continuing educational trends for laboratory personnel
TRANSCRIPT
3. Sun, T. et al. 1983. Morphologic and clinical observations in human infec- tion with Babesia microti. J. Infect. Dis. 148:239--248.
4. Iacopino, V. and T. Earnhart. 1990. Life-threatening babesiosis in a woman from Wisconsin. Arch. Intern. Med. 150:1527-1528.
5. Eklund, C. M., G. M. Kohls, and J. M. Brennan. 1955. Distribution of Colorado tick fever and virus-carrying ticks. JAMA 157:335-337.
6. Goodpasture, H. C. et al. 1978. Colo- rado tick fever: Clinical, epidemio- logic, and laboratory aspects of 228 cases in Colorado in 1973--1974. Ann. Intern. Med. 88:303-310.
7. McDade, J. E. 1990. Ehrlichiosis--A disease of animals and humans. J. In- fect. Dis. 161:609--617.
8. Eng, T. R. et al. 1990. Epidemio- logic, clinical, and laboratory findings of human ehrlichiosis in the United States, 1988. JAMA 264:2251-2258.
9. Dawson, J. E. et al. 1991. Isolation and characterization of an Ehrlichia
sp. from a patient diagnosed with hu- man ehrlichiosis. J. Clin. Microbiol. 29:2741-2745.
10. Dawson, J. E. et al. 1990. Diagnosis of human ehrlichiosis with indirect fluorescent antibody test: Kinetics and specificity. J. Infect. Dis. 162:91-95.
11. Steere, A. C. 1989. Lyrne disease. N. Engl. J. Med. 321:586-596.
12. Rahn, D. W., and S. E. Malawista. 1991. Lyme disease: Recommenda- tions for diagnosis and treatment. Ann. Intern. Med. 114:472-481.
13. Boyer, K. M. et al. 1977. Tick-borne relapsing fever: An interstate outbreak originating at Grand Canyon National Park. Am. J. Epidemiol. 105:469--479.
14. Southern, P. M. and J. P. Sanford. 1969. Relapsing fever. Medicine 48:129-149.
15. Centers for Disease Control. 1991. Outbreak of relapsing fever----Grand Canyon National Park, Arizona, 1990. 40:296-303.
16. McDade, J. E. and V. F. Newhouse. 1986, Natural history of Rickettsia
rickettsii. Ann. Rev. Microbiol. 40:287-309.
17. Centers for Disease Control. 1990. Rocky Mountain spotted fever and hu- man ehrlichiosis United States, 1989. MMWR 39:281-284.
18. Salgo, M. P. et al. 1988. A focus of Rocky Mountain spotted fever within New York City. N. Engl. J. Med. 318:1345-1348.
19. Kirk, J. L. et al. 1990. Rocky Moun- tain spotted fever: A clinical review based on 48 confirmed cases, 1943- 1986. Medicine 69:35-45.
20. Rohrbach, B. W., E. Westerman, and G. R. Istre. 1991. Epidemiology and clinical characteristics of tularemia in Oklahoma, 1979-1985. South. Med. J. 84:1091-1096.
21. Evans, M. E. et al. 1985. Tularemia: A 30-year experience with 88 cases. Medicine 64:251-269.
22. Keirans, J. E. and T. R. Litwak. 1989. Pictoral key to the adults of hard ticks. Family Ixodidae (Ixodida: Ixo- doidea), east of the Mississippi River. J. Med. Entomol. 26:435--448.
Editorial
Continuing Educational Trends for Laboratory Personnel
Sandra L. Marubio Midwestern Area Resource Director National Laboratory Training Network Chicago, IL 60612
You are the key to quality labora- tory testing. Today, laboratorians are facing unprecedented challenges re- garding computerization, cost contain- ment, staff shortages, increasing regulations, and new technologies. In order to stay up-to-date and provide an active role in health care, laboratorians must look to continuing education pro- grams. Training is an ongoing pro- cess, and knowing what is available and planning for the future is the re- sponsibility of all laboratory profes- sionals. Being an integral part of a national training network dedicated to laboratory technology, I would like to share with you some timely topics that are being addressed through continuing education programs.
