 11. No. 6, 2015

TalkingPoints:MethodsUsed• Consecutivepatientswhohadbeenhospitalizedtwiceina
singleyearwithanacuteCOPDexacerbationwerescreenedforeligibilityandadmittedif:– COPDGOLDstages2,3or4– (b)BodeIndexScoregreaterthanorequalto5;– (c)oneofthefollowing:
• PaO2lessthanorequalto60mmHgor• PacO2greaterthanorequalto52mmHgor• FEV1lessthanorequalto40%
• Patientsreceived:– Medicationreconciliationbyapharmacist,– The(continued)provisionofoxygen,– AVAPS-AEinitiationbyarespiratorytherapist– Ongoingrespiratorytherapist-ledcare

AVAPS-AE isaauto-titrationmodeofnoninvasiveventilationdesignedtobettertreatrespiratoryfailurepatients(OHS,COPDandNMD)inthehospitalandhomecareenvironments
AVAPS-AE
• ProvenperformanceofAVAPS– Maintainstargetedtidalvolume
• AutoEPAP– Maintains patentupperairwayatcomfortablepressureutilizingPRIclinicallyproven
proactivealgorithm
• Autobackuprate– Preventsbreathstacking
36
AutoBackupRate
• AutobackupratecombinedwiththetidalvolumeassuranceofAVAPSprovidesaminimumlevelofventilation
• Comfortableassistancewhenneeded
• Nomanualadjustments
• Allowsthepatienttofullyexhalebeforethenexttimedbreathisdeliveredtopreventbreathstacking.

Spontaneousratecalculatedandback-upratesetto12
IncompleteExhalation CompleteExhalation

39
Proventoreducereadmissions
*AllreceivingNIVandmeetingprogrameligibilityrequirements.Allsubjectswereadmittedatleasttwiceintheprior12monthsbeforeenrollment.1.CoughlinS.,LiangWE,Parthasarathy S.RetrospectiveAssessment ofHomeVentilationtoReduceRehospitalization inChronicObstructivePulmonaryDisease.JClin SleepMed.2015Jun15;11(6):663-70.
88%reductionInareviewof398COPDpatients*
inhospitalreadmissions1
40
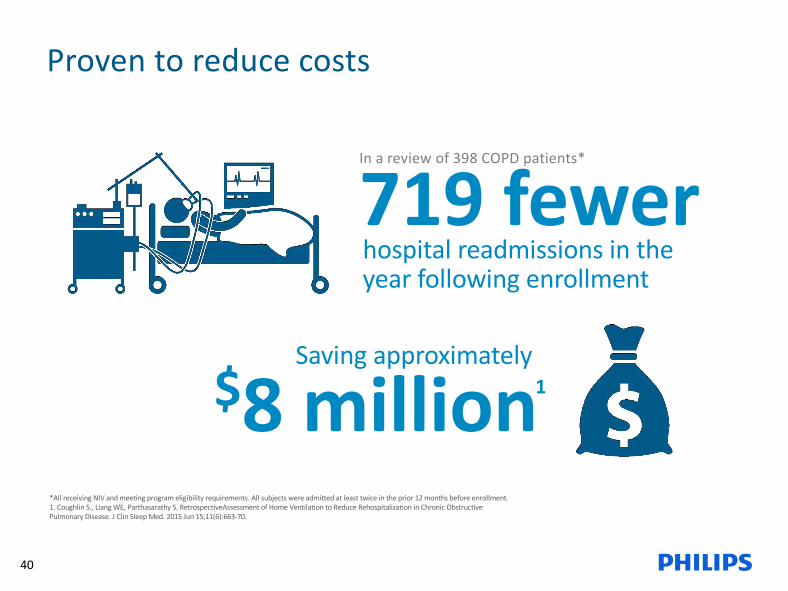
Proventoreducecosts
*AllreceivingNIVandmeetingprogrameligibilityrequirements.Allsubjectswereadmittedatleasttwiceintheprior12monthsbeforeenrollment.1.CoughlinS.,LiangWE,Parthasarathy S.RetrospectiveAssessment ofHomeVentilationtoReduceRehospitalization inChronicObstructivePulmonaryDisease.JClin SleepMed.2015Jun15;11(6):663-70.
719fewerInareviewof398COPDpatients*
hospitalreadmissionsintheyearfollowingenrollment
$8millionSavingapproximately
1

Dyspnea:keyconcernforCOPDpatients
InaCDCstudy,62%ofCOPDpatientssaidshortnessofbreathaffectedtheirqualityoflife1.
1.BehavioralRiskFactorSurveillanceSystem,UnitedStates,2011.Availableathttp://www.cdc.gov/brfss/annual_data/2011/pdf/codebook11_llcp.pdf

Solutionsexist;patientswantmore
Dailymedications
Rescueinhalers
Pursedlipbreathing
Anxietymanagementtechniques
Inspiratorymuscletraining
Pulmonaryrehabilitation

Dyspnea:keyconcernforCOPDpatients
InaPhilipsfocusgroup,55%ofCOPDpatientsindicatedthatshortnessofbreathwastheirbiggestconcern2.
2.InternalPhilipsRespironicsfocusgroupheld4/4/12with25COPDpatients

KeeppatientsoutofthecycleYourpatientfeels
breathless
Sheavoidsactivitiesthatmakeherbreathless
Hermusclesbecomeweakerandlessefficient
Shegetsmorebreathlesswhenshehastobeactive Shedoesfeweractivities

NIVstudiedwithCOPDpatientsNIValonewasmorebeneficialthansupplementaloxygenaloneinimprovingexercisetoleranceandqualityoflifeinsevereCOPDpatients3.
COPDpatientsusingNIVwhilewalkinghadlessdyspneaandwalkedfarther4.
COPDpatientswhousedNIVduringexercisetrainingshowedimprovementsinshuttlewalktestsandChronicRespiratoryDiseaseQuestionnaire5.
3.Borghi-Silvaetal.AdjunctstoPhysicalTrainingofPatientswithSevereCOPD:OxygenorNoninvasiveVentilation.RespiratoryCare2010,Jul:55(7),885-894.
4.Dreher,M.etal.NoninvasiveVentilationduringWalkinginPatientswithSevereCOPD:ARandomizedCrossoverTrial.ERJ,2007;29:930– 936.
5.Garrod etal.RandomizedControlledTrialofDomiciliaryNoninvasivePositivePressureVentilationandPhysicalTraininginSevereChronicObstructivePulmonaryDisease.AmJRespirCrit CareMed2000;162:1335-1341.

NIVhelpsCOPDpatientsrecover
Bi-levelof18/8demonstratedstatisticallysignificantreductioninrecoverytimecomparedtobaseline6
6.MahadevanA.etal.TheImpactofPEP,CPAPandBilevel inpost-exerciserecoveryfromdyspneainCOPDPatients.ERJSeptember1,2012vol.40no.Suppl 56P3532.
Exercise Recovery

KW10/20/15MCI4107017