Current Topics of Interest Needs assessment data collected
over the past 2 yr show that topics most frequently requested in laboratory management are regulation updates including CLIA '88, safety, quality control, quality assurance, hazardous waste management, and proficiency testing. For the microbiology labora- tory, subjects identified for technical training include basic reviews, anaer- obes, parasitology (especially proto- zoan and Cryptospordium identification), mycology (KOH preps and yeast identification), and myco- bacteriology (direct acid-fast smears, rapid tests and antimicrobial suscepti- bilities, and DNA probes). For the virology laboratory there is interest in basic HIV (HIV-1 and HIV-2) updates; determination of HIV-1 antibody status by EIA and Western blots (immuno- blots); testing for hepatitis A, hepatitis B, and hepatitis non A and non B; virus isolation and identification meth- ods; and rapid direct detection tests for influenza and measles viruses. Flow cytometry is also of high interest for laboratories that do HIV testing.
Public Health Issues As the number of cases of active
tuberculosis increases, a potential cri- sis exists; therefore, it is important that laboratorians develop strategies to re- duce the turnaround time for detection and reporting of Mycobacterium tuber- culosis. With the recent reports of multi-drug-resistant tuberculosis, the laboratory can make a difference by providing services for early recogni- tion. In this way, patient management is enhanced and the subsequent spread of infection can be minimized by the early institution of appropriate control measures. Numerous courses are now offered to help the laboratory meet this new demand.
Availability of Training The Centers for Disease Control
continue to provide training on the new and emerging technologies. Many professional organizations (e.g., American Society for Microbiology, American Society of Clinical Patholo- gists, and American Society for Medi- cal Technology) provide training not only at the national, but also at re-
108 0196-4399/92/$0.00 + 03.00 © 1992 Elsevier Science Publishing Co., Inc. Clinical Microbiology Newsletter 14:14.1992
gional and state levels. State public health laboratories also provide train- ing; check with the state training coor- dinator for scheduled programs. Institutions such as Mayo Clinic offer numerous courses and wet workshops. University-based programs such as LEND (Laboratory Education for North Dakota) and Project Safari are meeting the need for training in rural areas. Industry continues to demon- strate a strong commitment to provid- ing training. Self-study packages are available through the Colorado Associ- ation for Continuing Medical Educa- tion (CACMLE) and the Medical College of Georgia. The Association of State and Territorial Public Health Laboratory Directors continues to ac- tively deliver training for laboratori- ans. The Teleconference Network of Texas provides training seminars on a routine basis.
One of the major problems in the past has been knowing where to find the specific training program that is needed. This problem can now be addressed. Through the National Lab- oratory Training Network, a National Laboratory Training Calendar data base exists that lists training activities throughout the country. By phoning one of the seven area resource offices with a subject, you will be given the title, sponsoring organization, date, and contact telephone number for that course. Also in place is the National Laboratory Training Resource Guide, which catalogs laboratory training ma- terials provided by federal, state, and local government agencies, academic institutions, professional organizations, and proprietary groups in laboratory educational activities. In addition, each office has available for loan (at no cost) training materials that you can use in your laboratory to meet your training needs. The training materials consist of laboratory technique manu- als, videotapes of laboratory proce- dures, slide sets, and training course packages. The training course pack- ages can be used for workshops, inser- vices, lectures, or personal continuing education. They include a facilitator
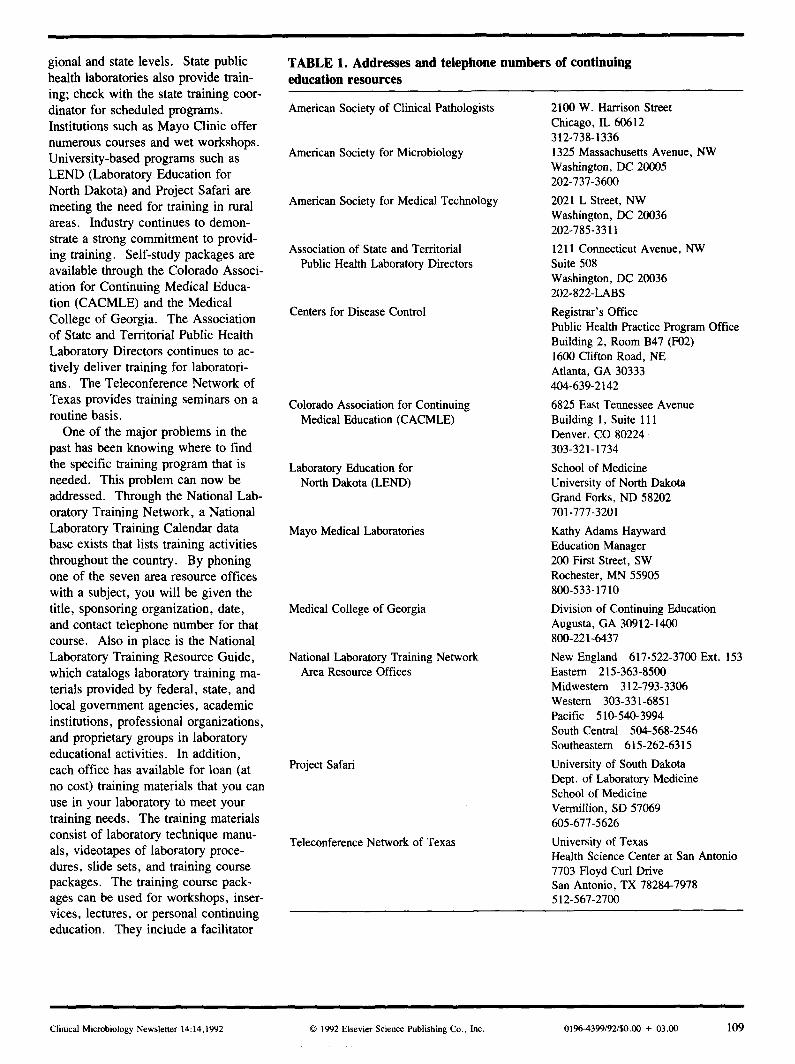
T A B L E 1. Addresses and te lephone n u m b e r s of cont inuing education resources
American Society of Clinical Pathologists
American Society for Microbiology
American Society for Medical Technology
Association of State and Territorial Public Health Laboratory Directors
Centers for Disease Control
Colorado Association for Continuing Medical Education (CACMLE)
Laboratory Education for North Dakota (LEND)
Mayo Medical Laboratories
Medical College of Georgia
National Laboratory Training Network Area Resource Offices
Project Safari
Teleconference Network of Texas
2100 W. Harrison Street Chicago, IL 60612 312-738-1336 1325 Massachusetts Avenue, NW Washington, DC 20005 202-737-3600
2021 L Street, NW Washington, DC 20036 202-785-3311
1211 Connecticut Avenue, NW Suite 508 Washington, DC 20036 202-822-LABS
Registrar's Office Public Health Practice Program Office Building 2, Room B47 (F02) 1600 Clifton Road, NE Atlanta, GA 30333 404-639-2142
6825 East Tennessee Avenue Building 1, Suite 111 Denver, CO 80224 303-321-1734
School of Medicine University of North Dakota Grand Forks, ND 58202 701-777-3201
Kathy Adams Hayward Education Manager 200 First Street, SW Rochester, MN 55905 800-533-1710
Division of Continuing Education Augusta, GA 30912-1400 800-221-6437
New England 617-522-3700 Ext. 153 Eastern 215-363-8500 Midwestern 312-793-3306 Western 303-331-6851 Pacific 510-540-3994 South Central 504-568-2546 Southeastern 615-262-6315
University of South Dakota Dept. of Laboratory Medicine School of Medicine Vermillion, SD 57069 605-677-5626
University of Texas Health Science Center at San Antonio 7703 Floyd Curl Drive San Antonio, TX 78284-7978 512-567-2700
Clinical Microbiology Newsletter 14:14,1992 © 1992 Elsevier Science Publishing Co., Inc. 0196-4399/92/$0.00 + 03.00 109

guide, lecture activities, "2 × 2" Ko- dachrome slides, and procedures for laboratory components. Audiocas- settes, manuals, or videotapes are in- cluded in some of the packages.
In order to meet these ever-changing
demands, there must be a cooperative effort from the bench-level technician, technologist, supervisor, laboratory director, and hospital administrators. Only through the pursuit of continuing education can the laboratory meet the
challenges of today and provide you with the key to tomorrow.
Table 1 lists addresses and tele- phone numbers of professional organi- zations that provide educational assistance programs and materials.
Case Report
Pseudoinfection Due to Simian Adenovirus
Ella M. Swierkosz, Ph.D. Diagnostic Virology Laboratory Cardinal Glennon Children's Hospital Department of Pathology and
Laboratory Medicine and St. Louis University School of Medicine Departments of Pediatrics and Pathology St. Louis, MO 63104
Tim Bonnot, MT(ASCP) St. Louis University School of Medicine, Departments of Pediatrics and Pathology, St. Louis, MO 63104
On February 6, 1991, a nasopharyn- geal swab specimen was submitted to the Diagnostic Virology Laboratory of Cardinal Glennon Children's Hospital, St. Louis University Medical Center. The swab was obtained from a 6-mo- old male who presented to the emer- gency room with a diagnosis of possible respiratory syncytial virus (RSV) infection. Upon receipt in the virology laboratory, the specimen was tested for RSV by enzyme immunoas- say (TESTPACK RSV, Abbott Labo- ratories, North Chicago, IL). Because of a negative TESTPACK RSV reac- tion, the specimen was inoculated into cell culture tubes for virus isolation: human embryonic kidney (HEK; Whit- taker Bioproducts, Walkersville, MD), MRC-5 (human diploid lung; Ortho Diagnostics, Inc., Raritan, N J), and primary rhesus monkey kidney (RhMK) from two sources (Viromed, Minnetonka, MN, and Whittaker Bio- products). HEK cells and one set of MRC-5 and RhMK tubes were incu- bated at 36°C while one set of MRC-5
and RhMK tubes was incubated at 33°C to optimize detection of rhinovi- rus and influenza viruses. On day 1 post-inoculation, adenovirus-specific cytopathic effect (CPE) was observed in a Viromed RhMK tube that had been incubated at 33°C. The isolate was confh'med as adenovirus by en- zyme immunoassay of the cell culture supernatant (Adenoclone, Cambridge BioScience, Worcester, MA) and a report was issued. No other cell cul- ture tubes inoculated with this speci- men were positive for CPE. Subsequently, adenovirus-specific CPE was observed in four additional Vi- romed RhMK that had been inoculated with other respiratory specimens. However, no adenovirus-specific CPE was observed in 61 Viromed RhMk tubes also inoculated with patient spec- imens. Because of our concern that the Viromed RhMK cells were con- taminated with simian adenovirus, three frozen ( - 70°C) original speci- mens that had shown adenovirus-spe- cific CPE only in Viromed RhMk were reinoculated to fresh cell culture tubes; all were ultimately culture nega- tive. In addition, these three speci- mens were tested by enzyme- immunoassay (Adenoclone) for the presence of adenovirus antigen and were also found to be negative.
Because adenovirus usually requires 5 to 13 d for isolation in cell culture (1), does not usually grow in RhMk, and because no other cell types, in particular the RhMk from Whittaker, were positive, we tentatively con- cluded that the Viromed RhMK were contaminated with a simian adenovi- rus. To confirm our suspicion, the first adenovirus isolate was sent to the Virus Reference Laboratory in San
Antonio, TX, where it was identified as simian adenovirus, SV 11, by neu- tralization with type specific antiserum (2).
Our experience underscores the ne- cessity for continual vigilance by labo- ratorians for the presence of nonhuman viruses in cell cultures. Latent virus infections of cell cultures derived from tissues of monkeys and non-primates have been well described (3, 4). Sim- ian viruses, particularly adenoviruses, herpes group viruses, and paramyxovi- ruses, are of special concern since pri- mary monkey kidney cell cultures are a mainstay of most diagnostic virology laboratories. Simian adenoviruses re- semble human adenoviruses by elec- tron microscopy, produce similar CPE in infected cell cultures, and share a complement-fixing antigen with human adenoviruses (3). Thus, commercial reagents that base adenovirus identifi- cation on the detection of the group- specific complement-fixing antigen, such as Adenoclone and Bartels adeno- virus-specific monoclonal antibody (Baxter Healthcare Corporation, West Sacramento, CA), cannot be relied upon to distinguish between human and simian adenoviruses.
In order to avoid misdiagnosis of simian virus contaminants as human isolates, we recommend using at least two sources of primary monkey kidney cells. Cytopathic effects produced in cells from one supplier but not in the other should be viewed with suspicion. We also recommend setting aside at least one tube from each lot of cell cultures without changing the medium. Thus any cytopathic changes observed in the segregated tube would be due to manufacturer-based contamination rather than to on-site contamination.
1 10 0196-4399/92/$0.00 + 03.00 © 1992 Elsevier Science Publishing Co., Inc. Clinical Microbiology Newsletter 14:14,1992